Embed Size (px)
Citation preview

The value of healthcare data for secondary uses in clinical research and development
Gary K. Mallow, Ph.D.Director, Healthcare IT
DISCLAIMER: The views and opinions expressed in this presentation are those of the author and do not necessarily represent official policy or position of HIMSS.

Conflict of Interest DisclosureGary K. Mallow, Ph.D.
• Salary: Merck & Co., Inc.
• Royalty:
• Receipt of Intellectual Property Rights/Patent Holder:
• Consulting Fees (e.g., advisory boards):
• Fees for Non-CME Services Received Directly from a Commercial Interest or
their Agents (e.g., speakers’ bureau):
• Contracted Research:
• Ownership Interest (stocks, stock options or other ownership interest excluding
diversified mutual funds):
• Other:
© 2012 HIMSS

Learning Objectives
• Recognize key secondary uses of health
care data in clinical research and
development.
• Associate secondary uses with business
outcomes.
• Understand key challenges and
opportunities for secondary use of
electronic health records (EHR) in clinical research and development in the life
sciences.

Hard trends in healthcare
• Pay for performance
• Cost pressure
• Shifting demographics
• Expiry
• Access to real-world data flows
• Variation in clinical practice
• Inefficient use of information
• Fragmented healthcare integrated care
• Inefficiency, defensive medicine, & waste
• Protracted adoption of innovation
Graphic from http://www.ted.com/talks/daniel_kraft_medicine_s_future.html

