Embed Size (px)
Citation preview

The Vascular Anatomy ofthe Vertebro -Spinal Axis
Tibor Becske, MDa,b,c, Peter Kim Nelson, MDa,b,c,*KEYWORDS� Spinal cord � Anterior spinal artery� Posterior spinal artery � Spinal vasculature
The vascular supply of the spinal axis is systemat-ically determined during the first few weeks ofdevelopment as a consequence of the somato-topic organization of the spine.1 During this em-bryologic interval, 31 somites are formed, eachreceiving one individual pair of segmental arteriesfrom the dorsal aorta. These paired segmentalarteries ultimately support a functionally distinctvascular compartment comprising each devel-oping metamere. The thoracolumbar spinal vascu-lature (Fig. 1) retains the classically pairedsegmental arrangement into adulthood, with minorchanges in appearance attributed to differences inthe longitudinal growth of the spinal cord andvertebral column, respectively, during skeletalmaturation. This disparity in comparative lengthaccounts for the increasing obliquity of the nerveroots and, correspondingly, the radicular arteriesand veins in relation to their named intercostal orsegmental levels.
By comparison, considerable modification ofthe segmental disposition occurs throughout thecervical spine. The development of seriallyconsecutive intersegmental anastomoses estab-lishes three dominant craniocaudal vascular chan-nels (from anterior to posterior): the anteriorcervical artery, the vertebral artery, and the deepcervical artery, each of which may independentlyand variably participate in the vascularization ofvertebrae, paraspinal musculature, and cervicalspinal cord (Fig. 2). With respect to the developingsacrum, paired lateral sacral arteries (Fig. 3) arise
a Department of Neurology, New York University, LangNew York, NY 10016, USAb Department of Neurosurgery, New York University, LanNew York, NY 10016, USAc Department of Radiology, New York University, LangoNew York, NY 10016, USA* Corresponding author. Department of Neurology, NewAvenue Room HE208, New York, NY 10016.E-mail address: [email protected] (P.K. Nelson).
Neurosurg Clin N Am 20 (2009) 259–264doi:10.1016/j.nec.2009.03.0021042-3680/09/$ – see front matter ª 2009 Elsevier Inc. All
from the internal iliac arteries to supply the sacralnerve roots, vertebrae, and paraspinal muscula-ture. Medially, the distal dorsal aorta regresses tobecome the middle sacral artery, which anasto-moses laterally with corresponding branches ofthe lateral sacral arteries at the sacralneuroforamina.
VASCULAR SUPPLY TO THE SPINE, SPINAL DURA,AND PARASPINAL MUSCULATURE
From an angiographic standpoint, the arterialsupply to the bony spine, spinal canal, and para-vertebral muscles may be divided into fourvascular territories at each vertebral level:2–4 (1)The main intercostal or lumbar segmental arteriesprovide fine branches to the anterolateral aspectof the vertebral body before giving off the dorsalspinal trunk. (2) The ventral division of the dorsalspinal artery supplies the structures of the spinalcanal, including the bony elements, epiduralspace, dura, and contents of the thecal sac. Ante-riorly, an arterial arcade situated beneath theposterior longitudinal ligament vascularizes theposterior surface of the vertebral body. Posteri-orly, branches run in the posterior epidural spaceto supply the anterior aspect of the lamina anda portion of the spinous process. (3) The dorsaldivision of the dorsal spinal artery ultimatelypasses posteriorly beneath the ipsilateral trans-verse process and along the outer surface of thelamina, forming an arterial plexus close to the
