Embed Size (px)
Citation preview
Midwifery 29 (2013) 407–415
Contents lists available at SciVerse ScienceDirect
Midwifery
0266-61
http://d
n Corr
E-m
journal homepage: www.elsevier.com/midw
The woman’s birth experience—The effect of interpersonal relationshipsand continuity of care
Unn Dahlberg, Master of Science in Education (Midwife)a,n, Ingvild Aune,Master of Public Health (Midwife, Associate Professor)b
a St. Olavs University Hospital, Trondheim, Department of Women’s Health, Olav Kyrres gate 17, 7006 Trondheim, Norwayb Department of Postgraduate Nursing Programmes, Midwifery Education, Sør-Trøndelag Univercity College, Mauritz Hansens gate 2, 7004 Trondheim, Norway
a r t i c l e i n f o
Article history:
Received 10 April 2012
Received in revised form
11 September 2012
Accepted 18 September 2012
Keywords:
Birth experience
Continuity of care
Holistic view
Trust
38/$ - see front matter & 2012 Elsevier Ltd. A
x.doi.org/10.1016/j.midw.2012.09.006
esponding author.
ail address: [email protected] (U. Dahlb
a b s t r a c t
Objective: the aim of the present study was to gain a deeper understanding of how relational continuity
in the childbearing process may influence the woman’s birth experience.
Research design/setting: a Q-methodological approach was chosen, as it allows the researcher to
systematically assess subjectivity. 23 women were invited to sort a sample of 48 statements regarding
their subjective view of birth experience after having participated in a pilot project in Norway, where
six midwifery students provided continuity of care to 58 women throughout the childbearing process.
The sorting patterns were subsequently factor-analysed, using the statistical software ‘PQ’ which
reveals one strong and one weaker factor. The consensus statements and the defining statements for
the two factors were later interpreted.
Findings: both factors seemed to represent experiences of psychological trust and a feeling of team
work along with the midwifery student. Both factors indicated the importance of quality in the relation.
Factor one represented experiences of presence and emotional support in the relationship. It also
represented a feeling of personal growth for the women. Factor two was defined by experiences of
predictability in the relation and process, as well as the feeling of interdependency in the relation.
According to quality in the relation, women defining factor two experienced that the content, not only
the continuity in the relation, was important for the birth experience.
Key conclusions: relational continuity is a key concept in the context of a positive birth experience.
Quality in the relation gives the woman a possibility to experience positivity during the childbearing
process. Continuity in care and personal growth related to birth promote empowerment for both the
woman and her partner. Relational continuity gives an opportunity for midwives to provide care in a
more holistic manner.
& 2012 Elsevier Ltd. All rights reserved.
Introduction
In Norway, antenatal care is part of the primary health-careservice, whereas the specialist health service is responsible forintrapartum and postnatal care. This leads to fragmented serviceswhere women encounter several different people and professionalsinstead of care based on continuity and trusting relationships.
The quality of relationships is fundamental for the quality ofcare provided during pregnancy, childbirth and the postnatalperiod (Lundgren, 2004; Olafsdottir, 2006; Hunter et al., 2008).The relationship between the midwife and the woman combinesall the aspects of the midwifery service (Hunter et al., 2008).Several studies show that a trusting relationship between the
ll rights reserved.
erg).
woman and midwife is important for the emotional aspect relatedto the birth experience (Waldenstrøm et al., 2004; Lundgren et al.,2009; Leap et al., 2010; Lyberg and Severinsson, 2010; Aune et al.,2012). A woman’s fear of childbirth is often a result of previousnegative birth experiences. An important factor is a lack of qualityin the relationship with the caregivers (Waldenstrøm, 2004;Nilsson and Lundgren, 2009; Lukasse et al., 2010; Nilsson et al.,2010). Midwives have highlighted the importance of establishinga trusting relationship in order to make the woman confident thatthe midwife care about her as a unique person and not considerher as just another woman in the crowd (Lundgren and Dahlberg,2002). A trusting relationship represents a holistic perspectivethat involves opportunities for personal growth and development(Allgood, 1994/1995).
Dickson (1997) emphasised that caring in midwifery servicesis the best way for women to have a positive birth experienceand that the presence of a midwife, her communication skills,

U. Dahlberg, I. Aune / Midwifery 29 (2013) 407–415408
knowledge and understanding are critical factors. Accordingto Halldorsdottir and Karlsdottir’s theory (2011), the quality ofmidwifery services is a key aspect of the woman’s experienceof childbirth. They highlight five principal factors in a midwife’sprofession: The professional caring, which is at the heart ofmidwifery, the midwife’s competence and wisdom, the midwife’sinterpersonal skills and finally her personal and professionaldevelopment. If any of these factors are missing, the servicesbecome insufficient. Professional and individualised care isemphasised as part of an ambition to promote long-term happi-ness and a good life.
‘With Woman’ and ‘in partnership with women’ are termsassociated with good clinical results and a higher level of satisfac-tion. The emphasis is on a trusting midwife–woman relationshipbased on a phenomenological approach highlighting the woman’sexperience (Kirkham, 2000; Page, 2003; Carolan and Hodnett,2007). Interdependency is essential in a supporting relationship(Allgood and Kvalsund, 2005). Interdependency underscores themutual nature of the relationship and is characterised by trust(Allgood and Kvalsund, 2003), which is a measure of psychologicalconfidence (Rogers, 1961).
Several studies show that women benefit from a consistent,continuing relationship during the childbearing process (Fontein,2010; Sandall et al., 2010; Williams et al., 2010; Gagnon, 2011).The concept of relational continuity refers to a continuous processof pregnancy, birth and postnatal care. Haggerty et al. (2003)define relational continuity of care as ‘an on-going therapeuticrelationship between a patient and one or more providers’.This means that it is the same midwife or midwives who areresponsible for following up the woman and her partner through-out the process. Continuity of care is associated with the fact thatwomen feel better prepared for the birth and that they are moreconfidence and experience a positive birth (Sandall et al., 2010).National professional guidelines for antenatal care (The Directoratefor Health and Social Affairs, 2005) emphasise that continuity andconfidence are typical components of high-quality antenatal andintrapartum care.
This study is a part of a project at Sør-Trøndelag UniversityCollege in 2009–2010, which was implemented in cooperationwith the municipality of Trondheim and St. Olav’s Hospital. Sixmidwifery students provided continuity of care to 58 womenthroughout pregnancy, childbirth and the postnatal period. Theyoffered antenatal care and antenatal classes that enabled thestudents to develop a personal relationship with the women. Oneof the six students provided one-to-one care during the child-birth, and the same student was present during the postnatalhome visit. The students were always under the supervision of aprofessional midwife. The women were not selected, but volun-teered to participate in the project. They became involved duringweeks 16–18 of the pregnancy after signing a written informedconsent form. Inclusion criteria were low-risk pregnancy andthe ability to speak Norwegian. The Regional Research EthicsCommittee approved the project.