View on healthcare ecosystem trends
Pressure to demonstrate value
Clinical data valuable but no natural ownership
HIT investment is experimental across
areas - placing small bets in consumer genomics and compliance solutions
Testing social media to engage
patients but little proven success
Life Sciences
Heads down on EHR and MU
Need solutions to identify best practices and measure performance (for P4P)
Large IDNs and AMCs ahead of the curve, accumulating longitudinal EHR, some coupled with genetic info
Providers
Investing in HIT to enable shifting from
volume play to value play
Gain access to clinical data and analytics through acquisition
Leverage claims data for CER and develop commercial data services
PBMs investing in CER and
pharmacogenomics
Payers / PBMs
“Play or Pay” – required to offer
“minimum essential coverage” or pay penalties
Promote health and wellness
Encourage adoption of PHR
Leverage HIT for benefit design
Employers
EHR dominates HIT market share; disruptive solutions emerging
Non-traditional players entering the HIT space through acquisition or partnership
Data integration and analytics in high demand (due to the anticipated needs from ACOs) and active for M&A
Consumer/ patient engagement platforms + consumer genomics gaining attention, need to demonstrate commercial viability
HIE holds the promise for future but models are still in infancy, with few having demonstrated economic viability
Technology Providers / Enablers
Desire wellness and self care but lack
effective tools and incentives
More open to share health info online, but value remains to be seen
Still low penetration of PHR with little utilization
Patients / Caregivers / Consumers
Developing primary care capabilities and
sharing medical records
Building eRx capabilities and encouraging widespread Provider adoption
Trying to increase medication compliance
Pharmacies
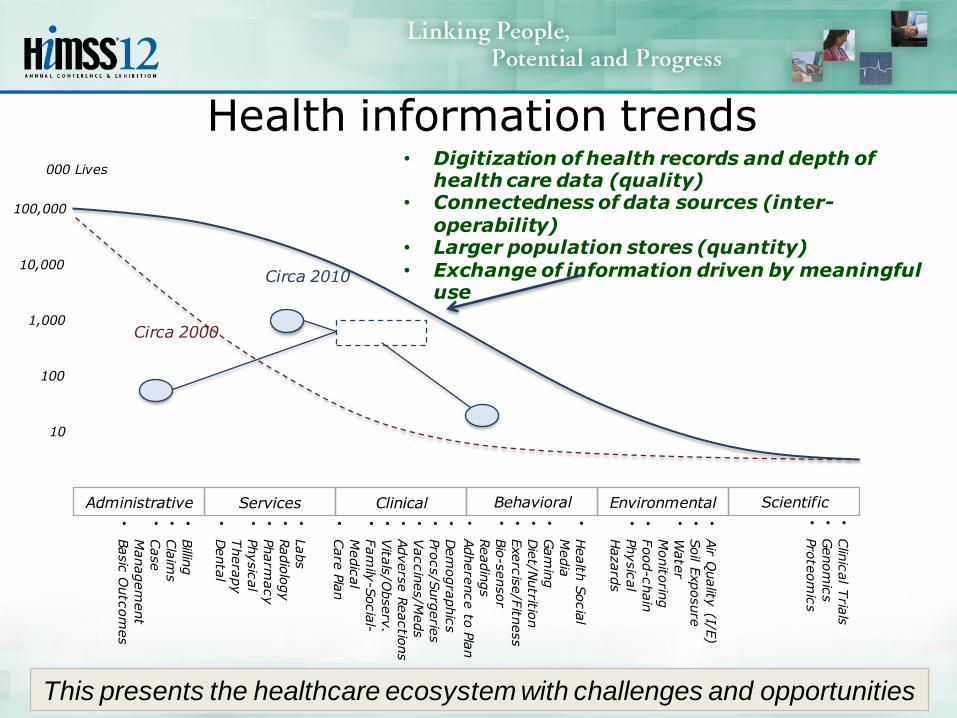
Health information trends
Administrative Services Clinical Behavioral Environmental Scientific
•Clin
ical T
rials
•Genom
ics
•Pro
teom
ics
•Billin
g•
Cla
ims
•Case
Managem
ent
•Basic
Outc
om
es
•Labs
•Radio
logy
•Pharm
acy
•Physic
al
Thera
py
•Denta
l
•Dem
ogra
phic
s•
Pro
cs/S
urg
erie
s•
Vaccin
es/M
eds
•Advers
e R
eactio
ns
•Vita
ls/O
bserv
.•
Fam
ily-S
ocia
l-
Medic
al
•Care
Pla
n
•Air Q
uality
(I/E)
•Soil E
xposure
•W
ate
r
Monito
ring
•Food-c
hain
•
Physic
al
Hazard
s
•Health
Socia
l
Media
•Gam
ing
•Die
t/Nutritio
n•
Exerc
ise/F
itness
•Bio
-sensor
Readin
gs
•Adhere
nce to
Pla
n
10
100
1,000
10,000
100,000
Circa 2000
Circa 2010
• Digitization of health records and depth of health care data (quality)
• Connectedness of data sources (inter-operability)
• Larger population stores (quantity)• Exchange of information driven by meaningful
use
000 Lives
This presents the healthcare ecosystem with challenges and opportunities

