Embed Size (px)
Citation preview

BEHAVIOR THERAPY 28, 419-429, 1997
The Value of Recognizing Our Differences and Promoting Healthy Competition: The Cognitive Behavioral Debate
DAVID REITMAN
Louisiana State University
RONALD S. DRABMAN
University of Mississippi Medical Center
Few issues within behavior therapy have aroused as much debate as the causal status of cognitions. We briefly trace the history of the debate, provide recent exemplars of misunderstanding, and seek to clarify important epistemological distinctions be- tween radical and cognitive behaviorism. It is suggested that cognitive and radical behavioral therapists share a pragmatic interest in effecting and demonstrating be- havior change, but differ significantly with respect to how change is explained. Less certain is the extent to which the practices of radical behavioral and cognitive thera- pists differ. It is concluded that radical (contextual) and cognitive (mechanistic) views, though distinct, are both scientifically respected approaches to studying human behavior with important roles to play in the future of behavior therapy. The multigenerational enterprise called behavior therapy stands to be enriched by promoting shared values, acceptance of our differences, and encouraging healthy competition.
The cognitive behavioral debate in behavior therapy is rooted in the early history of competing learning theories (Mahoney, 1974). Then and now, a focal point of the debate has been the role of thinking in the genesis, mainte- nance, and treatment of behavioral disturbance. Recent debates contain ele- ments of past unproductive exchanges, but they also reveal a clearer under- standing of the theoretical bases of the disagreement. A brief review of the antecedents of contemporary arguments serves to illustrate the tenacity of the misunderstandings that have perpetuated the debate.
Correspondence concerning this article should be addressed to David Reitman, Louisiana State University, Department of Psychology, 236 Audubon Hall, Baton Rouge, LA 70803; e-mail: [email protected].
An earlier version of this paper was presented in J. P. Forsyth and R. P. Hawkins (Co-Chairs) (1996, November), Behavior Therapy at its Best and Worst. Symposium presented at the 30th annual meeting of the Association for the Advancement of Behavior Therapy, New York, NY.
419 0005 -7894/97/0419-042951.00/0 Copyright 1997 by Association for Advancement of Behavior Therapy
All rights of reproduction in any form reserved.
420 REITMAN & DRABMAN
A Brief History of Past Debates Many writers credit Chomsky's (1959) critique of Verbal Behavior
(Skinner, 1957) with facilitating the "overthrow of behaviorism" and stimu- lating a "cognitive revolution" within psychology (e.g., Brewer, 1974). In his review, Chomsky argued that Skinner's account of verbal behavior was implausible and naive, asserting that a "stimulus-response" modeP was inade- quate to deal with the complexity of language. Several critiques of behavior- ism followed Chomsky's and some extended the "simplistic" "stimulus- response" criticism to the clinical setting (e.g., Bandura, 1974; Mahoney, 1974). Unfortunately, none of these critiques adequately distinguished methodological behaviorism from radical behaviorism, and they tended to dis- credit the latter position based on criticisms of the former (MacCorquodale, 1970; Todd & Morris, 1992). Today, numerous journal articles and books document radical behaviorist interest in complex human behavior (e.g., Ferster, 1972; Hayes, 1989; Hayes & Hayes, 1992; Skinner, 1953; Staats, 1996; Staats & Staats, 1963), but misunderstandings persist (Todd & Morris). Recent debates (e.g., the "self-efficacy debate" described below) sug- gest that misunderstandings are still commonplace, even among academic psychologists and philosophers.
The Self-Efficacy Debate in the Journal of Behavior Therapy and Experimental Psychiatry OBTEP)
Bandura's 1974 address to the American Psychological Association is often cited as a watershed event in the "cognitive revolution" and his advocacy for the causal primacy of thought in human action has periodically occasioned spirited responses from radical behaviorists (see Catania, 1995). Hawkins' (1992) critique of the causal status accorded the self-efficacy construct was the primary stimulus for the most recent round of debate, and was followed by a vigorous defense of self-efficacy theory published by Bandura (1995) in JBTER Replies from Hawkins (1995) and 11 other partisans were then pub- lished along with Bandura's defense. Their arguments illustrate important ele- ments of the cognitive behavioral debate.
