Embed Size (px)
DESCRIPTION
The Value of 3 Tesla Magnetic Resonance Imaging for the Detection and Aggressiveness Assessment of Prostate Cancer
Citation preview

The Value of 3 Tesla Magnetic ResonanceImaging for the Detection and Aggressiveness
Assessment of Prostate Cancer
- From Theory to Practice -
THOMAS HAMBROCK
SIEMENS

The Value of 3 Tesla Magnetic Resonance Imaging for the Detection and Aggressivenes
Assessment of Prostate Cancer
From Theory to Practice
THOMAS HAMBROCK
1

The studies presented in this thesis were carried out at the Department of Radiology, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands, This project was supported by the Queen Wilhelmina Fund from the Dutch Cancer Society.
Nov 2012
Copyright © Thomas Hambrock
Publisher:
ISBN:
2
.
978-90-9027256-6
Nov 2012
Copyright © Thomas Hambrock
Publisher: Drukkerij Efficiënt Nijmegen
ISBN: 978-90-902756-6

The Value of 3 Tesla Magnetic Resonance Imaging for the Detection and Aggressivenes
Assessment of Prostate Cancer
From Theory to Practice
PROEFSCHRIFT
TER VERKRIJGING VAN DE GRAAD VAN DOCTOR AAN DE RADBOUD UNIVERSITEIT NIJMEGEN OP GEZAG VAN DE RECTOR MAGNIFICUS, PROF.
MR. S.C.J.J. KORTMANN, VOLGENS BESLUIT VAN HET COLLEGE VAN DECANEN IN HET OPENBAAR TE VERDEDIGEN OP DINSDAG 4 DECEMBER
2012 OM 13:30 UUR PRECIES
DOOR
THOMAS HAMBROCK
GEBOREN OP 1 SEPTEMBER 1978 TE PRETORIA, ZUID-AFRIKA
3

PROMOTOR : Prof. dr. J.O. Barentsz
COPROMOTOREN : Dr. ir. H.J. Huisman
Dr. ir. T.W.J. Scheenen
Dr. C.A. Hulsbergen-van de Kaa
MANUSCRIPTCOMMISIE : Prof. dr. J. van Krieken
Dr. E. van Lin
Prof. dr. A. Villers (University of Lille)
4
PROMOTOR : Prof. dr. J.O. Barentsz
COPROMOTOREN : Dr. ir. H.J. Huisman
Dr. ir. T.W.J. Scheenen
Dr. C.A. Hulsbergen-van de Kaa
MANUSCRIPTCOMMISIE : Prof. dr. J. van Krieken
Dr. E. van Lin
Prof. dr. G. Villeirs (University of Gent)

Dedicated to my grandfather . . . . . .
HERMANN AUGUST HAMBROCK * 8. MAY 1907 -
Who died at the young age of 63 years due to metastatic prostate cancer.
5


Sir Bertrand Russels (1872-1970)
6


Table of Contents
PART ONE - INTRODUCTION AND BACKGROUND
Chapter 1 . . . . 11 28
Introduction.
Chapter 2 . . . . 29 59
Background to functional MR imaging.
PART TWO - DETECTION OF PRIMARY AND RECURRENT PROSTATE CANCER -
Chapter 3 . . . . 61 82
32-Channel 3T MR guided biopsies of prostate tumor suspicious regions identified on multi-
modality 3T MR imaging : Technique and feasibility. Invest Radiol 2009 [HAMBROCK T,
FÜTTERER JJ, HUISMAN HJ et al.]{Impact factor 4.7}
Chapter 4 . . . . 83 100
MRI guided prostate biopsies in men with repetitive negative biopsies and elevated PSA.
J Urol 2010 [HAMBROCK T, SOMFORD DM, HOEKS C et al.]{Impact factor 3.9}
Chapter 5 . . . . 101 114
MR guided prostate biopsies of DCE-MR imaging suspicious tumor regions for the diagnosis
of prostate cancer following radiotherapy. Invest Radiol 2010 [YAKAR D; HAMBROCK T,
HUISMAN HJ et al.] {Impact factor 4.7}
Chapter 6 . . . . 115 140
Multiparametric MR imaging for detection and localization of low vs. high-grade transition
zone prostate cancer. Radiology Accepted [HOEKS C, HAMBROCK T, YAKAR D et al.]
{Impact factor 6.1}
7

Table of Contents
PART THREE - ASSESSMENT OF PROSTATE CANCER AGGRESSIVENESS -
Chapter 7 . . . . 142 -165
The Relation of Apparent Diffusion Coefficient and prostate cancer Gleason grade in
Peripheral Zone. Radiology 2011 [HAMBROCK T, SOMFORD DM, HUISMAN HJ et al.]
{Impact factor 6.1}
Chapter 8 . . . . 166 182
Initial experience with identifying high-grade prostate cancer using diffusion-weighted MR
imaging in patie -guided biopsy. Invest
Radiol 2012 [HAMBROCK T, SOMFORD DM, OORT I et al.]{Impact factor 4.7}
Chapter 9 . . . . 183 199
In vivo assessment of prostate cancer aggressiveness using three-dimensional proton MR
spectroscopy at 3T with the combined endorectal coil and pelvic phased array coil. Eur
Urol 2011 [KOBUS T, HAMBROCK T, HULSBERGEN C et al.] {Impact factor 8.8}
Chapter 10 . . . . 200 219
Prospective Assessment of Prostate Cancer Aggressiveness using 3 Tesla diffusion weighted
MR imaging guided biopsies versus a systematic 10-Core transrectal ultrasound prostate
biopsy cohort Eur Urol 2012 [HAMBROCK T, HOEKS C, HULSBERGEN C et al.] {Impact
factor 8.8}
PART 4 CALIBRATION/COMPUTER ASSISTED DIAGNOSIS OF PROSTATE CANCER -
Chapter 11 . . . . 221 236
The effect of inter-patient normal peripheral zone apparent diffusion coefficient variation
on the prediction of prostate cancer aggressiveness. (Radiology Accepted) [LITJENS G,
HAMBROCK T, BARENTSZ JO et al.]{Impact factor 6.1}
Chapter 12 . . . . 238 259
Computer-aided diagnosis of prostate cancer using multiparametric 3T MR imaging: Effect
on observer performance. Radiology Accepted [HAMBROCK T, VOS P, BARENTSZ JO et
al.] {Impact factor 6.1}
8
Table of Contents
PART THREE - ASSESSMENT OF PROSTATE CANCER AGGRESSIVENESS -
Chapter 7 . . . . 142 -164
The Relation of Apparent Diffusion Coefficient and prostate cancer Gleason grade in
Peripheral Zone. Radiology 2011 [HAMBROCK T, SOMFORD DM, HUISMAN HJ et al.]
{Impact factor 6.1}
Chapter 8 . . . . 165 182
Initial experience with identifying high-grade prostate cancer using diffusion-weighted MR
imaging in patie -guided biopsy. Invest
Radiol 2012 [HAMBROCK T, SOMFORD DM, OORT I et al.]{Impact factor 4.7}
Chapter 9 . . . . 183 199
In vivo assessment of prostate cancer aggressiveness using three-dimensional proton MR
spectroscopy at 3T with the combined endorectal coil and pelvic phased array coil. Eur
Urol 2011 [KOBUS T, HAMBROCK T, HULSBERGEN C et al.] {Impact factor 8.8}
Chapter 10 . . . . 200 220
Prospective Assessment of Prostate Cancer Aggressiveness using 3 Tesla diffusion weighted
MR imaging guided biopsies versus a systematic 10-Core transrectal ultrasound prostate
biopsy cohort Eur Urol 2012 [HAMBROCK T, HOEKS C, HULSBERGEN C et al.] {Impact
factor 8.8}
PART 4 CALIBRATION/COMPUTER ASSISTED DIAGNOSIS OF PROSTATE CANCER -
Chapter 11 . . . . 221 236
The effect of inter-patient normal peripheral zone apparent diffusion coefficient variation
on the prediction of prostate cancer aggressiveness. (Radiology Accepted) [LITJENS G,
HAMBROCK T, BARENTSZ JO et al.]{Impact factor 6.1}
Chapter 12 . . . . 238 259
Computer-aided diagnosis of prostate cancer using multiparametric 3T MR imaging: Effect
on observer performance. Radiology Accepted [HAMBROCK T, VOS P, BARENTSZ JO et
al.] {Impact factor 6.1}

Table of Contents
PART 5 - DISCUSSION, CONCLUSIONS AND FUTURE PERSPECTIVES -
Chapter 13 . . . . 261 292
Discussion, conclusions and future perspectives
Chapter 14 . . . . 293 308
English summary - Nederlandse samenvatting
PART SIX POSTLUDE
A. List of Publications . . . . 310 314
B. List of Presentations Scientific Paper Presentations . . . . 315 316
C. List of Presentations Presentations on Invitation . . . . 317 317
D. List of Awards . . . . 318 318
E. Curriculum Vitae . . . . 319 319
F. Dankwoord . . . . 320 322
9
PART SIX POSTLUDE
A. List of Publications . . . . 311 315
B. List of Presentations Scientific Paper Presentations . . . . 316 317
C. List of Presentations Presentations on Invitation . . . . 318 318
D. List of Awards . . . . 319 319
E. Curriculum Vitae . . . . 320 320
F. Dankwoord . . . . 321 323


PART ONE
INTRODUCTION AND BACKGROUND


— CHAPTER 1 —
Introduction
CHAPTER 1CHAPTER 1

Introduction 1
GENERAL INTRODUCTION
March 2011, the Netherlands:
[UROLOGIST] : “Mr. v. R, your PSA levels have now continuously been rising over the last 8
years from 3 ng/ml to 50 ng/ml. You have severe allergies to multiple antibiotics. So I think
prostate biopsies are no option.”
[PATIENT MR. v. R]: “How can we exclude prostate cancer then?”
[UROLOGIST]: “Apart from biopsies, which we cannot perform in your case, there is no
alternative.”
[PATIENT MR. v. R]: “I have heard that MRI can be used for prostate cancer detection.”
[UROLOGIST]: “Nonsense, you cannot see prostate cancer on MRI!”
This is a true conversation which has taken place in a first world country at the beginning of the
year 2011. The patient mentioned above, was the second last patient (prior to writing this
introduction) the author of this book had scanned using multi-parametric MRI for the evaluation
of prostate cancer. After patient persistence, a biopsy was performed under special antibiotic
coverage. The final diagnosis on biopsy: prostate cancer in all 10 biopsy cores left and right,
Gleason Score 4+3=7. Following MR imaging, extracapsular extension with neurovascular
bundle infiltration and seminal vesicle invasion was diagnosed. In addition, the presence of
metastatic lymph nodes was also established. Radiological stage T3B N1 M0 disease. Treatment
with intent to cure: unlikely.
The author can only stand in awe and disbelief when such hesitancy, ignorance and lack of
knowledge in the year 2011 is still present in a first world country. A change has to be brought
about. Not a mere change, but more importantly “A PARADIGM SHIFT”.
There is probably no single word in human history which has caused so much fear, suffering,
and inner turmoil both on the side of the patient as well as the side of relatives and friends as the
word: “CANCER”. Celsus (28 BC - 50 AC), a Roman doctor, translated the Greek word "carcinos"
12
Introduction 1

Introduction 1
into the word "cancer", a Latin word meaning crab or crayfish as a symbol of being eaten and
torn apart by a crab (cancer). The fear this word arose has elicited the greatest battle fought on
earth, the battle of the inner mind. The author subjectively is of the opinion that in the 21st
century, cancer has become more of a mental burden to humans than a physical one, without
downplaying the severe physical suffering of millions of patients who die to this conglomerate of
diseases or suffer severe morbidity thereof.
The cover page of Section One – Introduction and Background, reveals the scene from Leonardo
da Vinci’s (1452-1519) lost painting, “The Battle of Anghiari” (1505), believed to be still hidden
beneath later frescoes in the Hall of Five Hundred in the Palazzo Vecchio, Florence, Italy. The
current picture is a painting of the original made by the famous Flemish painter Peter Paul
Rubens (1577-1640) and this copy can still be appreciated in the Louvre, Paris, France. To the
author, this painting is the perfect reflection on the current state of the diagnosis and
management of prostate cancer. It is a state of war, blood, tears, swords and horses and sounds
of thunder. Truly a state of chaos!
It is therefore the humble vision of the author that this current thesis may provide a stepping
stone to bring about A PARADIGM SHIFT in the Prostate World of Warcraft. This thesis is not
THE paradigm shift, but merely the beginning of a stone that has become dislodged, one that in
combination with many new scientific insights will bring about this future shift. It is inherent to
human nature to resist an alteration of one’s chosen path, especially if one had trod that path for
so many years. As the medical community gains more scientific evidence, and as the plight of the
patient is increasingly recognized, a more peaceful path can be taken along the long journey of
prostate cancer. There will be a different way of thinking and a different way of “doing”. The
author agrees with the Joker from the movie Batman, who said: “I like to rattle cages”. If cages
are rattled and people are stirred by the content of this thesis and awakenings happen, then it
has fulfilled its purpose already. May this hold true for radiologists, oncologists, urologists,
radiotherapists and patients alike!
It is exceptional in modern days for “new” discoveries, inventions or advances in science to be
labeled to the sole genius of a single persons work. For all scientific facts that we unravel and
discover in current year and age, the author humbly and whole heartedly is obliged to agree with
Bernard of Chatres († 1124) who said:
13
Introduction 1

Introduction 1
"Nos esse quasi nanos, gigantium humeris insidentes, ut possimus plura eis et remotiora videre, non
utique proprii visus acumine, aut eminentia corporis, sed quia in altum subvenimur et extollimur
magnitudine gigantea"
“We are like dwarfs on the shoulders of giants, so that we can see more than they, and things at a
great distance, not by virtue of any sharpness of sight on our part, or any physical distinction, but
because we are carried high and
Cedalion standing on the shoulders of the giant Orion, by Nicolas Poussin, 1658
In the current chain of inventions and groundbreaking discoveries, as well as the small
improvements which have lead to some of the MR imaging advances in prostate cancer as
outlined in this thesis, the author can merely acknowledge that we and our work are dwarfs on
the shoulders of giants. Many giants have been before us lifting us high to see what we currently
see. It is important in this thesis to mention a few of the hundreds of giants: Conrad Röntgen
(1845-1923) the discoverer of Röntgen rays and therefore the father of the most exciting field in
medicine: Radiology; Rudolf Virchow (1821-1902) whose pioneering work in the field of
14
Introduction 1

Introduction 1
histopathology has introduced the “gold standard” of all our work – the father of Histopathology.
Furthermore the ingenious work of Max Planck (1858-1947), regarded as the father of
Quantumphysics which underlies the crucial fundamentals of magnetic resonance imaging and
with which Walther Gerlach (1889-1979) later discovered the spin quantification in a magnetic
field, thereby serving as the beginning point of MRI. The ground breaking and fundamental
work on prostate cancer pathology and assessment, later referred to as the Gleason Scoring
system cannot be omitted by mentioning the giant: Donald F. Gleason (1920-2008).
In memory of these and many other “Giants” who paved the way of science…..
Conrad Röntgen Max Planck Rudolf Virchow
Walther Gerlach Donald Gleason
15
Introduction 1

Introduction 1
INTRODUCTION TO PROSTATE CANCER
Why is the prostate so important? This little organ which serves a crucial role in the
reproductive capabilities of the human species. However, for other reasons it has much greater
importance. The greatest importance is the effect that this organ has on the mind of the man
(agreeing that the external male sexual organs probably have a larger impact). It is rumored
that the sexual wellbeing of a woman is directly related to the wellbeing of the male prostate.
Most articles dealing with prostate cancer (PCa) all start with mentioning the prevalence and
mortality and the great burden prostate cancer has on society. Especially the notion that 1 in 6
men will develop prostate cancer is enough the let the war trumpets sound for the Battle of
Anghiari. A second disturbing phrase is so often mentioned in combination with PCa: “Surely sir,
you are more likely to die with prostate cancer than from it.” While this is true for a large
proportion of patients, this undoubtedly adds to the turmoil, chaos and bewilderment mostly on
the side of the patient. It is almost unfathomable that such a minute organ as the prostate has
become galactic in size (regarding the amount of literature on it and for some patients, this
organ, even in the benign state, can become truly gigantic). It is therefore purposeless and futile
to give a full introduction on this topic. To vaguely unravel the chaos of the Battle of Anghiari,
the author wishes to mention a few epidemiological, statistical and pathological points,
especially to introduce the unacquainted reader with some background to assist in reading this
thesis. More details especially on the anatomy and pathology of prostate cancers will become
evident in later chapters.
Indeed, PCa has become the most widely diagnosed cancer in males with 29% of all cancer
diagnoses being prostate cancer. Equally, in females, breast cancer has become the mostly
diagnosed malignancy, representing 29% of all cancers being diagnosed. For both, the absolute
mortality figures are only surpassed by lung cancer. These figures are surely shocking as regard
to the absolute numbers, being slightly over 240 000 diagnosed new cases for prostate and
220 000 breast cancers in the U.S.A. (1) and around 10 000 prostate cancers diagnosed in the
Netherlands in 2010. According to the American cancer statistics of 2012, around 12% of men
diagnosed with PCa succumb from their prostate cancer compared to 17% for females with
breast cancer. Therefore, a considerable difference exists in being diagnosed with PCa and
eventually dying from it. It is however important to consider the fact that patients currently
16
Introduction 1

Introduction 1
dying from PCa are more often elderly men who have “missed” the earlier screening and
effective therapy now offered to younger patients. Therefore the likelihood of dying from
prostate cancer when one is currently (in the year 2012) diagnosed with the disease, is expected
to be much lower. About 3.5% of all male deaths are from PCa, making the lifetime risk that a
man will succumb of this disease about 1 in 28. This compares to the lifetime risk of dying in a
car accident, about 1 in 4 000 or in an airline accident about 1 in 100 000 (2).
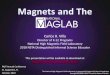
Figure 1. Cancer Statistics 2012 in U.SA. from Siegel et al.(1)
Prostate cancer has been known as a disease of elderly men. It is therefore not surprising that
2/3 of all PCa deaths occur in men > 75 years. Although ~ 1 in 7 (14%) of men die from PCa,
only 1 in 20 (5%) of these deaths are “premature” (the author acknowledges that this might be
arbitrarily in the modern age), occurring in men younger < 75 years. Diagnosis is rare before
age 50, but after this age incidence increases exponentially and the rate of increase is faster than
seen in other malignancies.
17
Introduction 1

Introduction 1
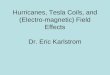
Figure 2. Worldwide incidence and mortality of prostate cancer. (3;4)
Yet, many publications advocated that at least 50% of currently diagnosed prostate cancer are
indolent or insignificant, comprising small (< 0.5 cc) tumours with only well differentiated
components (Gleason grade 3 or less) that apparently won’t lead to death or morbidity. From a
statistical point of view, this is true. There is a great advocacy that men diagnosed with such
cancers should be left alone and sent home. The author wishes to make a bold and provocative
statement that this is not true. Every cancer begins with one cell, then two then four …. until it
has reached great size and metastasizes. Additionally, it appears that most humans are not born
with cancers or with an increased likelihood of genetic mutation. These occur most often de
novo during their life time. Even if there are hereditary components, a two-hit sequence is often
needed for eventual manifestation of disease. From postmortem examination, the true
prevalence of prostate cancer in all ages is at the least to say, catastrophic. The author
contemplates that he himself (at the age of 33 years) has a likelihood of around 25% of
harboring PCa as these sentences are written. Yet this “toothless lion” sometimes grows teeth
and sometimes not. Sometimes it sleeps in its den and sometimes it comes out to feed. When
and why, we don’t know. At least, not yet!
18
Introduction 1

Introduction 1
Figure 3. Prevalence of PCa in Autopsy of white American males. Delongchamps et al.(3)
There is no current evidence (and this is also very difficult to prove) to show that aggressive
prostate cancers (that eventually lead to morbidity and mortality), start their life as aggressive
(meaning Gleason grade 4/5) small tumours. The vast majority of aggressive tumours have well
differentiated components as well. Would an aggressive proliferating cell suddenly turn benign?
The contrary is rather the case. Therefore, a substantial number of tumours begin as well
differentiated “good little cancers” – the wolf in sheepskin. For reasons unknown, some of these
tumours (probably undergoing additional mutations under carcinogenic or other influences)
undergo further dedifferentiation into tumours that cause eventual clinical problems.
It is the burden of the scientific community to unravel which tumours have the potential to cause
problems in the future from those who don’t. Probably this is not possible at all, as visiting the
“Oracle of Delphi” is not an option anymore and future additional mutations cannot be predicted.
They happen when they happen. Therefore the author undoubtedly is of the opinion that these
“good little cancers” should not be diagnosed at all (in their sheepskin phase) and only the
tumours with potential asocial behavior identified early and treated, BUT that all patients should
be offered a reliable method to follow them through life to identify when good tumours show
19
Introduction 1

Introduction 1
aggressive dedifferentiation and further treatment is necessary. This thesis presents some
important concepts that will lift the veil of what is possible, both now, and in the future.
Nearly every aspect of PCa generates controversies for both doctors and patients. While dietary
fat of animal origin has repeatedly been associated with the risk of developing and dying of
prostate cancer, there is no clear evidence yet that dietary alterations or supplementation of
micronutrients can prevent or modify the course of this disease. Similarly, diagnosis and staging
are also controversial. While the introduction of the serum Prostate Specific Antigen (PSA) has
dramatically changed the rate of PCa diagnosis and altered the stage at diagnosis, it has often
been criticized for its lack of specificity resulting in over performing random prostate biopsies
and leading to over detection of innocuous cancers. Despite this, its role in the current and
future diagnosis of prostate cancer remains.
Unfortunately many (especially older, for some reason, mostly German) physicians rely and
swear on their own fingers capabilities to “feel” and therefore diagnose prostate cancers with a
high certainty. Needless to say, only a small proportion of the prostate gland can be felt by
digital rectal examination (DRE). DRE is unfortunately too often used to stage prostate cancer
and to make decisions regarding preservation (albeit not) of the neurovascular bundles during
radical prostatectomy. The overall sensitivity for the digital rectal examination is only 37% (5).
The author is of the opinion that the digital rectal examination should rather be placed in the
spiritual, more theological realm. One definitely needs a divine finger to rely on (Fig. 4), when
dealing with prostate cancer. As Prof. Barentsz always says, “Our fingers have no eyes but we have
MRIs!” The fallen “Finger of God” in South-West Africa (fallen 1988) (Fig. 5) serves as an
understatement of the current role of DRE in prostate cancer diagnosis and management. Of
course, the exception is the case, where tumours are only initially identified using DRE. It
however still has some role to play in the subjective experience, both by patient and physician,
that a “thorough” examination was performed.
20
Introduction 1

Introduction 1
Figure 4. The Divine finger (needed to be good in cancer detection and staging) by
Michelangelo, Cistine chapel, 1511. Figure 5. in Namibia, fallen down
in 1988.
PCa is often (not always) detected by multiple, “systematic” but actually random, transrectal
needle biopsies of the prostate, rather than targeted biopsy of a palpable nodule or a lesion
visible by imaging. There is no other solid organ in which “blinded” biopsies are performed to
make a diagnosis. Both patient and clinicians alike would vehemently resist the possibility that
for example breast cancer should be diagnosed by performing 20 odd blind biopsies of the
breast on each side, hoping to have struck the tumour nodule hiding in the abundance of fat and
glandular tissue. This however was and is still the case with prostate cancer. Different biopsy
schemes have been advocated to “strike gold” more often.
Figure 6. Prostate biopsy schemes and cancer detection rates as advocated by Presti (6)
21
Introduction 1

Introduction 1
Once detected, the size, location and extent of the lesion, as well as its grade, are difficult to
determine with precision. It is commonly known that biopsy results underestimate the extent
and grade of the cancer. Unfortunately many clinicians still lack confidence in imaging, despite
substantial progress being made in the field of MRI. Clinicians’ recommendation for treatment,
therefore, arises from a profound sense of uncertainty about the precise nature of the cancer
they are treating. After diagnosis, treatment decisions are hampered by further difficulties in
accurately staging the disease. In this atmosphere it is no wonder that treatment decisions are
so difficult for patient and their physicians. For the patient who chooses active rather than
deferred therapy, which treatment is best: radical prostatectomy, external beam irradiation,
brachytherapy or some combination? Not only do the treatments differ in timing of onset and
degree of side effects, but the likelihood of cancer control. The number of complications and
side effects depend as much on the specific technique employed as well as the expertise of the
treating physician on the method of therapy chosen.
22
Introduction 1

Introduction 1
AIM OF THESIS
Figure 7. PCa
Undoubtedly a substantial number of factors play a role in the chaotic nature of the Battle of
Anghiari. The author started his thesis with the confident hope of trying to unravel this battle
with one overriding consideration:
, identify the clinical problem, then identify why there is a problem, then find a solution to
solve this problem.
The author was fortunate to have been able to build on the important foundations of MR imaging
of the prostate, laid down by the valuable research done in Nijmegen by his PhD predecessors.
Only with this foundation, is the continuous work and developments highlighted in this thesis
possible.
Problems faced by Clinicians:
1. Patients with an elevated/elevating PSA value but persistent negative TRUS
biopsies, are of considerable concern. Does he have cancer or not? Should further
TRUS biopsies be performed or not?
2. If MRI is accurate in identifying a tumour location, what effective method is there
to reliably obtain histological proof of this location?
23
Introduction 1

Introduction 1
3. After radiation therapy for PCa, diagnosing local recurrence vs. metastatic disease
when the PSA starts rising again, is challenging.
4. Pretreatment identification of prostate cancer aggressiveness is crucial for
management and prognostication. The current methods to determine this are
inaccurate. What in vivo methods are available to reliably predict PCa nature?
5. When a patient is diagnosed with PCa Gleason Score 3+3=6 on biopsy, is there a
method available to reliably aid in differentiating those patients where biopsies
represent an undergrading (and therefore need more radical therapy) from those
where it is a correct prediction (and therefore may be managed more
conservatively)?
6. Transrectal ultrasound guided biopsies only reflect the true aggressiveness i.e.
Gleason grade in about 60% of patients. Are there any methods to improve the
tumour aggressiveness representativeness in biopsy samples on which further
management decisions can be based?
Problems faced by Radiologists:
7. No prostate looks alike. In particular the transition zone is a radiologically chaotic
region. What multi-parametric MR imaging features and techniques are available
8. What is normal? In one sue looks different from
tissue in a different
quantitative measurements and our assessment of what is malignant?
9. It is often mentioned that prostate multi-parametric MR imaging should be left to
the experts. The prostate is too complex, too many imaging modalities are needed
and tumours are very heterogeneous. Is there any help for the non-expert?
THE AIM of this thesis therefore is to target these specific problems faced by doctors and
patients and develop and validate methods in order to provide solutions for them.
24
Introduction 1

Introduction 1
OUTLINE OF THESIS
In contrast to PhD theses in other non-medical fields, the fragmented nature of writing a thesis
in a medical science is based on the fact that a number of chapters should be based on peer
reviewed articles. Therefore each chapter has a similar repetitive composition being outlined in
an introduction, materials and methods, results, discussion and conclusions. Many chapters
start of with a similar introduction and to the unacquainted, this might appear cumbersome and
excessively repetitive. This is unfortunately a drawback of medical PhD theses. Yet, each
chapter can be read as a small thesis in itself, with a sufficient overview to provide the reader
with insight into the clinical question addressed in that chapter. Most chapters therefore will be
read and understood separately instead of seeing the complete picture. Many pictures, diagrams
and images are provided throughout the thesis. Radiologists are undoubtedly visually
stimulated creatures who are notoriously easily bored by great amounts of text.
This thesis is spread in 6 principal parts. PART ONE includes Chapter 1 and 2 which provide an
Introduction and Background to this thesis. PART TWO deals with the detection of primary
and recurrent prostate cancer and includes Chapter 3-6. PART THREE consists of the
assessment of PCa aggressiveness and includes Chapter 7-10. PART FOUR deals with
computerized calibration of “normal” peripheral zone tissue for increased accuracy in
assessment of aggressiveness and this is presented in Chapter 11. Chapter 12 deals with
computer aided diagnosis. PART FIVE is the finale, dealing with a discussion, conclusion and
future perspective, being outlined in Chapter 13. An English and Dutch summary is given in
Chapter 14. PART SIX is the usual postlude including a list of publications, presentations and
prizes, words of gratitude and ending with a short curriculum vitae.
25
Introduction 1

Introduction 1
PART ONE INTRODUCTION and BACKGROUND
Chapter 1 provides the non acquainted reader with a broad introduction in the interesting field
of prostate cancer demographics, diagnostics and sets the basis for the problem-solution
orientated approach as is presented in this thesis.
Chapter 2 provides an introduction and basis of understanding for the advanced functional MR
imaging modalities that are tested and validated in this thesis. These modalities consist of
Dynamic Contrast Enhanced MRI (DCE-MRI) and Diffusion Weighted Imaging (DWI) with the
derived Apparent Diffusion Coefficient (ADC) maps.
PART TWO DETECTION of PRIMARY and RECURRENT PROSTATE CANCER
Chapter 3 describes the feasibility and method of using an MR compatible transrectal biopsy
device within a 3 Tesla MRI scanner, to obtain biopsies of tumour suspicious regions on multi-
parametric MR imaging.
Chapter 4 goes further and determines the value of MR guided biopsies on the yield of prostate
cancer in men with elevated PSA > 4 ng/ml and more than two prior negative TRUS guided
biopsy sessions. Furthermore, it also determines the location of tumours not found by
conventional biopsy techniques and the significance of the detected tumours.
Chapter 5 determines if DCE-MRI can be a useful technique to detect local recurrence of PCa
following external beam radiotherapy. Furthermore it evaluates if the MR guided biopsy
procedure is a useful technique for providing definite histological proof thereof.
Chapter 6 deals with transition zone cancers and evaluates the role of the individual anatomical
and functional MR imaging modalities to detect and localize low- vs. high-grade tumours.
PART THREE ASSESMENT OF PROSTATE CANCER AGGRESIVENESS
Chapter 7 evaluates the relationship between ADC values of tumour in the peripheral zone and
aggressiveness of prostate cancer and establishes a basis for a further study which prospectively
determines the Gleason grades prior to treatment.
Chapter 8 reports on the initial experience with identifying PCa undergrading using DWI
derived ADC values in patients wi TRUS-guided biopsy.
26
Introduction 1

Introduction 1
Chapter 9 determines the potential value of 1H-MRSI in the assessment of prostate cancer
aggressiveness.
Chapter 10 evaluates the value of using DWI combined with MR guided biopsies to
prospectively improve the pretreatment prediction of true prostate cancer aggressiveness.
These findings are then compared to the conventional 10-core TRUS biopsy scheme.
PART FOUR COMPUTER AIDED DIAGNOSIS OF PROSTATE CANCER
Chapter 11 builds on the findings reported in Chapter 7. The substantial variation in normal
peripheral zone ADC values is used for calibration. Re-assessment is done for this this mixed
model incorporating both normal peripheral zone as well as tumour ADC values for
improvement in tumour aggressiveness differentiation.
Chapter 12 shows the development of a computer aided diagnosis (CAD) technique using both
quantitative pharmacokinetic parameters derived from DCE-MRI combined with quantitative
ADC values from DWI to differentiate tumour from benign tissue (but with tumour suspicious
characteristics) with a high diagnostic accuracy. This CAD system is then tested on multiple
less-experienced and experienced readers in evaluation of prostate MRI and determines if the
less-experience reader can be aided to improve his/her assessment of prostate tumours.
PART FIVE - DISCUSSION, CONCLUSION, FUTURE PERSPECTIVES
Chapter 12 provides a detailed discussion, conclusion and considers the future perspectives.
Chapter 13 an English and Dutch Summary
PART SIX THE POSTLUDE
List of Publications
List of Presentations both Scientific and Invited
Awards
27
Introduction 1

Introduction 1
REFERENCES
1. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J.Clin. 2012 Jan;62(1):10-29.
2. Scardino PT, Kelman J.K. Dr. Peter Scardino's Prostate Book. New York, Avery Press: 2005.
3. Delongchamps NB, Singh A, Haas GP. The role of prevalence in the diagnosis of prostate cancer. Cancer Control 2006 Jul;13(3):158-68.
4. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J.Clin. 2005 Mar;55(2):74-108.
5. Schroder FH, van der MP, Beemsterboer P, Kruger AB, Hoedemaeker R, Rietbergen J, Kranse R. Evaluation of the digital rectal examination as a screening test for prostate cancer. Rotterdam section of the European Randomized Study of Screening for Prostate Cancer. J.Natl.Cancer Inst. 1998 Dec 2;90(23):1817-23.
6. Presti JC, Jr., O'Dowd GJ, Miller MC, Mattu R, Veltri RW. Extended peripheral zone biopsy schemes increase cancer detection rates and minimize variance in prostate specific antigen and age related cancer rates: results of a community multi-practice study. J.Urol. 2003 Jan;169(1):125-9.
28
Introduction 1

Introduction 1
REFERENCES
1. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J.Clin. 2012 Jan;62(1):10-29.
2. Scardino PT, Kelman J.K. Dr. Peter Scardino's Prostate Book. New York, Avery Press: 2005.
3. Delongchamps NB, Singh A, Haas GP. The role of prevalence in the diagnosis of prostate cancer. Cancer Control 2006 Jul;13(3):158-68.
4. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J.Clin. 2005 Mar;55(2):74-108.
5. Schroder FH, van der MP, Beemsterboer P, Kruger AB, Hoedemaeker R, Rietbergen J, Kranse R. Evaluation of the digital rectal examination as a screening test for prostate cancer. Rotterdam section of the European Randomized Study of Screening for Prostate Cancer. J.Natl.Cancer Inst. 1998 Dec 2;90(23):1817-23.
6. Presti JC, Jr., O'Dowd GJ, Miller MC, Mattu R, Veltri RW. Extended peripheral zone biopsy schemes increase cancer detection rates and minimize variance in prostate specific antigen and age related cancer rates: results of a community multi-practice study. J.Urol. 2003 Jan;169(1):125-9.
28
Introduction 1


CHAPTER 2
Background to Functional MR Imaging of the Prostate
T. Hambrock; C. Hoeks, R. Somford et al.
CHAPTER 2CHAPTER 2

Background to Functional MRI of the Prostate 2
The content of this chapter is principally based on three publications:
Dynamic contrast enhanced MR imaging in the diagnosis and management of prostate
cancer; Categorical Course in Diagnostic Radiology: Genitourinary Radiology 2006.
Hambrock T, Padhani A, Tofts P et al.
Diffusion and perfusion MR imaging of the prostate; Magnetic Resonance Imaging Clinics
of North America 2008. Somford R, Fütterer J, Hambrock T.
Prostate Cancer: Multiparametric MR imaging for Detection, Localization and Staging;
Radiology 2011. Hoeks C, Barentsz J, Hambrock T et al.
INTRODUCTION
The development of clinical utilization of MRI, culminating from multiple important
breakthroughs in quantum mechanics, is according to the author one of the most ingenious
developments of the 20th century. The basic principals underlying magnetic resonance imaging
are extremely complex (and extremely interesting) and it is definitely beyond the scope of this
thesis to provide a thorough introduction to physical principals underlying it. However, the
principals underlying more recent developments in functional MR imaging modalities incl.
Diffusion Weighted Imaging (DWI) and Dynamic Contrast Enhanced Imaging (DCE) will be
explained in more detail as these were the most important techniques evaluated in this thesis.
Additionally, a brief overview is given of the pathophysiological processes which underlie
imaging of the prostate. For a more detailed understanding of the physics underlying MRI, the
reader is referred to: MRI in Practice by Catherine Westbrook (1).
BASIC PRINCIPALS OF MAGNETIC RESONANCE IMAGING
Certain atoms are characterized by their tendency to align their axis of magnetic moment to an
external magnetic field. This happens because of their inherent angular moment or spin, as they
contain positively charged protons, that is, they possess electrical charge. The laws of
electromagnetic induction (as described originally by Faraday) refer to three individual forces
30
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
motion, magnetism and charge. The law of Faraday states that if two of these forces are present,
then the third is automatically induced. Atoms that have the properties of aligning along a
magnetic field are amenable to MR imaging. The most important one is hydrogen (1H), partially
because of its profound abundance in living matter, but also because of its large gyromagnetic
ratio. Certain isotopes of particular nuclei including carbon (13C), phosphorus (31P) and fluorine
(19F) are also amenable to MR imaging.
Figure 1. Random positioning of hydrogen atoms in the absence of a magnetic field (left)
and alignment against/with the main magnetic field (depending on their energy) (right).
When hydrogen atoms are aligned within the external magnetic field, a precession occurs
around the field with a specific frequency (for a 3T magnet this is 127 MHz). If an external
radiofrequency pulse is applied at this exact frequency, low energy hydrogen atoms aligned with
the magnetic field (y-axis) are flipped over causing a change in the net magnetization moment.
The net magnetization is now in the transverse plane (x-axis). After the RF pulse, the net
magnetization slowly returns to the y-axis. Recovery of longitudinal magnetization (y-axis) is
caused by nuclei giving up their energy to the surrounding environment. The rate of recovery is
an exponential process with a recovery time constant called the T1 time. This is the time it takes
63% of the longitudinal magnetization to recover. T2 decay of transverse magnetization is
caused by nuclei exchanging energy with neighboring nuclei. The rate of loss of coherent
transverse magnetization is also an exponential process, with the T2 relaxation time of a tissue,
the time it takes for 63% of the transverse magnetization to be lost. Using a receiver coil placed
31
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
over the patient this change in magnetization after the RF pulse can be measured. The T1 and
T2 time for different tissues and molecules differs
between tissues on MR imaging.
Figure 2. Schematic presentation of the sequence of events in an MRI scanner. After the
RF pulse on the hydrogen atoms, placed in a magnetic field, spin magnetization is flipped
into the transverse direction.
A clinical 1.5T MRI scanner T1-w image of the prostate T2-w image of the prostate
The T1-weighted (T1-w) and T2-weighted (T2-w) images are considered anatomical images and
the functional MR imaging modalities considered hereafter are DCE-MRI and DWI-MRI with the
exception of MR spectroscopic imaging, not included in this chapter.
32
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
A. DYNAMIC CONTRAST ENHANCED MRI
Pathophysiological basis - Angiogenesis and the prostate
For a prostate tumour, one critical factor that affects development, growth, invasiveness, and
progression into the metastatic form is the ability of the tumour to generate new blood vessels.
Angiogenesis, which we define as the sprouting of new capillaries from existing blood vessels,
and vasculogenesis, the de novo generation of new blood vessels, are the two primary methods of
vascular expansion by which nutrient supply to tumour tissue is adjusted to match physiologic
needs. Angiogenesis is an essential component of several normal physiologic processes,
including menstrual cycle changes in the ovaries and uterus, organ regeneration, wound healing,
and the spontaneous growth of collateral vessels in response to ischemia (2). Pathologic
angiogenesis is an integral part of a number of disease states, including rheumatoid disease, age-
related macular degeneration, proliferative retinopathy, and psoriasis, as well as being critical
for the growth and metastasis of malignant tumours (3).
A number of different mechanisms are involved, including vessel sprouting and bridge
formation. These processes depend on the migration and proliferation of endothelial cells.
Circulating endothelial progenitor cells derived from bone marrow are also recruited to sites of
active angiogenesis by tumour-derived growth factors such as vascular endothelial growth
factor (VEGF) (4). Tumour growth larger than 1 2 mm in diameter in solid tissues cannot occur
without vascular support (5). Tumour neovascularization often lags behind tumour growth,
leaving areas of low oxygen tension (hypoxia). The decrease in oxygen tension stimulates
further angiogenesis through various signaling pathways by the production of numerous
transcriptional factors, the most important being hypoxia-inducible factors (HIFs), especially
HIF-1 and HIF-2 (6). In the presence of hypoxia, HIF-1 binds to HIF-1 at the HIF response
elements (HREs); this is made possible because HIF-1 does not undergo hydroxylation and
subsequent degradation. Many of the genes activated by the HIF-HRE complex are beneficial to
tumour survival, including those involved in angiogenesis (VEGF), glucose metabolism (glucose
transporter 1), proliferation (insulin-like growth factor 2), and pH regulation (carbonic
anhydrase 9) (7) (Fig 1). Mediation of the physiologic and pathologic stimulation that causes a
33
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
change in cellular phenotype is enacted by a variety of pro-angiogenic factors, which include the
following: (a) VEGF, the most prominent of the angiogenic stimulators; (b) thymidine
phosphorylase, also known as platelet-derived endothelial growth factor; (c) matrix
metalloproteinases (MMPs), a multifarious family of proteolytic enzymes involved in the
breakdown of extracellular matrix; (d) carbonic anhydrase 9, an enzyme that catalyzes the rapid
conversion of carbon dioxide and water into carbonic acid, protons, and bicarbonate ions; and
(e) cyclooxygenase-2, a key enzyme in the prostaglandin biosynthesis pathway that converts
arachidonic acid to prostaglandin (7).
Figure 1. Cascade of gene activations with HIF, after hypoxic stimulation. Cascade results
in eventual angiogenesis to overcome the hypoxia. CA-9 = carbonic anhydrase 9, COX-2 =
cyclooxygenase-2, GLUT-1 = glucose transporter 1.
The importance of angiogenesis in prostate cancer is well established. Angiogenesis is an
integral part of benign prostatic hyperplasia, is associated with prostatic intraepithelial
neoplasia, and is a key factor in the growth and metastasis of prostate cancer (Fig 2). The results
of some studies have demonstrated a direct correlation of angiogenesis with Gleason score,
tumour stage, progression, metastasis, and survival (8,9). Angiogenesis is not directly associated
34
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
with serum PSA levels, which might reflect the ability of PSA to convert plasminogen to
angiostatin-like fragments, possibly contributing to the slow growth of prostate tumours.
Expression of angiogenic cytokines in prostate cancer might be induced as a response to hypoxic
stress or by hormonal stimulation but can also result from activation of oncogenes. The
angiogenic process in prostate cancer is highly dependent on VEGF. VEGF is produced in
abundance by the prostatic secretory epithelium of normal, hyperplastic, and tumour-containing
prostate glands. With respect to the vasculature, it is clear that VEGF is required for vascular
homeostasis in benign prostatic hyperplasia, and the overproduction of VEGF maintains a high
fraction of immature vessels (those without investing pericytes and/or smooth muscle cells) in
prostate cancers (10,11). In the prostate, production of VEGF requires continual stimulation by
androgens, and at androgen withdrawal, VEGF expression is down-regulated, and tumours
undergo vascular regression before tumour cell death (12). VEGF has a positive association with
microvessel density, tumour stage and grade, and disease-specific survival in patients with
prostate cancer (13). As noted earlier in this section, HIF-1 is a key mechanism for VEGF
regulation, and it is known that HIF-1 is up-regulated in the majority of prostate tumour tissues
and that its expression is induced in prostate cancer in situ (14).
Figure 2. Growth and metastasis of tumour with hypoxia-induced angiogenesis, mediated
by VEGF.
35
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
Role of DCE-MRI in visualizing angiogenesis in the prostate
A number of distinguishing features are characteristic of malignant vasculature, many of which
are amenable to study with dynamic contrast agent enhanced MR imaging methods. These
features include (a) spatial heterogeneity and chaotic structure: little hierarchy of vascular
structures is observed, with abrupt changes in diameter and blind-ending vessels, particularly
within the centers of tumours; and few structurally complete arteries or veins are found with
sinusoidal capillary plexuses prevailing; the remodeling of the vasculature seen in inflammation
or wound healing is largely missing; (b) poorly formed fragile vessels with high permeability to
macromolecules because of the presence of large endothelial cell gaps or fenestrae, incomplete
basement membrane, and relative lack of pericytes or smooth muscle association with
endothelial cells; (c) arteriovenous shunting, high vascular tortuosity, and vasodilatation; (d)
intermittent or unstable blood flow (with acutely collapsing vessels and areas of spontaneous
hemorrhage; and (e) extreme heterogeneity of vascular density, with areas of low vascular
density mixed with regions of high angiogenic activity. These features are distinct from the
organized regular structure and normal blood flow seen in mature vessels. Angiogenic vessels
are also leaky, a feature that aids extracellular matrix signaling and metabolism, as well as
contributing to tumour cell invasion and metastasis (10). These tumour-induced vascular and
structural abnormalities result in functional impairments that are important to dynamic
contrast-enhanced MR imaging observations, including the following:
1. The interstitial pressure is increased because of an increased vascular permeability and
poor lymphatic drainage. As a result, the interstitial space is enlarged (by as much as five
times), allowing low-molecular weight contrast agents to accumulate. The higher interstitial
pressure also leads to compression of vessels and thus increased vascular resistance and
regional areas of acute perfusion-related hypoxia.
2. The transcapillary permeability increases, allowing a more rapid exchange of low-
molecular-weight contrast agents. As a consequence, contrast agents are more easily able to
access the interstitial extracellular space and flow out when plasma levels drop. This can be
observed as an increase in MR signal intensity followed by a subsequent decrease.
36
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
3. The total vascular cross-sectional area may increase and can be combined with arterio-
venous shunts. This gives rise to increased blood flow overall. The global increase in flow in
cancers causes the bolus of contrast agent to arrive just a little earlier than it does in
surrounding normal tissue. In the prostate, differences in arrival time between normal and
abnormal tissue are short (differences of only 1 second have been observed). It is important
to remember that all of these functional changes do not necessarily occur homogeneously
throughout the tumour but most often are heterogeneously distributed, and they need not
coincide spatially. Thus, areas of increased interstitial volume may occur separately (at
different locations) from areas of increased permeability.
Fast T1-weighted dynamic contrast-enhanced MR imaging for monitoring the uptake of an
intravascular contrast agent has proved itself to be a powerful technique for studying the
characteristics of the microvasculature of prostate tumours and normal prostatic tissues. The
essence of fast prostate T1- weighted dynamic contrast-enhanced MR imaging lies in the
differences in microvascular characteristics that have been observed between normal and
malignant prostatic tissues. Differences in the enhancement pattern observed in the prostate are
due to three physiologic processes in the microvasculature:
a) perfusion, or blood flow; the higher the perfusion, the quicker the contrast agent will be
available for diffusion into the extravascular extracellular space;
b) capillary permeability; the higher the permeability and the greater the microvessel
surface area, the faster the transfer of contrast agent to the extravascular extracellular
space and the greater the rate of T1-weighted enhancement; and
c) cellular density; the higher the cellular density outside the vasculature, the less free
interstitial fluid is available for relaxivity changes induced by the gadolinium-based
contrast agent (i.e., reduced extravascular extracellular space).
37
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
Permeability, or leakiness, of capillaries refers to the ability of molecules to pass through
interendothelial fenestrae and junctions into the interstitial compartment. Note that most
normal tissues are leaky to micromolecules (the exception being the brain because of the blood-
brain barrier), but macromolecular permeability is specific for tumours; that is, high
permeability of the vasculature is a characteristic of pathologic blood vessels in inflamed tissues
and tumours. It is because both benign and malignant tissues are leaky to low-molecular-weight
contrast agents that simple pre- and post-contrast images are usually ineffective in detecting the
intraprostatic location of prostate cancer; only minimal differences between benign tissue and
prostate cancer are seen unlike the case in the brain, which, as stated previously, has an
intrinsic low vascular permeability. Imaging performed for a few minutes after administration of
contrast agent has been described as a way to detect breast lesions (19); however, in the
prostate, nearly all tissues tend to enhance similarly on these images (20). It is for these reasons
that dynamic sequences acquired at high temporal resolution by exploiting differences in
perfusion are currently the only way of differentiating prostatic tissues.
Principals underlying DCE-MRI
Dynamic contrast-enhanced MR imaging with the routinely available low-molecular-weight
gadolinium chelates enables noninvasive imaging of tissue functional vascular features. The
three essential aspects of dynamic contrast-enhanced MR imaging include:
a) Fast dynamic imaging, referring to the temporal (time) component in imaging; complete
coverage of the anatomic area with a fast T1-weighted sequence is required before and
after the bolus injection of a lowmolecular-weight contrast agent;
b) Contrast agent administration, that is, intravenous administration of a low-molecular-
weight, usually gadolinium-based contrast agent; increases in signal intensity are seen
on the dynamically acquired T1-weighted MR images; and
38
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
c) Quantification of signal intensity changes, that is, semiquantitative and quantitative
estimation of signal intensity changes to determine the kinetic parameters of the
contrast agent.
Depending on the technique used, data can be obtained reflecting the tissue perfusion (blood
flow, blood volume, and mean transit time), the microvessel permeability surface area product,
and the extracellular leakage space. Insights into these physiologic processes can be obtained by
the evaluation of kinetic enhancement curves or by the application of complex compartmental
modeling techniques. In addition to the signal intensity increases observed with T1-weighted
MR sequences, it is possible to observe the effects of the contrast agent while still confined to the
early vascular phase. While in the vascular space, concentrated contrast agent produces focal
magnetic field inhomogeneities that result in a decrease in the signal intensity of the
surrounding tissues (T2* effect). Thus, MR sequences can be designed to be:
a) Sensitive to the vascular phase of contrast agent delivery (the so-called T2*-weighted or
susceptibility-based methods), which reflect tissue perfusion and blood volume; or
b) Sensitive to the presence of contrast agent in the extravascular space (also termed T1-
weighted or relaxivity-based methods) and reflecting the perfused microvessel area and
permeability, as well as the extravascular extracellular leakage space.
The choice of the dynamic contrast-enhanced MR imaging sequences and parameters to be used
will depend on the required anatomic coverage, the acquisition times, the susceptibility to
artifacts resulting from magnetic field variations, and the need for quantification (10).
Analysis of the tissue signal intensity or the uptake of gadolinium-based contrast agent can be
done semiquantitatively (eg, with the onset time, the maximum enhancement, or the time to
peak) or with more complicated but quantitative pharmacokinetic modeling approaches. The
latter methods quantify enhancement with parameters like the transfer constant (Ktrans), the
volume of interstitial extravascular extracellular space (Ve), and the rate constant (kep) (15). The
quantification of kinetic parameters has the advantages of being biologically meaningful, helping
39
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
to establish objective criteria for classifying tissues, and being able to be used to objectively
assess the response to therapy (9,16).
A relationship exists between the uptake rate for gadolinium-based contrast agent and the
surface area of perfused microvessels. Histopathologic examination can only show microvessel
density and does not provide information with regard to the functionality (perfusion) of the
microvessels. It is important to note that implanted tumour xenograft data show that there is a
discrepancy between perfused and visible microvessels at histologic examination. The perfusion
of microvessels shows a variation from 20% to 85% at any given time (17,18). Dynamic MR
imaging can therefore provide additional information on tumour neovascularity as well as the
perfused fraction of vessels. Two aspects of dynamic MR imaging are of extra importance:
contrast agents and microvasculature of the prostate. These two will be discussed in the
following sections.
Contrast Agents
A number of different groups of contrast agents could be used for assessment of the angiogenic
status in tumours. These groups include (a) low-molecularweight agents (<1000 Da) that rapidly
diffuse into the extracellular fluid space (extracellular fluid agents), such as gadoterate
meglumine and gadopentetate dimeglumine; (b) intermediate-molecular- weight agents; (c)
high-molecular-weight agents (>30 000 Da) designed for prolonged intravascular retention
(macromolecular contrast agents or blood pool agents), such as gadofosveset trisodium, which
itself is of low molecular weight but binds rapidly to plasma albumin and so effectively behaves
like a macromolecular contrast agent; however, there is a small fraction that remains unbound,
particularly in the first 1 minute after contrast agent administration; and (d) agents intended to
accumulate at sites of concentrated angiogenesis nanoparticulate gadoliniumcontaining
liposomes. In the United States, for dynamic contrast-enhanced MR imaging, only low-
molecular-weight gadolinium chelate contrast agents are currently approved. They shorten the
longitudinal (spin lattice) T1 relaxation of protons, resulting in increased signal intensity on T1-
weighted MR images. The increase in signal intensity is dependent on the native T1 relaxation of
tissue, the dose of the contrast agent, the imaging sequence and parameters used, and the gain
and scaling factors of the MR imaging equipment. These agents are unable to cross cell
40
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
membranes and thus will stay in the intravascular extracellular space (blood plasma) or the
extravascular extracellular space (interstitial fluid space). Note that although gadolinium
chelates affect protons in their immediate vicinity, proton diffusion occurs sufficiently quickly
for their sphere of influence to extend to the intracellular compartment. Thus, although
gadolinium chelates cannot enter intact cells, they can and do affect the proton relaxation in
cells. In Europe, a wider range of agents has recently become available: superparamagnetic iron
oxide agents like ferumoxides, which might be used in dynamic susceptibility-weighted MR
imaging, as well as the first clinically available blood pool contrast agent, gadofosveset
trisodium. The exact role of these contrast agents in oncologic imaging still needs to be defined.
Figure 3 shows a work-flow diagram for the technique of DCE-MR imaging.
Figure 3. Work-flow diagram to show the technique of DCE-MR imaging, from intravenous
(IV) administration of contrast agent to the generation of colored images.
41
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
Contrast Agent Administration
For optimal qualitative and quantitative estimation of dynamic contrast agent related changes
in prostatic tissue, controlled administration of a bolus of contrast agent into a peripheral vein is
required. Manual administration can result in distorted enhancement characteristics. To
minimize this problem, automatic power injectors should be used with fixed administration
rates (usually 2.5 mL/sec although a higher rate of. 4-5 ml/sec seems more advantageous). After
injection of the bolus of gadolinium-based contrast agent, a normal saline flush is also needed to
clear the line and to chase the injected bolus of contrast agent into the central circulation.
Dynamic Sequences
T1-weighted sequences. The T1-weighted signal intensity increase in tissue (Fig. 4) is
dependent on the baseline T1 value. In general, quantification is improved by estimating
changes in the T1 relaxation rate at each time point during the dynamic acquisition. T1-weighted
sequences, usually of gradient-echo or saturation-recovery/inversion-recovery snapshot types,
are used for data acquisition. High spatial resolution to cover the whole prostate can only be
achieved by compromising the temporal resolution and vice versa.
42
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
Figure 4. Graphs of signal intensity versus time for a T1-weighted dynamic contrast-
enhanced MR imaging acquisition. Different semiquantitative parameters are calculated
from the graph after curve-fitting algorithms have been applied.
As a result, two types of schemes having different temporal resolutions are used when
performing dynamic contrast-enhanced MR imaging of the prostate: a) slow sequences
(temporal resolution, approximately 30 seconds) with high spatial resolution; these in general
have high sensitivity and low specificity; and b) Fast sequences (imaging techniques with
temporal resolution of 1 4 seconds) with lower spatial resolution; these have low sensitivity
and high specificity.
The optimal temporal resolution and spatial resolution still need to be established to achieve the
highest sensitivity and specificity, and this will depend on the clinical question. To date, most
researchers have used strategies of high temporal resolution, but it seems that cancer might be
accurately depicted, at least in the peripheral zone, by using slower sequences (21). The great
advantage of higher temporal resolution, compared with low temporal resolution, is the ability
to accurately quantify enhancement parameters and gain valuable pharmacokinetic information.
Although most studies emphasize high temporal resolution at the expense of spatial resolution,
lower spatial resolution may not depict critical features needed for optimal staging (e.g., minimal
capsular penetration). Despite this, studies with high temporal resolution have shown that
43
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
dynamic contrast-enhanced MR imaging can improve the staging capabilities of less-experienced
radiologists (22).
Figure 5. Graphs of signal intensity versus time showing the difference between fast (left)
and slow (right) acquisition methods.
Data Processing
T1-weighted sequence data. From the raw data acquired with the T1-weighted sequence, a
pixel-by pixel analysis of signal intensity changes is made. Signal enhancement seen on T1-
weighted dynamic contrast-enhanced MR images can be assessed in two ways:
a) Semiquantitative analysis of signal intensity changes and
b) Quantitative analysis of contrast agent concentration (change in relaxivity) by using
pharmacokinetic modeling techniques.
Semiquantitative parameters describe signal intensity changes by using a number of descriptors.
These parameters include curve shape, onset time (t 0 = time from injection or appearance in an
44
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
artery to the arrival of contrast agent in the tissue of interest), gradient of the slope of
enhancement curves, maximum signal intensity, area under the signal intensity curve at a fixed
time point (usually 60 90 seconds after onset time), and washout gradient (late washout). These
parameters have the advantage of being relatively straightforward for calculation, but they are
limited by the fact that they are not biologically meaningful, may not accurately reflect contrast
agent concentration in tissues, and can be influenced by the imaging equipment s settings
(including gain and scaling factors). These factors limit the usefulness of semiquantitative
parameters and make between-patient and between-system comparisons difficult.
Quantitative techniques use pharmacokinetic modeling, which is usually applied to changes in
the contrast agent concentrations in tissue. Signal intensity changes observed during dynamic
acquisition are used to estimate contrast agent concentration in vivo (23). Concentration-time
curves are then mathematically fitted by using one of a number of recognized pharmacokinetic
models, and quantitative kinetic parameters are derived. Examples of modeling parameters
include the volume transfer constant of the contrast agent (Ktrans [formally called the
permeability surface area product per unit volume of tissue], measured in units per minute), the
interstitial fluid space as a percentage of unit volume of tissue (Ve), and the rate constant (kep,
measured in units per minute). These standard parameters are related mathematically (24): kep
= Ktrans/Ve (1). Quantitative parameters are more complicated to derive than those derived
semiquantitatively, which deters their use. However, commercially available software is
beginning to appear, and if contrast agent concentration can be measured accurately and if the
type, volume, and method of administration of contrast agent are consistent, then it is possible
to directly compare pharmacokinetic parameters acquired serially in a given patient and in
different patients imaged at the same or different imaging sites (25). Uncertainties exist with
regard to the reliability of kinetic parameter estimates derived from the application of contrast
agent kinetic models to T1-weighted dynamic contrast-enhanced MR imaging data. These
uncertainties derive from assumptions implicit in kinetic models and those assumptions made
for the measurement of the contrast agent concentration in tissue. The vascular input function
used in the calculations also affects the reliability of the data obtained; robust methods for
measuring arterial input function for routine dynamic contrast-enhanced MR imaging studies
are currently emerging but are still not widely available (26 28).
45
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
Figure 6. Body compartments accessed by low-molecular-weight contrast agents. IV =
intravenous.
Quantitative Dynamic Contrast-enhanced Parameters
1. Extravascular Extracellular Space Volume (Ve)
The volume of extravascular extracellular space (Ve) is defined as:
where [Cgd]plateau_prostate is the prostate gadolinium concentration at plateau of peak
enhancement (i.e., the signal amplitude at which the exponential curve levels off), and
[Cgd]plateau_ref_tissue is the gadolinium concentration at plateau of peak enhancement in the
reference tissue used for calibration purposes. Ve refers to the space into which gadolinium
can leak from a capillary and has the benefit of specifically excluding the vascular space.
There may be regions (such as fibrous tissue) that are in the extravascular extracellular space
and yet are inaccessible to gadolinium-based contrast agents. Alternatives terms would
therefore be leakage space or distribution space. This is a theoretical parameter, though; and
in practice, in leaky tumours the contribution of plasma contrast agent and interstitial
46
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
contrast agent cannot be discriminated. Thus, Ve in practice measures the total extravascular
extracellular volume and therefore, 1 - Ve represents the cellular fraction.
2. Rate Constant (kep)
The rate constant (kep) is defined as:
where ttpprostate is the time to peak enhancement in the prostate, and ttpref_tissue is the time to
peak enhancement in the reference tissue. The rate constant kep is formally the diffusion rate
constant between the extravascular extracellular space and blood plasma. Both the volume
transfer constant and the rate constant have the same units (units per minute). kep Is always
greater than the transfer constant Ktrans. For a range of typical extravascular extracellular
space fractional volumes seen in tumours (Ve = 20% 50%), kep is two to five times higher
than Ktrans. The kep is the exponential decay constant for tissue concentration that would result
if the arterial concentration could be (a) instantaneously raised from zero to a constant value
or (b) dropped to zero. The kep is also the mean residence time for contrast agent in the
extravascular extracellular space after a bolus arterial input (24).
3. Volume Transfer Constant (Ktrans)
The volume transfer constant Ktrans is defined as follows:
47
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
Ktrans has several physiologic interpretations, depending on the balance between capillary
permeability and blood flow in the tissue of interest. In high-permeability situations, where
diffusion through the interendothelial fenestrae is limited by flow, Ktrans is equal to the blood
plasma flow per unit volume of tissue. In the other limiting case of low permeability, where
contrast agent diffusion is limited by permeability, Ktrans is equal to the permeability surface
area product of the capillary vessel walls, per unit volume of tissue (24).
Limitations of the DCE-MERI technique
It should be evident that dynamic contrast-enhanced MR imaging combined with high-spatial
resolution T2-weighted imaging and Diffusion weighted imaging will remain the mainstay of
prostate cancer MR imaging for the foreseeable future. However, the limitations of dynamic
contrast-enhanced MR imaging should be borne in mind. The transition zone, often replaced by
benign prostatic hyperplasia, can be highly vascularized and show rapid and high levels of
enhancement. As noted previously, discriminating normal transition zone and benign prostatic
hyperplasia from tumours within the same region is often challenging. Pathologic but
nonmalignant lesions within the prostate can often also mimic tumour on dynamic contrast-
enhanced MR images. The most common of these lesions are high-grade prostatic intraepithelial
neoplasia and prostatitis; the underlying reasons for the overlap with tumour lies in the fact that
these lesions also incite angiogenic responses in tissues. Administration of a contrast agent is an
invasive procedure with additional costs and potential side effects. For quantitative dynamic
contrast-enhanced MR imaging to be widely applied in clinical practice, it is necessary to
develop standardized robust analytic approaches for the measurement of enhancement. This
includes the need for commercial equipment manufacturers to provide robust methods for
rapidly measuring time-varying change in T1 relaxation rates, incorporation of arterial input
function into kinetic modeling processes (or other reliable methods that substitute for arterial
input function measurement), and robust analytic software that allows input from the different
MR imagers (17). Finally, interpretation requires a certain level of experience because no
quantitative parameter is able to be used to reliably separate tumour from benign tissues. In
conclusion, dynamic contrast-enhanced MR imaging has established itself as a valuable imaging
tool with a wide variety of applications for patients with prostate cancer.
48
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
Figure 7. Dynamic contrast-enhanced MR imaging in localization of prostate cancer. (a)
Histologic determination of tumour areas. (b) T2-weighted MR image. Arrows indicate
tumour. (c e) Semiquantitative parameters. (c) Wash-in rate. (d) Late washout. (e)
Relative enhancement. Quantitative parameters: (f-h). (f) Rate constant (kep). (g) Leakage
space (Ve). (h) Volume transfer constant (Ktrans). (i) Graph of signal intensity versus time
shows the difference between enhancement characteristics of tumour and normal
peripheral zone (PZ).
49
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
B. DIFFUSION WEIGHTED IMAGING (DWI)
Pathophysiological basis and the role of DWI in depicting prostatic tissue
Water molecules exhibit random motion in tissue, related to temperature (Brownian effect)(29).
The intra- and extracellular movement of molecules in tissue is largely restricted by membranes
forming barriers to diffusion., The more barriers water molecules meet in a certain time interval,
the smaller the mean movement (diffusion) distance (32). The degree of restriction to water
diffusion in biological tissue is inversely correlated to tissue cellularity and the integrity of cell
membranes. Free motion of water molecules is more restricted in tissues with a high cellular
density. DWI can quantify this water motion in an indirect manner (30,31). The DWI pulse
sequence labels hydrogen nuclei in space, of which most is water molecules at any moment, and
determines the length of the path that water molecules travel over a short period of time
(labeling time in the order of 50 ms). DWI estimates the mean distance traveled by all hydrogen
nuclei in every voxel of imaged tissue. The greater this mean distance the higher the apparent
mobility of the water molecules in the tissue. In the clinical setting, diffusion-weighted
sequences are sensitized to detect diffusion distances ranging from 1 to 20 m predominantly
measuring microcapillary water movement (5% of total volume of voxel), intracellular and
extracellular space diffusion. From the DWI images quantitative values can be calculated, called
the apparent diffusion coefficients (ADC) with high values indicating free water movement and
low ADC values indicating restrictions to free movement.
DWI was initially used for the early detection of cerebral ischemia (36). The evolution of DWI
characteristics in cerebral ischemia over time has classically been attributed to the extracellular
to intracellular distribution of hydrogen nuclei caused by different types of edema (37). It has
been postulated that extracellular water molecules have a much higher range of mobility,
because they are not bound within membranes or by other cellular structures (38,39). When
this is translated to prostate tissue, which is predominantly glandular tissue, the predominant
contribution of the extracellular component is from tubular structures and their fluid content,
whereas the intracellular component is determined by the epithelial and stromal cells.
50
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
A prerequisite for the correct interpretation of diffusion and ADC images relies on good
knowledge of the diffusion characteristics of the different anatomic zones of the prostate and of
benign prostatic conditions compared with prostate cancer (40). The normal prostatic gland is
rich in tubular structures. This allows for abundant self-diffusion of water molecules within
these structure and provides high ADC values. In most cases, the peripheral zone can be easily
discriminated from the transition zone on DWI, because it displays relatively higher ADC values
(41-43). The exact background of this phenomenon remains unclear, because the exact ratio of
extracellular to intracellular components for the different anatomic zones of the prostate has not
yet been described. Moreover, exchange of water over membranes can obscure a fully
compartmentalized interpretation of the diffusion characteristics. The transition zone by
microscopic observation consists of more compact smooth muscle and sparser glandular
elements than the peripheral zone, leading to a lower extracellular to intracellular fluid ratio
(44). Furthermore, an age-related increase of T2 signal intensity of the peripheral zone
compared with the transition zone has also been demonstrated (45) and an age-related increase
in ADC values in both transition zone and peripheral zone has been seen (46), which are most
likely caused by atrophy in the prostate leading to reduced cell volume and enlarged glandular
ducts. Benign prostatic hyperplasia (BPH) gives rise to nodular adenomas in the transition zone
and with time these compress the central zone to form a pseudocapsule, consequently occupying
the complete transition zone. The peripheral zone is usually not affected by BPH and retains its
own histologic characteristics. BPH is defined by hyperplasia of all cells that constitute the
transition zone, with glandular, muscular, and fibrous compartments involved in various
degrees within a patient and between patients. This nodular hyperplasia gives rise to
inhomogeneous diffusion patterns and because tubular structures often remain in place, the
increased cellular density of hyperplasia, which is far less predominant than in prostate
carcinoma, might explain the observed reduction in ADC levels of the transition zone on DWI.
However since BPH has inhomogeneous diffusion characteristics, not only reduction in ADC but
also increases in ADCs have also been described (46).
Prostatitis almost uniquely originates in the peripheral zone. With respect to MR imaging,
chronic prostatitis is of far more importance than the acute prostatitis counterpart. Chronic
prostatitis is asymptomatic in many cases and symptoms may mimic BPH. Furthermore, both
are often associated with elevated prostate-specific antigen levels, raising the suspicion of
51
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
prostate cancer. Histologically, chronic prostatitis is characterized by extracellular edema
surrounding the involved prostatic cells with concomitant aggregation of lymphocytes, plasma
cells, macrophages, and neutrophils in the prostatic stroma. This abundance in cells as compared
with normal prostatic tissue may lead to an ADC decrease because of increased cellular density
and therefore restriction free water motion
on the DWI characteristics of chronic prostatitis.
Prostate carcinoma is histologically characterized by a higher cellular density than normal
prostate tissue, with replacement of the normal glandular tissue. This leads to a decrease in ADC
values, compared with normal prostate gland (Fig. 1) (40,47). Concomitantly with destruction of
tubular structures in prostate carcinoma, fractional anisotropy is also reduced (48,49).
Interestingly, whereas well-differentiated prostate carcinomas display some tubular formation,
with worsening differentiation the tubular structures become less predominant, and the cellular
component of the cancer increases.
Figure 8. Schematic presentation of the increased diffusivity of molecules in low-cellular
tissue (left) and severe restriction in highly cellular tissue (right).
52
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
Figure 9. The left shows a histological slide of the glandular composition of normal
peripheral zone tissue with high diffusivity. The histological images on the right
represent a highly cellular Gleason grade 5 prostate adenocarcinoma.
Principals underlying DWI
The sensitivity of the DWI sequence to water motion is introduced by diffusion sensitizing
gradients in which a certain combination of amplitude, duration, and spacing in time is
expressed in a b value. The relationship between signal intensity and b value encompasses a
continuous spectrum ranging from fast signal decay due to flowing water molecules in
microcappillaries, intermediate signal decay due to freely diffusing water down to slow signal
decay due to many restrictions. The number of b-values and the signal-to-noise of the
measurements define whether it is feasible to fit anything more than a mono-exponential decay
(50) curve to this data. The slope of the decay curve at low b-values quantifies a fast apparent
diffusion coefficient (ADCfast) reflecting distances traveled by protons in microcapillaries. At
higher b-values, the slope of the signal decay curve quantifies the slow component of the
apparent diffusion coefficient (ADCslow), reflecting distances traveled by protons in the 1 10 m
range in the extracellular space. In theory, very high b-values can be used to interrogate the
short diffusion distances traveled by intracellular protons as they encounter intracellular
membranes, but in practice the low signal-to-noise ratio (SNR) from these very high b-value
images makes the data unreliable (51).
53
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
Figure 10. (a) Graph illustrating the signal intensity versus b-values at diffusion-weighted
imaging (DWI) of a model of two compartments: tissue with normal versus restricted
diffusion. (b) Graph illustrates the logarithm of signal intensity versus b values at
diffusion-weighted imaging of normal peripheral zone (PZ) prostate tissue versus
prostate tumour. The signal of water molecules decays exponentially with increasing b-
values for different tissue types. The decay in signal is reduced in tissues with restricted
diffusion (e.g., tumour). The ADC represents the slope (gradient) of the plotted lines
(logarithmic conversion of the exponential decay). The greater the number of b- values
used in the analysis, the more accurate the ADC calculation.
In a large volume of pure water, self-diffusion is equal in all directions, hence isotropic, and not
restricted by any barrier. In organized tissue water mobility can have a preferred direction: if
water molecules experience less restrictions in one dimension their mobility can appear
anisotropic. The fractional anisotropy is determined along the axis of the tubular structures of
normal prostate tissue, and can potentially be used for tissue characterization.. Because
diffusion in tissue is limited by cellular structures, to establish a reliable estimate of this mean
distance traveled by hydrogen nuclei, DWI is acquired in at least three different orthogonal
directions for each b-value (32,33). In linearly aligned tissue this anisotropy is more pronounced
because there is one direction that contributes most to the DWI. Diffusion tensor imaging is a
specific technique that quantifies the level of anisotropy in tissue, expressed in a fractional
anisotropy value. This is low in imaged tissue without substantial anisotropy and is higher in
54
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
imaged tissue in which the larger part of diffusion takes place in one direction (33,34). Diffusion
tensor imaging can be used in addition to DWI to determine the structural organization of tissue
along which diffusion takes place.
Images from DWI typically have both T2-weighted and diffusion-weighted characteristics. The
intensity of the signal on the diffusion-weighted image represents a combination of signal from
the inherent T2 relaxation of the tissue as well as the dephasing caused by water motion in the
presence of the diffusion gradients. At low b-values there is greater contribution from the T2-
weighted signal, and at higher b-values, contrast is determined more by the relative diffusion of
molecules. When a high b-value diffusion weighted image has high signal intensities, this can be
due to two phenomena: a) the brightness (signal intensity) is due to an inherent long T2
relaxation of the tissue, referred to as the - or; b) the tissue of interest
portrays clear restriction in the Brownian proton movement due to increased cellularity,
macromolecules etc. Therefore ADC maps should also be obtained in every instance to
differentiate these two effects. The current guidelines advocated at least three different b-values
to obtain accurate ADC estimates using a low b-value, between 50-100 s/mm2, and two higher b-
values around 400-500 and 800-1000 s/mm2. Because vascular microperfusion can contaminate
the signal attenuation in DWI acquisition, it is essential not to include b-values < 50 s/mm2,
except when more complex bi-exponential fitting of the signal data is performed. To minimize
the influence of bulk motion as a distorting factor and minimizing T2 shine-through, typically a
TE as short as possible is chosen in addition to performing parallel imaging acquisition
techniques.
Limitations of Diffusion-Weighted MR Imaging
One of the main drawbacks of DWI of the prostate is its suboptimal spatial resolution, even with
currently widely available 3-T MR imaging systems, combining pelvic phased array surface coil
in combination with an endorectal coil for signal reception. The authors
improved spatial resolution with the use of DWI at 3 T improves zonal and tumour delineation
and allows improved ability to compare ADC mapping with whole-mount sectioned
prostatectomy specimens for research purposes. It has been shown that use of an endorectal coil
significantly improves imaging quality in T2-weighted imaging. Rectal gas in the absence of an
endorectal coil may lead to susceptibility artifacts (46). The endorectal coil enables better
55
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
staging performance and improves sensitivity for the localization of prostate carcinoma with
conventional MR imaging (52, 53). In the experience, the use of an endorectal coil in
conjunction with surface coils and parallel imaging improves image quality of DWI. This may
result in improved overall performance of DWI in the localization, characterization, and
delineation of prostate carcinoma. A further drawback of DWI is that it is very susceptible to
motion artifact resulting in distorted inaccurate ADC calculation. To some degree this can be
overcome by using a combination of surface and endorectal coil, which facilitate shortened
imaging time and allow using a lower echo time (TE).
Figure 11. A 68-year-old man with prostate cancer of the right peripheral zone. (A) Axial
T2-weighted MR image shows a low signal intensity area in the right peripheral zone.
Color parametric maps were calculated (B) and demonstrated increased washout in the
right peripheral zone, (C and D) increased Ktrans and kep. (E) ADC map at the same level
as in image A shows reduced ADC compared with the normal peripheral zone. (F)
Histopathology confirmed these findings and showed a tumour with Gleason Score of
4+3=7.
56
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
REFERENCES
1. Westbrook C. MRI in Practice. 4ed. John Wiley and Sons; 2011.
2. Conway EM, Collen D, Carmeliet P. Molecular mechanisms of blood vessel growth. Cardiovasc Res 2001;49(3):507 521.
3. Folkman J. Angiogenesis in cancer, vascular, rheumatoid and other disease. Nat Med 1995;1(1):27 31.
4. Carmeliet P, Jain RK. Angiogenesis in cancer and other diseases. Nature 2000;407:249 257.
5. Folkman J. New perspectives in clinical oncology from angiogenesis research. Eur J Cancer 1996;32A(14):25342539.
6. Harris AL. Hypoxia: a key regulatory factor in tumour growth. Nat Rev Cancer 2002;2:38 47. 7. Charlesworth PJ, Harris AL. Mechanisms of disease: angiogenesis in urologic malignancies. Nat Clin Pract Urol
2006;3(3):157 169.
8. Borre M, Offersen BV, Nerstrom B, Overgaard J. Microvessel density predicts survival in prostate cancer patients subjected to watchful waiting. Br J Cancer 1998;78:940 944.
9. Bono AV, Celato N, Cova V, Salvadore M, Chinetti S, Novario R. Microvessel density in prostate carcinoma. Prostate Cancer Prostatic Dis 2002;5(2):123 127.
10. Padhani AR, Harvey CJ, Cosgrove DO. Angiogenesis imaging in the management of prostate cancer. Nat Clin Pract Urol 2005;2(12):596 607.
11. Jackson MW, Bentel JM, Tilley WD. Vascular endothelial growth factor (VEGF) expression in prostate cancer and benign prostatic hyperplasia. J Urol 1997;157:2323 2328.
12. Jain RK, Safabakhsh N, Sckell A, et al. Endothelial cell death, angiogenesis, and microvascular function after castration in an androgen-dependent tumour: role of vascular endothelial growth factor. Proc Natl Acad Sci U S A 1998;95(18):10820 10825.
13. Borre M, Nerstrom B, Overgaard J. Association between immunohistochemical expression of vascular endothelial growthfactor (VEGF), VEGF-expressing neuroendocrine-differentiated tumour cells, and outcome in prostate cancer patients subjected to watchful waiting. Clin Cancer Res 2000;6:1882 1890.
14. Du Z, Fujiyama C, Chen Y, Masaki Z. Expression of hypoxiainducible factor 1alpha in human normal, benign, and malignant prostate tissue. Chin Med J (Engl) 2003;116(2):1936 1939.
15. Leach MO, Brindle KM, Evelhoch JL, et al. The assessment of antiangiogenic and antivascular therapies in early-stage clinical trials using magnetic resonance imaging: issues and recommendations. Br J Cancer 2005;92:15991610.
16. van der Sanden BP, Rozijn TH, Rijken PF, et al. Noninvasive assessment of the functional neovasculature in 9L-glioma growing in rat brain by dynamic 1H magnetic resonance imaging of gadolinium uptake. J Cereb Blood Flow Metab 2000;20(5):861 870.
17. Collins DJ, Padhani AR. Dynamic magnetic resonance imaging of tumour perfusion. IEEE Eng Med Biol Mag 2004;23(5):65 83.
18. Endrich B, Vaupel P. The role of microcirculation in the treatment of malignant tumours: facts and fiction. Blood Perfusion Microenviron Hum Tumours 1998;3:19 39.
19. Boetes C, Barentsz JO, Mus RD, et al. MR characterization of suspicious breast lesions with a gadolinium-enhanced TurboFLASH subtraction technique. Radiology 1994;193(3):777 781.
20. Huisman HJ, Engelbrecht MR, Barentsz JO. Accurate estimation of pharmacokinetic contrast-enhanced dynamic MRI parameters of the prostate. J Magn Reson Imaging 2001;13(4):607 614.
21. Rouviere O, Valette O, Grivolat S, et al. Recurrent prostate cancer after external beam radiotherapy: value of contrast-enhanced dynamic MRI in localizing intraprostatic tumour correlation with biopsy findings. Urology 2004;63(5):922 927.
22. Fütterer JJ, Engelbrecht MR, Huisman HJ, et al. Staging prostate cancer with dynamic contrast-enhanced endorectal MR imaging prior to radical prostatectomy: experienced versusess experienced readers. Radiology 2005;237(3):541 549.
23. Parker GJ, Suckling J, Tanner SF, et al. Probing tumour microvascularity by measurement, analysis and display of contrast agent uptake kinetics. J Magn Reson Imaging 1997;7:564 574.
57
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
24. Tofts PS, Brix G, Buckley DL, et al. Estimating kinetic parameters from dynamic contrast-enhanced T(1)-weighted MRI of a diffusable tracer: standardized quantities and symbols. J Magn Reson Imaging 1999;10(3):223 232.
25. Padhani AR, Leach MO. Antivascular cancer treatments: functional assessments by dynamic contrast-enhanced magnetic resonance imaging. Abdom Imaging 2005;30:324 341.
26. Rijpkema M, Kaanders JH, Joosten FB, van der Kogel AJ,Heerschap A. Method for quantitative mapping of dynamic MRI contrast agent uptake in human tumors. J Magn Reson Imaging 2001;14:457 463.
27. Port RE, Knopp MV, Brix G. Dynamic contrast-enhanced MRI using Gd-DTPA: interindividual variability of the arterial input function and consequences for the assessment of kinetics in tumors. Magn Reson Med 2001;45:1030 1038.
28. Hara N, Okuizumi M, Koike H, Kawaguchi M, Bilim V. Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) is a useful modality for the precise detection and staging of early prostate cancer. Prostate 2005;62(2):140 147.
29. Crank J. The mathematics of diffusion. New York: Oxford University Press; 1956.
30. Stejskal EO, Tanner JE. Spin diffusion measurements: spin echoes in the presence of a time-dependentfieldgradient. J Chem Phys 1965;42:288 92.
31. Basser PJ, Mattiello J, LeBihan D. Estimation of the effective self-diffusion tensor from the NMR spin echo. J Magn Reson 1994;103:247 54.
32. Bammer R, Skare S, Newbould R, et al. Foundations of advanced magnetic resonance imaging. NeuroRx 2005;2:167 95.
33. Basser PJ. Inferring microstructural features and the physiological state of tissues from diffusionweighted images. NMR Biomed 1995;8:333 44.
34. Westin CF, Maier SE, Mamata H, et al. Processing and visualization for diffusion tensor MRI. Med Image Anal 2002;6:93 108.
35. Bammer R. Basic principles of diffusion-weighted imaging. Eur J Radiol 2003;45:169 84.
36. Schaefer PW, Copen WA, Lev MH, et al. Diffusionweighted imaging in acute stroke. Magn Reson Imaging Clin N Am 2006;14:141 68.
37. Moseley ME, Butts K, Yenari MA, et al. Clinical aspects of DWI. NMR Biomed 1995;8:387 96.
38. Moseley ME, Kucharczyk J, Mintorovitch J, et al. Diffusion- weighted MR imaging of acute stroke: correlation with T2-weighted imaging and magnetic susceptibility-enhanced MR imaging in cats. AJNR Am J Neuroradiol 1990;11:423 9.
39. Lansberg MG, Norbash AM, Marks MP, et al. Advantages of adding diffusion-weighted magnetic resonance imaging to conventional magnetic resonance imaging for evaluating acute stroke. Arch Neurol 2000;57:1311 6.
40. Anderson AW, Xie J, Pizzonia J, et al. Effects of cell volume fraction changes on apparent diffusion in human cells. Magn Reson Imaging 2000;18:689 95.
41. Kumar V, Jagannathan NR, Kumar R, et al. Apparent diffusion coefficient of the prostate in men prior to biopsy: determination of a cut-off value to predict malignancy of the peripheral zone. NMR Biomed 2007;20:505 11.
42. Kim CK, Park BK, Lee HM, et al. Value of diffusionweighted imaging for the prediction of prostate cancer location at 3T using a phased-array coil: preliminary results. Invest Radiol 2007;42:842 7.
43. Tamada T, Sone T, Toshimutsu S, et al. Age-related and zonal anatomical changes of apparent diffusion coefficient values in normal human prostatic tissues. J Magn Reson Imaging 2008;27:552 6.
44. Hricak H, Dooms GC, McNeal JE, et al. MR imaging of the prostate gland: normal anatomy. AJR Am J Roentgenol 1987;148:51 8.
45. Allen KS, Kressel HY, Arger PH, et al. Age-related changes of the prostate: evaluation by MR imaging. AJR Am J Roentgenol 1989;152:77 81.
46. Ren J, Huan Y, Wang H, et al. Diffusion-weighted imaging in normal prostate and differential diagnosis of prostate diseases. Abdom Imaging 2008.
47. Song SK, Qu Z, Garabedian EM, et al. Improved magnetic resonance imaging detection of prostate cancer in a transgenic mouse model. Cancer Res 2002;62:1555 8.
48. Manenti G, Carlani M, Mancino S, et al. Diffusion tensor magnetic resonance imaging of prostate cancer. Invest Radiol 2007;42:412 9.
49. Gibbs P, Pickles MD, Turnbull LW. Diffusion imaging of the prostate at 3.0 Tesla. Invest Radiol 2006;41: 185 8.
58
Background to Functional MRI of the Prostate 2