The “burning platform” for Life Sciences

Importance of secondary use
Pace of change has accelerated exponentially
Focus on patients and their healthcare team
Requirement to demonstrate product value / fee for service fee for performance
Clinical data valuable but no natural ownership
HIT investment is experimental across areas - placing small bets in consumer genomics
and compliance solutions, clinical trial ops
Testing social media to engage patients but still experimental
Pharma
1.0
Pharma
2.0
Pharma
3.0
Developing drugs,
vertically integrated,
blockbuster model
Developing drugs, More
interdependent ecosystem,
diversified portfolios, V&B,
Licensing, Partnering,
Outsourcing
Delivery of healthy outcomes,
comparative effectiveness
research (CER), entrance of non-
traditional companies, business
models, collaborations
2009 “Zeros”Birth EO 20th Century
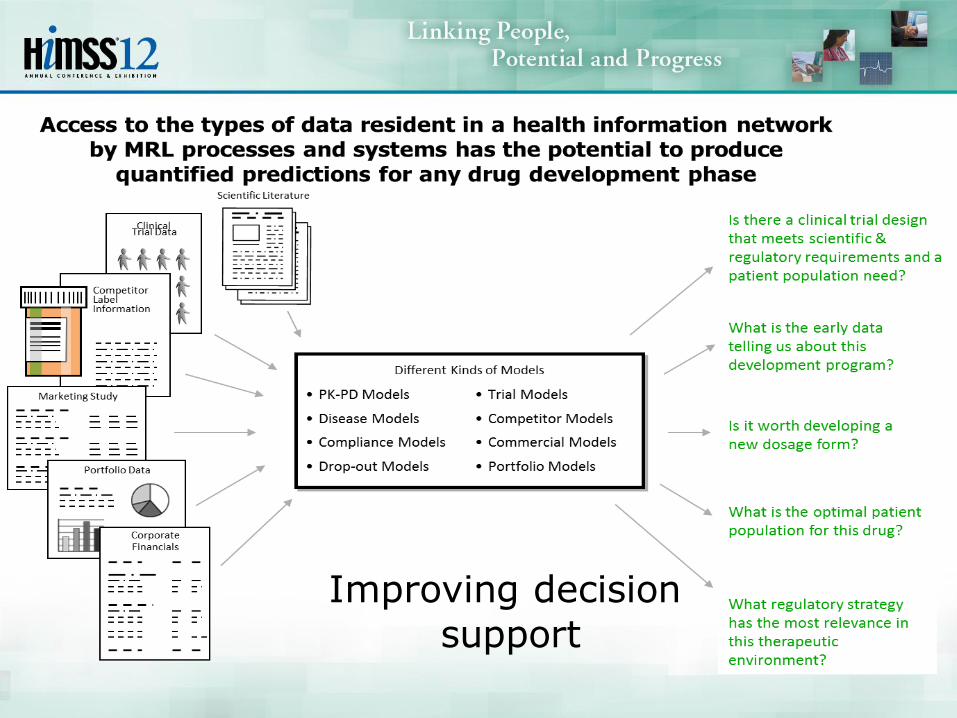
Improving decision
support

Examples of some key
clinical R&D outcomes desired
• Improved ability to execute EHR-driven Comparative Effectiveness Research
• New insights into disease prevalence and incidence in populations
• Longitudinal patient views to better understand population/ sub-population trends
CER, Disease & Demographic Models
• Comparator models to provide best in class guidance
• Improved compound selection when analyzing pharmacologic data for early stage trials
Comparator Modeling
• Improved predictability of patient/ dose response
• Better models through enhanced understanding of disease courses within patients
• Better identification of patients who will not benefit/ respond to therapy
Disease Progression & Therapy Treatment Models
• Improved identification of patients who qualify for a study and their subsequent enrollment
• Improved site identification and assessment of country feasibility
• Improved protocol refinement process
• Increased patient adherence
• Improved data quality
• Identification of linkages between active / post-trial data
Predictable Trial Execution and Cycle Time Reduction
• Better clinical risk mitigation through medical literacy directed capabilities
• Patient access to Merck owned medical records
• Improved credentialing and tracking of investigators through digital signatures enabling secure access
Effectiveness and Outcomes
• Today:– Life Science companies each own the transactional infrastructure – Systems are not well integrated across organizational boundaries
– Variations in requirements can lead to investigator frustration, decreased productivity, etc.
– Economic basis for sharing data for secondary use is not sustainable
– Effort to ensure data completeness and quality of intended use is high
• Aspiration:– Investigators leverage the same technology for clinical research as
is used in daily patient care– Infrastructure will be externalized– Variations largely hidden from users– Primary and secondary uses deliver much more value across the
pipeline– External EHR/PHR support MRL research needs in Discovery and
Preclinical Sciences, Development, Regulatory Affairs, and Informatics
“As is” “To be”
for secondary use of healthcare data

A virtuous cycle will be created between primary and secondary use of healthcare data
Patient PCPElectronic
clinical dataImproved and informed
cl inical care
Modeling
Patient ID &
Enrollment
Amendments
Improved modeling through
use of electronic clinical
data (e.g., epidemiology,
observational, interventional
s tudies, etc.)
More rapid,
comprehensive data -
driven patient ID &
enrollment
Fewer amendments through
improved data - driven
protocol design
• Improved understanding and
awareness of:
– Patient populations
– Disease progression and
natural history
– Therapeutics
– Upcoming and ongoing
clinical trials
– Comparative
effectiveness
– Safety and adherence to
medical guidelines
Doctor - patient
interaction
Record cl inical data
in medical record
Primary Use of Data
Secondary Use of Data
Feedback into
clinical care
Diagram from Booz & Company, prepared for PACeR Institute