one Medical Center, 560 First Avenue Room HE208,
gone Medical Center, 560 First Avenue Room HE208,
ne Medical Center, 560 First Avenue Room HE208,
York University, Langone Medical Center, 560 First
rights reserved. neur
osur
gery
.thec
lini
cs.c
om
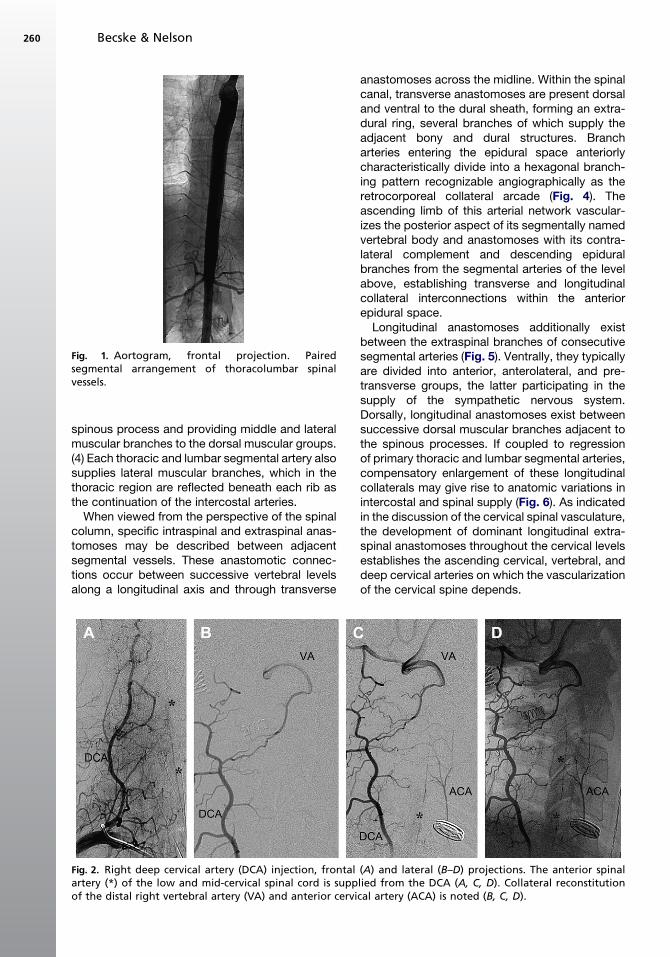
Fig. 1. Aortogram, frontal projection. Pairedsegmental arrangement of thoracolumbar spinalvessels.
Becske & Nelson260
spinous process and providing middle and lateralmuscular branches to the dorsal muscular groups.(4) Each thoracic and lumbar segmental artery alsosupplies lateral muscular branches, which in thethoracic region are reflected beneath each rib asthe continuation of the intercostal arteries.
When viewed from the perspective of the spinalcolumn, specific intraspinal and extraspinal anas-tomoses may be described between adjacentsegmental vessels. These anastomotic connec-tions occur between successive vertebral levelsalong a longitudinal axis and through transverse
Fig. 2. Right deep cervical artery (DCA) injection, frontalartery (*) of the low and mid-cervical spinal cord is suppof the distal right vertebral artery (VA) and anterior cervi
anastomoses across the midline. Within the spinalcanal, transverse anastomoses are present dorsaland ventral to the dural sheath, forming an extra-dural ring, several branches of which supply theadjacent bony and dural structures. Brancharteries entering the epidural space anteriorlycharacteristically divide into a hexagonal branch-ing pattern recognizable angiographically as theretrocorporeal collateral arcade (Fig. 4). Theascending limb of this arterial network vascular-izes the posterior aspect of its segmentally namedvertebral body and anastomoses with its contra-lateral complement and descending epiduralbranches from the segmental arteries of the levelabove, establishing transverse and longitudinalcollateral interconnections within the anteriorepidural space.
Longitudinal anastomoses additionally existbetween the extraspinal branches of consecutivesegmental arteries (Fig. 5). Ventrally, they typicallyare divided into anterior, anterolateral, and pre-transverse groups, the latter participating in thesupply of the sympathetic nervous system.Dorsally, longitudinal anastomoses exist betweensuccessive dorsal muscular branches adjacent tothe spinous processes. If coupled to regressionof primary thoracic and lumbar segmental arteries,compensatory enlargement of these longitudinalcollaterals may give rise to anatomic variations inintercostal and spinal supply (Fig. 6). As indicatedin the discussion of the cervical spinal vasculature,the development of dominant longitudinal extra-spinal anastomoses throughout the cervical levelsestablishes the ascending cervical, vertebral, anddeep cervical arteries on which the vascularizationof the cervical spine depends.