The aim of this study was to examine how relational con-tinuity through pregnancy and childbirth may influence the birthexperience.
Methodology
Design
A retrospective Q-methodology study involving 23 womenfrom the project described earlier was conducted between threeand eight months post partum. These women experienced con-tinuity of care throughout pregnancy, childbirth and postnatal
period. The Q-methodology is based on the principle thatsubjective views are communicable, and constitutes a tool forsystematic study in order to obtain an understanding of personalexperience (Brown, 1993). In this study, Q-methodology has thepotential of discovering patterns or perspectives with regard towomen’s experience of the relational continuity of care andthe birth experience. The methodology consists of five stages:(1) developing the concourse, (2) sampling the concourse, (3)constructing the Q sample, (4) sorting the Q sample, and (5)analysis and interpretation.
The concourse and representative sample
The ‘Concourse’ represents the universe of possible communica-tion regarding a topic; in this case relational continuity and birthexperience. A representative sample of the ‘concourse’ is respondedto and in that process the underlying structure can be made visibleand meaningful Discoveries emerge (Brown, 1993). The represen-tative sample was derived from several sources. Statements weregathered from the women who participated in the project. Six toeight weeks post partum the 58 women answered a questionnaireand added comments and thoughts related to their experiencesfrom participating in the project. Eight of the participants attendeda group interview two months post partum where their experienceof continuity of care was the topic. Theory and research on thephenomenon also provided source material from the concourse,which was used for the sample.
Constructing the Q sample
Experimental design is primarily a structured way for research-ers to express their theoretical basis, and it also acts as a guide toselect the Q sample from a population of statements (Brown,1993). Fisher’s experimental block design provides opportunitiesfor systematic thinking about a phenomenon (Kvalsund, 1998)while creating a temporary structure and providing internalvalidity (Brown, 1993). The dimensions or criteria that are implicitin the design reflect the discussion about the phenomenon(McKeown and Thomas, 1988).
The design reflects a theoretical structure of continuity inmaternity care, which is based on relational continuity and birthexperience (Table 1). The selected foci or effects derived from theconcourse are the Interpersonal relation, Psychological trust andView of man. The levels for the Interpersonal relation weredependency, independency and mutuality. The levels for Trustwere positive trust and lacking trust. The levels for View of manwere fragmented and holistic. Four replications of each cell werechosen, resulting in 48 statements that created a sample forQ-sorting. The aim at this stage is to select the number of state-ments per combination on the basis of balance. All effects musthave the same presentation and heterogeneous representation,which mean that there should be as many statements as possiblewith the same structural logic (Kvalsund, 1998). The statementsare numbered and randomised before being presented to theparticipant in the form of cards were each card represents astatement. On the basis of feedback from two pilot participants,changes were made in the formulation of some statements.Finally, the two researchers together assessed the cell placementand balance of the sample.
The P-set
Forty-six women in the project who experienced very goodcontinuity of care and were satisfied with the care in general wereinvited by mail to participate in this study. Twenty-three womenvolunteered to participate and they became the population set or
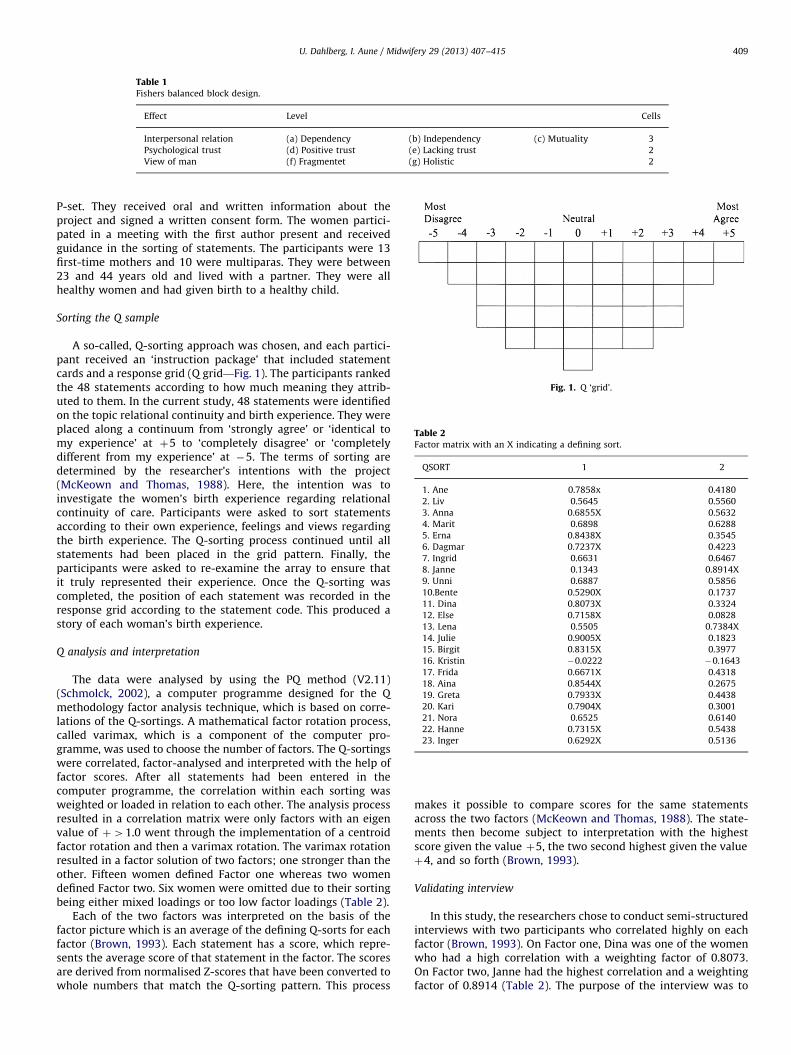
Fig. 1. Q ‘grid’.
Table 2Factor matrix with an X indicating a defining sort.
QSORT 1 2
1. Ane 0.7858x 0.4180
2. Liv 0.5645 0.5560
3. Anna 0.6855X 0.5632
4. Marit 0.6898 0.6288
5. Erna 0.8438X 0.3545
6. Dagmar 0.7237X 0.4223
7. Ingrid 0.6631 0.6467
8. Janne 0.1343 0.8914X
9. Unni 0.6887 0.5856
10.Bente 0.5290X 0.1737
11. Dina 0.8073X 0.3324
12. Else 0.7158X 0.0828
13. Lena 0.5505 0.7384X
14. Julie 0.9005X 0.1823
15. Birgit 0.8315X 0.3977
16. Kristin �0.0222 �0.1643
17. Frida 0.6671X 0.4318
18. Aina 0.8544X 0.2675
19. Greta 0.7933X 0.4438
20. Kari 0.7904X 0.3001
21. Nora 0.6525 0.6140
22. Hanne 0.7315X 0.5438
23. Inger 0.6292X 0.5136
Table 1Fishers balanced block design.