Background to Functional MRI of the Prostate 2
50. Riches SF, Hawtin K, Charles-Edwards EM, de Souza NM. Diffuison-weighted imaging of the prostate and rectal wall : comparison of biexponential and mono-exponential modelled diffusion and associated perfusion coefficients. NMR Biomed 2009; 318-325
51. Kim CK, Park BK, Kim B. High-b-value diffusion weighted imaging at 3 T to detect prostate cance: comparison between b values of 1000 and 2000 s/mm2. AJR 2010; 194:172 (33-37).
52. Futterer JJ, Engelbrecht MR, Jager GJ, et al. Prostate cancer: comparison of local staging accuracy of pelvic phased-array coil alone versus integrated endorectal-pelvic phased-array coils: local staging accuracy of prostate cancer using endorectal coil MR imaging. Eur Radiol 2007;17:1055 65.
53. Futterer JJ, Engelbrecht MR, Huisman HJ, et al. Staging prostate cancer with dynamic contrastenhanced endorectal MR imaging prior to radical prostatectomy: experienced versus less experienced readers. Radiology 2005;237:541 9.
59
Background to Functional MRI of the Prostate 2


PART TWO
DETECTION OF PRIMARY AND
RECURRENT PROSTATE CANCER


CHAPTER 3
32-Channel Coil 3T MR Guided Biopsies of Prostate Tumour Suspicious Regions on MRI
- Technique and Feasibility -
T. Hambrock; J. Fütterer; Henkjan Huisman et al.
CHAPTER 3CHAPTER 3

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
Thirty-two-Channel Coil 3 Tesla Magnetic Resonance Imaging Guided Biopsies of Prostate Tumour Suspicious Regions Identified on
Multiparameteric 3T MRI: Technique and Feasibility
Hambrock T, Fütterer JJ, Huisman HJ, Hulsbergen-van de Kaa CA, van Basten JP, van Oort I, Witjes JA, Barentsz JO
First Prize Award Society of Uroradiology and European Society of Uroradiology,
Bonita Springs, Apr 2007
Advances in Knowledge
Tumour suspicious regions identified on multiparametric 3T MR imaging can effectively
be translated to T2-weighted images during an MR biopsy session.
MR guided biopsies of tumour suspicious regions, with an MR compatible biopsy device
using a 32 channel coil, 3T MRI, is a feasible technique, which can be performed in a
clinically acceptable time and needs only a low number of biopsy cores.
Implications for Patient Care
This study shows the great potential for using an MR guided biopsy device to improve
tumour detection in patients with previous negative biopsies and tumour suspicious PSA
levels.
Summary Statement
MR guided biopsies of tumour suspicious regions identified on multiparametric 3T MR imaging, using an endorectal MR compatible
biopsy device, is a feasible technique to establish a diagnosis of tumour in patients with repeat negative biopsies but persistent
suspicion for tumour based on PSA values.
62

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
ABSTRACT
Objectives: To test the technique and feasibility of translating tumour suspicious region maps
in the prostate, obtained by multi-modality, anatomical and functional 3T MRI data to 32
channel coil, T2-weighted, 3T MR images, for directing MR guided biopsies. Furthermore to
evaluate the practicability of MR guided biopsy on a 3T MR scanner using a 32-channel coil and a
MR compatible biopsy device.
Materials and Methods: 21 Patients with a high PSA (> 4.0 ng/ml) and at least two prior
negative transrectal ultrasound guided biopsies of the prostate, underwent an endorectal coil 3T
MRI, which included T2-weighted, Diffusion Weighted and Dynamic Contrast Enhanced MR
imaging. From these multi-modality images, tumour suspicious regions (TSR) were determined.
The 3D localization of these TSRs within the prostatic gland were translated to the T2-weighted
MR images of a subsequent 32 channel coil 3T MRI. These were then biopsied under 3T MR
guidance.
Results: In all patients, TSRs could be identified and accurately translated to subsequent 3T MR
images and biopsied under MR guidance. Median MR biopsy procedure time was 35 min. Of the
21 patients, 8 (38%) were diagnosed with prostate cancer, 6 (29%) had evidence of prostatitis, 6
(29%) had combined inflammatory and atrophic changes while only 1 (5%) patient had no
identifiable pathology.
Conclusions: Multi modality, 3T MRI determined TSRs, could effectively be translated to T2-
weighted images, to be used for MR biopsies. 3T MR guided biopsy based on these translated
TSRs was feasible, performed in a clinical useful time and resulted in a high number of positive
results.
63

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
INTRODUCTION
Like many cancers, prostate cancer is treated most effectively when detected early(1). Two of
the most important tests for the early diagnosis of prostate cancer are the digital rectal
examination (DRE) and the prostate specific antigen (PSA) blood test(2). Currently, prostate
cancer is most often confirmed following biopsy of the prostate(3) and the histopathological
examination of tissue obtained from these biopsies remains the reference standard for diagnosis
of prostate cancer.
Standard sextant transrectal ultrasound (TRUS) guided biopsy of the prostate up till few years
ago was the most common method used to detect prostate cancer in patients following an
abnormal DRE or high serum PSA levels(4). Recently, it was shown that extended schemes
incorporating laterally directed biopsies, significantly increase the detection rate(5;6). Biopsy
techniques consisting of 12 cores including laterally directed cores, seem a current compromise
between maximizing the cancer detection rate and minimizing adverse events(6).
Tumour detection rates at initial biopsy sessions vary according to the extent and site of
biopsies. Schemes involving sextant and octant cores, reported cancer detection rates of 22-
29%(7;8), while ten to twelve core schemes reported initial detection rates of between 33-
36%(9;10). If patients with initial negative biopsies were subjected to subsequent sextant or
octant biopsies the tumour detection rates were between 10-19%(7;11;12) while using
extended 10-12 core schemes, tumour detection rates at second biopsy, were reported to range
between 17-35%(9;10;12;13).Unfortunately, the literature is still very heterogeneous on the
biopsy schemes performed and no clear consensus is reached yet by urologists(5;8;14-19).
Because PSA is a non-specific marker for prostate cancer, urologists are often faced with the
dilemma of managing a patient with a high index of suspicion for prostate cancer after an initial
set of negative prostate biopsies. Hence, the possibility remains that these patients may still
have tumour, as prostate cancer is often multifocal and heterogeneous in nature and the volume
of prostatic tissue sampled relatively small(7). Patient anxiety about the possibility of cancer is
particularly high when there is a high index of tumour suspicion(20). Therefore, more accurate
methods need to be found to detect or rule out significant disease.
MR imaging of the prostate has established itself as a very useful modality to accurately localize
prostate cancer within the gland(21;22). On a T2-weighted (T2-w) MR image, the characteristic
pattern of prostate cancer is a low-signal-intensity lesion. But despite high-resolution imaging
(e.g., when using an endorectal coil for MR imaging at 3T), the diagnostic localization accuracy of
64

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
T2-weighted imaging, remains quite low(23;24). Therefore, functional MR imaging modalities
have been used to increase this accuracy. Dynamic contrast enhanced MR imaging (DCE-MRI),
diffusion weighted imaging (DWI) and proton spectroscopic MR imaging (H-MRS) have all been
established as reliable techniques for this purpose: localization accuracies of DCE-MRI being
between 80 90%(21;25), DWI-MRI between 82-89%(26-28), and H-MRS around 85
%(21;29;30). Because the sensitivity of gray-scale ultrasound to localize prostate cancer is quite
low (38% to 44%)(31), MRI, with its higher tumour localization ability, can potentially be used
as a modality for directing biopsies of tumour lesions. Despite the fact that most current data on
MR of the prostate is for 1.5T imaging, recent publications on functional imaging at 3T, show a
tendency of increased accuracy(26;32;33).
Recent publications on the use of MR spectroscopic imaging to guide TRUS biopsies have shown
an improved detection yield(34;35). Because translation of MR images to ultrasound images is
technically challenging, prostate tissue sampling techniques under direct MR guidance have
been developed. Initial experience of using such MR guided devices at 1.5T, to biopsy tumour
suspicious regions on T2-w imaging, have shown promising results(36;37).
If MR guided biopsies are considered and functional imaging modalities (DCE-MRI, DWI or H-
MRS) added to anatomical images (to increase tumour localization accuracies), a robust and
accurate technique is needed to exchange information from the localization MRI to the biopsy
MR images. This accurate translation of data is crucial to improve tumour detection yield,
especially if this is to be done with a low number of cores and performed in a clinically
acceptable time.
The principal aim of our study was to test the technique and feasibility of translating tumour
suspicious region maps obtained by multi-modality, anatomical and functional, 3T MRI data to
32 channel coil, T2-weighted, 3T MR images for directing MR guided biopsies. Furthermore, we
evaluated the practicability of MR guided biopsy on a 3T MR scanner using a 32-channel coil and
a MR compatible biopsy device.
65

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
MATERIALS AND METHODS
Patients
Between Aug 2006 and Mar 2007, 21 consecutive patients were referred for tumour localization,
from the departments of urology at the Radboud University Nijmegen Medical Centre (RUMCN)
and the Canisius Wilhelmina Hospital (CWZ) in Nijmegen, Netherlands, for MR imaging of the
prostate. In 20 of these patients there was a suspicion for prostate cancer based on an elevated
PSA of > 4.0 ng/ml and/or abnormal DRE. One patient had a PSA of 1ng/ml with an abnormal
DRE and previous high-grade prostate intra-epithelial neoplasia on biopsy. All patients had
received at least two prior negative TRUS guided biopsy sessions of the prostate. In all patients,
prior biopsies had been at least 6 weeks before referral. Eight patients have received more than
two prior TRUS biopsies because of continuous concern for the presence of prostate cancer,
based on excessive high PSA > 10ng/ml or continuous rising PSA.
In 8 of 21 patients, at least one extended biopsy session was performed, which included a 9-core
sampling technique (6 lateral peripheral zone, 2 transition zone, one apically directed) while the
remaining 13 had at least one 10-core biopsy (8 peripheral zone cores and 2 transition zone
cores). Median age was 62 years (range 54 to 71) and the median PSA value was 15 ng/ml
(range 1 to 123). This study was approved by the Institutional Review Board and the
requirement for signed informed consent was waivered.
Localization MR Imaging
To identify possible tumour location(s), MR imaging was performed on these patients using a 3T
MR scanner (Siemens Trio Tim, Erlangen, Germany) with the use of an endorectal coil (Medrad,
Pittsburgh, U.S.A). The endorectal coil was inserted and filled with a 40 ml perfluorocarbon
preparation (FOMBLIN, Solvay-Solexis, Milan, Italy). Peristalsis was suppressed with an
intramuscular administration of 20 mg butylscopolaminebromide (BUSCOPAN, Boehringer-
Ingelheim, Ingelheim, Germany) and 1 mg of glucagon (GLUCAGEN, Nordisk, Gentofte,
Denmark). Following this, all patients were examined using a 3T MRI.
The imaging protocol, after fast evaluation of correct endorectal coil position with fast gradient
echo imaging, included the following sequences: first, T2-weighted turbo spin echo sequences
were performed with an in-plane resolution of 0.4 x 0.4 mm (TR 3250 ms/TE 116 m; flip angle
120; 15-19 slices; 3 mm slice thickness; echo train length 15; 180 x 180 mm field of view and
448 x 448 matrix) in axial, coronal and sagittal planes, covering the prostate and seminal
vesicles. Second, a single-shot-echo-planar imaging sequence with diffusion module and fat
66

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
suppression pulses was implemented. Water diffusion in 3 directions was measured using b-
values of 0, 50, 500 and 800 s/mm2 and a TR of 2500ms, TE of 91 ms, slices 15-19, 3mm slice
thickness and an in-plane resolution of 1.5 x 1.5 mm. ADC-maps were automatically calculated
by the scanner software. Thirdly, 3D T1-weighted spoiled gradient-echo images (TR/TE 34/1.6
ms, 14° flip angle, 10 transverse partitions on a 3D slab, 4-mm section thickness, 192-mm field of
view, 128 x 128 matrix, GRAPPA parallel imaging, factor 2) were acquired during an intravenous
bolus injection of a paramagnetic gadolinium chelate 0.1 mmol of gadopentetate dimeglumine
(DOTAREM, Guerbet, Paris, France) per kilogram of body weight which was administered with
a power injector (Spectris; Medrad) at 2.5 ml/sec and followed by a 15-ml saline flush. With this
sequence, a 3D volume with 10 partitions was acquired every 2.5 seconds during 210 seconds,
with the same positioning angle and center as the transverse T2-weighted sequence, covering
the entire prostate. Before contrast material injection, the same transverse 3D T1-weighted
gradient echo sequence (with the exception of TR/TE of 800/1.6 and an 8° flip angle) was used
to obtain proton-density images, with identical positioning to allow calculation of the relative
gadolinium chelate concentration curves.
Localization MR Data Analysis
The prostate images were viewed on an in-house developed analytical software workstation
(38), which calculated the pharmacokinetic DCE-MRI parameters and projected these
parameters as color overlay maps over the T2-w images. Additionally, ADC maps calculated
from DWI were also projected as color overlays. DWI images as such were not used as part of
the evaluation. If patient related movement caused misregistration of the different modalities,
these were corrected using a manual co-registration tool, built into the software.
Images of all patients were read in consensus by two readers with one (T.H) and four years (J.F)
experience in prostate MR imaging. The high-resolution, axial T2-w images were used as basis
for evaluation of the prostate and all other functional imaging modalities were interpreted in
relation to these. On T2-w imaging, the generally known tumour criteria were used to detect
TSRs. These included (a) low signal intensity areas in the peripheral zone (PZ), (b) within the
transition zone, a homogeneous low T2 signal intensity area with ill-defined margins or a
lenticular shape(39) and (c) within the central zone, areas of homogenous low signal intensity
with an ill-defined margin. After identification of tumour suspicious regions on T2-w images,
the ADC maps and multi-parametric pharmacokinetic (DCE-MRI derived) color maps - Ktrans, Ve,
Kep and WashOut, were analyzed in a color overlay mode on the T2-w images. The generally
known features of tumour on DCE-MR imaging(21;40) (high Ve, Ktrans, Kep and negative
67

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
WashOut) as well as areas of restriction on ADC maps (especially in the PZ and transition zone),
were used to increase the specificity of the T2-w identified TSRs.
Additionally, after the functional data from DWI and DCE images were evaluated in relation to
the TSR findings on the T2-w images, the DWI and DCE images were viewed separately and in
combination to determine additional TSRs not evident on T2-w images. Eventually, the
information from all the imaging modalities were combined and used to determine the (up to
three) most suspicious TSRs within the prostate.
Figure 1 shows an example of how the prostate was divided into different axial and sagittal
regions for 3D spatial position estimation of the TSR. This was done as follows: on the sagittal
T2-w images, the prostate was divided into 5 slabs, equating to: apex, apex-mid, mid, mid-basis
and basis levels. These slabs were equal in thickness and parallel to the axial T2-w images. The
axial T2-w slice(s) containing the TSR were then related to the corresponding sagittal slab. On
the axial T2-w images, distinction was made between peripheral zone, central zone and
transition zone and the relationship of the TSRs to these was noted. Furthermore, each axial
zone was divided into the following sub-zone regions. Peripheral zone for each left and right
half of the prostate, using the urethra as dividing point : 1) anterior horn 2) dorso-lateral region
3) dorsal region. The central zone was divided in four quadrants while the transition zone was
divided into left and right regions only. The apical and basal slabs, where the PZ and CG often do
not clearly co-exist, were divided into simple quadrants. The TSR in relation to the sub-zone
region was then noted. Therefore, for each TSR position, the slab, zone and sub-zone, were
recorded. This position was used as basis for re-identification of a TSR on the T2-w images
during the biopsy MR session.
68

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
Figure. 1. Anatomical T2-weighted images in the axial (a,c,e) and sagittal plane (g). The
sagittal images (h) were divided into 5 levels: base (B), mid-base (MB), mid (M), apex-mid
(AM) and apex (A). On the axial images the apical (b) and basal slabs (f) were divided into
quadrants, while the axial images corresponding to the apex-mid, mid and mid-basis
slabs (d) were subdivided into anatomical regions corresponding to the peripheral zone
(blue), central zone (red) and transition zone (yellow). The transition zone was divided
into left/right halves, the central zone into a quadrant while the left/right halves of the
peripheral zone, each were subdivided into the anterior horns (1), dorso-lateral region
(2) and dorsal region (3).
69

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
MR Guided biopsy
On average, two weeks (range 1 week 4 weeks) after the initial tumour localization MRI,
patients received a 32-channel coil (Invivo, Schwerin, Germany), 3T MR guided biopsy (Trio Tim,
Siemens, Germany). For antibiotic prophylaxis, all patients took oral ciprofloxacin 500 mg
(CIPROXIN, Bayer, Leverkusen, Germany) the evening before, on the morning of the biopsy, as
well as 6 hours post biopsy. Prostate biopsies were performed with the patient in the prone
position, with the 32 channel coil elements positioned beneath as well as on the back of the
patient.
A gadolinium filled needle guider was inserted rectally and attached to the arm of a MR
compatible biopsy device (Invivo, Schwerin, Germany). Figure 2 shows the MR guided biopsy
device attached to the patient, lying prone on the scanner table. The used method and
adjustments made to the device during scanning, were previously described (36;37). In
summary, the arm onto which the needle guider was attached, enabled the needle guider to be
rotated, moved forward and backward, and adjusted in height. The insertion angle can be
adjusted by rotating the needle guide about a point inside the rectum. The needle guide was
then directed to the defined TSR within the prostate. After correct alignment, the needle guide
was fixed in position for obtaining tissue samples with an 18-gauge, fully automatic, core-needle,
double-shot biopsy gun (Invivo, Schwerin, Germany) with needle length of 150 mm and tissue
core sampling length of 17 mm.
T2-w turbo spin-echo images in the axial and sagittal direction (TR 3500 ms/TE 116 ms, flip
angle 180, slice thickness 3 mm, in-plane resolution 0.7 x 0.7 mm, number of slice 15) were
obtained for anatomical visualization of the prostate. The axial T2-w slices had a similar
angulation relative to the dorsal surface of the prostate as during the localization MR session.
The MR images of the previous localization MRI were projected on a monitor, positioned next to
the MR console.
Re-identification of the TSRs on the new T2-w images was done firstly by using the relative 3D
position, which incorporated the 5 slabs, the zones and different sub-zonal regions. For this
purpose, on the sagittal T2-w images, the prostate was divided into the five slabs from apex to
base. The axial T2-w slices corresponding to the TSR slab were then identified. These were
visually divided into the different zones and sub-zone regions (see localization for details).
When the desired sub-zone region was re-identified, the positioning was a fine-tuned. This was
done by noting heterogeneous features within the gland, e.g. features relating to nodular and
stromal appearances, position of urethra and other prominent characteristics within the zones.
70

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
These were established on the T2-w images of the initial MRI, which were projected on the
computer screen next to the console and then compared to the features visible on the biopsy MR
images. If a low-signal intensity lesion was evident on the original T2-w images and re-
identified on the current T2-w images within the desired zone-region, a certain TSR re-
identification was evident. Otherwise one or two slices were scrolled up or down (axial T2-w
slices) for identification of the T2-w evident lesion.
After re-identification of the desired TSR, adjustments were made to the biopsy device to aim
the gadolinium-filled needle guider exactly towards this area. In-between adjustments, fast T2-
w TRUE-FISP images (TR 4.48ms/TE 2.24/Flip angle 70º, FOV 228 x 228 mm, Matrix 228 x 228,
Slice thickness 3mm) were made in the axial and sagittal direction (imaging time 11 seconds for
each direction) to visualize correct guider position and used to plan further adjustments.
Biopsies were obtained and to verify correct needle position within the TSR, fast T2-w TRUE-
FISP images were again obtained with the needle left in situ. This was done for each TSR that
was biopsied. One to three biopsies were taken per TSR, depending on the certainty of correct
needle position within a TSR as well as the size of the TSR. A maximum of three different TSRs
were biopsied per patient. All biopsies were performed by one radiologist (TH).
Samples were subsequently processed by a routine fixation in formaldehyde, embedded in
paraffin, stained with hematoxylin-eosin, before being evaluated by a histopathologist for the
presence of tumour or other benign pathologies.
Figure 2. Patient in prone position, with a gadolinium filled needle guider inserted
endorectally and attached to a 3D manipulating, MR compatible biopsy device (Invivo,
Schwerin, Germany)
71

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
RESULTS
The tumour localization MRI had an average scanning duration of 22 min. In all 21 patients
referred for a tumour localization MRI, one or more TSRs could be identified. On average two
TSRs were identified per patient (range 1 to 3). Using the described translation technique, all
TSR regions could be confidently re-identified during the biopsy MR session. Patients tolerated
the MR guided biopsies well and apart from one transient transurethral hemorrhage
immediately following the procedure, only minor pain after tissue sampling was reported as a
side effect by some patients. By imaging with the needle left in situ, identification of needle
position confirmed correct sampling of all the TSRs.
In total, 84 prostate cores were obtained from 40 different TSRs in 21 patients. The average
number of biopsies per patient was 4 (range 1 to 7). Of the 40 different TSRs sampled, 23%
(9/40) contained tumour, while 77% (26/40) were normal, containing benign pathological
changes in 65% (26/40) and no changes in 13% (5/40). Histopathological analysis of the
prostate samples revealed adenocarcinoma in 31% of cores (26/84) and in 38% of patients (8
out of 21). Of all core samples, 27% revealed prostatitis (23/84) while 21% (18/84) showed
combined atrophic and inflammatory changes, 1 core (1%) showed atypia and 1 (1 %) core
revealed necrosis. No identifiable pathology was found in 18% (15/84) of cores and in only one
patient.
Of the 8 patients identified with adenocarcinoma, one patient had a tumour with Gleason score
5, four had a tumour with Gleason score 6, one with two TSRs positive for tumour, each with a
Gleason score 7 and two patients with a Gleason score of 8. Of the 9 TSRs positive for tumour,
67% (6 out of 9) were in the ventral aspect of the transition zone, 22% (2 out of 9) in the
peripheral zone and 11% (1 out of 9) in the central zone.
The median duration of MR imaging guided biopsies was 35 min (range 21-75 min). A learning
curve was evident in manipulating the biopsy device and performing biopsies, quickly and
effectively. This was also reflected in the median imaging time of 41 min for the first 10 patients,
which subsequently decreased to 32 min for the following 11 patients. Table 1 reveals a
summary of the patient and biopsy findings. The imaging features of the TSRs, positive for
tumour, are summarized in Table 2. Figure 3 shows the multi-modality MR images of a patient,
which include: T2-w, DWI and DCE-MRI, used for identifying the TSRs. In this patient, the
tumour was situated in the right ventral aspect of the prostate, on the border between the
transition and central zone. Figure 4 shows this TSR, which was subsequently re-identified on
the T2-w images during the MR guided biopsy session.
72

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
Patient Age PSA Nr.previous TRUS biopsies
Nr. TSRs
Nr. Biopsies
Diagnosis Tumour Gleason Score
1 69 20 3 2 3 Tumour 6 (3+3)
2 63 1 2 1 1 Prostatitis
3 65 17 4 2 3 Tumour 6 (3+3)
4 66 20 2 2 3 Prostatitis/
Necrosis
-
5 68 58 2 1 6 Prostatitis/
Atrophy
-
6 62 7 2 1 3 Prostatitis/
Atrophy
-
7 60 4 2 1 3 Prostatitis -
8 59 8 3 3 3 Prostatitis -
9 59 20 2 3 4 Prostatitis -
10 54 12 2 1 1 Prostatitis -
11 57 8 2 2 6 N.A.D -
12 62 32 3 3 7 Prostatitis/
Atrophy
-
13 58 123 4 2 5 Tumour 6 (3+3)
14 63 14 2 3 6 Tumour 7 (4+3)
15 70 21 3 3 4 Prostatitis/
Atrophy
-
16 63 9 2 2 5 Prostatitis -
17 70 34 2 1 4 Tumour 8 (4+4)
18 61 16 4 3 3 Prostatitis
19 62 5 3 1 6 Tumour 5 (3+2)
20 71 17 3 1 3 Tumour 6 (3+3)
21 70 15 2 1 4 Tumour 8 (5+3)
Table 1. Patient and biopsy characteristics of the 21 patients biopsied.
73

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
TSR T2-w DWI DCE-MRI
1 + + +
2 + + +
3 0 + +
4 0 + +
5 + + -
6 + + -
7 + - +
8 - - +
9 - + +
Table 2. MR imaging features of TSRs positive for tumour on biopsy. A “+” indicates that a
lesion is visible while “-“ indicates no lesion visibility. Features indicated with “0” denote
non-specific heterogeneous low-signal intensity lesions on T2-w, within the central gland.
DISCUSSION
Our principal aim was to test the technique and feasibility of translating multi-modality,
anatomical and functional, 3T MRI data of tumour suspicious regions, to subsequent 32 channel
coil, T2-w, 3T MR images. We have shown this to be feasible and can be performed without
much difficulty. We further demonstrated that such a technique could be used to direct and
perform MR guided biopsies in a clinically acceptable manner on a 3T MR scanner using a 32-
channel coil and an MR compatible biopsy device.
To achieve accurate tumour localization, we performed an endorectal coil, 3T MRI, using
validated, multi-modality MR sequences with high diagnostic accuracies for tumour localization.
Additionally, because reading of these images was performed using a high sensitivity approach,
TSRs could be identified in all patients. To use multi-modality 3T MR imaging for directing 3T
MR guided biopsies is unique and contrasts to prior studies in which only T2-w imaging at low-
field systems was utilized(36;37;41).
We established that using high-resolution T2-w images as basis for image interpretation of
functi -
tuning, resulted in an accurate 3D translation of TSRs between the MR sessions. In all 21
74

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
patients, we were confident that every TSR could be adequately re-identified during the biopsy
MR session. Apart from the translation technique, this can also be related to using high-
resolution images, obtained with a 3T 32-channel coil for biopsy guidance.
We found that 32-channel coil 3T MR imaging guided biopsy, with the patient in the prone
position, is well tolerated and feasible to perform within a clinically acceptable time. The
practicability of using the current biopsy technique and equipment is in agreement with two
prior 1.5T studies (36;37) which describe a similar setup. In comparison to these prior studies,
our imaging time was remarkably reduced with an average duration of 35 min, compared to 55
min and 2 hours respectively. It should however be mentioned, that the latter reported imaging
times were also particularly high because of an initial learning curve in performing MR biopsies
and additionally a higher number of cores were obtained. We found that using the fast (11 s) T2-
w TRUE-FISP sequences at 3T, resulted in adequate visibility of anatomical details to orientate
the needle guider effectively. Faster imaging and higher anatomical detail is probably the
biggest advantage of 3T MR biopsy over 1.5T, especially with the use of a 32 channel surface coil
and parallel imaging.
Despite the fact that re-identification of the translated TSRs remains somewhat subjective; the
high tumour detection rate directed towards these regions (31% of samples and 38% of
patients) and the high prevalence of benign pathological diagnoses (67% - 27/40 of TSRs), is a
good indirect validation of satisfactory re-identification. The preliminary results also show a
higher tumour detection percentage (38%) compared to sextant and octant TRUS guided
biopsies after two prior negative biopsies, reported in the literature (8-14%)(7;11;12). It has to
be emphasized that the detection of prostate cancer in subsequent biopsy sessions is strongly
dependent on the biopsy scheme used during the initial and subsequent sessions(42) as well as
patient related factors like PSA value, prostate volume and the population prevalence of prostate
cancer(43;44). In an attempt to increase the detection rate during rebiopsy, saturation biopsy
techniques with greatly increased the number of samples (> 20 cores), have been advocated by
some researchers. These saturation biopsy strategies were shown to increase detection rates
(25-41%)44,45,46, but at the expense of pain and complications, as well as the unduly high cost of
processing the large amount of pathological material. The preliminary results of our current
research may not show an increased detection performance to such saturation schemes but at a
similar performance, our technique will be a more appealing alternative. Furthermore,
saturation biopsies are not yet advocated by the European Guidelines for Prostate Cancer and
only performed by few urologists in our country.
75

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
Figure 3. A case example with images from the endorectal coil, multi-modality 3T MRI.
The axial T2-w image (a) shows a low signal intensity area in the transitions zone, right
(arrow). The ADC map (b) from the DWI shows the same area with restriction in diffusion
ability while the WashOut pharmacokinetic map (c), calculated from the DCE-MRI data,
shows an enhanced removal rate of gadolinium. Images (d) and (e) show the TSR
identified by the readers. The subsequent “crude” estimation of the 3D location within
the gland shows the TSR to be predominantly within the right aspect of the transition
zone (f) and in the mid-base (MB) slab (g).
76

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
Figure 4. The TSR (yellow interrupted circle) identified from the multi-modality,
endorectal coil, 3T MR images, is translated to the 32 channel coil T2-w images using the
3D localization method. The mid-base (MB) level containing the TSR is first identified (a).
On the axial T2-w images (b) within this level, the right transition zone area with TSR is
found. The gadolinium filled needle guider is directed on sagittal (c) and axial (d) images
towards this re-identified region. Correct needle positioning and tissue sampling from
the TSR is verified by imaging with the needle left insitu (e).
77

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
All our patients have received at least one prior TRUS session with tissue sampling of the
transition zone. Despite this, 67 % of our tumour containing TSRs were situated in the
transition zone. Although our results are too preliminary to make definite conclusions, it does
seem as if the lack of extended transition zone sampling in rebiopsy session could account for
the large number of tumours missed. It is known that 25% of prostate cancers arise in the
transition zone(45), yet most studies on extended biopsy techniques, conclude that laterally
directed cores, apical sampling or sampling of the anterior horns, increases the detection yield,
while additional sampling of the transition zone, does not. (6;46-48)
The transrectal sampling approach has the advantage of being the least invasive and requiring
no anesthesia, compared to other described MR biopsy approaches, of which transperineal(49)
and transgluteal(41;50) are the best known techniques. However, infection risk is increased
when an endorectal approach to tissue sampling is used(51). Djavan et al.(51) has shown that
complications due to prostatic biopsies are not trivial. Of all their patients that underwent
biopsies, 11% developed infectious complications, 63% had bleeding related problems while up
to 8% had significant pain or discomfort. We have demonstrated that by limiting the biopsy
cores to MR determined, tumour suspicious regions only, a lower number of cores can be
obtained, with an average of 4 in our study. This has the advantageous potential to reduce
bleeding risk, infection risk as well as patient discomfort and pain.
Other authors have shown that using T2-w imaging alone for tumour localization can be
valuable in guiding biopsies performed in a closed-bore MRI scanner. It is known that T2-w
imaging on its own has a quite poor sensitivity for localizing prostate cancer, reported in the
literature to range between 58% and 65%(32;52). Only one study has looked at a possible
advantage of adding DCE-MRI imaging to T2-w imaging for guidance of MR biopsies.
Unfortunately, a too small patients group was evaluated to assess the possible benefit(53).
Because of the currently available data on tumour localization accuracies by MRI, we decided to
maximize the possibility of tumour detection likelihood, by utilizing high-spatial resolution
imaging with an endorectal coil at 3T and obtaining DCE and DWI imaging in addition to T2-w
imaging. This approach however, has the drawback that performing a localization MRI and
biopsy MRI in the same imaging session is deemed unpractical. Changing the endorectal coil,
awaiting software post-processing of the DCE data and the time consuming evaluation of images,
were all considered practical reasons to postpone the MR guided biopsy to another session.
Additionally because recent evidence by Heijmink et al. (23) has shown that the localization
accuracy of endorectal coil, T2-w 3T MR imaging is significantly improved compared to using a
78

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
surface coil for T2-w, 3T imaging (Az 0.68 vs 0.62), we decided to use the endorectal coil for
localization.
The preliminary data on the 9 TSRs positive for tumour (Table 2) indicated that for 2 TSRs,
functional imaging modalities directed the biopsies towards tumour whereas T2-w images
showed no lesion visible. Additionally, for another 2 TSRs, the heterogeneous nature of the
central gland with diffuse low signal intensities on T2-w imaging was found unhelpful for clear
localization of the TSRs, something that was only possible with the addition of functional data.
One of the limitations of this study is the small number of patients used. However, this study
was designed as a pilot to assess the technique of translating multi-modality MR data and the
feasibility of MR imaging guided biopsies at 3 Tesla. Additionally, an arbitrarily defined
maximum of 3 TSRs was chosen, as increasing this number further would have resulted in
prolonged, clinically unacceptable imaging time and discomfort to the patient. Interpreting
anatomical and functional MR images of the prostate requires a degree of experience, which
might make routine clinical application of this technique somewhat difficult. However, recently
Vos et al.(54) showed that by using computer aided diagnostic (CAD) software support for DCE-
MRI, a method can be found to aid radiologists to improve the accuracy of tumour localization.
CONCLUSIONS
Our conclusions are that TSR maps identified on multi-modality, anatomical and functional, 3T
MR imaging can effectively be translated to T2-weighted images during a MR biopsy session by
using simple visual criteria. Furthermore, MR guided biopsies of these TSRs, with the MR
compatible biopsy device using a 32 channel coil, 3T MRI, is a feasible technique, which can be
performed in a clinically acceptable time and needs only a low number of biopsy cores. This
shows great potential for improving tumour detection in patients with previous negative
biopsies and tumour suspicious PSA levels. Assessing the true overall tumour detection
capabilities, the benefit of MR guided biopsies over extended biopsy techniques in rebiopsy
sessions and the need for using an endorectal coil, is part of an ongoing study.
79

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
REFERENCES
1. McLeod DG. Success and failure of single-modality treatment for early prostate cancer. Rev.Urol. 2004;6 Suppl 2:S13-S19.
2. Bigliocchi M, Marini M, Nofroni I, Perugia G, Shahabadi H, Ciccariello M. Prostate cancer detection rate of transrectal ultrasonography, digital rectal examination, and prostate-specific antigen: results of a five-year study of 6- versus 12-core transperineal prostate biopsy. Minerva Urol.Nefrol. 2007 Dec;59(4):395-406.
3. Hodge KK, McNeal JE, Terris MK, Stamey TA. Random systematic versus directed ultrasound guided transrectal core biopsies of the prostate. J.Urol. 1989 Jul;142(1):71-4.
4. Raja J, Ramachandran N, Munneke G, Patel U. Current status of transrectal ultrasound-guided prostate biopsy in the diagnosis of prostate cancer. Clin.Radiol. 2006 Feb;61(2):142-53.
5. Djavan B, Margreiter M. Biopsy standards for detection of prostate cancer. World J.Urol. 2007 Mar;25(1):11-7.
6. Eichler K, Hempel S, Wilby J, Myers L, Bachmann LM, Kleijnen J. Diagnostic value of systematic biopsy methods in the investigation of prostate cancer: a systematic review. J.Urol. 2006 May;175(5):1605-12.
7. Djavan B, Ravery V, Zlotta A, Dobronski P, Dobrovits M, Fakhari M, Seitz C, Susani M, Borkowski A, Boccon-Gibod L, et al. Prospective evaluation of prostate cancer detected on biopsies 1, 2, 3 and 4: when should we stop? J.Urol. 2001 Nov;166(5):1679-83.
8. Gosselaar C, Roobol MJ, Roemeling S, Wolters T, van Leenders GJ, Schroder FH. The value of an additional hypoechoic lesion-directed biopsy core for detecting prostate cancer. BJU.Int. 2008 Mar;101(6):685-90.
9. Mian BM, Naya Y, Okihara K, Vakar-Lopez F, Troncoso P, Babaian RJ. Predictors of cancer in repeat extended multisite prostate biopsy in men with previous negative extended multisite biopsy. Urology 2002 Nov;60(5):836-40.
10. Philip J, Hanchanale V, Foster CS, Javle P. Importance of peripheral biopsies in maximising the detection of early prostate cancer in repeat 12-core biopsy protocols. BJU.Int. 2006 Sep;98(3):559-62.
11. Keetch DW, Catalona WJ, Smith DS. Serial prostatic biopsies in men with persistently elevated serum prostate specific antigen values. J.Urol. 1994 Jun;151(6):1571-4.
12. Roehl KA, Antenor JA, Catalona WJ. Serial biopsy results in prostate cancer screening study. J.Urol. 2002 Jun;167(6):2435-9.
13. Hong YM, Lai FC, Chon CH, McNeal JE, Presti JC, Jr. Impact of prior biopsy scheme on pathologic features of cancers detected on repeat biopsies. Urol.Oncol. 2004 Jan;22(1):7-10.
14. Djavan B, Zlotta AR, Ekane S, Remzi M, Kramer G, Roumeguere T, Etemad M, Wolfram R, Schulman CC, Marberger M. Is one set of sextant biopsies enough to rule out prostate Cancer? Influence of transition and total prostate volumes on prostate cancer yield. Eur.Urol. 2000 Aug;38(2):218-24.
15. Djavan B, Remzi M, Marberger M. When to biopsy and when to stop biopsying. Urol.Clin.North Am. 2003 May;30(2):253-62, viii.
16. Eskew LA, Bare RL, McCullough DL. Systematic 5 region prostate biopsy is superior to sextant method for diagnosing carcinoma of the prostate. J.Urol. 1997 Jan;157(1):199-202.
17. Presti JC. Prostate biopsy: current status and limitations. Rev.Urol. 2007;9(3):93-8. 18. Presti JC, Jr., Chang JJ, Bhargava V, Shinohara K. The optimal systematic prostate biopsy scheme should include
8 rather than 6 biopsies: results of a prospective clinical trial. J.Urol. 2000 Jan;163(1):163-6.
19. Roobol MJ, Grenabo A, Schroder FH, Hugosson J. Interval cancers in prostate cancer screening: comparing 2- and 4-year screening intervals in the European Randomized Study of Screening for Prostate Cancer, Gothenburg and Rotterdam. J.Natl.Cancer Inst. 2007 Sep 5;99(17):1296-303.
20. Carlsson S, Aus G, Wessman C, Hugosson J. Anxiety associated with prostate cancer screening with special reference to men with a positive screening test (elevated PSA) - Results from a prospective, population-based, randomised study. Eur.J.Cancer 2007 Jul 20.
21. Futterer JJ, Heijmink SW, Scheenen TW, Veltman J, Huisman HJ, Vos P, Hulsbergen-Van de Kaa CA, Witjes JA, Krabbe PF, Heerschap A, et al. Prostate cancer localization with dynamic contrast-enhanced MR imaging and proton MR spectroscopic imaging. Radiology 2006 Nov;241(2):449-58.
22. Tanimoto A, Nakashima J, Kohno H, Shinmoto H, Kuribayashi S. Prostate cancer screening: the clinical value of diffusion-weighted imaging and dynamic MR imaging in combination with T2-weighted imaging. J.Magn Reson.Imaging 2007 Jan;25(1):146-52.
23. Heijmink SW, Futterer JJ, Hambrock T, Takahashi S, Scheenen TW, Huisman HJ, Hulsbergen-Van de Kaa CA, Knipscheer BC, Kiemeney LA, Witjes JA, et al. Prostate cancer: body-array versus endorectal coil MR imaging at 3 T--comparison of image quality, localization, and staging performance. Radiology 2007 Jul;244(1):184-95.
80

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
24. Jager GJ, Ruijter ET, van de Kaa CA, de la Rosette JJ, Oosterhof GO, Thornbury JR, Barentsz JO. Local staging of prostate cancer with endorectal MR imaging: correlation with histopathology. AJR Am.J.Roentgenol. 1996 Apr;166(4):845-52.
25. Ito H, Kamoi K, Yokoyama K, Yamada K, Nishimura T. Visualization of prostate cancer using dynamic contrast-enhanced MRI: comparison with transrectal power Doppler ultrasound. Br.J.Radiol. 2003 Sep;76(909):617-24.
26. Kim CK, Park BK, Lee HM, Kwon GY. Value of diffusion-weighted imaging for the prediction of prostate cancer location at 3T using a phased-array coil: preliminary results. Invest Radiol. 2007 Dec;42(12):842-7.
27. Haider MA, van der Kwast TH, Tanguay J, Evans AJ, Hashmi AT, Lockwood G, Trachtenberg J. Combined T2-weighted and diffusion-weighted MRI for localization of prostate cancer. AJR Am.J.Roentgenol. 2007 Aug;189(2):323-8.
28. Miao H, Fukatsu H, Ishigaki T. Prostate cancer detection with 3-T MRI: Comparison of diffusion-weighted and T2-weighted imaging. Eur.J.Radiol. 2007 Feb;61(2):297-302.
29. Futterer JJ, Scheenen TW, Heijmink SW, Huisman HJ, Hulsbergen-Van de Kaa CA, Witjes JA, Heerschap A, Barentsz JO. Standardized threshold approach using three-dimensional proton magnetic resonance spectroscopic imaging in prostate cancer localization of the entire prostate. Invest Radiol. 2007 Feb;42(2):116-22.
30. Jung JA, Coakley FV, Vigneron DB, Swanson MG, Qayyum A, Weinberg V, Jones KD, Carroll PR, Kurhanewicz J. Prostate depiction at endorectal MR spectroscopic imaging: investigation of a standardized evaluation system. Radiology 2004 Dec;233(3):701-8.
31. Halpern EJ, Strup SE. Using gray-scale and color and power Doppler sonography to detect prostatic cancer. AJR Am.J.Roentgenol. 2000 Mar;174(3):623-7.
32. Kim CK, Park BK, Kim B. Localization of prostate cancer using 3T MRI: comparison of T2-weighted and dynamic contrast-enhanced imaging. J.Comput.Assist.Tomogr. 2006 Jan;30(1):7-11.
33. Manenti G, Carlani M, Mancino S, Colangelo V, Di RM, Squillaci E, Simonetti G. Diffusion tensor magnetic resonance imaging of prostate cancer. Invest Radiol. 2007 Jun;42(6):412-9.
34. Prando A, Kurhanewicz J, Borges AP, Oliveira EM, Jr., Figueiredo E. Prostatic biopsy directed with endorectal MR spectroscopic imaging findings in patients with elevated prostate specific antigen levels and prior negative biopsy findings: early experience. Radiology 2005 Sep;236(3):903-10.
35. Yuen JS, Thng CH, Tan PH, Khin LW, Phee SJ, Xiao D, Lau WK, Ng WS, Cheng CW. Endorectal magnetic resonance imaging and spectroscopy for the detection of tumour foci in men with prior negative transrectal ultrasound prostate biopsy. J.Urol. 2004 Apr;171(4):1482-6.
36. Anastasiadis AG, Lichy MP, Nagele U, Kuczyk MA, Merseburger AS, Hennenlotter J, Corvin S, Sievert KD, Claussen CD, Stenzl A, et al. MRI-guided biopsy of the prostate increases diagnostic performance in men with elevated or increasing PSA levels after previous negative TRUS biopsies. Eur.Urol. 2006 Oct;50(4):738-48.
37. Beyersdorff D, Winkel A, Hamm B, Lenk S, Loening SA, Taupitz M. MR imaging-guided prostate biopsy with a closed MR unit at 1.5 T: initial results. Radiology 2005 Feb;234(2):576-81.
38. Futterer JJ, Engelbrecht MR, Huisman HJ, Jager GJ, Hulsbergen-Van de Kaa CA, Witjes JA, Barentsz JO. Staging prostate cancer with dynamic contrast-enhanced endorectal MR imaging prior to radical prostatectomy: experienced versus less experienced readers. Radiology 2005 Nov;237(2):541-9.
39. Akin O, Sala E, Moskowitz CS, Kuroiwa K, Ishill NM, Pucar D, Scardino PT, Hricak H. Transition zone prostate cancers: features, detection, localization, and staging at endorectal MR imaging. Radiology 2006 Jun;239(3):784-92.
40. Engelbrecht MR, Huisman HJ, Laheij RJ, Jager GJ, van Leenders GJ, Hulsbergen-Van de Kaa CA, de la Rosette JJ, Blickman JG, Barentsz JO. Discrimination of prostate cancer from normal peripheral zone and central gland tissue by using dynamic contrast-enhanced MR imaging. Radiology 2003 Oct;229(1):248-54.
41. Zangos S, Eichler K, Engelmann K, Ahmed M, Dettmer S, Herzog C, Pegios W, Wetter A, Lehnert T, Mack MG, et al. MR-guided transgluteal biopsies with an open low-field system in patients with clinically suspected prostate cancer: technique and preliminary results. Eur.Radiol. 2005 Jan;15(1):174-82.
42. Hong YM, Lai FC, Chon CH, McNeal JE, Presti JC, Jr. Impact of prior biopsy scheme on pathologic features of cancers detected on repeat biopsies. Urol.Oncol. 2004 Jan;22(1):7-10.
43. Dong F, Jones JS, Stephenson AJ, Magi-Galluzzi C, Reuther AM, Klein EA. Prostate cancer volume at biopsy predicts clinically significant upgrading. J.Urol. 2008 Mar;179(3):896-900.
44. Presti JC, Jr., Chang JJ, Bhargava V, Shinohara K. The optimal systematic prostate biopsy scheme should include 8 rather than 6 biopsies: results of a prospective clinical trial. J.Urol. 2000 Jan;163(1):163-6.
45. Sakai I, Harada K, Hara I, Eto H, Miyake H. A comparison of the biological features between prostate cancers arising in the transition and peripheral zones. BJU.Int. 2005 Sep;96(4):528-32.
81

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
46. Damiano R, Autorino R, Perdona S, De SM, Oliva A, Esposito C, Cantiello F, Di LG, Sacco R, D'Armiento M. Are extended biopsies really necessary to improve prostate cancer detection? Prostate Cancer Prostatic.Dis. 2003;6(3):250-5.
47. Inahara M, Suzuki H, Kojima S, Komiya A, Fukasawa S, Imamoto T, Naya Y, Ichikawa T. Improved prostate cancer detection using systematic 14-core biopsy for large prostate glands with normal digital rectal examination findings. Urology 2006 Oct;68(4):815-9.
48. Siu W, Dunn RL, Shah RB, Wei JT. Use of extended pattern technique for initial prostate biopsy. J.Urol. 2005 Aug;174(2):505-9.
49. D'Amico AV, Tempany CM, Cormack R, Hata N, Jinzaki M, Tuncali K, Weinstein M, Richie JP. Transperineal magnetic resonance image guided prostate biopsy. J.Urol. 2000 Aug;164(2):385-7.
50. Zangos S, Herzog C, Eichler K, Hammerstingl R, Lukoschek A, Guthmann S, Gutmann B, Schoepf UJ, Costello P, Vogl TJ. MR-compatible assistance system for punction in a high-field system: device and feasibility of transgluteal biopsies of the prostate gland. Eur.Radiol. 2007 Apr;17(4):1118-24.
51. Djavan B, Waldert M, Zlotta A, Dobronski P, Seitz C, Remzi M, Borkowski A, Schulman C, Marberger M. Safety and morbidity of first and repeat transrectal ultrasound guided prostate needle biopsies: results of a prospective European prostate cancer detection study. J.Urol. 2001 Sep;166(3):856-60.
52. Jager GJ, Ruijter ET, van de Kaa CA, de la Rosette JJ, Oosterhof GO, Thornbury JR, Barentsz JO. Local staging of prostate cancer with endorectal MR imaging: correlation with histopathology. AJR Am.J.Roentgenol. 1996 Apr;166(4):845-52.
53. Singh AK, Krieger A, Lattouf JB, Guion P, Grubb RL, III, Albert PS, Metzger G, Ullman K, Smith S, Fichtinger G, et al. Patient selection determines the prostate cancer yield of dynamic contrast-enhanced magnetic resonance imaging-guided transrectal biopsies in a closed 3-Tesla scanner. BJU.Int. 2008 Jan;101(2):181-5.
54. Vos P, Hambrock T, Hulsbergen-Van de Kaa CA, Futterer JJ, Barentsz J, Huisman HJ. Computerized analysis of prostate lesions in the peripheral zone using dynamic contrast enhanced MRI. Med.Phys. 2008;Accepted, awaiting publication.
82

MR Guided Biopsies of the Prostate Technique and Feasibility - 3
46. Damiano R, Autorino R, Perdona S, De SM, Oliva A, Esposito C, Cantiello F, Di LG, Sacco R, D'Armiento M. Are extended biopsies really necessary to improve prostate cancer detection? Prostate Cancer Prostatic.Dis. 2003;6(3):250-5.
47. Inahara M, Suzuki H, Kojima S, Komiya A, Fukasawa S, Imamoto T, Naya Y, Ichikawa T. Improved prostate cancer detection using systematic 14-core biopsy for large prostate glands with normal digital rectal examination findings. Urology 2006 Oct;68(4):815-9.
48. Siu W, Dunn RL, Shah RB, Wei JT. Use of extended pattern technique for initial prostate biopsy. J.Urol. 2005 Aug;174(2):505-9.
49. D'Amico AV, Tempany CM, Cormack R, Hata N, Jinzaki M, Tuncali K, Weinstein M, Richie JP. Transperineal magnetic resonance image guided prostate biopsy. J.Urol. 2000 Aug;164(2):385-7.
50. Zangos S, Herzog C, Eichler K, Hammerstingl R, Lukoschek A, Guthmann S, Gutmann B, Schoepf UJ, Costello P, Vogl TJ. MR-compatible assistance system for punction in a high-field system: device and feasibility of transgluteal biopsies of the prostate gland. Eur.Radiol. 2007 Apr;17(4):1118-24.
51. Djavan B, Waldert M, Zlotta A, Dobronski P, Seitz C, Remzi M, Borkowski A, Schulman C, Marberger M. Safety and morbidity of first and repeat transrectal ultrasound guided prostate needle biopsies: results of a prospective European prostate cancer detection study. J.Urol. 2001 Sep;166(3):856-60.
52. Jager GJ, Ruijter ET, van de Kaa CA, de la Rosette JJ, Oosterhof GO, Thornbury JR, Barentsz JO. Local staging of prostate cancer with endorectal MR imaging: correlation with histopathology. AJR Am.J.Roentgenol. 1996 Apr;166(4):845-52.
53. Singh AK, Krieger A, Lattouf JB, Guion P, Grubb RL, III, Albert PS, Metzger G, Ullman K, Smith S, Fichtinger G, et al. Patient selection determines the prostate cancer yield of dynamic contrast-enhanced magnetic resonance imaging-guided transrectal biopsies in a closed 3-Tesla scanner. BJU.Int. 2008 Jan;101(2):181-5.
54. Vos P, Hambrock T, Hulsbergen-Van de Kaa CA, Futterer JJ, Barentsz J, Huisman HJ. Computerized analysis of prostate lesions in the peripheral zone using dynamic contrast enhanced MRI. Med.Phys. 2008;Accepted, awaiting publication.
82