Rehashing Old Misunderstandings
The most obvious fact emerging from the self-efficacy debate is that the radical behavioral position on thinking and complex human behavior remains poorly understood and undifferentiated from methodological behaviorist posi- tions. Put simply, radical behaviorists do not, unlike methodological behav- iorists, exclude thinking and feeling from the analysis of human behavior. Nevertheless, Garcia (1995) repeats the often stated, but inaccurate assertion that contemporary radical behaviorists reject an analysis of private events. Another critic suggests, "no behavior therapist actually practices behavior t h e r a p y . . , for the simple reason that it is impossible to treat an unhappy
' Skinner's approach to verbal behavior was not based upon a stimulus-response model.
VALUE OF RECOGNIZING OUR DIFFERENCES 421
client without dealing with how he is feeling and thinking" (Locke, 1995, pp. 267-268). Thus, Locke, like Garcia, assumes that behavior therapists do not acknowledge the role of thinking and feeling in therapy, and then asserts that those who do are not practicing behavior therapy. The fact is, contem- porary cognitive and radical behaviorists share an interest in human thinking and feeling. Present day radical behavioral therapies all explicitly point to thinking and feeling as salient aspects of psychotherapy (e.g., Hayes, 1995; Hayes & Wilson, 1995; Kohlenberg & Tsai, 1991). However, radical behav- iorists study thinking and other private events from within a contextual sci- entific framework that places, a priori, all causal events outside of the organism itself (e.g., Dougher, 1995; Hayes & Brownstein, 1986). What is at issue is not whether thinking, feeling, or even self-efficacy are legitimate subject matters for scientific psychology, but how thinking, feeling, and self- efficacy are best studied and what their role might be in causal explanations. As will become apparent, what constitutes the "best" means of studying a given phenomenon will largely be determined by the scientific framework adopted by the scientist.
Newer Trends One of the most welcome trends in the cognitive behavioral debate is increased
attention to epistemology. In responding to Hawkins' (1992) critique, Bandura (1995) concluded that behaviorist criticisms of self-efficacy derive from a dog- matic commitment to direct observation (again implying a rejection of private events). However, radical behaviorist criticism of the self-efficacy construct does not arise from an objection to the inclusion of private events in the analysis. Instead, radical behaviorist concerns derive from a different set of assump- tions regarding causality and the means by which causal relations are demon- strated. Consequently, though the Hawkins-Bandura exchange appeared to concern only the causal status of self-efficacy, Dougher (1995) suggests that it actually reflected a much more fundamental disagreement about "scientific objectives, units of analysis, causation, and explanation" (p. 215).
