Embed Size (px)
Citation preview
The view across Scotland – the work of the National Managed Clinical Network
Dr Lance SloanConsultant in Rehabilitation Medicine
NHS FifeChair Remote and Rural subgroup of ABI NMCN

Recommendations
• Better training for rural doctors• Better use of transport and technology• Guaranteed minimal levels of service despite
geography

Highlands and Islands Medical Service Committee Report to the Lords Commissioners
of His Majesty’s Treasury
Sir John Dewar, 1912
Royal College of Physicians of Edinburgh report 1851
• Only 62 of 170 parishes had a resident doctor• 41 parishes would be regarded as ‘destitute of
medical aid’
• What about brain injury services in 2011??
Differences between rural and urban health in Scotland
• Higher suicide rates (Paykel et al, 2000)• Higher incidence of alcohol related disease• There are a higher number of accidents in rural areas: on
roads, through climbing, farming, diving and fishing• Palliative Care workload is proportionally higher than
might be seen in urban areas, as patients from remote areas often prefer to or are enabled to die at home, rather than in a distant centre (Baird et al, 2003)
• Seasonal fluctuation in population
Delivering for remote and rural healthcare, 2007
Development of Acquired Brain Injury (ABI) National Managed Clinical Network (NMCN)
• 2000, Scottish Needs assessment report (SNAP)• 2003 review of progress – one of
recommendations referred to MCNs• 24th Jan 2005 – group of clinicians from across
Scotland met to agree a proposal for NMCN for ABI to submit to the National Services Division
• Proposal agreed in 2006 with NHS Lothian hosting MCN