— CHAPTER 4 —
Magnetic Resonance Imaging Guided Prostate Biopsies in Men
with Repetitive Negative Biopsies and Elevated PSA
T. Hambrock; D. Somford; C. Hoeks et al.
CHAPTER 4CHAPTER 4

Magnetic Resonance Imaging Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
Journal of Urology, 2010 Feb; 183(2):520-7
Hambrock T, Somford DM, Hoeks C, Bouwense SA, Huisman HJ, Yakar D,
van Oort IM, Witjes JA, Fütterer JJ, Barentsz JO
Cum Laude Award Society of Computed Body Tomography and Magnetic Resonance, 2009
Advances in Knowledge
3T Multiparametric MRI is a highly effective method for the detection and localization of
clinically significant prostate cancer.
MR guided biopsies towards tumour suspicious regions on MRI is a very useful method
for accurately validating correct sampling of prostatic tissue.
Tumour detected in patients with repeat negative biopsies are mostly located in areas
not explicitly sampled by routine schemes.
Implications for Patient Care
MRI should be considered essential in any workup protocol of patients who are
suspected of harboring malignancy but who have successive negative biopsies.
Because of the low numbers of cores needed, MR guided biopsies is an appealing
alternative to procedures such as saturation biopsies.
Summary Statement
3T Multiparametric MR imaging in combination with MR guided biopsies, represent a very effective method for diagnosing clinically significant prostate cancer in men with repeat negative biopsies and
abnormal PSA values.
84
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

ABSTRACT
Background: Undetected cancer in repeat transrectal ultrasound guided prostate biopsies
(TRUS-GB) in patients with elevated Prostatic specific antigen (PSA) > 4 ng/mL is a considerable
concern. We investigated the tumour detection rate of biopsies from tumour suspicious regions
on multi-modality 3T Magnetic Resonance Imaging (m-m MRI) and subsequent MR-guided
biopsy (MR-GB) in sixty eight men with repetitive negative TRUS-GB and compared this to a
matched TRUS-GB population. Furthermore we aimed to determine the clinical significance of
detected tumours.
Methods: Seventy one consecutive patients with PSA >4 ng/ml and -GB
sessions received a m-m MRI. In 68 patients this was followed by MR-GB directed towards
tumour suspicious regions. A matched, multi-session TRUS-GB population from our institutional
database was used for comparison. Clinical significance of tumours detected was established
using accepted criteria (PSA, gleason grade, stage, tumour volume).
Results: The tumour detection rate (DR) with m-m MRI MR-GB was 59% (40/68) using a
median of 4 cores. The tumour DRs were significantly (p <0.01) higher than TRUS-GB in all
patient subgroups except those with PSA >20 ng/ml, prostate volumes >65 cc and PSA density
>0 tumours,
93% (37/40) were considered highly likely to harbor clinically significant disease.
Conclusions: Multi-modality MRI is an effective technique for localizing prostate cancer and
MR-guided biopsy of tumour suspicious regions is an accurate method of detecting clinically
significant prostate cancer in men with repetitive negative biopsies and elevated PSA.
85
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

INTRODUCTION
In 2008, prostate cancer was the most frequently diagnosed cancer in men, accounting for 25%
of all cancers. The most widely used tests for the screening of prostate cancer are digital rectal
examination and the prostate specific antigen (PSA) blood-serum test. An elevated PSA is not
cancer-specific as numerous benign prostatic conditions can elevated PSA levels. Urologists are
increasingly faced with the dilemma of how best to manage a patient with elevated PSA in which
repeat Transrectal Ultrasound Guided Biopsies (TRUS-GB) reveal no cancer.
Systematic TRUS-GB of the prostate is the standard procedure for histological sampling of the
prostate. Prostate cancer is often multifocal and the volume sampled by systematic TRUS-GB
relatively small. The value of MRI in accurately localizing prostate cancer is well established(1).
The accuracy of cancer localization on anatomical T2-w imaging remains low(2), therefore
dynamic contrast enhanced MR imaging (DCE-MRI) and diffusion weighted imaging (DWI) have
been implemented and shown to improve the accuracy of prostate cancer localization. A multi-
modality approach using a combination of these techniques appears the optimal approach(3).
Imaging-guided biopsies have been advocated to improve tumour detection. However, grey-
scale TRUS, the most commonly used technique for guidance of biopsies, has a low sensitivity
for localizing prostate cancer(4). A combined approach using systematic and additional lesion
directed biopsies of contrast-enhanced suspicious areas, appears more useful(5;6).
The principal aim of our study was to determine the tumour detection yield of m-m MRI
followed by directed MR-GB in a large patient group with clinical suspicion of cancer but with
repetitive negative systematic TRUS-GBs. Furthermore we aimed to determine whether the
detected tumours were clinically significant.
MATERIALS AND METHODS
Patients
Between August 2006 and March 2008, 71 consecutive patients with PSA >4 ng/ml and
negative TRUS-GB sessions (of which the last session included at least an extended scheme of 8-,
9- or 10-cores, including transition zone sampling) were referred from the departments of
Urology at the Radboud University Nijmegen Medical Centre (RUNMC) and the Canisius
86
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

Wilhelmina Hospital (CWZ) in Nijmegen, the Netherlands, for clinically routine m-m MRI of the
prostate. The Institutional Review Board approved this study.
The RUNMC histopathology database was searched for consecutive patients (January 2000 - Dec
2006) with two or more TRUS-GB sessions. Only patients who underwent at least one
systematic biopsy protocol of 8- to 10-cores, including transition zone (TZ) biopsies, were
included. At each TRUS-GB session, the principal diagnosis, age, PSA and prostate volumes were
noted. To remove the bias effect of differences in PSA and prostate volumes, tumour detection
rates for patients were compared by subgroup analysis of PSA, prostate volume and PSA density.
Localization MR Imaging
To identify possible tumour location(s), MR imaging was performed using a 3T MR scanner
(Siemens Trio Tim, Erlangen, Germany) with endorectal coil (Medrad, Pittsburgh, U.S.A) in 28
patients and the pelvic phased array coils only, in 40 patients. Axial, sagittal and coronal T2-w
images, axial DWI and DCE-MR images (using15 ml gadopentetate dimeglumine (DOTAREM,
Guerbet, Paris, France) were obtained.
Localization MR Data Analysis
Prostate images were viewed on an in-house developed analytical software workstation, which
projected the calculated DCE-MRI parameters(7) and apparent diffusion coefficient (ADC) maps
as color overlays over the T2-w images. All patient images were read in consensus by two
readers with two (T.H) and five (J.F) years experience in prostate MR imaging. MR-images were
used to determine up to three tumour suspicious regions (TSRs) for biopsy, using features
described in literature(8;9).
MR Guided biopsy
On average two weeks (range 1– 6) after the initial MRI to localize possible tumours and
identify TSR for MR-GB planning, patients received a 3T MR-GB of the prostate. Antibiotic
prophylaxis using oral ciprofloxacin 500 mg (CIPROXIN, Bayer, Leverkusen, Germany) was
given. A previously described(10) translation technique using an MR compatible biopsy device
(Invivo, Schwerin, Germany) was used for obtaining 18-gauge biopsy cores (MR-compatible
biopsy gun, Invivo, Germany) of re-identified TSRs. In brief: a needle guider attached to the arm
of the biopsy device was inserted rectally. It was subsequently adjusted to aim towards the TSR
in the prostate. Biopsies were then obtained through the needle guider. No random and only
TSRs directed biopsies were obtained. All biopsies were performed by one radiologist (TH).
87
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

Samples were subsequently processed by routine histopathological fixation and staining and
evaluated by a histopathologist.
Statistical analysis
Chi-square tests were performed to calculate for significant difference between MR-GB and
TRUS-GB subgroups. The Mann-Whitney U was performed for comparing mean age, mean PSA,
mean prostate volumes and mean PSAD between groups. A significant difference was considered
when p <0.05. Statistical analyses were performed with SPSS software (SPSS, version 16.0.01,
Chicago, U.S.A).
Evaluation of clinical significance of tumours
The clinical significance of tumours detected was determined by using currently accepted
criteria(11-14). In patients where prostatectomy was performed after a positive biopsy, a
Gleason grade 4 or 5 component, stage pT3 or tumour volume >0.5 cc were considered to
represent clinical significant disease (CSD). In patients diagnosed with cancer in whom no
prostatectomy was performed, cancer was considered significant if PSA values at biopsy were
>10 ng/ml and PSA densities were >0.15 ng/ml/cc, or a Gleason grade 4 or 5 was found on
biopsy.
RESULTS
In 70/71 patients, TSRs could be identified on MRI. One patient refused biopsies, while in
another patient no biopsies were performed because of a high bleeding risk and no certain
evidence of tumour on MRI, leaving 68 patients who received MR-GB.
The 68 patients had a mean age of 63 years (range 48-74), a median PSA of 13 ng/ml (range 4-
243) and a median of 3 (range 2-7) previous negative TRUS-GB sessions. MR-GBs of the prostate
had a median procedure duration of 30 min (range 14-75).
The tumour DR with MR-GB was 59% (40/68). In total 260 prostate cores -only directed and
no random cores- were obtained from 114 different TSRs (TSR tumour DR 40%, 46/114). The
median number of biopsies per patient was 4 (range 2 to 7). A summary of patient and
pathological findings is given in Table 1.
88
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

All patients Tumour No Tumour Patient Characteristics - Number of patients 68 40 28 - Mean Age in years (range) 63 (48-76) 65 (48-76) 62 (54-70) - Median PSA ng/ml (range) 13 (4-243) 13 (5-243) 12 (4-58) - Positive family history for prostate cancer 4 (6%) 2 (50%) 2 (50%) - Suspicious DRE 2 (3%) 1 (50%) 1 (50%) - Median number of previous TRUS-GB 3 (2-8) 3 (2-7) 3 (2-8) Imaging and Biopsy Characteristics -TSRs per patient (range) 1 (1-3) 1 (1-3) 2 (2-3) - Median biopsy cores obtained (range) 4 (2-7) 3 (2-6) 4 (2-7) - Median MR biopsy time – min. (range) 30 (14-75) 29 (14-75) 33 (15-55) - Principal histological diagnosis ~ Tumour ~ Chronic Prostatitis ~ Prostatitis + Reactive Atypia ~ Acute Prostatitis ~ Atypia suspect for malignancy ~ Atypical adenomatous hyperplasia ~ Fibromuscular Nodule ~ Necrosis ~ No abnormality detected
40
15 2 1 2 2 2 1 3
- Patient highest tumour GS distribution (40 Patients) 5 6 7 8 9
3 (7%) 19 (48%) 10 (25%) 5 (12%) 3 (8%)
- Clinically significance of disease (40 Patients with tumour) Criteria (Determined in RP) (Determined in MR-GB + no RP) ~ Tumour ~ Stage pT3 on RP ~ PSA > 10 + PSA density > 0.15 ~ Insignificant disease cannot be ruled out
18 (10) (9) 8 1 2 5
10
3
- Advanced disease ~ M+/N+ ~ Stage T3 in RP
20% (8/40) 3 5
Table 1. Summary findings of patient, radiological and pathological features. (RP =
radical prostatectomy, M = Metastasis, N = Nodal Metastasis)
89
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

Radical prostatectomy was performed in 20 of the 40 patients with tumour. Gleason score (GS)
(30%). In 10/20 a tumour volume > 0.5cc (with GS 6) was found. All of the prostatectomy
patients therefore harbored CSD. In the remaining 20 patients, external beam radiotherapy
(11/20), brachytherapy (3/20), hormonal ablation (3/20) or active surveillance (3/20) was
performed. In these patients, biopsy GS, prostatic volumes and PSA values were used to assess
the presence of CSD with 9/20 patients having a bi
PSAD > 0.15ng/ml/cc. One patient had skeletal metastasis. Therefore CSD was considered to be
present in 85% (17/20) of these patients and in 93% (37/40) of all tumour patients. Aggressive
cancer was evident in at least 48% (19/40) of all tumour The
tumour characteristics are summarized in Table 2.
2nd TRUS-GB 3rd TRUS-GB MR-GB Statistical significance
p value Number of patients ~ Tumour patients ~ Non-tumour patients
248 55 (22%) 193
65 10 (15%) 55
68 40 (59%) 28
A ** B **
Mean Age in years (range) ~ All patients ~ Tumour patients ~ Non-tumour patients
64 (74-80) 66 (52-78) 64 (52-78)
65 (48-76) 64 (57-75) 65 (48-76)
63 (48-76) 65 (48-76) 62 (54-70)
A B A B
Median PSA ng/ml (range) ~ All patients ~ Tumour patients ~ Non-tumour patients
-63) 9 (2-60) -63)
10 (2-36) 13 (6-29) 10 (2-36)
13 (4-243) 13 (5-243) 12 (4-58)
A ** A ** A ** B
Atypia in previous biopsies ~ All patients ~ Tumour patients ~ Non-tumour patients
34 (14%) 10 (29%) 24 (71%)
14 (22%) 4 (29%) 10 (71%)
14 (21%) 6 (43%) 8 (57%)
A B A B
HGPIN in previous biopsies ~ All patients ~ Tumour patients ~ Non-tumour patients
12 (5%) 4 (33%) 8 (66%)
7 (11%) 2 (29%) 5 (71%)
3 (4%) 2 (67%) 1 (33%)
A B A B
90
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

2nd TRUS-GB 3rd TRUS-GB MR-GB Signif. p-val. PSA Subgroups ~ PSA < 4 ng/ml
Total patients Tumour patients
~ PSA 4 – 10 ng/ml Total patients Tumour patients
– Total patients Tumour patients
~ – Total patients Tumour patients
~ Total patients Tumour patients
22 4 (18%) 142 29 (20%) 45 8 (18%) 16 4 (25%) 23 10 (43%)
4 0 (0%) 28 4 (11%) 20 1 (5%) 6 2 (33%) 7 3 (43%)
0 - 21 10 (48%) 17 11 (65%) 14 11 (79%) 16 8 (50%)
A ** B ** A** B ** A ** B ** A B
Prostate Volumes ~ Median prostate volume
Total
Tumour patients
~ < 30 cc Total patients Tumour patients
– 50 cc Total patients Tumour patients
– 65 cc Total patients Tumour patients
Total patients Tumour patients
# 58 (15-201) 42 (15-160) 31 9 (29%) 67 21 (31%) 50 10 (20%) 96 14 (14%)
## 61 (17-212 30 (17-94) 7 5 (71%) 14 1 (7%) 15 1 (7%) 27 2 (7%)
48 (12-152) 42 (12-83) 14 14 (100%) 21 15 (71%) 14 7 (50%) 19 5 (26%)
A B ** A B A ** B ** A ** B ** A ** B ** A B
PSA Density ~ Median PSA density (range)
Total
Tumour patients
Total patients Tumour patients
– Total patients Tumour patients
– Total patients Tumour patients
Total patients Tumour patients
# 0 - - 138 19 (14%) 68 17 (25%) 28 11 (39%) 10 7 (70%)
## - - 32 2 (6%) 20 2 (20%) 6 1 (17%) 5 4 (80%)
- - 12 2 (17%) 23 13 (57%) 17 12 (71%) 16 13 (81%)
< 0.01A ** 0.01B ** 0.02A ** 0.69B
A B A **
B ** A ** B ** A B
91
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

Table 2. Comparison between TRUS-GB and MR-GB populations - tumour detection rates
a different PSA levels, prostate volumes and PSADs. (Statistical significance is calculated
for MR-GB vs. each TRUS-GB population seperately; A denotes MR-GB vs. 2nd session
TRUS-GB and B MR-GB vs. 3rd session TRUS-GB; N.A Not applicable; ** Statistically
Significant; # - in 4 patients no prostate volume obtained; ## - in 2 patients no prostate
volume obtained)
The principal tumour location was the most ventral aspect of the transition zone (TZ) in 57%
(26/46), followed by the paramedian region of the peripheral zone (PZ) in 20% (9/46) and
anterior horns of the PZ in 11% (5/46) (Figure 1). Figure 5 shows the MR images of a patient in
whom tumour was detected with MR-GB.
Figure 1. Schematic presentation of the prevalence of the 46 different tumour positive
TSRs (for 9 biopsies, two adjacent regions were both positive giving 55 tumour maps)
within the prostate as detected with MR-GB. The prostate was divided into 5 cranial-
caudal segments equating to a) apex b) apex-mid c) mid d) mid-base and e) basal level.
R=Right; L=Left; VT=Ventral Transition zone; MT=Middle Transition zone; DT=Dorsal
Transition zone; AH=Anterior Horn of peripheral zone; DL=Dorsolateral peripheral zone;
D=Dorsal peripheral zone.
92
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

From our reference database, 248 patients were identified with at least 2 TRUS-GB sessions and
65 patients with 3 sessions. No MR imaging was performed prior to biopsy in these subjects and
biopsies were performed on a systematic basis only. The overall tumour DR at the second and
third biopsy sessions were 22% (55/248) and 15% (10/65) respectively. The comparison of
tumour DR for TRUS-GB and MR-GB subgroups, stratified according to PSA, prostate volume and
PSAD are given in Table 2. MR-GB achieved significantly higher tumour DRs for all PSA
ts with a
PSA >20 ng/l (Figure 2), prostate volumes >65 cc (Figure 3 l/cc and
), where superior results were evident but not significant (p > 0.05).
One self-limiting transurethral hemorrhage and one uncomplicated urinary tract infection were
the only procedure related complications.
Figure 2. Tumour detection rates (%) in different PSA subgroups, at 2nd, 3rd TRUS-GB and
MR-GB session.
93
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

Figure 3. Tumour detection rates (%) in different prostate volume subgroups, at 2nd, 3rd
TRUS-GB session and MR-GB session.
Figure 4. Tumour detection rates (%) in different prostate PSA density subgroups, at 2nd,
3rd TRUS-GB session and MR-GB session (PSA density values in ng/ml/cc).
94
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

DISCUSSION
By using state-of-the-art multi-modality 3T MRI for tumour localization, we have shown that a
definite diagnosis of prostate cancer could be made in 59% (40/68) of patients in whom
repetitive prostate biopsies remained negative, but continuous concern regarding the presence
of cancer was evident. Ninety-three percent (37/40) of patients diagnosed with prostate cancer
were considered to harbor CSD. It is therefore justifiable to deduce, that MRI of the prostate
accurately portrays the locations of tumours, and thus offers urologists a method to improve
their biopsy outcomes. As MR-GB is limited by the restricted general availability, other methods
of MRI targeted biopsy techniques, such as MR-TRUS fusion(15) during TRUS biopsies, could be
considered. Nevertheless, MR-GB is probably the most accurate technique, because translation
of the TSR to another imaging modality is not required.
For comparison, we selected a TRUS-GB population from our institution which was clinically
matched for: age, prevalence of atypia in previous biopsies, PSA, prostate volume and PSAD. We
also determined the tumour DR for each subgroup. Most literature reporting on extended
schemes of 8-12 cores detect cancer in around 10-17%(16-18) of patients at second biopsy. The
overall tumour detection rate of 22% at the second and 15% at third TRUS-GB session in our
institution is therefore in agreement with reported data.
As different PSA values can predict the likelihood of finding tumour and constitutes a bias for
comparison, patients were substratified according to different PSA levels. Our study shows that
the MR-GB DR is superior (p< 01) to the repeat TRUS-GB sessions in all PSA subgroups except
in the very high PSA of >20 ng/ml group, where a similar DR was achieved (50% vs. 43%).
Prostatic volume constitutes another important factor that plays a role in the tumour detection
rate achieved by different biopsy protocols. In previous series it appears that 8-cores are
appropriate in patients with prostates <30 cc, whereas 10-12 cores are needed in 30-50 cc sized
prostates and >12-cores in large prostates of >50 cc(19). For all prostate volume groups, MR-GB
significantly outperformed TRUS-GB in tumour detection , except in excessively large
prostates of >65 cc, where similar rates were achieved.
In patients with tumour, a 15 ng/ml/cc is considered a good prognostic feature, with
low rates of progression(13). MR-GB did not achieve significant detection improvements over
TRUS-GB in this subset of patients with probable insignificant disease. On the contrary, in the
50 ng/ml/cc, tumours are likely to have a larger volume and therefore more
easily diagnosed with TRUS-GB.
95
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

Figure 5. Endorectal coil 3T MR images of a 64 yr old male with 4 previous negative
TRUS-GB (incl. 2 x 8-, 10-, 12-core) and a PSA of 18 ng/ml. T2-weighted axial (a) and
coronal (b) images show a low signal intensity lesions in the ventral portion of the apex.
This area also shows restriction on the ADC map (c) as well as a high Ktrans on DCE-MRI
(d). Axial (e) T2-w TRUE-FISP images during the MR-GB session, showing the needle
guider directed towards the TSR. Histopathological analysis of the biopsy cores, revealed
an adenocarcinoma with GS 4+3=7. Subsequent pelvic lymph node dissection revealed
metastatic disease.
96
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

In case of negative TRUS-GBs, radical measures involving saturation biopsies of 24-64 cores
have been advocated, with reported detection rates of between 18-34%(20;21) at second
session. No widespread application and acceptance of this technique by urologists exist with
conflicting results having been published(22;23). Moreover, saturation biopsies do appear to
offer a method of increasing tumour detection in high-risk patients however the additional use
of analgesia/anaesthesia, the higher incidence of side-effects and the high cost of processing the
large amount of pathological material are the biggest drawbacks of these techniques. As our
study has shown that MR-GB has a high tumour detection yield, requiring a very low number of
cores (median 4), this method could offer a very appealing alternative to the patient, urologist
and pathologist alike.
Whether MR-GB of the prostate detects a substantial proportion of potentially insignificant
tumours, is a very legitimate question. It stands to reason that a higher sensitivity for detecting
tumours implies a higher chance of finding tumours that do not need treatment, so called
clinically insignificant cancers. For prostate cancer the discussion on overtreatment of these
tumours remains a controversial issue(24). The concept of ‘insignificant’ prostate cancer, based
on tumour size and favourable pathological characteristics, was proposed in the 1990’s(25), and
the clinical criteria for predicting such tumours were 10 ng/ml, GS
pT2 and tumour 5 cc(11;12;26).
According to prostatectomy series, the predominant location of tumours, is the peripheral zone
in almost 70% of cases(27). Therefore, current systematic biopsy schemes extensively sample
the peripheral zone and thus the dorsal region of the prostate. In contrast, 68% (31/46) of
tumours in our series were very anteriorly located, 57% ( 26/46) in the ventral TZ and 11%
(5/46) in the anterior horns of the PZ. This may be the explanation within our group of patients
for having previous negative biopsies.
The current literature on MR guided biopsies of the prostate(28-30) is sparse and the few
reports currently available included small numbers of patients, had excessively long imaging and
biopsy times, and reported only on the use of conventional T2-weighted MR imaging to
determine TSRs for MR-GB after one previous negative TRUS biopsy.
Limitations of the current study relate principally to the fact that a direct comparison of our
results to other literature could not be made. This was because of differences in PSA values,
prostatic volumes, the number of previous biopsies as well as the biopsy schemes used during
the initial sessions. A prospective randomized trial would have appeared superior. However to
determine the potential benefit, we compared our study patient cohort with our own
97
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

institutional database, selecting similar patients but with TRUS guided multiple biopsies and
sub-grouped according to PSA, prostate volume and PSAD. Since our institution is a referral
hospital, the MR-GB patients had very heterogeneous previous biopsy protocols, with the
highest number of cores per biopsies session, ranging from 8-, 9-, 10-, 12- , 18 core and even
saturation biopsies. Patients that were selected for inclusion based on PSA of >10 ng/ml, can
represent a selection bias in relation to determining clinical significance of the detected
tumours.
CONCLUSIONS
In conclusion this study most importantly indicates that MRI is a highly effective method for the
detection and localization of clinically significant prostate cancer. As we have shown that guided
biopsies towards TSRs on MRI, detect clinically significant tumour in a substantial portion of
patients, MRI should be considered essential in any workup protocol of patients who are
suspected of harboring malignancy but who have successive negative biopsies. Secondly, this
study also concludes that MR-GB directed towards TSRs on m-m MRI is a very useful method of
accurately validating correct sampling of suspicious prostatic tissue. Because of the low
numbers of cores needed, MR-GB appears an appealing alternative to procedures such as
saturation biopsies. Finally we have shown that tumours detected were mostly located in areas
not explicitly sampled by routine schemes. Future studies for tumour DR using MR-TRUS fusion
during TRUS-GB incl. saturation targeting of suspicious areas, transperineal sampling of the
anterior prostate or changing locations for sampling under TRUS-GB in repeat sessions patients,
are needed and ideally should be compared to an MRI directed MR-GB technique.
98
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

REFERENCES
1. Umbehr M, Bachmann LM, Held U, Kessler TM, Sulser T, Weishaupt D, Kurhanewicz J, Steurer J. Combined Magnetic Resonance Imaging and Magnetic Resonance Spectroscopy Imaging in the Diagnosis of Prostate Cancer: A Systematic Review and Meta-analysis. Eur.Urol. 2008 Oct 18.
2. Heijmink SW, Futterer JJ, Hambrock T, Takahashi S, Scheenen TW, Huisman HJ, Hulsbergen-Van de Kaa CA, Knipscheer BC, Kiemeney LA, Witjes JA, et al. Prostate cancer: body-array versus endorectal coil MR imaging at 3 T--comparison of image quality, localization, and staging performance. Radiology 2007 Jul;244(1):184-95.
3. Tanimoto A, Nakashima J, Kohno H, Shinmoto H, Kuribayashi S. Prostate cancer screening: the clinical value of diffusion-weighted imaging and dynamic MR imaging in combination with T2-weighted imaging. J.Magn Reson.Imaging 2007 Jan;25(1):146-52.
4. Halpern EJ, Strup SE. Using gray-scale and color and power Doppler sonography to detect prostatic cancer. AJR Am.J.Roentgenol. 2000 Mar;174(3):623-7.
5. Mitterberger M, Pinggera GM, Horninger W, Bartsch G, Strasser H, Schafer G, Brunner A, Halpern EJ, Gradl J, Pallwein L, et al. Comparison of contrast enhanced color Doppler targeted biopsy to conventional systematic biopsy: impact on Gleason score. J.Urol. 2007 Aug;178(2):464-8.
6. Pelzer A, Bektic J, Berger AP, Pallwein L, Halpern EJ, Horninger W, Bartsch G, Frauscher F. Prostate cancer detection in men with prostate specific antigen 4 to 10 ng/ml using a combined approach of contrast enhanced color Doppler targeted and systematic biopsy. J.Urol. 2005 Jun;173(6):1926-9.
7. Huisman HJ, Engelbrecht MR, Barentsz JO. Accurate estimation of pharmacokinetic contrast-enhanced dynamic MRI parameters of the prostate. J.Magn Reson.Imaging 2001 Apr;13(4):607-14.
8. Akin O, Sala E, Moskowitz CS, Kuroiwa K, Ishill NM, Pucar D, Scardino PT, Hricak H. Transition zone prostate cancers: features, detection, localization, and staging at endorectal MR imaging. Radiology 2006 Jun;239(3):784-92.
9. Futterer JJ, Heijmink SW, Scheenen TW, Veltman J, Huisman HJ, Vos P, Hulsbergen-Van de Kaa CA, Witjes JA, Krabbe PF, Heerschap A, et al. Prostate cancer localization with dynamic contrast-enhanced MR imaging and proton MR spectroscopic imaging. Radiology 2006 Nov;241(2):449-58.
10. Hambrock T, Futterer JJ, Huisman HJ, Hulsbergen-vandeKaa C, van Basten JP, van O, I, Witjes JA, Barentsz JO. Thirty-two-channel coil 3T magnetic resonance-guided biopsies of prostate tumour suspicious regions identified on multimodality 3T magnetic resonance imaging: technique and feasibility. Invest Radiol. 2008 Oct;43(10):686-94.
11. Augustin H, Hammerer PG, Graefen M, Erbersdobler A, Blonski J, Palisaar J, Daghofer F, Huland H. Insignificant prostate cancer in radical prostatectomy specimen: time trends and preoperative prediction. Eur.Urol. 2003 May;43(5):455-60.
12. Bastian PJ, Mangold LA, Epstein JI, Partin AW. Characteristics of insignificant clinical T1c prostate tumours. A contemporary analysis. Cancer 2004 Nov 1;101(9):2001-5.
13. Nakanishi H, Wang X, Ochiai A, Trpkov K, Yilmaz A, Donnelly JB, Davis JW, Troncoso P, Babaian RJ. A nomogram for predicting low-volume/low-grade prostate cancer: a tool in selecting patients for active surveillance. Cancer 2007 Dec 1;110(11):2441-7.
14. Ochiai A, Troncoso P, Babaian RJ. The relationship between serum prostate specific antigen level and tumour volume persists in the current era. J.Urol. 2007 Mar;177(3):903-6.
15. Xu S, Kruecker J, Turkbey B, Glossop N, Singh AK, Choyke P, Pinto P, Wood BJ. Real-time MRI-TRUS fusion for guidance of targeted prostate biopsies. Comput.Aided Surg. 2008 Sep;13(5):255-64.
16. Mian BM, Naya Y, Okihara K, Vakar-Lopez F, Troncoso P, Babaian RJ. Predictors of cancer in repeat extended multisite prostate biopsy in men with previous negative extended multisite biopsy. Urology 2002 Nov;60(5):836-40.
17. Philip J, Hanchanale V, Foster CS, Javle P. Importance of peripheral biopsies in maximising the detection of early prostate cancer in repeat 12-core biopsy protocols. BJU.Int. 2006 Sep;98(3):559-62.
18. Roehl KA, Antenor JA, Catalona WJ. Serial biopsy results in prostate cancer screening study. J.Urol. 2002 Jun;167(6):2435-9.
19. Eskicorapci SY, Guliyev F, Akdogan B, Dogan HS, Ergen A, Ozen H. Individualization of the biopsy protocol according to the prostate gland volume for prostate cancer detection. J.Urol. 2005 May;173(5):1536-40.
20. Campos-Fernandes JL, Bastien L, Nicolaiew N, Robert G, Terry S, Vacherot F, Salomon L, Allory Y, Vordos D, Hoznek A, et al. Prostate Cancer Detection Rate in Patients with Repeated Extended 21-Sample Needle Biopsy. Eur.Urol. 2008 Jun 23.
21. Pepe P, Aragona F. Saturation prostate needle biopsy and prostate cancer detection at initial and repeat evaluation. Urology 2007 Dec;70(6):1131-5.
99
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

22. Stav K, Leibovici D, Sandbank J, Lindner A, Zisman A. Saturation prostate biopsy in high risk patients after
multiple previous negative biopsies. Urology 2008 Mar;71(3):399-403.
23. Walz J, Graefen M, Chun FK, Erbersdobler A, Haese A, Steuber T, Schlomm T, Huland H, Karakiewicz PI. High incidence of prostate cancer detected by saturation biopsy after previous negative biopsy series. Eur.Urol. 2006 Sep;50(3):498-505.
24. Taylor JA, III, Gancarczyk KJ, Fant GV, McLeod DG. Increasing the number of core samples taken at prostate needle biopsy enhances the detection of clinically significant prostate cancer. Urology 2002 Nov;60(5):841-5.
25. Dugan JA, Bostwick DG, Myers RP, Qian J, Bergstralh EJ, Oesterling JE. The definition and preoperative prediction of clinically insignificant prostate cancer. JAMA 1996 Jan 24;275(4):288-94.
26. Miyake H, Sakai I, Harada K, Hara I, Eto H. Prediction of potentially insignificant prostate cancer in men undergoing radical prostatectomy for clinically organ-confined disease. Int.J.Urol. 2005 Mar;12(3):270-4.
27. Sakai I, Harada K, Hara I, Eto H, Miyake H. A comparison of the biological features between prostate cancers arising in the transition and peripheral zones. BJU.Int. 2005 Sep;96(4):528-32.
28. Anastasiadis AG, Lichy MP, Nagele U, Kuczyk MA, Merseburger AS, Hennenlotter J, Corvin S, Sievert KD, Claussen CD, Stenzl A, et al. MRI-guided biopsy of the prostate increases diagnostic performance in men with elevated or increasing PSA levels after previous negative TRUS biopsies. Eur.Urol. 2006 Oct;50(4):738-48.
29. Beyersdorff D, Winkel A, Hamm B, Lenk S, Loening SA, Taupitz M. MR imaging-guided prostate biopsy with a closed MR unit at 1.5 T: initial results. Radiology 2005 Feb;234(2):576-81.
30. Engelhard K, Hollenbach HP, Kiefer B, Winkel A, Goeb K, Engehausen D. Prostate biopsy in the supine position in a standard 1.5-T scanner under real time MR-imaging control using a MR-compatible endorectal biopsy device. Eur.Radiol. 2006 Jun;16(6):1237-43.
100
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4

22. Stav K, Leibovici D, Sandbank J, Lindner A, Zisman A. Saturation prostate biopsy in high risk patients after
multiple previous negative biopsies. Urology 2008 Mar;71(3):399-403.
23. Walz J, Graefen M, Chun FK, Erbersdobler A, Haese A, Steuber T, Schlomm T, Huland H, Karakiewicz PI. High incidence of prostate cancer detected by saturation biopsy after previous negative biopsy series. Eur.Urol. 2006 Sep;50(3):498-505.
24. Taylor JA, III, Gancarczyk KJ, Fant GV, McLeod DG. Increasing the number of core samples taken at prostate needle biopsy enhances the detection of clinically significant prostate cancer. Urology 2002 Nov;60(5):841-5.
25. Dugan JA, Bostwick DG, Myers RP, Qian J, Bergstralh EJ, Oesterling JE. The definition and preoperative prediction of clinically insignificant prostate cancer. JAMA 1996 Jan 24;275(4):288-94.
26. Miyake H, Sakai I, Harada K, Hara I, Eto H. Prediction of potentially insignificant prostate cancer in men undergoing radical prostatectomy for clinically organ-confined disease. Int.J.Urol. 2005 Mar;12(3):270-4.
27. Sakai I, Harada K, Hara I, Eto H, Miyake H. A comparison of the biological features between prostate cancers arising in the transition and peripheral zones. BJU.Int. 2005 Sep;96(4):528-32.
28. Anastasiadis AG, Lichy MP, Nagele U, Kuczyk MA, Merseburger AS, Hennenlotter J, Corvin S, Sievert KD, Claussen CD, Stenzl A, et al. MRI-guided biopsy of the prostate increases diagnostic performance in men with elevated or increasing PSA levels after previous negative TRUS biopsies. Eur.Urol. 2006 Oct;50(4):738-48.
29. Beyersdorff D, Winkel A, Hamm B, Lenk S, Loening SA, Taupitz M. MR imaging-guided prostate biopsy with a closed MR unit at 1.5 T: initial results. Radiology 2005 Feb;234(2):576-81.
30. Engelhard K, Hollenbach HP, Kiefer B, Winkel A, Goeb K, Engehausen D. Prostate biopsy in the supine position in a standard 1.5-T scanner under real time MR-imaging control using a MR-compatible endorectal biopsy device. Eur.Radiol. 2006 Jun;16(6):1237-43.
100
MRI Guided Prostate Biopsies in Men with Repetitive Negative Biopsies and Elevated PSA
4


— CHAPTER 5 —
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation
Therapy
D. Yakar; T. Hambrock; H. Huisman et al.
CHAPTER 5CHAPTER 5

Feasibility of 3 Tesla Dynamic Contrast Enhanced Magnetic Resonance Guided Biopsy in Localizing Local Prostate Cancer Recurrence after
Radiation Therapy
Investigative Radiology 2010 Mar; 45(3):121-5
Yakar D, Hambrock T, Huisman H, Hulsbergen-vandeKaa CA, van Lin E, Vergunst H, Hoeks CM, van Oort IM, Witjes JA, Barentsz JO, Fütterer JJ
Young Investigators Award European Society for Urogential Radiology, München,
2008 (Derya Yakar)
Advances in Knowledge
Dynamic contrast enhanced MR imaging is a very accurate method in detecting prostate
cancer recurrence following external beam radiotherapy.
It is feasible to perform MR guided biopsies of patients with abnormal MRI after
radiotherapy to make a definite diagnosis of local recurrence.
Implications for Patient Care
In patients with elevated PSA following external radiotherapy, DCE-MRI can play an
important role in diagnosing local recurrence and therefore guide therapy for systemic
vs. local therapy.
Summary Statement
3T DCE-MRI followed by MR guided biopsies is a feasible and useful technique for diagnosing local recurrence of prostate cancer following
external beam radiotherapy.
102
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation Therapy
5

ABSTRACT
Objectives: The objective of this study was to assess the feasibility of the combination of
magnetic resonance (MR)-guided biopsy (MRGB) and diagnostic 3T MR imaging in the
localization of local recurrence of prostate cancer (PCa) after external beam radiation therapy
(EBRT).
Materials and Methods: Twenty-four consecutive men with biochemical failure suspected of
local recurrence after initial EBRT were enrolled prospectively in this study. All patients
underwent a diagnostic 3T MR examination of the prostate. T2-weighted and dynamic contrast-
enhanced MR images (DCE-MRI) were acquired. Two radiologists evaluated the MR images in
consensus for tumour suspicious regions (TSRs) for local recurrence. Subsequently, these TSRs
were biopsied under MR-guidance and histopathologically evaluated for the presence of
recurrent PCa. Descriptive statistical analysis was applied.
Results: Tissue sampling was successful in all patients and all TSRs. The positive predictive
value on a per patient basis was 75% (15/20) and on a per TSR basis 68% (26/38). The median
number of biopsies taken per patient was 3, and the duration of an MRGB session was 31
minutes. No intervention-related complications occurred.
Conclusions: The combination of MRGB and diagnostic MR imaging of the prostate was a
feasible technique to localize PCa recurrence after EBRT using a low number of cores in a
clinically acceptable time.
103
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation Therapy
5

INTRODUCTION
Approximately 30% of the patients diagnosed with prostate cancer (PCa) are treated with
external beam radiation therapy (EBRT) as initial definitive treatment (1). Of these patients,
20% to 60% develop biochemical failure (2). Biochemical failure is considered to represent
cancer recurrence (3) and correlates well with clinical progression as evidenced by local clinical
control rates after 5 years in patients with and without biochemical failure of 86% and 99%,
respectively (4).
The diagnosis of recurrent PCa entails a prostate-specific antigen (PSA) test, digital rectal
examination (DRE), transrectal ultrasound (TRUS)-guided prostate biopsy, and a bone scan.
However, each of these diagnostic tools has definite shortcomings (5). The PSA nadir, PSA half-
life, time interval from treatment to PSA nadir, and PSA doubling time are all associated with
both clinical and biochemical failure (6). Yet, there is no absolute cut-off value to accurately
discriminate on an individual basis, between local recurrence and distant metastases (7).
Diagnosing local recurrence after EBRT by DRE is challenging because of radiation-induced
fibrosis and shrinkage of the prostate, whereas the sensitivity and specificity of TRUS after
radiotherapy were found to be 49% and 57%, respectively (8). Magnetic resonance (MR)
imaging of the prostate is a well established modality for accurately localizing PCa. Evaluation of
the radiated prostate gland is restricted because of treatment-induced changes, resulting in
homogeneously low signal on T2-w images (9,10). Hence, MR imaging of the prostate after EBRT
is much more challenging.
Functional imaging techniques, like dynamic contrast enhanced MR imaging (DCE-MRI)(11,12),
diffusion-weighted imaging, and proton MR spectroscopy, can improve the accuracy of localizing
recurrence after EBRT (13–15). This diagnostic information can be used for directing biopsies to
tumour suspicious regions (TSRs). Thus far, TRUS is the most widely used imaging modality, and
systematic sextant TRUS-guided biopsy is considered as the gold standard for histologic
assessment of a local recurrence, with a positive predictive value (PPV) of only 27% (8).
However, this may be improved by DCE-MRI with a PPV of 46% to 78% (11,12). To our
knowledge, there are no studies available on 3T MR-guided biopsy (MRGB) in the localization of
local recurrence of PCa after EBRT.
The purpose of our study was to assess the feasibility of the combination of MRGB and
diagnostic 3T MR imaging in the localization of local recurrence of PCa after EBRT.
104
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation Therapy
5

MATERIALS AND METHODS
Patients
This study was approved by the ethics review board of our institution, and informed consent
was obtained. From October 2006 to March 2009, 24 consecutive patients (median age, 70
years; range, 60–83) with biochemical failure (using the ASTRO definition of 3 consecutive rises
in PSA after reaching PSA nadir) after initial EBRT were enrolled in this prospective study.
Patients were referred for MR imaging of the prostate followed by MRGB. Exclusion criteria
were contraindications to MR imaging (eg, cardiac pacemakers, intracranial clips). The pre- and
postradiotherapy characteristics are given in Table 1.
Median age (yr) 70 (60-83)
Preradiotherapy stage
T1
T2
T3
3
4
13
Median preradiotherapy Gleason Score 7 (5-9) 2
Median preradiotherapy PSA (ng/ml) 15.6 (6.1-96.0) 1
Median radiation therapy dose (Gy) 67.5 (66.0-78) 3
No. patients who received hormonal therapy 15
Median PSA nadir (ng/ml) 0.26 (0.0-6.3)
Median PSA (ng/ml) prior to MRI 4.4 (1.1-13.4)
Median time (wk) between MRI and MR biopsy 4.1 (1.3-10.0)
Table 1. The pre- and postradiotherapy characteristics of the patients
MR Imaging Protocol
MR imaging of the prostate was performed using a 3T MR scanner (Siemens Trio Tim, Erlangen,
Germany) with the use of a phased array coil. The ERC was inserted and filled with either a 40
ml perfluorocarbon or water preparation (FOMBLIN, Solvay-Solexis, Milan, Italy). Peristalsis was
suppressed with an intravenous injection of 20 mg butylscopolamine bromide (BUSCOPAN,
Boehringer-Ingelheim, Ingelheim, Germany), intramuscular injection of 20 mg
butylscopolaminebromide and 1 mg of glucagon (GLUCAGEN, Nordisk, Gentofte, Denmark).
105
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation Therapy
5

The imaging protocol included the following sequences: T2-weighted turbo spin echo sequences
were acquired (TR 4260 milliseconds/ TE 99 milliseconds; flip angle, 120; 3 mm slice thickness;
echo train length, 15; 180x90 mm field of view, and 448x448 matrix; voxel size, 0.4x0.4x 3 mm)
in axial, coronal, and sagittal planes. A 3-dimensional (3D) T1-weighted gradient echo sequence
(TR 4.90 milliseconds/TE 2.45 milliseconds; flip angle, 10; 176 slices per 3D slab; 0.9 mm slice
thickness; 288 x 288 field of view and 320 x 320 matrix; voxel size 0.9 mm x 0.9 mm x 0.9 mm)
was used to assess lymph node and skeletal status. Finally, an axial 3D T1-weighted gradient
echo sequence (TR 800 milliseconds/TE 1.47 milliseconds; flip angle, 14; 3 mm slice thickness;
field of view 230 x 230 and 128 x 128 matrix; voxel size 1.8 mm x 1.8 mm x 3 mm) was used to
obtain proton-density images, with the same positioning angle and center as the axial T2-
weighted sequence (to allow calculation of the relative gadolinium chelate concentration
curves), followed by 3D T1-weighted spoiled gradient-echo images (TR 38 milliseconds/TE 1.35
milliseconds; flip angle, 14; 10 transverse partitions on a 3D slab; 3 mm section thickness; 230 x
230 mm field of view; 128 x 128 matrix; voxel size 1.8 x 1.8 x 3 mm; GRAPPA parallel imaging
factor 2; 2.5s temporal resolution; and 2 minutes 30 seconds acquisition time) acquired during
an intravenous bolus injection of a paramagnetic gadolinium chelate— 0.1 mmol of
gadopentetate dimeglumine (DOTAREM, Guerbet, Paris, France) per kilogram of body weight.
This was administered with a power injector (Spectris; Medrad) at 2.5 ml/s and followed by a
20-mL saline flush.
MR Data Analysis
The prostate images of all patients were read in consensus by 2 radiologists with respectively 2
and 5 years of experience in prostate MR imaging. Functional dynamic imaging parameters were
estimated from a fitted general bi-exponential signal intensity model for each MR signal
enhancement–time curve, as described previously (16,17). The pharmacokinetic parameters
(Ktrans, Ve, Kep, and WashOut) were computed using the standard 2-compartment model (18)
and the arterial input function was estimated using the reference tissue method (19) and
automated per-patient calibration (20). Finally, these parameters were projected as color
overlay maps over the T2-weighted images.
This patented procedure (21) for calculating pharmacokinetic parameters is being used in
multiple centers. For the first 2 patients, lesions were identified as suspicious purely whether a
focally enhancing region with DCE-MRI was seen irrespective of the degree of enhancement. To
determine whether regions enhancing in the prostate were representing tumour, we applied a
lesion directed biopsy approach. To establish a “cut-off” in the color coding of the
106
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation Therapy
5

pharmacokinetic maps, we used the “normal” regions of these 2 patients as a cut-off for future
color coding. Above this “normal” threshold, radiologists then defined suspicious regions as
focally enhancing spots shown on the color maps.
The criterion for TSRs on DCE-MRI in the peripheral zone, the transition zone, and the seminal
vesicles was a cutoff value of 3.5 (/s) for Ktrans and -0.225 (AU) for washout. The criterion for
TSRs on T2-weighted MR images was a low signal-intensity region within the prostate. Per
patient, the T2-w images were evaluated for TSRs individually and in color overlay (DCE-MRI).
To locate the TSRs, the prostate was divided into 22 different axial and sagittal segments, to
make a 3D spatial position estimation of the identified TSRs which was used during the second
MRGB-session. A similar translation technique was described before by Hambrock et al. (22).
MR-Guided Biopsy
After the initial tumour localization MR examination (median time between biopsy and initial
localization MRI was 4.1 weeks; range, 1.3–10.0), patients underwent an MRGB using an MR-
compatible biopsy device (In vivo, Schwerin, Germany) at 3T. All patients received oral
ciprofloxacin 500 mg (CIPROXIN, Bayer, Leverkusen, Germany) the evening before, in the
morning of the biopsy, and 6 hours after biopsy.
Relocation of the TSRs (by using the 3D spatial position estimation) determined during the first
MR imaging localization was done by obtaining T2-weighted anatomic images in the axial
direction. Prostate biopsies were performed with the patient in prone position, and a needle
guider inserted rectally, which was attached to the arm of the biopsy device. The needle guider
was pointed toward the TSR before obtaining the biopsy specimen (22). All biopsies were
supervised by one experienced radiologist (4 years of experience) with MRGB of the prostate.
Histopathology
Samples were subsequently processed by a routine fixation in 10% buffered formalin, embedded
in paraffin, stained with hematoxylin-eosin, before being evaluated by an experienced
genitourinary pathologist (18 years experience of PCa histopathology) for the presence of
tumour. The biopsies were classified as negative if there was no evidence of carcinoma or
residual indeterminate carcinoma with severe treatment effect, defined as isolated tumour cells
or poorly formed glands with abundant clear or vacuolated cytoplasm. All positive biopsies were
assigned a Gleason score.
107
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation Therapy
5

Statistical Analysis
Descriptive statistical analysis was applied. The positive predictive value of TSRs seen on MR
images was calculated. The patient characteristics were calculated by using SPSS 16.0
RESULTS
Three patients with contraindications to an ERC (e.g., anorectal surgery, inflammatory bowel
disease) were scanned with a pelvic phased-array coil only. Metastatic disease was evident on
MR imaging in 4 of 24 patients. One patient had multiple low signal intensity areas in the left
iliac and sacral bone and multiple enlarged lymph nodes (diameter greater than 10 mm) next to
the right internal iliac artery. Two patients had multiple enlarged lymph nodes next to the right
internal iliac artery. One patient had multiple areas with focal low signal intensities in the body
of L4, the right acetabulum, and in the right anterior superior iliac spine. These patients received
hormonal therapy and were excluded in the further analysis.
In the remaining 20 patients, a total of 38 TSRs were identified on combined T2-weighted and
DCE-MRI and subsequently biopsied with MRGB. All TSRs that were identified on T2-weighted
imaging were also identified on DCE-MRI. With DCE-MRI 8 TSRs, in 5 patients, were identified
that were not identified on T2-weighted imaging. One patient had a hyperintense region
compared with uninvolved prostate tissue as TSR on T2-weighted MR imaging and increased
permeability on DCE-MRI (Fig. 1), which turned out to be recurrent PCa on histologic
examination.
Median MRGB time was 31 minutes (range, 18–47) per patient and a median of 3 biopsy cores
per patient (range, 2–5) was obtained. Median number of biopsies per TSR was 2 (range, 1–4).
The MRGBs were tolerated well and no procedure-related complications occurred. Tissue
sampling was successful in all patients and TSRs.
Histologically proven local recurrence was evident in 15 patients (Fig. 2). These patients were
either treated with salvage cryosurgery (5 patients), salvage prostatectomy (1 patient), wait and
see (1 patient), hormonal therapy (2 patients), were lost to follow-up (4 patients), or died (2
patients). Of the 38 different TSRs identified on MR imaging, 26 contained histologically proven
recurrence (68%), 8 revealed radiotherapy induced atypia in preexisting glands (21%), 1
contained residual indeterminate PCa with severe radiation changes (3%), and the remaining 3
contained fibrosis (8%).
108
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation Therapy
5

Figure 1. MR images obtained from a 70 year old man with a TSR seen in the right ventral
part in the midprostate, with a PSA of 0.4 ng/ml. The T2-weighted images showed a
hyperintense TSR in the right ventral part in the midprostate (arrow) (A), also on DCE-
MRI there was a TSR (high Ktrans) visible (arow) (B). During a second session, an MRGB
was performed, the needle guide was pointed toward the TSR in axial (TRUE-FISP image)
(C) plane, and subsequently biopsied. Histopathology revealed a Gleason 9 prostate
cancer recurrence.
The PPV of MRGB for detecting local recurrence on per patient basis and per TSR basis was 75%
(15/20) and 68% (26/38), respectively. There was no significant difference of the PPV when
peripheral, transition zone, and seminal vesicles were considered separate and also the use of a
pelvic phased-array coil only had no influence on these results. Gleason score 10 was present in
109
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation Therapy
5

2/26 (8%), Gleason score 9 in 8/26 (31%), Gleason score 8 in 3/26 (12%), Gleason score 7 in
9/26 (35%), and Gleason score 6 in 4/26 (15%) TSRs.
The site of recurrence within the prostate was present in the apical region in 6 of 26 TSRs, in the
apex-mid in 5, in the mid in 9, in the midbase in 3, in the base in 1, and in the seminal vesicle in 2
TSRs. The local recurrence was identified in the peripheral zone in 19 of 26 (73%) TSRs and in
the transition zone in 7 of 26 (27%) TSRs.
Of the 5 patients, 3 with negative histology received hormonal therapy, 1 underwent salvage
cryosurgery, and 1 underwent a follow-up MR examination. The patient with the follow-up MR
had unchanged MR findings in combination with a declining PSA (PSA during the first MR
examination was 6.4 ng/ml and during the follow-up MR imaging was 3.7 ng/ml).
DISCUSSION
Results of our study show that local recurrence after EBRT could be localized with the
combination of MRGB and diagnostic MR imaging in a substantial proportion of patients (PPV of
8% and 75% on a per TSR and a per patient basis, respectively). With a median intervention
time of 31 minutes, and no procedure-related complications, MRGB can be considered a feasible
method in localizing local PCa recurrence following EBRT.
MRGB was not able to assess the effect of false negatives, i.e., areas of prostate cancer which did
not enhance, because of the relative time-consuming character of this procedure. However,
previous studies that have used 6 core TRUS-guided biopsy as the standard of reference in
localizing radiation therapy recurrence, including from regions that did not enhance on DCE-
MRI, have shown that the negative predictive value of this technique is between 78% and 95%
(11,12). Undoubtedly, 6 core TRUS-guided biopsies have many limitations when used as the gold
standard (e.g., high false negatives and underestimating of true Gleason score), which probably
means that these negative predictive values of the above mentioned studies are somewhat
overrated.
Correlating DCE-MRI with radical prostatectomy samples would be the best option and should
be the next step in correlating recurrent disease seen on DCE-MRI. Nonetheless, when selecting
patients with prostate cancer recurrence the mostly followed treatment strategy is still some
form of whole-gland salvage therapy. Hence, false negatives are less of a problem. Merely
detecting a recurrence, rather than mapping the recurrent tumour, will suffice for this particular
110
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation Therapy
5

group of patients. Thus, only biopsying TSRs seen on DCE-MRI should be considered as an
advantage rather than a disadvantage of MRGB biopsies.
MRGB is capable of detecting a recurrence with only 3 biopsies per patient omitting TRUS biopsy
core schemes (with a PPV of 27%) that use between 6 and 12 cores per patient. Consequently, it
may lead to higher patient satisfaction. The main advantage of TRUS-guided biopsy over 3T DCE-
MRGB is that the expertise and the technique itself are more generally available in routine
clinical practice. Probably, performing MR-TRUS fusion for targeted biopsies by combining the
high spatial resolution of MR imaging with the wide-spread availability of TRUS is the most
optimal strategy as evidenced by promising results in 2 different studies (23,24).
However, MRGB has the advantage of being directed toward TSRs using the same imaging
modality used for localization. This way spatial misregistration between MR imaging and the
biopsy core can be reduced to a minimum, which probably makes it a more precise method.
Unfortunately, randomized controlled trials comparing MRGB, TRUS-guided biopsy, and MR-
TRUS fusion are not available yet. Future studies should focus on inclusion of a larger number of
patients and to improve the reproducibility of quantitative pharmacokinetic parameters (25) as
well as to limit the subjectiveness of reader evaluation, an automated per-patient arterial input
function estimation, which was shown in a recent publication to be superior to fixed input
models (20) is more preferred.
The widely known and accepted criterion for prostate cancer on T2-weighted MR imaging, a
region of low signal intensity, was used by us for localizing recurrence of PCa. It is interesting to
note that we had a specific case with a hyperintense region compared with surrounding prostate
tissue as a TSR, which was confirmed on histologic evaluation as PCa recurrence. This indicates
that after EBRT a recurrence can also have a hyperintense character, compared with
surrounding prostate tissue on T2-weighted MR imaging. Furthermore, future studies may
include other functional MR imaging techniques such as diffusion-weighted imaging26 and MR
spectroscopy in guiding MRGB after EBRT. This may lead to a higher detection rate with a
minimum number of biopsy cores.
111
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation Therapy
5

Figure 2. MR images obtained from a 68-year-old man with a TSR seen in the right
peripheral zone at the apex-mid, with a PSA of 2.1 ng/mL. The T2-weighted images
showed a diffuse low signal intensity of the entire prostate and no TSR was detectable (A);
however, on DCE-MRI, there was a TSR (high Ktrans) visible (arrow) (B). During a second
session, an MRGB was performed, by pointing the needle guider toward the TSR in axial
(TRUE-FISP image) (C), plane and subsequently biopsied. Histopathology revealed a
Gleason 7 prostate cancer recurrence.
Limitations of our study are related to the relatively small number of patients included and the
incomplete data concerning patient characteristics, which was due to patient referral from
outside our university hospital. In our study, we did not have any patient with a negative DCE-
MRI on local prostate level. In other words, each patient we imaged had at least one TSR in the
prostate detected with DCE-MRI. This can be interpreted as a selection bias. However, this is not
112
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation Therapy
5

surprising because of the inclusion criteria being 3 consecutive rises of PSA after reaching PSA
nadir.
Only 3 patients were examined without the use of an ERC. Because of the small number of this
group, no further conclusions can be drawn from this result. Because our current study is
prospective and no other studies exist on defining true pharmacokinetic cut-off values for the
irradiated prostate we had to base our cut-off values on the first 2 patients we imaged and
biopsied. Defining a cut-off for tumour is impossible with only 2 patients. These 2 were only
used to define a cut-off for “normal.” Above this “normal” threshold, radiologists then defined
suspicious regions as focally enhancing spots shown on the color maps. To define true
pharmacokinetic cut-off values for tumour versus benign enhancing spots versus normal in the
irradiated prostate is subjective of a future publication and can only be determined
retrospectively on a larger group of patients.
Salvage therapies can offer a possibility of cure in selected patients. This underlines the
importance to select the patients who would benefit from it carefully (27). Unfortunately, the
conventional methods for diagnostic workup of PCa recurrence (e.g., DRE, PSA, TRUS, bone scan)
all have their limitations. Therefore, there is a need for more accurate and versatile diagnostic
tools like MR imaging, which has the advantage that both local and distant prostatic disease can
be evaluated at the same time. Moreover, the addition of other functional MR imaging techniques
such as DWI can even possibly play a role in the assessment of tumour aggressiveness (28).
CONCLUSION
In conclusion, the combination of MRGB and diagnostic MR imaging of the prostate was a
feasible technique to localize PCa recurrence after EBRT using a low number of cores in a
clinically acceptable time.
113
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation Therapy
5

REFERENCES
1. Stanford JL, Stephenson RA, Coyle LM, et al. Prostate Cancer Trends 1973–1995, SEER Program. Bethesda, MD: National Cancer Institute; 1999.
2. D’Amico AV, Whittington R, Malkowicz SB, et al. Biochemical outcome after radical prostatectomy or external beam radiation therapy for patients with clinically localized prostate carcinoma in the prostate specific antigen era. Cancer. 2002;95:281–286.
3. Aus G, Abbou CC, Bolla M, et al. EAU guidelines on prostate cancer. Eur Urol. 2005;48:546 –551. 4. Horwitz EM, Vicini FA, Ziaja EL, et al; American Society of Therapeutic Radiology and Oncology. The correlation
between the ASTRO Consensus Panel definition of biochemical failure and clinical outcome for patients with prostate cancer treated with external beam irradiation. Int J Radiat Oncol Biol Phys. 1998;41:267–272.
5. Nudell DM, Wefer AE, et al. Imaging for recurrent prostate cancer. Radiol Clin North Am. 2000;38:213–229. 6. Kestin LL, Vicini FA, Ziaja EL, et al. Defining biochemical cure for prostate carcinoma patients treated with
external beam radiation therapy. Cancer. 1999;86:1557–1566. 7. Pound CR, Brawer MK, Partin AW. Evaluation and treatment of men with biochemical prostate-specific antigen
recurrence following definitive therapy for clinically localized prostate cancer. Rev Urol. 2001;3:72– 84. 8. Crook J, Robertson S, Collin G, et al. Clinical relevance of trans-rectal ultrasound, biopsy, and serum prostate-
specific antigen following external beam radiotherapy for carcinoma of the prostate. Int J Radiat Oncol Biol Phys. 1993;27:31–37.
9. Chan TW, Kressel HY. Prostate and seminal vesicles after irradiation: MR appearance. J Magn Reson Imaging. 1991;1:503–511.
10. Coakley FV, Hricak H, Wefer AE, et al. Brachytherapy for prostate cancer: endorectal MR imaging of local treatment-related changes. Radiology. 2001; 219:817– 821.
11. Rouviere O, Valette O, Grivolat S, et al. Recurrent prostate cancer after external beam radiotherapy: value of contrast-enhanced dynamic MRI in localizing intraprostatic tumour—correlation with biopsy findings. Urology. 2004;63:922–927.
12. Haider MA, Chung P, Sweet J, et al. Dynamic contrast-enhanced magnetic resonance imaging for localization of recurrent prostate cancer after external beam radiotherapy. Int J Radiat Oncol Biol Phys. 2008;70:425– 430.
13. Coakley FV, Teh HS, Qayyum A, et al. Endorectal MR imaging and MR spectroscopic imaging for locally recurrent prostate cancer after external beam radiation therapy: preliminary experience. Radiology. 2004;233:441–448.
14. Menard C, Smith IC, Somorjai RL, et al. Magnetic resonance spectroscopy of the malignant prostate gland after radiotherapy: a histopathologic study of diagnostic validity. Int J Radiat Oncol Biol Phys. 2001;50:317–323.
15. Kim CK, Park BK, Lee HM. Prediction of locally recurrent prostate cancer after radiation therapy: incremental value of 3T diffusion-weighted MRI. J Magn Reson Imaging. 2009;29:391–397.
16. Futterer JJ, Heijmink SW, Scheenen TW, et al. Prostate cancer localization with dynamic contrast-enhanced MR imaging and proton MR spectroscopic imaging. Radiology. 2006;241:449–458.
17. Huisman HJ, Engelbrecht MR, Barentsz JO. Accurate estimation of pharmacokinetic contrast-enhanced dynamic MRI parameters of the prostate. J Magn Reson Imaging. 2001;13:607– 614.
18. Tofts PS, Brix G, Buckley DL, et al. Estimating kinetic parameters from dynamic contrast-enhanced T(1)-weighted MRI of a diffusable tracer: standardized quantities and symbols. J Magn Reson Imaging. 1999;10:223
19. Kovar DA, Lewis M, Karczmar GS. A new method for imaging perfusion and contrast extraction fraction: input functions derived from reference tissues. J Magn Reson Imaging. 1998;8:1126 –1134.
20. Vos PC, Hambrock T, Barentsz JO, et al. Automated calibration for computerized analysis of prostate lesions using pharmacokinetic magnetic resonance images. In: Yang GZ, Hawkes DJ, Rueckert D, et al, eds. Medical Image Computing and Computer-Assisted Intervention MICCAI 2009. Part II, Volume 5761. Berlin, Germany: SpringerLink; 2009:836–843.
21. Huisman HJ, Karssemeijer N. Processing and displaying dynamic contrastenhanced MRI 2008 22. Hambrock T, Futterer JJ, Huisman HJ, et al. Thirty-two-channel coil 3T magnetic resonance-guided biopsies of
prostate tumour suspicious regions identified on multimodality 3T magnetic resonance imaging: technique and feasibility. Invest Radiol. 2008;43:686–694.
23. Kaplan I, Oldenburg NE, Meskell P, et al. Real time MRI-ultrasound image guided stereotactic prostate biopsy. Magn Reson Imaging. 2002;20:295–299.
24. Singh AK, Kruecker J, Xu S, et al. Initial clinical experience with real-time transrectal ultrasonography-magnetic resonance imaging fusion-guided prostate biopsy. BJU Int. 2008;101:841– 845.
25. Lowry M, Zelhof B, Liney GP, et al. Analysis of prostate DCE-MRI: comparison of fast exchange limit and fast exchange regimen pharmacokinetic models in the discrimination of malignant from normal tissue. Invest Radiol. 2009;44:577–584.
26. Kim CK, Park BK, Park W, et al. Prostate MR imaging at 3T using a phased-arrayed coil in predicting locally recurrent prostate cancer after radiation therapy: preliminary experience. Abdom Imaging. In press.
27. Stephenson AJ, Scardino PT, Bianco FJ, et al. Salvage therapy for locally recurrent prostate cancer after external beam radiotherapy. Curr Treat Options Oncol. 2004;5:357–365.
28. Gibbs P, Liney GP, Pickles MD, et al. Correlation of ADC and T2 measurements with cell density in prostate cancer at 3.0 Tesla. Invest Radiol. 2009;44:572–576.
114
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation Therapy
5

REFERENCES
1. Stanford JL, Stephenson RA, Coyle LM, et al. Prostate Cancer Trends 1973–1995, SEER Program. Bethesda, MD: National Cancer Institute; 1999.
2. D’Amico AV, Whittington R, Malkowicz SB, et al. Biochemical outcome after radical prostatectomy or external beam radiation therapy for patients with clinically localized prostate carcinoma in the prostate specific antigen era. Cancer. 2002;95:281–286.
3. Aus G, Abbou CC, Bolla M, et al. EAU guidelines on prostate cancer. Eur Urol. 2005;48:546 –551. 4. Horwitz EM, Vicini FA, Ziaja EL, et al; American Society of Therapeutic Radiology and Oncology. The correlation
between the ASTRO Consensus Panel definition of biochemical failure and clinical outcome for patients with prostate cancer treated with external beam irradiation. Int J Radiat Oncol Biol Phys. 1998;41:267–272.
5. Nudell DM, Wefer AE, et al. Imaging for recurrent prostate cancer. Radiol Clin North Am. 2000;38:213–229. 6. Kestin LL, Vicini FA, Ziaja EL, et al. Defining biochemical cure for prostate carcinoma patients treated with
external beam radiation therapy. Cancer. 1999;86:1557–1566. 7. Pound CR, Brawer MK, Partin AW. Evaluation and treatment of men with biochemical prostate-specific antigen
recurrence following definitive therapy for clinically localized prostate cancer. Rev Urol. 2001;3:72– 84. 8. Crook J, Robertson S, Collin G, et al. Clinical relevance of trans-rectal ultrasound, biopsy, and serum prostate-
specific antigen following external beam radiotherapy for carcinoma of the prostate. Int J Radiat Oncol Biol Phys. 1993;27:31–37.
9. Chan TW, Kressel HY. Prostate and seminal vesicles after irradiation: MR appearance. J Magn Reson Imaging. 1991;1:503–511.
10. Coakley FV, Hricak H, Wefer AE, et al. Brachytherapy for prostate cancer: endorectal MR imaging of local treatment-related changes. Radiology. 2001; 219:817– 821.
11. Rouviere O, Valette O, Grivolat S, et al. Recurrent prostate cancer after external beam radiotherapy: value of contrast-enhanced dynamic MRI in localizing intraprostatic tumour—correlation with biopsy findings. Urology. 2004;63:922–927.
12. Haider MA, Chung P, Sweet J, et al. Dynamic contrast-enhanced magnetic resonance imaging for localization of recurrent prostate cancer after external beam radiotherapy. Int J Radiat Oncol Biol Phys. 2008;70:425– 430.
13. Coakley FV, Teh HS, Qayyum A, et al. Endorectal MR imaging and MR spectroscopic imaging for locally recurrent prostate cancer after external beam radiation therapy: preliminary experience. Radiology. 2004;233:441–448.
14. Menard C, Smith IC, Somorjai RL, et al. Magnetic resonance spectroscopy of the malignant prostate gland after radiotherapy: a histopathologic study of diagnostic validity. Int J Radiat Oncol Biol Phys. 2001;50:317–323.
15. Kim CK, Park BK, Lee HM. Prediction of locally recurrent prostate cancer after radiation therapy: incremental value of 3T diffusion-weighted MRI. J Magn Reson Imaging. 2009;29:391–397.
16. Futterer JJ, Heijmink SW, Scheenen TW, et al. Prostate cancer localization with dynamic contrast-enhanced MR imaging and proton MR spectroscopic imaging. Radiology. 2006;241:449–458.
17. Huisman HJ, Engelbrecht MR, Barentsz JO. Accurate estimation of pharmacokinetic contrast-enhanced dynamic MRI parameters of the prostate. J Magn Reson Imaging. 2001;13:607– 614.
18. Tofts PS, Brix G, Buckley DL, et al. Estimating kinetic parameters from dynamic contrast-enhanced T(1)-weighted MRI of a diffusable tracer: standardized quantities and symbols. J Magn Reson Imaging. 1999;10:223
19. Kovar DA, Lewis M, Karczmar GS. A new method for imaging perfusion and contrast extraction fraction: input functions derived from reference tissues. J Magn Reson Imaging. 1998;8:1126 –1134.
20. Vos PC, Hambrock T, Barentsz JO, et al. Automated calibration for computerized analysis of prostate lesions using pharmacokinetic magnetic resonance images. In: Yang GZ, Hawkes DJ, Rueckert D, et al, eds. Medical Image Computing and Computer-Assisted Intervention MICCAI 2009. Part II, Volume 5761. Berlin, Germany: SpringerLink; 2009:836–843.
21. Huisman HJ, Karssemeijer N. Processing and displaying dynamic contrastenhanced MRI 2008 22. Hambrock T, Futterer JJ, Huisman HJ, et al. Thirty-two-channel coil 3T magnetic resonance-guided biopsies of
prostate tumour suspicious regions identified on multimodality 3T magnetic resonance imaging: technique and feasibility. Invest Radiol. 2008;43:686–694.
23. Kaplan I, Oldenburg NE, Meskell P, et al. Real time MRI-ultrasound image guided stereotactic prostate biopsy. Magn Reson Imaging. 2002;20:295–299.
24. Singh AK, Kruecker J, Xu S, et al. Initial clinical experience with real-time transrectal ultrasonography-magnetic resonance imaging fusion-guided prostate biopsy. BJU Int. 2008;101:841– 845.
25. Lowry M, Zelhof B, Liney GP, et al. Analysis of prostate DCE-MRI: comparison of fast exchange limit and fast exchange regimen pharmacokinetic models in the discrimination of malignant from normal tissue. Invest Radiol. 2009;44:577–584.
26. Kim CK, Park BK, Park W, et al. Prostate MR imaging at 3T using a phased-arrayed coil in predicting locally recurrent prostate cancer after radiation therapy: preliminary experience. Abdom Imaging. In press.
27. Stephenson AJ, Scardino PT, Bianco FJ, et al. Salvage therapy for locally recurrent prostate cancer after external beam radiotherapy. Curr Treat Options Oncol. 2004;5:357–365.
28. Gibbs P, Liney GP, Pickles MD, et al. Correlation of ADC and T2 measurements with cell density in prostate cancer at 3.0 Tesla. Invest Radiol. 2009;44:572–576.
114
3T DCE-MRI Guided Biopsy in Localizing Prostate Cancer Recurrence after Radiation Therapy
5