Yield of the Self-Efficacy Debate: Understanding Our Similarities and Differences
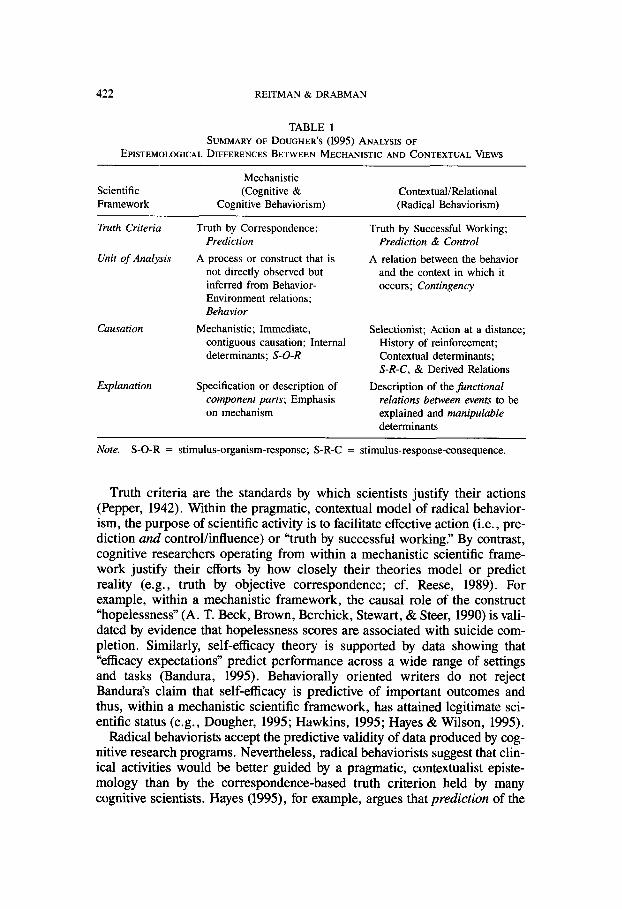
According to Dougher (1995), the mechanistic and contextual frameworks underlying cognitive and radical behavioral therapies can be distinguished along four dimensions: the truth criterion adopted, the unit of analysis selected, how causality is defined, and relatedly, what constitutes an accept- able explanation. What is exemplary about Dougher's analysis of the differ- ences between cognitive and radical behavioral epistemology is its concep- tual clarity and potential for revealing areas of consensus and divergence. Table 1 presents a brief summary of Dougher's analysis of the fundamental distinctions between the cognitive (mechanistic) and radical behavioral (con- textual) scientific frameworks.
422 REITMAN & DRABMAN
TABLE 1
SUMMARY OF DOUGHER'S (1995) ANALYSIS OF EPISTEMOLOG1CAL DIFFERENCES BETWEEN MECHANISTIC AND CONTEXTUAL VIEWS
Mechanistic Scientific (Cognitive &
Framework Cognitive Behaviorism) Contextual/Relational (Radical Behaviorism)
Truth Criteria
Unit of Analysis
Causation
Explanation
Truth by Correspondence; Prediction
A process or construct that is not directly observed but inferred from Behavior- Environment relations; Behavior
Mechanistic; Immediate, contiguous causation; Internal determinants; S-O-R
Specification or description of component parts; Emphasis on mechanism
Truth by Successful Working; Prediction & Control
A relation between the behavior and the context in which it occurs; Contingency
Selectionist; Action at a distance; History of reinforcement; Contextual determinants; S-R-C, & Derived Relations
Description of the functional relations between events to be explained and manipulable determinants
Note. S-O-R = stimulus-organism-response; S-R-C = stimulus-response-consequence.
Truth criteria are the standards by which scientists justify their actions (Pepper, 1942). Within the pragmatic, contextual model of radical behavior- ism, the purpose of scientific activity is to facilitate effective action (i.e., pre- diction and control/influence) or "truth by successful working" By contrast, cognitive researchers operating from within a mechanistic scientific frame- work justify their efforts by how closely their theories model or predict reality (e.g., truth by objective correspondence; cf. Reese, 1989). For example, within a mechanistic framework, the causal role of the construct "hopelessness" (A. T. Beck, Brown, Berchick, Stewart, & Steer, 1990) is vali- dated by evidence that hopelessness scores are associated with suicide com- pletion. Similarly, self-efficacy theory is supported by data showing that "efficacy expectations" predict performance across a wide range of settings and tasks (Bandura, 1995). Behaviorally oriented writers do not reject Bandura's claim that self-efficacy is predictive of important outcomes and thus, within a mechanistic scientific framework, has attained legitimate sci- entific status (e.g., Dougher, 1995; Hawkins, 1995; Hayes & Wilson, 1995).