National MCN for ABI
• Steering group first met on 1st Feb 2007• Chair Dr Brian Pentland• Wide membership including physicians, health
professionals, patient representation, Social Work, voluntary agencies, research workers
Objectives of ABI MCN in 2007
• Map out current services for people with ABI• Promote adoption of recognised standards of
care• Identify the educational needs of health care
groups involved in the care of people with ABI• Identify information requirements of patients and
carers
• Website development www.sabin.scot.nhs.uk
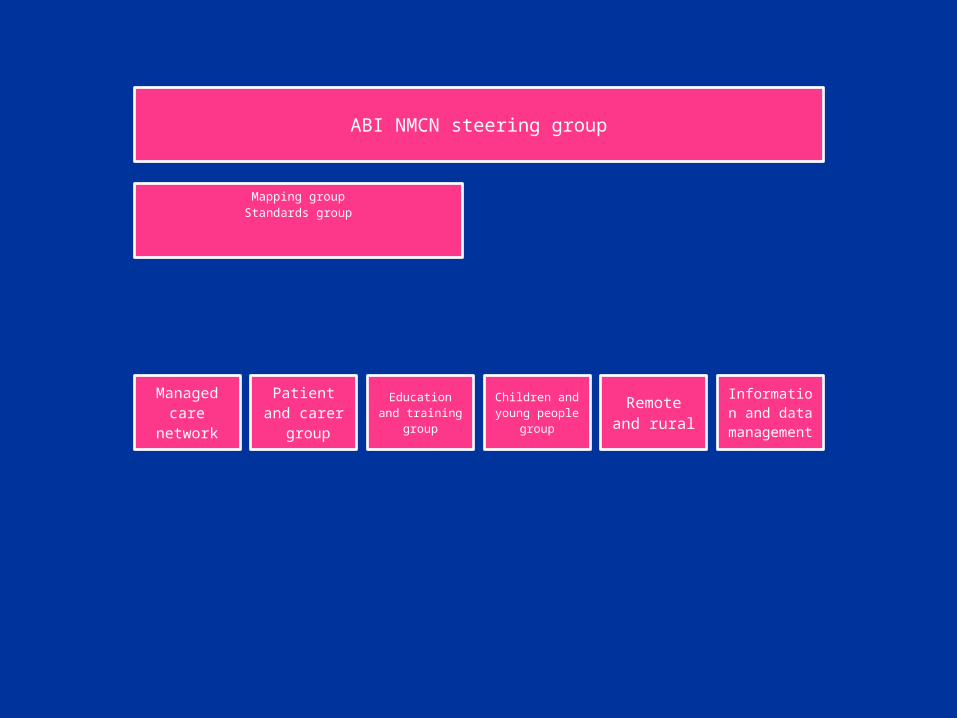
ABI NMCN steering group
Mapping groupStandards group
Managed care
network
Patient and carer
group
Education and training
group
Children and young people group
Remote and rural
Information and data
management
Equity of access
DefiningRural or Remote? Living In Scotland: An Urban-Rural
Analysis Of The Scottish Household Survey
2003. Rural Development Department,Social Research Branch with assistance from the
Scottish Agricultural College
Definitions
Rural Settlement < 3,000 pop < 30 min. from urban centre >10,000 pop
Remote> 30 minute from
urban centre >10,000 pop
Very Remote> 60 minute from
urban centre of >10,000 pop
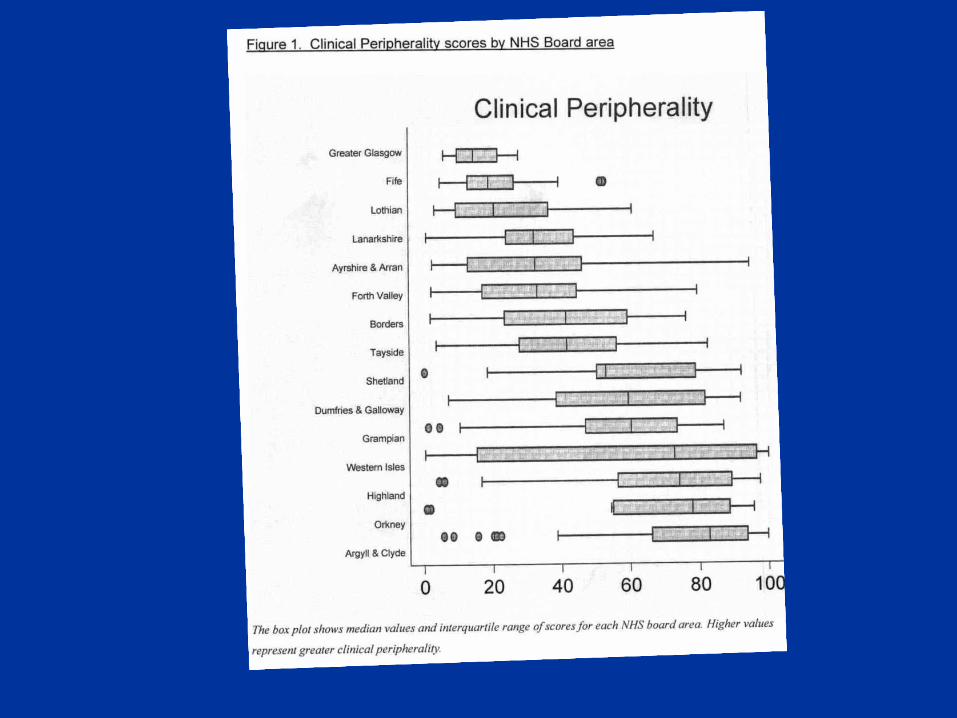
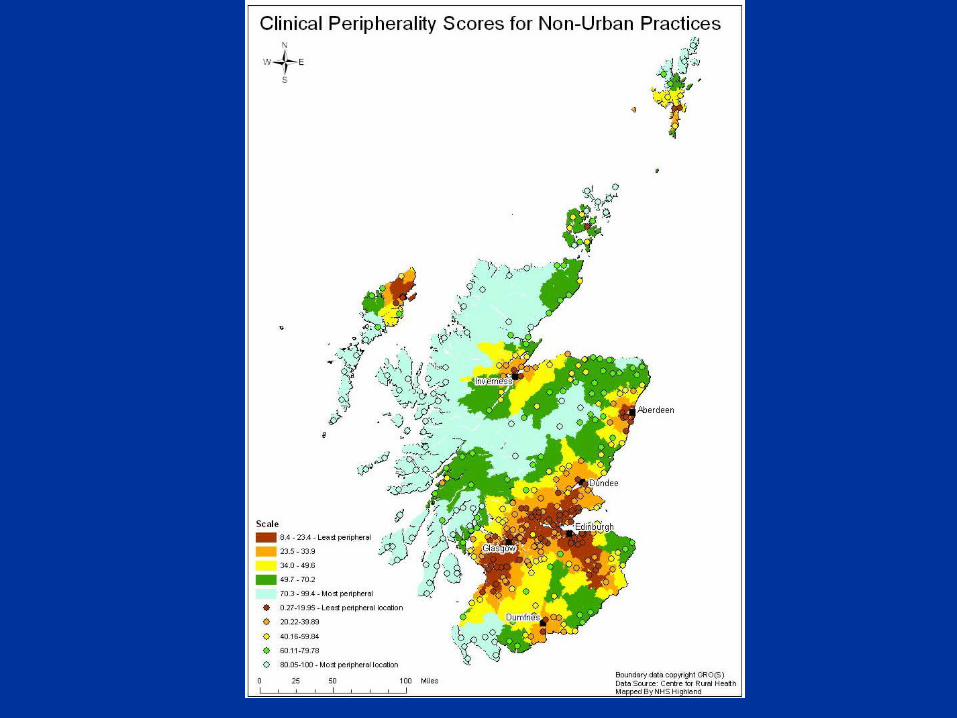
Clinical peripherality
• Clinical peripherality index devised by Centre for Rural Health
• Takes account of factors such as population density, practice size and time to reach secondary care
Aim of Remote and Rural subgroup of ABI MCN
• To bring together interested individuals to explore and scope the remote and rural issues around ABI and produce an Action Plan
Rural / Remote Rehabilitation
Traumatic Brain Injury• Increased incidence?• Increased severity?
Residents ofrural areas have a higher incidence of andmortality from TBI than residents of urban
areas, but they have poorer access to specialistbrain injury rehabilitation resources
• Woodward A, Dorsch MM, Simpson D. Head injuries in country and city. Med J Aust 1984; 141: 13-17.
• Glabella B, Hoffman R, Marine W, et al. Urban and rural traumatic brain injuries in Colorado. Ann Epidemiol 1997; 7: 207-212.
• Johnstone B, Nossaman L, Schopp L, et al. Distribution of services and supports for people with traumatic brain injury in rural and urban Missouri. J Rural Health 2002; 18: 109-117.
• Sample P, Darragh A. Perceptives of care access: the experience of rural and urban women following brain injury. Brain Inj 1998; 12: 855-874.
• Schootman M, Fuortes L. Functional status following traumatic brain injuries: Population-based rural-urban differences. Brain Inj1999 Dec;13(12):995-1004.