CHAPTER 6
Multiparametric MR Imaging for Detection and Localization of
Transition Zone prostate cancer
C. Hoeks, T. Hambrock; D. Yakar et al.
CHAPTER 6CHAPTER 6

Multiparametric MR imaging for detection and localization of transition zone prostate cancer
Radiology (Accepted)
Hoeks C, Hambrock T, Yakar D, Hulsbergen-van de Kaa CA, Wijtes JA,
Fütterer JJ, Barents JO
Advances in knowledge:
3T Multiparametric MR imaging, consisting of T2-weighted imaging (T2-w) + Diffusion
Weighted imaging + Dynamic Contrast-Enhanced MR imaging is of added value for the
detection of Gleason Grade (GG) 2-3 transition zone (TZ) cancers.
Detection rates of Gleason Grade 4-5 TZ cancers are significantly higher than detection
rates of Gleason Grade 2-3 TZ cancers on multiparametric MR imaging.
The overall localization accuracy for both GG 2-3 and GG 4-5 TZ cancers with
multiparametric MRI is superior compared to T2-w imaging alone .
Implications for patient care:
In patients with an increased PSA and one or more negative TRUS biopsy sessions, MR
imaging can detect the vast majority of aggressive tumours and almost the half of all low-
grade TZ tumours.
MR imaging can have a valuable role in identifying and selecting patients undergoing
active surveillance or targeting focal therapy.
Summary Statement:
Multiparametric 3T MR imaging is an accurate technique to detect and localize clinically significant, aggressive transition zone cancer.
116
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

ABSTRACT
Purpose: To retrospectively determine GG 2-3 and GG 4-5 transition zone (TZ) cancer detection
and localization accuracy of multiparametric MR imaging (MP-MRI) using radical prostatectomy
(RP) specimens as a gold standard.
Materials and Methods: The need for informed consent was waived by the IRB. Inclusion
criteria were TZ cancer >0.5 cm 3 upon RP and prior performed 3T endorectal multiparametric
MR imaging (T2-weighted (T2-w), diffusion weighted and dynamic contrast enhanced MRI
(DCE-MRI)). From 96 RP, 20 patients with TZ cancers were included and twenty-two patients
without TZ but with PZ cancers were randomly selected as control-group. Four radiologists
randomly scored patients for T2-w, and MP-MRI protocols: T2-w+ADC, T2-w+DCE-MRI and T2-
w+ADC+DCE-MRI consecutively with an interval of TZ cancer suspicion was rated (5-
point scale) in 6 regions of interest (ROI). A score of 4-5 was defined as a positive detection
result on a patient level. Localization was analyzed using ROI-ROC with generalized estimation
equations.
Results: MP-MRI (T2-w+ADC+/DCE-MRI, accuracy 60-61 %) improved detection of GG 2-3 TZ
cancers compared to T2-w alone (44%, p=0.01-0.02). Significantly more GG 4-5 (91%) versus
GG 2-3 (47%) TZ cancers were detected (p<0.05). Localization on ROI level was slightly
improved by MP-MRI for GG 4-5 TZ cancers only (AUC: 0.94 versus T2-w 0.91, p=0.02).
Conclusion: Only for GG 2-3 TZ cancers MP-MRI improves detection accuracy in comparison to
T2-w. Detection rates of GG 4-5 cancers are significantly higher than those of GG 2-3 cancers.
MP-MRI is only of slightly added value to T2-w for TZ cancer localization.
117
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

INTRODUCTION
Prostate cancer accounts for more than a quarter of male cancer incidence and had mortality
rates over 15% in 2008 (1). Twenty-five to 30% of these cancers are transition zone (TZ)
cancers (2;3). No uniform histopathologic definition of TZ cancers exists, although a cancer
volume of 50-70% or higher within the TZ, is commonly used as a histopathologic definition for
probable TZ origin (4). TZ prostate cancers have shown to have a relatively lower Gleason score
(5), local stage (6) and biochemical recurrence rate (7;8) in comparison to peripheral zone (PZ)
cancers. However, zonal location of a high Gleason Grade (GG) prostate cancer has shown not to
influence biochemical relapse-free survival (9). Furthermore, in prostatectomy series, a GG 4 or
5 with extra capsular extension and positive resection margins was present in 9% of all TZ
cancers (10). Therefore, improvement of TZ cancer detection remains an important goal in
prostate cancer diagnostics. Especially detection of TZ cancers with a GG 4-5 is important, as a
higher GG is an independent factor for poorer prognosis (11).
In current prostate cancer diagnostics, especially very anteriorly situated TZ cancers are often
subject to biopsy error due to dorsal to medial sample reach in random transrectal ultrasound
guided biopsies (TRUSGB) (12). Moreover, in patients with an elevated prostate specific antigen
(PSA) and 2 or more previous negative TRUSGB sessions, 57% of MR guided biopsy detected
cancers are situated within the ventral TZ (13).
On T2-weighted MR imaging (T2-w), TZ prostate cancers are difficult to differentiate from
benign prostatic hyperplasia, as the latter has heterogeneous signal intensity (SI)
similar to those of prostate cancer. In spite of this, T2-w has been advocated as an accurate
technique for TZ cancer detection (14;15). Several features on T2-w, like a homogeneously low
SI (sensitivity 76-78%, specificity 78-87%), ill-defined margins (sensitivity 76-78%, specificity
78-89%) and lenticular shape (sensitivity 48-56%, specificity 85-98%) may accurately predict
TZ cancer (16-18).
Functional MR imaging on 1.5 T has not shown to be of added value to T2-w for TZ cancer
detection (19). Diffusion weighted MR imaging (DWI) has shown to increase TZ cancer detection
accuracy when high b-values (>1000 s/mm2) are used (20-23). In dynamic contrast enhanced
MR imaging (DCE-MRI) quantitative parameters like Ktrans are able to differentiate TZ cancer
from glandular BPH, however not from stromal BPH (24). To our knowledge, 3T endorectal
118
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

multiparametric MR imaging including DWI and DCE-MRI has not earlier been evaluated for TZ
cancer detection and localization accuracy. Application of a higher field strength may have the
advantage of a higher SNR in the ventral prostate.
Therefore, the purpose of this study is to retrospectively determine GG 2-3 and GG 4-5 transition
zone (TZ) cancer detection and localization accuracy of multiparametric MR imaging (MP-MRI)
using radical prostatectomy (RP) specimens as a gold standard.
MATERIALS AND METHODS
Patients
The need for informed consent was waived by the Institutional Review Board. Inclusion criteria
were patients who had TZ cancer with a cancer volume > 0.5 cm3 upon prostatectomy and a pre-
prostatectomy endorectal 3T multiparametric MR imaging examination including T2-w, DWI
and DCE-MRI. Patients who had prior radiotherapy or transurethral resection of the prostate
were excluded.
Twenty-three TZ cancer patients were retrospectively selected from 98 consecutive
prostatectomies performed within our referral center between January 2007 and May 2009.
Subsequently, 25 patients with PZ cancer without co-existent TZ cancer were randomly selected
to serve as a control group, of which 22 patients were finally included. Three PZ cancer patients
were excluded due to earlier transurethral resection of the prostate (n=2) or due to a post-
radiotherapy status (n=1). A flow diagram for patient selection is shown in Figure 1.
MR imaging acquisition protocol
MR images were obtained on a 3T MR system (Trio Tim, Siemens, Erlangen, Germany) with the
use of a pelvic phased-array coil and an endorectal coil (Medrad, Pittsburgh, USA) filled with 40
ml of perfluorocarbon (Fomblin, Solvay-Solexis, Milan, Italy). Multiparametric MR imaging
parameters are presented in Table 1.
119
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

Axial T2-w images of the prostate and seminal vesicles were followed by axial DWI with the
same slice positions using diffusion modules and fat suppression pulses. Proton diffusion was
measured in three directions and apparent diffusion coefficient (ADC) maps were calculated
automatically. Prior to the DCE series an axial 3D proton density weighted gradient echo was
obtained. This was followed by an axial 3D T1 weighted spoiled gradient-echo sequences,
acquired during intravenous administration of 0.1 mmol of gadopentetate dimeglumine
(DOTAREM, Guerbet, Paris, France) per kilogram of bodyweight at a rate of 2.5 ml/s followed by
a 20 ml saline flush. Data post-processing of DCE-MR imaging was performed on in-house
software. Quantitative pharmacokinetic analysis was based on the Toft's model (25), using an
automatic per-patient calibration for estimation of the arterial input function (26).
MR image interpretation
Four radiologists (two with 2 years, one with 4 years and one with 9 years of experience with
prostate MR imaging) independently scored all cases in random order on in-house developed
software. Radiologists were blinded for the zonal location of the prostate cancer. T2-w, T2-
w+ADC, T2-w+DCE-MRI and T2-w+ADC+DCE-MRI were prospectively scored in 4 separate
consecutive sessions with an interval of at least 2 weeks. T1-weighted MR images were available
for evaluation of post-biopsy hematoma to avoid false-positive results. The TZ was divided into 6
regions of interest (ROI). In the coronal plane the TZ was divided in 3 parts: the level of the
verumontanum and the level inferior and superior to this plane. The sagittal plane through the
verumontanum was used to divide the TZ into a right and a left half.
A five-point scale rating was used for every ROI and for every reading session: 1) definitely no,
2) probably no, 3) possible, 4) probable and 5) definite presence of TZ cancer. For T2-w, existing
TZ cancer multiparametric MR imaging features were used to evaluate the presence of TZ
cancer. These included: homogeneously low SI, irregular boundaries around a low SI, lenticular
shape, interruption of the pseudocapsule and invasion of the anterior fibromuscular stroma
(AFS) or the ventrolateral TZ boundary (27-29). For DWI, a homogeneously low ADC value in
comparison to the surrounding TZ was used (30).
120
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

Figure 1. Flow diagram for patient selection. MR= magnetic resonance, TZ= transition
zone, PZ= peripheral zone, DWI= diffusion weighted MR imaging, DCE-MRI = dynamic
contrast enhanced MR imaging, TURP= transurethral resection of the prostate and
GT= ground truth or reference standard, 3T= 3 tesla.
Radical Prostatectomies
2007-2009 n= 98
Endorectal 3T MR imaging
including T2w, DWI and DCE
n=59
Exclusion: No combined DWI
and/or DCE n=28
No endorectal coil n= 11
TZ cancers n= 20
Random selection control group:
PZ cancers without co-existent
n= 25
TZ cancers positive GT
n= 20 Control group: PZ cancers without co-existent TZ
n= 22
Exclusion control group: n=2 TURP n= 1 post-radiotherapy
121
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

ADC maps were shown using window levels on which the highest ADC values within the bladder
ranged from 1800-2843 x 10-6 mm2/s. The darkest ADC values within the endorectal coil were 0
mm2/s and ADC values of the darkest regions within the TZ ranged from 251-1200 x 10-6 mm2/s.
For DCE-MRI (31), a pharmacokinetic signal intensity time-curve, in which washout occurred
immediately after early enhancement, was considered suspicious for TZ cancer. Both the lack of
washout and the presence of a plateau phase after early enhancement were considered less
suspicious for TZ cancer presence. The following features were applied for TZ cancer suspicion:
homogeneous, asymmetric and AFS enhancement (32-34), washout and the lack of a type 1 and
2 curve on Ktrans parametric maps (35).
Histopathologic analysis
Prostatectomy specimens served as a reference standard for multiparametric MR imaging
results and were processed into 4 mm step section slices (36). An experienced urogenital
pathologist, who was blinded for multiparametric MR imaging results, determined location,
stage and GG components for every individual cancer (according to 2005 ISUP criteria (37)).
Cancer volume was calculated while assuming elliptical tumour shape (38). Presence of a cancer
(39).
Correlation of MR data to the gold standard
Two radiologists (one with 2 years and one with 4 years of experience in prostate
multiparametric MR imaging) correlated MR data and prostatectomy in consensus using
landmarks like the verumontanum and calcifications. Correlation of prostate multiparametric
MR imaging to histopathology is known to be difficult (40).
Statistical Analyses
For all analyses significance levels of 2 sided p-value < 0.05 were used. An independent t-test
was used to test for differences in characteristics between patient groups. A Z-score was used to
test for differences in proportions.
TZ cancers consisting of a GG 4 and/or 5, were considered high GG TZ cancers, while TZ cancers
consisting of a GG 2 and/or 3 only were considered low GG TZ cancers.
122
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

Localization of TZ cancer was defined as finding a cancer in a certain ROI area of the prostate.
Localization accuracy for all TZ cancers, for GG 2-3- and for GG 4-5 TZ cancers was analyzed by
comparing areas under the receiver operating characteristic (ROC) curve (AUC) of different MR
imaging protocols using a generalized estimation equation (GEE) to account for correlation of
the same patient. The GENMOD procedure (version 9, SAS Institute, Cary,
NC) was used to calculate Pearson X2 tests for differences in ROI-ROC values between
multiparametric MR imaging protocols.
(41).
Protocol Sequence TR (ms)
TE (ms)
Slice thickness
FOV Matrix size
Voxel size
b-values (s/mm2)
Temp. resol.(s)
T2-w
TSE axial
coronal
sagittal
4280
3599
4290
99
98
98
3
3
3
179 179
192 192
192 192
448 448
384 384
384 384
0.4 0.4
0.5 0.5
0.5 0.5
DWI SSEPI 2600 90 3 204 204 136 136 1.5 1.5 0/50/500/800
DCE-MRI GE 800 1.51 3 192 192 128 128 1.5 1.5
DCE-MRI Spoiled GE 36 1.4 3 192 192 128 128 1.5 1.5 2.5
Table 1. MR imaging parameters. T2-w = T2-weighted MR imaging, DWI= diffusion
weighted MR imaging, DCE-MRI= dynamic contrast enhanced MR imaging, TSE= turbo
spin echo, SSEPI= single-shot echoplanar imaging, GE= gradient echo, TR= repetition time
and TE=echo time.
121
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6
123

MRI All TZ cancers vs. no TZ cancers GG 4-5 TZ vs. no TZ cancers GG 2-3 TZ vs. no TZ cancers
Sens. Spec. Accur. Sens. Spec. Accur. Sens. Spec. Accur.
T2-w 60%
(48/80)
[49-70]
74%
(65/88)
[64-82]
67%
(113/168)
[60-74]
86%
(38/44)
[73-94]
74%
(65/88)
[64-82]
78%
(103/132)
[70-84]
28%
(10/36)
[14-41]
51%
(45/88)
[41-61]
44%
(54/124)
[35-52]
T2-w + ADC
68%
(54/80)
[57-77]
68%
(60/88)
[58-77]
68%
(114/168)
[60-74]
86%
(38/44)
[73-94]
68%
(60/88)
[58-77]
74%
(98/132)
[66-81]
44%
(16/36)
[30-60]
68%
(60/88)
[58-77]
61%
(76/124)
[52-69]
T2-w + DCE-MRI
63%
(50/80)
[52-72]
69%
(61/88)
[59-78]
66%
(111/168)
[59-73]
89%
(39/44)
[76-96]
72%
(63/88)
[61-80]
77%
(102/132)
[69-84]
33%
(12/36)
[20-50]
72%
(63/88)
[61-80]
60%
(75/124)
[52-69]
T2-w + ADC +
DCE-MRI
59%
(47/80)
[48-69]
65%
(57/88)
[54-74]
62%
(104/168)
[54-69]
91%
(40/44)
[78-97]
81%
(71/88)
[71-88]
84%
(111/132)
[77-89]
47%
(17/36)
[32-63]
65%
(57/88)
[54-74]
60%
(74/124)
[51-68]
Table 3. Diagnostic accuracy for detection of all TZ cancers, of GG 4-5 and of GG 2-3 TZ
cancers for all readers for the different multiparametric MR imaging protocols.
Percentages are placed as numbers and proportions are placed in between brackets. 95%
confidence intervals are placed in square brackets. T2-w = T2-weighted MR imaging,
ADC= apparent diffusion coefficient, DCE-MRI= dynamic contrast enhanced MR imaging,
TZ= transition zone, MR= magnetic resonance, GG= Gleason Grade.
RESULTS
For 19 patients with TZ cancer only one tumour was present and for 1 patient 2 TZ cancers, both
with a GG 3+2 were present in the TZ upon prostatectomy specimens. Eleven out of 20 (55%) TZ
cancers had a GG 4-5 and nine out of 20 (45%) TZ cancers had a GG 2-3. Mean cancer volume of
GG 4-5 TZ cancers (6.6 cm3) did not differ significantly from mean cancer volume of GG 2-3 TZ
cancers (6.8 cm3, p=0.96). This was also the case for PZ cancers (GG 4-5 PZ cancers mean volume
of 0.95 cm3 versus GG 2-3 PZ cancers mean volume of 0,73 cm3, p=0.51). Mean PSA levels,
histopathological stage pT2A and cancer volume differed significantly between TZ and PZ cancer
124
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

patients (respectively p=0.01, p=0.02 and p<0.001). Differences between patients with TZ
cancers and patients with PZ cancers are presented in Table 2.
For detection of all TZ cancers, GG 4-5 TZ cancers and GG 2-3 TZ cancers on a patient level,
diagnostic accuracies are presented in Table 3. The accuracy did not differ significantly between
MR imaging protocols (T2-w, T2-w+ADC, T2-w+DCE-MRI and T2-w+ADC+DCE-MRI) for
detection of both all TZ cancers and for GG 4-5 TZ cancers. However, for detection of GG 2-3 TZ
cancers accuracies of T2-w+ADC, T2-w+DCE-MRI and T2-w+ADC+DCE-MRI were significantly
higher in comparison to T2-w: T2-w+ADC versus T2-w p=0.01, T2-w+DCE-MRI versus T2-w
p=0.01 and T2-w+ADC+DCE-MRI versus T2-w,p=0.02.
For both T2-w and multiparametric MR imaging, detection rates of GG 4-5 TZ cancers were
significantly higher in comparison to detection rates of GG 2-3 TZ cancers: T2-w (28% of GG 2-3
cancers versus 86% of GG4-5 cancers, p=0.001), T2-w+ADC (44% versus 86%, p=0.001), T2-
w+DCE-MRI (33% versus 89%, p=0.001) and T2-w+ADC+DCE-MRI (47% versus 91%, p=0.001).
These results are presented in Table 4.
For localization of GG 4-5 TZ cancers on an ROI level, AUC of T2-w+ADC+DCE-MRI (0.94) was
higher in comparison to AUC of T2-w alone (0.91, p=0.02) and in comparison to AUC of T2-
w+DCE-MRI (0.91, p=0.01). For localization of all TZ cancers and GG 2-3 TZ cancers on an ROI
level, there were no significant differences between different multiparametric MR imaging
protocols. Results of these ROI-ROC analyses are presented in Table 5 and Figure 2.
Interobserver agreement for TZ cancer detection was moderate to substantial. Mean weighted
kappa values for all protocols (T2-w, T2-w+ADC, T2-w+DCE-MRI and T2-w+ADC+DCE-MRI)
ranged from 0.56-0.71.
125
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

Characteristic Patients with
TZ cancer
(n = 20)
Patients with PZ cancer only
(n = 22)
Independent t-test patients with
vs. patients without TZ
cancer
Patients with GG4-5 TZ
cancer
(n=11)
Patients with GG2-3 TZ
cancer
(n=9)
Age (yr) (range) 67 (55-73) 64.5 (53-71) 0.98 67 (55-73) 67 (55-70)
PSA (ng/ml) (range) 10.3 (1.9-44) 6.3 (3.2-14.8) 0.01* 17.6 (5.3-44.0) 8.7(1.9-11)
Tumour volume (cm3) 4.9 (0.5-22) 0.5 (0.01-2.36) <0.001* 7.4 (0.5-15.7) 3.5 (0.5-22)
MR I to Surgery interval (wk) (range)
7(1-21) 7 (1-21) 0.78 5 (1-21) 8(1-22)
Histopathologic Stage
pT2A 0 7 p=0.02* 0 1
pT2C 9 9 p=0.96 3 6
pT3A 7 6 p=0.83 5 1
pT3B 2 0 p=0.43 2 0
pT4 2 0 p=0.43 1 1
Gleason score in prostatectomy
2+2 0 1 p=0.96 0 0
2+3 3 0 p=0,20 0 3
2+4 1 0 p=0.96 1 0
3+2 3 1 p=0.54 0 3
3+3 3 9 p=0.13 0 3
3+4 2 7 p=0.18 2 0
4+2 1 0 p=0.96 1 0
4+3 5 4 p=0.87 5 0
4+5 2 0 p=0.43 2 0
Table 2. Patient and prostatectomy characteristics. TZ= transition zone, PZ= peripheral
zone, PSA= prostate specific antigen. *= under threshold for significance (2 tailed p-value
<0.05), N.A. = not available, n= number, GG= Gleason Grade. Median values are reported.
126
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

MR imaging protocol Detection rate
GG 2-3 TZ cancers Detection rate
GG 4-5 TZ cancers Z score, p value
T2-w
28% (10/36)
86% (38/44)
5.09, p<0.001*
T2-w+ADC
44% (16/36)
86% (38/44)
3.74, p<0.001*
T2-w+DCE
33% (12/36)
89% (39/44)
4.89, p<0.001*
T2-w+ADC+DCE
47% (17/36)
91% (40/44)
4.05, p<0.001*
Table 4. Comparison of detection rates of GG 2-3 versus GG 4-5 TZ cancers. Percentages
are placed as numbers and proportions are placed in between brackets. TZ= transition
zone, * = under threshold for significance (2 tailed p-value <0.05), GG= Gleason Grade,
T2-w= T2-weighted MR imaging, ADC= apparent diffusion coefficient, DCE-MRI= dynamic
contrast enhanced MR imaging, MR= magnetic resonance.
Localization all TZ cancers X2 test and AUC
Localization GG 4-5 TZ cancers versus PZ cancers
Localization GG 2-3 TZ cancers versus PZ cancers
X2(3)=6.68, p=0.08 X2(3)=8.55, p=0.04 X2(3)=4.44, p=0.22
T2-w 0.78 (0.71-0.84)
T2-w 0.91
(0.86-0.96)
T2-w 0.56
(0.43-0.68)
T2-w+ADC 0.82 (0.76-0.89)
T2-w+ADC 0.92
(0.86-0.97)
T2-w+ADC 0.66
(0.53-0.79)
T2-w+DCE-MRI 0.80 (0.73-0.86)
T2-w+DCE-MRI 0.91
(0.87-0.96)
T2-w+DCE-MRI 0.60
(0.47-0.73)
T2-w+ADC+
DCE-MRI 0.83 (0.77-0.89)
T2-w+ADC+DCE-MRI 0.94
(0.91-0.98)
T2-w+ADC+DCE-MRI
0.64
(0.53-0.75)
Significant differences Significant differences Significant differences
N.S. T2-w < T-2w+ADC+DCE
T2-w+DCE-MRI <
T2-w+ADC+DCE-MRI
p=0.02
p=0.01
N.S.
Table 5. Results of ROI-ROC analyses for localization of all TZ cancers, of GG 4-5 and of GG
2-3 TZ cancers. ROI-ROC values were compared using a generalized estimation equation
(GEE). Pearson X2 tests were calculated to test for differences in ROI-ROC values between
MR imaging protocols. 95% confidence intervals are placed between brackets. T2-w= T2-
weighted MR imaging, ADC= apparent diffusion coefficient maps, DCE-MRI= dynamic
contrast enhanced MRI, TZ= transition zone, PZ= peripheral zone, GG= Gleason Grade.
127
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

Figure 2 Receiver operating characteristic curves of the different multiparametric MR
imaging protocols for localization of TZ cancers (a), of GG 4-5 TZ cancers (b)( AUC values
of T2-w+ADC+DCE-MRI (0.94) were significantly higher in comparison to AUC of T2-w
only (0.91, p=0.02) and to AUC of T2-w+DCE-MRI (0.91, p=0.01)) and of GG 2-3 TZ cancers
(c) respectively. Diagonal black line= reference line of a 0.50 area under the curve, TZ=
transition zone, T2-w= T2-weighted MR imaging, ADC= apparent diffusion coefficient
maps, DCE-MRI= dynamic contrast enhanced MR imaging, GG= Gleason Grade. A legend on
the right side indicates which colors belong to which MR imaging protocol, AUC= area
under the receiver operating characteristic curve, *= under threshold for significance (2
tailed p-value <0.05).
128
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

DISCUSSION
To our knowledge, this is the first study, which compared more than one endorectal MR imaging
technique at 3T for TZ prostate cancer detection and localization. Our results indicate that
multiparametric MR imaging (T2-w+ADC and/or DCE-MRI) significantly improves detection
accuracy in comparison to T2-w for GG 2-3 TZ cancers, as opposed to GG 4-5 TZ cancers. For
detection of GG 4-5 TZ cancers, T2-w may be sufficient as multiparametric MR imaging did not
significantly improve detection accuracy in comparison to T2-w. All analyses within our study
reflect significantly increased detection rates of GG 4-5 TZ cancers versus GG 2-3 TZ cancers for
both T2-w only and for multiparametric MR imaging. Cancer volume may have influenced these
measurements to some extent. Whereas mean cancer volumes did not differ significantly
between GG 2-3 and GG 4-5 TZ cancers, the latter ones were, nonetheless, often larger in volume.
A few studies on 1.5T have evaluated detection and localization of TZ cancer with
multiparametric MR imaging. These studies, however, did not always use a histopathological
definition for TZ cancer, used different b-values and applied either pelvic phased-array or
endorectal coils (42-45). For TZ cancer detection, our accuracy for T2-w+ADC of 62-68% for all
TZ cancers is lower compared to other studies (46-49). Possible reasons for better DWI results
of Yoshizako et al. (accuracies of 62-81% respectively) are inclusions of larger lesions (10-28
mm versus our median of 3.56 cc), and the use of higher b- 2), which have
improved TZ cancer detection accuracy for T2-w+DWI(50;51). Our results are in agreement
with studies, which used b-values of <1000 mm/s2 (52;53), and did not show added value of
DWI in general TZ cancer detection. Furthermore the lack of use of a standard ADC window-
level (54) and quantitative threshold values for ADC reader evaluation (55) may further explain
our lower detection accuracy for T2-w+ADC in comparison to results of Haider et al. (accuracy of
81%).
Considering T2-w+DCE-MRI, our results are comparable to those of Yoshizako et al. at 1.5T
(sensitivity 69%, specificity 68% and accuracy 69%)(56). However, our results differ from those
of Delongchamps et al.(57), this study had a sensitivity of 47% and a specificity of 77% for TZ
cancer detection. Their lower sensitivity in comparison to ours (63%) may be explained by their
population existing predominantly out of GG 2-3 TZ cancers and by using a lower field strength.
Performed studies of the TZ often used semi-quantitative analysis instead of our quantitative
pharmacokinetic analysis, which makes comparison difficult (58;59). Our detection results for
multiparametric MR imaging are in contrast with those of Delongchamps et al., who found no
added value of multiparametric MR imaging techniques compared to T2-w for TZ cancer
129
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

detection in a sub-group of predominantly low GG TZ cancers (60). The lower field strength and
the lack of a histopathologic definition for TZ cancers may explain these conflicting results for
detection of low GG TZ cancers. Within the same study, also no influence of Gleason score on
multiparametric MR imaging TZ cancer detection accuracy was found. This may be due to the
low number of GG 4-5 TZ cancers in their population.
For TZ cancer localization on ROI level, multiparametric MR imaging adds little value to T2-w.
Only for GG 4-5 TZ cancers, multiparametric MR imaging (T2-w+ADC+DCE-MRI AUC 0.94)
slightly improves TZ cancer localization accuracy in comparison to T2-w (AUC 0.91, p=0.02) and
in comparison to T2-w+DCE-MRI (AUC 0.91, p=0.01). Our TZ cancer localization accuracy for T2-
w+ADC is lower (AUC 0.82) in comparison to Delongchamps et al. (AUC 0.88), while our T2-
w+DCE-MRI (AUC 0.80) results are in agreement with their T2-w+DCE-MRI results (AUC
0.70)(61). The mentioned lack of use of a standard ADC window-level (62) and quantitative
thresholds may explain our lower T2-w+ADC performance. Our T2-w+ADC+DCE-MRI
localization results (AUC 0.83) are somewhat higher in comparison to the same study (AUC
0.75). As mentioned, this difference may be explained by our use of a higher field strength.
This study has limitations. As mentioned, we did not use high b-values, standard ADC settings
and quantitative ADC reading in DWI. However, no quantitative ADC thresholds have been
defined for ADC maps created out of DWI with b values< 1000 s/mm2. Secondly, in order to
acquire the most optimal gold standard, we only selected prostatectomy patients. This may have
introduced selection bias in our results. Our population is rather small and consists for 54% out
of TZ cancers. This is not an optimal representation of the general population where prevalence
of TZ cancers is 25%(63). Thirdly, significant differences between TZ cancer and PZ cancer
(healthy TZ) patient groups were present for PSA level, cancer volume and clinical stage. This
could not be adjusted for with stratification as patient numbers in subpopulations were too low
for valid analyses. A relatively higher PSA level, cancer volume and clinical stage in TZ cancer
patients versus PZ cancer patients, may have biased our results. Fourthly, we only included TZ
cancers with a volume >0.5 cm3. The median volume of undetected TZ cancers in a 1.5T study
with a higher in plane resolution than our study (0.31 0.31 mm), was 0.44 cm3 (range 0.26-
0.58)(64). By including TZ cancers with a volume> 0.5 cm3, all TZ cancers should be detectable
on 3T MR imaging.
130
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

Figure 3. Sixty-five year old male patient, with a PSA of 44 ng/mL, 2 previous TRUS guided
prostate biopsy sessions and a clinical stage T2 and a Gleason score of 4+5=9 prostate
cancer found in a third session in all five cores on the right side, who underwent
endorectal MR imaging for local prostate cancer localization and staging. The cancer
suspicious region is visible on T2WI as well as on different multi-parametric MR imaging
protocols. (a) Axial endorectal T2WI turbo spin echo at mid-prostate level shows a low
zone (white demarcation). This finding is a feature of transition zone cancer on T2WI. (b)
Axial ADC map at the same level as image a. A low ADC value (mean ADC 758 x 10-6
mm2/s) is present in the ventral transition zone (white demarcation). A low ADC value
within the transition zone may be suspect for transition zone cancer. (c) Axial T2-
weighted turbo spin echo at the same level as (a), with a superimposed Ktrans parametric
map. Homogeneous enhancement of the transition zone is present. (d) Axial whole mount
section histopathology at the corresponding level (a-c) demonstrates a pT4N1R1 Gleason
score 4+5=9 prostate TZ cancer (black demarcation).
131
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

Figure 4. A 59-year old man with a PSA of 10.3 ng/ml, a clinical stage T2 and a Gleason
score 3+3 prostate cancer in 2 out of 5 cores on the left side and in 1 out of 5 cores on the
right side upon random TRUS guided biopsy. Endorectal MR imaging was performed upon
a clinical localization and staging indication. The cancer suspicious region is more clearly
defined on multiparametric MR imaging techniques in comparison to T2-w.
a) Axial T2-weighted images at the apex-mid level. A homogeneous low signal intensity
te arrows).
b) Axial ADC map at the same level as a. In the right transition zone an irregular
shaped low ADC value (median 422x10-6 mm2/s), suspect for TZ cancer is present
(white and black demarcation). In the left TZ a low ADC value is also present (white
line demarcation).
132
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

c) Axial T2-w image at the same level as (a) with a superimposed wash-out parametric
map The right TZ shows an asymmetric increased contrast washout, which is
suspect for transition zone cancer. A red-colored ring shape pattern can be
appreciated. Some washout is also present in the left transition zone.
d) The relative Gadolinium-concentration-
lesion.
e) Axial whole mount section histopathology at the corresponding level (a-c) shows a
multifocal prostate cancer, with a dominant lesion in the right ventral transition
zone Gleason score 3+4=7 (black demarcation). The lesion in the left transition
zone (L) had a Gleason score of 3+2=5.
133
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

Figure 5. A 67-year old male patient with a PSA of 18 ng/ml, a clinical stage T3 Gleason score of
7 prostate cancer underwent endorectal MR imaging for pre-surgical staging.
a) Axial T2-weighted image at mid-prostate level. Next to a well defined inhomogeneous
nodular pattern of the dorsal transition zone, a low homogeneous signal intensity with
poorly defined edges is seen in the right ventral transition zone. A lenticular shape and
interruption of the pseudo-capsule are present (white demarcation). These findings are
suspect for transition zone cancer.
b) Axial ADC map at the same level as (a). A low ADC value (median 511x10-6 mm2/s) is
present in the right ventral transition zone (white demarcation).
134
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

c) Axial endorectal T2-weighted turbo spin echo at the same level as (a) with a
superimposed Ktrans parametric map. A suspect sign for transition zone cancer is the
increased enhancement of the anterior fibromuscular stroma (white demarcation).
d) The relative Gadolinium-contrast-versus-
fast rise, fast time-to-peak and wash-out, which is suspect for prostate cancer.
e) Axial whole mount section histopathology at the corresponding level (a-c) shows a pT3b
Gleason score 4+5=9 transition zone cancer in the right transition zone with extension to
the left (black demarcation).
135
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

Future studies, in which (high b-value) endorectal multiparametric MR imaging at 3T is
evaluated for detection of clearly defined TZ cancers in large populations, are necessary. Our
results have the following clinical implications; (a) in patients with increased PSA levels and one
or more negative TRUS biopsy sessions, addition of either DWI ADC maps or DCE-MRI to T2-w
is required to establish a diagnosis in case of low Gleason Grade (2-3) TZ cancer presence.
Timely TZ cancer diagnosis prevents unnecessary PSA measurements and TRUSGB sessions and
may also prevent progression of lower GG cancers and positive anterior resection margins. And
(b) in patients with proven TZ cancer who are considered for focal therapy, application of 3T T2-
w may be sufficient for TZ cancer localization, as 3T endorectal multiparametric MR imaging
(T2-w+ADC+DCE-MRI) only slightly improves T2-w localization results.
CONCLUSION
In conclusion, multiparametric MR imaging (T2-w+ADC and/or DCE-MRI), improves detection
accuracy in comparison to T2-w alone for GG 2-3 TZ cancers only, as opposed to GG 4-5 cancers.
GG 4-5 TZ cancers have significantly higher detection rates in comparison to their GG 2-3
counterparts, both on T2-w and on multiparametric MR imaging. For TZ cancer localization at
3T, multiparametric MR imaging is of little added value to T2-w alone.
136
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

REFERENCES
1. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ. Cancer statistics, 2008. CA Cancer J.Clin. 2008 Mar;58(2):71-96.
2. Augustin H, Erbersdobler A, Graefen M, Fernandez S, Palisaar J, Huland H, Hammerer P. Biochemical recurrence following radical prostatectomy: a comparison between prostate cancers located in different anatomical zones. Prostate 2003 Apr 1;55(1):48-54.
3. McNeal JE, Redwine EA, Freiha FS, Stamey TA. Zonal distribution of prostatic adenocarcinoma. Correlation with histologic pattern and direction of spread. Am.J.Surg.Pathol. 1988 Dec;12(12):897-906.
4. McNeal JE, Redwine EA, Freiha FS, Stamey TA. Zonal distribution of prostatic adenocarcinoma. Correlation with histologic pattern and direction of spread. Am.J.Surg.Pathol. 1988 Dec;12(12):897-906.
5. Augustin H, Erbersdobler A, Hammerer PG, Graefen M, Huland H. Prostate cancers in the transition zone: Part 2; clinical aspects. BJU Int 2004 Dec;94(9):1226-9.
6. Greene DR, Wheeler TM, Egawa S, Weaver RP, Scardino PT. Relationship Between Clinical Stage and Histological Zone of Origin in Early Prostate-Cancer - Morphometric Analysis. British Journal of Urology 1991;68(5):499-509.
7. Erbersdobler A, Huhle S, Palisaar J, Graefen M, Hammerer P, Noldus J, Huland H. Pathological and clinical characteristics of large prostate cancers predominantly located in the transition zone. Prostate Cancer Prostatic.Dis. 2002;5(4):279-84.
8. King CR, Ferrari M, Brooks JD. Prognostic significance of prostate cancer originating from the transition zone. Urol Oncol. 2009 Nov;27(6):592-7.
9. King CR, Ferrari M, Brooks JD. Prognostic significance of prostate cancer originating from the transition zone. Urol Oncol. 2009 Nov;27(6):592-7.
10. Shannon BA, McNeal JE, Cohen RJ. Transition zone carcinoma of the prostate gland: a common indolent tumour type that occasionally manifests aggressive behaviour. Pathology 2003 Dec;35(6):467-71.
11. Gleason DF, Mellinger GT. Prediction of prognosis for prostatic adenocarcinoma by combined histological grading and clinical staging. J.Urol 1974 Jan;111(1):58-64.
12. Pelzer AE, Bektic J, Berger AP, Halpern EJ, Koppelstatter F, Klauser A, Rehder P, Horninger W, Bartsch G, Frauscher F. Are transition zone biopsies still necessary to improve prostate cancer detection? Results from the tyrol screening project. Eur Urol 2005 Dec;48(6):916-21.
13. Hambrock T, Somford DM, Hoeks C, Bouwense SA, Huisman H, Yakar D, van O, I, Witjes JA, Futterer JJ, Barentsz JO. Magnetic resonance imaging guided prostate biopsy in men with repeat negative biopsies and increased prostate specific antigen. J.Urol 2010 Feb;183(2):520-7.
14. Akin O, Sala E, Moskowitz CS, Kuroiwa K, Ishill NM, Pucar D, Scardino PT, Hricak H. Transition zone prostate cancers: features, detection, localization, and staging at endorectal MR imaging. Radiology 2006 Jun;239(3):784-92.
15. Li H, Sugimura K, Kaji Y, Kitamura Y, Fujii M, Hara I, Tachibana M. Conventional MRI capabilities in the diagnosis of prostate cancer in the transition zone. AJR Am.J.Roentgenol. 2006 Mar;186(3):729-42.
16. Hricak H, Choyke PL, Eberhardt SC, Leibel SA, Scardino PT. Imaging prostate cancer: a multidisciplinary perspective. Radiology 2007 Apr;243(1):28-53.
17. Akin O, Sala E, Moskowitz CS, Kuroiwa K, Ishill NM, Pucar D, Scardino PT, Hricak H. Transition zone prostate cancers: features, detection, localization, and staging at endorectal MR imaging. Radiology 2006 Jun;239(3):784-92.
18. Li H, Sugimura K, Kaji Y, Kitamura Y, Fujii M, Hara I, Tachibana M. Conventional MRI capabilities in the diagnosis of prostate cancer in the transition zone. AJR Am.J.Roentgenol. 2006 Mar;186(3):729-42.
19. Delongchamps NB, Rouanne M, Flam T, Beuvon F, Liberatore M, Zerbib M, Cornud F. Multiparametric magnetic resonance imaging for the detection and localization of prostate cancer: combination of T2-weighted, dynamic contrast-enhanced and diffusion-weighted imaging. BJU Int 2010 Nov 2.
20. Delongchamps NB, Rouanne M, Flam T, Beuvon F, Liberatore M, Zerbib M, Cornud F. Multiparametric magnetic resonance imaging for the detection and localization of prostate cancer: combination of T2-weighted, dynamic contrast-enhanced and diffusion-weighted imaging. BJU Int 2010 Nov 2.
21. Haider MA, van der Kwast TH, Tanguay J, Evans AJ, Hashmi AT, Lockwood G, Trachtenberg J. Combined T2-weighted and diffusion-weighted MRI for localization of prostate cancer. AJR Am.J.Roentgenol. 2007 Aug;189(2):323-8.
22. Yoshizako T, Wada A, Hayashi T, Uchida K, Sumura M, Uchida N, Kitagaki H, Igawa M. Usefulness of diffusion-weighted imaging and dynamic contrast-enhanced magnetic resonance imaging in the diagnosis of prostate transition-zone cancer. Acta Radiol. 2008 Dec;49(10):1207-13.
137
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

23. Katahira K, Takahara T, Kwee TC, Oda S, Suzuki Y, Morishita S, Kitani K, Hamada Y, Kitaoka M, Yamashita Y.
Ultra-high-b-value diffusion-weighted MR imaging for the detection of prostate cancer: evaluation in 201 cases with histopathological correlation. Eur Radiol. 2011 Jan;21(1):188-96.
24. Oto A, Kayhan A, Jiang Y, Tretiakova M, Yang C, Antic T, Dahi F, Shalhav AL, Karczmar G, Stadler WM. Prostate Cancer: Differentiation of Central Gland Cancer from Benign Prostatic Hyperplasia by Using Diffusion-weighted and Dynamic Contrast-enhanced MR Imaging. Radiology 2010 Sep 15.
25. Tofts PS, Brix G, Buckley DL, Evelhoch JL, Henderson E, Knopp MV, Larsson HB, Lee TY, Mayr NA, Parker GJ, et al. Estimating kinetic parameters from dynamic contrast-enhanced T(1)-weighted MRI of a diffusable tracer: standardized quantities and symbols. J.Magn Reson.Imaging 1999 Sep;10(3):223-32.
26. Vos PC, Hambrock T, Barenstz JO, Huisman HJ. Automated calibration for computerized analysis of prostate lesions using pharmacokinetic magnetic resonance images. Med Image Comput.Comput.Assist.Interv. 2009;12(Pt 2):836-43.
27. Hricak H, Choyke PL, Eberhardt SC, Leibel SA, Scardino PT. Imaging prostate cancer: a multidisciplinary perspective. Radiology 2007 Apr;243(1):28-53.
28. Akin O, Sala E, Moskowitz CS, Kuroiwa K, Ishill NM, Pucar D, Scardino PT, Hricak H. Transition zone prostate cancers: features, detection, localization, and staging at endorectal MR imaging. Radiology 2006 Jun;239(3):784-92.
29. Li H, Sugimura K, Kaji Y, Kitamura Y, Fujii M, Hara I, Tachibana M. Conventional MRI capabilities in the diagnosis of prostate cancer in the transition zone. AJR Am.J.Roentgenol. 2006 Mar;186(3):729-42.
30. Kim CK, Park BK, Han JJ, Kang TW, Lee HM. Diffusion-weighted imaging of the prostate at 3 T for differentiation of malignant and benign tissue in transition and peripheral zones: preliminary results. J.Comput.Assist.Tomogr. 2007 May;31(3):449-54.
31. Ren J, Huan Y, Wang H, Chang YJ, Zhao HT, Ge YL, Liu Y, Yang Y. Dynamic contrast-enhanced MRI of benign prostatic hyperplasia and prostatic carcinoma: correlation with angiogenesis. Clin.Radiol. 2008 Feb;63(2):153-9.
32. Li H, Sugimura K, Kaji Y, Kitamura Y, Fujii M, Hara I, Tachibana M. Conventional MRI capabilities in the diagnosis of prostate cancer in the transition zone. AJR Am.J.Roentgenol. 2006 Mar;186(3):729-42.
33. Lemaitre L, Puech P, Poncelet E, Bouye S, Leroy X, Biserte J, Villers A. Dynamic contrast-enhanced MRI of anterior prostate cancer: morphometric assessment and correlation with radical prostatectomy findings. Eur Radiol. 2008 Aug 29.
34. Engelbrecht MR, Huisman HJ, Laheij RJ, Jager GJ, van Leenders GJ, Hulsbergen-Van De Kaa CA, de la Rosette JJ, Blickman JG, Barentsz JO. Discrimination of prostate cancer from normal peripheral zone and central gland tissue by using dynamic contrast-enhanced MR imaging. Radiology 2003 Oct;229(1):248-54.
35. Ren J, Huan Y, Wang H, Chang YJ, Zhao HT, Ge YL, Liu Y, Yang Y. Dynamic contrast-enhanced MRI of benign prostatic hyperplasia and prostatic carcinoma: correlation with angiogenesis. Clin.Radiol. 2008 Feb;63(2):153-9.
36. van Niekerk CG, van der Laak JA, Borger ME, Huisman HJ, Witjes JA, Barentsz JO, Hulsbergen-Van De Kaa CA. Computerized whole slide quantification shows increased microvascular density in pT2 prostate cancer as compared to normal prostate tissue. Prostate 2009 Jan 1;69(1):62-9.
37. Epstein JI, Allsbrook WC, Jr., Amin MB, Egevad LL. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am.J.Surg.Pathol. 2005 Sep;29(9):1228-42.
38. van Niekerk CG, van der Laak JA, Borger ME, Huisman HJ, Witjes JA, Barentsz JO, Hulsbergen-Van De Kaa CA. Computerized whole slide quantification shows increased microvascular density in pT2 prostate cancer as compared to normal prostate tissue. Prostate 2009 Jan 1;69(1):62-9.
39. Bouye S, Potiron E, Puech P, Leroy X, Lemaitre L, Villers A. Transition zone and anterior stromal prostate cancers: zone of origin and intraprostatic patterns of spread at histopathology. Prostate 2009 Jan 1;69(1):105-13.
40. Futterer JJ, Heijmink SW, Scheenen TW, Veltman J, Huisman HJ, Vos P, Hulsbergen-Van de Kaa CA, Witjes JA, Krabbe PF, Heerschap A, et al. Prostate cancer localization with dynamic contrast-enhanced MR imaging and proton MR spectroscopic imaging. Radiology 2006 Nov;241(2):449-58.
41. Kundel HL, Polansky M. Measurement of observer agreement. Radiology 2003 Aug;228(2):303-8.
42. Akin O, Sala E, Moskowitz CS, Kuroiwa K, Ishill NM, Pucar D, Scardino PT, Hricak H. Transition zone prostate cancers: features, detection, localization, and staging at endorectal MR imaging. Radiology 2006 Jun;239(3):784-92.
43. Haider MA, van der Kwast TH, Tanguay J, Evans AJ, Hashmi AT, Lockwood G, Trachtenberg J. Combined T2-weighted and diffusion-weighted MRI for localization of prostate cancer. AJR Am.J.Roentgenol. 2007 Aug;189(2):323-8.
138
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

44. Delongchamps NB, Rouanne M, Flam T, Beuvon F, Liberatore M, Zerbib M, Cornud F. Multiparametric magnetic
resonance imaging for the detection and localization of prostate cancer: combination of T2-weighted, dynamic contrast-enhanced and diffusion-weighted imaging. BJU Int 2010 Nov 2.
45. Yoshizako T, Wada A, Hayashi T, Uchida K, Sumura M, Uchida N, Kitagaki H, Igawa M. Usefulness of diffusion-weighted imaging and dynamic contrast-enhanced magnetic resonance imaging in the diagnosis of prostate transition-zone cancer. Acta Radiol. 2008 Dec;49(10):1207-13.
46. Delongchamps NB, Rouanne M, Flam T, Beuvon F, Liberatore M, Zerbib M, Cornud F. Multiparametric magnetic resonance imaging for the detection and localization of prostate cancer: combination of T2-weighted, dynamic contrast-enhanced and diffusion-weighted imaging. BJU Int 2010 Nov 2.
47. Yoshizako T, Wada A, Hayashi T, Uchida K, Sumura M, Uchida N, Kitagaki H, Igawa M. Usefulness of diffusion-weighted imaging and dynamic contrast-enhanced magnetic resonance imaging in the diagnosis of prostate transition-zone cancer. Acta Radiol. 2008 Dec;49(10):1207-13.
48. Akin O, Sala E, Moskowitz CS, Kuroiwa K, Ishill NM, Pucar D, Scardino PT, Hricak H. Transition zone prostate cancers: features, detection, localization, and staging at endorectal MR imaging. Radiology 2006 Jun;239(3):784-92.
49. Haider MA, van der Kwast TH, Tanguay J, Evans AJ, Hashmi AT, Lockwood G, Trachtenberg J. Combined T2-weighted and diffusion-weighted MRI for localization of prostate cancer. AJR Am.J.Roentgenol. 2007 Aug;189(2):323-8.
50. Katahira K, Takahara T, Kwee TC, Oda S, Suzuki Y, Morishita S, Kitani K, Hamada Y, Kitaoka M, Yamashita Y. Ultra-high-b-value diffusion-weighted MR imaging for the detection of prostate cancer: evaluation in 201 cases with histopathological correlation. Eur Radiol. 2011 Jan;21(1):188-96.
51. Yoshizako T, Wada A, Hayashi T, Uchida K, Sumura M, Uchida N, Kitagaki H, Igawa M. Usefulness of diffusion-weighted imaging and dynamic contrast-enhanced magnetic resonance imaging in the diagnosis of prostate transition-zone cancer. Acta Radiol. 2008 Dec;49(10):1207-13.
52. Delongchamps NB, Rouanne M, Flam T, Beuvon F, Liberatore M, Zerbib M, Cornud F. Multiparametric magnetic resonance imaging for the detection and localization of prostate cancer: combination of T2-weighted, dynamic contrast-enhanced and diffusion-weighted imaging. BJU Int 2010 Nov 2.
53. Haider MA, van der Kwast TH, Tanguay J, Evans AJ, Hashmi AT, Lockwood G, Trachtenberg J. Combined T2-weighted and diffusion-weighted MRI for localization of prostate cancer. AJR Am.J.Roentgenol. 2007 Aug;189(2):323-8.
54. Haider MA, van der Kwast TH, Tanguay J, Evans AJ, Hashmi AT, Lockwood G, Trachtenberg J. Combined T2-weighted and diffusion-weighted MRI for localization of prostate cancer. AJR Am.J.Roentgenol. 2007 Aug;189(2):323-8.
55. Delongchamps NB, Rouanne M, Flam T, Beuvon F, Liberatore M, Zerbib M, Cornud F. Multiparametric magnetic resonance imaging for the detection and localization of prostate cancer: combination of T2-weighted, dynamic contrast-enhanced and diffusion-weighted imaging. BJU Int 2010 Nov 2.
56. Yoshizako T, Wada A, Hayashi T, Uchida K, Sumura M, Uchida N, Kitagaki H, Igawa M. Usefulness of diffusion-weighted imaging and dynamic contrast-enhanced magnetic resonance imaging in the diagnosis of prostate transition-zone cancer. Acta Radiol. 2008 Dec;49(10):1207-13.
57. Delongchamps NB, Rouanne M, Flam T, Beuvon F, Liberatore M, Zerbib M, Cornud F. Multiparametric magnetic resonance imaging for the detection and localization of prostate cancer: combination of T2-weighted, dynamic contrast-enhanced and diffusion-weighted imaging. BJU Int 2010 Nov 2.
58. Delongchamps NB, Rouanne M, Flam T, Beuvon F, Liberatore M, Zerbib M, Cornud F. Multiparametric magnetic resonance imaging for the detection and localization of prostate cancer: combination of T2-weighted, dynamic contrast-enhanced and diffusion-weighted imaging. BJU Int 2010 Nov 2.
59. Yoshizako T, Wada A, Hayashi T, Uchida K, Sumura M, Uchida N, Kitagaki H, Igawa M. Usefulness of diffusion-weighted imaging and dynamic contrast-enhanced magnetic resonance imaging in the diagnosis of prostate transition-zone cancer. Acta Radiol. 2008 Dec;49(10):1207-13.
60. Delongchamps NB, Rouanne M, Flam T, Beuvon F, Liberatore M, Zerbib M, Cornud F. Multiparametric magnetic resonance imaging for the detection and localization of prostate cancer: combination of T2-weighted, dynamic contrast-enhanced and diffusion-weighted imaging. BJU Int 2010 Nov 2.
61. Delongchamps NB, Rouanne M, Flam T, Beuvon F, Liberatore M, Zerbib M, Cornud F. Multiparametric magnetic resonance imaging for the detection and localization of prostate cancer: combination of T2-weighted, dynamic contrast-enhanced and diffusion-weighted imaging. BJU Int 2010 Nov 2.
62. Haider MA, van der Kwast TH, Tanguay J, Evans AJ, Hashmi AT, Lockwood G, Trachtenberg J. Combined T2-weighted and diffusion-weighted MRI for localization of prostate cancer. AJR Am.J.Roentgenol. 2007 Aug;189(2):323-8.
139
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

63. Reissigl A, Pointner J, Strasser H, Ennemoser O, Klocker H, Bartsch G. Frequency and clinical significance of
transition zone cancer in prostate cancer screening. Prostate 1997 Feb 1;30(2):130-5.
64. Villers A, Puech P, Mouton D, Leroy X, Ballereau C, Lemaitre L. Dynamic contrast enhanced, pelvic phased array magnetic resonance imaging of localized prostate cancer for predicting tumour volume: correlation with radical prostatectomy findings. J.Urol 2006 Dec;176(6 Pt 1):2432-7.
140
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6

63. Reissigl A, Pointner J, Strasser H, Ennemoser O, Klocker H, Bartsch G. Frequency and clinical significance of
transition zone cancer in prostate cancer screening. Prostate 1997 Feb 1;30(2):130-5.
64. Villers A, Puech P, Mouton D, Leroy X, Ballereau C, Lemaitre L. Dynamic contrast enhanced, pelvic phased array magnetic resonance imaging of localized prostate cancer for predicting tumour volume: correlation with radical prostatectomy findings. J.Urol 2006 Dec;176(6 Pt 1):2432-7.
140
Multi-parametric MR Imaging for Detection and Localization of Transition Zone Prostate Cancer
6


PART THREE
ASSESSMENT OF PROSTATE CANCER
AGGRESSIVENESS


CHAPTER 7
Relation of Apparent Diffusion Coefficient Values at 3T MRI with Prostate Cancer Gleason Grade in
the Peripheral Zone
T. Hambrock; D. Somford; H. Huisman et al.
CHAPTER 7CHAPTER 7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
Relation of Apparent Diffusion Coefficient Values at 3 Tesla Magnetic Resonance Imaging with Prostate Cancer Gleason Grade in the
Peripheral Zone
Hambrock T, Somford D, Huisman H, van Oort I, Witjes J, Hulsbergen-van de Kaa C, Scheenen T, Barentsz JO
First Prize Award International Cancer Imaging Society, Bath, UK, Oct 2008
Advances in Knowledge
Apparent diffusion coefficient (ADC) values of prostate cancer in the peripheral zone
inversely relate to prostate cancer Gleason grades, with low-, intermediate- and high-
grade tumours showing significant differences in ADC values (p<0.001)
Using the median ADC values of the most aggressive tumour regions a high
discriminatory accuracy is achieved for discerning low-grade from combined
intermediate- and high-grade cancers (AUC=0.90).
Implications for Patient Care
Non-invasive prediction of Gleason grades may improve patient management by more
accurate risk-stratification, follow-up in patients undergoing active surveillance or
targeting biopsies towards the most aggressive components.
Summary Statement
ADC values determined from DW-MR imaging at 3T represents a useful biomarker for prostate cancer aggressiveness in the peripheral
zone.
142
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
ABSTRACT
Purpose: To retrospectively determine the relation of apparent diffusion coefficients (ADC)
from 3 Tesla Diffusion weighted MRI with prostate cancer Gleason grades in the peripheral zone.
Materials and methods: IRB approval was waived. 51 Patients underwent MR imaging prior to
prostatectomy including DWI-MRI using b-values 0, 50, 500 and 800s/mm2. In prostatectomy
specimens, separate slice-by-slice determinations of Gleason grades groups (GGG) based on
primary, secondary and tertiary Gleason grades was done. Additionally, qualitative grade (QG)
groups (low-; intermediate- or high-grade) of tumours were made. ADC maps were aligned to
step-sections and regions-of-interest annotated for each tumour slice. Median ADC (mADC) of
tumours was related to QG groups with a linear mixed model regression analysis. The accuracy
of mADC of the most aggressive tumour component, to differentiate low- from combined
intermediate- and high-grade tumours was summarized using the area (AUC) under the receiver
operating characteristics curve (ROC).
Results: In 51 prostatectomy specimens, 62 different tumours and 251 step-section tumour
lesions were identified. Tumour mADC values showed a negative association with GGG and were
significantly different between the three QG groups (p<0.001). Overall, with an increase of one
QG group, the mADC decreases with 0.18x10-3 mm2/s (±0.02). Low-, intermediate- and high-
grade tumours had a mADC of.1.30±0.30 x10-3 mm2/s, 1.07±0.30 x10-3 mm2/s and 0.94±0.30
x10-3 mm2/s respectively. ROC analysis showed a discriminatory performance of AUC=0.90 in
discerning low-grade from combined intermediate- and high-grade lesions.
Conclusion: 3T ADC values inversely relate to prostate cancer Gleason grades in the peripheral
zone. A high discriminatory performance is achieved in differentiating between low-,
intermediate- and high-grade cancer.
143
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
INTRODUCTION
Gleason grade of prostate cancer is an important determinant of biological activity and
aggressiveness. A vast body of literature has established Gleason score as one of the paramount
pathologic factors in predicting disease outcome in prostate cancer. In fact, the grading scheme
has now become so vital that it is often used as an integral piece of information in both
management and treatment stratification of patients with prostate cancer before and after
definitive therapy(1-5). Pre-treatment knowledge of final Gleason grade would be an important
advance, but currently, such information remains elusive.
Biopsy determination of Gleason grade often does not provide an accurate reflection of final
Gleason Grade, i.e., whole-organ pathology(6-8). Partin tables and risk stratification(9;10)
schemes that incorporate information from biopsy Gleason grades into decision making are
therefore rendered less accurate and less reliable. A definite need for a more accurate and non-
invasive method therefore exists to improve the accuracy of determination of true pretreatment
Gleason grades.
Diffusion Weighted MR imaging (DW-MRI) is a functional imaging technique that quantifies
random Brownian motion properties of water molecules (diffusion) in tissue. The degree of
restriction to water diffusion in biologic tissue is inversely correlated to tissue cellularity and the
integrity of cell membranes(11). Diffusion of molecules also occurs across tissues, especially
from areas of restricted diffusion to areas with free diffusion. The net displacement of molecules
is called the apparent diffusion coefficient (ADC). On MR imaging, the ADC can be calculated by
acquiring two or more images with a different magnetic field gradient duration and
amplitude (b-values). The contrast in the ADC map depends on the spatially distributed
diffusion coefficient of the acquired tissues and does not contain T1 and T2* values (12).
The role of DW-MRI in tumour localization within the prostate has been extensively reported
before(13-16). However, its use in stratifying low and high grade prostate cancer has not
received much attention and is limited to biopsy-determined Gleason grades (17;18).
144
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7 Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
The purpose of our study was to determine the relationship between ADC values from 3T DW-
MRI and peripheral zone (PZ) prostate cancer Gleason grades determine from step-section
specimens after prostatectomy.
MATERIALS AND METHODS
Patients
Between August 2006 and January 2009, 70 consecutive patients with biopsy proven prostate
cancer, scheduled for radical prostatectomy, were referred from the departments of urology at
the Radboud University Nijmegen Medical Centre and the Canisius Wilhelmina Hospital in
Nijmegen, Netherlands, for a clinically routine preoperative MRI of the prostate. The need for
informed consent was waived by the Institutional Review Board.
MR Imaging Protocol
MR imaging was performed using a 3T MR system (Siemens Trio Tim, Erlangen, Germany) with
the use of combined endorectal coil (ERC)(Medrad, Pittsburgh, U.S.A) and pelvic phased array
(PPA) coils. The ERC was filled with a 40-mL Perfluorocarbon preparation (Fomblin;Solvay-
Solexis, Milan, Italy). Peristalsis was suppressed with an intramuscular administration of 20-mg
Butylscopolaminebromide (Buscopan; Boehringer-Ingelheim, Ingelheim, Germany) and 1 mg of
glucagon (Glucagen; Nordisk, Gentofte, Denmark).
The imaging protocol, after evaluation of correct endorectal coil position with fast gradient echo
imaging, included the following sequences: first, T2-weighted turbo spin echo sequences were
performed with an in-plane resolution of 0.4 x 0.4 mm (TR 3250 ms/TE 116 m; flip angle 120;
15-19 slices; 3 mm slice thickness; echo train length 15; 180 x 180 mm field of view and 448 x
145
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
448 matrix) in axial, coronal and sagittal planes, covering the prostate and seminal vesicles.
Second, a single-shot-echo-planar imaging sequence with diffusion module and fat suppression
pulses was implemented. Water diffusion in 3 directions was measured using b-values of 0, 50,
500 and 800 s/mm2 and a TR of 2500ms, TE of 81 ms, parallel imaging factor 3, 15-19 slices,
3mm slice thickness and an in-plane resolution of 1.5 x 1.5 mm. ADC-maps were automatically
calculated by the scanner software using all 4 b-values.
Reconstructed whole-mount step-section preparation
Following radical prostatectomy, prostate specimens were uniformly processed and entirely
submitted for histological investigation. Immediately after surgical resection, specimens were
fixed in 10% neutral-buffered formalin, using fine needle formalin injections and fixation
overnight. Subsequently, the entire surface was marked with ink using three different colours,
after which the entire prostate specimen was cut into serial transverse 4 mm thick slices,
perpendicular to the dorsal-rectal surface and all slices were macroscopically photographed
with a CCD-camera. The apex and base were sagittally sectioned to assess the caudal and cranial
surgical margins. Seminal vesicles were amputated at their junction with the prostate and
sectioned parallel to their junction and embedded in total. The remaining slices were subdivided
into halves or quadrants to fit routine cassettes. After histological staining all specimens were
evaluated by one expert urological pathologist (C.H, 17 years experience). Tumours were
outlined on the microscopic slides and subsequently mapped on the macroscopic photographs
to allow reconstruction of tumour extent and multifocality. Each individual tumour was graded
according to the 2005 ISUP Modified Gleason Grading System (19). Tumours were staged
according to the 2002 TNM classification.
Annotations of MR images
Retrospectively, after radical prostatectomy, annotations of MR images were performed in
consensus by one radiologist (T.H) and one urologist (D.S). To achieve good objective spatial co-
alignment accuracy, a number of strategies were applied. First, both ADC maps and
146
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
prostatectomy step-sections were obtained perpendicular to the dorsal surface of the prostate.
Secondly, a similar slice thickness was chosen. Thirdly, objective mapping of MR slices to
prostatectomy step-sections, was performed by aligning the apex and base on MR and step-
sections in the cranial-caudal direction (Figure1A). Starting from the apex, each consecutive
ADC map was matched to the consecutive pathology step-section. Finally, a per-slice subdivision
was made. On each slice, the PZ and transition zone (TZ) were identified and using the urethra
as reference, the tumour maps were translated to a schematic subdivision of the peripheral zone
(Figure 1B) incl. anterior horns (AH), dorso-lateral region (DL) and dorsal segment (D) in both
left and right halves. The PZ, TZ and urethra are well visible on ADC maps, thus allowing the
schematic subdivision applicable to ADC maps as well. The urethra again served to identify the
AH, DL and D segments. This schematic mapping allowed objective translation of tumour
containing regions from prostatectomy to ADC maps with a high degree of certainty.
A Region-of-Interest (ROI) was annotated and drawn to match the size and extent of the tumour
(ROITumour) determined from histology, as closely as possible (Fig. 1). ROIs were also placed in
the contra lateral segment of the peripheral zone in mirror position (ROINorm_Mirror) to the tumour
and of similar size as the ROITumour. Normal regions were annotated purely to provide a visual
reference of heterogeneity within the peripheral zone compared to tumour values. Each
separate step-section - ADC slice match, was annotated as a different tumour ROI and normal
ROI. Only tumours originating in the peripheral zone were annotated. Annotation of the
following were omitted if applicable: 1) ROITumour of a particular slice if the corresponding
pathology step-section revealed a tumour < 5x5 mm. This was due to the limit in spatial
resolution of the DWI images. 2) ROINorm_Mirror of a particular slices if the tumour was extending
beyond the midline (no mirror possible) or a second tumour was present in the mirror position
of the first tumour,
147
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
Figure 1A. Matching prostatectomy step-sections with ADC maps according to a
systematic method. The prostate was cut into step-sections perpendicular to the dorsal
surface of the prostate (left). According to the number of step-sections obtained, the MR
images were divided into the same number of slices (centre). For each step-section, the
corresponding ADC map was identified.
148
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
B. The step-sections were subsequently schematically subdivided into three different
peripheral zone regions: AH (Anterior Horns), DL (Dorso-lateral) region, D (dorsal)
region. The position of the urethra was identified. The peripheral zone on the
corresponding ADC was similarly divided. The relative position of the tumour (T) was
therefore translatable and annotated on the ADC maps, to match size and distribution of
the tumour.
149
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
Histological tumour grading assessment
Following annotations of ROIs on ADC maps, one radiologist (T.H) together with one
genitourinary pathologist (C.H) re-evaluated all step-sections containing tumour. For each
tumour present in the peripheral zone of the prostate, separate Gleason grades were identified
and quantified in percentages of the tumour section volume. For each step-section, the primary,
secondary and tertiary tumour grade component were noted, referred hereafter as the Gleason
Grade Group. An additional qualitative grading per step-section was also made: a) low-grade
lesion consisting of grade 2 or 3 components only; b) intermediate-grade lesions consisting of
grade 4 as secondary or tertiary component (without any grade 5) c) high-grade lesions
consisting of grade 4 as primary and/or grade 5 as primary, secondary or tertiary component.
Each ROITumour on ADC maps was subsequently correlated to the matching Gleason grade group
and qualitative grade assessments made per step-section slice. An in-house developed MR
analytical software workstation was used to draw ROIs and summarize the median and standard
deviation (SD) of ADC values (in x10-3 mm2/s) calculated for each ROI.
Statistical Analysis
To determine the relation between tumour median ADC (mADC) values and ordinal Gleason
grade groups, a linear mixed effect regression model with random tumour effect was used. This
mixed-model regression analysis incorporates the dependency of repeated measurements
within the same tumour. In an additional mixed-model analysis, the differences in mADC
between the three QG groups were estimated.
Apart from establishing a relation between ADC and Gleason score, the diagnostic accuracy of
using ADC in differentiating low-grade from combined intermediate- and high-grade tumours is
of clinical importance. To this end, for every tumour, the histopathology slice with the highest
Gleason grade was matched to the corresponding ADC slice, thereby identifying the mADC value
matching to the most aggressive part of the tumour. If identical highest Gleason grade
compositions were evident for different slices within the same tumour, the slice showing the
150
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7 Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
lowest mADC was used. The diagnostic accuracy (AUC) of mADC values in discriminating low-
vs. combined intermediate- and high-grade grade groups was quantified with the area under the
receiver operating characteristic curve (ROC). A significant difference was considered when p
<0.05. Statistical analyses were performed with SPSS software (SPSS, version 16.0.01, Chicago,
U.S.A).
RESULTS
Of the 70 consecutive patients, 56 had clinically significant peripheral zone tumours (>0.5cc). In
the remaining 14 patients, 11 patients had transition zone tumours only and in 3 patients,
peripheral zone tumours were < 0.5 cc in volume (with Gleason grade 2/3 components only). In
addition, 5 of the 56 patients were excluded due to: severe motion artifacts (3); widespread
intraprostatic hemorrhage (1) or severe ghosting artifacts on the MRI images (1). In the 51
prostatectomy specimens from these patients, histological analysis revealed a total of 62
different PZ tumours and 251 tumour lesions on different step-sections of the specimens. In
none of the patients tumours were identified with a volume < 0.5 cc and containing a Gleason
grade 4/5 component. In total 14 different Gleason grade groups were identified according to
primary, secondary and tertiary features present. The patient and tumour characteristics are
summarized in Table 1 and the ADC demographics summarized in Table 2.
The tumour mADC values showed an association with the 14 Gleason grade groups (Fig. 2). The
linear mixed model analysis showed an inverse relationship (slope -0.18x10-3 mm2/s, SE ± 0.04,
p<0.001) between the mADC and the three QG groups (Fig. 3). Additional mixed model analysis
revealed that the mADC difference between low- and intermediate grade tumours was 0.22x10-3
mm2/s (SE±0.03)(p<0.001). The difference between intermediate- and high-grade tumours was
0.14x10-3 mm2/s (SE±0.03) (p<0.001) and between low- and high-grade was 0.36x10-3 mm2/s
(SE±0.04) (p<0.001). Low-, intermediate- and high-grade tumours had a mADC of 1.30x10-3
mm2/s (SE±0.30), 1.07x10-3 mm2/s (SE± 0.30) and 0.94x10-3 mm2/s (SE± 0.30), respectively.
Overall, mADC values for mirror normal peripheral zone were 1.60x10-3 mm2/s (SE±0.25).
151
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7 Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
Number of patients 51
Clinical Demographics
- Median PSA ng/ml (range)
- Median Age yrs (range)
6.8 (1.7-42)
64 (49-69)
Pathology Demographics
Stage
- T2a
- T2c
- T3a
- T3b
- T4
5
23
18
4
1
Number of different PZ tumours
- Gleason 3+2
- Gleason 3+3
- Gleason 2+4
- Gleason 3+4
- Gleason 3+4+5
- Gleason 4+3
- Gleason 4+3+5
- Gleason 4+4
- Gleason 4+5
3
18
1
13
4
13
5
2
3
Table1. Patient clinical data, pathological stage , and Gleason Grade
152
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7 Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
Number Median ADC (±SE)
(x10-3s/mm2)
Peripheral Zone lesions
- Gleason 2+3
- Gleason 3+2
- Gleason 2+3+4
- Gleason 3+2+4
- Gleason 3+3
- Gleason 3+3+4
- Gleason 2+4
- Gleason 3+4
- Gleason 3+4+5
- Gleason 4+3
- Gleason 4+3+5
- Gleason 4+4
- Gleason 4+4+5
- Gleason 4+5
251
4
11
3
3
74
3
1
46
8
54
7
17
2
19
1.02 (±0.29)
1.40 (±0.18)
1.16 (±0.14)
0.95 (±0.04)
1.20 (±0.05)
1.36 (±0.26)
1.29 (±0.02)
1.25 (±0)
0.97 (±0.22)
0.99 (±0.11)
0.92 (±0.17)
0.79 (±0.15)
0.68 (±0.13)
0.74 (±0.02)
0.79 (±0.10)
Peripheral Zone lesions
a) Low-grade
b) Intermediate-grade
c) High-grade
94
50
107
1.30 (±0.30)
1.07 (±0.30)
0.94 (±0.30)
Normal mirror PZ 1861
1.60 (±0.25)
Table 2. Gleason grades and ADC Values of 251 Step Sections . 1 In 65 matches no normal
mirror PZ could be annotated due to presence of contra lateral tumour or tumour
extending beyond midline)
153
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
Using ROC analysis of the most aggressive part of the tumour only, mADC was able to
discriminate between low-grade and combined intermediate and high-grade tumours with an
AUC=0.90 (CI 0.81-0.98) (Fig. 4). Furthermore, it was noted that in 94% of tumours (58 of 62),
the ADC slice with lowest mADC for tumour was in exact concordance with the most aggressive
composition slice in pathology. Figure 5 shows the visibility of different grade tumours on ADC
maps.
Figure 2. Association between median tumour ADC vs. Gleason grade groups.
1554
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
154