Radical behaviorists accept the predictive validity of data produced by cog- nitive research programs. Nevertheless, radical behaviorists suggest that clin- ical activities would be better guided by a pragmatic, contextualist episte- mology than by the correspondence-based truth criterion held by many cognitive scientists. Hayes (1995), for example, argues that prediction of the

VALUE OF RECOGNIZING OUR DIFFERENCES 423
"average client's response" to treatment is insufficient for guiding treatment planning. That is, the scientific framework adopted by cognitive scientists may not be optimal even for the cognitive therapist. Though not contextually ori- ented, cognitive therapists respect empiricism and treatment outcome (A. T. Beck, 1991). In this sense, the cognitive therapist operates by the same prag- matic truth criterion as the radical behavior therapist. Even "eclectic" thera- pists seem to adopt a pragmatic ("successful working") treatment philosophy as a guiding principle (e.g., Lazarus, 1981). Thus, the case can be made that radical behavioral, cognitive, and eclectic therapists do not substantially differ in the way in which they justify their t r e a t m e n t efforts-all are pragmatic.
In the second dimension, the unit of analysis selected, lies an important but subtle distinction between the contextual and mechanistic perspectives. In order to accomplish the goal of "successful working" the radical behavior therapist or researcher seeks to identify manipulable (at least in principle) variables that participate in functional relations with behavior, with the latter broadly defined to include thinking and feeling, as well as overt behavioral acts. That relation, the contingency of reinforcement, constitutes the unit of analysis adopted by radical behaviorists, rather than behavior per se (e.g., Hawkins & Forsyth, 1997). The radical behaviorist position is nicely sum- marized by Carr (1993):
• . . true behavior analysts have very little interest in behavior. Thus, knowing that a young boy diagnosed as autistic exhibits self-injury is not very interesting. What is interesting is why the self-injury occurs (i.e., of what variables is it a function?). (p. 48)
In cognitive therapy, cognitions (i.e., covert or private behavior) serve as the unit of analysis, whereas in cognitive-behavior therapy cognitions serve as one of the units of analysis. Thus, a key element of cognitive therapies is to identify negative automatic thoughts and associated underlying core beliefs• Assuming that an automatic thought is distressing and distorted, the cognitive therapist then proceeds, in collaboration with the client, to challenge or ques- tion the validity of this maladaptive cognition• An automatic thought is chal- lenged by (a) examining the evidence for it and exploring alternative expla- nations, (b) discussing possible outcomes of the thought if it were true, (c) evaluating the consequences of thoughts, (d) developing more adaptive alter- native responses, and (e) perspective-taking (J. S. Beck, 1995).
Commenting on how such cognitive approaches differ from Acceptance and Commitment Therapy (ACT), Hayes and Wilson (1994) state,
In the usual view, certain undesirable emotions or thoughts are believed to cause undesirable patterns of living. On that basis these thoughts or emotions are tar- geted for change, control, or elimination. Avoidance of

424 REITMAN & DRABMAN
a variety of private events can be understood as both a socially encouraged outcome and as a natural outcome. • . . Rather than trying to change the form of private events, ACT attempts to alter their psychological func- tions by altering the social/verbal context in which pri- vate events occur. (pp. 289-290)
Unfortunately, there is a lack of comparative data on the behavior of radical behavioral and cognitive therapists. The existing process literature suggests that, relative to cognitive therapists, radical behavioral practitioners might be expected to place more emphasis on the client's acceptance of their thoughts and emotions, on the context and function of problematic thoughts and feel- ings, and on the explicit analysis of the aspects of the client-therapist relation- ship that are relevant to the presenting problem. Rather than emphasizing cog- nitive change as a means to behavioral change, the radical behavioral approach emphasizes the relation of problem behavior to the environmental context in which it is displayed both in-session and in the "real world" As radical behavioral therapies are actually practiced, it is interesting to note that they often look more like gestalt or existential therapies than like cognitive therapy or traditional behavior therapy (Dougher, 1989). In summary, the subtle yet important distinctions between cognitive and radical behavioral therapies derive essentially from radical behavior therapists' analysis of behavior-in-context (contingency)•