Effect Level Cells
Interpersonal relation (a) Dependency (b) Independency (c) Mutuality 3
Psychological trust (d) Positive trust (e) Lacking trust 2
View of man (f) Fragmentet (g) Holistic 2
U. Dahlberg, I. Aune / Midwifery 29 (2013) 407–415 409
P-set. They received oral and written information about theproject and signed a written consent form. The women partici-pated in a meeting with the first author present and receivedguidance in the sorting of statements. The participants were 13first-time mothers and 10 were multiparas. They were between23 and 44 years old and lived with a partner. They were allhealthy women and had given birth to a healthy child.
Sorting the Q sample
A so-called, Q-sorting approach was chosen, and each partici-pant received an ‘instruction package’ that included statementcards and a response grid (Q grid—Fig. 1). The participants rankedthe 48 statements according to how much meaning they attrib-uted to them. In the current study, 48 statements were identifiedon the topic relational continuity and birth experience. They wereplaced along a continuum from ‘strongly agree’ or ‘identical tomy experience’ at þ5 to ‘completely disagree’ or ‘completelydifferent from my experience’ at �5. The terms of sorting aredetermined by the researcher’s intentions with the project(McKeown and Thomas, 1988). Here, the intention was toinvestigate the women’s birth experience regarding relationalcontinuity of care. Participants were asked to sort statementsaccording to their own experience, feelings and views regardingthe birth experience. The Q-sorting process continued until allstatements had been placed in the grid pattern. Finally, theparticipants were asked to re-examine the array to ensure thatit truly represented their experience. Once the Q-sorting wascompleted, the position of each statement was recorded in theresponse grid according to the statement code. This produced astory of each woman’s birth experience.
Q analysis and interpretation
The data were analysed by using the PQ method (V2.11)(Schmolck, 2002), a computer programme designed for the Qmethodology factor analysis technique, which is based on corre-lations of the Q-sortings. A mathematical factor rotation process,called varimax, which is a component of the computer pro-gramme, was used to choose the number of factors. The Q-sortingswere correlated, factor-analysed and interpreted with the help offactor scores. After all statements had been entered in thecomputer programme, the correlation within each sorting wasweighted or loaded in relation to each other. The analysis processresulted in a correlation matrix were only factors with an eigenvalue of þ41.0 went through the implementation of a centroidfactor rotation and then a varimax rotation. The varimax rotationresulted in a factor solution of two factors; one stronger than theother. Fifteen women defined Factor one whereas two womendefined Factor two. Six women were omitted due to their sortingbeing either mixed loadings or too low factor loadings (Table 2).
Each of the two factors was interpreted on the basis of thefactor picture which is an average of the defining Q-sorts for eachfactor (Brown, 1993). Each statement has a score, which repre-sents the average score of that statement in the factor. The scoresare derived from normalised Z-scores that have been converted towhole numbers that match the Q-sorting pattern. This process
makes it possible to compare scores for the same statementsacross the two factors (McKeown and Thomas, 1988). The state-ments then become subject to interpretation with the highestscore given the value þ5, the two second highest given the valueþ4, and so forth (Brown, 1993).
Validating interview
In this study, the researchers chose to conduct semi-structuredinterviews with two participants who correlated highly on eachfactor (Brown, 1993). On Factor one, Dina was one of the womenwho had a high correlation with a weighting factor of 0.8073.On Factor two, Janne had the highest correlation and a weightingfactor of 0.8914 (Table 2). The purpose of the interview was to

U. Dahlberg, I. Aune / Midwifery 29 (2013) 407–415410
verify the interpretation and try to get a deeper understanding ofthe factors. They both found it easy to sort and the statementsproved relevant for their birth experience. During the sorting pro-cess they revisited their experiences and emotions from the birth.
Findings
Consensus between the factors
From Table 2 the scores from Anna, Hanne and Inger correlaterelatively strongly with Factor two but are significant with Factorone. This means that even if the factors are quite recognisablethere seems to be certain similarities between the two factors.By looking at examples sorted for each factor and by comparingand studying the importance of scores between the factors, weare able to identify different and more nuanced meanings. A fewselected examples are highlighted here. The ranking of each factoris shown in brackets (Factors one and two).
A common feature of both factors is the importance ofrelational continuity; having an established relationship withthe person who provides care (Statements 21, 43, 14). This viewis based on the process of continuity that affects psychologicalconfidence and trust, which are also evident in both factors (43,14). The women with the most positive overall score on Factorsone and two (þ4, þ5) represent the vision that marks factor 2;the feeling of being part of a team during the childbearing process(Table 3).
Table 3Consensus statements.
21. I felt that the birth was a team work between me,
my husband and the midwifery student. It was an
amazing experience to be accompanied by a person
who knew my needs and thoroughly understood me. (þ4, þ5).
43. The fact that I knew someone familiar who would be
present during the birth, made me confident and calm
as the birth got underway (þ3, þ5)
14. I felt confident during the birth as I knew the one who
was with me. She was close and supportive, and it made
my birth experience very positive. I think both the student
and I have grown from this experience (þ5, þ2)
36. The fact that I got safely through my birth is something
I should have the whole credit for. I will definitely not have
more children (�4, �5)
31. The fact that she seemed so absent made
the experience traumatic (�4, �3)
Table 4Key statement in factor 1.
Statement 2 She was there for me all the time. I was given attention and take
handle the birth in a positive way (Bdg)
Statement 14 I felt confident during the birth as I knew the one who was with
and it made my birth experience very positive. I think both the s
Statement 30 She made me feel like the best, it was fantastic to know that I w
I’m very proud of myself (Adg)
Statement 44 The fact that she was present for me all the time, understood m
made me feel free, safe and gave confident in my own strengths
Statement 10 Her ability to be present for us all the time, made me and my hu
We felt a mutual trust and warmth that was very important in c
Statement 13 The fact that we knew each other already, her care and ability to
my husband made me feel confident during the birth and contri
Statement 12 I felt that she was present for me all the time, yet it did not mak
Statement 16 It was nice to get help, she respected my decisions but still I wa
Statement 27 I did not have a positive birth experience, partly because I was n
Statement 31 The fact that she seemed so absent made the experience trauma
Statement 46 After this birth, I have become even more afraid of giving birth.