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
Figure 3. Relation between median ADC vs. Qualitative grade groups and normal mirror
PZ using tumour slice with lowest mADC value. Linear mixed effect regression model
slope estimate -0.18x10-3mm2/s.
155
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
Figure 4. ROC curve of the discriminating performance of mADC to differentiate between
low-grade vs. intermediate- and high-grade lesions using tumour slice with highest
Gleason grade composition.
DISCUSSION
This study has shown that Gleason Grade, and by inference aggressivity, is related to ADC-MRI
values. Using a linear mixed model approach, we determined that the mADC significantly
decreased, on average 0.18x10-3 mm2/s per QG group interval. Further analysis showed a larger
difference in mADC between low and intermediate grade tumours compared to the difference
between mADC of intermediate and high-grade tumours. Using the most aggressive component
within the tumour as end-point, mADC revealed an AUC=0.90 in separating low-grade tumours
from combined intermediate- and high-grade ones.
The Gleason grade sub-grouping allows a better comparison and assessment of the effect of
microscopic glandular differentiation, growth features and structure of different prostatic
156
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
carcinoma sub-grades, on the free diffusivity of water. Correlation of ADC to qualitative grade
groups potentially allows a more practical utilization of the information in routine clinical
decision making, risk stratification and patient tailored treatment options. Furthermore, the
subdivision into low-, intermediate- and high-grade, can allow meaningful cut-off points to be
defined and used to help differentiate patient groups with different prognoses and therefore
different management needs.
DW-MRI is increasingly being incorporated into oncologic imaging and information obtained
from this technique is appealing as an imaging biomarker(20). The low ADC values found in
most tumours has been attributed to increased cellular density but diffusion can also be
influenced by fibrosis, glandular and stromal organization and shape(21). Within the prostate,
the predominant contribution of DW-MRI signal is from the extracellular component (from
tubular structures and their fluid content), with a lesser contribution from the extracellular
stromal space and the intracellular components (epithelial and stromal cells). Because of the
abundant self-diffusion of water molecules within the predominant tubular components within
the peripheral zone, their contents provides a high signal on ADC(22).
A rationale for the relation of prostate cancer aggressiveness with ADC can be suggested from
the current understanding of the structural and organizational features of epithelial, glandular
and extraductal components existing in different grades of cancer(23-25). With increasing
Gleason grade, the change in tissue organization to a more solid and compact architecture (with
higher cellular density) ought to be reflected in restrictions in the distances of free water motion
within the tissue. Well-differentiated prostate carcinomas display tubular formation with a
concomitant higher contribution of unrestricted water motion to ADC values. Lower grade
tumours are also known to have a remarkable heterogeneity in glandular size and ability to
grow between pre-existing ducts. In contrast, poorly-differentiated adenocarcinomas show
more expansile masses of small, tightly packed cell groups with small to absent lumina. Gleason
Grade 2 tumours are defined histologically by tightly packed, well-differentiated glandular
components, while grade 3 tumours show wider spaced tubuli with heterogeneity in ductal size
and density, imposing less restrictions on extra-glandular free water diffusivity motion. This
basis also seems to be reflected in the slightly lower ADC for tumours with grade 2 component
compared to tumours that are purely grade 3. Of the different Gleason grade groups, pure grade
157
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
3 (3+3) tumours show the largest variation in mADC possibly reflecting the heterogeneity of
sparse vs. dense growing lesions, akin to these. A large space for diffusion both between ducts
and within ductal lumina in well-differentiated compared to poorly differentiated tumours is the
most likely explanation for the observed differences in ADC values in low-grade compared to
high-grade tumours.
Despite the fact that true Gleason score is not represented in transrectal ultrasound guided
biopsy cores in 30-50% of patients, biopsy determined GS remains one of the most important
factors in decision-making. An accurate non-invasive method that improves prediction of
prostate cancer GS may allow a significant improvement in patient management by better
treatment selection, performing more targeted and therefore Gleason representative biopsies,
better risk-stratification and follow-up in patients on active surveillance protocols as well as
planning intensity modulated radiotherapy to the dominant aggressive component.
For correlation analysis, each step-section containing tumour was matched to an ADC map as a
separate tumour lesion. The reasoning behind this approach was that tumours display
remarkable intratumoural heterogeneity in their Gleason grade patterns and ability to grow in-
between existing normal ducts and stromal tissue. This is evident for example, when for the
same tumour, different sections reveal pure grade 4 components for the one, a mixed of grade 4
and 3 for another and a pure grade 3 for a final. As the ADC maps and pathology section are
matched to a high degree of certainty and for each an individual Gleason grade and ADC
quantification made, a better matching on the assessment of the effect of Gleason grade on water
diffusivity is obtained. On DWI, the slice with tumour showing the lowest mADC values will in
clinical practice most often be used prospectively to predict aggressivity, guide therapy or direct
targeted biopsies. Because this study was set up as a validation study,, data selection for ROC
analysis was done by choosing the tumour slice with the highest Gleason grade composition (i.e.
tumour slice with the highest proportions of Gleason grade 4 or 5 components). In 94% of
tumours, this was the exact same slice that showed the lowest mADC for the tumour, therefore
indicating that in a prospective setting, using the tumour slice with lowest mADC as starting
point,might be useful.
The clinical relevance of this imaging biomarker has noticeable potential. On a solitary basis,
mADC may contribute in risk-stratifying patients. With a good discriminatory performance
158
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
between low-, intermediate- and high-grade tumours, incorporating this information into
decision-making, will depend on the clinical question and off-course the particular sensitivity
and specificity that is desired. Differentiating men who can be managed expectantly (active
surveillance) from those requiring active management is therefore a potential application of
DWI-MRI (26). Patient with high-grade cancer including Gleason grade 4 as primary, or Gleason
grade 5 as primary, secondary or tertiary pattern, represent a group with a particularly
detrimental prognosis(27-29). Non-invasively identifying these patients before surgery could
be of importance to avoid unnecessary surgery, consider early adjuvant therapy or warrant
additional diagnostic test for metastasis assessment. A prospective advantage of identifying the
most abnormal part of the tumour based on mADC is that this can facilitate targeted biopsies to
obtain cores from the regions with the worst Gleason scores providing a better basis for further
patient management. Furthermore, when focal therapy (i.e. IMRT) is used, the most aggressive
component could receive the highest dose and therefore improve outcome. With currently
available prognostic factors such as preoperative PSA, stage, biopsy Gleason grading, such a
selection cannot be made with sufficient accuracy on an individual level(30). Our findings
suggest a potential role that DWI-MR imaging can play as a non-invasive adjuvant in
characterizing prostatic carcinomas. To which degree our findings will in practice affect
individual patient management, should be assessed by future prospective studies.
Though multi-parametric MR imaging has firmly defined its role in accurately staging and
localizing prostate cancer(31-34), limited data is currently available on the value in improving
the prediction of prostate cancer aggressiveness. A correlation of H-MRS determined
choline+creatine/citrate ratios at 1.5T to prostatectomy GS has been reported(35;36), however,
the overlapping groups appear to be too large to determine meaningful cut-off points. Further
observations have confirmed that T2-w signal intensity correlates to GS(37), as poorly
differentiated tumours are more readily detected on T2-w imaging compared to well
differentiated ones(38). A correlation between ADC values and prostate cancer cellularity,
proliferation activity and density of growth has recently been demonstrated in two studies
(39;40). Additionally, a correlation between ADC and biopsy determined GS has been reported
by Tamada et al.(41). These authors have shown a significant correlation ( =0.497, 0.0001)
of the biopsy Gleason grade findings with ADC. Furthermore, the same visual trend in
159
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
association between Gleason grades and ADC as shown in our Gleason grade group vs. mADC
was also shown.
Our study had a number of limitations. We did not include transition zone (TZ) tumours in this
study. TZ tumours are known to have different genetic mutations, biological behavioral features
and prognoses(42-44). Therefore the conclusions drawn from this study cannot be applied to
TZ tumours which are known to have different ADC values compared to the PZ(45). Another
potential limitation is the reliability of the method of matching axial MR images to step-section
maps from histology we used(31;36;46). We believe that using a number of strategies to
improve the spatial mapping of MR images and step-sections, allowed us to obtain good
matching with a high degree of certainty. Following slice-by-slice matching of step-sections to
ADC maps, we annotated ROIs based on a schematic translation of the ground truth based on
zonal subdivision and urethral land marking.
Having demonstrated the relationship between ADC and tumour aggressivity, in the future it is
necessary to prospectively validate the ability of DW-MR imaging to improve risk stratification
on an individual patient basis, in addition to clinical parameters through a prospective multi-
reader study. Evaluating the impact of such stratification on patient management is also
necessary. Reproducibility of absolute ADC values between vendors and field-strengths as well
as correlating ADC with TZ cancers, should have future priority as well.
CONCLUSIONS
Our conclusions are that quantitative DW-MR imaging may be a well-suited non-invasive
biomarker for prostate cancer aggressiveness. Median tumour ADC values inversely relate to
Gleason grade groups and qualitative grade groups. A high discriminatory accuracy of
AUC=0.90 suggests that ADC will prove to be a useful biomarker that can help improve
identification of patients with particular tumour aggressiveness risk.
160
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
Figure 5. Histological step-section and corresponding ADC maps for three patients with
tumours of different aggressivity. Window levels were kept the same for all patients.
Patient with a low-grade tumour (T) - Gleason grade 3+3 (1) and tumour mADC of 1.24
(x10-3mm2/s). Intermediate-grade tumour Gleason grade 3+4 (2) in patient where
mADC of tumour was 0.99 (x10-3mm2/s). Patient (3) with high-grade tumour Gleason
4+5 with tumour mADC of 0.66 (x10-3mm2/s). Tumour region on ADC indicated with red
dashed ROI.
161
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
REFERENCES
1. Blute ML, Bergstralh EJ, Iocca A, Scherer B, Zincke H. Use of Gleason score, prostate specific antigen, seminal vesicle and margin status to predict biochemical failure after radical prostatectomy. J.Urol. 2001 Jan;165(1):119-25.
2. Brachman DG, Thomas T, Hilbe J, Beyer DC. Failure-free survival following brachytherapy alone or external beam irradiation alone for T1-2 prostate tumours in 2222 patients: results from a single practice. Int.J.Radiat.Oncol.Biol.Phys. 2000 Aug 1;48(1):111-7.
3. Egevad L, Granfors T, Karlberg L, Bergh A, Stattin P. Prognostic value of the Gleason score in prostate cancer. BJU.Int. 2002 Apr;89(6):538-42.
4. Egevad L, Granfors T, Karlberg L, Bergh A, Stattin P. Percent Gleason grade 4/5 as prognostic factor in prostate cancer diagnosed at transurethral resection. J.Urol. 2002 Aug;168(2):509-13.
5. Narain V, Bianco FJ, Jr., Grignon DJ, Sakr WA, Pontes JE, Wood DP, Jr. How accurately does prostate biopsy Gleason score predict pathologic findings and disease free survival? Prostate 2001 Nov 1;49(3):185-90.
6. Divrik RT, Eroglu A, Sahin A, Zorlu F, Ozen H. Increasing the number of biopsies increases the concordance of Gleason scores of needle biopsies and prostatectomy specimens. Urol.Oncol. 2007 Sep;25(5):376-82.
7. Kvale R, Moller B, Wahlqvist R, Fossa SD, Berner A, Busch C, Kyrdalen AE, Svindland A, Viset T, Halvorsen OJ. Concordance between Gleason scores of needle biopsies and radical prostatectomy specimens: a population-based study. BJU.Int. 2008 Dec 22.
8. Rajinikanth A, Manoharan M, Soloway CT, Civantos FJ, Soloway MS. Trends in Gleason score: concordance between biopsy and prostatectomy over 15 years. Urology 2008 Jul;72(1):177-82.
9. Dong F, Kattan MW, Steyerberg EW, Jones JS, Stephenson AJ, Schroder FH, Klein EA. Validation of pretreatment nomograms for predicting indolent prostate cancer: efficacy in contemporary urological practice. J.Urol. 2008 Jul;180(1):150-4.
10. Makarov DV, Trock BJ, Humphreys EB, Mangold LA, Walsh PC, Epstein JI, Partin AW. Updated nomogram to predict pathologic stage of prostate cancer given prostate-specific antigen level, clinical stage, and biopsy Gleason score (Partin tables) based on cases from 2000 to 2005. Urology 2007 Jun;69(6):1095-101.
11. Uhl M, Altehoefer C, Kontny U, Il'yasov K, Buchert M, Langer M. MRI-diffusion imaging of neuroblastomas: first results and correlation to histology. Eur.Radiol. 2002 Sep;12(9):2335-8.
12. Pagani E, Bizzi A, Di SF, De SN, Filippi M. Basic concepts of advanced MRI techniques. Neurol.Sci. 2008 Oct;29 Suppl 3:290-5.
13. Haider MA, van der Kwast TH, Tanguay J, Evans AJ, Hashmi AT, Lockwood G, Trachtenberg J. Combined T2-weighted and diffusion-weighted MRI for localization of prostate cancer. AJR Am.J.Roentgenol. 2007 Aug;189(2):323-8.
14. Kim CK, Park BK, Lee HM, Kwon GY. Value of diffusion-weighted imaging for the prediction of prostate cancer location at 3T using a phased-array coil: preliminary results. Invest Radiol. 2007 Dec;42(12):842-7.
15. Miao H, Fukatsu H, Ishigaki T. Prostate cancer detection with 3-T MRI: Comparison of diffusion-weighted and T2-weighted imaging. Eur.J.Radiol. 2007 Feb;61(2):297-302.
16. Somford DM, Futterer JJ, Hambrock T, Barentsz JO. Diffusion and perfusion MR imaging of the prostate. Magn Reson.Imaging Clin.N.Am. 2008 Nov;16(4):685-95, ix.
17. deSouza NM, Riches SF, Vanas NJ, Morgan VA, Ashley SA, Fisher C, Payne GS, Parker C. Diffusion-weighted magnetic resonance imaging: a potential non-invasive marker of tumour aggressiveness in localized prostate cancer. Clin.Radiol. 2008 Jul;63(7):774-82.
18. Van AN, Charles-Edwards E, Jackson A, Jhavar S, Reinsberg S, Desouza N, Dearnaley D, Bailey M, Thompson A, Christmas T, et al. Correlation of diffusion-weighted MRI with whole mount radical prostatectomy specimens. Br.J.Radiol. 2008 Jun;81(966):456-62.
19. Epstein JI, Allsbrook WC, Jr., Amin MB, Egevad LL. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am.J.Surg.Pathol. 2005 Sep;29(9):1228-42.
162
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
20. Padhani AR, Liu G, Mu-Koh D, Chenevert TL, Thoeny HC, Takahara T, Dzik-Jurasz A, Ross BD, Van CM, Collins D, et al. Diffusion-weighted magnetic resonance imaging as a cancer biomarker: consensus and recommendations. Neoplasia. 2009 Feb;11(2):102-25.
21. Chenevert TL, Sundgren PC, Ross BD. Diffusion imaging: insight to cell status and cytoarchitecture. Neuroimaging Clin.N.Am. 2006 Nov;16(4):619-ix.
22. Tamada T, Sone T, Jo Y, Yamamoto A, Yamashita T, Egashira N, Imai S, Fukunaga M. Prostate cancer: relationships between postbiopsy hemorrhage and tumour detectability at MR diagnosis. Radiology 2008 Aug;248(2):531-9.
23. Histological grading of prostatic carcinoma. In Pathology of the Prostate. Churchill Livingstone; 1990. p. 83-93.
24. Amin MB, Crignon DJ, Humphrey PA, Srigley JR. Gleason Grading of Prostate Cancer: A contemporary apprroach. Lippincott Williams & Wilkins; 2004.
25. Gleason DF. Histologic grading of prostate cancer: a perspective. Hum.Pathol. 1992 Mar;23(3):273-9.
26. Bastian PJ, Carter BH, Bjartell A, Seitz M, Stanislaus P, Montorsi F, Stief CG, Schroder F. Insignificant Prostate Cancer and Active Surveillance: From Definition to Clinical Implications. Eur.Urol. 2009 Mar 6.
27. Chan TY, Partin AW, Walsh PC, Epstein JI. Prognostic significance of Gleason score 3+4 versus Gleason score 4+3 tumour at radical prostatectomy. Urology 2000 Nov 1;56(5):823-7.
28. Hattab EM, Koch MO, Eble JN, Lin H, Cheng L. Tertiary Gleason pattern 5 is a powerful predictor of biochemical relapse in patients with Gleason score 7 prostatic adenocarcinoma. J.Urol. 2006 May;175(5):1695-9.
29. Whittemore DE, Hick EJ, Carter MR, Moul JW, Miranda-Sousa AJ, Sexton WJ. Significance of tertiary Gleason pattern 5 in Gleason score 7 radical prostatectomy specimens. J.Urol. 2008 Feb;179(2):516-22.
30. Epstein JI, Partin AW, Sauvageot J, Walsh PC. Prediction of progression following radical prostatectomy. A multivariate analysis of 721 men with long-term follow-up. Am.J.Surg.Pathol. 1996 Mar;20(3):286-92.
31. Futterer JJ, Heijmink SW, Scheenen TW, Veltman J, Huisman HJ, Vos P, Hulsbergen-Van de Kaa CA, Witjes JA, Krabbe PF, Heerschap A, et al. Prostate cancer localization with dynamic contrast-enhanced MR imaging and proton MR spectroscopic imaging. Radiology 2006 Nov;241(2):449-58.
32. Heijmink SW, Futterer JJ, Hambrock T, Takahashi S, Scheenen TW, Huisman HJ, Hulsbergen-Van de Kaa CA, Knipscheer BC, Kiemeney LA, Witjes JA, et al. Prostate cancer: body-array versus endorectal coil MR imaging at 3 T--comparison of image quality, localization, and staging performance. Radiology 2007 Jul;244(1):184-95.
33. Reinsberg SA, Payne GS, Riches SF, Ashley S, Brewster JM, Morgan VA, deSouza NM. Combined use of diffusion-weighted MRI and 1H MR spectroscopy to increase accuracy in prostate cancer detection. AJR Am.J.Roentgenol. 2007 Jan;188(1):91-8.
34. Tanimoto A, Nakashima J, Kohno H, Shinmoto H, Kuribayashi S. Prostate cancer screening: the clinical value of diffusion-weighted imaging and dynamic MR imaging in combination with T2-weighted imaging. J.Magn Reson.Imaging 2007 Jan;25(1):146-52.
35. Shukla-Dave A, Hricak H, Kattan MW, Pucar D, Kuroiwa K, Chen HN, Spector J, Koutcher JA, Zakian KL, Scardino PT. The utility of magnetic resonance imaging and spectroscopy for predicting insignificant prostate cancer: an initial analysis. BJU.Int. 2007 Jan 11.
36. Zakian KL, Sircar K, Hricak H, Chen HN, Shukla-Dave A, Eberhardt S, Muruganandham M, Ebora L, Kattan MW, Reuter VE, et al. Correlation of proton MR spectroscopic imaging with gleason score based on step-section pathologic analysis after radical prostatectomy. Radiology 2005 Mar;234(3):804-14.
37. Wang L, Mazaheri Y, Zhang J, Ishill NM, Kuroiwa K, Hricak H. Assessment of biologic aggressiveness of prostate cancer: correlation of MR signal intensity with Gleason grade after radical prostatectomy. Radiology 2008 Jan;246(1):168-76.
38. Ikonen S, Karkkainen P, Kivisaari L, Salo JO, Taari K, Vehmas T, Tervahartiala P, Rannikko S. Magnetic resonance imaging of prostatic cancer: does detection vary between high and low gleason score tumours? Prostate 2000 Apr 1;43(1):43-8.
39. Wang XZ, Wang B, Gao ZQ, Liu JG, Liu ZQ, Niu QL, Sun ZK, Yuan YX. Diffusion-weighted imaging of prostate cancer: correlation between apparent diffusion coefficient values and tumour proliferation. J.Magn Reson.Imaging 2009 Jun;29(6):1360-6.
40. Langer DL, van der Kwast TH, Evans AJ, Sun L, Yaffe MJ, Trachtenberg J, Haider MA. Intermixed normal tissue within prostate cancer: effect on MR imaging measurements of apparent diffusion coefficient and T2--sparse versus dense cancers. Radiology 2008 Dec;249(3):900-8.
163
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
41. Tamada T, Sone T, Jo Y, Toshimitsu S, Yamashita T, Yamamoto A, Tanimoto D, Ito K. Apparent diffusion coefficient values in peripheral and transition zones of the prostate: comparison between normal and malignant prostatic tissues and correlation with histologic grade. J.Magn Reson.Imaging 2008 Sep;28(3):720-6.
42. Augustin H, Hammerer PG, Graefen M, Erbersdobler A, Blonski J, Palisaar J, Daghofer F, Huland H. Insignificant prostate cancer in radical prostatectomy specimen: time trends and preoperative prediction. Eur.Urol. 2003 May;43(5):455-60.
43. Guo CC, Zuo G, Cao D, Troncoso P, Czerniak BA. Prostate cancer of transition zone origin lacks TMPRSS2-ERG gene fusion. Mod.Pathol. 2009 Apr 24.
44. Noguchi M, Stamey TA, Neal JE, Yemoto CE. An analysis of 148 consecutive transition zone cancers: clinical and histological characteristics. J.Urol. 2000 Jun;163(6):1751-5.
45. Pickles MD, Gibbs P, Sreenivas M, Turnbull LW. Diffusion-weighted imaging of normal and malignant prostate tissue at 3.0T. J.Magn Reson.Imaging 2006 Feb;23(2):130-4.
46. Jager GJ, Ruijter ET, van de Kaa CA, de la Rosette JJ, Oosterhof GO, Thornbury JR, Barentsz JO. Local staging of prostate cancer with endorectal MR imaging: correlation with histopathology. AJR Am.J.Roentgenol. 1996 Apr;166(4):845-52.
164
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7

Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7
41. Tamada T, Sone T, Jo Y, Toshimitsu S, Yamashita T, Yamamoto A, Tanimoto D, Ito K. Apparent diffusion coefficient values in peripheral and transition zones of the prostate: comparison between normal and malignant prostatic tissues and correlation with histologic grade. J.Magn Reson.Imaging 2008 Sep;28(3):720-6.
42. Augustin H, Hammerer PG, Graefen M, Erbersdobler A, Blonski J, Palisaar J, Daghofer F, Huland H. Insignificant prostate cancer in radical prostatectomy specimen: time trends and preoperative prediction. Eur.Urol. 2003 May;43(5):455-60.
43. Guo CC, Zuo G, Cao D, Troncoso P, Czerniak BA. Prostate cancer of transition zone origin lacks TMPRSS2-ERG gene fusion. Mod.Pathol. 2009 Apr 24.
44. Noguchi M, Stamey TA, Neal JE, Yemoto CE. An analysis of 148 consecutive transition zone cancers: clinical and histological characteristics. J.Urol. 2000 Jun;163(6):1751-5.
45. Pickles MD, Gibbs P, Sreenivas M, Turnbull LW. Diffusion-weighted imaging of normal and malignant prostate tissue at 3.0T. J.Magn Reson.Imaging 2006 Feb;23(2):130-4.
46. Jager GJ, Ruijter ET, van de Kaa CA, de la Rosette JJ, Oosterhof GO, Thornbury JR, Barentsz JO. Local staging of prostate cancer with endorectal MR imaging: correlation with histopathology. AJR Am.J.Roentgenol. 1996 Apr;166(4):845-52.
164
Relation of ADC Values at 3T MRI with Prostate Cancer Gleason Grade in the Peripheral Zone
7


— CHAPTER 8 —
Initial Experience with Identifying High-Grade Prostate Cancer using
Diffusion-Weighted MRI in Patients
Schematic TRUS-guided Biopsy.
T. Hambrock; D. Somford; van Oort et al.
CHAPTER 8CHAPTER 8

Initial Experience with Identifying High-grade Prostate Cancer using Diffusion Weighted Magnetic Resonance Imaging in Patients with a
Gleason Score Biopsy. A radical Prostatectomy Correlated Series.
Hambrock T, Somford D, van Oort I, Witjes J, Hulsbergen-van de Kaa C, van Basten J, Fütterer J, Barentsz J
Advances in Knowledge
Transrectal ultrasound guided biopsies of the prostate substantially undergrade prostate
cancer tumours.
Quantitative 3T Diffusion Weighted Imaging is able to accurately differentiate patients
e cancer who represent undergrading of true
Gleason score from those subjects where it is a correct assessment of true Gleason score
at radical prostatectomy
A high diagnostic accuracy using ADC values is achieved in separating patients with low
and high-grade prostate cancer.
Implications for Patient Care
Accurate pretreatment assessment of true prostate aggressiveness is of paramount
importance in selecting optimal treatment methods.
3T DWI imaging can be a valuable method in assessing pretreatment aggressiveness and
should be part of any patient diagnosed with prostate cancer.
Summary Statement
3T DWI MR imaging is a very valuable technique for accurately identifying patients in whom biopsies represent an underestimation
of prostate cancer aggressiveness.
166
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

ABSTRACT
Introduction: Diffusion-weighted magnetic resonance (MR) Imaging (DWI) might be able to
fulfill the need to accurately identify high-grade prostate carcinoma, in patients initially selected
for active surveillance in the PSA screening era based upon transrectal ultrasound (TRUS)-
guided biopsy Gleason score. We aimed to retrospectively determine whether DWI is able to
and/or 5 components in their radical prostatectomy (RP) specimen.
Materials and methods: Whole-mount RP specimens were used to identify regions of interest
(ROI) corresponding with tumour on the DWI-derived Apparent Diffusion Coefficient (ADC)
maps in 23 patients with a Glea ADC values were correlated with RP
Gleason grades. Statistical analysis was performed using the area under the ROC-curve (AUC) of
median ADC to separate patients with Gleason 4 and/or 5 components vs. those without. Mann-
Whitney U-testing was performed to detect differences in mean ADC values for tumours with
Results: Median ADC values had an AUC of 0.88 for identifying patients subject to TRUS-guided
biopsy undergrading using RP Gleason score as a reference. In patients harboring a Gleason 4
and/or 5 component the median ADC was 0.86 x10-3 mm2/s (±0.21), whereas patients harboring
no Gleason 4 and/or 5 component displayed a median ADC of 1.16x10-3 mm2/s (±0.19) for the
single tumour slice with lowest median ADC (p<0.002).
Conclusions: 3T DWI is accurate in predicting the presence of high-grade tumour in patients
wi
treatment selection.
167
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

INTRODUCTION
PSA testing for prostate carcinoma has led to earlier detection of prostate carcinoma in most
men, with a tendency to downstaging for the entire population(1;2). Recent publications from
the ERSPC trial showed a significant prostate cancer mortality reduction from PSA screening,
however at the cost of 1410 men screened and, more importantly, 48 additional cases of
prostate cancer treated to prevent one prostate cancer death(3).
The dilemma of the clinical insignificant tumour has been addressed with increasing frequency
and would even become more important with the implementation of PSA screening(4;5). In a
recent European Association of Urology position statement on PSA screening for prostate
cancer, the authors underline the paramount importance of the development of reliable
monitoring and prognostic markers and/or imaging modalities to prevent overtreatment before
widespread implementation of population-based PSA screening (6). Clinical staging and accurate
grade assessment of prostate carcinoma has become of utmost importance in decision making
regarding the need for active treatment at any time point following the diagnosis of prostate
cancer in individual cases.
Accurate identification of insignificant and/or low-risk prostate carcinoma remains the
cornerstone of selection of patients for active surveillance, but is currently severely hampered
by absence of reliable pre-treatment predictors(7;8). PSA levels in patients with histological
proven prostate carcinoma do grossly correlate with the risk of extraprostatic extension (EPE),
seminal vesicle invasion and positive surgical margins, but correlate poorly with
differentiation(9). Other prostate cancer markers, such as PCA3 or hK2, have not been able to
identify low-risk prostate cancers with sufficient accuracy for clinical decision making(10;11). In
current practice, transrectal ultrasound (TRUS)-guided schematic prostate biopsies are the
predominant method to obtain a histological diagnosis of prostate carcinoma and to determine
pathological characteristics of the tumour. Subsequently, biopsy-determined combined Gleason
score remains a cornerstone of pre-treatment risk stratification for localized prostate carcinoma.
However, when correlated with radical prostatectomy (RP) specimens, Gleason grading
obtained by TRUS-guided biopsy has been shown to underestimate tumour Gleason score in up
to 40% of cases(12;13), a phenomenon further referred to as Gleason undergrading in this
paper.
RP series including patients considered eligible for active surveillance according to
contemporary inclusion criteria showed that up to 27% of patients had a Gleason score of at
least 7 upon RP(14;15). An active surveillance series by Duffield et al. outlined that most
168
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

patients progressing on such a protocol did so 1 to 2 years after diagnosis, suggesting significant
undergrading upon initial TRUS-guided biopsy(16). Only 52% of patients consequently
need
for more accurate grading and staging of prostate carcinoma precluding inclusion in active
surveillance protocols.
Diffusion-weighted magnetic resonance (MR) Imaging (DWI) is a functional MR technique that
quantifies the freedom of movement of protons, predominantly a part of water molecules in
tissue. In prostate carcinoma the diffusion of water will be limited due to increased cellular
density of tumour compared with normal glandular prostate tissue, leading to lower apparent
diffusion coefficient (ADC) levels in prostate carcinoma when compared with benign prostate
tissue(17). Previous reports on the value of DWI in the detection and localization of prostate
cancer have been published(18-20). Furthermore the correlation of ADC to tumour Gleason
score and tumour volume has recently been shown(21-23). Therefore, another merit of DWI
might be in correctly identifying those patients that would have been selected for active
surveillance protocols based on their TRUS-guided bio
Gleason 4 and/or 5 components not sampled by random biopsies. In this series we aimed to
establish the potential value of DWI to identify patients subject to pre-operative Gleason
undergrading by TRUS-guided biopsy, using RP Gleason score as a gold standard, thus enabling
more accurate pre-treatment risk stratification and treatment decision making.
MATERIALS AND METHODS
Study population
Inclusion criteria were histologically proven prostate cancer with a Gleason s
upon TRUS-guided biopsy in patients consequently scheduled for radical prostatectomy (RP).
Patients were referred for MRI from two hospitals, following the histological diagnosis of
prostate cancer by 8-10 core schematic TRUS-guided biopsies. In these patients, endorectal coil
multi-parametric MR imaging at 3 Tesla (3T) preceding RP was performed. Patients in whom the
diagnosis of prostate cancer was established using MR-guided biopsy were excluded. Patient
characteristics for the complete cohort were registered.
169
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

Imaging parameters
MR imaging of the prostate was performed using a 3T MR scanner (Siemens Trio Tim, Erlangen,
Germany) combined with an endorectal coil (Medrad, Pittsburgh, USA) in combination with a
pelvic phased array coil. The routine MR imaging protocol consisted of anatomical T2-weighted
turbo spin echo sequences in the axial, sagittal and coronal direction, covering the prostate and
seminal vesicles. Axial images were obtained perpendicular to the dorsal surface of the prostate
to facilitate comparison with whole-mount sectioned RP specimens. DWI was performed using a
fat saturated single-shot-echo-planar imaging sequence with 3-scan trace imaging with b-values
of 0, 50, 500, and 800 s/mm2. DWI images were obtained in 4:32 min. The scanner software
automatically calculated ADC maps using all b-values. Further imaging parameters are shown in
table 1.
Sequence
name Sequence
Type
TR (ms) TE (ms) Voxel size Slice thickness
b-values FOV (mm)
Matrix
T2-w axial TSE 3250 ms 108 ms 0.4x0.4 mm 3 mm - 192 448
T2-w coronal TSE 4100 ms 108 ms 0.5x0.5 mm 3 mm - 192 384
T2-w sagital TSE 3760 ms 108 ms 0.5x0.5 mm 3 mm - 192 384
DWI axial SS-EPI 2700 ms 81 ms 1.5x1.5 mm 3 mm 0, 50, 500, 800
180 120
Table 1. Imaging parameters at 3T. TSE = Turbo Spin Echo; SS-EPI = Single Shot Echo
Planar Imaging; TR = Repitition time; TE = Echo time; ms = milliseconds; b-values in
s/mm2; FOV = Field of view.
Specimen handling
Following RP, prostate specimens were fixed overnight in 10% neutral buffered formaldehyde
and routinely processed according to protocol(24). In brief, after inking of the surface, the
prostate specimen was cut into serial transverse 3-4 mm thick slices, perpendicular to the
dorsal-rectal surface and all slices were macroscopically photographed. The apex and base were
sagittally sectioned to assess the caudal and cranial surgical margins. Seminal vesicles were
amputated at their junction with the prostate and sectioned parallel to their junction and
embedded in total. The remaining slices were subdivided into halves or quadrants to fit routine
cassettes. After histological staining, all specimens were evaluated by one expert urological
170
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

pathologist (CH). Tumours were outlined on the microscopic slides and subsequently mapped
on the macroscopic photographs to allow reconstruction of tumour extent and multifocality. For
every RP specimen and for each separate tumour, the presence of each primary, secondary and
tertiary Gleason grade pattern as well as a combined Gleason score was recorded. For every
tumour slice a separate Gleason grade assessment was made. The presence of EPE was reported
for all cases.
Data retrieval
Retrospectively, after radical prostatectomy, annotations of MR images were performed in
consensus by one urologist (DS) and one radiologist (TH). To achieve good objective spatial co-
alignment accuracy, a number of strategies were applied. First, both ADC maps and
prostatectomy step-sections were obtained perpendicular to the dorsal surface of the prostate.
Secondly, a similar slice thickness was chosen. Thirdly, objective mapping of MR slices to RP
step-sections, was performed by aligning the apex and base on MR and step-sections in the
cranial-caudal direction. Starting from the apex, each consecutive ADC map was matched to the
consecutive pathology step-section. Finally, a per-slice subdivision was made. On each slice, the
peripheral zone (PZ) and transition zone (TZ) were identified and using the urethra as
reference, the tumour maps were translated to a schematic subdivision of the PZ (Figure 1)
including anterior horns, dorsolateral region and dorsal segment in both left and right halves.
The PZ, TZ and urethra are well visible on ADC maps, thus allowing the schematic subdivision
applicable to ADC maps as well. This schematic mapping allowed objective translation of
tumour containing regions from RP to ADC maps with a high degree of certainty. A region of
interest (ROI) was annotated and drawn to match the size and extent of the tumour determined from histology, as closely as possible. Separate ROI’s were placed on every ADC slice containing tumour. Therefore, for each tumour, multiple ROI’s were determined, depending on the tumour
extent on different step-sections. Tumour foci with a inplane area less than 5x5 mm were
excluded from analysis due to the limit in spatial resolution obtained with DWI (inplane voxel
sizes 1.5 x 1.5 mm).
171
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

Figure 1. Schematic translation of tumour regions from macroscopic step-section
histopathology maps to ADC maps. Left image shows prostatectomy step-section with
tumour in the left-peripheral zone. The middle image shows the subdivision of the
prostate in the peripheral zone (PZ – red dashed lines) and transition zone (TZ – blue
dashed line). The urethra (U) is identified in the centre. The peripheral zone is
furthermore subdivided using the urethra as reference landmark into left and right
anterior horns (AH), dorsolateral regions (DL) and dorsal (D) region. The schematic
subdivision is anatomically translated to the corresponding ADC maps (image on right)
with tumour translated and annotated in yellow dashed lines. For each tumour slice, the
pathologist made a separate mention of the presence and proportions of the primary,
secondary and tertiary Gleason grade components. Prim.= Primary; Second. = Secondary;
Tert. = Tertiary. From each of the designated ROI’s, median ADC values were calculated on a per-slice basis.
Following median ADC estimation, for the purpose of this study, the index tumour was identified
as the tumour within the whole RP specimen revealing the highest Gleason Score and having a
tumours revealed the same Gleason score, the tumour with the
largest volume was subsequently identified as the index tumour. For this tumour only, the slice
with the lowest median ADC was used for further analysis. As prior studies have identified ADC
values to correlate with Gleason score, the assumption was made that the region within the
tumour with the lowest ADC should also reflect the region with largest proportions of highest
Gleason grade components. To validate this, for the index tumour, the pathology slice with
highest Gleason grade components were matched to the corresponding ADC slices.
Subsequently this ADC slice was evaluated if it also represented the ADC slice where the lowest
median ADC value was identified. In addition, the index tumour volume and zonal location was
also noted
172
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

Statistical analysis
-guided biopsy were stratified according to
their final radical prostatectomy revealing the presence or absence of a Gleason 4 and/or 5
component. This resulted in two groups. The first, where the TRUS-guided biopsy Gleason score
and the second, where TRUS-guided
for the tumour slice with lowest ADC values was identified and matched to these two groups.
Area-under the receiver operating characteristic (AUC) curves were determined for the median
for median PSA values predicting correct Gleason grading versus Gleason undergrading was
calculated. The Mann-Witney U-test was performed to determine whether there was a
significant difference in mean PSA, mean ADC (of the single slice with the lowest median tumour
ADC) and mean index tumour volume for these groups. Level of significance was set at P<0.05.
Statistical analysis was performed using SPSS software (SPSS, version 16.0.01, Chicago, Illinois,
USA.)
RESULTS
Twenty-three patients with a TRUS- -
parametric 3T MR imaging before RP. The mean age was 61 years (range 42 - 69) with a mean
PSA of 8.0 ng/ml (range 1.7 - 37.5). In 23 prostatectomies, 56 different tumours were found.
The prevalence of PZ tumours was 68% (38/56) and for TZ tumours this was 32% (18/56).
In all patients, one index prostate cancer exceeding a volume of 0.2cc in the RP specimen was
identified. The median index tumour volume was 4.09 cc (range 0.31 – 28cc). Almost all index
tumour were located in the PZ (96%; 22/23). In one patient tumour substantially involved both
the PZ and TZ, therefore primary zone of origin was not determinable. A summary of the patient
and pathology characteristics is provided in Table 2.
Eleven of the 23 (48%) included patients had a primary or secondary Gleason 4 and/or 5
component in their final RP specimen, leaving 12 cases that were correctly identified as low-
grade prostate cancer by pre-operative TRUS-guided biopsy. Patients subject to Gleason
undergrading had a median PSA of 6.10 (range 1.7 - 37.5), while patients with a Gleason score of
RP had a median PSA of 6.08 (range 2.2 - 9.8; p=0.11). Furthermore, the median
index tumour volume in patients with Gleason undergrading was 6.62 cc (range 0.31 – 28 cc)
173
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

nge 0.36 –
10.01; p=0.006). None of the patients correctly identified by TRUS-guided biopsy as Gleason
undergraded by TRUS-guided biopsy displayed EPE upon RP.
The diagnostic accuracy of median ADC in correctly discriminating patients subject to pre-
operative Gleason undergrading was an AUC of 0.88 (95% CI: 0.64-1.00) (figure 2). In patients
harboring a primary or secondary Gleason 4 and/or 5 component the median ADC was 0.86 x
10-3 mm2/s (SD±0.21), whereas patients harboring no Gleason 4 and/or 5 component displayed
a significantly higher median ADC of 1.16x10-3 mm2/s (SD±0.19; p<0.002) for the tumour slice
with the lowest ADC (figure 3).
Retrospective analysis revealed that the index tumour slice with the lowest median ADC in all
patients also corresponded with the highest Gleason grade component of the tumour upon RP.
The diagnostic accuracy of mean PSA values in discriminating patients into these two groups
revealed an AUC of 0.58 (95% CI: 0.32 – 0.83).
No Undergrading Undergrading p-values
Number 12 11 N.A.
Median PSA value ng/ml (range) 6.08 (2.2 - 9.8) 6.10 (1.7 - 37.5) 0.11
Median Index Tumour Volume cc (range)
2.59 (0.36 – 10.01) 6.62 (0.31 – 28) 0.006 *
Stage T3 disease 0% (0/12) 82% (9/11) N.A.
Median ADC values x10-3 mm2/s (±SD) 1.16 (±0.19) 0.86 (±0.21) 0.002 *
Table 2. Patient, pathology and ADC characteristics
174
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

Figure 2. ROC curve for differentiation of low-grade (no Gleason 4 and/or 5 component)
and high-grade prostate carcinoma upon RP using median ADC in a TRUS-biopsy Gleason
Figure 3. Box-plot of median ADC of low-grade (no primary or secondary Gleason 4
and/or 5 component) and high-grade prostate carcinoma upon RP in a TRUS-biopsy
175
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

DISCUSSION
In this study we have primarily shown that median quantitative ADC values obtained from 3T
prostate cancer upon TRUS-guided biopsy represents undergrading of true Gleason score from
those subjects where it is a correct assessment of true Gleason score at radical prostatectomy.
Because it is known that biopsy Gleason score is a poor predictor of true Gleason score identified
in RP, a definite need exists to improve identification of undergraded patients as this has
important implications in treatment selection and prognostication. From our results, it seems
that DWI has a strong potential to fill this current gap in pretreatment aggressiveness
determination for prostate cancer.
DWI has been established to reliably localize areas of prostate cancer within a 3T multi-
parametric MR imaging approach. Reported ADC values for prostate cancer (1.13 – 1.38x10-3
mm2/s) and normal prostate tissue (1.58 – 1.95x10-3 mm2/s) differ widely (20;25;26), which to
some degree can be explained by different sequences using varied b-values, and thus obtaining
different levels of diffusion-weighting. Also, population-based differences in Gleason score
prevalences can also account for differences in ADC values for prostate cancer in different series.
Reliable pre-treatment grading of prostate cancer remains a major issue, especially with the
emergence of active surveillance programs for low-risk prostate cancer and the growing interest
for focal ablative therapies. A RP correlated series by Haider et al. showed a very promising role
of DWI in combination with T2-weighted imaging in the detection of significant prostate cancer,
tumour diameter > 4mm. They reported a sensitivity of 81%
and a specificity of 84% for T2-weighted MRI and DWI combined(27).
ADC-values have been shown to correlate with cellular density in human cancers. The
proliferative activity of low-grade prostate cancer is relatively lower than that of higher-grade
cancers. Low-grade tumours reveal low tumour cellularity, intermixed with various amounts of
normal prostatic stroma and glands as well as showing larger extracellular and glandular
luminal spaces compared with higher-grade tumours. The latter are characterized by higher
cellularity density and loss of glandular duct formation (28;29). As a consequence, the space for
free water movement both intraluminally and extracellularly, reduces, the higher the grade of
the tumour becomes. Based on the results from Wang et al.(30) it is evident that the ADC of
prostate cancer decreased with an increase in tumour cellularity and proliferation rate. This
association has also been shown by Zelhof et al(31).
176
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

Apart from inherent tumour cellularity, the degree of tumour intermixing with normal prostatic
tissue, also infers variation in ADC values between tumours. Langer et al.(32) identified sparse
vs. dens growing prostate tumours and determined a correlation with ADC. They identified that
all sparse growing tumours Therefore,
it appears that inherent tumour cellularity (which is related to the Gleason grade) as well as
intermixing pattern, are important factors that influence the diffusion characteristics of prostate
cancer on ADC.
The ability of ADC to predict biopsy Gleason score has been established in several series(33-35),
but this approach is methodologically hampered by the well-known phenomenon of Gleason
undergrading of true combined Gleason score by pre-operative biopsies. Two earlier reports on
the correlation of ADC and radical prostatectomy Gleason score have recently been published
showing a high diagnostic accuracy of ADC in predicting high-grade prostate cancer(36;37). To
our knowledge we are the first to report on the use of DWI in identifying patients subject to
Gleason undergrading upon TRUS-guided biopsy.
For selection of patients for active surveillance protocols or focal therapy, a reliable technique
with a high sensitivity for any Gleason 4 and/or 5 component could be a parameter of
paramount importance to increase reliability and safety of such protocols. In this retrospective
series we were able to identify cases subject to pre-operative biopsy Gleason undergrading with
great accuracy using median ADC of the most aggressive part of the tumour. It is also known that
higher PSA values as such are associated with increased odds of undergrading by TRUS biopsies.
Isariyawongse et al.(38) have shown that patients with PSA values between 10-20 ng/ml had
odds ratios of 2.11 compared to patients with PSA < 10 ng/ml for representing undergrading of
true GS in prostatectomy. Despite this, PSA values alone are insufficient for accurate
stratification in this regard. This was reaffirmed by the relative poor AUC of 0.58 achieved using
PSA values as classifier.
A major limitation of our series might be the establishment of pre-operative Gleason score based
upon 8-10 core TRUS-guided biopsies. However, while more extensive TRUS-guided biopsy
schemes have been shown to improve detection rates and decrease the rate of Gleason
undergrading, this issue still remains substantial(39). We therefore are of the opinion that the
effect of more TRUS-guided biopsies taken might not have altered the outcome of our series
significantly; further investigation in a series with extended biopsy schemes is however
warranted.
177
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

A fur
TRUS-guided biopsy for our analysis. However, as the clinical approach is based on a biopsy
-guided biopsy as representative of the true tumour features,
we opted to only include these patients for this series. This however resulted in a fairly low
number of patients in each subgroup. A further drawback is that although TZ tumours
represented 32% of all tumours found in our patients, the index tumour in 96% of patients (22
of 23) was a peripheral zone tumour. Because the normal TZ and PZ are known to have different
ADC values, our results may therefore be biased towards revealing the discriminatory
performance of ADC more in the light of PZ tumour undergrading. The larger cohort with more
patients harboring TZ index tumour undergrading is needed to view the value of ADC in a larger
perspective.
CONCLUSIONS
DWI has been established as a diagnostic modality in oncology now for over a decade. Its main
merits lie in the detection of solid tumour within surrounding normal tissue and more recently
research has focused upon the ability of DWI to characterize aggressiveness of tumours. We
confirmed this potential of DWI to characterize prostate cancer aggressiveness. DWI should be
an integral part of any multi-parametric MRI approach for prostate cancer, whether localizing or
characterizing the tumour is the aim. Its main contribution to the diagnostic arena for prostate
cancer might lie in its ability to identify high-grade components in prostate cancer precluding
adequate pre-treatment risk stratification and aiding in therapeutic decision making.
Prospective research will need to focus upon the performance of DWI in candidates for active
surveillance to predict and evaluate progression to curative therapy.
178
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

Figure 4. Patient with biopsy Gleason 3+3=6 and PSA 5.2 ng/ml. Histopathological step
sections 1a - 3a reveal the extent of prostate carcinoma in the peripheral zone (light-blue
area). For every seperate slice, a Gleason grade composition expressed in grade and
percentage of tumour region is given. Every histopathology slice is matched to the
corresponding ADC map (1b - 3b) and the tumour containing region translated for
placement of a ROI placed over the tumour. For each ADC slice, a seperate median ADC
(mADC) value was calculated. The mADC values are expressed in x10-3 mm2/s. The
region of tumour with the largest proportion of higher Gleason grades (3a) corresponds
also to the slice with the lowest mADC tumour values (3b). The window level for ADC
maps are defined to range from 0.5 - 1.5 x 10-3 mm2/s. A small additional insignificant
transition zone tumour (green region) is also shown in 1a. The red line indicates the area
of extraprostatic extension. The final diagnosis on RP was Gleason 3+4=7, stage pT3a.
179
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

REFERENCES
1. Postma R, Schroder FH, van Leenders GJ, Hoedemaeker RF, Vis AN, Roobol MJ, van der Kwast TH. Cancer detection and cancer characteristics in the European Randomized Study of Screening for Prostate Cancer (ERSPC)--Section Rotterdam. A comparison of two rounds of screening. Eur.Urol. 2007 Jul;52(1):89-97.
2. Cremers RG, Karim-Kos HE, Houterman S, Verhoeven RH, Schroder FH, van der Kwast TH, Kil PJ, Coebergh JW, Kiemeney LA. Prostate cancer: trends in incidence, survival and mortality in the Netherlands, 1989-2006. Eur.J.Cancer 2010 Jul;46(11):2077-87.
3. Schroder FH, Hugosson J, Roobol MJ, Tammela TL, Ciatto S, Nelen V, Kwiatkowski M, Lujan M, Lilja H, Zappa M, et al. Screening and prostate-cancer mortality in a randomized European study. N.Engl.J.Med. 2009 Mar 26;360(13):1320-8.
4. Augustin H, Hammerer PG, Graefen M, Erbersdobler A, Blonski J, Palisaar J, Daghofer F, Huland H. Insignificant prostate cancer in radical prostatectomy specimen: time trends and preoperative prediction. Eur.Urol. 2003 May;43(5):455-60.
5. Jeldres C, Suardi N, Walz J, Hutterer GC, Ahyai S, Lattouf JB, Haese A, Graefen M, Erbersdobler A, Heinzer H, et al. Validation of the contemporary epstein criteria for insignificant prostate cancer in European men. Eur.Urol. 2008 Dec;54(6):1306-13.
6. Abrahamsson PA, Artibani W, Chapple CR, Wirth M. European Association of Urology Position Statement on Screening for Prostate Cancer. Eur.Urol. 2009 May 19.
7. Anast JW, Andriole GL, Bismar TA, Yan Y, Humphrey PA. Relating biopsy and clinical variables to radical prostatectomy findings: can insignificant and advanced prostate cancer be predicted in a screening population? Urology 2004 Sep;64(3):544-50.
8. Bastian PJ, Carter BH, Bjartell A, Seitz M, Stanislaus P, Montorsi F, Stief CG, Schroder F. Insignificant Prostate Cancer and Active Surveillance: From Definition to Clinical Implications. Eur.Urol. 2009 Mar 6.
9. Freedland SJ, Hotaling JM, Fitzsimons NJ, Presti JC, Jr., Kane CJ, Terris MK, Aronson WJ, Amling CL. PSA in the new millennium: a powerful predictor of prostate cancer prognosis and radical prostatectomy outcomes--results from the SEARCH database. Eur.Urol. 2008 Apr;53(4):758-64.
10. Raaijmakers R, de Vries SH, Blijenberg BG, Wildhagen MF, Postma R, Bangma CH, Darte C, Schroder FH. hK2 and free PSA, a prognostic combination in predicting minimal prostate cancer in screen-detected men within the PSA range 4-10 ng/ml. Eur.Urol. 2007 Nov;52(5):1358-64.
11. Hessels D, van Gils MP, van HO, Jannink SA, Witjes JA, Verhaegh GW, Schalken JA. Predictive value of PCA3 in urinary sediments in determining clinico-pathological characteristics of prostate cancer. Prostate 2010 Jan 1;70(1):10-6.
12. Fine SW, Epstein JI. A contemporary study correlating prostate needle biopsy and radical prostatectomy Gleason score. J.Urol. 2008 Apr;179(4):1335-8.
13. Narain V, Bianco FJ, Jr., Grignon DJ, Sakr WA, Pontes JE, Wood DP, Jr. How accurately does prostate biopsy Gleason score predict pathologic findings and disease free survival? Prostate 2001 Nov 1;49(3):185-90.
14. Griffin CR, Yu X, Loeb S, Desireddi VN, Han M, Graif T, Catalona WJ. Pathological features after radical prostatectomy in potential candidates for active monitoring. J.Urol. 2007 Sep;178(3 Pt 1):860-3.
15. Louie-Johnsun M, Neill M, Treurnicht K, Jarmulowicz M, Eden C. Final outcomes of patients with low-risk prostate cancer suitable for active surveillance but treated surgically. BJU.Int. 2009 Nov;104(10):1501-4.
16. Duffield AS, Lee TK, Miyamoto H, Carter HB, Epstein JI. Radical prostatectomy findings in patients in whom active surveillance of prostate cancer fails. J.Urol. 2009 Nov;182(5):2274-8.
17. Somford DM, Futterer JJ, Hambrock T, Barentsz JO. Diffusion and perfusion MR imaging of the prostate. Magn Reson.Imaging Clin.N.Am. 2008 Nov;16(4):685-95, ix.
18. Haider MA, van der Kwast TH, Tanguay J, Evans AJ, Hashmi AT, Lockwood G, Trachtenberg J. Combined T2-weighted and diffusion-weighted MRI for localization of prostate cancer. AJR Am.J.Roentgenol. 2007 Aug;189(2):323-8.
19. Hosseinzadeh K, Schwarz SD. Endorectal diffusion-weighted imaging in prostate cancer to differentiate malignant and benign peripheral zone tissue. J.Magn Reson.Imaging 2004 Oct;20(4):654-61.
20. Mazaheri Y, Shukla-Dave A, Hricak H, Fine SW, Zhang J, Inurrigarro G, Moskowitz CS, Ishill NM, Reuter VE, Touijer K, et al. Prostate cancer: identification with combined diffusion-weighted MR imaging and 3D 1H MR spectroscopic imaging--correlation with pathologic findings. Radiology 2008 Feb;246(2):480-8.
21. Mazaheri Y, Hricak H, Fine SW, Akin O, Shukla-Dave A, Ishill NM, Moskowitz CS, Grater JE, Reuter VE, Zakian KL, et al. Prostate tumour volume measurement with combined T2-weighted imaging and diffusion-weighted MR: correlation with pathologic tumour volume. Radiology 2009 Aug;252(2):449-57.
180
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8

22. Verma S, Rajesh A, Morales H, Lemen L, Bills G, Delworth M, Gaitonde K, Ying J, Samartunga R, Lamba M.
Assessment of aggressiveness of prostate cancer: correlation of apparent diffusion coefficient with histologic grade after radical prostatectomy. AJR Am.J.Roentgenol. 2011 Feb;196(2):374-81.
23. Hambrock T, Somford DM, Huisman HJ, van O, I, Witjes JA, Hulsbergen-van de Kaa CA, Scheenen T, Barentsz JO. Relationship between Apparent Diffusion Coefficients at 3.0-T MR Imaging and Gleason Grade in Peripheral Zone Prostate Cancer. Radiology 2011 May;259(2):453-61.
24. van O, I, Bruins HM, Kiemeney LA, Knipscheer BC, Witjes JA, Hulsbergen-van de Kaa CA. The length of positive surgical margins correlates with biochemical recurrence after radical prostatectomy. Histopathology 2010 Mar;56(4):464-71.
25. Pickles MD, Gibbs P, Sreenivas M, Turnbull LW. Diffusion-weighted imaging of normal and malignant prostate tissue at 3.0T. J.Magn Reson.Imaging 2006 Feb;23(2):130-4.
26. Sato C, Naganawa S, Nakamura T, Kumada H, Miura S, Takizawa O, Ishigaki T. Differentiation of noncancerous tissue and cancer lesions by apparent diffusion coefficient values in transition and peripheral zones of the prostate. J.Magn Reson.Imaging 2005 Mar;21(3):258-62.
27. Haider MA, van der Kwast TH, Tanguay J, Evans AJ, Hashmi AT, Lockwood G, Trachtenberg J. Combined T2-weighted and diffusion-weighted MRI for localization of prostate cancer. AJR Am.J.Roentgenol. 2007 Aug;189(2):323-8.
28. Amin MB, Crignon DJ, Humphrey PA, Srigley JR. Gleason Grading of Prostate Cancer: A contemporary apprroach. Lippincott Williams & Wilkins; 2004.
29. Gleason DF. Histologic grading of prostate cancer: a perspective. Hum.Pathol. 1992 Mar;23(3):273-9.
30. Wang XZ, Wang B, Gao ZQ, Liu JG, Liu ZQ, Niu QL, Sun ZK, Yuan YX. Diffusion-weighted imaging of prostate cancer: correlation between apparent diffusion coefficient values and tumour proliferation. J.Magn Reson.Imaging 2009 Jun;29(6):1360-6.
31. Zelhof B, Pickles M, Liney G, Gibbs P, Rodrigues G, Kraus S, Turnbull L. Correlation of diffusion-weighted magnetic resonance data with cellularity in prostate cancer. BJU.Int. 2009 Apr;103(7):883-8.
32. Langer DL, van der Kwast TH, Evans AJ, Sun L, Yaffe MJ, Trachtenberg J, Haider MA. Intermixed normal tissue within prostate cancer: effect on MR imaging measurements of apparent diffusion coefficient and T2--sparse versus dense cancers. Radiology 2008 Dec;249(3):900-8.
33. deSouza NM, Riches SF, Vanas NJ, Morgan VA, Ashley SA, Fisher C, Payne GS, Parker C. Diffusion-weighted magnetic resonance imaging: a potential non-invasive marker of tumour aggressiveness in localized prostate cancer. Clin.Radiol. 2008 Jul;63(7):774-82.
34. Tamada T, Sone T, Jo Y, Toshimitsu S, Yamashita T, Yamamoto A, Tanimoto D, Ito K. Apparent diffusion coefficient values in peripheral and transition zones of the prostate: comparison between normal and malignant prostatic tissues and correlation with histologic grade. J.Magn Reson.Imaging 2008 Sep;28(3):720-6.
35. Woodfield CA, Tung GA, Grand DJ, Pezzullo JA, Machan JT, Renzulli JF. Diffusion-weighted MRI of peripheral zone prostate cancer: comparison of tumour apparent diffusion coefficient with Gleason score and percentage of tumour on core biopsy. AJR Am.J.Roentgenol. 2010 Apr;194(4):W316-W322.
36. Hambrock T, Somford DM, Huisman HJ, van O, I, Witjes JA, Hulsbergen-van de Kaa CA, Scheenen T, Barentsz JO. Relationship between Apparent Diffusion Coefficients at 3.0-T MR Imaging and Gleason Grade in Peripheral Zone Prostate Cancer. Radiology 2011 May;259(2):453-61.
37. Verma S, Rajesh A, Morales H, Lemen L, Bills G, Delworth M, Gaitonde K, Ying J, Samartunga R, Lamba M. Assessment of aggressiveness of prostate cancer: correlation of apparent diffusion coefficient with histologic grade after radical prostatectomy. AJR Am.J.Roentgenol. 2011 Feb;196(2):374-81.
38. Isariyawongse BK, Sun L, Banez LL, Robertson C, Polascik TJ, Maloney K, Donatucci C, Albala D, Mouraviev V, Madden JF, et al. Significant discrepancies between diagnostic and pathologic Gleason sums in prostate cancer: the predictive role of age and prostate-specific antigen. Urology 2008 Oct;72(4):882-6.
39. San F, I, Dewolf WC, Rosen S, Upton M, Olumi AF. Extended prostate needle biopsy improves concordance of Gleason grading between prostate needle biopsy and radical prostatectomy. J.Urol. 2003 Jan;169(1):136-40.
181
Identifying High-Grade Prostate Cancer using DW-MRI in Patients with a Biopsy
8


CHAPTER 9
In vivo assessment of prostate cancer aggressiveness using MR
Spectroscopic Imaging at 3T
T. Kobus; T. Hambrock; C. Hulsbergen van de Kaa et al.
Leonardo da Vinci “Anatomical sketches”
CHAPTER 9CHAPTER 9

assessment of prostate cancer aggressiveness using MR
Spectroscopic Imaging at 3T with an endorectal coil
Kobus T, Hambrock T, Hulsbergen-van de Kaa C, Wright A, Barentsz J,
Heerschap A, Scheenen T
Advances in Knowledge
3T MR spectroscopic imaging is an in vivo technique to identify changes in prostate cancer
metabolism related to tumour aggressiveness.
The maximum Choline+Creatine/Citrate ratio, maximum Choline/Crreatine ratio, and
malignancy rating of a standardized threshold approach can all separate low from higher
grade tumours with considerable accuracy.
Implications for Patient Care
In vivo pretreatment knowledge of tumour aggressiveness and biochemical characteristics
can offer important information for patient treatment selection and assessment of tumour
response to therapy.
Summary Statement
3T 1H-MRSI offers potential for non-invasive assessment of prostate cancer aggressiveness.
184
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