The most fundamental differences between the mechanistic and contextual frameworks emerge in the third and fourth dimensions of Dougher's (1995) analysis. Rather than objectivism, the most fundamental distinctions between cognitivists and radical behaviorists emerge in the area of causation and expla- nation. Cognitive and cognitive behavioral models of psychological distur- bance are mechanistic in that they require thoughts to mediate behavior- environment relations and thus they explain behavior change in terms of internal mechanisms or processes (e.g., cognitive shifts). In contrast, a con- textual approach emphasizes historical and current environmental factors. In a clinical setting, this means that explanations at the level of specification and description of mechanisms omit an important facet of the analysis (the context) for radical behaviorists, whereas explanations that ignore internal mechanisms will be similarly inadequate for cognitive therapists and re- searchers. Radical behaviorists argue that internal processes of the sort dis- cussed by cognitivists cannot be changed directly and must be altered through the interaction of the individual with the environment, including the activities of the therapist. Thus, the radical behaviorist's rejection of the causality of thought as an initiating cause derives from a pragmatic, primary interest in accomplishing behavior change. Though logically an individual's thinking might sometimes be considered part of the causal chain (Forsyth, Lejuez, Hawkins, & Eifert, 1996), within radical behaviorism that part of the chain

VALUE OF RECOGNIZING OUR DIFFERENCES 425
cannot be accessed directly, it can only be influenced indirectly through person-environment interactions.
Given the substantial differences between cognitive and radical behavioral scientific frameworks, we are inclined to conclude that both should be con- sidered distinct, but uniquely valuable for their purposes. Although Over- skeid (1995) argued that the differences between cognitive and behavioral views are minimal, the present analysis suggests that such a conclusion is only possible if one ignores the radical behaviorist's rejection of private events as initiating causes of behavior (cf. Flora & Kestner, 1995), Thus, we would concur with Ross (1985) that the term "cognitive behavioral" is an oxy- moron. Yet it is an oxymoron only with respect to differing views of causality, explanation, and the proper units of analysis, not with respect to what is the most valuable subject matter for psychology.
The Future of the Cognitive Behavioral Debate in Behavior Therapy Though this paper has highlighted differences between contextual behav-
ioral and cognitive epistemology, shared values can also be identified. Both radical behavioral therapists and cognitive therapists are likely to agree that therapy should facilitate observable behavior change and both are committed to empirically validated practice. Until recently, viable contextual or radical behavioral alternatives to cognitive or cognitive behavioral therapies for adults were unavailable in any useful form (though see Ferster, 1972, for an early attempt). Now that contextually oriented alternatives to cognitive therapy exist (e.g., Hayes, Jacobson, Follette, & Dougher, 1996; Kohlenberg & Tsai, 1991), we might hope that future debates will take on a more "empiri- cal" tone. A few studies have already shown that contextual approaches (e.g., those emphasizing the use of acceptance-based methods, in-session operant and exposure-based procedures, the therapeutic relationship, and functional analysis) may provide viable supplements (Kohlenberg & Tsai, 1994) or alter- natives (Dougher & Hackbert, 1994) to cognitive therapy. Likewise, several radical behaviorists have recently attempted to bridge cognitive concepts with behavior analysis by providing interpretive analysis of cognitive phenomena in terms consistent with behavior analytic principles (e.g., see the March 1997 special issue of the Journal of Behavior Therapy and Experimental Psy- chiatry, for a recent series of representative articles; Reyna, 1997).