(A) and lateral (B–D) projections. The anterior spinallied from the DCA (A, C, D). Collateral reconstitutioncal artery (ACA) is noted (B, C, D).
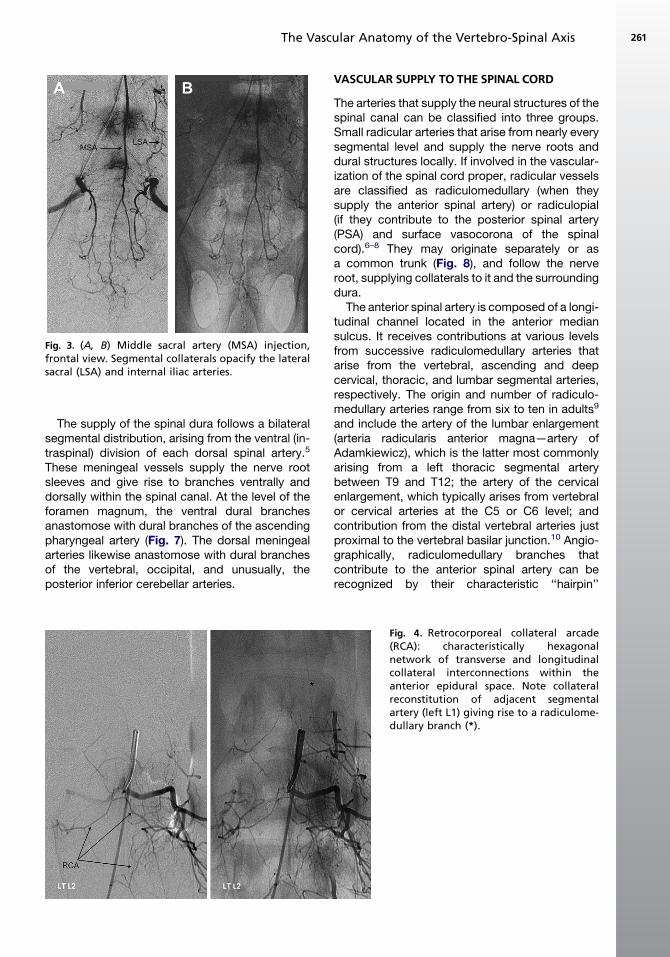
Fig. 3. (A, B) Middle sacral artery (MSA) injection,frontal view. Segmental collaterals opacify the lateralsacral (LSA) and internal iliac arteries.
The Vascular Anatomy of the Vertebro-Spinal Axis 261
The supply of the spinal dura follows a bilateralsegmental distribution, arising from the ventral (in-traspinal) division of each dorsal spinal artery.5
These meningeal vessels supply the nerve rootsleeves and give rise to branches ventrally anddorsally within the spinal canal. At the level of theforamen magnum, the ventral dural branchesanastomose with dural branches of the ascendingpharyngeal artery (Fig. 7). The dorsal meningealarteries likewise anastomose with dural branchesof the vertebral, occipital, and unusually, theposterior inferior cerebellar arteries.
VASCULAR SUPPLY TO THE SPINAL CORD
The arteries that supply the neural structures of thespinal canal can be classified into three groups.Small radicular arteries that arise from nearly everysegmental level and supply the nerve roots anddural structures locally. If involved in the vascular-ization of the spinal cord proper, radicular vesselsare classified as radiculomedullary (when theysupply the anterior spinal artery) or radiculopial(if they contribute to the posterior spinal artery(PSA) and surface vasocorona of the spinalcord).6–8 They may originate separately or asa common trunk (Fig. 8), and follow the nerveroot, supplying collaterals to it and the surroundingdura.