Factor one includes three themes; emotional presence, caring and
personal growth
15 women defined Factor one. Concepts such as presence,emotional support and trust are emphasised in this factor.Furthermore, it appears that personal growth and developmentare highlighted as a separate view related to this factor. Table 4shows the key statements in Factor one with rounded scores andscores in Factor two in brackets.
The women who contribute most to a positive definition ofFactor one (þ5, þ4) clearly emphasise the presence of themidwifery student and the growth potential of the relationship.Both statements placed on þ5 seem to have a focus onphenomena like closeness and presence. Being present implicitlydenotes closeness in the relationship. This seems to be at theheart of what gives meaning for the women defining Statementstwo and 14. A sense of personal closeness in the relationshipmay indicate a relationship based on interdependence betweenthe woman and the midwifery student, as well as the feeling ofpsychological trust. Confidence and trust are stressed as neces-sary factors for a positive birth experience (Statement 14). Itseems like the psychological confidence the women experiencedis related to a relational process where trust is established beforebirth. Of great importance for these women is the feeling ofgetting the attention of the person who provides the care. This isinterpreted as a desire to be met with holistic values, whereelements like congruence, acceptance and empathy are domi-nant (Statement 2). The statement ‘She paid attention to me andmy needs’ (Statement 44) indicates that the women find itimportant to be approached with a holistic perspective whichreflects that every person is unique and valuable. Important hereis the presence of the midwifery student and ‘awareness’ in thepersonal encounter. This is also important for the women’s birthexperience.
To be cared for and supported in connection with childbirthseems to be very important for women who define Factor onein the most positive way (Statement 2). To be taken care of maycontain several dimensions in an assisting relation. Here, it isinterpreted in the context of women attaching importance todependence in the relationship with the caregiver. To be takencare of may also contain the sense of psychological trust, emo-tional support and closeness (Statements 14 and 10). A sense ofmutuality in the relationship is related to an experience ofpositive trust and a feeling of human warmth (Statement 10).A feeling of warmth in the relation gives associations to qualitiessuch as congruence and empathy, which are in turn emphasisedas important for a positive birth experience.
n care of and this made me þ5 (0)
me. She was close and supportive,
tudent and I have grown from this experience (Cdg)
þ5 (2)
orked with the strength of the birth and not against it, þ4 (2)
e and knew what I needed,
during birth (Cdg)
þ4 (0)
sband confident.
reating a good experience (Cdg)
þ3 (3)
be there for me and
buted to a positive birth experience (Adg)
þ3 (3)
e me feel secure and I therefore had to rely on myself (Beg) 0 (�1)
s not confident (Aeg) 0 (1)
ot paid attention to during the birth (Cef) �4 (�2)
tic (Aef) �4 (�3)
I had no confidence in those who said they would help me (Cef) �5 (1)

Table 5Key statement in factor 2.
Statement 43 The fact that I knew someone familiar who
would be present during the birth,
made me confident and calm as the
birth got underway (Bdg)
þ5 (3)
Statement 21 I felt that the birth was a team work between me,
my husband and the midwifery student.
It was an amazing experience to be accompanied
by a person who knew my needs and thoroughly
understood me (Adg)
þ5 (4)
Statement 4 It was so nice to have someone there who I knew
and who was more familiar with this than me.
Still, I just wanted run away from all of it (Adf)
þ4 (2)
Statement 8 I felt that it was helpful because we knew
each other, and it made things turn out well,
but it was not a positive experience (Cdf)
þ4 (1)
Statement 9 I was so confident and coped with my own birth
because I knew the one who was going to assist
me and I could trust the help she gave me (Bdg)
þ3 (2)
Statement 13 The fact that we knew each other already,
her care and ability to be there for me and
my husband made me feel confident during the
birth and contributed to a positive birth
experience (Adg)
þ3 (3)
Statement 6 We really had good contact and she was always
present to help me, yet I felt that she did not
listen to what I said (Aeg)
0 (1)
Statement 16 It was nice to get help, she respected my
decisions but still I was not confident (Aeg)
0 (�2)
Statement 36 The fact that I got safely through my birth is
something I should have the whole credit for.
I will definitely not have more children (Bef)
�5 (�4)
Statement 26 Even though she was there all the time,
I felt she was not there for me, she was inattentive
and not very supportive (Aef)
�5 (�3)
U. Dahlberg, I. Aune / Midwifery 29 (2013) 407–415 411
The women’s experience of personal growth in relation tochildbirth is clearly evident in both the statements of þ5(Statements two and 14). The women who rated Statement 14as the most positive one (þ5) tend to experience a feeling ofmutuality with regard to the growth perspective in the relation-ship. An interpretation of this is that the interdependency withthe midwifery student has been a positive experience and thatthis perspective has affected the birth experience. Both state-ments of þ4 give further meaning to Factor one and are morefocused on personal growth as a possibility in interpersonalrelationships (Statements 30 and 44). By feeling clever, free andself-confident, it seems that the women experienced personalgrowth in connection with their childbirth (Statement 44). Thefeeling of an inner pride related to the childbirth is emphasised asimportant (Statement 30), and it also seems that this may haveproduced a feeling of ‘empowerment’. This emphasises theimportance of a positive atmosphere surrounding the birth as afactor that promotes personal growth for the individual woman.Furthermore, Factor one emphasises that women are concernedabout the relationship with her partner during childbirth. It isimportant for the women that their partners feel confident(Statement 10). The partner’s experience of presence and close-ness in the relationship was important for women in Factor one(Statement 13). This indicates that it is important to include thewoman’s partner in the relational process.
The negative side of Factor one seems to confirm the views onthe positive side. Statements that are most negative (�5 and �4)include a lack of trust and confidence, a fragmented perspectiveand an absence of closeness in the relationship with the caregiver.This supports the idea that attention to process, quality andvarious aspects in the relationship are important. It seems thatanxiety associated with childbirth is related to the level of trustexperienced in the relationship (Statement 46), and a relationshipwhich is not viewed in a holistic perspective leads to negativeassociations regarding childbirth (Statement 27). Furthermore,it appears that the lack of closeness in relation to the caregiver maybe associated with a negative birth experience (Statement 31).
Factor two includes three themes; predictability, quality of relation
and being part of a team
There are two women who help define Factor two (Table 4),where confidence and team work are prominent themes. Accordingto this view it is not sufficient to know the midwifery student. Theimportant thing is the quality of the relationship; in other words, thecontent of it. Furthermore, the concept of predictability is evident inthis factor.
Table 5 shows the key statements in Factor two with roundedscore and scores in factor one in brackets.