Concluding Thoughts: The Survival of a Science of Human Behavior and Behavior Change
Debates about causal status of cognition cannot be resolved empirically. The debate is entrenched in differing scientific frameworks, mechanistic or contextual, held by the participants. Though past debates have been neces- sary to achieve this insight, it is time to move on. At present, we need to encourage variation to insure that new and better therapies emerge. In our view it is too soon to grant any particular type of therapy, cognitive or be-
426 REITMAN & DRABMAN
havioral, with the title "empirically-validated treatment" if such a title limits scientifically informed innovation in psychotherapy. To date, no one is satisfied completely with the results reported in any psychotherapy treatment outcome, especially when considering comorbidity and dropout issues (Bergin & Garfield, 1994). There is a need for improvement in therapeutic outcomes, but new techniques must be demonstrated as superior to old ones before their widespread dissemination (cf. Wolpe, 1993; see also Bergin & Garfield, 1994; Elkin, 1994). Even when a technique is shown to be superior, we must be cognizant that the explanations offered for therapeutic changes will be constrained by the scientifiC framework adopted by the practitioner or researcher.
Ultimately, behavior therapy's survival may depend upon recognizing the strengths and limitations of both contextual and mechanistic approaches. There is no a priori reason why mechanistic and contextualistic questions cannot be pursued. We believe that radical behavioral therapies constitute an important alternative to mechanistic strategies and may turn out to be a supe- rior approach for some problems. Yet within some research areas, a com- bination of mechanistic and contextual strategies may be essential. For example, in the health behavior domain, Wulfert and Biglan (1994) noted that while mechanistic theories, such as the theory of reasoned action (Azjen & Fishbein, 1980), identify numerous cognitive correlates of condom use, con- textual approaches may be more beneficial in the design and implementation of HIV-prevention programs. Whether this kind of two-pronged mechanistic- contextual approach leads to the development of interventions that produce better outcomes is an open question. Finally, correlational research con- ducted from a mechanistic framework can have important practical implica- tions. The clinical benefits of identifying variables predictive of suicide are obvious and pragmatic, even though such research derives primarily from a mechanistic rather than a contextual scientific framework. In our view, behavior therapy has historically made room for both contextual and mech- anistic approaches, and we suspect that the co-existence of both approaches will likely continue in the future.
The mission for research clinicians remains to answer Gordon Paul's (1967) now famous question: What treatment, by whom, is most effective for this individual with that specific problem, under which set of circumstances, and how does it come about? We should not allow philosophical arguments to stand in the way of this mission. To answer Paul's question, we must first acknowledge that mechanistic and contextual approaches are distinct but potentially complementary (cf. Forsyth et al., 1996). Behavior therapists should, when confronted with the issue of cognition and causality, "agree- to-disagree" Yet, in the context of psychotherapy, our differences may serve as a stimulus to compete within comparative treatment protocols. For example, what does the addition of cognitive restructuring add to "behav- ioral" treatments for various kinds of problems? What can cognitive thera- pists learn about teaching new cognitions by studying the teaching techniques
VALUE OF RECOGNIZING OUR DIFFERENCES 427
developed by radical behaviorists? Empirical challenges to the status quo in behavior therapy will ultimately strengthen the field and lay a solid founda- tion for the next 30 years of behavior therapy. The multigenerational enter- prise called behavior therapy stands to be enriched by promoting shared values, accepting our differences, and encouraging healthy competition.
References Azjen, I., & Fishbein, M. (1980). Understanding attitudes and predicting social behavior.
Englewood Cliffs, NJ: Prentice Hall. Bandura, A. (1974). Behavior theory and the models of man. American Psychologist, 29,
859-869. Bandura, A. (1995). Comments on the crusade against the causal efficacy of human thought.
Journal of Behavior Therapy and Experimental Psychiatry, 26, 179-190. Beck, A. T. (1991). Cognitive therapy: A 30-year retrospective. American Psychologist, 46,
368-375. Beck, A. T., Brown, G., Berchick, R. J., Stewart, B. L., & Steer, R. A. (1990). Relationship
between hopelessness and ultimate suicide: A replication with psychiatric outpatients. American Journal of Psychiatry, 147, 190-195.
Beck, J. S. (1995). Cognitive therapy: Basics and beyond. New York: Guilford Press. Bergin, A. E., & Garfield, S. L. (1994). Overview, trends, and future issues. In A. E. Bergin
& S. L. Garfield (Eds.), Handbook of psychotherapy and behavior change (pp. 821-830). New York: John Wiley.