The anterior spinal artery is composed of a longi-tudinal channel located in the anterior mediansulcus. It receives contributions at various levelsfrom successive radiculomedullary arteries thatarise from the vertebral, ascending and deepcervical, thoracic, and lumbar segmental arteries,respectively. The origin and number of radiculo-medullary arteries range from six to ten in adults9
and include the artery of the lumbar enlargement(arteria radicularis anterior magna—artery ofAdamkiewicz), which is the latter most commonlyarising from a left thoracic segmental arterybetween T9 and T12; the artery of the cervicalenlargement, which typically arises from vertebralor cervical arteries at the C5 or C6 level; andcontribution from the distal vertebral arteries justproximal to the vertebral basilar junction.10 Angio-graphically, radiculomedullary branches thatcontribute to the anterior spinal artery can berecognized by their characteristic ‘‘hairpin’’
Fig. 4. Retrocorporeal collateral arcade(RCA): characteristically hexagonalnetwork of transverse and longitudinalcollateral interconnections within theanterior epidural space. Note collateralreconstitution of adjacent segmentalartery (left L1) giving rise to a radiculome-dullary branch (*).
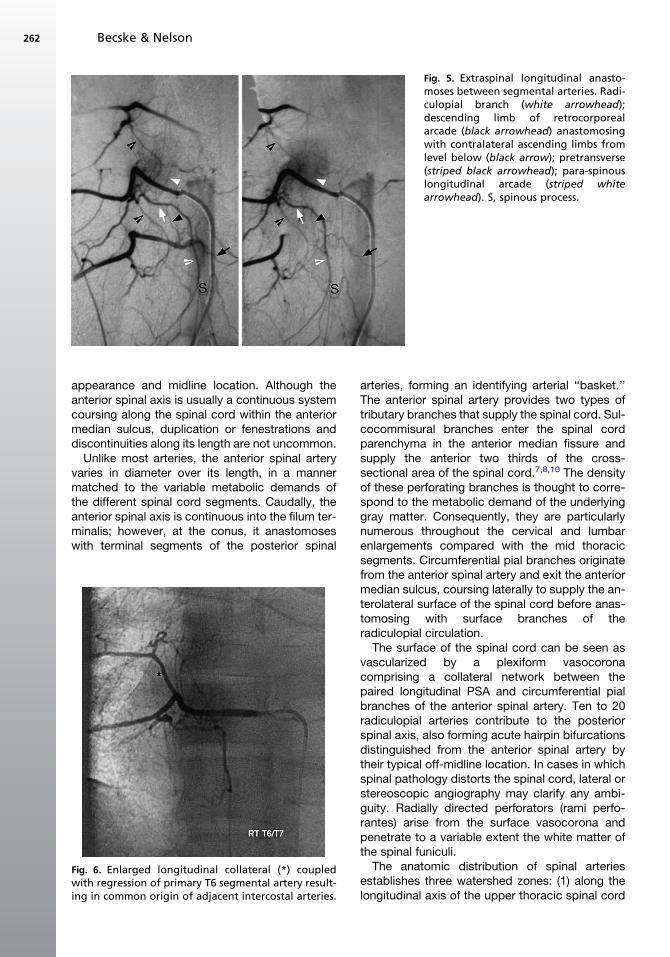
Fig. 5. Extraspinal longitudinal anasto-moses between segmental arteries. Radi-culopial branch (white arrowhead);descending limb of retrocorporealarcade (black arrowhead) anastomosingwith contralateral ascending limbs fromlevel below (black arrow); pretransverse(striped black arrowhead); para-spinouslongitudinal arcade (striped whitearrowhead). S, spinous process.
Becske & Nelson262
appearance and midline location. Although theanterior spinal axis is usually a continuous systemcoursing along the spinal cord within the anteriormedian sulcus, duplication or fenestrations anddiscontinuities along its length are not uncommon.