ABSTRACT
Background: One of the most important clinical challenges in prostate cancer management is an
assessment of cancer aggressiveness.
Objective: To validate the performance of MR spectroscopic imaging (MRSI) of the prostate at
3T to assess tumour aggressiveness, based on the choline plus creatine to citrate ratio
(Cho+Cr/Cit) and choline to creatine ratio (Cho/Cr), using the Gleason score of the radical
prostatectomy (RP) specimen as the gold standard.
Design, Setting, and Participants: A total of 43 biopsy-proven prostate cancer patients with 53
clinically relevant tumour foci were retrospectively included in this study.
Measurements: Patients underwent a MRI and MRSI exam followed by RP. From MRSI, all
spectroscopy voxels containing tumour were selected by a radiologist guided by the
prostatectomy histopathology map only. For each tumour, two spectroscopists determined the
maximum Cho+Cr/Cit, Cho/Cr and malignancy rating by a standardized threshold approach,
incorporating both metabolic ratios. The maximum Cho+Cr/Cit, Cho/Cr, and malignancy ratings
showed a relation to tumour aggressiveness and so were used to differentiate between tumour
aggressiveness classes.
Results and limitations: The maximum Cho+Cr/Cit ratio, maximum Cho/Cr ratio, and
malignancy rating of a standardized threshold approach separated low from higher grade
tumours with areas under the receiver operating characteristic curves of 0.70, 0.74 and 0.78,
respectively.
Conclusions: MR spectroscopic imaging offers possibilities for an non-invasive
assessment of prostate cancer aggressiveness. The combination of the different metabolite ratios
was used with promising results for discrimination between different aggressiveness classes.
185
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

INTRODUCTION
Prostate cancer is the most frequently diagnosed non-cutaneous cancer in European men and
accounted for 9.3% of cancer-related deaths in men in 2008(1). A large European study(2)
showed that screening for prostate cancer by means of prostate-specific antigen (PSA) levels will
result in a mortality reduction of 20% at the cost of overdiagnosis of many indolent cancers. If
unnecessary side-effects due to overtreatment of indolent tumours are to be prevented, while at
the same time all aggressive tumours are to be treated, accurate discrimination between
indolent and life-threatening cancers is essential.
Generally, transrectal ultrasound-guided biopsies are performed to confirm the presence of
prostate cancer and to determine the Gleason score of the tumour. However, the multi-focal
nature and heterogeneity of these tumours cause sampling errors and may lead to
underestimation of their aggressiveness. Several studies demonstrate discrepancies between the
Gleason score identified in biopsies and the subsequent radical prostatectomy (RP)
specimens(3, 4). For optimal diagnosis the most aggressive tumour focus should be identified.
Proton magnetic resonance spectroscopic imaging (1H-MRSI) provides spatial mapping of the
tissue levels of the metabolites citrate, choline and creatine in the whole prostate gland(5, 6).
Prostate cancer tissue is characterized by lower citrate levels and/or higher choline levels
compared to normal tissue(7), resulting in the ratio of choline and creatine to citrate
(Cho+Cr/Cit) as a marker for prostate cancer(7, 8). MRI and 1H-MRSI have detected high grade
tumours in patients with elevated PSA with high sensitivity(9). Other studies found a
correlation(10) and a trend(11) between the Gleason score and the Cho+Cr/Cit ratio at 1.5T
with the use of an endorectal coil. No relation with aggressiveness was found at 1.5T without the
use of an endorectal coil(12). At 3T also no relation was found using just body-array coils(6).
The use of an endorectal coil increases the signal to noise and might provide enough sensitivity
at 3T to classify tumour aggressiveness.
Incorporation of the choline/creatine (Cho/Cr) ratio is interesting since choline supposedly
increases in malignant tissue due to altered phospholipid metabolism(13) and increased choline
to creatine ratios have been used in standardized scoring systems for 1H-MRSI of the
prostate(14, 15). High-resolution Magic-Angle-Spinning NMR of prostate biopsies
186
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

showed a significant correlation of the Gleason score to the Cho/Cr ratio, among other
ratios(16). These studies suggest that the Cho/Cr ratio has additional potential to classify
tumour aggressiveness .
The purpose of this study is to validate the performance of 1H-MRSI of the prostate at 3T with an
endorectal coil to assess tumour aggressiveness based on the Cho+Cr/Cit and Cho/Cr ratio using
the Gleason score from histopathology of the RP specimen as the gold standard.
MATERIALS AND METHODS
Patients
This study was approved by the institutional ethics review board and the need for informed
consent was waived for the retrospective study. 108 consecutive patients with biopsy-proven
prostate cancer had a 3T MR exam between October 2006 and February 2009 as well as a RP
between October 2006 and April 2009. Of these patients, 72 had a 1H-MRSI exam and were
retrospectively selected for this study. Patients were excluded if they were not examined with an
endorectal coil (n=4); had prior neoadjuvant therapy (n=9); had no tumour foci with a volume of
at least 0.5cc according to the histopathological analysis (n=14); or had no reliable
histopathology (n=2).
MR data acquisition
All MR-exams were performed on a 3T MR system (Magnetom Trio, Siemens, Erlangen,
Germany). An endorectal surface coil (Medrad, Pittsburgh, PA) was combined with body-array
coils for signal reception. In all patients an intramuscular injection of 1mg glucagon (Glucagen,
Nordisk, Gentofte, Denmark) and an injection of 20 mg of Butylscopolaminebromide (Buscopan,
Boehringer-Ingelheim, Ingelheim, Germany) were used to suppress peristalsis.
Fast gradient-echo-sequences were used to check the position of the coils. High spatial
resolution T2-weighted images were made in three directions. A prostate specific MRSI
sequence was used(17), including suppression of water and fat signals and an adapted sampling
scheme(5, 18). The actual volume of the spherical voxels was 0.37 or 0.64cm3(5).
187
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

Histopathological analysis
All RP specimens were uniformly processed and completely embedded according to a clinical
protocol(19). After formalin fixation and inking of the surface, the prostate specimen was
serially sectioned at 4 mm intervals, perpendicular to the dorsal-rectal surface, and all slices
were macroscopically photographed. One urological pathologist (C.A.H.K.) evaluated all RP
specimens and outlined for each slice the location of the tumour(s) on the photographs. Each
tumour focus was graded according to the 2005 ISUP Modified Gleason Grading System(20) and
each patient was staged following the 2002 TNM classification(21).
The primary, secondary and tertiary Gleason grades were used for a qualitative grading of the
tumour aggressiveness. Tumours were classified as low grade if consisting only of grades 2
and/or 3; intermediate grade with a secondary or tertiary grade of 4, but no 5 component; or
high grade with 4 as primary and/or 5 as primary/secondary or tertiary grade (Table 1).
Voxel selection
One radiologist (T.H.), blinded to the spectra, used the results of the histopathological analysis to
assign all spectroscopic voxels containing tumour tissue on high resolution T2-weighted images
with the voxel matrix of the spectroscopic exam projected over these images (Fig. 1c). Only
clinically significant tumours with a minimal size of 0.5cc(22, 23) on the histopathologic analysis
were included. Figure 1 shows an example of a T2-weighted image and corresponding
histopathology.
The signals of interest were fitted with a prototype software package (Metabolite report,
Siemens Medical Solutions, Germany) and the Cho+Cr/Cit and Cho/Cr ratios were calculated
automatically. Two spectroscopists independently (T.K. and T.W.J.S.) inspected the quality of the
automated fit for sufficient signal to noise, the absence of lipid signals and the absence of
baseline distortions. Only voxels that were approved by both spectroscopists were included in
the remainder of the study.
For every tumour, the voxel with the highest Cho+Cr/Cit ratio and the voxel with the highest
Cho/Cr ratio were determined. The highest Cho+Cr/Cit and Cho/Cr values of all data from each
188
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

aggressiveness class were checked for normality and compared with each other using a Kruskal-
Wallis test. The Pearson correlation coefficient was used to determine the correlation between
Number of patients 43
Mean PSA level ** 8.33 ng/ml (range 2.08 - 40.96)
Mean age 61 years (range 42-70)
Clinical stage T2 T3 T4
19 23 1
Gleason score
Peripheral zone:
3+2
3+3
3+3+4
3+4
3+4+5
4+3
4+3+5
4+4
4+5
Central gland:
2+3
3+2
3+2+4
2+4+5
4+3
4+3+5
Both zones:
4+3
4+4
Number of tumours:
2
10
1
10
3
9
2
1
2
2
3
1
1
1
3
1
1
low: 17
intermediate: 12
high: 24
Table 1. Patient and tumour characteristics
* The tumours are classified according to their aggressiveness as explained in the
materials and method section.
** PSA = Prostate specific antigen
189
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

the two ratios. To test the correlation between the ratios and the different aggressiveness
classes the Kendall-tau rank-correlation coefficient was determined.
To enable incorporation of both metabolite ratios in discrimination of aggressiveness classes the
standardized threshold approach(14, 15) was used. The conventional standardized threshold
approach uses an initial malignancy rating (ranging from 1, definitely benign, to 5, definitely
malignant) based upon the mean and standard deviation of the Cho+Cr/Cit ratio of non-cancer
tissue (distinction is made between peripheral zone (PZ) and central gland (CG)) with an
adjustment to the initial rating based upon the Cho/Cr ratio (Table 2.)(15). This malignancy
rating was determined for all accepted voxels in each tumour using the mean Cho+Cr/Cit ratios
and standard deviations of non-cancer tissue described earlier(6). In order to optimize the
standardized scoring system for aggressiveness assessment with 3T data, the Cho/Cr cut off
level, which adjusts the initial malignancy rating, was varied between 1 and 4 with 0.1 intervals.
For all 31 of these Cho/Cr adaptation levels the highest malignancy rating per tumour was
calculated and used to obtain ROC curves to determine the accuracy.
Five-point standardized scoring system
Score and Score definition PZ Cho+Cr/Cit ratio
CG Cho+Cr/Cit ratio
Cho/Cr ratio adjustment
adjust 3 and 2 into 4.
If Cho/Cr ratio < 2, then: adjust 5 into 4 and 4 into 3.
1: Definitely benign tissue
2: Probably benign tissue
3: Possibly malignant tissue
4: Probably malignant tissue
5: Definitely malignant tissue
>0.70 >0.90
PZ = peripheral zone, CG = central gland, Cho+Cr/Cit and CC/C = choline plus creatine to citrate, Cho/Cr = choline to creatine
Table 2. Conventional Standardized Threshold Approach definitions
190
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

Statistical analysis
The AUCs of the ROC curves were determined to study the performance of discrimination of low
grade from higher grade tumours and high grade from lower grade tumours using the maximum
Cho+Cr/Cit, maximum Cho/Cr and the 5 point scale of the standardized threshold approach. All
AUCs were compared for statistical differences(24).
Statistical analyses were performed with GraphPad Prism (GraphPad Software Inc, La Jolla, USA)
and Matlab (The Mathworks Inc, Natick, USA). For all statistical tests a P-value of 0.05 was used
to show significance.
RESULTS
Of the 108 patients, 43 passed the inclusion criteria. A summary of patient and tumour
characteristics is given in Table 1. The mean time between the MR exam and RP was 6 weeks
(range 0-21 weeks). The MR-exam (example in Fig. 1) was performed on average 46 days after
transrectal ultrasound-guided biopsy (range 19-107 days). The total number of clinically
significant tumours was 53 in 43 patients. 40 tumours were located in the PZ, 11 in the CG and 2
tumours covered both zones (assigned as PZ tumour for analysis). The average tumour size on
histopathology was 6.3 cm3 (range 0.52-33.5 cm3). The patient Gleason scores of the tumours
that were excluded because the volume was smaller than 0.5cc were 2+3 (n=2), 3+3 (n=9), 3+4
(n=2) and no malignancy detected (n=1).
In total, 1892 tumour voxels were selected by the radiologist. Of these voxels, 77% (1463/1892)
passed the quality inspection of both spectroscopists. Three patients, and therefore 5 tumours,
had to be excluded from the analysis, since none of the spectra of the selected voxels were
usable.
A small, but significant correlation was found between the maximum Cho+Cr/Cit ratio and the
aggressiveness classes (p=0.02, r=0.27)(Fig 2). The comparison of the medians of the three
aggressiveness classes revealed a significant difference between the low and high grade
tumours. The maximum Cho/Cr ratio also correlated significantly with the aggressiveness
191
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

classes (p<0.01, r=0.31)(Fig 3). The median Cho/Cr of the low grade tumours was significantly
different from the high grade tumours. Table 3 shows the AUCs representing the performance of
the aggressiveness assessments.
The correlation between the maximum Cho+Cr/Cit ratio and the maximum Cho/Cr ratio was
0.51 (p<0.001). For each tumour the maximum Cho+Cr/Cit was plotted against the maximum
Cho/Cr value (Fig 4). A Cho/Cr adaptation level of 2.3 for the standardized threshold approach
gave the highest AUCs when discriminating high from low and intermediate grade tumours
(AUC=0.73) and low from the combined high and intermediate grade tumours (AUC=0.78). The
malignancy ratings using an adaptation level of 2.3 are shown in Figure 5 and the median
malignancy rating of the high (median=5) and low (median=3) grade tumours was significantly
different. In all discriminations between aggressiveness classes (Table 3), the AUCs of the
standardized threshold method with adaptation level of 2.3 were higher than the AUCs for the
maximum Cho+Cr/Cit or Cho/Cr ratio alone, but these differences were not significant.
Low vs. high and intermediate grade tumours
High vs. low and intermediate grade tumours
Maximum Cho+Cr/Cit 0.70 0.69
Maximum Cho/Cr 0.74 0.71
Standardized threshold approach*
0.78 0.73
Table 3. The areas under the ROC curves for the discrimination between different
aggressiveness classes using the maximum Cho+Cr/Cit and Cho/Cr ratios and the
standardized threshold approach.
* For the standardized threshold approach an optimized Cho/Cr rating adaptation level of
2.3 was used.
192
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

Figure 2. The distribution of the maximum Cho+Cr/Cit ratios per tumour aggressiveness
class. The horizontal bars indicate the median. One high grade tumour had a maximum
Cho+Cr/Cit ratio of 58 which has been plotted at a Cho+Cr/Cit ratio of 3 for displaying
purposes.
Figure 3. Distribution of the maximum Cho/Cr ratio per aggressiveness class. The
horizontal bars indicate the median.
193
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

Figure 4. The maximum Cho+Cr/Cit ratio for each tumour focus plotted against the
maximum Cho/Cr ratio of that focus. The tumours are divided by aggressiveness class.
The Cho+Cr/Cit ratio of one high grade tumour was cut off at 3 for displaying purposes
.
Figure 5. The highest malignancy ratings according to the standardized threshold
approach for each tumour in the aggressiveness classes. A Cho/Cr adaptation level of 2.3
was used.
194
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

DISCUSSION
With an increasing number of reports on overdiagnosis(2, 25), an individualized prostate cancer
aggressiveness assessment is essential. Currently the pre-treatment aggressiveness is
determined with biopsies, but often the Gleason score is underestimated(3, 4). MR(S)I could be a
prognostic non-invasive approach to differentiate between patients as suitable candidates for
active surveillance and patients that need immediate treatment. Moreover, it would enable
targeted therapy, like intensity-modulated radiotherapy or high-intensity focused ultrasound, to
be applied to the most aggressive part of the tumour. In a detection setting, it could guide a
biopsy to be taken from the most aggressive part of a tumour. Validation is the first step in the
development of such a prognostic MRSI approach. We assessed the tumour aggressiveness
differentiation by the AUC of the ROC curves and this gave similar results when using either the
Cho+Cr/Cit (0.70) or the Cho/Cr (0.74) ratio. The performance of combining both ratios was
better (0.78), though this was not statistically significant, due to a relative small sample size. The
AUCs reflect considerable overlap between the ratios in the different aggressiveness classes,
similar to what has been reported in other studies to the relationship between the Cho+Cr/Cit
ratio and Gleason score(10, 11).
We investigated whether a combination of both ratios would increase the performance of
separating low from higher grade tumours. The original standardized threshold approach was
developed to improve tumour localization at 1.5T with a Cho/Cr level of 2 to adjust the initial
malignancy rating(14, 15). As the timing of the MRSI pulse sequence at 3T is different(17) from
the timing at 1.5T, we optimized the Cho/Cr adaptation level of the standardized threshold
approach for tumour aggressiveness classification at 3T, retaining the original concept of
defining the thresholds based on the mean and standard deviations of non-cancer PZ and CG
tissues. When all tumours with a malignancy rating of 4 or 5 would be classified as high grade,
only 10% of the high grade tumours would be misclassified as a lower grade. 52% of the
intermediate and low grade tumours would be misclassified as high grade, which is better than
previous results (68%) using MRI and 1H-MRSI in patients with an elevated PSA level(9).
As in current clinical practice MR examinations of the prostate are often multiparametric, the
standardized threshold approach could even be extended to include more predictive variables
for the assessment of aggressiveness. Features like the apparent diffusion coefficient or
195
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

pharmacokinetic parameters of dynamic-contrast-enhanced MRI could be included to improve
the performance(26).
The tumours were divided in three clinically useful classes of aggressiveness: low, intermediate
and high. The nature of the Gleason score does not lend itself to a linear relationship with an
aggressiveness marker. Using three aggressiveness classes, the tertiary Gleason scores could be
taken into account and Gleason 7 tumours could be divided in primary grade 3 and primary
grade 4 tumours. The primary grade 4 tumours are more aggressive and have an increased risk
for progression(27, 28). Tumours with a tertiary Gleason score of 5 have a higher risk of
extraprostatic extension(29) and PSA recurrence(28, 30) than tumours with the same score
without a tertiary pattern. For these reasons, three classes of aggressiveness were used, which
still enabled us to answer clinically relevant questions on aggressiveness.
Our study had several limitations. This was a retrospective single-institution study with a
limited number of patients; therefore, our results may not be extrapolated to the general patient
population. Therefore, the data can be considered as very promising but preliminary, and our
conclusions need confirmation by a prospective multicentre trial, which is currently underway.
We did not correct for possible correlation between multiple tumours in a single patient (6 cases
of two clinically significant tumours within one prostate). Although we distinguished between
tumours in the PZ and those in the CG, we did not do a separate aggressiveness analysis for the
two regions due to the limited number of CG tumours(n=11). We excluded 14 patients from our
initial patient cohort because of tumour size on histopathology of less than 0.5cc. Next to the fact
that these small tumours are clinically insignificant (no high grade cancer present), the actual
volume of the voxels of our MRSI examinations was too large to represent tumour foci of these
sizes without too much surrounding non-cancer tissue within the voxel of interest. Metabolite
ratios of these voxels would represent a mixture between cancer and non-cancer tissue.
CONCLUSION
In conclusion, this study showed that 1H-MRSI offers potential for non-invasive
assessment of prostate cancer aggressiveness, which has important implications. We have
modified the existing standardized threshold approach to assess tumour aggressiveness at 3T.
196
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

The initial results of combining the Cho+Cr/Cit and Cho/Cr ratio were promising for the
discrimination between different aggressiveness classes.
Figure 1. MRI and MRSI of a 65-year old patient with prostate cancer (PSA 5.3 ng/ml,
Gleason Score 4+5) (A) T2 weighted image of the prostate with tumour in the left
peripheral zone. Histopathology (B) is used as the gold standard. The spectroscopy grid
is displayed on top of the T2 weighted image in (C). In the right and left peripheral zone a
non-cancer voxel and cancer voxel, respectively, are indicated. (D) shows a spectrum of
non cancer tissue, while in (F) the spectrum of a cancer voxel is shown with deviating
signal intensities for the different metabolites. The calculated choline and creatine to
citrate ratio (Cho+Cr/Cit) and the choline to creatine ratio (Cho/Cr) are indicated in the
spectra of both tissues. The metabolite map in (E) shows the Cho+Cr/Cit distribution over
the prostate.
197
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

REFERENCES
1. Ferlay J, Parkin DM, Steliarova-Foucher E. Estimates of cancer incidence and mortality in Europe in 2008. Eur J Cancer 2010; 46:765-781.
2. Schroder FH, Hugosson J, Roobol MJ, et al. Screening and prostate-cancer mortality in a randomized European study. N Engl J Med 2009; 360:1320-1328.
3. Tomioka S, Nakatsu H, Suzuki N, Murakami S, Matsuzaki O, Shimazaki J. Comparison of Gleason grade and score between preoperative biopsy and prostatectomy specimens in prostate cancer. Int J Urol 2006; 13:555-559.
4. Rajinikanth A, Manoharan M, Soloway CT, Civantos FJ, Soloway MS. Trends in Gleason Score: Concordance Between Biopsy and Prostatectomy over 15 Years. Urology 2008; 72:177-182.
5. Scheenen TW, Klomp DW, Roll SA, Futterer JJ, Barentsz JO, Heerschap A. Fast acquisition-weighted three-dimensional proton MR spectroscopic imaging of the human prostate. Magn Reson Med 2004; 52:80-88.
6. Scheenen TW, Heijmink SW, Roell SA, et al. Three-dimensional proton MR spectroscopy of human prostate at 3 T without endorectal coil: feasibility. Radiology 2007; 245:507-516.
7. Kurhanewicz J, Vigneron DB, Hricak H, Narayan P, Carroll P, Nelson SJ. Three-dimensional H-1 MR spectroscopic imaging of the in situ human prostate with high (0.24-0.7-cm3) spatial resolution. Radiology 1996; 198:795-805.
8. Heerschap A, Jager GJ, Van Der Graaf M, et al. In vivo proton MR spectroscopy reveals altered metabolite content in malignant prostate tissue. Anticancer Res 1997; 17:1455-1460.
9. Villeirs GM, De Meerleer GO, De Visschere PJ, Fonteyne VH, Verbaeys AC, Oosterlinck W. Combined magnetic resonance imaging and spectroscopy in the assessment of high grade prostate carcinoma in patients with elevated PSA: A single-institution experience of 356 patients. Eur J Radiol 2009; Epub ahead of print.
10. Kurhanewicz J, Vigneron DB, Males RG, Swanson MG, Yu KK, Hricak H. The prostate: MR imaging and spectroscopy: Present and future. Radiol Clin North Am 2000; 38:115-138.
11. Zakian KL, Sircar K, Hricak H, et al. Correlation of proton MR spectroscopic imaging with gleason score based on step-section pathologic analysis after radical prostatectomy. Radiology 2005; 234:804-814.
12. Jambor I, Borra R, Kemppainen J, et al. Functional imaging of localized prostate cancer aggressiveness using 11C-acetate PET/CT and 1H-MR spectroscopy. J Nucl Med 2010; 51:1676-1683.
13. Ackerstaff E, Pflug BR, Nelson JB, Bhujwalla ZM. Detection of increased choline compounds with proton nuclear magnetic resonance spectroscopy subsequent to malignant transformation of human prostatic epithelial cells. Cancer Res 2001; 61:3599-3603.
14. Jung JA, Coakley FV, Vigneron DB, et al. Prostate depiction at endorectal MR spectroscopic imaging: investigation of a standardized evaluation system. Radiology 2004; 233:701-708.
15. Fütterer JJ, Scheenen TWJ, Heijmink SWTPJ, et al. Standardized threshold approach using three-dimensional proton magnetic resonance spectroscopic imaging in prostate cancer localization of the entire prostate. Invest Radiol 2007; 42:116-122.
16. Van Asten JJA, Cuijpers V, Hulsbergen-Van De Kaa C, et al. High resolution magic angle spinning NMR spectroscopy for metabolic assessment of cancer presence and Gleason score in human prostate needle biopsies. MAGMA 2008; 21:435-442.
17. Scheenen TWJ, Gambarota G, Weiland E, et al. Optimal timing for in vivo 1H-MR spectroscopic imaging of the human prostate at 3T. Magn Reson Med 2005; 53:1268-1274.
18. Pohmann R, von Kienlin M. Accurate phosphorus metabolite images of the human heart by 3D acquisition-weighted CSI. Magn Reson Med 2001; 45:817-826.
19. Van Oort IM, Bruins HM, Kiemeney LALM, Knipscheer BC, Witjes JA, Hulsbergen-Van De Kaa CA. The length of positive surgical margins correlates with biochemical recurrence after radical prostatectomy. Histopathology 2010; 56:464-471.
20. Epstein JI, Allsbrook Jr WC, Amin MB, et al. The 2005 International Society of Urological Pathology (ISUP) consensus conference on Gleason grading of prostatic carcinoma. Am J Surg Pathol 2005; 29:1228-1242.
21. Greene FL, Page DL, Flemming ID, et al. AJCC Cancer Staging Manual. 6th edition New York: Springer-Verlag, 2002.
198
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9

22. Augustin H, Hammerer PG, Graefen M, et al. Insignificant prostate cancer in radical prostatectomy specimen: time trends and preoperative prediction. Eur Urol 2003; 43:455-460.
23. Stamey TA, Freiha FS, McNeal JE, Redwine EA, Whittemore AS, Schmid HP. Localized prostate cancer. Relationship of tumor volume to clinical significance for treatment of prostate cancer. Cancer 1993; 71:933-938.
24. Metz CE, Herman BA, Roe CA. Statistical comparison of two ROC-curve estimates obtained from partially-paired datasets. Med Decis Making 1998; 18:110-121.
25. Andriole GL, Crawford ED, Grubb RL, 3rd, et al. Mortality results from a randomized prostate-cancer screening trial. N Engl J Med 2009; 360:1310-1319.
26. Seitz M, Shukla-Dave A, Bjartell A, et al. Functional Magnetic Resonance Imaging in Prostate Cancer. Eur Urol 2009; 55:801-814.
27. Chan TY, Partin AW, Walsh PC, Epstein JI. Prognostic significance of Gleason score 3+4 versus Gleason score 4+3 tumor at radical prostatectomy. Urology 2000; 56:823-827.
28. Hattab EM, Koch MO, Eble JN, Lin H, Cheng L. Tertiary Gleason Pattern 5 is a Powerful Predictor of Biochemical Relapse in Patients With Gleason Score 7 Prostatic Adenocarcinoma. J Urol 2006; 175:1695-1699.
29. Mosse CA, Magi-Galluzzi C, Tsuzuki T, Epstein JI. The Prognostic Significance of Tertiary Gleason Pattern 5 in Radical Prostatectomy Specimens. Am J Surg Pathol 2004; 28:394-398.
30. Pan CC, Potter SR, Partin AW, Epstein JI. The prognostic significance of tertiary Gleason patterns of higher grade in radical prostatectomy specimens: A proposal to modify the Gleason grading system. Am J Surg Pathol 2000; 24:563-569.
199
In Vivo Assessment of Prostate Cancer Aggressiveness using MR Spectroscopic Imaging at 3T
9


Prospective Assessment of Prostate Cancer Aggressiveness
using 3T DWI-MRI Guided Biopsies vs. a 10-Core TRUS Biopsy Cohort
T. Hambrock; C. Hoeks, C.Hulsbergen-van de Kaa et al.
CHAPTER 10CHAPTER 10

Prospective Assessment of Prostate Cancer Aggressiveness using 3T Diffusion Weighted Magnetic Resonance Imaging Guided Biopsies versus a 10-Core Transrectal Ultrasound Prostate Biopsy Cohort
Hambrock T, Hoeks C, Scheenen T, Hulsbergen-van de Kaa C, Bouwense S, Schröder F, Fütterer J, Huisman J, Barentsz J
Lauterbur Award Society of Body CT and MR, San Diego, Mar 2010
Advances in knowledge: 10-Core Transrectal ultrasound (TRUS) guided systematic prostate biopsy determined
highest Gleason grades reveal a poor concordance with true highest Gleason grades
(HGG) in prostatectomy specimens.
TRUS biopsy show a substantial undergrading for tumours with a HGG of 5.
3T Diffusion weighted MR imaging is an accurate and valuable technique for identifying
the most aggressive components within a prostate tumour.
MR guided biopsies targeted towards the most abnormal regions on DWI has a vastly
superior accuracy for determining the true HGG compared to TRUS.
Implications for patient care: Biopsies targeted towards the most abnormal regions on 3T DWI MR imaging represent
a substantially improved method for assessment of true tumour aggressiveness and can
therefore represent an indispensable tool in the diagnosis and management of patients
with prostate cancer.
Summary Statement
MR guided biopsies targeted towards the most abnormal regions on DWI MRI represent a substantially improved prospective method for
assessment of true tumour aggressiveness
202
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

ABSTRACT
Background: Accurate pretreatment assessment of prostate cancer aggressiveness is becoming
more important in decision making. Gleason grade is one of the most important predictors of
prostate cancer aggressiveness. Transrectal ultrasound guided biopsies (TRUS-GB) show
substantial undergrading of Gleason grade found in prostatectomy specimens. Diffusion
weighted MR-imaging (DWI) has been shown to be a valuable biomarker of tumor
aggressiveness.
Objective: To improve pretreatment assessment of prostate cancer aggressiveness, this study
prospectively evaluated the value of MRI guided prostate biopsies (MR-GB) of abnormalities
determined on DWI apparent diffusion coefficient (ADC) maps. Results were compared to those
of a clinical cohort using 10-core TRUS-GB. Prostatectomy findings were the gold standard.
Measurements: A multi-parametric 3T MRI incl. DWI was performed to identify tumour
suspicious regions in patients (n=34) with a negative TRUS-GB. Subsequently, the regions with
highest restriction on ADC maps within the suspicions regions, were used to direct MR-GB. A 10-
core TRUS-GB was used in a matched cohort of 64 men. Following prostatectomy, the highest
Gleason grades (HGG) in biopsies and prostatectomy (RP) specimens were identified. Biopsy and
prostatectomy Gleason grade performances were evaluated using Chi-square analysis.
Results and Limitations : No significant differences were observed for the proportions of
patients on RP having a HGG=3 (35% vs. 28%; p=0.50), HGG=4 (32% vs. 41%; p=0.51) and
HGG=5 (32% vs. 31%; p=0.61) for the MR-GB and TRUS-GB cohort respectively. MR-GB showed
an exact performance with RP for overall HGG in 88% (30/34) while for the TRUS-GB this was
55% (35/64; p=0.001). In the MR-GB cohort, an exact performance with a HGG=3 was 100%
(12/12), for HGG=4, 91% (10/11) and for HGG=5, 73% (8/11). The corresponding performance
rates for TRUS-GB were 94% (17/18; p=0.41), 46% (12/26;p=0.02) and 30% (6/20; p=0.01)
respectively.
Conclusions: This study prospectively shows the ability of DWI directed MR-GBs to improve
pretreatment risk-stratification by obtaining biopsies, which are representative for true
prostatectomy Gleason grade.
203
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

INTRODUCTION
The Gleason grading system is one of the most important features describing the pathological
characteristics of prostate cancer. Of all clinically determinable parameters, the Gleason score
(GS) has been proven to be one of the most important in measuring aggressiveness, disease
outcome and risk of mortality from prostatic cancer(1).
Currently, transrectal ultrasound guided prostate biopsy (TRUS-GB) is the most accepted
method for establishing a definite diagnosis of prostate cancer in patients with a clinical
suspicion based on prostate specific antigen (PSA) values or digital rectal examination (DRE).
The most widely used biopsy schemes include sampling by 10-12 cores with emphasis on the
lateral peripheral zone and transition zone (2;3). The tumor containing tissues cores obtained
at TRUS-GB are scored according to the Gleason grading scheme in order to determine prostate
cancer aggressiveness and prognosis .
Prostate cancer can be multifocal in location and also heterogeneous in composition, often
presenting with well, moderately- and poorly-differentiated components in the same tumor.
TRUS-GB determined GS has been shown (4-6) to be substantially discordant (under-grading in
34-38%) with the GS determined in analysis of radical prostatectomy (RP) specimens. Because
risk-stratification will affect individualized treatment decisions and prognosis, an accurate
pretreatment prediction of GS, which is the major component of the currently used risk
nomograms, remains essential.
Multi-parametric MR imaging, including T2-weighted imaging (T2-w MRI), diffusion-weighted
imaging (DWI) and dynamic contrast enhanced MR imaging (DCE-MRI) have all been shown
(especially in combination) to accurately localize prostate cancer (7;8). Due to improved
localization, suspicious regions on multi-parametric MRI have also been biopsy targeted under
direct MR guidance and shown to substantially increase the tumour detection rates (9;10).
Especially DWI has recently been shown to provide information about tumor aggressiveness
(11;12).
The aim of this study, therefore, was to prospectively determine whether 3T DWI guided
prostate tissue sampling could improve the pretreatment assessment of prostate cancer
aggressiveness. These results were compared to a standard clinical cohort of patients, where
204
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

tissue sampling was done using a systematic 10-core sampling approach for the same purpose.
In both cohorts the performance of Gleason grades in biopsy and prostatectomy specimens,
serving as a gold standard, was determined.
MATERIALS AND METHODS
Patients
Between Aug 2006 and Apr 2009, 123 consecutive patients underwent a RP at the Radboud
University Nijmegen Medical Centre, Nijmegen, Netherlands and were retrospectively included if
a diagnosis of prostate cancer was made either with a 10-core systematic TRUS-GB scheme or
MR-GB. Patients with hormonal or radiotherapy prior to prostatectomy were excluded.
TRUS-GB sampling
Extended systematic 10-core TRUS-GB's (incl. 6 lateral and 4 transition zone biopsies) were
obtained using a Pro Focus B and K ultrasound device (Medical, Herlen, Denmark) with an
Endfire probe transducer (8667 convex array, 8.0 MHz, B and K Medical, Herlen, Denmark) and
an 18 Gauge needle with 17 mm sampling length. The indication for performing biopsies was
based on routine clinical parameters i.e. an elevated PSA above 4 ng/ml and/or abnormal DRE,
requiring further assessment. TRUS-GB represented the first biopsy session in these patients.
MR imaging
Multi-parametric MR imaging at 3T (Trio Tim, Siemens, Erlangen, Germany) which included
DWI, T2-w MRI, and DCE-MRI was performed in patients with at least one prior negative 10-core
TRUS-GB session, however with ongoing clinical suspicion for prostate cancer. This suspicion
was defined by a rising or persistently elevated PSA. MR imaging parameters are presented in
Table 1. Apparent diffusion coefficient (ADC) maps were automatically calculated from the DWI
by the scanner software. Two radiologists determined up to 3 tumour suspicious regions (TSR)
per patient in consensus using the combined information of the features suspicious for
malignancy on the different modalities of the multi-parametric MRI. The patient PSA values were
available to radiologists for all evaluated patients. Each of the three imaging modalities was
205
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

scored on a tumour probability scale of 1 to 5 with a maximum cumulative score of 15. Per
modality, the scale is defined in as such that 1 indicates: definitely no tumour; 2: probably no
tumour; 3: possibly tumour; 4: probably tumour and 5: definitely tumour. A biopsy indication
8/15. Subsequently, for each TSR
that was biopsied, the region on the ADC for that particular TSR, revealing the darkest spot, was
used as target for the MR-GB.
Sequence
Type Slice
thickness Number of slices
In-plane resolution
TR TE Averages b-values
T2-w Axial
TSE 4 mm 15-19 0.6 x 0.6 mm 3540 ms 104 ms 2 -
T2-w Coronal
TSE 4 mm 15-19 0.6 x 0.6 mm 3350 ms 105 ms 2 -
T2-w Sagital
TSE 4 mm 15-19 0.6 x 0.6 mm 3810 ms 105 ms 2 -
DWI SE-EPI 4 mm 15-19 2.0 x 2.0 mm 2800 ms 81 ms 10 0, 50, 500, 800 mm2/s
T1-w DCE
GRE FLASH
4 mm 14 1.8 x 1.8 mm 37 ms 1.47 ms 1 -
Table 1. MR imaging sequence parameters. T2-w: T2-weighted; T1-w: T1-weighted; DWI:
Diffusion weighted imaging; DCE: Dynamic contrast enhanced imaging; TSE: Turbo Spin
Echo; SE-EPI: Spin Echo – Echo Planar Imaging; TR: Repetition Time; TE: Echo Time;
GRAPPA: Parallel imaging factor; GRE: Gradient echo imaging; FLASH: Fast low angle shot
imaging.
206
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

MRI guided biopsy (MR-GB)
On average 4 weeks (range 2 – 6 weeks) following the tumour detection multi-parametric MRI
study, MR-GB (using MR compatible 18 gauge needles with sampling length of 17 mm) of the
previously determined TSRs was performed using a commercially available transrectal MR-
biopsy device (Invivo, Schwerin, Germany) under direct 3T MR guidance. The translation of
initial MR imaging findings to the subsequent MR-GB has been described in detail before (13).
The lowest signal areas on the ADC maps within the TSR were used to target the biopsy cores.
Histopathological analysis of biopsy specimens
Immediately after biopsy, tissue cores were fixed in 10% neutral-buffered formalin. After
histological staining with hematoxylin and eosin (H&E), tissue section of 5 m were prepared
and thereafter evaluated by one urogenital pathologist (C.A.H.K) with 17 years experience in
prostate pathology. For all included patients, clinical features incl. PSA were available to the
histopathologist. For cores containing cancer, a Gleason score using the International Society of
Urogential Pathology (ISUP) criteria of 2005 was assessed. The primary, secondary and tertiary
Gleason grades were determined and the highest Gleason grade (HGG) was identified within the
biopsy cores.
Reconstructed whole-mount step-section preparation
Following radical prostatectomy, prostate specimens were uniformly processed and entirely
submitted for histopathological investigation. After inking of the surface, the prostate specimens
were cut into 4-mm thick slices, perpendicular to the dorsal-rectal surface in a plane parallel to
the transverse T2-weighted imaging plane, and macroscopically photographed with a CCD-
camera. All slices were completely processed and evaluated on 5 μm hematoxylin-eosins stained
sections. The presence and extent of cancer were outlined on the glass slide cover by the same
expert urological pathologist who reviewed all prior biopsies. Subsequently tumours were
mapped on the macroscopic photographs to allow reconstruction of tumour extent and
multifocality. Each individual tumour was graded according to the 2005 ISUP Modified Gleason
Grading System (14). As with the assessment of biopsies, the primary to tertiary Gleason grades
and the HGG identified within the prostate was noted.
207
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

Statistical analysis
Cross tabulation analysis of the biopsy and RP findings was done. For both MR-GB and TRUS-GB
cohorts, performance rates (%) with RP were determined for the HGG. Secondly, for a RP HGG of
5, undergrading was further defined as if the Bx HGG was 3. Thirdly, performance
rates between Bx and the RP HGG groups were determined separately for respectively patients
with a PSA 10 ng/ml and those with a PSA >10ng/ml. Chi-square analyses with Fisher’s exact tests were performed to evaluate the significance of differences between MR-GB and TRUS-GB
performance rates. The t-test was performed to determine for differences in mean PSA, prostate
volume and dominant tumour volume. A significant difference was considered present when p
<0.05. Statistical analyses were performed with SPSS software (SPSS, version 16.0.01, Chicago,
U.S.A).
RESULTS
Ninety-eight patients fulfilled the inclusion criteria. In 34/98 patients a tumour diagnosis was
made using MR-GB (median of 3 cores, range 1-5; median number of biopsies per TSR: 2, range 1
to 3) and in 64/98 patients a diagnosis using 10-core TRUS-GB. The median procedure duration
for MR-GB was 29 min (range 15-75 min). The median duration between MR-GB and RP was 6
weeks (range 3- 11 weeks) and between TRUS-GB and RP, 5 weeks (range 2-9 weeks). The
patient demographic and clinical parameters are summarized in Table 2.
No significant differences between the MR-GB and TRUS-GB cohorts were observed for
percentage pT3 tumours (35% vs. 38%; p=0.83), mean dominant aggressive tumour volume
(4.85 cc vs. 4.52 cc; p=0.69) or mean prostate volume (41 cc vs. 36 cc; p=0.61). Furthermore, no
significant differences were observed for the overall proportions of patients on RP having a
HGG=3 (35% vs. 28%; p=0.50), HGG=4 (32% vs. 41%; p=0.51) and HGG=5 (32% vs. 31%;
p=1.00) for the MR-GB and TRUS-GB cohort respectively. In our two cohorts, the RP presence of
HGG 4 was associated with extra-capsular extension in 39-46% and the presence of a HGG of 5 in
64-70%.
208
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

MR-GB 10-core Significance (p-value)
Number of Patients 34 64 N.A.
Age 66 (51-74) 66 (41-74) 0.22
Number of biopsies (range)
3 (1-5) 10 N.A.
Stage
- pT2
- pT3
22/34 (65%)
12/34 (35%)
40/64 (62%)
24/64 (38%)
0.83
Prostate Volume
- Median [cc] (range)
PSA
- Median [ng/ml] (range)
D.A. Tumour Volume
- Median [cc] (range)
41 (12-79)
12 (3 – 40)
4.85 (0.1-33)
36 cc (17-126)
8 (2– 47)
4.52 (0.1-33.5)
0.61
0.02 *
0.69
Prevalence of Tumours in RP
HGG category
- HGG 3
- HGG 4
- HGG 5
35% (12 of 34)
0% (0/12)
32% (11 of 34)
45% (5/11)
32% (11 of 34)
64% (7/11)
28% (18 of 64)
0% (0/18)
41% (26 of 64)
38% (10/26)
31% (20 of 64)
80% (16/20)
0.50
N.A.
0.51
0.73
1.00
0.41
Tabel 2. Patient and pathology characteristics. (D.A. = Dominant aggressive; *=denotes
significance; N.A.=not applicable)
209
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

A summary of the Bx and RP findings are presented in Tables 3 and 4. When patients were
categorized based on the HGG on Bx and RP, the overall performance rate for MR-GB was 88%
(30/34) vs. 55% (35/64) for TRUS-GB patients. In the MR-GB cohort, an exact performance with
a RP HGG=3 was 100% (12/12), for HGG=4 this was 91% (10/11) and for HGG=5, 73% (8/11).
The corresponding performance rates for TRUS-GB were 94% (17/18; p=0.41), 46%
(12/26;p=0.01) and 30% (6/20; p=0.02) respectively. For biopsies determined as low-grade
(HGG=3), the positive predictive value (PPV) for MR-GB to represent true low-grade tumour was
92% (12/13) while the PPV for TRUS-GB was 45% (17/38; p=0.001). Overall, undergrading of
tumors with a RP HGG 4 or 5 was 46% (25/46) for the TRUS-GB cohort and 5% (1/22) for the
MR-GB cohort.
Prostatectomy
HGG 3 HGG 4
HGG 5
HGG 3 17 14 8 44% (17/39) TRUS-GB HGG 4 1 12 6 63% (12/19) HGG 5 0 0 6 100% (6/6)
94% (17/18) 46% (12/26)
73%(8/11)
55% (35/64)
Prostatectomy
HGG 3
HGG 4
HGG 5
HGG 3 12 1 0 92% (12/13) MR-GB HGG 4 0 10 3 77% (10/13) HGG 5 0 0 8 100% (8/8)
100%(12/12) 91% (10/11)
73% 8/11)
88% (30/34)
Table 3. Crosstabs for cohorts based on HGG grouping
210
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

Performance rates
MR-GB
Performance rates
10-core TRUS-GB
Significance (p-value)
- Overall Bx concord. with RP HGG
- Bx concord. with RP HGG 3
- Bx concord. with RP HGG 4
- Bx concord. with RP HGG 5
- Bx concord. with RP HGG 4/5
- PPV for Bx and RP HGG=3
88% (30/34)
100% (1212)
91% (10/11)
73% (8/11)
95% (21/22)
92% (12/13)
55% (35 of 64)
94% (17 of 18)
46% (12 of 26)
30% (6 of 20)
54% (25 of 46)
45% (17/38)
0 .001*
0.41
0.01 *
0.02 *
0.001 *
0.003 *
PSA
-
~ Overall HGG performance
- > 10 ng/ml
~ Overall HGG performance
12/34 (35%)
100% (12/12)
22/34 (65%)
82% (18/22)
44/64 (69%)
59% (26/44)
20/64 (31%)
45% (9/20)
0.01 *
0.01 *
0.01 *
0.01 *
Table 4. Performance analysis between Bx and RP cohorts. (PPV=Positive predictive
value; *=denotes significance; N.A.= Not applicable)
With MR-GB there was no over-grading while this was the case in one patient (false HGG=4
instead of 3) in the TRUS-GB cohort. The under-grading for a RP HGG=5 was 27% (3/11) for MR-
GB compared to 70% (14/20) for TRUS-GB. Furthermore, TRUS-GB showed a substantial under-
grading in 57% (8/14) of the under-graded HGG=5 cases, whereas no substantial under-grading
occurred with MR-GB.
As the MR-GB (median PSA of 12 ng/ml) and TRUS-GB groups (median PSA of 8 ng/ml) showed
a significant difference in pre-biopsy PSA levels (p=0.02), a sub-group analysis was performed
showed a 0% (0/12) undergrading
for MR-GB in patients 10 ng/ml. In contrast, in this PSA sub-group, with TRUS-GB,
under-grading occurred in 41% (18/44; p=0.01). For patients with PSA levels >10 ng/ml, MR-GB
revealed an under-grading of 18% (4/22) and TRUS-GB revealed an under-grading of 55%
(11/20; p=0.01).
211
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

Figure 1. Performance rates according to HGG categorization. 10-Core TRUS-GB vs. MR-
GB
DISCUSSION
In this prospective study, 3T Diffusion Weighted MR imaging (DWI) guided prostate tissue
sampling improved the pretreatment assessment of prostate cancer aggressiveness. The Gleason
grades as determined with DWI showed a high performance rate of 88% with prostatectomy.
This is in sharp contrast with a clinical routine 10-core TRUS biopsy protocol, which showed a
performance rate of only 55%, which is in agreement with rates reported in literature (15-17).
In this study the most abnormal regions on ADC, following a multi-parametric localization
approach of the tumour, were used to target the biopsies. To our knowledge, this is the first
prospective report on the use of DWI in obtaining prostate cancer tissue samples, which are
more representative for true prostatectomy specimen Gleason grade. These results confirm
prior retrospective studies on the ability of MR imaging to visualize tumour aggressivity and
provide a method to improve pretreatment prediction of true Gleason grades(18;19).
212
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

The importance of establishing a correct pretreatment assessment of prostate cancer
aggressiveness has generally been accepted. In recent years, a shift from radical therapy to a
more patient tailored focal therapy has been advocated (20). One of the cornerstones of
pretreatment risk stratification in order to tailor treatment on a patient level is the correct
prediction and assessment of the true Gleason grades within the tumour. Patients without
Gleason grade 4/5 components, are potential candidates for less invasive treatment options,
such as active surveillance or local therapy incl. brachytherapy or high-intensity focused
ultrasound (21). Patients with the presence of high-grade components are in definite need for
additional evaluation for the presence of extra capsular extension or metastasis to lymph nodes
or bone. In addition, high-grade PCa managed with non-curative intent, substantially reduces life
expectancy (22). An EORTC trial showed that high-risk stratified patients have a definite benefit
from adjuvant hormone therapy. Therefore, correctly stratifying patients into low/high risk is of
utmost importance (23).
Numerous studies have addressed the correlation between Gleason scores in needle biopsy and
corresponding radical prostatectomy specimens. These show, that increasing the number of
biopsies, increases the performance. For earlier studies, using sextant biopsies, under-grading
was reported in 44-60% of cases (24;25) while more recent studies with extended biopsy
schemes reported lower values of 32-38% (4;5;16;24). Most studies have shown that over-
grading (8-10%)(15;17) by biopsy cores is of less importance than under-grading. When
comparing the overall performance rates between studies, the most important factor that needs
careful consideration and interpretation is the prevalence of low-grade tumours. Using an
extended scheme with a median of 12-cores, San Fransisco et al. (26) showed an exact GS
performance rate of 76%. However, the prevalence of low-grade tumours in their RP was 72%.
This artificially increases the overall performance rates. When only evaluating high-grade
tumours (HGG of 4/5), an under-grading of 32% was still evident in their series. Data from a
large cohort from John Hopkins Hospital (27) revealed an overall GS agreement of 76%. Also
here, the prevalence of low-grade tumours in RP was high at 67%. When only the high-grade
tumours on RP were chosen, an under-grading of 42% was noted.
Our 10-core TRUS-GB revealed a 46% under-grading of tumours indentified as HGG=4/5 on RP.
This is in agreement with these two prior studies. Yet, for MR-GB, only 5% under-grading of
213
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

high-grade tumours was seen. In addition, TRUS-GB revealed a substantial under-grading in
57% of cases of the HGG 5 tumor, i.e. showing a HGG of 3. In all cases of HGG 5 under-grading,
biopsies performed by MR targeting, revealed a HGG of 4, thus showing a more acceptable
underestimation. The prevalence of HGG 3, 4 and 5 groups in our two cohorts did not show
statistically significant differences. We therefore feel that our results with MR-GB show a
substantial improvement of performance rates compared to current practice and literature. In
addition, with MR-GB, only a median of 3 biopsy cores per patient were taken, instead of 10 with
TRUS-GB.
A number of clinical important factors exist which may be associated with prostate biopsy
undergrading. Isariyawongse et al.(28) have shown that both age and PSA values are important
in this respect. Biopsies in patients with PSA values 10-20 ng/ml and PSA > 20 ng/ml had odds
ratios of 2.11 and 3.64 respectively compared to PSA < 10 ng/ml for representing undergrading
of true Gleason scores in prostatectomy. Our overall baseline PSA values for the two cohorts did
indeed show a significant difference, however, to the detriment of the MR-GB where slightly
higher PSA values were found. Usually a PSA cut-off value of 10 ng/ml is used as an integral part
in decision-making regarding further diagnostic tests or type of treatment, i.e. opting for active
surveillance(29). We therefore, performed
and those >10 ng/ml. For both subgroups, MR-
compared to TRUS-GB. Evidently, the PSA value did not influence the performance rates of
biopsies with RP findings in our study. Stackhouse et al.(30) evaluated additional factors that
may predict undergrading in biopsies. Of relevance to our study would also be their identified
factors: patient age and prostate weight (and thus prostate volume). Increasing age has been
shown to have increasing odds ratios for undergrading. In our cohort both groups had the same
median ages of 66 years (p=0.22). No significant differences in prostate volumes (p=0.61) or
dominant tumour volume (p=0.69) were seen in our cohorts. Furthermore, no difference in the
prevalence of stage pT3 disease was noticed (p=0.83) between the two cohorts.
214
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

Figure 2. Patient with PSA of 11 ng/ml. TRUS-GB revealed a Gleason 3+4. a) T-2w image
shows a large tumor region in the entire dorsal peripheral zone (arrows). On b) the ADC
maps, restriction is clearly visible for the same lesion. On DCE imaging, the Ktrans map (c)
shows irregular enhancement of the tumor. However d) within the restricted regions,
two regions with higher restriction are visible (yellow asterisks). On the corresponding
pathology step section, the tumor is delineated in light blue, corresponding to the findings
on MR. Regions with focal Gleason grade 5 are delineated with a dotted line correspond
exactly to the ADC “hot spots” findings. Final pathology showed Gleason 3+4+5, pT3
tumour.
In addition, we have evaluated two further factors that in our opinion may also represent biases
in cohorts possibly having an influence on degree of undergrading: dominant aggressive tumour
volume and tumour stage on at radical prostatectomy. In a paper by Resnick et al.(31), biopsy
and prostatectomy features of patients at first, second and third TRUS-GB session were
215
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

Figure 3. Patient with PSA 12ng/ml. Four times prior negative TRUS-GB. a) T2-w image
with focal lesion visible in right peripheral zone. b) On DCE-Ktrans map, diffuse
enhancement of the peripheral zone is seen. c) ADC derived from DWI shows focal small
lesion with clear restriction (yellow asterisk). d) True-FISP images during biopsy with
the needle guider directed towards the most suspicious region, prior to taking a MR-GB.
MR-GB revealed a Gleason 4 component. e) Prostatectomy step section showed a pT2c
tumor in the right peripheral zone (light blue=Gleason 3 and red=Gleason 4 component).
The volume of the Gleason 3 component is underestimated by the MRI, however volume
of the focal “hot-spot” on the ADC images exactly match with final pathology: Gleason 4.
evaluated. In their large cohort of 2411 patients, with each increase in the number of biopsy
sessions, the undergrading of Gleason score
second to 58% at third biopsy session, despite the increasing overall prevalence of Gleason score
6 tumors with every subsequent session. These findings would actually suggest an increased
likelihood of undergrading for our repeat biopsies. On the contrary however, despite
representing a re-biopsy session, our MR-GB still outperformed a first session 10-core TRUS-GB.
We therefore are of the opinion, that despite these minor differences between our cohorts, no
216
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

important clinical or pathological factor could be determined that might bias our MR-GB cohort
to a more favorable group regarding the likelihood of undergrading.
Diffusion weighted MR imaging is rapidly gaining importance as a valuable non-invasive
biomarker for determining tumour response to therapy in a large variety of tumours (32). In
addition, DWI is also increasingly being used to non-invasively determine tumour
aggressiveness. It’s role for assessment of aggressiveness and cellularity in breast tumours (33),
soft tissue sarcomas (34), renal tumours (35) and hepatocellular tumours (36) has been
reported before. For prostate cancer, recent data has shown that ADC values derived from the
DWI images, have a high discriminatory performance in separating low- vs. combined
intermediate- and high-grade cancers(18).
A practical utilization of our findings on a larger scale warrants some consideration. We have
chosen to obtain biopsies of the abnormal region under direct MR guidance. Despite being more
exact in targeting biopsies, its use is limited by widespread availability and practicality for a
large number of patients. We therefore envision that DWI in future should facilitate MR based
targeted biopsies under TRUS guidance once fusion software has become widely available.
A number of limitations exist. A randomized trial between MR imaging biopsies vs. TRUS biopsy
or performing both TRUS and MR guided biopsies in the same patient would represent the ideal
scenario. Our approach was, however, to determine the performance in a routine clinical setup
as performed in our hospital. A second limitation represents the relative low number of patients.
Nonetheless, differences were statistically significant, even with this low number of patients.
Furthermore, because of the equal predominant proportion of high-grade tumours in both our
cohorts, valid conclusions on the amount of TRUS-GB and MR-GB undergrading can be made,
based even on this relatively low number of patients. Although a multi-parameteric approach is
proven to be the most useful for evaluation of prostate cancer on MR imaging, it still requires a
high level of expertise and is known to suffer from observer variability(37). Our results
therefore represent findings of an expert centre which utilizes in-house developed analytical
software and numerous years of experience. This might therefore be an overoptimistic
prediction of performance attainable in smaller, non-expert institutions. A final limitation, as
thoroughly discussed previously, is the potential differences of the two cohorts. MRI and
subsequent MR guided biopsies were only performed when a first systematic TRUS-GB was
217
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

negative despite clinical suspicion for prostate cancer. However, there were no differences
between the groups, except for PSA value, where a separate sub-group analysis was made.
CONCLUSIONS
Our final conclusions are that biopsies targeted towards the most abnormal regions on 3T DWI
MR imaging represent a substantially improved method for assessment of true tumour
aggressiveness and can therefore represent an indispensable tool in the diagnosis and
management of patients with prostate cancer. This will probably also hold true for other
malignancies. Its utilization is therefore strongly advocated.
218
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

REFERENCES
1. Egevad L, Granfors T, Karlberg L, Bergh A, Stattin P. Prognostic value of the Gleason score in prostate cancer. BJU.Int. 2002 Apr;89(6):538-42.
2. Presti JC, Jr., O'Dowd GJ, Miller MC, Mattu R, Veltri RW. Extended peripheral zone biopsy schemes increase cancer detection rates and minimize variance in prostate specific antigen and age related cancer rates: results of a community multi-practice study. J.Urol. 2003 Jan;169(1):125-9.
3. Siu W, Dunn RL, Shah RB, Wei JT. Use of extended pattern technique for initial prostate biopsy. J.Urol. 2005 Aug;174(2):505-9.
4. Divrik RT, Eroglu A, Sahin A, Zorlu F, Ozen H. Increasing the number of biopsies increases the concordance of Gleason scores of needle biopsies and prostatectomy specimens. Urol.Oncol. 2007 Sep;25(5):376-82.
5. Kvale R, Moller B, Wahlqvist R, Fossa SD, Berner A, Busch C, Kyrdalen AE, Svindland A, Viset T, Halvorsen OJ. Concordance between Gleason scores of needle biopsies and radical prostatectomy specimens: a population-based study. BJU.Int. 2008 Dec 22.
6. Lattouf JB, Saad F. Gleason score on biopsy: is it reliable for predicting the final grade on pathology? BJU.Int. 2002 Nov;90(7):694-8.
7. Delongchamps NB, Rouanne M, Flam T, Beuvon F, Liberatore M, Zerbib M, Cornud F. Multiparametric magnetic resonance imaging for the detection and localization of prostate cancer: combination of T2-weighted, dynamic contrast-enhanced and diffusion-weighted imaging. BJU.Int. 2010 Nov 2.
8. Kitajima K, Kaji Y, Fukabori Y, Yoshida K, Suganuma N, Sugimura K. Prostate cancer detection with 3 T MRI: comparison of diffusion-weighted imaging and dynamic contrast-enhanced MRI in combination with T2-weighted imaging. J.Magn Reson.Imaging 2010 Mar;31(3):625-31.
9. Anastasiadis AG, Lichy MP, Nagele U, Kuczyk MA, Merseburger AS, Hennenlotter J, Corvin S, Sievert KD, Claussen CD, Stenzl A, et al. MRI-guided biopsy of the prostate increases diagnostic performance in men with elevated or increasing PSA levels after previous negative TRUS biopsies. Eur.Urol. 2006 Oct;50(4):738-48.
10. Hambrock T, Somford DM, Hoeks C, Bouwense SA, Huisman H, Yakar D, van O, I, Witjes JA, Futterer JJ, Barentsz JO. Magnetic resonance imaging guided prostate biopsy in men with repeat negative biopsies and increased prostate specific antigen. J.Urol. 2010 Feb;183(2):520-7.
11. deSouza NM, Riches SF, Vanas NJ, Morgan VA, Ashley SA, Fisher C, Payne GS, Parker C. Diffusion-weighted magnetic resonance imaging: a potential non-invasive marker of tumour aggressiveness in localized prostate cancer. Clin.Radiol. 2008 Jul;63(7):774-82.
12. Tamada T, Sone T, Jo Y, Toshimitsu S, Yamashita T, Yamamoto A, Tanimoto D, Ito K. Apparent diffusion coefficient values in peripheral and transition zones of the prostate: comparison between normal and malignant prostatic tissues and correlation with histologic grade. J.Magn Reson.Imaging 2008 Sep;28(3):720-6.
13. Hambrock T, Futterer JJ, Huisman HJ, Hulsbergen-vandeKaa C, van Basten JP, van O, I, Witjes JA, Barentsz JO. Thirty-two-channel coil 3T magnetic resonance-guided biopsies of prostate tumor suspicious regions identified on multimodality 3T magnetic resonance imaging: technique and feasibility. Invest Radiol. 2008 Oct;43(10):686-94.
14. Epstein JI, Allsbrook WC, Jr., Amin MB, Egevad LL. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am.J.Surg.Pathol. 2005 Sep;29(9):1228-42.
15. Boorjian SA, Karnes RJ, Crispen PL, Rangel LJ, Bergstralh EJ, Sebo TJ, Blute ML. The impact of discordance between biopsy and pathological Gleason scores on survival after radical prostatectomy. J.Urol. 2009 Jan;181(1):95-104.
16. Coogan CL, Latchamsetty KC, Greenfield J, Corman JM, Lynch B, Porter CR. Increasing the number of biopsy cores improves the concordance of biopsy Gleason score to prostatectomy Gleason score. BJU.Int. 2005 Aug;96(3):324-7.
17. Serkin FB, Soderdahl DW, Cullen J, Chen Y, Hernandez J. Patient risk stratification using Gleason score concordance and upgrading among men with prostate biopsy Gleason score 6 or 7. Urol.Oncol. 2008 Dec 29.
18. Hambrock T, Somford DM, Huisman HJ, van O, I, Witjes JA, Hulsbergen-Van de Kaa CA, Scheenen T, Barentsz JO. Relationship between apparent diffusion coefficients at 3.0-T MR imaging and gleason grade in peripheral zone prostate cancer. Radiology 2011 May;259(2):453-61.
219
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10
19. Verma S, Rajesh A, Morales H, Lemen L, Bills G, Delworth M, Gaitonde K, Ying J, Samartunga R, Lamba M. Assessment of aggressiveness of prostate cancer: correlation of apparent diffusion coefficient with histologic grade after radical prostatectomy. AJR Am.J.Roentgenol. 2011 Feb;196(2):374-81.
20. Ahmed HU, Pendse D, Illing R, Allen C, van der Meulen JH, Emberton M. Will focal therapy become a standard of care for men with localized prostate cancer? Nat.Clin.Pract.Oncol. 2007 Nov;4(11):632-42.
21. de la RJ, Ahmed H, Barentsz J, Johansen TB, Brausi M, Emberton M, Frauscher F, Greene D, Harisinghani M, Haustermans K, et al. Focal therapy in prostate cancer-report from a consensus panel. J.Endourol. 2010 May;24(5):775-80.
22. Tewari A, Divine G, Chang P, Shemtov MM, Milowsky M, Nanus D, Menon M. Long-term survival in men with high grade prostate cancer: a comparison between conservative treatment, radiation therapy and radical prostatectomy--a propensity scoring approach. J.Urol. 2007 Mar;177(3):911-5.
23. Bolla M, Van TG, Warde P, Dubois JB, Mirimanoff RO, Storme G, Bernier J, Kuten A, Sternberg C, Billiet I, et al. External irradiation with or without long-term androgen suppression for prostate cancer with high metastatic risk: 10-year results of an EORTC randomised study. Lancet Oncol. 2010 Nov;11(11):1066-73.
24. Paulson DF. Impact of radical prostatectomy in the management of clinically localized disease. J.Urol. 1994 Nov;152(5 Pt 2):1826-30.
25. Steinberg DM, Sauvageot J, Piantadosi S, Epstein JI. Correlation of prostate needle biopsy and radical prostatectomy Gleason grade in academic and community settings. Am.J.Surg.Pathol. 1997 May;21(5):566-76.
26. San F, I, Dewolf WC, Rosen S, Upton M, Olumi AF. Extended prostate needle biopsy improves concordance of Gleason grading between prostate needle biopsy and radical prostatectomy. J.Urol. 2003 Jan;169(1):136-40.
27. Fine SW, Epstein JI. A contemporary study correlating prostate needle biopsy and radical prostatectomy Gleason score. J.Urol. 2008 Apr;179(4):1335-8.
28. Isariyawongse BK, Sun L, Banez LL, Robertson C, Polascik TJ, Maloney K, Donatucci C, Albala D, Mouraviev V, Madden JF, et al. Significant discrepancies between diagnostic and pathologic Gleason sums in prostate cancer: the predictive role of age and prostate-specific antigen. Urology 2008 Oct;72(4):882-6.
29. Dall'Era MA, Konety BR, Cowan JE, Shinohara K, Stauf F, Cooperberg MR, Meng MV, Kane CJ, Perez N, Master VA, et al. Active surveillance for the management of prostate cancer in a contemporary cohort. Cancer 2008 Jun 15;112(12):2664-70.
30. Stackhouse DA, Sun L, Schroeck FR, Jayachandran J, Caire AA, Acholo CO, Robertson CN, Albala DM, Polascik TJ, Donatucci CF, et al. Factors predicting prostatic biopsy Gleason sum under grading. J.Urol. 2009 Jul;182(1):118-22.
31. Resnick MJ, Lee DJ, Magerfleisch L, Vanarsdalen KN, Tomaszewski JE, Wein AJ, Malkowicz SB, Guzzo TJ. Repeat prostate biopsy and the incremental risk of clinically insignificant prostate cancer. Urology 2011 Mar;77(3):548-52.
32. Harry VN, Semple SI, Parkin DE, Gilbert FJ. Use of new imaging techniques to predict tumour response to therapy. Lancet Oncol. 2010 Jan;11(1):92-102.
33. Costantini M, Belli P, Rinaldi P, Bufi E, Giardina G, Franceschini G, Petrone G, Bonomo L. Diffusion-weighted imaging in breast cancer: relationship between apparent diffusion coefficient and tumour aggressiveness. Clin.Radiol. 2010 Dec;65(12):1005-12.
34. Schnapauff D, Zeile M, Niederhagen MB, Fleige B, Tunn PU, Hamm B, Dudeck O. Diffusion-weighted echo-planar magnetic resonance imaging for the assessment of tumor cellularity in patients with soft-tissue sarcomas. J.Magn Reson.Imaging 2009 Jun;29(6):1355-9.
35. Squillaci E, Manenti G, Cova M, Di RM, Miano R, Palmieri G, Simonetti G. Correlation of diffusion-weighted MR imaging with cellularity of renal tumours. Anticancer Res. 2004 Nov;24(6):4175-9.
36. Muhi A, Ichikawa T, Motosugi U, Sano K, Matsuda M, Kitamura T, Nakazawa T, Araki T. High-b-value diffusion-weighted MR imaging of hepatocellular lesions: estimation of grade of malignancy of hepatocellular carcinoma. J.Magn Reson.Imaging 2009 Nov;30(5):1005-11.
37. Lim HK, Kim JK, Kim KA, Cho KS. Prostate cancer: apparent diffusion coefficient map with T2-weighted images for detection--a multireader study. Radiology 2009 Jan;250(1):145-51.
220
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10

Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10
19. Verma S, Rajesh A, Morales H, Lemen L, Bills G, Delworth M, Gaitonde K, Ying J, Samartunga R, Lamba M. Assessment of aggressiveness of prostate cancer: correlation of apparent diffusion coefficient with histologic grade after radical prostatectomy. AJR Am.J.Roentgenol. 2011 Feb;196(2):374-81.
20. Ahmed HU, Pendse D, Illing R, Allen C, van der Meulen JH, Emberton M. Will focal therapy become a standard of care for men with localized prostate cancer? Nat.Clin.Pract.Oncol. 2007 Nov;4(11):632-42.
21. de la RJ, Ahmed H, Barentsz J, Johansen TB, Brausi M, Emberton M, Frauscher F, Greene D, Harisinghani M, Haustermans K, et al. Focal therapy in prostate cancer-report from a consensus panel. J.Endourol. 2010 May;24(5):775-80.
22. Tewari A, Divine G, Chang P, Shemtov MM, Milowsky M, Nanus D, Menon M. Long-term survival in men with high grade prostate cancer: a comparison between conservative treatment, radiation therapy and radical prostatectomy--a propensity scoring approach. J.Urol. 2007 Mar;177(3):911-5.
23. Bolla M, Van TG, Warde P, Dubois JB, Mirimanoff RO, Storme G, Bernier J, Kuten A, Sternberg C, Billiet I, et al. External irradiation with or without long-term androgen suppression for prostate cancer with high metastatic risk: 10-year results of an EORTC randomised study. Lancet Oncol. 2010 Nov;11(11):1066-73.
24. Paulson DF. Impact of radical prostatectomy in the management of clinically localized disease. J.Urol. 1994 Nov;152(5 Pt 2):1826-30.
25. Steinberg DM, Sauvageot J, Piantadosi S, Epstein JI. Correlation of prostate needle biopsy and radical prostatectomy Gleason grade in academic and community settings. Am.J.Surg.Pathol. 1997 May;21(5):566-76.
26. San F, I, Dewolf WC, Rosen S, Upton M, Olumi AF. Extended prostate needle biopsy improves concordance of Gleason grading between prostate needle biopsy and radical prostatectomy. J.Urol. 2003 Jan;169(1):136-40.
27. Fine SW, Epstein JI. A contemporary study correlating prostate needle biopsy and radical prostatectomy Gleason score. J.Urol. 2008 Apr;179(4):1335-8.
28. Isariyawongse BK, Sun L, Banez LL, Robertson C, Polascik TJ, Maloney K, Donatucci C, Albala D, Mouraviev V, Madden JF, et al. Significant discrepancies between diagnostic and pathologic Gleason sums in prostate cancer: the predictive role of age and prostate-specific antigen. Urology 2008 Oct;72(4):882-6.
29. Dall'Era MA, Konety BR, Cowan JE, Shinohara K, Stauf F, Cooperberg MR, Meng MV, Kane CJ, Perez N, Master VA, et al. Active surveillance for the management of prostate cancer in a contemporary cohort. Cancer 2008 Jun 15;112(12):2664-70.
30. Stackhouse DA, Sun L, Schroeck FR, Jayachandran J, Caire AA, Acholo CO, Robertson CN, Albala DM, Polascik TJ, Donatucci CF, et al. Factors predicting prostatic biopsy Gleason sum under grading. J.Urol. 2009 Jul;182(1):118-22.
31. Resnick MJ, Lee DJ, Magerfleisch L, Vanarsdalen KN, Tomaszewski JE, Wein AJ, Malkowicz SB, Guzzo TJ. Repeat prostate biopsy and the incremental risk of clinically insignificant prostate cancer. Urology 2011 Mar;77(3):548-52.
32. Harry VN, Semple SI, Parkin DE, Gilbert FJ. Use of new imaging techniques to predict tumour response to therapy. Lancet Oncol. 2010 Jan;11(1):92-102.
33. Costantini M, Belli P, Rinaldi P, Bufi E, Giardina G, Franceschini G, Petrone G, Bonomo L. Diffusion-weighted imaging in breast cancer: relationship between apparent diffusion coefficient and tumour aggressiveness. Clin.Radiol. 2010 Dec;65(12):1005-12.
34. Schnapauff D, Zeile M, Niederhagen MB, Fleige B, Tunn PU, Hamm B, Dudeck O. Diffusion-weighted echo-planar magnetic resonance imaging for the assessment of tumor cellularity in patients with soft-tissue sarcomas. J.Magn Reson.Imaging 2009 Jun;29(6):1355-9.
35. Squillaci E, Manenti G, Cova M, Di RM, Miano R, Palmieri G, Simonetti G. Correlation of diffusion-weighted MR imaging with cellularity of renal tumours. Anticancer Res. 2004 Nov;24(6):4175-9.
36. Muhi A, Ichikawa T, Motosugi U, Sano K, Matsuda M, Kitamura T, Nakazawa T, Araki T. High-b-value diffusion-weighted MR imaging of hepatocellular lesions: estimation of grade of malignancy of hepatocellular carcinoma. J.Magn Reson.Imaging 2009 Nov;30(5):1005-11.
37. Lim HK, Kim JK, Kim KA, Cho KS. Prostate cancer: apparent diffusion coefficient map with T2-weighted images for detection--a multireader study. Radiology 2009 Jan;250(1):145-51.
220
Prospective Assessment of PCa Aggressiveness using 3T DWI-MRI Guided Biopsies vs. 10-core TRUS Biopsy Cohort
10


PART FOUR
COMPUTER ASSISTED DIAGNOSIS OF PROSTATE
CANCER


CHAPTER 11
The Effect of Inter-patient Normal Peripheral Zone Apparent Diffusion
Coefficient Variation on the Prediction of Prostate Cancer
Aggressiveness
Geert Litjens; Thomas Hambrock; Jelle Barentsz et al.
CHAPTER 11CHAPTER 11

The effect of inter-patient normal peripheral zone Apparent Diffusion Coefficient variation on the Prediction of Prostate Cancer Aggressiveness
Radiology (Accepted)
Litjens G, Hambrock T, Barentsz J, Huisman J
Advances in knowledge: A large inter-patient variability exists for normal peripheral zone apparent diffusion
coefficient values (1.2 2.0 x10-3 mm2/s) derived from diffusion weighted MR imaging at 3
Tesla. This inter-patient variability is significant (p=0.006).
Correcting for inter-patient variability results in a significant increase in diagnostic accuracy
for separating low-grade and high-grade cancer, from 0.91 to 0.96 for the area under the
ROC curve (p=0.04).
A clinically useful nomogram is created to aid the radiologists in improving his assessment
of prostate cancer aggressiveness.
Implications for patient care:
Correcting for patient related variation in tissue composition allows an improved method
for noninvasively predicting prostate Gleason grade, which is a very important marker used
for prognostication and management.
Summary Statement
Peripheral Zone ADC values show a significant inter-patient variation,
which has a significant effect on the prediction of prostate cancer
aggressiveness. Correcting this effect results in a significant increase in
diagnostic accuracy.
222
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11

ABSTRACT
Purpose: To determine the inter-patient variability of prostate peripheral zone (PZ) apparent
diffusion coefficient values (ADC) at 3T and the effect this has on the assessment of prostate cancer
aggressiveness.
Materials and Methods: The requirement to obtain institutional review board approval was
waived. Intra- and inter-patient variation of PZ ADC values was determined by repeated
measurements of normal PZ ADC values in a retrospective cohort of 10 consecutive patients with
high PSA level, negative transrectal ultrasound biopsy and three separate MR imaging sessions at
3T. In these patients no signs of cancer were found in all three imaging sessions. The effect of the
intra, and inter-patient variation on assessment of prostate cancer aggressiveness was examined in
a second retrospective cohort of 51 patients with PZ prostate cancer who underwent an MRI, prior
to prostatectomy. Whole-mount step-section pathology served as reference standard for placement
of regions of interest (ROIs) on PZ tumours and normal peripheral zone. Repeated-measures
ANOVA were performed to determine the significance of the inter-patient variations in PZ ADC
values. Linear logistic regression was used to assess whether incorporating normal PZ ADC values
improves the prediction of cancer aggressiveness. The effect on the diagnostic performance was
assessed using receiver-operating characteristic (ROC) analysis.
Results: The repeated-measures ANOVA revealed that inter-patient variability (1.2 2.0 x10-3
mm2/s) was significantly larger than measurement variability (average measurement standard
deviation 0.068 ± 0.027 x10-3 mm2/s) (p = 0.006). Analysis of standalone tumour ADC values
showed an AUC of 0.91 for discriminating low- vs. high-grade tumours. Incorporating normal PZ
ADC using linear logistic regression, significantly improved the AUC to 0.96 (p = 0.04).
Conclusion: Peripheral zone ADC values show a significant inter-patient variation, which has a
substantial effect on the prediction of prostate cancer aggressiveness. Accounting for this effect
results in a significant increase in diagnostic accuracy.
223
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11
ABSTRACT
Purpose: To determine the inter-patient variability of prostate peripheral zone (PZ) apparent
diffusion coefficient values (ADC) at 3T and the effect this has on the assessment of prostate cancer
aggressiveness.
Materials and Methods: The requirement to obtain institutional review board approval was
waived. Intra- and inter-patient variation of PZ ADC values was determined by repeated
measurements of normal PZ ADC values in a retrospective cohort of 10 consecutive patients with
high PSA level, negative transrectal ultrasound biopsy and three separate MR imaging sessions at
3T. In these patients no signs of cancer were found in all three imaging sessions. The effect of the
intra, and inter-patient variation on assessment of prostate cancer aggressiveness was examined in
a second retrospective cohort of 51 patients with PZ prostate cancer who underwent an MRI, prior
to prostatectomy. Whole-mount step-section pathology served as reference standard for placement
of regions of interest (ROIs) on PZ tumours and normal peripheral zone. Repeated-measures
ANOVA were performed to determine the significance of the inter-patient variations in PZ ADC
values. Linear logistic regression was used to assess whether incorporating normal PZ ADC values
improves the prediction of cancer aggressiveness. The effect on the diagnostic performance was
assessed using receiver-operating characteristic (ROC) analysis.
Results: The repeated-measures ANOVA revealed that inter-patient variability (1.2 2.0 x10-3
mm2/s) was significantly larger than measurement variability (average measurement standard
deviation 0.068 ± 0.027 x10-3 mm2/s) (p = 0.006). Analysis of standalone tumour ADC values
showed an AUC of 0.91 for discriminating low- vs. high-grade tumours. Incorporating normal PZ
ADC using linear logistic regression, significantly improved the AUC to 0.96 (p = 0.04).
Conclusion: Peripheral zone ADC values show a significant inter-patient variation, which has a
substantial effect on the prediction of prostate cancer aggressiveness. Accounting for this effect
results in a significant increase in diagnostic accuracy.