Rural / Remote
Rural NSW residentshave similar rehabilitation outcomesto urban residents after severe TBI
Harradine PG, et al. Severe traumatic brain injury in New South Wales: Comparable outcomes for rural and urban residents. Medical Journal of Australia 2004 Aug 2;181(3):130-4.
Remote and rural subgroup
• Review available documents• Equity of access• Pathways • AHP workforce and aspects• Telemedicine• Health Informatics• Clinical standards• Case scenarios
• The National Framework for Service Change in NHS Scotland - Rural Access Action Team, 2004
• Delivering for Remote and Rural Healthcare, 2007

Farmer J, Kilpatrick S. Are rural health professionals also social entrepreneurs?. Social Science & Medicine 2009 Dec;69(11):1651-8.
Farmer J, West C, Whyte B, Maclean M. Primary health-care teams as adaptive organizations: Exploring and explaining work variation using case studies in rural and urban scotland. Health Services Management Research 2005 Aug;18(3):151-64.
Farmer J. Connected care in a fragmented world: Lessons from rural health care. British Journal of General Practice 2007 Mar; 57 (536) :225-30.
Case scenario 1
• The individual who has no significant physical impairment and is sufficiently orientated to be allowed home but has persisting cognitive impairments
Case scenario 2
• A patient who is medically stable but has mixed physical and cognitive impairment without major behavioural issues. He requires physical assistance with transfers and all mobility activities and because of mixed cognitive and language difficulties needs supervision in activities of daily living
Case scenario 3
• An acutely behaviourally disturbed person who, because of cognitive/language impairment, is unco-operative with ward staff, attempts to leave hospital and can be aggressive to staff
Case scenario 4
• Persisting challenging behaviour in a person who is aggressive to staff but lacks cognitive capacity to comply with the staff or go to the community
Case scenario 5
• An individual in a vegetative state/minimally conscious state. Medically stable but requires nursing care for all needs and has been in this state for some weeks
Humpty Dumpty sat on a
wall,Humpty Dumpty had a
great fall,All the king’s horses,And all the king’s men,Couldn’t put Humpty
together again
Conclusions
• Opportunity• Scottish islands and mountains will always
pose difficulty for delivery of healthcare• But history indicates it can be can be a source
of innovation in technology, professional team working and education
Is rural and remote ABI service provision a problem or part of a wider solution?
(adapted from Dr James Douglas, 2005)