Unlike most arteries, the anterior spinal arteryvaries in diameter over its length, in a mannermatched to the variable metabolic demands ofthe different spinal cord segments. Caudally, theanterior spinal axis is continuous into the filum ter-minalis; however, at the conus, it anastomoseswith terminal segments of the posterior spinal
Fig. 6. Enlarged longitudinal collateral (*) coupledwith regression of primary T6 segmental artery result-ing in common origin of adjacent intercostal arteries.
arteries, forming an identifying arterial ‘‘basket.’’The anterior spinal artery provides two types oftributary branches that supply the spinal cord. Sul-cocommisural branches enter the spinal cordparenchyma in the anterior median fissure andsupply the anterior two thirds of the cross-sectional area of the spinal cord.7,8,10 The densityof these perforating branches is thought to corre-spond to the metabolic demand of the underlyinggray matter. Consequently, they are particularlynumerous throughout the cervical and lumbarenlargements compared with the mid thoracicsegments. Circumferential pial branches originatefrom the anterior spinal artery and exit the anteriormedian sulcus, coursing laterally to supply the an-terolateral surface of the spinal cord before anas-tomosing with surface branches of theradiculopial circulation.
The surface of the spinal cord can be seen asvascularized by a plexiform vasocoronacomprising a collateral network between thepaired longitudinal PSA and circumferential pialbranches of the anterior spinal artery. Ten to 20radiculopial arteries contribute to the posteriorspinal axis, also forming acute hairpin bifurcationsdistinguished from the anterior spinal artery bytheir typical off-midline location. In cases in whichspinal pathology distorts the spinal cord, lateral orstereoscopic angiography may clarify any ambi-guity. Radially directed perforators (rami perfo-rantes) arise from the surface vasocorona andpenetrate to a variable extent the white matter ofthe spinal funiculi.
The anatomic distribution of spinal arteriesestablishes three watershed zones: (1) along thelongitudinal axis of the upper thoracic spinal cord
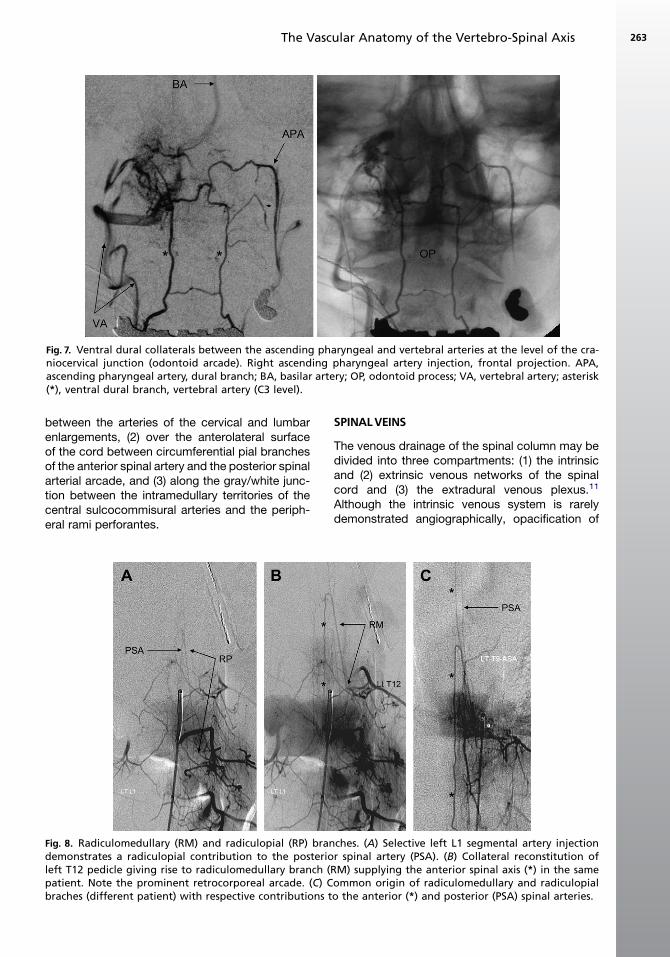
Fig. 7. Ventral dural collaterals between the ascending pharyngeal and vertebral arteries at the level of the cra-niocervical junction (odontoid arcade). Right ascending pharyngeal artery injection, frontal projection. APA,ascending pharyngeal artery, dural branch; BA, basilar artery; OP, odontoid process; VA, vertebral artery; asterisk(*), ventral dural branch, vertebral artery (C3 level).