Current: Culture of oneone
information flows
Many sources with varying curation and little standardization, and overhead to manage all links as “one offs”
Independent interactions i.e. for trial ops and franchise initiatives e.g. translational research
ProviderA
ProviderB
ProviderC Provider
G
ProviderH
ProviderI
ProviderD
ProviderE
ProviderF
ProviderK
Provider...”N”
ProviderJ

Aspirational “To be”Healthcare
Data Aggregator
1
Provider1-1
Provider1-2
Provider1-3..N
Provider2-2
Provider2-3..N
ProviderN-1
ProviderN-2
ProviderN-3..N
ProviderA
ProviderB
Healthcare Data
Aggregator“N”
Healthcare Data
Aggregator2
ProviderC..Z
Services e.g. curate, ensure standards, broker, links back to providers, etc.Support broad/deep data for secondary uses across franchises and
therapeutic areas
Some of the challenges facing growth of secondary use
• Accelerated data generation / EHR adoption fueled by ARRA/HITECH
– A national resource of EHR for secondary will depend on sustainable business models that can support EHR aggregation
• Data may be “miles wide,” but data are often shallow in various areas / don’t cover what is “fit for purpose” for some/all secondary uses
• Diverse data types and formats = integration hurdles for IT
• Multiple organizational silos: data & people
• Increasing number of external collaborations and partnerships
plethora of interchange points
• Limited collaborative data management support
Conclusion: Smart Identification of potential sources, evaluation, and gaining access to EHR is a critical capability for the foreseeable future.

Obtaining EHR for secondary use
• Everything we do in the healthcare ecosystem is for the people.
• Global EHR can be a resource for humanity more valuable than any other
• The healthcare community, including life sciences all have needs for information, and partnering and sharing are the keys to our joint success
• To obtain:1. Be clear what is needed and the value it will provide patients
/ consumers – by therapeutic area, targeted therapy, and its R&D plan
2. Seek3. Find, Refine, Filter4. Evaluate5. Obtain access “fit for purpose”6. Steward as befits information central to human well being and
happiness, assuring privacy and informed consent7. Use responsibly 8. Document value by sharing results as appropriate

A virtuous cycle for
healthcare data
17
Value
Intended
Use
Human Healthcare Ecosystem
Evaluate /
Choose
Obtain,
Steward, Use
Find
Refine
Filter

Where should one start?
0
1
2
3
4
5
6
7
8
9
Need
See
k
Find,
Ref
ine,
Filter
Eva
luate
Obt
ain
Ste
war
d
Use
resp
onsibly
Docu
men
t valu
e
Importance
Implementation Cost
Mean
1. Clarity of need
2. Robust Evaluation

2 case studies• Signature Discovery
– Merck and H. Lee Moffitt Cancer Center & Research Institute Collaboration
– Science requires rich, longitudinal data set which includes de-identified
patient healthcare information and OMICS data e.g. RNA expression appropriate to oncology research
– Information pipeline recognized with the 2008 Bio-IT World Best
Practices Award in Translational and Personalized Medicine
• Clinical trial protocol refinement
– Global Trial Optimization (GTO) team receives protocol draft
– ID draft inclusion and exclusion criteria and required values, and any clinical data collection capabilities that are essential for the trial e.g.
for COPD, quantitative spirometry test data
– Iteratively refine parameters
– Query EMR identifying patients that meet inclusion and exclusion criteria
– Refine query parameters to reduce failure rate for communication back to protocol authors.