INTRODUCTION
Only 15% of men diagnosed with prostate cancer show a disease specific mortality. The mortality in
the US in 2010 was 30000, with 220000 new prostate cancer cases diagnosed (1). Thus in order to
tailor treatment from more radical therapy to active surveillance protocols, accurate cancer
aggressiveness risk stratification is very important. The most useful estimator of cancer
aggressiveness is the Gleason score (GS), a histopathological scoring system used on biopsy and
prostatectomy specimens. It has become such an integral part in prostate cancer evaluation, that
patient management is largely influenced by the assessment thereof (2,3,4).
Recently, the apparent diffusion coefficient (ADC) values determined from diffusion-weighted
magnetic resonance imaging (DWI-MRI) showed to be inversely correlated to GS (5,6,7). As a result,
ADC has been proposed as a useful non-invasive biomarker for prostate cancer aggressiveness (5,7).
However, the discriminative power of ADC depends in part on the variability of the ADC
measurement. This variability is machine i.e. vendor, settings, noise - and patient dependent, the
latter caused by natural tissue heterogeneity. Based on the large inter-patient distribution of normal
PZ ADC values (1.2 2.2 x10-3 mm2/s) observed on a single MR scanner, we hypothesize that a
substantial histo-physiological heterogeneity between patients must exist (inter-patient variation)
(8,7).
Inter-patient ADC variation could affect the discriminative power of ADC both for prostate cancer
localization as well as for the determination of prostate cancer aggressiveness. Since normal
prostate PZ tissue fluctuates significantly in ADC value, the ADC values of an aggressive tumour may
show similar fluctuations. If normal PZ and tumour ADC are correlated, considering both
simultaneously, may lead to better estimates of aggressiveness.
The purpose of this study was to determine the inter-patient variability of prostate peripheral zone
(PZ) apparent diffusion coefficient values (ADC) at 3T and the effect this has on the assessment of
prostate cancer aggressiveness.
224
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11

MATERIALS AND METHODS
Patients
Imaging data of two retrospective patient cohorts was used in our experiments. The requirement to
obtain institutional review board approval was waived for both cohorts. To determine the
significance of the inter-patient variance relative to the measurement variability, we included 10
consecutive patients (February 2008 to June 2011, interval between scans: 6 12 months) who had
repeated measurements of normal PZ ADC values at 3 three separate MR imaging sessions at 3T.
The indication for the studies was continuously high PSA level and at least one negative transrectal
ultrasound biopsy. Patients were followed up if PSA level remained high. In these patients no cancer
was found in all three imaging sessions by an expert radiologist (J.O.B., with 18 years of experience).
If a suspicious lesion was indicated by the radiologist subsequent MR-guided biopsy found no traces
of tumour.
In addition, to determine the effect of the inter-patient variation of ADC on the prediction of
prostate cancer aggressiveness, a second cohort was included. Between August 2006 and January
2009, 51 consecutive patients with biopsy proven PZ prostate cancer (in total 61 tumours),
scheduled for radical prostatectomy, were referred from the departments of urology at the Radboud
University Nijmegen Medical Centre and the Canisius Wilhelmina Ziekenhuis in Nijmegen for MRI of
the prostate (7).
MR Imaging Protocol
MR imaging of the prostate was performed using a 3T MR scanner (Siemens Trio Tim, Erlangen,
Germany). The first cohort of 10 patients was scanned only with the pelvic phased array coils.
The second cohort was scanned with the use of a combined endorectal coil (ERC) (Medrad,
Pittsburgh, U.S.A) and pelvic phased array coils. The ERC was filled with a 40-mL Perfluorocarbon
preparation (Fomblin, Solvay-Solexis, Milan, Italy)
225
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11

In both cohorts peristalsis was suppressed with an intramuscular administration of 20-mg
Butylscopolaminebromide (Buscopan, Boehringer-Ingelheim, Ingelheim, Germany) and 1 mg of
glucagon (Glucagen, Nordisk, Gentofte, Denmark).
The MR imaging protocol included: anatomical T2-weighted turbo spin echo sequences in axial,
sagittal and coronal planes covering the entire prostate and seminal vesicles. Axial diffusion
weighted imaging was performed using a single-shot-echo-planar imaging sequence with diffusion
modules and fat suppression pulses implemented. Water diffusion was measured in 3-scan trace
mode using b-values of 0, 50, 500, and 800 s/mm2. ADC-maps were automatically calculated by the
scanner software using all b-values. . Complete pulse sequence details can be found in table 1 for the
first cohort containing 10 patients with repeated measurements and table 2 for the second cohort.
Sequence Type
Slice thickness
Number of slices
In-plane resolution
TR TE Averages GRAPPA b-values
T2-w Axial
TSE 3.5-4 mm 13-19 0.6 mm 3540 ms 104 ms 2 -3 - -
T2-w Coronal
TSE 3.5-4 mm 15-19 0.6 0.8 mm 3350 ms 105 ms 2 3 - -
T2-w Sagital
TSE 3.5-4 mm 15-19 0.6-0.8 mm 3810 ms 105 ms 2 3 - -
DWI SE-EPI 3.5-4 mm 15-20 1.6-2.0 mm 2300 ms 61 ms 6 - 10 2 0, 50, 500, 800 mm2/s
T1-w DCE GRE
(FLASH 3D)
3.5-4 mm 14 1.8 mm 37 ms 1.47 ms 1 - -
Table 1: Pulse sequence details for the first patient cohort with repeated measurements. In-
plane resolution is the same in both directions.
226
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11

Sequence Type
Slice thickness
Number of slices
In-plane resolution
TR TE Averages GRAPPA b-values
T2-w Axial
TSE 4 mm 15-19 0.4 mm 3540 ms 104 ms 2 - -
T2-w Coronal
TSE 4 mm 15-19 0.5 mm 3350 ms 105 ms 2 - -
T2-w Sagital
TSE 4 mm 15-19 0.5 mm 3810 ms 105 ms 2 - -
DWI SE-EPI 4 mm 15-19 2.0 mm 2800 ms 81 ms 10 2 0, 50, 500, 800 mm2/s
T1-w DCE GRE
(FLASH 3D)
4 mm 14 1.8 mm 37 ms 1.47 ms 1 - -
Table 2: Pulse sequence details for the second patient cohort. In-plane resolution is the same in both
directions.
Reconstructed Whole-Mount Step-Section Preparation
The second cohort of patients underwent radical prostatectomy after imaging. After the radical
prostatectomy, prostate specimens were uniformly processed and entirely submitted for histologic
investigation. After histologic staining, all specimens were evaluated by one expert urological
pathologist (C.A.H.v.d.K. with 17 years of experience). Each individual tumour was graded according
to the 2005 International Society of Urological Pathology Modified Gleason Grading System.
Peripheral zone tumours, with a size of >0.5cc in volume, were divided in two groups, and classified
as low- and high-grade tumours. Tumours with a Gleason grade 4 or 5 component were defined as
high-grade. Low-grade tumours were defined as tumours harboring only Gleason grades 2 and 3.
227
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11

Annotation of MR images
All annotations were performed using an in-house developed MR viewing and reporting system. In
the first cohort the center slice of the prostate in the axial direction was used to annotate the
peripheral zone. For this slice the whole peripheral zone was annotated and the median ADC value
was extracted from this annotation.
For the second cohort, ADC maps were acquired in the same orientation and of similar thickness as
the histopathology step-section. A previously described translation technique was used to match
every tumour containing histopathology step-section to a corresponding ADC map (7). Using
histopathology as gold standard, a region of interest (ROI) was placed by one radiologist (T.H. with
four years of experience) and one urologist (with one year of experience) in consensus, on the ADC
maps. The size and extent of the ROI were chosen such that it matched the tumour size and extent
obtained from histological examination as closely as possible. Median ADC values were extracted for
each tumour slice separately. In clinical practice, the ADC slice revealing the lowest signal intensity
for tumour alerts radiologists. Therefore, for each individual PZ tumour, the tumour slice revealing
the lowest ADC values was used for further assessment (7).
Lastly, to determine the effect of incorporating normal PZ ADC values on the prediction of cancer
aggressiveness, an ROI was placed in the normal PZ tissue of every patient. This region was always
selected adjacent to the tumour, in order to be the most representative area of normal PZ ADC value
at the tumour location. This was done to attempt to minimize intra-patient heterogeneity. Median
ADC values were extracted from all ROIs. Median values were used because they are more robust to
image artifacts that might occur due to ADC calculation by the scanner.
Statistical analysis
Our first hypothesis is that there is a significant degree of inter-patient variation in normal PZ ADC
values. This was assessed using a repeated-measures ANOVA. The repeated measure was the
median ADC value of normal PZ tissue, which was obtained three times for each of the 10 patients in
the first cohort.
228
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11

Our second hypothesis is that joint analysis of the normal PZ ADC values and the tumour ADC values
will result in an improved prediction of cancer aggressiveness, because this implicitly corrects for
the inter-patient variations in normal PZ ADC. Multivariate linear logistic regression was used to
test this hypothesis. We can express a regression model of cancer grade as:
Z = C + T ADCT + N ADCN (1)
e z p = (2)
1 + e z
The p indicates the probability that a cancer is high-grade and the ADC variables indicate the
median ADC of the corresponding ROI. Subscripts T and N are tumour and normal PZ respectively.
The beta terms are the regression coefficient corresponding to these variables. Equation 2
represents the conversion from z to the probability p.
The linear logistic regression results in values for and and the significance of these variables
in the regression model. Two regression models were created to compare diagnostic performance:
using only tumour ADC values and using tumour and normal PZ ADC values. SPSS (SPSS, version
16.0.01, Chicago, U.S.A.) was used for the statistical analysis. Furthermore, a visual assessment is
given for the correlation between tumour ADC and normal peripheral zone ADC by plotting the low-
and high-grade tumours with respect to their ADC values and the corresponding normal PZ ADC
values.
Our third hypothesis is that the improved prediction of prostate cancer aggressiveness may result in
a significant improvement in diagnostic accuracy in separating low- and high-grade cancer.
Receiver-operating characteristic (ROC) curves were constructed for a standalone tumour ADC
regression model and the regression model, which incorporates normal PZ ADC values. The areas
under the ROC curves were tested for significant differences using the ROCKIT software package
(Kurt Rossmann Laboratories, University of Chicago, Chicago) (9).
229
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11

Nomogram construction
Additionally, the regression model incorporating tumour and normal PZ ADC can be used to
construct a nomogram by evaluating the obtained equation for a range of ADC values. The ranges
used to construct the nomogram are 0.5 1.7 x10-3 mm2/s for the tumour ADC value and 0.8 2.2
x10-3 mm2/s for the normal PZ ADC value. These ranges are slightly larger than the ranges found in
this study to accommodate more extreme values.
RESULTS
Assessment of inter-patient variation of normal PZ ADC values
Normal PZ ADC values differed significantly between patients relative to measurement variability
(p-value < 0.001) as assessed using the repeated measures ANOVA. The ADC measurements are
plotted in figure 1.
Figure 1: Three median ADC measurements of the peripheral zone of 10 patients. The black
dots represent the individual measurements, the vertical axis shows the median ADC value,
the horizontal axis shows to which patient the measurement belongs
230
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11

Effect of including normal PZ ADC values in the prediction of cancer aggressiveness
Normal peripheral zone ADC correlates with ADC of high-grade tumours. Its addition to the
regression model results in a significantly improved prediction of aggressiveness (p = 0.01). This
was determined using the logistic regression procedure; the results are summarized in table 3.
Included parameters in the model
Tumour median ADC Tumour and normal PZ median ADC
9.103 0.000 -18.82 0.003
- - 13.43 0.013
C 10.76 0.000 0.126 0.978
Table 3: Result of the linear logistic regression for three regressions based on equation 1 and
2. Regressions performed: using only tumour ADC and using tumor and normal PZ median
ADC. The second row shows the values used in each regression. The regression parameters
are presented in the bottom three rows, their value and significance respectively for each
regression.
Both regression models show a significant contribution of the tumour ADC (p = 0.003). Normal PZ
ADC values also show a significant contribution to the regression model (p = 0.01).
The regression model using standalone tumour ADC values can then be expressed as:
z = 10.76 9.103 ADCT (3)
and the model combining tumour and normal PZ ADC values can be expressed as:
z = 0.126 18.82 ADCT + 13.43 ADCN (4)
231
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11

In combination with equation 2 these models result in a probability that a given sample is a high-
grade cancer. The model incorporating normal PZ ADC (Eq. 4), together with the data used in the
regression, is shown in figure 2. This plot indicates that a relatively high tumour ADC value might
still constitute a high-grade tumour if the normal PZ ADC is high. In addition one can appreciate that
using a static threshold on tumour ADC (a vertical line/contour in figure 2) to determine cancer
aggressiveness could result in incorrect diagnosis in some patients.
Figure 2: Decision Boundary at p=.5 of the logistic regression model. The line represents the
decision boundary, the green dots the low-grade cancer and the red dots the high-grade
cancers.
232
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11

Diagnostic performance of the regression models
Including normal PZ, significantly (p = 0.04) improved the diagnostic accuracy. The ROC curves for
the regression models in equations 3 and 4 are shown in figure 3. The area under the curve
increases from 0.91 to 0.96.
Figure 3: ROC curve of the regression models. The red line shows the diagnostic accuracy
when including the adjacent PZ tissue median ADC in addition to the tumor ADC, the blue line
show the diagnostic accuracy when only using tumor ADC
233
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11

Nomogram
The constructed nomogram is shown in figure 4. This nomogram can be used in a clinical setup to
quickly lookup the change of a certain region with the peripheral zone being a aggressive cancer.
Figure 4: Contour of the probabilities of having an aggressive cancer given the adjacent PZ
tissue ADC (vertical axis) and the tumor ADC (horizontal axis). The point corresponding to
these two values will correspond to the probability of a high-grade cancer. The probability
values are specified along the contours and in the color bar on the right of the figure.
234
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11

DISCUSSION
In this study we have shown that there is a significant inter-patient variation in normal peripheral
zone ADC values (1.2 2.0 x10-3 mm2/s), which cannot be solely attributed to measurement
variability (average measurement standard deviation 0.068 ± 0.027 x10-3 mm2/s). We hypothesize
that the inter-patient variations arise from natural variations in prostate physiology.
Secondly, adding normal PZ ADC values to the linear logistic regression, results in a significantly
improved prediction of cancer aggressiveness (p = 0.01). This suggests that tumour ADC values
normal PZ tissue composition.
Thirdly, the improvement also results in an increased area under the ROC curve, from 0.91 to 0.96
(p < 0.05), thus an improved diagnostic accuracy.
This study has a number of limitations. First, the use of ADC to assess aggressiveness of transition
zone tumours has not been investigated in this study. Second, this study was limited to the
peripheral zone. This was done because it is known that ADC in peripheral and transition zone
tumours can differ substantially. However, the majority of prostate tumours arise in the PZ. Third,
the annotation of ROIs was performed by a single observer; the effect of the inter-observer
variability on the regression model was not assessed. Our nomogram must be tested and validated
in a prospective multi-reader study.
CONCLUSION
In conclusion, there is a large inter-patient variation in prostate peripheral zone ADC values. This
variation propagates into tumour ADC values. Compensating for this variation by combining tumour
and normal PZ ADC when assessing cancer grade significantly increases diagnostic performance.
235
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11

REFERENCES
1. Jemal A, Siegel R, Xu J, and Ward E. Cancer statistics, 2010. CA Cancer J Clin, 60:277 300, 2010.
2. Blute M.L, Bergstralh E.J, Iocca A, Scherer B, and Zincke H. Use of gleason score, prostate specific antigen, seminal vesicle and margin status to predict biochemical failure after radical prostatectomy. J Urol, 165(1):119 125 2001.
3. Egevad L, Granfors T, Karlberg L, Bergh A, and Stattin P. Percent gleason grade 4/5 as prognostic factor in prostate cancer diagnosed at transurethral resection. J Urol, 168(2):509 513 2002.
4. Narain V, Bianco F.J, Grignon D.J, Sakr W.A, Pontes J.E, and Wood D.P. How accurately does prostate biopsy gleason score predict pathologic findings and disease free survival? Prostate, 49(3):185 190 2001.
5. Itou Y, Nakanishi K, Narumi Y, Nishizawa Y, and Tsukuma H. Clinical utility of apparent diffusion coefficient (ADC) values in patients with prostate cancer: can ADC values contribute to assess the aggressiveness of prostate cancer? J Magn Reson Imaging, 33(1):167 172 2011.
6. Turkbey B, Pinto P.A, Mani H, Bernardo M, Pang Y, McKinney Y.L, Khurana K, Ravizzini G.C, Albert P.S, Merino M.J, and Choyke P.L. Prostate cancer: value of multiparametric mr imaging at 3 t for detection histopathologic correlation. Radiology, 255(1):89 99 2010.
7. Relation of Apparent Diffusion Coefficient Values at 3 Tesla Magnetic Resonance Imaging with Prostate Cancer Gleason Grade in the Peripheral Zone. Hambrock T, Somford D, Huisman H, van Oort I, Witjes J, Hulsbergen van de Kaa C, Scheenen T, Barentsz JO. Radiology 2011 May; 259 (2): 453-461
8. Vargas H.A, Akin O, Franiel T, Mazaheri Y, Zheng J, Moskowitz C, Udo K, Eastham J, and Hricak H. Diffusion-weighted endorectal MR imaging at 3 T for prostate cancer: Tumour detection and assessment of aggressiveness. Radiology 259(3):775-784 2011.
9. Metz C.E, Herman B.A, and Roe C.A. Statistical comparison of two roc-curve estimates obtained from partially-paired datasets. Med Decis Making, 18(1):110 121, 1998.
236
Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11

Effect of Inter-patient Normal Peripheral Zone ADC Variation on Prediction of Prostate Cancer Aggressiveness
11


CHAPTER 12
CAD of prostate cancer using 3T MP-MRI: Effect on Observer
Performance
Thomas Hambrock; Pieter Vos; Christina Hulsbergen et al.
CHAPTER 12CHAPTER 12

Computer-aided Diagnosis of Prostate Cancer using Multiparametric 3 Tesla Magnetic Resonance Imaging: Effect on Observer Performance
Radiology (Accepted)
Hambrock T, Vos P, Hulsbergen-van de Kaa C, Barentsz J, Huisman J
Advances in knowledge: Development of a Computer Assisted Diagnosis (CAD) method using quantitative features
obtained from 3T DWI and DCE MR imaging for prostate lesions characterization, is feasible.
The stand-alone performance (AUC=0.90) of a Computer Assisted Diagnosis (CAD) method
using quantitative features obtained from 3T Diffusion Weighted and Dynamic Contrast
Enhanced MR imaging for prostate lesions characterization, is similar to prostate
experienced radiologists (AUC=0.88).
The addition of CAD significantly improved lesion discriminating performance for less-
experienced radiologists both for the peripheral zone (p<0.001) as well as the transition
zone (p=0.01).
After CAD, less-experienced radiologists (AUC=0.91) reached similar performances as
experienced radiologists (AUC=0.93).
Implications for patient care:
CAD methods that aid radiologists especially those less experienced in prostate MRI, may
expedite utilization of multi-parametric MR imaging for accurate detection and localization
of prostate cancer.
Summary Statement
The addition of CAD for evaluation of prostate cancer suspicious regions on 3T multi-parametric MRI, significantly improves the discriminating
performance for less experienced observers for both the peripheral and transition zone.
238
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

ABSTRACT
Purpose: To determine the effect of computer-aided diagnosis (CAD) on less-experienced and
experienced observer performance in differentiating benign and malignant prostate lesions on 3T
multi-parametric MRI (MP-MRI).
Materials and Methods: The institutional review board waived the need for informed consent.
Retrospectively 34 patients were included that had: prostate cancer, received an MP-MRI including
T2-weighted, diffusion weighted and dynamic contrast enhanced MRI prior to radical
prostatectomy. Six less-experienced and 4 experienced prostate radiologists were asked to
characterize different cancer suspicious regions as benign or malignant on MP-MRI, first without
and subsequently with the use of CAD software. The effect of CAD was statistically analyzed using a
multiple-reader, multi-case, receiver operating characteristic analysis and linear mixed-model
analysis.
Results: In 34 patients, 206 pre-annotated regions, including 67 malignant and 64 benign regions in
the peripheral zone (PZ) and 19 malignant and 56 benign regions in the transition zone (TZ) were
evaluated. Stand-alone CAD had an overall area-under the receiver operating characteristic curve
(AUC) of 0.90. For PZ and TZ lesions, the AUC’s were 0.92 and 0.87 respectively. Less-experienced
observers (LEO) had a 0.81 overall pre-CAD AUC which significantly increased to 0.91(p=0.001)
post-CAD. For experienced observers (EO) the pre-CAD AUC was 0.88 which increased to
0.91(p=0.17). For PZ lesions, LEOs increased their AUC from 0.86 to 0.95(p<0.001) post-CAD. EOs
showed an increase from 0.91 to 0.93(p=0.13). For TZ lesions, LEOs significantly increased their
performances from 0.72 to 0.79(p=0.01) post-CAD and EOs from 0.81 to 0.82(p=0.42).
Conclusion: The addition of CAD significantly improved the performance of less experienced
observers in distinguishing benign and malignant lesions, who when using CAD, reached similar
performance as experienced observers. The stand-alone performance of CAD was similar to
experienced observers.
239
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

INTRODUCTION
Despite high-resolution imaging, the signal intensities on anatomic T2-weighted MR images (T2-w)
show overlap between prostate cancer, post-biopsy hematoma, benign prostatic hypertrophy,
fibrosis and prostatitis. Therefore, functional imaging modalities like dynamic contrast enhanced
MR imaging (DCE-MRI), diffusion weighted MR imaging (DWI) and spectroscopic MR imaging have
been employed. Multi-parametric MR imaging both at 1.5T and 3T, has proven to be valuable in
detection, localization and characterization of prostate cancer(1-4).
High-temporal resolution DCE-MRI, allows both qualitative and quantitative estimations of
perfusion, capillary surface area and extravascular extracellular space. All these parameters are
modified by angiogenesis. Different techniques for compartment modeling, to determine arterial
input function (AIF) and gadolinium concentration, have been studied in order to improve the
objectivity and reproducibility of quantitative pharmacokinetic parameters(5;6). Reference tissue
techniques have shown promising results in generating more robust and accurate estimations of the
AIF(7;8). DWI which measures the restriction of free proton movement, has been used increasingly
in prostate MR imaging, not only for detection and localization, but also to assess the degree of
aggressiveness of the lesion(9;10). The apparent diffusion coefficient (ADC) values calculated from
the DWI, allow a more objective quantitative assessment of the tissue micro-environment.
However, despite the quantitative nature of pharmacokinetic DCE MRI and ADC values, prostate
cancer analysis on MP-MRI is still challenging, as it requires a high level of expertise and suffers
from observer variability(11). Therefore a need exists to help radiologists improve their assessment
of MP-MRI and to reduce their inter-observer variability.
Computer assisted diagnosis (CAD) techniques for the radiological assessment of various
malignancies such as for breast cancer(12), lung cancer(13;14) and colorectal cancer(15) have been
developed. CAD appears to be particularly helpful to less-experienced radiologists in improving
their ability to detect tumors(16;17). Studies that incorporated various features of MRI did show
the feasibility of CAD to discriminate benign and malignant lesions in the prostate with reported
high accuracies(18-20). However, there has been no evaluation of a CAD system in a reader study
240
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

with experienced and less experienced radiologists to determine the effect of CAD on observer
performance in for distinguishing benign from malignant prostate lesions.
The purpose of this study was to determine the effect of computer-aided diagnosis (CAD) on less-
experienced and experienced observer performance in differentiating benign and malignant
prostate lesions on 3T multi-parametric MRI (MP-MRI).
MATERIALS AND METHODS
Study population
The institutional review board waived the need for informed consent. Between Jan 2008 and
January 2009, 50 consecutive patients with biopsy proven prostate cancer who were scheduled for
radical prostatectomy, were referred from the department of urology at the Radboud University
Nijmegen Medical Centre, Nijmegen, Netherlands. All patients received a clinically routine MP-MRI
for tumor localization and staging prior to radical prostatectomy. Inclusion criteria for the study
were: a) MR imaging performed at 3 Tesla using an endorectal coil combined with pelvic phased
array coils; b) MR imaging included T2-w imaging in 3 planes, DWI and DCE-MRI; c) prostatectomy
performed in our institution and analyzed by one expert prostate pathologist. Exclusion criteria
were: previous hormonal or radiotherapy or substantial imaging artifacts related to patient
movement.
10 Patients were excluded because imaging was performed without the endorectal coil, 4 due to
severe imaging artifacts and 2 because no DCE-MRI was performed. Finally 34 patients were
included with a mean age of 64 years (range 53-74) and mean PSA of 7.5 ng/ml (range 3.4 – 21.8).
241
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

Figure 1: Flow chart diagram of patient inclusion. PZ=peripheral zone; TZ=Transition zone;
DWI=Diffusion weighted imaging; DCE=Dynamic contrast enhanced MRI; T2-w=T2 weighted
imaging.
Radical Prostatectomies
2008-2009
Endorectal 3T MR imaging
including T2-w,
DWI and DCE
n= 34 patients
Exclusion:
No combined DWI
and/or DCE
n= 2No endorectal coil
n= 10
Severe motion artifacts
n= 4
TZ lesions
n= 75
PZ tumors
n= 67
TZ benign lesions n= 56
PZ lesions
n= 131
PZ benign lesions n= 64
TZ tumors
n= 19
242
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

MR Imaging
MR imaging was performed using a 3T MR scanner (Siemens, Trio Tim, Erlangen, Germany) with the
use of an endorectal coil (Medrad, Pittsburgh) and pelvic phased array coil. The endorectal coil was
filled with a 40-mL perfluorocarbon preparation (Fomblin;Solvay-Solexis, Milan, Italy). Peristalsis
was suppressed with an intramuscular administration of 20-mg Butylscopolaminebromide
(Buscopan; Boehringer-Ingelheim, Ingelheim, Germany) and 1 mg of glucagon (Glucagen; Nordisk,
Gentofte, Denmark). The imaging sequence parameters are shown in Table 1. Gadopentetate
dimeglumine (Dotarem; Guerbet, Paris, France), of which 15 ml was administered with a power
injector (Spectris; Medrad) at 2.5mL/s and followed by a 30-mL saline flush, was used as contrast
agent.
Sequence Type
Slice thickness
Slices In-plane resolution
TR TE Averages GRAPPA b-values
T2W Axial TSE 3 mm 15-19 0.4x0.4 mm 4260 ms 99 ms 2 - -
T2W Coronal TSE 3 mm 15-19 0.5x0.5 mm 3590 ms 98 ms 2 - -
T2W Sagital TSE 3 mm 15-19 0.5x0.5 mm 4290 ms 105 ms 2 - -
DWI SE-EPI 3 mm 15-19 1.5x1.5 mm 2800 ms 81 ms 10 3 0, 50, 500, 800 mm2/s
T1-w DCE GRE FLASH 3 mm 16 1.5x1.5 mm 34 ms 1.4 ms 1 2 -
Table 1. MR imaging sequence parameters. T2-w: T2-weighted; T1-w: T1-weighted; DWI:
Diffusion weighted imaging; DCE: Dynamic contrast enhanced imaging; TSE: Turbo Spin Echo;
SE-EPI: Spin Echo Echo Planar Imaging; TR: Repetition Time; TE: Echo Time; GRAPPA:
Parallel imaging factor; GRE: Gradient echo imaging; FLASH: Fast low angle shot imaging.
243
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

Pharmacokinetic MRI
Pharmacokinetic maps were generated offline by an in-house developed system in three steps.
Firstly, kinetic DCE imaging parameters were estimated by fitting each MR signal enhancement-time
curve to a general exponential signal enhancement model as described previously(21). Secondly,
the signal enhancement-time curves were converted to tracer concentration [mmol/ml] time curves
by applying the approach of Hittmair et al.(22). Thirdly, inter-patient plasma profile variability was
removed using the reference tissue method presented by Kovar et al.(23). The reference tissue
method assumes that a tissue area within the patient is available with a known tissue model based
on literature values. For this experiment, the reference tissue was manually determined in
consensus by two radiologists, by placing a region of interest (ROI) of 5x5 mm in the normal
appearing peripheral zone which was visually characterized by a high-signal intensity on T2-w and
ADC as well as homogeneous enhancement after contrast. Estimation of pharmacokinetic
parameters was thereafter performed, conform to the theoretical derivations(24). An extensive
description of the method can be found in Vos et al.(25). The pharmacokinetic parameters estimated
are Ve, kep and Ktrans (=Ve x kep) and Washout, where Ve is an estimate of the extravascular
extracellular volume (expressed as a percentage), Ktrans is the volume transfer constant (1/minute),
Kep is the rate constant (1/minute) between the extracellular extravascular space and the plasma
space and Washout (semi-quantitative) the slope of the curve following peak enhancement
(1/minute).
Histopathological evaluation of prostatectomies
Following radical prostatectomy, prostate specimens were uniformly processed and entirely
submitted for histological investigation. Immediately after surgical resection, specimens were fixed
in 10% neutral-buffered formalin, using fine needle formalin injections and fixation overnight.
Subsequently, the entire surface was marked with ink using three different colours, after which the
entire prostate specimen was cut into serial transverse 4 mm thick slices, perpendicular to the
dorsal-rectal surface in the same plane the axial MR images were acquired. All slices were
macroscopically photographed with a CCD-camera. After histological staining all specimens were
244
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

evaluated by one expert urological pathologist (C.A.H.K, 17 years experience). Tumors were
outlined on the microscopic slides and subsequently mapped on the macroscopic photographs to
allow depiction of tumor extent and multi-focality. From prostatectomy the calculated median
tumor volume was 2.34 cc (range 0.5-32) and median Gleason score 7 (range 5-9) in the PZ while
the median tumor volume in the TZ was 2.5 cc (range 0.5-12.48) and median Gleason score was 6
(range 5-7). Fifty-six percent of patients had stage pT2 and 44% stage pT3.
Standard of Reference
Histology tumor maps were used as ground truth for cancerous regions. Annotations of MR images
were performed in consensus by two radiologists (T.H and P.V. both with 6 years experience in
prostate MRI). The morphology of the central gland, peripheral zone, cysts, calcifications, and
urethra were used as landmarks to find the corresponding MRI slices. Translation techniques as
described previously were used(26). The anatomy of the prostate is best depicted on the axial T2-w
images. These were compared with the histopathologic slices. First, based on histopathology, all
tumor regions were identified and a region of interest (ROI) placed in the peripheral and transition
zone corresponding to tumor extent on histopathology. Only tumors >0.5 cc were annotated. Only
based on imaging findings, additional benign regions were annotated when: a) focal low-signal
intensity on T2-w images and/or b) relative focal low signal on ADC maps and/or c) suspicious
irregular focal enhancing areas were evident but the underlying histopathology revealed no cancer.
Therefore, all cancerous areas and areas minimal to strongly suspicious of malignancy based on
current known features on multi-parametric imaging were annotated. To allow exact spatial
matching of the different imaging sets, a manual registration was applied for all patients, to correct
for patient related movement. In the 34 patients, 120 benign and 86 malignant lesions were
annotated and evaluated. Of the 120 benign lesions, 64 were in the PZ and 56 in the TZ. Of the 86
malignant lesions, 67 were in the PZ and 19 in the TZ. The median number of ROIs per patient was 5
(range 2 to 8).
245
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

CAD system
An in-house developed CAD system was used to assist the radiologists in the diagnosis of prostate
lesions. An extensive description of the system can be found in previous publications(27;28).
Briefly, the CAD system can visualize multi-parametric MRI and derived maps simultaneously in
multiple linked views either as background or as transparent color-coded overlays. Figure 2
demonstrates the CAD system with a dedicated prostate hanging protocol as it was used in the
experiment. The CAD system characterizes a region of interest by extracting a relevant feature set
from the available quantitative DCE and ADC maps. The extracted set of features is presented to a
trained classifier that calculates the likelihood of malignancy. Thereafter, the calculated likelihood is
presented to the radiologist to assist in their diagnosis, as shown in Figure 3. For this observer
study, two linear discriminant analysis classifiers were trained separately for the PZ and TZ. For the
two classifiers, the selection of features was carried out by Sequential Forward Floating Selection
(SFFS)(29) to establish the most discriminant features. The SFFS procedure uses leave-one-patient-
out training and testing with the area under the Receiver Operating Characteristic (ROC) curve as
the criterion to be optimized. For the PZ, the 25th percentile of ADC values, 75th percentiles of Ktrans
and Ve and 25th percentile of WashOut were selected. For the TZ, the 25th percentile of ADC values
and 25th percentile of WashOut were selected. The bootstrap resampling approach with 1000
iterations was used for estimating the bootstrap mean area-under-the (AUC) receiver operator
characteristic curve as well as the 95% confidence intervals(30).
246
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

Figure 2: Example patient case of the observer study. The MRCAD observer hanging protocol
shows on the top row from left to right a) T2-w axial b) T2-w coronal c) T2-w sagittal and d)
ADC map. On the bottom row T1-w axial images are displayed with the pharmacokinetic
maps as transparent color overlays representing e) Ktrans , f) Ve, g) WashOut and h) native T1-
w image prior to contrast. The separate window shows the scoring interactive screen tool
that the observer uses to enter a malignancy likelihood for the provided region of interest
(see figure 3 for more info).
247
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

Observer Study
The anonimized studies of all patients and the resultant ROIs were shown in identical order to 10
observers. The observers varied in their level of experience: 6 less experienced observers in multi-
parametric MR imaging of the prostate (<50 prostate MRIs evaluated) and 4 prostate experienced
observers (>100 prostate MRIs evaluated). Observers were informed that all patients had biopsy
proven prostate cancer followed by prostatectomy. The CAD system was designed to include an
experimental environment where predefined ROIs were automatically displayed for
characterization by the observers. For each ROI to be evaluated, the axial, coronal and sagital T2-w
images, the ADC map, the pre-contrast T1-w images and as color-coded transparent overlays, the
DCE parameters: Ktrans, WashOut and Ve were shown. An automated hanging protocol ensured that
all images and maps of each patient were synchronized to display each ROI. Lookup tables provided
encoding of scalar values. Window and level settings were automatically set and fixed to a
predefined intensity range: ADC (0.5 – 1.5x10-3 mm/s2) and Pharmacokinetic: Ktrans (1-3/s);
Washout (-1 – -10/s) and Ve (20 – 70%). See 2 for an example.
For every ROI shown, the observer was instructed to first provide an estimate of the likelihood of
malignancy on a scale of 0-100%. An interactive tool was displayed on top of the CAD system to
guide the observer through the successive ROIs of each patient. The tool recorded a (pre-CAD)
malignancy likelihood entered by the observer for a given ROI. Hereafter the ROI CAD likelihood
was displayed to the observer in combination with a distribution of the predicted likelihoods that
was obtained during training of the classifier in relation to their reference standard (Figure 3).
Subsequently, the observer entered an additional (post-CAD) malignancy likelihood before the next
ROI was shown. Observers were provided with the stand-alone performance of the of the CAD
system as the area-under the receiver operating characteristic curve (AUC) in the PZ and TZ
respectively. Prior to the study, all observers were trained and familiarized with the CAD system,
evaluating 4 cancer patients with a total of 25 different ROIs in the PZ and TZ with and without CAD.
248
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

Figure 3: The interactive screen tool used for scoring in this observer study. The observer is
asked to provide a malignancy likelihood for the provided region after which the observer
presses the Score button. After the observer provides the pre-CAD malignancy likelihood, the
CAD system calculates a malignancy score which is presented (dashed vertical line) in a
density plot. The green area in the density plot summarizes the smoothed distribution of all
the calculated likelihoods for all benign regions from the database used for training the
classifier. Likewise, the blue and red area corresponds with the normal and malignant
regions, respectively. Hereafter, the observer can enter a post-CAD malignancy likelihood
while taking the CAD prediction into account.
249
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

Statistical Analysis
A multiple-reader multiple-case (MRMC) ROC analysis (DBM MRMC 2.2, Kurt Rossmann
Laboratories, Chicago, U.S.A) was performed. The average AUC for less experienced observers and
experienced observers for the whole prostate as well as the PZ and TZ separately, were established
before and after CAD. As MRMC analysis cannot provide statistical significance in repeated
observational studies, additional linear mixed model analysis (using SPSS version 17) was
performed to determine the significance. P-values less than .05 were considered to indicate a
significant difference.
RESULTS
CAD Stand-Alone Performance
The overall CAD stand-alone AUC was 0.90 (CI 0.83-0.96) while for the PZ and TZ this was
respectively 0.92 (CI 0.88-0.96) and 0.87 (CI 0.78-0.96).
Observer Performance without CAD
Less-experienced observers had an overall pre-CAD AUC of 0.81 (CI 0.76-0.85); for the PZ this was
0.86 (CI 0.83-0.88) and for the TZ, 0.72 (CI 0.66-0.77). Experienced observerss had an overall AUC
of 0.88 (CI 0.85-0.93), for the PZ and TZ this was 0.91 (CI 0.89-0.93) and 0.81 (CI 0.69-0.94)
respectively.
Observer Performance with CAD
When the observers were allowed to change their ratings depending on CAD predictions, the overall
average AUC for less-experienced observers improved significantly to 0.91 (CI 0.90-0.93; p=0.001)
and for experienced observers to 0.91 (CI 0.86-0.97; p=0.17). For less-experienced observers this
was more evident for the PZ where the average AUC increased to 0.95 (CI 0.94–0.95; p<0.001)
compared to the TZ, where the average AUC improved to 0.79 (CI 0.76-0.83; p=0.01). Experienced
250
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

observers revealed no significant improvement in overall PZ (post-CAD AUC=0.93 [0.90-0.97];
p=0.13) or TZ lesion characterization (post-CAD AUC=0.82 [0.68-1.00]; p=0.42). A summary of the
pre- and post-CAD performances are shown in Table 1 and 2 as well as Figure 4.
Pre-CAD performance (AUC)
Post-CAD performance (AUC)
Significance (p-values)
Less-experienced observers
Overall
PZ
TZ
0.81 (0.76-0.85)
0.86 (0.83-0.88)
0.72 (0.66-0.77)
0.91 (0.90-0.93)
0.95 (0.94-0.95)
0.79 (0.76-0.83)
0.001 *
< 0.001*
0.01*
Experienced observers
Overall
PZ
TZ
0.88 (0.85-0.93)
0.91 (0.89-0.93)
0.81 (0.69-0.94)
0.91 (0.86-0.97)
0.93 (0.90-0.97
0.82 (0.68-1.00)
0.17
0.13
0.42
Table 2. Summary of mean pre- and post-CAD performances for readers grouped into less-
experienced and experienced readers. * denotes a statistical significance. PZ=Peripheral
zone; TZ=Transitional zone; AUC=area-under the receiver operating characteristics curve.
DISCUSSION
In our study, we have demonstrated the effectiveness of CAD in aiding radiologists in the
characterization of prostate lesions as benign or malignant using information obtained from
quantitative pharmacokinetic DCE parameters and ADC values. The performance in discriminating
lesions in the PZ and TZ significantly improved for less experienced observers when assisted by
CAD. Furthermore, when CAD was used, the performance of the less experienced observers were
comparable to that of the experienced observers CAD however, did not significantly improve the
performance of experienced observers. Furthermore it was evident that the inter-observer
251
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

variability for less experienced observers was large (CI 0.76-0.85) and that CAD not only improved
the overall performance to the level of experienced observers, but also appears to decrease inter-
observer variability (CI 0.90-0.93).
Multi-parametric MR imaging is the most accurate imaging technique available to detect, localize
and stage prostate cancer(31-35). The additional value of information obtained from DWI is also
gaining importance as a tumor aggressiveness biomarker, especially at 3T. T2-w imaging can still
be regarded as the cornerstone of prostate evaluation as anatomy is exquisitely well depicted
although low-grade tumors might not be depicted and therefore detected as easily as high-grade
tumors(36). The overall accuracy of T2-w imaging has therefore been rather low with AUC ranging
between 0.68 and 0.81(37;38). DCE-MR imaging suffers from a similar lack of specificity as
prostatitis, high-grade PIN and normal BPH can also show increased vascularization and perfusion.
For DWI, BPH and fibrosis also reveal increased proton movement restriction. Therefore, a multi-
parametric approach combining all three imaging modalities has been shown to be most
optimal(39;40). These authors showed that information obtained from the combination of the
different imaging techniques provides a better discriminating performance than each technique
individually. Yet, MP-MRI evaluation remains challenging, is largely dependent on experience and
substantial inter-observer variability in interpretation exists.
As most MR imaging modalities lack specificity, the goal of our CAD approach was to improve the
ability to differentiate benign and malignant lesions using multi-parametric information from DCE
and DWI. This was done using linear discriminant analysis to determine the likelihood that a region
represents malignancy or not. The current standard paradigm for the use of CAD systems is to use
CAD as a second reader. After the radiologist has evaluated the multiple imaging sets, CAD indicates
the likelihood that a given suspicious region is malignant, thus aiding in differentiation. The CAD
system we used has a performance of (AUC TZ: 0.87, PZ: 0.92) in discriminating benign from
malignant lesions, similar to that of an experienced radiologist (AUC TZ: 0.81, PZ: 0.91). In routine
clinical practice, many radiologists tend to evaluate MR images without quantitative analysis. For
example, on DCE-MRI, enhancement patterns that indicate the presence of tumor are compared to
the relative enhancement of the normal surrounding prostate tissue. In addition, ADC maps are
252
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

visually evaluated by looking at a focal area of relative restriction that may be indicative of tumor
although absolute values are also often used. The lack of consensus on standardized cut-off values
both for DCE and ADC limits widespread utilization and uniformity of results. The evaluation of
multi-parametric MRI requires a high level of experience and induces observer variability(41).
Figure 4: Average receiver operating characteristics (ROC) curves for the less experienced
(A. and B.) and experienced readers (C. and D.). For the peripheral zone (A. and C.) and
transition zone (C. and D.) the pre-CAD and post-CAD curves as well as the area-under the
ROC (AUC) values are provided. The dotted green lines donates the 0.5 value. The dotted
blue line represents the pre-CAD curve and the continuous black line represents the post-
CAD curve.
253
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

Histologically the normal PZ consists of more glandular components than the TZ, which due to
common BPH formation has a larger stromal component including compact muscle fibers. On MR
imaging this results in a lower T2-w signal and ADC values compared to the normal PZ where higher
values are seen. In addition, the higher vascularity of BPH nodules result in enhancement patterns
on DCE that are similar to that of cancer(42). The differences in MR appearances of TZ cancers
compared to PZ cancers have been reported before(43;44). Transition zone tumors are known to
have different genetic mutations, biological behavior and overall prognosis (being more favorable)
compared to PZ tumors(45;46). TZ tumors are also often larger in volume and are associated with
higher PSA values, yet these are often of lower grade and more likely to be confined to the prostate.
For this reason, the CAD system we used, consists of two separate classifiers for characterization of
the PZ and TZ lesions. The results of our study confirm that the TZ is indeed a more challenging
location to evaluate than the PZ, since lower stand-alone CAD performance (AUC 0.87 vs. 0.91 in the
PZ) and lower overall observer performance (AUC 0.72-0.81) were observed compared to the PZ
(AUC 0.86-0.91).
Our study has a number of limitations. First, we have used multiple ROI observations per patient,
which may hamper a straightforward interpretation of the results. A linear mixed model analysis
which incorporates findings from multiple observations in the same patient was used to determine
significance. Secondly, the number of TZ tumors was fairly low compared to PZ tumors. This is
consistent with the known overall lower prevalence (30%) of these tumors identified clinically(47).
Therefore, the overall performance of both the CAD system as well as that of the readers may rather
constitute a PZ dominated result. Thirdly, as an integral part of DCE MRI quantification, the
reference tissue calibration method requires an annotation of normal PZ. For this study, this was
done manually prior to the experiment. Ideally, such annotation should be performed automatically
without requiring any user interaction. Previous studies have shown that despite the fact that
automatic calibration performs better compared to a general estimate, manual calibration is still
superior at this stage(7). Fourthly, all regions scored by the observer were annotated and
predefined beforehand. Although this is substantial drawback, primarily evaluating the potential of
a CAD system for prostate cancer evaluation on MRI requires limitating the observer variability
254
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

caused by self annotating. Subsequent studies should first identify the improvement when readers
identify potential suspicious regions themselves and then obtain the CAD support for that region. If
this proves to be useful as well, CAD systems should ideally calculate tumor probability maps, but
this requires further prostate segmentation algorithms which are part of ongoing developments.
Exact geometrical alignment of histopathology and MR imaging is considered very difficult but a
number of strategies have been implemented incl. using percentiles (25/75) to capture hot-spot
features within ROI’s. A final limitation relates to the fact that hydrogen spectroscopic MR imaging
was not included in our CAD system but future systems should be developed using these additional
features as well.
CONCLUSIONS
In conclusion, we have shown that the addition of CAD on multi-parametric 3T MP-MRI, significantly
improves the discriminating performance for less experienced observes for both the PZ and TZ.
Furthermore less experienced observers assisted by CAD, reached similar performance compared to
experienced observers. Therefore, CAD appears to be a promising method for implementation into
routine clinical environment for the MR imaging assessment of suspected prostate cancer.
255
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

APPENDIX
Pre-CAD performance
(AUC)
Post-CAD performance
(AUC) Less-experienced observers
PZ - Reader 1 - Reader 2 - Reader 3 - Reader 4 - Reader 5 - Reader 6
TZ - Reader 1 - Reader 2 - Reader 3 - Reader 4 - Reader 5 - Reader 6
0.83 0.84 0.84 0.87 0.88 0.87
0.73 0.72 0.65 0.65 0.80 0.74
0.95 0.95 0.93 0.95 0.95 0.94
0.81 0.77 0.80 0.77 0.85 0.76
Experienced observers
PZ - Reader 7 - Reader 8 - Reader 9 - Reader 10
TZ - Reader 7 - Reader 8 - Reader 9 - Reader 10
0.92 0.89 0.91 0.91
0.89 0.87 0.80 0.71
0.95 0.94 0.96 0.91
0.92 0.88 0.88 0.69
Table 3. Summary of the individual performances pre- and post-CAD for all readers.
256
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

REFERENCES
1. Haider MA, van der Kwast TH, Tanguay J, Evans AJ, Hashmi AT, Lockwood G, Trachtenberg J. Combined T2-weighted and diffusion-weighted MRI for localization of prostate cancer. AJR Am.J.Roentgenol. 2007 Aug;189(2):323-8.
2. Kitajima K, Kaji Y, Fukabori Y, Yoshida K, Suganuma N, Sugimura K. Prostate cancer detection with 3 T MRI: comparison of diffusion-weighted imaging and dynamic contrast-enhanced MRI in combination with T2-weighted imaging. J.Magn Reson.Imaging 2010 Mar;31(3):625-31.
3. Puech P, Potiron E, Lemaitre L, Leroy X, Haber GP, Crouzet S, Kamoi K, Villers A. Dynamic contrast-enhanced-magnetic resonance imaging evaluation of intraprostatic prostate cancer: correlation with radical prostatectomy specimens. Urology 2009 Nov;74(5):1094-9.
4. Tanimoto A, Nakashima J, Kohno H, Shinmoto H, Kuribayashi S. Prostate cancer screening: the clinical value of diffusion-weighted imaging and dynamic MR imaging in combination with T2-weighted imaging. J.Magn Reson.Imaging 2007 Jan;25(1):146-52.
5. Hittmair K, Gomiscek G, Langenberger K, Recht M, Imhof H, Kramer J. Method for the quantitative assessment of contrast agent uptake in dynamic contrast-enhanced MRI. Magn Reson.Med. 1994 May;31(5):567-71.
6. Tofts PS. Modeling tracer kinetics in dynamic Gd-DTPA MR imaging. J.Magn Reson.Imaging 1997 Jan;7(1):91-101.
7. Vos P, Hambrock T, Futterer J, Hulsbergen-van de Kaa CA, Barentsz J.O., Huisman HJ. Effect of calibration on computerized analysis of prostate lesions using quantitative dynamic contrast-enhanced magnetic resonance imaging. In: Maryellen L.Giger NK, editor. 2007.
8. Kovar DA, Lewis M, Karczmar GS. A new method for imaging perfusion and contrast extraction fraction: input functions derived from reference tissues. J.Magn Reson.Imaging 1998 Sep;8(5):1126-34.
9. Vargas HA, Akin O, Franiel T, Mazaheri Y, Zheng J, Moskowitz C, Udo K, Eastham J, Hricak H. Diffusion-weighted Endorectal MR Imaging at 3 T for Prostate Cancer: Tumor Detection and Assessment of Aggressiveness. Radiology 2011 Jun;259(3):775-84.
10. Verma S, Rajesh A, Morales H, Lemen L, Bills G, Delworth M, Gaitonde K, Ying J, Samartunga R, Lamba M. Assessment of aggressiveness of prostate cancer: correlation of apparent diffusion coefficient with histologic grade after radical prostatectomy. AJR Am.J.Roentgenol. 2011 Feb;196(2):374-81.
11. Lim HK, Kim JK, Kim KA, Cho KS. Prostate cancer: apparent diffusion coefficient map with T2-weighted images for detection--a multireader study. Radiology 2009 Jan;250(1):145-51.
12. Karssemeijer N, Otten JD, Verbeek AL, Groenewoud JH, de Koning HJ, Hendriks JH, Holland R. Computer-aided detection versus independent double reading of masses on mammograms. Radiology 2003 Apr;227(1):192-200.
13. Ge Z, Sahiner B, Chan HP, Hadjiiski LM, Cascade PN, Bogot N, Kazerooni EA, Wei J, Zhou C. Computer-aided detection of lung nodules: false positive reduction using a 3D gradient field method and 3D ellipsoid fitting. Med.Phys. 2005 Aug;32(8):2443-54.
14. de HB, De Boo DW, Gietema HA, van HF, Mearadji B, Schijf L, van GB, Prokop M, Schaefer-Prokop C. Computer-aided detection of lung cancer on chest radiographs: effect on observer performance. Radiology 2010 Nov;257(2):532-40.
15. Graser A, Kolligs FT, Mang T, Schaefer C, Geisbusch S, Reiser MF, Becker CR. Computer-aided detection in CT colonography: initial clinical experience using a prototype system. Eur.Radiol. 2007 Oct;17(10):2608-15.
16. Baker ME, Bogoni L, Obuchowski NA, Dass C, Kendzierski RM, Remer EM, Einstein DM, Cathier P, Jerebko A, Lakare S, et al. Computer-aided detection of colorectal polyps: can it improve sensitivity of less-experienced readers? Preliminary findings. Radiology 2007 Oct;245(1):140-9.
257
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

17. Szucs-Farkas Z, Patak MA, Yuksel-Hatz S, Ruder T, Vock P. Improved detection of pulmonary nodules on energy-subtracted chest radiographs with a commercial computer-aided diagnosis software: comparison with human observers. Eur.Radiol. 2010 Jun;20(6):1289-96.
18. Chan I, Wells W, III, Mulkern RV, Haker S, Zhang J, Zou KH, Maier SE, Tempany CM. Detection of prostate cancer by integration of line-scan diffusion, T2-mapping and T2-weighted magnetic resonance imaging; a multichannel statistical classifier. Med.Phys. 2003 Sep;30(9):2390-8.
19. Langer DL, van der Kwast TH, Evans AJ, Trachtenberg J, Wilson BC, Haider MA. Prostate cancer detection with multi-parametric MRI: logistic regression analysis of quantitative T2, diffusion-weighted imaging, and dynamic contrast-enhanced MRI. J.Magn Reson.Imaging 2009 Aug;30(2):327-34.
20. Vos P, Hambrock T, Futterer JJ, Hulsbergen-Van de Kaa CA, Barentsz JO, Huisman HJ. Computerized analysis of prostate lesions using quantitative dynamic contrast enhanced magnetic-resonance imaging. 2007. Ref Type: Generic
21. Huisman HJ, Engelbrecht MR, Barentsz JO. Accurate estimation of pharmacokinetic contrast-enhanced dynamic MRI parameters of the prostate. J.Magn Reson.Imaging 2001 Apr;13(4):607-14.
22. Hittmair K, Gomiscek G, Langenberger K, Recht M, Imhof H, Kramer J. Method for the quantitative assessment of contrast agent uptake in dynamic contrast-enhanced MRI. Magn Reson.Med. 1994 May;31(5):567-71.
23. Kovar DA, Lewis M, Karczmar GS. A new method for imaging perfusion and contrast extraction fraction: input functions derived from reference tissues. J.Magn Reson.Imaging 1998 Sep;8(5):1126-34.
24. Tofts PS, Brix G, Buckley DL, Evelhoch JL, Henderson E, Knopp MV, Larsson HB, Lee TY, Mayr NA, Parker GJ, et al. Estimating kinetic parameters from dynamic contrast-enhanced T(1)-weighted MRI of a diffusable tracer: standardized quantities and symbols. J.Magn Reson.Imaging 1999 Sep;10(3):223-32.
25. Vos PC, Hambrock T, Hulsbergen-Van de Kaa CA, Futterer JJ, Barentsz JO, Huisman HJ. Computerized analysis of prostate lesions in the peripheral zone using dynamic contrast enhanced MRI. Med.Phys. 2008 Mar;35(3):888-99.
26. Hambrock T, Somford DM, Huisman HJ, van O, I, Witjes JA, Hulsbergen-Van de Kaa CA, Scheenen T, Barentsz JO. Relationship between apparent diffusion coefficients at 3.0-T MR imaging and gleason grade in peripheral zone prostate cancer. Radiology 2011 May;259(2):453-61.
27. Vos PC, Hambrock T, Hulsbergen-Van de Kaa CA, Futterer JJ, Barentsz JO, Huisman HJ. Computerized analysis of prostate lesions in the peripheral zone using dynamic contrast enhanced MRI. Med.Phys. 2008 Mar;35(3):888-99.
28. Vos PC, Hambrock T, Barenstz JO, Huisman HJ. Computer-assisted analysis of peripheral zone prostate lesions using T2-weighted and dynamic contrast enhanced T1-weighted MRI. Phys.Med.Biol. 2010 Mar 21;55(6):1719-34.
29. Pattern Recognition Letters. Vol. 15, 1994.
30. Obuchowski NA. Determining sample size for ROC studies: what is reasonable for the expected difference in tests' ROC areas? Acad.Radiol. 2003 Nov;10(11):1327-8.
31. Futterer JJ, Heijmink SW, Scheenen TW, Veltman J, Huisman HJ, Vos P, Hulsbergen-Van de Kaa CA, Witjes JA, Krabbe PF, Heerschap A, et al. Prostate cancer localization with dynamic contrast-enhanced MR imaging and proton MR spectroscopic imaging. Radiology 2006 Nov;241(2):449-58.
32. Futterer JJ, Heijmink SW, Scheenen TW, Jager GJ, Hulsbergen-Van de Kaa CA, Witjes JA, Barentsz JO. Prostate cancer: local staging at 3-T endorectal MR imaging--early experience. Radiology 2006 Jan;238(1):184-91.
33. Haider MA, van der Kwast TH, Tanguay J, Evans AJ, Hashmi AT, Lockwood G, Trachtenberg J. Combined T2-weighted and diffusion-weighted MRI for localization of prostate cancer. AJR Am.J.Roentgenol. 2007 Aug;189(2):323-8.
258
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12

34. Hambrock T, Somford DM, Hoeks C, Bouwense SA, Huisman H, Yakar D, van O, I, Witjes JA, Futterer JJ, Barentsz JO. Magnetic resonance imaging guided prostate biopsy in men with repeat negative biopsies and increased prostate specific antigen. J.Urol. 2010 Feb;183(2):520-7.
35. Tanimoto A, Nakashima J, Kohno H, Shinmoto H, Kuribayashi S. Prostate cancer screening: the clinical value of diffusion-weighted imaging and dynamic MR imaging in combination with T2-weighted imaging. J.Magn Reson.Imaging 2007 Jan;25(1):146-52.
36. Wang L, Mazaheri Y, Zhang J, Ishill NM, Kuroiwa K, Hricak H. Assessment of biologic aggressiveness of prostate cancer: correlation of MR signal intensity with Gleason grade after radical prostatectomy. Radiology 2008 Jan;246(1):168-76.
37. Delongchamps NB, Rouanne M, Flam T, Beuvon F, Liberatore M, Zerbib M, Cornud F. Multiparametric magnetic resonance imaging for the detection and localization of prostate cancer: combination of T2-weighted, dynamic contrast-enhanced and diffusion-weighted imaging. BJU.Int. 2010 Nov 2.
38. Heijmink SW, Futterer JJ, Hambrock T, Takahashi S, Scheenen TW, Huisman HJ, Hulsbergen-Van de Kaa CA, Knipscheer BC, Kiemeney LA, Witjes JA, et al. Prostate cancer: body-array versus endorectal coil MR imaging at 3 T--comparison of image quality, localization, and staging performance. Radiology 2007 Jul;244(1):184-95.
39. Tanimoto A, Nakashima J, Kohno H, Shinmoto H, Kuribayashi S. Prostate cancer screening: the clinical value of diffusion-weighted imaging and dynamic MR imaging in combination with T2-weighted imaging. J.Magn Reson.Imaging 2007 Jan;25(1):146-52.
40. Turkbey B, Pinto PA, Mani H, Bernardo M, Pang Y, McKinney YL, Khurana K, Ravizzini GC, Albert PS, Merino MJ, et al. Prostate cancer: value of multiparametric MR imaging at 3 T for detection--histopathologic correlation. Radiology 2010 Apr;255(1):89-99.
41. Lim HK, Kim JK, Kim KA, Cho KS. Prostate cancer: apparent diffusion coefficient map with T2-weighted images for detection--a multireader study. Radiology 2009 Jan;250(1):145-51.
42. Engelbrecht MR, Huisman HJ, Laheij RJ, Jager GJ, van Leenders GJ, Hulsbergen-Van de Kaa CA, de la Rosette JJ, Blickman JG, Barentsz JO. Discrimination of prostate cancer from normal peripheral zone and central gland tissue by using dynamic contrast-enhanced MR imaging. Radiology 2003 Oct;229(1):248-54.
43. Akin O, Sala E, Moskowitz CS, Kuroiwa K, Ishill NM, Pucar D, Scardino PT, Hricak H. Transition zone prostate cancers: features, detection, localization, and staging at endorectal MR imaging. Radiology 2006 Jun;239(3):784-92.
44. Kayhan A, Fan X, Oommen J, Oto A. Multi-parametric MR imaging of transition zone prostate cancer: Imaging features, detection and staging. World J.Radiol. 2010 May 28;2(5):180-7.
45. Guo CC, Zuo G, Cao D, Troncoso P, Czerniak BA. Prostate cancer of transition zone origin lacks TMPRSS2-ERG gene fusion. Mod.Pathol. 2009 Apr 24.
46. Noguchi M, Stamey TA, Neal JE, Yemoto CE. An analysis of 148 consecutive transition zone cancers: clinical and histological characteristics. J.Urol. 2000 Jun;163(6):1751-5.
47. McNeal JE, Redwine EA, Freiha FS, Stamey TA. Zonal distribution of prostatic adenocarcinoma. Correlation with histologic pattern and direction of spread. Am.J.Surg.Pathol. 1988 Dec;12(12):897-906.
259
Computer Aided Diagnosis of Prostate Cancer using 3T Multiparametric MRI: Effect on Observer Performance
12