The Vascular Anatomy of the Vertebro-Spinal Axis 263
between the arteries of the cervical and lumbarenlargements, (2) over the anterolateral surfaceof the cord between circumferential pial branchesof the anterior spinal artery and the posterior spinalarterial arcade, and (3) along the gray/white junc-tion between the intramedullary territories of thecentral sulcocommisural arteries and the periph-eral rami perforantes.
Fig. 8. Radiculomedullary (RM) and radiculopial (RP) brandemonstrates a radiculopial contribution to the posterioleft T12 pedicle giving rise to radiculomedullary branch (patient. Note the prominent retrocorporeal arcade. (C) Cbraches (different patient) with respective contributions t
SPINALVEINS
The venous drainage of the spinal column may bedivided into three compartments: (1) the intrinsicand (2) extrinsic venous networks of the spinalcord and (3) the extradural venous plexus.11
Although the intrinsic venous system is rarelydemonstrated angiographically, opacification of
ches. (A) Selective left L1 segmental artery injectionr spinal artery (PSA). (B) Collateral reconstitution of
RM) supplying the anterior spinal axis (*) in the sameommon origin of radiculomedullary and radiculopialo the anterior (*) and posterior (PSA) spinal arteries.
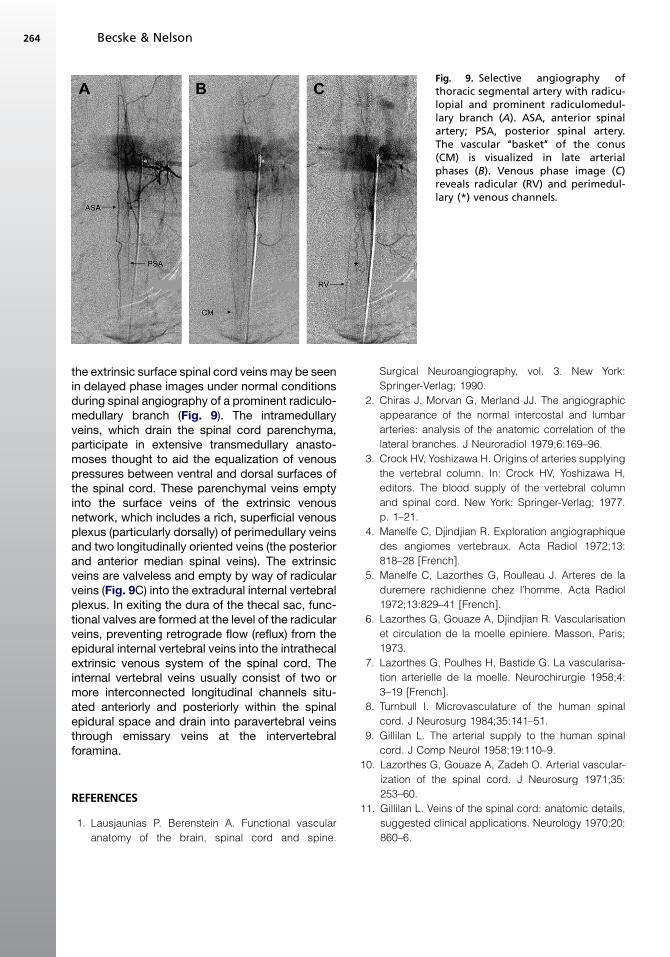
Fig. 9. Selective angiography ofthoracic segmental artery with radicu-lopial and prominent radiculomedul-lary branch (A). ASA, anterior spinalartery; PSA, posterior spinal artery.The vascular ‘‘basket’’ of the conus(CM) is visualized in late arterialphases (B). Venous phase image (C)reveals radicular (RV) and perimedul-lary (*) venous channels.