The women who define this factor in the most positive way(þ5, þ4) are clearly concerned about confidence in relation tothe caregiver. Both statements placed on þ5 tell us somethingabout the importance of the relationships which have beenestablished in the early stages of pregnancy. The relationshipenables people to get to know each other, it facilitates a holisticview and makes both the woman and the midwifery studentconfident during the childbirth (Table 5). It also seems thatmeeting a familiar person helps women stay calm and confidentwhen preparing for the birth (Statement 43). Furthermore,being in a relationship with someone who puts emphasis on aholistic perspective is important for the view that defines Factortwo. Being confident in the relationship and being cared forare important aspects (Statement 21). This could indicate thatwomen wish predictability during pregnancy and childbirth,and that positive relationships are required to create morepredictability.
Statements placed on þ4 are both concerned with havingsomeone familiar present during birth. However, it does not looklike it is enough to know the midwifery student. Both Statementsfour and eight indicate that knowing the caregiver is not sufficientfor a positive birth experience. An interpretation of this is thatother elements than the relationship could influence the birthexperience. Here, several perspectives may be highlighted. It wasappreciated to have a familiar person present, but the womanwould still like to escape the whole situation (Statement 4).Childbirth is not just a mental experience; it is also a greatphysical strain. In addition to internal forces, unpredictable exter-nal factors, such as pain and complications, may have an impact.Statement eight describes the view that even if the childbirthwent well, it was hardly a great experience (Table 5). In relationto the theoretical design of the study these two statementsrepresent a fragmented perspective. They seem to rely on aperspective where the relationship is seen as negative, and wherethe woman does not feel she was taken care of. It is not enough tohave a relationship with the caregiver; it is the quality of therelationship that is the most significant factor. The vision whichrepresents statements placed on þ3 confirm the view that waspreviously highlighted in Factor two relating to confidence as animportant and positive part of the experience (Table 5).
Being in a team with the midwifery student represents aseparate view in Factor two. This view is advocated by the womenwho have placed statements related to the importance of being ina team with the midwifery student during the birth at þ5(Statement 21). This could be interpreted to mean that the womenexperienced mutual dependency as a positive experience and thatthe relationship during childbirth was marked by congruence,trust, respect and mutuality. This view also gives meaning to themidwifery student. In order to satisfy the woman’s needs, it isimportant to work ‘with the women’ rather than ‘for the woman’.

U. Dahlberg, I. Aune / Midwifery 29 (2013) 407–415412
This implicitly underscores the significance of being aware of one’srole as a caregiver in relation to the woman.
Factor two can generally be seen as an indication that thedimension of dependence is more important than mutuality inthe relationship with the midwifery student during the childbirth(Statements 43, 21, four and eight). This means that the quality ofthe relationship seems to be more important and that quality tellssomething about the potential for mutuality in the relationship.
Statements scoring þ3 on Factor two confirm the significance ofexperiencing trust in the relationship (Statement nine). Havingconfidence in the midwifery student tells something about thepsychological trust that is present in the relationship. Statement 13supports the view that women want to be part of a team duringbirth. The ability of both the woman and her partner to be presentseems to boost the confidence of the woman and may subsequentlyresult in a good experience. Both statements placed on þ3 refer to atheoretical design where confidence and a holistic perspective areemphasised. The perspective of mutuality does not emerge as themost important factor in relation to the theoretical design. It lookslike the view that represents Factor two to some extent depends onthe personality of the caregiver, but that the woman also wishes tobe part of a team and on equal footing with the caregivers. This isinterpreted as an emphasis on both dependency and mutualityamong the women who define Factor two.
The opposite side of Factor two confirms this view by the state-ments placed most negatively (�5) and reflects a lack of emotionalsupport, attention and presence on the part of the caregiver.Statement 36 confirms that a lack of emotional support does notprovide a good birth experience, and that future pregnanciesare not wanted because of this (Table 5). Statement 26 supportsthat being present or familiar with the midwifery student is notsufficient; the quality and dimensions of the relationship are thedecisive factors.
Discussion
The qualities of interpersonal relations and its impact
on the birth experience
Women’s positive experience of relational continuity throughpregnancy, childbirth and post partum was a common feature of thetwo factors. Hunter et al. (2008) emphasise this important perspec-tive. The visible factors in maternity care are the clinical outcomesand technology, whereas the relationships that hold it all togetherare a hidden factor in the final result and difficult to measure.
The women in the study thought that experiencing closenessto the midwifery student was important for their birth experi-ence. To be close at a personal level depends on a relationshipthat is genuine, where you approach the woman with a holisticperspective (Rogers, 1961). The main factor causing a negativebirth experience are midwives who do not listen to the needs ofthe woman and her partner while displaying a lack of emotionalsupport during the birth (Nilsson et al., 2010). Empathic knowl-edge (Rogers, 1961) is essential in order to get close to the womanand her partner. This provides opportunities for ‘awareness’ in thepersonal meeting (Hostrup, 2009).
When the midwife is present and close to the woman it helpsthe woman to face the unknown, to trust her own body and herown abilities (Lundgren, 2004). Psychological confidence in therelationship between the woman and the midwife is important forthe emotional aspect related to childbirth (Leap et al., 2010; Lybergand Severinsson, 2010). In order to be emotionally supportiveand close to the woman during birth, confidence already estab-lished during pregnancy is a key factor (Thorstensson et al., 2008).
The feeling of warmth in the relationship could be linked to factorslike confidence and closeness (Spurkeland, 2005).
It may seem difficult for confidence and trust to emerge duringa period of a few hours. The women in this study thought that thefeeling of confidence was important for their birth experience.Psychological trust in the relationship could come as a result ofrelational continuity during the childbearing process (Hunteret al., 2008). This supports what the women highlighted; theimportance of establishing a relationship during pregnancy inorder to create confidence during birth.
The women emphasised that it was important to get attentionand encounter an attitude based on a holistic perspective.This view requires an individual approach where each individualis considered unique and valuable (Allgood, 1994/1995). It alsorequires awareness of interdependency and community in therelationship (Kvalsund, 2005). On a maternity ward where thepractice is to provide care to several women at the same time,distance may be a natural consequence. Midwives adopt the roleof an ‘expert’, in which she knows what is best for the woman(Blaaka, 2002; Allgood and Kvalsund, 2005).
The women in this study thought it was important to be takencare of by those who provide the care. Dependence on supportingrelationships is characterised by the need to rely on the compe-tence of others (Kvalsund, 1998). Women trust the expertise andadvice of the midwife when there is continuity in the relationship(Leap et al., 2010). At this stage, women may feel vulnerable andin some cases prefer to be at the mercy of their midwife. Thewomen depend on the midwife for her personal development andgrowth (Allgood and Kvalsund, 2005).