Brewer, W. E (1974). There is no convincing evidence for operant or classical conditioning in adult humans. In W. B. Weimer & D. S. Palermo (Eds.), Cognition and the symbolic processes (pp. 1-42). Hillsdale, NJ: Lawrence Erlbaum.
Carr, E. G. (1993). Behavior analysis is not ultimately about behavior. The Behavior Analyst, 16, 47-49.
Catania, A. C. (1995). Higher-order behavior classes: Contingencies, beliefs, and verbal behavior. Journal of Behavior Therapy and Experimental Psychiatry, 26, 191-200.
Chomsky, N. (1959). Verbal behavior. By B. E Skinner. Language, 35, 26-58. Dougher, M. J. (1989, November). Radical behaviorism: What it is and what it isn't. Impli-
cations for the clinical context. In E. M. Heilby (Chair), Unified theories in behavior therapy. Symposium conducted at the meeting of the Association for the Advancement of Behavior Therapy, New York, NY.
Dougher, M. J. (1995). The bigger picture: Cause and cognition in relation to differing scientific frameworks. Journal of Behavior Therapy and Experimental Psychiatry, 26, 215-219.
Dougher, M. J., & Hackbert, L. (1994). A behavior-analytic account of depression and a case report using acceptance-based procedures. The Behavior Analyst, 17, 321-334.
Elkin, I. (1994). The NIMH treatment of depression collaborative research program: Where we began and where we are. In A. E. Bergin & S. L. Garfield (Eds.), Handbook of psy- chotherapy and behavior change (pp. 114-139). New York: John Wiley.
Ferster, C. B. (1972). An experimental analysis of clinical phenomena. The Psychological Record, 22, 1-16.
Flora, S. R., & Kestner, J. (1995). Cognitions, thoughts, private events, etc. are never initiating causes of behavior: Reply to Overskeid. The Psychological Record, 45, 577-589.
Forsyth, J. P., Lejuez, C. W., Hawkins, R. P., & Eifert, G. H. (1996). Cognitive vs. contextual causation: Different world views but perhaps not irreconcilable. Journal of Behavior Therapy and Experimental Psychiatry, 27, 369-376.
Gareia, J. (1995). Mind is back in control of Pavlovian and Skinnerian responses: Was it ever away? Journal of Behavior Therapy and Experimental Psychiatry, 26, 229-234.
428 REITMAN & DRABMAN
Hawkins, R. M. E (1992). Self-efficacy: A predictor but not a cause of behavior. Journal of Behavior Therapy and Experimental Psychiatry, 23, 251-256.
Hawkins, R. M. E (1995). Self-efficacy: A cause of debate. Journal of Behavior Therapy and Experimental Psychiatry, 26, 235-240.
Hawkins, R. P., & Forsyth, J. P. (1997). The behavior analytic perspective: Its nature, pros- pects, and limitations for behavior therapy. Journal of Behavior Therapy and Experimental Psychiatry, 28, 7-16.
Hayes, S. C. (Ed.). (1989). Rule-governed behavior: Cognition, contingencies, and instruc- tional control. New York: Plenum.
Hayes, S. C. (1995). Why cognitions are not causes, the Behavior Therapist, 18, 59-60. Hayes, S. C., & Brownstein, A. J. (1986). Mentalism, behavior-behavior relations, and a
behavior-analytic view of the purposes of science. The Behavior Analyst, 9, 175-190. Hayes, S. C., & Hayes, L. J. (1992). Some clinical implications of contextualistic behaviorism:
The example of cognition. Behavior Therapy, 23, 225-249. Hayes, S. C., Jacobson, N. S., Follette, V. M., & Dougher, M. J. (Eds.). (1996). Acceptance
and change: Content and context in modern psychotherapy. Reno, NV: Context Press. Hayes, S. C., & Wilson, K. G. (1994). Acceptance and Commitment Therapy: Altering the
verbal support for experiential avoidance. The Behavior Analyst, 17, 289-303. Hayes, S. C., & Wilson, K. G. (1995). The role of cognition in complex human behavior: A
contextualist perspective. Journal of Behavior Therapy and Experimental Psychiatry, 26, 241-248.