Becske & Nelson264
the extrinsic surface spinal cord veins may be seenin delayed phase images under normal conditionsduring spinal angiography of a prominent radiculo-medullary branch (Fig. 9). The intramedullaryveins, which drain the spinal cord parenchyma,participate in extensive transmedullary anasto-moses thought to aid the equalization of venouspressures between ventral and dorsal surfaces ofthe spinal cord. These parenchymal veins emptyinto the surface veins of the extrinsic venousnetwork, which includes a rich, superficial venousplexus (particularly dorsally) of perimedullary veinsand two longitudinally oriented veins (the posteriorand anterior median spinal veins). The extrinsicveins are valveless and empty by way of radicularveins (Fig. 9C) into the extradural internal vertebralplexus. In exiting the dura of the thecal sac, func-tional valves are formed at the level of the radicularveins, preventing retrograde flow (reflux) from theepidural internal vertebral veins into the intrathecalextrinsic venous system of the spinal cord. Theinternal vertebral veins usually consist of two ormore interconnected longitudinal channels situ-ated anteriorly and posteriorly within the spinalepidural space and drain into paravertebral veinsthrough emissary veins at the intervertebralforamina.
REFERENCES
1. Lausjaunias P. Berenstein A. Functional vascular
anatomy of the brain, spinal cord and spine.
Surgical Neuroangiography, vol. 3. New York:
Springer-Verlag; 1990.
2. Chiras J, Morvan G, Merland JJ. The angiographic
appearance of the normal intercostal and lumbar
arteries: analysis of the anatomic correlation of the
lateral branches. J Neuroradiol 1979;6:169–96.
3. Crock HV, Yoshizawa H. Origins of arteries supplying
the vertebral column. In: Crock HV, Yoshizawa H,
editors. The blood supply of the vertebral column
and spinal cord. New York: Springer-Verlag; 1977.
p. 1–21.
4. Manelfe C, Djindjian R. Exploration angiographique
des angiomes vertebraux. Acta Radiol 1972;13:
818–28 [French].
5. Manelfe C, Lazorthes G, Roulleau J. Arteres de la
duremere rachidienne chez l’homme. Acta Radiol
1972;13:829–41 [French].
6. Lazorthes G, Gouaze A, Djindjian R. Vascularisation
et circulation de la moelle epiniere. Masson, Paris;
1973.
7. Lazorthes G, Poulhes H, Bastide G. La vascularisa-
tion arterielle de la moelle. Neurochirurgie 1958;4:
3–19 [French].
8. Turnbull I. Microvasculature of the human spinal
cord. J Neurosurg 1984;35:141–51.
9. Gillilan L. The arterial supply to the human spinal
cord. J Comp Neurol 1958;19:110–9.
10. Lazorthes G, Gouaze A, Zadeh O. Arterial vascular-
ization of the spinal cord. J Neurosurg 1971;35:
253–60.
11. Gillilan L. Veins of the spinal cord: anatomic details,
suggested clinical applications. Neurology 1970;20:
860–6.












![Imaging of Hereditary Hemorrhagic Telangiectasia · Spinal and cerebral vascular malformations are mani-festations of underlying vascular dysplasia [12]. These lesions represent abnormal](https://img.pdfslide.us/doc/110x75/5ed59c731b7fdd786a1b540e/imaging-of-hereditary-hemorrhagic-telangiectasia-spinal-and-cerebral-vascular-malformations.jpg)