Predictability during pregnancy and childbirth was importantfor the women in this study. By establishing a relationship duringthis period, the unpredictability is reduced. The women stressthat relationships are an important part of the transition tothe unknown during pregnancy (Lundgren, 2004). Predictabilityis associated with the experience of trust in the relationship(Spurkeland, 2005). Lyberg and Severinsson (2010) found thatwomen with previous negative birth experiences were betterprepared for the birth in cases where there was a trusting relation-ship between the woman and the midwife. Allgood and Kvalsund(2005) point out that predictability is linked to a more maturephase in the relationship where mutual dependence is developed.The bureaucratic organisation of care during pregnancy andbirth in Norway may prevent women from having the opportunityto experience predictability in the relationships. This could resultin the women depending more on the relationship than theyactually want. If women feel this need as something negative,it could create distance and lack of trust between the midwifeand the woman giving birth (Kvalsund, 2005). Where womenare met with a top-down approach from a midwife when establish-ing the relationship in the maternity ward, the woman tendsto adopt a passive role of dependency in the relationship (Blaaka,2002).
The women in this study highlighted the quality of therelationship as important for their birth experience. Continuityin the relationship is linked to the ability to provide care of highquality (Hunter et al., 2008; Sandall et al., 2010). Studies showthat quality in the relationship creates mutuality and trust. Theseare qualities that make relationships meaningful (Olafsdottir,2006; Hunter et al., 2008). A meaningful relationship is basedon interdependency which facilitates personal growth (Allgoodand Kvalsund, 2005). Midwifery care based on a fragmentedperspective with a focus on object, disease and diagnosis willnot pay attention to the relational aspects of midwifery care(Blaaka, 2002). Satisfaction with care and the quality of interper-sonal relationships is difficult to measure (Hunter et al., 2008).By focusing on the relational process, and not only on the event

U. Dahlberg, I. Aune / Midwifery 29 (2013) 407–415 413
itself, it becomes easier to achieve a high-quality relationship(Kvalsund, 2005).
Not all the women in the study had a good birth experience,even if they experienced satisfaction with the continuity of care.According to Carolan and Hodnett (2007), satisfaction with the caredoes not necessarily give a good birth experience. Waldenstrom(2004) found that pain in labour, medical procedures and compli-cations were factors associated with a negative birth experience. Inthe interview with Janne, this phenomenon is well documented.One year after birth she had a positive birth experience and thiswas due to the care provided and confidence she developedthrough the relationship. Studies show that what women remem-ber after birth is the emotional support they received from mid-wives (Waldenstrom, 2004).
A midwife who is not confident in herself will not be able topromote a high-quality relationship (Rogers, 1961). The quality ofthe relationship depends on trust and can be viewed as interactionexperienced over time (Spurkeland, 2005). It is also important toreflect on what it means to be congruent in the relationship andwhat it means to show an empathic understanding towards thewoman and her partner (Rogers, 1961). Congruence can be experi-enced as a genuine interest and understanding of the individualwoman and her birth. It is also important to be aware that trustneeds to be nurtured if it is to be maintained (Spurkeland, 2005).Trust can be developed through displaying interest and involve-ment in the situation of the woman and her partner. Equally, toshow and share enjoyment together with the couple may be animportant factor. Interpersonal competence is emphasised in thetheory of Halldorsdottir and Karlsdottir (2011). This theory high-lights that the midwife has the ability to connect and co-operatewith the woman towards a shared goal. Cooperation between thewoman and the midwife is at the heart of the theory and is basedupon the care, competence and insight of the midwife. Hunter et al.(2008) stress that all kinds of procedures, formulate on of objec-tives, equipment and policies are of limited value as long as therelationship between the woman and the midwife is not optimal.
Although the current organisation of maternity care in Norwayaims at establishing a secure framework and continuity (TheDirectorate for Health and Social Affairs, 2005; Ministry of Healthand Care Services, 2009), this may prove difficult in an environ-ment where fragmentation and an object-oriented focus prevail(Blaaka, 2002). An organisation in which the midwife has to assistseveral women at the same time makes it difficult to create spacefor relationships and confidence-building. The dominant perspec-tive tends to measure quality in terms of complications andmortality (Blaaka, 2002).
There is an association between negative memories of the birthexperience and the perception of the caregiver or staff as beingnegative or ‘rushed’ (Rijnders et al., 2008). Midwives and obste-tricians have different ideologies (Blaaka, 2002) and this causesmajor challenges for midwives. According to Bluff and Holloway(2008), this creates the risk of midwives following the doctor’sprescriptions and not paying attention to the women’s needsduring labour. Facilitating normal pregnancy and birth rather thanintervening medically requires midwives to develop both self-confidence and trust in the physiological process (Gagnon, 2011).
Mutuality and its impact on the birth experience
A common view in the study was that team work is importantfor the birth experience. This involved being included in a teamwith a familiar person who was able to pay attention to thecouple and their needs. In this way, a positive birth experiencewill be related to relationships that are developing towards amature phase (Allgood and Kvalsund, 2005). It indicated that thewomen in the study experienced mutuality in the relationship.
The women who advocated this view emphasised a sense ofpersonal growth and development as important for a positiveexperience of the childbearing process. When forging a closerelationship with the woman and her partner the midwife ispresent in all parts of the relationship and has the ability tomotivate and facilitate personal growth (Allgood, 1994/1995;Hunter et al., 2008). This was typical of the women in the studywho felt an inner pride a long time after their births and whoenjoyed a positive experience during the postnatal period.Thomson and Downe (2010) highlight that in order to achieve apositive birth experience it is vital that the woman is ’connected’to the midwife. In a model of continuity of care this ’connection’ isbased on trust, mutuality and respect. The women’s sense of prideand accomplishment after birth enhance their confidence andself-esteem. According to Lundgren (2004) and Nilsson andLundgren (2009), a relationship based on trust between themidwife and the woman strengthens the woman’s confidenceand her sense of inner strength to handle the birth. This may givethe woman the opportunity to experience a positive birth andreduce the risk of suffering during the childbirth (Nilsson andLundgren, 2009). Women with a previous negative birth experi-ence emphasise that they lack faith in their ability to give birthcombined with having limited confidence in the maternity careprovided (Nilsson et al., 2010).
The women in this study emphasised the interdependencerelated to growth and development as important for the birthexperience. When the women highlight the interdependence asa positive experience, it indicates that the relationship hascontinued over time (Allgood and Kvalsund, 2005; Spurkeland,2005). A supporting relationship must be based on the woman’sneeds and the caregiver’s competence. When the relationshipis developing positively, it will gradually be characterised bya greater degree of mutuality (Allgood and Kvalsund, 2003).Relational continuity of care provides opportunities for boththe midwives and women to get to know each other and tobuild trust and relationship, which gives both a sense of‘empowerment’ (Kirkham, 2000; Lundgren, 2004). Midwiveslearn a great deal about themselves through their work withthe women, helping to improve their self-awareness (Gagnon,2011).