Intended use: Protocol Refinement
20
Patient
Patient history &
demographics
History of Present
Illness /
Differential
Diagnosis
Physical
Diagnosis
Therapy / Meds
Outcomes

Intended use: signature discovery and
development
21
Patient
Patient history &
demographics
History of
Present Illness /
Differential
Diagnosis
Physical
Diagnosis
Therapy / Meds
Outcomes
Pathology
Detailed
therapeutic area
data
OMICS Data

Data evaluation...the hard way
• “I can’t be sure of the quality / completeness etc. of the data I have unless I can look at it in a way that is meaningful to me.”
• “These data are not really what I need.”
• The next most common complaint is, “It is too hard to explore the data to ensure it is what I need.”
SDD
Programming
Clinical Data Biosamples
Clinical DataRepository
MolecularData Files
Data Request
Data Results
Days\Weeks
Scientists
Data Managers
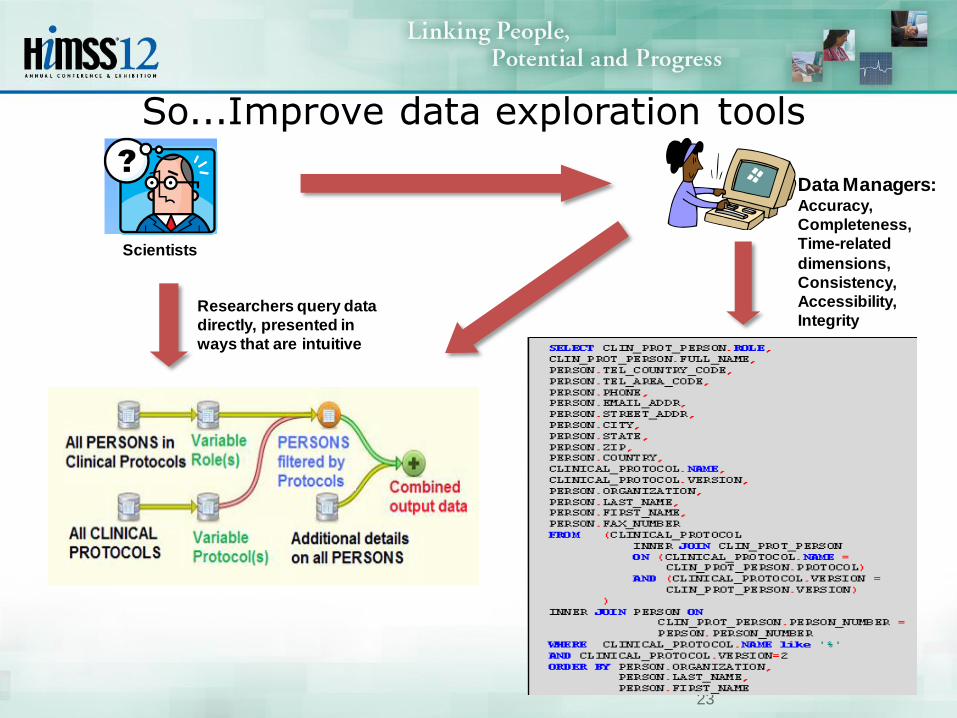
So...Improve data exploration tools
23
Data Managers: Accuracy,
Completeness,
Time-related
dimensions,
Consistency,
Accessibility,
IntegrityResearchers query data
directly, presented in
ways that are intuitive
Scientists

Concluding thoughts• National health reform efforts are moving towards outcome-based
payments, followed by Health IT investments to enable transparency through the capture and exchange of real-world data.
• Outcomes research based on real-world health information is becoming faster, cheaper, and therefore more common. It is essential to improving healthcare.
• Today, life sciences companies have limited access to real-world patient health information, but insights for safety, comparative effectiveness, efficient trial operations, and other areas are within this domain.
• In the face of uncertainty (e.g., equivalent of the dot-com era), too much is lost by waiting.
• Stakeholders across the healthcare ecosystem can proactively partner to ensure stakeholder communities have the differentiated access to real-world health information flows they need to perform their role.

Contact information http://www.merck.com
Gary K. Mallow, Ph.D. MRL IT Director, Healthcare Information Technology Merck & Co., Inc.126 E. Lincoln AvenueRY34-A112Rahway, New Jersey 07065
Office Phone: 732 594-2355 [email protected]