Kohlenberg, R. J., & Tsai, M. (1991). Functional analytic psychotherapy: Creating intense and therapeutic relationships. New York: Plenum.
Kohlenberg, R. J., & Tsai, M. (1994). Improving cognitive therapy for depression with func- tional analytic psychotherapy: Theory and case study. The Behavior Analyst, 17, 305-319.
Lazarus, A. A. (1981). Multimodal therapy. New York: McGraw-Hill. Lee, C. (1992). On cognitive theories and causation in human behavior. Journal of Behavior
Therapy and Experimental Psychiatry, 23, 257-268. Lee, C. (1995). Comparing the incommensurable: Where science and politics collide. Journal
of Behavior Therapy and Experimental Psychiatry, 26, 259-263. Locke, E. A. (1995). Beyond determinism and materialism, or isn't it time we took conscious-
ness seriously? Journal of Behavior Therapy and Experimental Psychiatry, 26, 265-273. MacCorquodale, K. W. (1970). On Chomsky's review of Skinners Verbal Behavior. The
Journal of the Experimental Analysis of Behavior, 13, 83-99. Mahoney, M. J. (1974). Cognitive and behavior modification. Cambridge, MA: Ballinger. Mahoney, M. J. (1995). Cognition and causation in human experience. Journal of Behavior
Therapy and Experimental Psychiatry, 26, 275-278. Overskeid, G. (1995). Cognitivist or behaviorist-Who can tell the difference: The case of
implicit and explicit knowledge. British Journal of Psychology, 86, 517-522. Paul, G. L. (1967). Strategy of outcome research in psychotherapy. Journal of Consulting Psy-
chology, 31, 111. Pepper, S. C. (1942). World hypotheses. A study in evidence. Berkeley, CA: University of Cali-
fornia Press. Reese, H. W. (1989). Rules and rule-governance: Cognitive versus behavioristic views. In S. C.
Hayes (Ed.), Rule-governed behavior: Cognition, contingencies, and instructional control (pp. 3-84). New York: Plenum.
Reyna, L. J. (Ed.). (1997). Special Issue III: Bridging the gap. Cognition, behavior, and causal- ity: A broad exchange of views stemming from the debate on the causal efficacy of human thought [Special issue]. Journal of Behavior Therapy and Experimental Psychiatry, 28(1).
Ross, A. O. (1985). To form a more perfect union: It is time to stop standing still. Behavior Therapy, 16, 195-204.

VALUE OF RECOGNIZING OUR DIFFERENCES 429
Skinner, B. F. (1957). Verbal behavior. New York: Appleton-Century-Crofts. Staats, A. W. (1996). Behavior and personality: Psychological behaviorism. New York:
Springer. Staats, A. W., & Staats, C. K. (1963). Complex human behavior: A systematic extension of
learning principles. New York: Holt, Reinhart, & Winston. Todd, J. T., & Morris, E. K. (1992). Case histories in the great power of steady misrepresen-
tation. American Psychologist, 47, 1441-1453. Wilson, G. T. (1995). Behavior therapy. In R. J. Corsini & D. Wedding (Eds.), Currentpsy-
chotherapies (pp. 197-228). Itasca, IL: E E. Peacock. Wolpe, J. (1993). The cognitivist oversell and comments on symposium contributions. Journal
of Behavior Therapy and Experimental Psychiatry, 24, 141-147. Wulfert, E., & Biglan, A. (1994). A contextual approach to research on AIDS prevention. The
Behavior Analyst, 17, 353-363.
RECEIVED: March 15, 1997 ACCEPTED: June 6, 1997





