For the women in the study it was important that their partnerexperienced confidence and trust in the relationship in order forthe birth to become a positive experience. The need to include thepartner says something about the importance of having a familyfocus that could lead to ‘empowerment’ for the whole family.The partner’s emotional support for the woman is valuableand promotes the well-being of the new family (Premberg et al.,2011). In organisations where a scientific approach to childbirthis common, there may be cases where the partner is not ableto get involved in the way preferred by him and his partner(Blaaka, 2002).
Midwifery care where midwives ‘work with’ rather than ‘for’the woman, paves the way for holistic care (Kirkham, 2000; Sandallet al., 2010). Emotional, physical, spiritual and psychologicalpresence in the relationship is central to the philosophy under-pinning the concept of ‘being with women’ in midwifery care(Kirkham, 2000; Hunter et al., 2008). This supports Rogers’ (1961)theory about what is important when establishing a relationship.‘Being with woman’ involves creating a trustful relationshipbetween the midwife and the woman that will enable personalgrowth. It was important for the women in this study to have afamiliar person they could trust and relate to during the birth.These types of relationships are valuable and meaningful, also fromthe perspective of the midwife. Being ‘with woman’ throughout theprocess is different from providing random and fragmented careto a number of women (Olafsdottir, 2006; Sandall et al., 2010).

U. Dahlberg, I. Aune / Midwifery 29 (2013) 407–415414
This difference could reflect the difference between a phenomen-ological and a scientific approach to an individual (Blaaka, 2002).By relying on a phenomenological approach to the woman, theunderstanding of the community’s importance is included as a keydimension (Kvalsund, 1998; Allgood and Kvalsund, 2005). Theapproach includes a holistic perspective that does not distinguishbetween the profession and the individual (Allgood and Kvalsund,2003).
Factors one and two represent some common views on what isimportant for a positive birth experience. The significance of therelational continuity has been highlighted along with the need forpsychological trust in the relationship. Both factors emphasise thequality of the relationship as important, but the importance ofquality is perceived differently for the women in Factors one andtwo. Women defining Factor one stress closeness and individualcare as important aspects of quality. The women who rely on thisperspective may have a greater need for dependence in relation tothe midwife (Allgood and Kvalsund, 2005). For the women whodefined Factor two, the personal dimension was important intheir perception of quality. This indicates the importance of themidwife’s self-confidence in order to be able to promote quality inthe relationship (Allgood and Kvalsund, 2005). These womenwere more concerned about the predictability of the relationshipthan the ones relying on the perspective reflected in Factor one.This may explain why women in Factor two experienced inter-dependence in the relationship as important for their birthexperience. For the women who emphasised Factor one, it wasimportant to experience personal growth, whereas those stressingFactor two were more concerned about the experience of mutual-ity in the relationship. This may be associated with a maturephase in the relationship. It appears that the growth perspectiveis important in both factors, though in different respects.To experience interdependence, which leads to independence,implies the ability to identify both dependence and independenceas important aspects in the relationship (Allgood and Kvalsund,2005).
Verifying the interviews
The two interviews confirm the researchers’ interpretations ofthe findings. Factor two included a point that required clarifica-tion. The women who defined Factor two felt confident and takencare of, but they did not have a positive birth experience.
For Janne, this perspective was quite obvious. She experiencedthe pain during labour overwhelmingly and much more challen-ging than she had imagined. After birth, she did not have thefeeling of pride that was typical of Factor one. The experience ofpain was with her for a long time even if she had a good experi-ence of the process. When she managed to put some distancebetween herself and the birth experience, it became a morepositive memory.
Limitations
Through its design the study is limited to include only certaineffects and levels. Participants gave their own meaning to thestatements, which made it necessary to subject the results of thefactor analysis to interpretation. As the researchers were involvedin the project ‘continuity through pregnancy, childbirth and thepostnatal period’ there is a risk that the themes and issues in thisstudy may be given too much emphasis compared to how theparticipants perceive them. The focus of the study, choice oftopic, participants and interpretations are always coloured bysubjectivity. It is therefore important to recognise subjectiveinfluences and include them as important aspects in the researchprocess. The interpretation of the various factors is a subjective
process based on the ability to draw conclusions from meaningfulstatements. To avoid bias, the researchers made active efforts tosuspend preconceptions during the process of interpretation. Thesubjective preconception is the reason for the choice of metho-dology as this type of analysis makes it possible to gain somedistance from the material. The two interviews that elaboratedand clarified the interpretation of the findings made the studymore robust. There was consistency between the interpretationsthe researchers made and what the women in the interviewshighlighted. The sample size is a limitation and the result cansubsequently not be generalised. On the other hand, the resultmay be a stepping stone for further discussions about quality inmidwifery care and how quality in the relationship could beincluded as a factor in this professional field. Further research isrequired.
Conclusions
Relational continuity and the quality of relationships are keyelements in a positive birth experience. The fact that the midwifeis aware of the significance of interpersonal relationships tends tostrengthen the possibility of mutuality and quality in the relation-ship. Through relational continuity, psychological trust and predict-ability may be created. Relational continuity allows the midwifeto meet the woman in the context of a holistic perspective.This may promote well-being and a potential for personal growthfor the individual woman and her partner, and could in turnpromote ‘empowerment’ for the whole family.
Acknowledgements
The authors would like to thank the women who participatedin the study. We also wish to thank Sør-Trøndelag UniversityCollege, St. Olavs Hospital, Municipality of Trondheim and EC Dahl’sfoundation for their financial support.
Appendix A. Supplementary material
Supplementary data associated with this article can be found inthe online version at http://dx.doi.org/10.1016/j.midw.2012.09.006.
References
Allgood, E., Kvalsund, R., 2005. Learning and Discovery for Professional Educators:Guides, Counselors, Teachers: An Interactive Experiential Approach to Practiceand Research. Tapir Academic Press, Trondheim.
Allgood, E., Kvalsund, R., 2003. Personhood, Professionalism and the HelpingRelation: Dialogues and Reflections. Tapir akademisk forlag, Trondheim.
Allgood, E., 1994/1995. Persons-In-Relation and Q Methodology, vol. 18. Depart-ment of Political Science, Kent Ohio, Operant Subjectivity, pp. 17–35.
Aune, I., Dahlberg, U., Ingebrigtsen, O., 2012. Parents’ experiences of midwiferystudents providing continuity of care. Midwifery 28, 372–378.
Blaaka, G., 2002. Grunnlagstenkning i et kvinnefag: teori, empiri og metode(Fundamental Thinking in a Woman’s Profession). Fagbokforlaget, Bergen.
Bluff, R., Holloway, I., 2008. The efficacy of midwifery role models. Midwifery 24,301–309.
Brown, S.R., 1993. Primer on Q-methodology. Operant Subjectivity 16, 91–138.Carolan, M., Hodnett, E., 2007. With woman’s’ philosophy: examining the
evidence, answering the questions. Nursing Inquiry 14, 140–152.Dickson, N., 1997. A theory of caring for midwifery. Australian College of Midwives
Incorporated Journal 10, 23–28.Fontein, Y., 2010. The comparison of birth outcomes and birth experiences of
low-risk women in different sized midwifery practices in the Netherlands.Women and Birth 23, 103–110.
Gagnon, R., 2011. Midwifery in a new context: expanding our reference pointsand embracing new representations of pregnancy and birth. Midwifery 27,360–367.

U. Dahlberg, I. Aune / Midwifery 29 (2013) 407–415 415
Haggerty, J.L., Reid, R.J., Freeman, G.K., Starfield, B.H., Adair, C.E., McKendry, R.,2003. Continuity of care: a multidisciplinary review. British Medical Journal327, 1219–1221.
Halldorsdottir, S., Karlsdottir, S.I., 2011. The primacy of the good midwife in
midwifery services: an evolving theory of professionalism in midwifery.Scandinavian Journal of Caring Sciences 25, 806–817.
Hostrup, H., 2009. Gestaltterapi: indføring i gestaltterapiens grundbegreber
(Gestalt Therapy: Education in the Fundamental Conceptions of GestaltTherapy).. Hans Reitzel, København.
Hunter, B., Berg, M., Lundgren, I., Olafsdottir, O., Kirkham, M., 2008. Relationships:
the hidden threads in the tapestry of maternity care. Midwifery 24, 132–137.Kirkham, M., 2000. How can we relate?. In: Kirkham, M. (Ed.), The Midwife–
Mother Relationship. MacMillan, Basingstoke, pp. 227–250.Kvalsund, R., 2005. Coaching: metode, prosess, relasjon (Coaching: Method,
Process, Relation). Synergy Publishing, Norway.Kvalsund, R., 1998. A Theory of the Person: A Discourse on Personal Reality and
explication of Personal Knowledge Through Q-Methodology—With Implica-tions for Counseling and Education. Ph.D. Thesis. The Norwegian University ofScience and Technology, Trondheim.
Leap, N., Sandall, J., Buckland, S., Huber, U., 2010. Journey to confidence: women’sexperiences of pain in labour and relational continuity of care. Journal ofMidwifery and Women’s Health 55, 234–242.
Lukasse, M., Vangen, S., Oian, P., Kumle, M., Ryding, E.L., Schei, B., 2010. on behalfof the Bidens Study Group, 2010. Childhood abuse and fear of childbirth—apopulation-based study. Birth 37, 267–274.
Lundgren, I., 2004. Releasing and relieving encounters: experiences of pregnancyand childbirth. Scandinavian Journal of Caring Sciences 18, 368–375.
Lundgren, I., Dahlberg, K., 2002. Midwives’ experience of the encounter with
women and their pain during childbirth. Midwifery 18, 155–164.Lundgren, I., Karlsdottir, S.I., Bondas, T., 2009. Long-term memories and experi-
ences of childbirth in a nordic context—a secondary analysis. International
Journal of Qualitative Studies on Health and Well-Being 4, 115–128.Lyberg, A., Severinsson, E., 2010. Midwives’ supervisory styles and leadership role
as experienced by Norwegian mothers in the context of a fear of childbirth.Journal of Nursing Management 18, 391–399.
McKeown, B., Thomas, D., 1988. Q Methodology. Sage, Newbury Park, California.Ministry of Health and Care Services, 2009. White Paper 12. A Happy Event—A
Continuous Pregnancy. Birth and Post Natal Care, Oslo.
Nilsson, C., Bondas, T., Lundgren, I., 2010. Previous birth experience in women withintense fear of childbirth. Journal of Obstetric, Gynaecologic, and NeonatalNursing 39, 298–309.
Nilsson, C., Lundgren, I., 2009. Women’s lived experience of fear of childbirth.Midwifery 25, e1–e9.
Olafsdottir, O.A., 2006. An Icelandic Midwifery Saga—Coming to Light. WithWomen and Connective Ways of Knowing. Ph.D. Dissertation. Thames ValleyUniversity.
Page, L., 2003. One-to-one midwifery: restoring the ‘with woman’ relationship inmidwifery. Journal of Midwifery and Women’s Health 48, 119–125.
Premberg, A., Carlsson, G., Hellstrom, A.L., Berg, M., 2011. First-time fathers’experiences of childbirth—a phenomenological study. Midwifery 27, 848–853.
Rijnders, M., Baston, H., Schonbeck, Y., Prins, K., Green, M., Buitendijk, S., J., 2008.Perinatal factors related to negative or positive recall of birth experience inwomen 3 years postpartum in the Netherlands. Birth 35, 107–116.
Rogers, C.R., 1961. On Becoming a Person: A Therapist’s View of Psychotherapy.Houghton Mifflin, Boston.
Sandall, J., Devane, D., Soltani, H., Hatem, M., Gates, S., 2010. Improving quality andsafety in maternity care: the contribution of midwife-led care. Journal ofMidwifery and Women’s Health 55, 255–261.
Schmolck, P., 2002. ‘PQ-method’ 2.11 for Windows. /http://www.Irz-muenchen.de/-schmolck/qmethod/01.03.2012S.
Spurkeland, J., 2005. Interpersonal Skills: Results Through Collaboration. Univer-sitetsforlaget, Oslo.
The Directorate for Health and Social Affairs, 2005. Guidelines for Antenatal Care,Oslo, IS-1179, pp. 28–64.
Thomson, G.M., Downe, S., 2010. Changing the future to change the past: women’sexperiences of a positive birth following a traumatic birth experience. Journalof Reproductive and Infant Psychology 28, 102–112.
Thorstensson, S., Nissen, E., Ekstrom, A., 2008. An exploration and description ofstudent midwives’ experiences in offering continuous labour support towomen/couples. Midwifery 24, 451–459.
Waldenstrom, U., 2004. Why do some women change their opinion about child-birth over time? Birth 31, 102–107.
Waldenstrom, U., Hildingsson, I., Rubertsson, C., Radestad, I., 2004. A negativebirth experience: prevalence and risk factors in a national sample. Birth 31,17–27.
Williams, K., Lago, L., Lainchbury, A., Eagar, K., 2010. Mothers’ views of caseloadmidwifery and the value of continuity of care at an Australian regionalhospital. Midwifery 26, 615–621.