PART FIVE
DISCUSSION, CONCLUSIONS AND
FUTURE PERSPECTIVES


Discussion, Conclusions and Future Perspectives
T. Hambrock
CHAPTER 13CHAPTER 13

DISCUSSION
March 2014, Netherlands:
[UROLOGIST] : “Mr. v. S, your PSA levels have been rising over the last 2 years from 2 ng/ml to
7 ng/ml. The wisest next step is to perform an MRI to exclude significant
prostate cancer.
[PATIENT MR. v.S]: “My brother received 12 biopsies of his prostate 3 years ago. Is this still
necessary?”
[UROLOGIST]: “No, if the MRI reveals no significant prostate cancer we can safely observe you
with confidence. When the MRI detects suspicious lesions, targeted biopsies
with a maximum of 4 biopsies will be performed. The MRI with targeted
biopsies would not only provide us with the information, whether you have
cancer or not, but also give an indication of the aggressiveness of the cancer and
assess as to whether there has been spread of tumour outside the prostate or
not”
[PATIENT MR. v.S]: “Amazing, all that information with an MRI”
[UROLOGIST]: “Yes! We will be able to have a much clearer picture of what treatment will be
most required in your particular case.”
The author of this thesis predicts that this hypothetical conversation taking place in the year
2014 (that is if the Maya’s weren’t correct about the end of the world occurring on 21st Dec
2012) could be a reality. However, this will imply that a PARADIGM SHIFT has occurred.
For a PARADIGM SHIFT to occur, many stones need be dislodged. The author is undoubtedly
aware of the fact that the anticipated paradigm shift is a very daunting and verly “bold”. He also
fully acknowledges that this statement will be criticized by many physicians and that the Battle
of Anhiari will still rage in its fiercest moment and much blood, sweat, tears and heated
arguments will still occur. But the end of the Battle of Anhiari is unlikely to occur in the
262
Discussion, Conclusions and Future Perspectives 13

lifetime. It will only change to a more structured organized and precisely orientated battle with
only the true enemy destroyed while collateral damage to the civilians minimized.
From the philosophical conclusion drawn from the current thesis, we can move to a more
scientific discussion of its merits and weaknesses: In the introduction a number of clinical
problems were stated, both faced by clinicians directly dealing with patients and some faced by
radiologists evaluating MR images.
Problems faced by Clinicians:
Clinical Problem 1 : Patients with an elevated/elevating PSA value but the TRUS biopsies remain
negative, are a considerable concern. Does the patient have cancer or not? Should further TRUS
biopsies be performed or not?
Clinical Problem 2 : If MRI is accurate in identifying a tumour location, what effective method is
available to reliably obtain histological proof of this location?
Background
Currently prostate cancer detection is performed by using tools with limited accuracies
(PSA, DRE and TRUS biopsies). Because the specificity of PSA measurement is low, it is often
the case that many unnecessary repeat systematic random biopsies are performed.
Additionally, because an inherent sampling error occurs with systematic biopsies, tumours
which are present can be missed.
Multiparametric MR imaging techniques including anatomical T2-weighted imaging and
functional techniques such as DCE, DWI and MR spectroscopic imaging have been shown in
combination, to have considerable value in prostate cancer detection. Because these MR
techniques have a relatively high specificity in comparison with PSA measurement, they
could prevent unnecessary systematic random biopsies. These techniques in combination
also have a high sensitivity. In a recent evaluation of multiparametric MR imaging at 3T, the
addition of dynamic contrast-enhanced and/or DWI to T2-weighted MR imaging
significantly improved prostate cancer detection sensitivity from 63% to 80% in the
peripheral zone, while maintaining a stable specificity. Multiparametric MR imaging
techniques may also contribute in detection of transition zone prostate cancers (chapter 6).
263
Discussion, Conclusions and Future Perspectives 13

The combined use of DWI, DCE and T2-weighted MR imaging leads to an increased accuracy
in detection of transition zone cancer especially for high grade tumours with a 91%
detection rate vs. 47% for low-grade tumours.
Solution to clinical problem 1 and 2 : Multiparametric MR imaging at 3T incl. T2-weighted
imaging, DWI and DCE-MRI is an accurate technique for the detection of significant tumour in
these patients. Furthermore, the use of an MR guided biopsy device, to perform targeted biopsies
towards tumour suspicious regions, is a useful and accurate technique to make a definite diagnosis.
A considerable number of patients with persistent abnormal PSA values harbor tumour and should
therefore receive further evaluation with MRI.
Discussion
In Chapter 3 of this thesis, the author tested the technique and feasibility of translating
tumor suspicious region maps of the prostate, obtained by multiparametric, anatomical and
functional 3T MRI data, to imaging at a separate MR imaging session for directing MR
guided biopsies. Furthermore, the practicability of MR guided biopsy on a 3T MR scanner
using a 32-channel coil and an MR compatible biopsy device was determined. It was shown
that a basic translation technique can be developed to transfer information from the initial
detection MRI to a subsequent MR biopsy session. It was also shown that the procedure
was feasible to perform in a clinically acceptable time frame. The initial patient cohort
consisted of patients in whom at least two prior negative TRUS biopsies had been
performed, but PSA was still elevated. Using the above developed translation and biopsy
technique a 38% cancer detection yield was determined.
264
Discussion, Conclusions and Future Perspectives 13

.
.
Figure 1. Principal aspects of Chapter 3: Top two images – schematic presentation of the
procedure. Bottom three: Detection – Translation – MR biopsy.
In Chapter 4, the developed technique of MR guided biopsies was performed in a large
clinical cohort of patients with persistently elevated PSA and at least two prior negative
TRUS biopsy sessions. The purpose of this study was to determine the maximum tumour
detection rate using 3T multiparametric MRI and MR-GB in a cohort mentioned above. A
low threshold for evaluating the images was applied with any regions vaguely to strongly
suspicious for cancer eventually biopsied. In a consecutive group of 68 men we were able to
diagnose cancer in 59% of the patients. Furthermore we determined that these tumours
265
Discussion, Conclusions and Future Perspectives 13

were deemed clinically significant in 93% of the cases. Additionally, we established that
tumours missed with serial TRUS biopsies are located in regions not explicitly sampled by
TRUS biopsy schemes. The results were compared to the tumour detection rates at the 2nd
and 3rd TRUS biopsy in a separate cohort. MR guided biopsies significantly outperformed
conventional TRUS biopsy detection rates for different PSA, prostate volume and PSA
density subgroups. MRI should therefore be part of any workup protocol of patients who
are suspected of harboring malignancy but who have successive negative biopsies. Because
of the low numbers of cores needed, MR guided biopsies are an appealing alternative to
procedure such as saturation biopsies.
266
Discussion, Conclusions and Future Perspectives 13

Figure 2. Principal findings of Chapter 4: Tumor detection rates of MR-guided biopsies vs. 2nd
and 3rd TRUS biopsy session sub grouped according to PSA (top left) and PSA density (top right).
Location map of tumour identified with MR-GB.
Clinical problem 3 : After radiation therapy for PCa, diagnosing local recurrence vs. metastatic
disease when the PSA starts rising again, is challenging.
Background
External beam radiotherapy is performed as first line treatment in around 30% of patients
with prostate cancer. As the prostate is not destroyed completely, viable normal prostate
tissue remains which can continue producing PSA. The utilization of PSA to detect
recurrence of radiation therapy is therefore hampered. Based on the current knowledge,
biochemical failure is defined in these patients when three consecutive rises in PSA occur
after reaching a nadir. Furthermore the PSA value should be > 2 ng/ml. This however is
hampered by the fact that biochemical failure does not define if tumour production of PSA is
due to local recurrence or metastases to lymph nodes or the skeleton. The implication of
accurately determining the location of tumour in this scenario is that salvage therapy (cryo-,
laser-, HIFU-therapy or salvage radical prostatectomy can be offered for patients with local
recurrence only.
Due to radiation effects, the normal prostate undergoes shrinkage, fibrosis and normal
glandular function ceases, all factors which make imaging using conventional MR imaging
problematic. On T2-weighted images, the whole prostate exhibits low signal intensity.
Similarly on ADC maps, a high diffusion restriction occurs in normal tissue (due to loss of
glandular luminal spaces and fibrosis) and on spectroscopic imaging, the normal citrate
production is significantly reduced. Initial reports indicated that DCE-MRI and MRSI may
have a potential to detect local recurrence.
Solution to clinical problem 3: 3T DCE MRI followed by MR guided biopsies is a feasible and very
useful technique for diagnosing local recurrence of prostate cancer following external beam
radiotherapy.
267
Discussion, Conclusions and Future Perspectives 13

Discussion
In Chapter 5 MR imaging at 3T with DCE-MRI was performed in a group of 24 patients with
a PSA biochemical failure following external beam radiotherapy. Initial MRI or bone
scintigraphy detected metastatic disease in 4 patients. In the remaining patients DCE-MRI
was performed and in all patients focal abnormalities on DCE-MRI were identified. All these
focal regions were subsequently biopsied using MR-guided biopsies. The conclusion drawn
from this chapter was that a definite diagnosis of local recurrence was made in 75%
(15/20) of these patients. Only 3 biopsy cores were taken and the median MR biopsy time
was 30 min. Overall, the positive predictive value of focal DCE-MRI abnormalities in the
post-radiated prostate was 68% with the vast majority of the remaining non-malignant
enhancing regions representing radiation induced reactive atypia in preexisting glandular
tissue (with or without some inflammation). Furthermore, the strict criteria of biochemical
recurrence especially the absolute PSA value did not appear to hold true in all cases. Large
volume Gleason 5+5=10 cancer was detected in a patient with a single PSA rise from 0 to 0.4
ng/ml. Thus in patients with elevated PSA following external radiotherapy, DCE MRI can
play an important role in diagnosing local recurrence and therefore guide therapy for
systemic vs. local therapy.
Figure 3. Principal findings of Chapter 5: Tumor detection with MR-guided biopsy of abnormal
region on DCE-MRI (but normal on T2-weighted imaging) in a patient with biochemical
recurrence.
268
Discussion, Conclusions and Future Perspectives 13

Clinical problem 4 : Pretreatment identification of prostate cancer aggressiveness is crucial for
management and prognostication. The current methods to determine this are inaccurate. What in
vivo methods are available to reliably predict the nature of the PCa?
Background
The histologically determined Gleason score of prostate cancer is probably the most
important determinant of its biological activity and aggressiveness. A vast body of
literature has established Gleason score as one of the most important markers in predicting
disease outcome in prostate cancer. In fact, this grading scheme has now become so
important that it is often used as an integral piece of information in both management and
treatment stratification of patients with prostate cancer before and after definitive therapy.
Pre-treatment knowledge of true Gleason score would be an important advance, but
currently, such information remains elusive. This is explained by the fact that biopsy
determination of Gleason score often undergrades and therefore gives a poor reflection of
true Gleason score, determined at prostatectomy. Partin tables and risk stratification
schemes that incorporate information from biopsy Gleason scores into decision making are
therefore rendered less accurate and less reliable. Therefore, a definite need for a more
accurate and non-invasive methods exists to improve the accuracy of determination of true
pretreatment Gleason score.
Diffusion Weighted MR imaging measures the diffusivity of water molecules in tissue and
quantifies this random Brownian motion property of water molecules (diffusion) in tissue.
The degree of restriction to water diffusion in biologic tissue is inversely correlated to
tissue cellularity and the integrity of cell membranes. The principal microscopic differences
that are evident for low Gleason grade tumours compared to higher grades, is that the size
of the ductal lumina decrease (the diffusion space reduces) and the cellular density is
markedly increased as the Gleason score increase.
Proton magnetic resonance spectroscopic imaging provides spatial mapping of the tissue
levels of the metabolites citrate, choline and creatine in the whole prostate gland. Prostate
cancer tissue is characterized by lower citrate levels and/or higher choline levels compared
to normal tissue resulting in the ratio of choline and creatine to citrate (Cho+Cr/Cit) as a
269
Discussion, Conclusions and Future Perspectives 13

marker for prostate cancer. The choline/creatine (Cho/Cr) ratio is also of note since choline
increases in malignant tissue due to altered phospholipid metabolism. Furthermore
increased choline to creatine ratios have been identified in high-resolution ex vivo Magic-
Angle-Spinning NMR of prostate biopsies which showed a significant correlation of the
Gleason score to the Cho/Cr ratio, among other ratios.
Solution to clinical problem 4 : ADC values determined from DWI MR imaging and spectroscopic
imaging at 3T both represent useful biomarkers for prostate cancer aggressiveness.
Discussion
In Chapter 7 the author evaluated the hypothesis that the increase in cellular density
associated with increasing tumour Gleason grades should be reflected by an increasing
water movement restriction and therefore decreasing ADC values. In 51 patients who
received 3T DWI MRI prior to radical prostatectomy a separate step-section by ADC slice
analysis of all peripheral zone tumour were made. For each slice on pathology and
corresponding ADC slice, a meticulous analysis of the proportion of Gleason grade
compositions and the matching ADC values were determined. The results from this analysis
showed that the ADC values of prostate cancer in the peripheral zone inversely relate to
prostate cancer Gleason grades, with low-, intermediate- and high-grade tumors showing
significant differences in ADC values. Furthermore using the median ADC values of the most
aggressive tumor regions a high discriminatory accuracy is achieved for discerning low-
grade (Gleason grade 2/3) from combined intermediate- and high-grade cancers (Gleason
grade 4/5) with an AUC of 0.90. Non-invasive prediction of peripheral zone Gleason grades
may improve patient management by more accurate risk-stratification.
As tumours originating in the transition zone are known to have different behavioral
characteristics, different genetic mutations and originate in a different background of
“normal” tissue, these were excluded from the primary analysis. However ADC values of
transition zone tumours were analyzed (but not presented in this thesis) and no correlation
between ADC values and Gleason grades observed. For still incompletely understood
reasons (probably a decrease in stroma), low grade transition zone tumors especial Gleason
270
Discussion, Conclusions and Future Perspectives 13

2+3=5 tumours often show significant restriction on ADC making a discrimination with
more aggressive tumours using this technique unsuitable.
Figure 4. Principal findings of Chapter 7: The relationship between tumor Gleason grades and
ADC values from 3T DWI in the peripheral zone.
In Chapter 9 a further potentially MR biomarker was evaluated to obtain insight as to its
usefulness for the assessment of aggression. The study was performed to validate the
performance of MR spectroscopic imaging of the prostate at 3T to assess tumour
aggressiveness, based on the choline plus creatine to citrate ratio (Cho+Cr/Cit) and choline
to creatine rato (Cho/Cr), using the Gleason score of the radical prostatectomy (RP)
specimen as the gold standard. We assessed the tumour aggressiveness differentiation by
the AUC of the ROC curves and this gave similar results when using either the Cho+Cr/Cit
(0.70) or the Cho/Cr (0.74) ratio. The performance of combining both ratios was better
(0.78). A significant correlation was found between the maximum Cho+Cr/Cit ratio and the
aggressiveness classes. The comparison of the medians of the three aggressiveness classes
revealed a significant difference between the low and high grade tumours. The maximum
Cho/Cr ratio also correlated significantly with the aggressiveness classes and the median
Cho/Cr of the low grade tumours was significantly different from the high grade tumours. A
Cho/Cr adaptation level of 2.3 for the standardized threshold approach gave the highest
AUCs when discriminating high- from low- and intermediate-grade tumours (AUC=0.73)
and low- from the combined high- and intermediate-grade tumours (AUC=0.78).
271
Discussion, Conclusions and Future Perspectives 13

MR spectroscopic imaging for the evaluation of aggressiveness reflects different aspects of
tumour biology to DWI. However, some features of a tumour which make them amenable
for DWI evaluation, also reflect changes observed in the spectroscopic analysis. The
principal metabolites in spectroscopic imaging of the prostate are choline, creatine and
citrate. The later is part of the normal excretory production of prostate epithelial cells and
is mainly present in the intraluminal space of the ducts and serves as energy supply for the
sperm. The relative ductal size in normal prostate tissue is large, being reflected by a high
citrate signal on MR. Reduction of the citrate levels in tumour relates to two changes that
occur. The less differentiated the malignant epithelial cells become, the less of the normal
exocrinic function remains and the production of citrate decreases or is used for de novo
lipid synthesis for tumour growth Furthermore, as discussed previously, the size of the
luminal spaces decrease as the tumour progresses from Gleason grade 3 to 5. Therefore the
primary compartment where citrate is located also decreases independent of the reduction
in the production thereof. The other two metabolites, choline and creatine are
intracellularly located in the epithelial cells. The increased signal from choline in malignant
tissue reflects the turnover of cell membrane synthesis. Cellular density increases with
increasing Gleason grade. Therefore the same effects that make ADC a useful marker of
cellularity and Gleason grade estimation, also partially explain the changes observed in
spectroscopic imaging.
A standardized threshold approach was developed to make the evaluation of spectroscopic
data in a clinical setting more robust and improve the inter-reader agreement of the
evaluation. This approach also appeared to offer an equally good assessment of
aggressiveness compared to a more quantitative evaluation of the absolute ratios of
different metabolites. For the above mentioned study, spectroscopic data was pooled both
for transition zone and peripheral zone tumours because of the relative small sample size
especially for transition zone. Therefore, a potential value for the transition zone (TZ) vs.
peripheral zone (PZ) tumours in aggressiveness assessment could not be assessed.
In a subsequent study (not included in this thesis) which has recently been accepted for
publication in Radiology, the value of combined DWI and MRS for TZ vs. PZ aggressiveness
assessment was evaluated. The principal conclusion drawn from that study was that the
combination of both techniques did not improve overall aggressiveness prediction.
272
Discussion, Conclusions and Future Perspectives 13

However, it did determine that DWI was the best modality for PZ tumours grade assessment
while MRS, the most suited for the TZ. Quantitative DCE-MRI and quantitative T2 would
constitute further interesting research topics on their value in assessment of prostate
cancer aggressiveness.
Figure 5. Principal findings of Chapter 9: Metabolic rations and malignancy rating score using
MRS for differentiation of aggressiveness groups of prostate cancer (combined PZ and TZ).
Clinical problem 5 : When a patient is diagnosed with PCa Gleason Score 3+3=6 on biopsy, is
there a method available to reliably aid in differentiating those patients where biopsies represent
an undergrading (and therefore need more radical therapy) from those where it is a correct
prediction (and therefore may be managed more conservatively)?
Background
Radical prostatectomy and external beam radiotherapy have been the primary treatment
methods for many patients diagnosed with prostate cancer for a considerable time. With
the increasing awareness that many tumours do not progress or cause disease related
morbidity and mortality, a more conservative approach which includes active surveillance
has been advocated for these tumours. Yet, the current methods to reliable determine
which patients need radical therapy from those where a conservative approach is desirable
remains elusive. As mentioned in a previous discussion, the Gleason grade and therefore
Gleason Score remains one of the most crucial components for this assessment. In the
current
being less than 0.5 cc in volume are classified as being indolent. It however needs to be
273
Discussion, Conclusions and Future Perspectives 13

emphasized that future dedifferentiation into a more malignant phenotype cannot be
assessed as yet. The grey area of larger > 0.5 cc, Gleason Score
more uncertain und no clear consensus on the management of these tumours exist.
of a
biopsy core with tumour < 33% and PSA levels < 10 ng/ml are currently used to predict
patients that harbor indolent tumour. As PSA levels are related to prostate volume, a
correction has also been implemented whereby a PSA density of < 0.2 ng/ml/cc is also
included in the above mentioned criteria. The principal shortcoming of the above
mentioned strategy is that tumours are often missed and located in regions, sampled
inadequately with systematic biopsy (as described in Chapter 4). It is also known from
literature that undergrading of biopsy schemes is substantial (up to 40%). Therefore any
information obtained from biopsy cores may result in non-optimal management of the
patient. Especially patients who harbor aggressive tumours (but have false low Gleason
score 3+3=6 on biopsy) need additional assessment for the presence of extracapsular
extension or metastatic disease. It is therefore of paramount importance to determine if
biopsy findings reflect the true state prior to any further treatment.
Solution to problem 5: 3T DWI MR imaging is a very valuable technique for accurately
identifying patients in whom biopsies represent an underestimation of prostate cancer
aggressiveness.
Discussion
In Chapter 8, the initial experience of patients with a biopsy Gleason Score
evaluated. To test the hypothesis from previous knowledge that DWI is useful biomarker
for prostate cancer aggressiveness and that it may be of value in indentifying patients with
undergrading, MRI was performed prior to radical prostatectomy. This was a retrospective
study but for testing this hypothesis a definite gold standard (prostatectomy) was needed.
Of the 23 included patients with TRUS biopsy Gleason Score
identified undergrading in 48% (11/23). A further histological finding of considerable
concern was that 82% (9/11) of the patients with undergrading also had extracapsular
extension (Stage pT3). This underlines the considerable problem using biopsy Gleason
grade for risk assessment and prognostication. In the remaining 12 patients with a correct
identification of their Gleason score, none revealed extraprostatic growth. On ADC maps,
274
Discussion, Conclusions and Future Perspectives 13

measurement of tumour ADC were determined and for final evaluation only the ADC slice
per patient where the tumour showed the lowest ADC values was used for further
assessment. The reasoning behind this approach is that if ADC is to be used in a
prospective manner, radiologists will identify the hotspot (of low ADC) and use these values
to infer prediction of the Gleason grades present in the tumour. When using only the most
abnormal slice on ADC and comparing the ADC values for the 12 patients with no
undergrading vs. the 11 patients with undergrading, a significant difference was identified.
For ADC values the AUC of the ROC analysis was 0.88. AUC ROC analysis however does not
determine sensitivity or specificity. For cut-off purposes the desired sensitivity or
specificity level need to be identified. In this clinical setting a high sensitivity is most
desirable. This chapter therefore shows that DWI can indeed be of clinical value in patients
emphasizes that MR imaging SHOULD be part of any
patient with a diagnosis of prostate cancer.
Figure 6. Principal findings of Chapter 8: ADC values of tumour in patients with no-
undergrading vs. undergrading of their TRUS
Clinical problem 6 : Transrectal ultrasound guided biopsies only reflect the true aggressiveness
i.e. Gleason grade in about 60% of patients. Are there any methods to improve the tumour
aggressiveness representativeness in biopsy samples on which further management decisions can
be based?
275
Discussion, Conclusions and Future Perspectives 13

Background
As discussed previously, undergrading of biopsy determined Gleason Score is a
considerable problem faced in diagnosis and management of prostate cancer. Methods to
improve this have included increasing the number of biopsies, adjusting the biopsies
according to prostate volume or even performing saturation biopsies. Of paramount
importance in evaluating the current literature on the concordance between biopsy Gleason
Score and radical prostatectomy Gleason score, is the inherent prevalence of different
Gleason Score in the series evaluated. Overgrading (a higher Gleason Score found in biopsy
compared to radical prostatectomy), is of lesser importance as this usually constitutes less
than 10% of the discordance in most series. In many reports on improved overall
concordance rates using different biopsy schemes, a meticulous analysis of the data actually
reveals a high proportion of Gleason Score 3+3=6 tumours in prostatectomy. As these are
not undergraded on biopsy, the overall concordance rates give a false impression of the
exact undergrading of the higher Gleason grades, which were shown to still range between
30-40%. Grey-scale transrectal ultrasound, power Doppler ultrasound and contrast-
enhanced ultrasound are inherently insensitive in detecting and localizing tumour although
improvements have been found with the latter two techniques.
Solution to clinical problem 6: MR guided biopsies targeted towards the most abnormal regions
on DWI MR imaging represent a substantially improved prospective method for assessment of true
tumour aggressiveness.
Discussion
The findings and the study shown in Chapter 10 probably represent the crown of the
current thesis as it incorporates findings of multiple different studies into one single
conclusion. This prospective study incorporates the high diagnostic accuracy of
multiparametric, T2-w, DWI and DCE-MRI at 3T for tumour detection, the value of DWI in
determining the most aggressive component in the tumour, as well as MR guided biopsies
not only for diagnosis of malignancy but also for representing a much improved method to
obtain a reliable estimation of the true aggressiveness with a minimum of just 3 biopsy
cores. This was shown in a cohort of 34 patients with a prior negative TRUS biopsy and
276
Discussion, Conclusions and Future Perspectives 13

elevated PSA who received MR-DWI guided biopsies and a comparison cohort of 64 patients
in whom a tumour diagnosis was established using a 10-core TRUS biopsy scheme. In both,
radical prostatectomy served as gold standard to determine to what degree the highest
Gleason grade (HGG) identified in the respective biopsy techniques matched the highest
Gleason grades present in prostatectomy. MR guided biopsies targeted towards the most
abnormal regions on DWI were shown to have a vastly superior accuracy for determining
the true HGG compared to TRUS. When patients findings were sub grouped into patients
having a HGG of 2/3 vs. 4/5, MR guided biopsies had a 95% accuracy in defining the true
HGG group in prostatectomy, compared to 54% for routine 10-core TRUS biopsies.
The presence of Gleason grade 5 components in a tumour infers a particularly bad
prognosis for the patient. Identification of this component at biopsy is therefore considered
essential. When the overall accuracy rate for this component in biopsy-prostatectomy is
evaluated, conventional TRUS biopsies only identify 30% of grade 5 components, compared
to 73% for MR guided biopsy. A substantial undergrading in biopsy would occur if the HGG
on biopsy was 3 while in prostatectomy a HGG of 5 was identified. This occurred 57% of
patients when conventional TRUS biopsy was performed and did not occur in any patients
using MR guided biopsies. In the 27% of MR patients where the biopsy did not represent a
HGG of 5 but the prostatectomy did, the HGG was 4 on biopsy, representing a more
favorable underestimation.
Figure 7. Principal findings of Chapter 10. Performance of MR-GB and 10-core TRUS
biopsy to predict the true highest Gleason grade (HGG) in prostatectomy.
277
Discussion, Conclusions and Future Perspectives 13

Problems faced by Radiologists:
Clinical problem 7 : No prostate looks alike. The transition zone is an especially chaotic region.
What multiparametric MR imaging features and techniques are available and what is the
diagnostic accuracy for these techniques at 3T.
Background
The transition zone (TZ) exhibits age related changes in prostate anatomy. Under the
influence of dihydrotestosterone, the TZ undergoes hyperplastic changes with various
degrees of glandular hyperplasia and/or fibromuscular hyperplasia giving the TZ of the
aged man (usually > 50 years) a typical heterogeneous appearance. Adenocarcinomas
developing within the TZ often have different behavioral characteristics being more often
confined to the gland, are associated with higher PSA levels and often tend to be larger at
diagnosis compared to PZ tumours. Furthermore it is also known that other types of genetic
mutations may be present in these tumours. Nevertheless, they still cause considerable
diagnostic challenges but they are important to find as Chapter 4 indicated that the
majority of tumours in patients with persistent elevated/elevating PSA levels and negative
TRUS biopsies are located in the TZ. From a histopathological point of view, it is also
important to consider the fact that the growth pattern of most prostate tumours does not
consist of a mere spherical enlargement of a tumour mass but represent a mixture of tumor
growing in-between normal pre-existing ducts and stroma. Apart from the more sheet like
growth pattern of extremely high-grade components (Gleason grade 5), the visibility of
tumours on any imaging modality for that sake, is influenced by the relative contribution of
normal and intermixed tumour tissue within a particular region. The peripheral zone,
containing numerous large ducts filled with fluid, usually has a high signal intensity on T2-
weighted imaging. Identification of tumour is therefore more readily possible as lower-
signal intensity regions of tumour relative to the high signal intensity surrounding it is
present. For the TZ, this is much more difficult as the fibromuscular regions of BPH tissue
in the TZ also show low signal intensity on T2-w imaging as well as water movement
restriction on DWI. Furthermore, the TZ is a highly vascularized region and enhancement
patterns in “normal” TZ tissue are similar to peripheral zone tumours. This makes the
278
Discussion, Conclusions and Future Perspectives 13

evaluation of the TZ for the presence of tumour much more challenging. Identifying tumour
in the TZ is best summoned up by what a dear colleague, Dr. Joe Bush from Chattanooga,
Tennessee says about finding tumour there:
TZ is identified by observing disorganized chaos within a region of organized
Furthermore one needs to have an artistic approach as well, as hobby artist, Prof. Barentsz
appreciates the “erased charcoal sign” on T2-w, as a strong indicator of TZ tumour. This
refers to the visual effect of smearing fine charcoal on a painting or artwork.
This challenge has long been a reason why radiologists not familiar with prostate MR
imaging have been reluctant to become more involved in prostate imaging.
Solution to clinical problem 7 : Multiparametric 3T MR imaging is a very accurate technique to
detect and localize clinically significant aggressive transition zone cancer.
Discussion
Contrary to common belief, detection of prostate cancer in the TZ is possible with a high
diagnostic accuracy using multiparametric MR imaging. In Chapter 6 we evaluated the
performance of detecting and localizing TZ cancer using 4 experienced prostate radiologists.
It is of crucial importance to consider the prevalence of low-grade (Gleason grade 2/3) vs.
high-grade (Gleason 4/5) tumours in any analysis of the performance in detecting,
localizing, staging as well as the concordance rate between biopsy and prostatectomy. As
discussed in previous chapters, a high prevalence in a cohort of low-grade tumours for
example, will result in a good concordance between biopsy Gleason grade and
prostatectomy Gleason grade. Furthermore it will result in a good staging accuracy (low
prevalence of pT3 disease) on MR imaging but will result in poor detection and localization
accuracies. This is probably one of the most important reason why results differ so much in
literature for the accuracies of biopsy techniques and MR for localization. It is therefore
important to consider the specific value of MRI for low-grade disease vs. high-grade disease,
similar to Chapter 10, instead of reporting on the overall value.
279
Discussion, Conclusions and Future Perspectives 13

From the study reported in Chapter 6 a number of important points came to light. Firstly,
high-resolution T2-w imaging remains the cornerstone for evaluation of any prostate. To
the trained eye, features indicative of tumour in the TZ can sufficiently serve to allow
detection (86%) of high-grade tumours. The addition of functional imaging DCE and DWI,
does improve the overall detection rate, but does so only moderately (91%). On the
contrary, low-grade tumors are notoriously undetectable using T2-w imaging alone (24%).
The addition of functional imaging however improves this detection to 47%.
Two specific points need further explanation. Detection vs. localization. In the study
reported in Chapter 6, detection refers to: does the patient have a TZ tumour – yes/no
while localization refers to the exact mapping of tumour in the TZ in 6 different regions.
While the first is sufficient to determine if a patient has tumour and where to direct the
needle for biopsy purposes, the localization is needed for optimal surgical planning,
planning of intensity modulated radiotherapy (IMRT) and for low-grade tumours, also the
planning of brachytherapy, cryotherapy or laser therapy. The study evaluated both.
Although the addition of functional imaging only slightly, but not significantly, improved the
detection accuracy of high-grade tumours, it did however improve the overall localization
accuracy from an AUC of 0.91 to 0.94 (p=0.01). For low-grade tumours, the detection rates
increased substantially from 24% to 47% (p=0.02) while the overall localization improved,
however not significantly, from an AUC of 0.56 to 0.64.
Not detecting low-grade tumours and therefore not overdiagnosing indolent (clinically
insignificant) tumours would according to current knowledge and understanding, be ideal.
-grade tumours
should be ideal candidates for active surveillance. A finding of the above mentioned study
however does put a question mark on the validity of these criteria for TZ tumours. Our
study did confirm prior reports that TZ tumours tend to be large. Of note was that the
median tumour volume of low-grade tumours in our study was 3.5 cm3 (range 0.5 – 22 cm3)
compared to 7.4 cm3 (0.5 -15.7 cm3) for high-grade tumours. Therefore all the TZ tumours
in our study would therefore be considered as not being indolent (i.e. not suitable for active
surveillance). The truly massive sizes of some of the low-grade tumours would evoke the
question on what the management should be of these tumours? Although the absolute
number of patients with TZ tumours in our study was rather small, it is important to
280
Discussion, Conclusions and Future Perspectives 13

consider that 22% (2/9) of the patients with low-grade TZ revealed extracapsular extension
(one pT3a and one pT4) while 72% (9/11) of the high-grade tumours where of stage pT3/4.
Multiparametric imaging misses 50% of low-grade tumours. Based on the above findings,
the author is of the opinion that the Gleason Score should not be the most important feature
to consider for the best management of TZ tumours. Future research should definitely
focus on the behavioral characteristics especially as some of these “benign” tumours were
associated with locally advanced disease (extracapsular extension).
Figure 8. Principal findings of Chapter 6. Detection rates (top) and localization AUC for
multiparametric MRI for low-grade and high-grade TZ tumours.
Clinical problem 8 :
prostate tissue in a dif
quantitative measurements and our assessment of what is malignant?
281
Discussion, Conclusions and Future Perspectives 13

Background
What do we usually mean by 'normal'?
“Referring to humans, we mean that he or she is like everyone else, behaves as most people
behave, and stays within current conventions. But we have a problem, because now-a-days
the idea of what is normal changes from one decade to another. Fortunately the popular
press keeps us up-to-date by surveys and advice columns. Normality for humans in fact has
nothing to do with statistics. It refers to a norm, a model of perfection, an example to be
followed. It indicates what we should be. Normality is therefore something to strive for,
something at which to aim, it is not what most people do. It is what they would do if they
lived up to their human potential.”
“Every normal person, in fact, is only normal on the average. His ego approximates to that of
the psychotic in some part or other and to a greater or lesser extent.” ( )
“To study the abnormal is the best way of understanding the normal. “
“Normal is in the eye of the beholder. Normal is nothing more than a cycle on a washing
machine. “
Based on the above mentioned opinions about normality it is clear that from a philosophical
point it is quite bothersome to define what is normal. From a scientific point of view
especially looking at physical characteristics of the prostate one can however get closer to
defining normality. Any pathologist and radiologist dealing with the prostate will attest that
no prostate looks alike needless to say, no tumour looks exactly alike. Based on our
findings in Chapter 7 it was observed that the median ADC values for the “normal”
peripheral zone varied substantially between patients. Tumours in the prostate are not
mass-like, expansile growing lesions but intermixed with various amounts of “normal”
background tissue and develop out of pre-existing glandular tissue. Since normal prostate
PZ tissue fluctuates significantly in ADC value, the ADC values of an aggressive tumour may
show similar fluctuations. If normal PZ and tumour ADC are correlated, considering both
simultaneously, may lead to better estimates of aggressiveness. Inter-patient ADC variation
could therefore affect the discriminative power of ADC both for prostate cancer localization
as well as for the determination of prostate cancer aggressiveness.
282
Discussion, Conclusions and Future Perspectives 13

Solution to problem 8 : Peripheral zone ADC show a significant inter-patient variation, which has
a significant effect on the prediction of prostate cancer aggressiveness. Correcting this effect on a
per patient basis results in a significant increase in diagnostic accuracy.
Discussion
In Chapter 11 we have evaluated normality and “normalness” of the peripheral zone. In a
first set of 10 patients who received 3 separate 3T MR imaging sets at different time points,
the variation of ADC values for a fixed given region of “normal” appearing peripheral zone
was measured. Here we showed that the normal PZ ADC differed significantly between
patients relative to measurement variability (p<0.01). This significant inter-patient
variation in normal peripheral zone ADC values (1.2 – 2.0 x 10-3 mm2/s), is something we
could not solely attribute to measurement variability (average measurement SD 0.068 ±
0.027 x 10-3 mm2 /s). We therefore hypothesize that the inter-patient variations arise from
natural variations in prostate physiology.
In the same chapter another cohort of 51 patients were used and we have determined that
adding normal PZ ADC values to the tumour ADC values (using linear regression analysis),
resulted in a significantly improved prediction of cancer aggressiveness (p=0.01). This
suggests that tumour ADC values should not be considered absolute but that these values
are influenced by “background” variation of normal PZ tissue composition. Adding the
information of normal PZ ADC, increased the AUC from 0.91 to 0.96 (p<0.05) in separating
low-grade from combined intermediate- and high-grade prostate cancer.
Figure 9. Clinical useful nomogram for assessment PZ cancer aggressiveness.
283
Discussion, Conclusions and Future Perspectives 13

Clinical problem 9 : Prostate multiparametric MR imaging should be left to the experts. The
prostate is too complex, too many imaging modalities are needed and tumours are very
heterogeneous. Is there any help for the non-expert?
Background
Numerous publications have shown the necessity of performing multiparametric MR
imaging to improve the tumour localization capabilities. As discussed previously, not only
a natural heterogeneity of the normal prostate anatomy is present, also tumours reveal
heterogeneous features. Furthermore benign conditions like prostatitis, high-grade PIN,
atrophy, atypical adenomatous hyperplasia, BPH and fibrosis can all reveal features that
mimic tumour on all MR imaging modalities. Currently, quantitative cut-off values on MRI
are not used routinely to differentiate tumour from benign or normal changes in the
prostate. Images are evaluated qualitatively that is, a relative abnormality identified in
relation to a normal surrounding tissue. T2-w imaging is purely qualitative and further
affected by coil profile changes. Therefore signal intensity as such on T2-w imaging cannot
reliably be used to differentiate tumour from non-tumour tissue. Quantitative T2-w
imaging is possible but is of excessive imaging duration and of low spatial resolution. ADC
maps obtained from DWI imaging are quantitative but from literature no clear cut-off values
have reliably been reproduced as b-factor differences, TE differences and imaging at 1.5T vs.
3 T resulting in different ranges are being reported. Absolute values for DCE-MRI are also
difficult to determine as correct assessment of the arterial input function as well as the
normal heterogeneity of microvascular features in tissue, affecting the absolute values. All
these factors have lead to a great reluctance on part of radiologists to evaluated MR imaging
of the prostate. Additionally substantial reader variability especially for less-experienced
observers has been reported. Therefore techniques that can aid radiologists in improving
their evaluation of the prostate and reducing the inter-reader variability are in great need.
Solution to problem 9 : The addition of computer aided diagnosis (which incorporates
quantitative ADC values and quantitative pharmacokinetic DCE values) for evaluation of prostate
cancer suspicious regions on 3T MRI, significantly improves the discriminating performance for less
experienced observers for both the peripheral and transition zone.
284
Discussion, Conclusions and Future Perspectives 13

Discussion
In Chapter 12 we report on the development of a computer aided diagnosis (CAD)
technique for prostate cancer evaluation in the PZ and TZ. A novel technique of
determining quantitative pharmacokinetic DCE parameters using the normal peripheral
zone for normalization and calibration was used. This has the advantage that both the
arterial input for the prostate itself as well as the inherent per patient variability in normal
microvascular features, are compensated for. Combining these features with ADC values, a
computer was trained to discriminate tumour lesions and benign but tumour suspicious
lesions (on MRI) both in the PZ and TZ. The results presented in Chapter 12 indicate that
such a CAD technique can be developed and revealed a stand-alone AUC ROC performance
of 0.92 for the PZ and 0.87 for the TZ.
Using such a CAD technique to aid radiologists in improving their evaluation of
multiparametric MRI of the prostate was then further evaluated. In this study 6 less-
experienced and 4 experienced prostate radiologists evaluated 206 different prostate
regions in 34 patients using 3T multiparametric MRI. For each region, a tumour likelihood
had to be given before and after a CAD tumour likelihood was shown to the reader. In this
study it was firstly shown that the stand-alone performance of CAD is similar to prostate
experienced radiologists (overall AUC of CAD 0.90 vs. AUC of 0.88 for experienced
radiologists). Secondly, the addition of CAD significantly improved lesion discriminating
performance for less experienced radiologists both for the peripheral zone (pre-CAD AUC
0.86 to post-CAD AUC of 0.95) as well as the transition zone (pre-CAD AUC 0.72, post-CAD
0.79). A final important finding of this study indicated that after CAD, less experienced
radiologists reached similar performances as experienced radiologists in evaluating the
prostate. It therefore appears promising that in due time, by using CAD, more radiologists
would be willing and able to use MRI for prostate analysis. This will therefore result in
better support for urologists and radiotherapists in finding solutions and answers to most
of their eminent problems in the diagnosis and management of prostate cancer.
285
Discussion, Conclusions and Future Perspectives 13

Figure 10. Principal findings of Chapter 12. AUC for less-experienced and experienced
observers grouped according to overall, PZ and TZ performances.
286
Discussion, Conclusions and Future Perspectives 13

LIMITATIONS
The vast majority of any PhD research work is devoted to the positive and “ground-breaking”
discoveries presented in one’s thesis. This is an inherent human error. Sir Bertrand Russell has
strikingly identified this by stating:
work is terribly
The author cannot but stress that this thesis is but a drop of water in the vast ocean of
knowledge. A mere drop and nothing more. The information presented in this thesis, might
mean life or death, hope or despair, meaning or nihility to many patients, but in the vastness of
space, time and things to come, it will not have any substantial influence whatsoever.
Having a state-of-the art 3T MRI scanner, the availability of MR guided biopsy equipment, in-
house dedicated analytical software, motivated urologists, radiologists, pathologists, physicists
and off-course the immense importance of funding for research, is an exceptional combination
that is (and for the time being) of particular scarcity. Therefore, the value of 3T MRI in the
diagnosis and management of prostate cancer will for a number of years to come be reserved to
a few centers of excellence. All the links in the above mentioned chain need be in place to fully
show its true value.
Another important consideration is to acknowledge the fact that making mistakes and being
uncertain in evaluating the prostate will definitely happen on some occasions - even to the most
hardened prostate radiologists. MRI is an exceptionally good technique, yet it is not perfect. In
the pressure of “normal” routine radiological work, outside an experimental research setting,
results will always be worse than the most optimistic research. That is a known fact. Also, it
does not matter how many patients one has seen, how many images one has viewed or number
of publications written, in medicine exceptions are the rule. The author can truly attest that
tumours in some patients can be seen clearly in others not at all. The one is regarded as highly
malignant, while in reality it is benign.
Although MR imaging even at 1.5T is generally available, MR guided biopsy equipment is not
(yet). Despite being commercially available, investing in such equipment requires a dedicated
team of urologists and radiologists. To the opinion, MR imaging should only performed
287
Discussion, Conclusions and Future Perspectives 13

by experienced and trained radiologists in this field, who are expected to deal with prostate MR
imaging on a daily basis. In this thesis a number of publications dealt with MR guided biopsies
(Chapter 3, 4, 5, 10). One might argue that with dedicated fusion software, biopsies might be
performed under ultrasound guidance. As for now, at least the gold standard of biopsying areas
abnormal on MRI, has been determined. If in future, MR guided ultrasound biopsies may prove
to be equally accurate and may result in a future financial advantage. Although MR biopsies are
performed within 30 minutes, MR time remains valuable.
Chapters 7, 8 and 9 were chapters dealing with the evaluation of MR imaging and
aggressiveness using radical prostatectomy as gold standard. These studies were retrospective
in nature. It is of paramount importance that such findings should also be validated in a
prospective ideally multi-centre setup. For Chapter 10 this was attempted, as DWI was used to
guide the needle towards the darkest most “aggressive” spot. The results prospectively indicate
that at least DWI allows sampling of tissue being truly representative of the most aggressive
component. Furthermore slight imaging differences exist between different MRI vendors and
more importantly differences exist between 1.5T and 3T. Quantitative values on the one scanner
do not necessarily equate to the same quantitative values on the scanner of a different vendor.
The presented results should therefore also be evaluated between different vendors and for
different field strength. Chapter 11 did reveal that inter-patient variations for PZ ADC exist.
However no satisfactory explanation could be identified to explain the intra-patient temporal
variation. Further research should focus on addressing the potential temporal effect of
ejaculation, amount of bicycle riding etc. as external / internal influences of our absolute
measurements.
Chapter 12 described the use of a CAD system to aid radiologists in improving their
performance. A drawback of the current setup was that tumour suspicious regions were
identified upfront and radiologists were asked to characterize those presented regions only.
This was done to test the potential value of a CAD system. In the manner that our current CAD
system works, a widespread implementation at this stage is not possible. In future, this system
will be changed (work in progress) to make the radiologists themselves, identify the region of
concern and then obtain a second opinion from CAD or alternatively, the CAD should project
tumor probability maps.
288
Discussion, Conclusions and Future Perspectives 13

A final thought on the limitations of the current thesis. Although some important clinical
questions have been answered, a legion more, still exist. For the prostate gland itself, local
staging is another further crucial point especially to aid in decisions on preservation of
neurovascular bundles and to reduce positive surgical margins. The predecessors have
performed initial studies in this regard, but the final word has not been spoken yet. The current
thesis dealt insufficiently with methods to determine aggressiveness of TZ tumours and
hopefully current ongoing work will find some solution for this.
289
Discussion, Conclusions and Future Perspectives 13

FUTURE PERSPECTIVES
Local prostate : Diagnostics
Active surveillance is becoming of increasing importance. There is tremendous value for
MR imaging in identifying patients who are not true candidates for active surveillance as
well as identifying patients over time, when their tumours are differentiating into more
aggressive phenotypes that need active intervention.
Tumor mapping – although information on tumour localization accuracies using MRI are
published, information on the capabilities of MRI based exact mapping of tumour (for
focal therapy), is still lacking and further work is needed prior to full implementation of
prostate sparing therapy.
Currently, many histopathological features underlying the visibility and effect that these
features have on multiparametric imaging have not been studied sufficiently. It is crucial
for any scientist working on developing new techniques for imaging to understand the
pathophysiological processes underlying imaging parameters. The Gleason Score is not
the only marker for aggressiveness and other histological markers of aggressiveness
should also be evaluated and correlated to MRI in future. Novel techniques are rapidly
gaining importance for more reliable predictors of tumour characteristics and behavior.
The most important at this stage appears to be the upcoming techniques in genomics and
proteomics whereby tissue (preferably only a biopsy sample) analyzed, can be
characterized on the presence of pathological mutations and molecular compositions
which may facilitate decision making on management beyond and in addition to the most
widely used Gleason Score. MRI facilitated (either via MR-guided biopsies or MR-TRUS
biopsies) targeting of tissues for these purposes would be a further important future
development.
Screening with MRI – To many a blasphemous statement! The author believes this to
hopefully be the greatest contribution of MRI in the next few years. Having a short (15
min), highly sensitive (for aggressive tumours) imaging protocol, will certainly have its
merit in identifying patients with an elevated PSA who should or should not receive
targeted biopsies. The author hopes to eventually see the day when this paradigm shift
has occurred.
290
Discussion, Conclusions and Future Perspectives 13

MR imaging at > 3 Telsa field strength – Researchers will always find such things
interesting. The value? The future will tell.
Local prostate therapeutics
Focal therapy – many very exciting MR guided focal therapy techniques are being
developed and tested. Of special note are MR compatible cryotherapy, laser therapy and
also high intensity focused ultrasound. These would hopefully establish themselves as
useful techniques for managing small, relative benign tumours or they will serve a
valuable role as salvage therapy after prior brachytherapy or radiotherapy and maybe
also prostatectomy.
Metastatic disease diagnostics
MR lymphography – with the loss of the only proven lymphnode imaging agent Sinerem,
the future management of advanced prostate cancer received a major blow and setback.
Currently however, new lymphotrophic particles are in development and hopefully will
emerge again, like the Phoenix from the ashes, in not too distant future.
Skeletal metastasis – currently 99mTc bone scintigraphy is still heavily relied upon for
exclusion or identification of bone metastases. Unfortunately the sensitivity and
specificity are generally not good. Recent publications have identified that MRI is
superior in identifying skeletal metastasis in prostate cancer. Ongoing research which
includes “whole-body” diffusion weighted imaging might eventually prove to be the
modality of choice for skeletal metastasis assessment and potentially make 99mTc bone
scinitigraphy obsolete, at least for the establishment of the presence of prostate
metastasis or not. The comparative value of MRI vs. 18F (NaF) PET or 11C
(Choline/Acetate) PET in detection of tumour recurrence and metastasis is still an open
undecided battlefield.
Metastatic disease therapeutics
With improved identification of metastatic lymph nodes and bony metastases,
therapeutic modalities including intensity modulated radiotherapy, proton therapy or
even selective surgery may become MR guided and hopefully provide a valuable
contribution in future to reduce morbidity and mortality.
291
Discussion, Conclusions and Future Perspectives 13

FINALE
Following the conclusions made in this thesis, there are but a few obstacles in the way for
clinicians and patients to have an extremely useful weapon in their arsenal against prostate
cancer. Now it is time that treating clinicians should be made aware of the great potential of
MRI, that radiologists learn and become confident and good in the evaluation thereof. Patients
should be comfortable with the knowledge that they are receiving top of the range diagnostics.
Lack of awareness is therefore one of the greatest obstacles.
The cautioned reader would certainly raise the valid question of cost? Our health systems are
already overburdened with medical costs and reductions. The author believes that cost will
always be an issue. There will never be enough funding to deliver all the groundbreaking
discoveries/techniques and treatments to patients. That is unfortunately the world we live in.
Cost however, should not necessarily be the principal obstacle. In the long run, the improved
early diagnosis and more efficient management will (daunting to say) reduce morbidity and
mortality and be more cost-efficient. The large European trial on using PSA for PCa screening
has already revealed a 20-30% reduction in mortality. Undoubtedly adding MRI on top of this,
hopefully not only mortality will be reduced but also unnecessary morbidity.
Prior studies at 1.5T necessitating the endorectal coil for adequate imaging seemed a major
hurdle for widespread utilization. For accurate determination of minimal extracapsular
extension, even at 3T, the endorectal coil is still needed and remains a valuable tool, despite its
drawbacks. It is however, currently feasible to perform MR imaging without the endorectal coil
incl. high-resolution T2-weighted imaging, DWI and DCE in 20 min duration, making
implementation into routine clinical use (here this is already the case) absolutely feasible.
Imaging is however performed at 3T but it is merely a matter of time that 3T MR imaging will be
the standard MR performed in most hospitals and that 1.5T will become increasingly obsolete.
Like the old English saying: ”Time and tide waiteth for no man!” so does routine MRI for prostate
cancer diagnosis and management – it will come!
Yes We Scan!
292
Discussion, Conclusions and Future Perspectives 13

FINALE
Following the conclusions made in this thesis, there are but a few obstacles in the way for
clinicians and patients to have an extremely useful weapon in their arsenal against prostate
cancer. Now it is time that treating clinicians should be made aware of the great potential of
MRI, that radiologists learn and become confident and good in the evaluation thereof. Patients
should be comfortable with the knowledge that they are receiving top of the range diagnostics.
Lack of awareness is therefore one of the greatest obstacles.
The cautioned reader would certainly raise the valid question of cost? Our health systems are
already overburdened with medical costs and reductions. The author believes that cost will
always be an issue. There will never be enough funding to deliver all the groundbreaking
discoveries/techniques and treatments to patients. That is unfortunately the world we live in.
Cost however, should not necessarily be the principal obstacle. In the long run, the improved
early diagnosis and more efficient management will (daunting to say) reduce morbidity and
mortality and be more cost-efficient. The large European trial on using PSA for PCa screening
has already revealed a 20-30% reduction in mortality. Undoubtedly adding MRI on top of this,
hopefully not only mortality will be reduced but also unnecessary morbidity.
Prior studies at 1.5T necessitating the endorectal coil for adequate imaging seemed a major
hurdle for widespread utilization. For accurate determination of minimal extracapsular
extension, even at 3T, the endorectal coil is still needed and remains a valuable tool, despite its
drawbacks. It is however, currently feasible to perform MR imaging without the endorectal coil
incl. high-resolution T2-weighted imaging, DWI and DCE in 20 min duration, making
implementation into routine clinical use (here this is already the case) absolutely feasible.
Imaging is however performed at 3T but it is merely a matter of time that 3T MR imaging will be
the standard MR performed in most hospitals and that 1.5T will become increasingly obsolete.
Like the old English saying: ”Time and tide waiteth for no man!” so does routine MRI for prostate
cancer diagnosis and management – it will come!
Yes We Scan!
292
Discussion, Conclusions and Future Perspectives 13


English Summary - Nederlandse Samenvatting -
T. Hambrock; J. Barentsz
Auguste Rodin The Thinker
CHAPTER 14CHAPTER 14

English Summary
nce Imaging for the Detection and Aggressiveness
Assessment of Prostate Cancer
- From Theory to Practice -
SUMMARY STATEMENT OF THESIS
Every man with a DIAGNOSIS of prostate cancer SHOULD receive a Multi-
parametric MRI
Every man with the persistent SUSPICION for having prostate cancer
SHOULD receive a Multi-parametric MRI, and
Every man who needs correct AGRESSIVENESS assessment of his prostate
cancer SHOULD receive an MRI!
Prostate cancer has become a substantial burden to society. It has surpassed lung cancer as the
number one most commonly diagnosed malignancy in men. Furthermore it is the number 2
killer of men due to cancer. The U.S.A. has an annual rate of new prostate cancer (PCa)
diagnoses of around 220.000. This fact adds a substantial burden to doctors, patients and the
society, notably also as a psychological and financial burden.
Despite being a malignancy of predominantly older men, it appears from postmortem studies,
that the prevalence of prostate cancer in 30-40 year olds is high (25%), increasing to 60% at the
age of 60-70 year old,, and to >80% at 80 years. Nonetheless, most men die with prostate
cancer, and only 15% from it. Of further note is that 2/3rd of death occurs in elderly patients
(>75 years) . This translates to the following: of all patients diagnosed with PCa, only 5% (in the
U.S., equating to 11 000 deaths) of PCa deaths are in young men. Although disease specific
mortality for PCa is only 15%, a substantial additional number of patients suffer significant
morbidity i.e. impotence, incontinence, cystitis, proctitis, lymph edema and wound infections
following attempted radical treatment. The immense psychological trauma, like anxiety,
294
English Summary – Nederlandse Samenvatting – 14

uncertainty, worry and often depression, experienced by patients who have increasing PSA
values (thereby suggesting local disease recurrence or metastases) after attempted curative
radical treatment, cannot be denied.
Most prostate cancers are low-aggressive, and do not cause morbidity or even mortalitity. Until
now the determination of the tumour aggression is done by pathologic evaluation of tissue
samples, and expressed in the so called Gleason grade or scores. The correct establishment of
the Gleason grade/score is therefore of utmost importance for prognostication. It is associated
with advanced disease stage, associated with disease recurrence and overall survival. Herein
lies of one of the greatest pitfalls in current diagnosis and management of PCa: The current
random trans-rectal ultrasound guided biopsy techniques performed to make a definite
histological diagnosis of prostate cancer, do not only miss a substantial number of tumours but
also often miss (up to 40%) the most aggressive part of the tumour, resulting not only in an
under diagnosis of cancer but also in an under grading of tumours. Furthermore, following
radical treatment, clinicians often struggle to identify the sources of tumour tissue recurrence
following a post-treatment rise in PSA.
On a routine basis, patients undergo “screening” with blood serum Prostate Specific Antigen
(PSA) quantification. In general, PCa is associated with higher PSA values, yet PSA is non-
specific (specificity of 63%) due to other non-malignant disease processes also increasing blood
values. This poses a particular challenge to physicians. An arbitrarily PSA cut-off value is most
often used to decide on obtaining histological sampling of the prostate. At the cut-off value of 4
ng/ml, the sensitivity for detecting tumour is around 85%. Under this value around 15% of
tumours are missed while of these again, 15% are considered high-grade, representing tumours
that warrant definite treatment. For the values above 4 ng/ml, especially between 4 – 10 ng/ml
a low specificity is found resulting in a substantial amount of patients undergoing unnecessary
invasive diagnostic procedures. For a definite diagnosis of prostate cancer, clinicians most often
utilize transrectal ultrasound guided, random but systematic biopsies techniques, using 10-12
biopsy cores, spaced throughout the prostate gland. Such “brutal and archaic” methods are still
the cornerstone in current day and age. Fortunately, females have chosen the path of
enlightenment much earlier than men. Random multi-core sampling of breast tissue for
detection of malignancy is not part of the 21st century clinical practice or even the 20th century
practice for that matter.
295
English Summary – Nederlandse Samenvatting – 14

The author of this thesis therefore envisioned that a change to the initial management and
diagnosis of prostate cancer had to occur. A PARADIGM SHIFT is the only way forward. This
thesis therefore evaluated the important challenges faced by clinicians and patients and the
author sought to develop new techniques, apply current, recently developed techniques into
routine PCa care and determine the value that these can have on patient management. The aim
was to evaluate how it is possible reduce the number of biopsy needles and to increase its yield
and aggressiveness representation. This thesis was set up and evaluated these aspects from
“Theory to Practice”.
The following summary findings and conclusions can be drawn from this thesis:
In Chapter 3 the principal aim of our study was to test the technique and feasibility of
identifying tumour suspicious region maps obtained by multi-parametric 3T MRI and a 32
channel coil for directing MR guided biopsies. Furthermore, we evaluated the practicability of
MR guided biopsy on a 3T MR scanner using a MR compatible biopsy device. In this chapter we
concluded that multi-parametric MR imaging at 3T using T2-weighted imaging, DWI and DCE-
MRI is an accurate technique for the detection of tumour in these patients. Furthermore the use
of an MR guided biopsy device, to perform targeted biopsies towards tumour suspicious regions,
is a useful and accurate technique to make a definite diagnosis. A considerable number of
patients with persistent abnormal PSA values harbor tumour and should therefore receive
further evaluation with MRI.
In Chapter 4, the technique developed in chapter 3, using MR guided biopsies was performed in
a large clinical cohort of patients with persistently elevated PSA and at least two prior negative
TRUS biopsy sessions. The purpose of this chapter was to determine the absolute tumour
detection rate possible using 3T multi-parametric MRI and MR-GB in this cohort. Furthermore
we aimed to determine whether the detected tumours were clinically significant. In a
consecutive group of 68 men we were able to diagnose cancer in 59% of the patients.
Furthermore we determined that these tumours were deemed clinically significant in 93% of the
cases. Additionally, we established that tumours missed with serial TRUS biopsies are located
in regions not explicitly sampled by TRUS biopsy schemes. MR guided biopsies also significantly
outperformed conventional TRUS biopsy detection rates for different PSA, prostate volume and
PSA density subgroups. We concluded that MRI should therefore be part of any workup protocol
296
English Summary – Nederlandse Samenvatting – 14

of patients who are suspected of harboring malignancy but who have successive negative
biopsies.
In Chapter 5 we evaluated the feasibility of the combination of MR guided biopsy and diagnostic
3T MR imaging, in localization of PCa local recurrence after external beam radiation therapy. We
have shown that the positive predictive value of focal abnormal DCE enhancement for local
recurrence was 75% and concluded that 3T DCE-MRI followed by MR guided biopsies is a
feasible and very useful technique for diagnosing local recurrence of prostate cancer following
external beam radiotherapy.
The detection and localization of transition zone tumours is a particular challenge to
radiologists. Therefore, in Chapter 6 we sought to retrospectively determine Gleason grade 2/3
(low-grade) and Gleason Grade 4/5 (high-grade) transition zone cancer detection and
localization accuracies, using individual and combined multi-parametric MR imaging. Firstly, we
identified that high-resolution T2-w imaging remains the cornerstone for evaluation of any
prostate. For the experienced radiologist, T2-w imaging alone allows detection of 86% of high-
grade tumours. The addition of functional imaging: DCE and DWI, improves the overall
detection rate to 91%. On the contrary, low-grade tumours were found to be notoriously
undetectable using T2-w imaging alone (24%). The addition of functional imaging however
improved this detection to 47%. Our conclusion was that multi-parametric 3T MR imaging is a
very accurate technique to detect and localize clinically significant, aggressive transition zone
cancer.
The importance of accurately and non-invasively assessing the aggressiveness (i.e. Gleason
Score) of a tumour has many important implications in the clinical management of patients. Up
to now this has been elusive, therefore a great need exists for techniques to be developed to
assess this more accurately. In Chapter 7 we evaluated the relationship between ADC values
from 3T DWI-MRI and peripheral zone prostate cancer Gleason grades determined from step-
section specimens after prostatectomy. As the physical principals underlying diffusion weighted
imaging are sensitive to regions with high cellularity, our hypothesis was that this technique
could be useful to quantify and correlate tumour Gleason Score, which is known to be related to
cellularity. We showed that ADC values of prostate cancer in the peripheral zone inversely
related to prostate cancer Gleason grades, with low-, intermediate- and high-grade tumours
showing significant differences in ADC values (p<0.001). Furthermore, using the median ADC
297
English Summary – Nederlandse Samenvatting – 14

values of the most aggressive tumour regions, a high discriminatory accuracy was achieved for
discerning low-grade from combined intermediate- and high-grade cancers (AUC=0.90). We
therefore concluded that ADC values determined from DW-MR imaging at 3T represents a useful
biomarker for prostate cancer aggressiveness in the peripheral zone.
In Chapter 9 an additional potential biomarker for prostate cancer aggressiveness at 3 Tesla
was evaluated. Proton magnetic resonance spectroscopic imaging (MRSI) provides spatial
mapping of the tissue levels of the metabolites citrate, choline and creatine in the whole prostate
gland. Prostate cancer tissue is characterized by lower citrate levels and/or higher choline levels
compared to normal tissue resulting in the ratio of choline and creatine to citrate (Cho+Cr/Cit)
as a marker for prostate cancer. We validated the performance of MR spectroscopic imaging of
the prostate at 3T to assess tumour aggressiveness, based on the choline plus creatine to citrate
ratio (Cho+Cr/Cit) and choline to creatine rato (Cho/Cr), using the Gleason score of the radical
prostatectomy (RP) specimen as the gold standard. The metabolite ratios Cho+Cr/Cit and
Cho/Cr resulted in a tumour aggressiveness differentiation AUC of 0.70 and 0.74 respectively
and a combined AUC performance of 0.78. A significant correlation was found between the
maximum Cho+Cr/Cit ratio and the aggressiveness classes. A standardized threshold approach
was also developed to make the evaluation of spectroscopic data in a clinical setting more robust
and improve the inter-reader agreement of the evaluation. We concluded that 3T 1H-MRSI offers
potential for in vivo non-invasive assessment of prostate cancer aggressiveness.
To evaluate the potential clinical impact of our identified non-invasive aggressiveness
biomarker, DWI-MRI, we performed two different studies. The first study, being retrospectively
performed on a prostatectomy series of patients with prior multi-parametric MRI, is presented
in Chapter 8. An important clinical problem is that patients diagnosed with PCa Gleason Score
3+3=6 on biopsy, often represent an undergrading (and therefore need more radical therapy)
from those where it is a correct prediction (and therefore may be managed more
conservatively). In our study of 23 patients with TRUS biopsy Gleason Score
prostatectomy identified undergrading in 48% (11/23). This furthermore emphasizes and
underlines the considerable problem using biopsy Gleason grade for risk assessment and
prognostication. On ADC maps, measurements of tumour ADC were determined and for final
evaluation only the ADC slice per patient where the tumour showed the lowest ADC values was
used for further assessment. When using only the most abnormal slice on ADC and comparing
298
English Summary – Nederlandse Samenvatting – 14

the ADC values for the 12 patients with no undergrading vs. the 11 patients with undergrading, a
significant difference was identified. For ADC values the AUC of the ROC analysis was 0.88. This
chapter therefore showed that DWI can indeed be of clinical value in patients with Gleason Score
whom biopsies represent an underestimation of prostate cancer aggressiveness. This represents
another important emphasis that MR imaging SHOULD be part of any patient with a diagnosis of
prostate cancer.
The findings and the study shown in Chapter 10 probably represent the crown of the current
thesis as it incorporates findings of multiple different studies into one single conclusion. This
prospective study incorporated the high diagnostic accuracy of multi-parametric, T2-w, DWI and
DCE-MRI at 3T for tumour detection, the value of DWI in determining the most aggressive
component in the tumour, as well as MR guided biopsies not only for diagnosis of malignancy
but also for representing a much improved method to obtain a reliable estimation of the true
aggressiveness with a minimum of just 3 biopsy cores. MR guided biopsies targeted towards the
most abnormal regions on DWI were shown in this chapter to have a vastly superior accuracy
for determining the true highest Gleason grades compared to conventional 10-core transrectal
guided biopsies. We showed that MR guided biopsies had a 95% accuracy to represent the true
highest Gleason grade group (low vs. high) in prostatectomy, compared to 54% for routine 10-
core TRUS biopsies.
Based on our findings in Chapter 7,
peripheral zone varied substantially between patients. Since normal prostate PZ tissue
fluctuates significantly in ADC value, the ADC values of tumour may show similar fluctuations. If
normal peripheral zone and tumour ADC are correlated, we hypothesized that considering both
simultaneously, might lead to better estimates of aggressiveness. Inter-patient ADC variation
could therefore affect the discriminative power of ADC both for prostate cancer localization as
well as for the determination of prostate cancer aggressiveness. In Chapter 11 we have
We measured the intra-patient
variation of . Here we
showed that the normal PZ ADC differed significantly between patients relative to measurement
variability per patient (p<0.01). A significant inter-patient variation in normal peripheral zone
ADC values (1.2 – 2.0 x 10-3 mm2/s) was noted and we attributed this to natural variations in
299
English Summary – Nederlandse Samenvatting – 14

prostate physiology. We then further determined that adding normal PZ ADC values to the
tumour ADC values (using linear regression analysis), resulted in a significantly improved
prediction of cancer aggressiveness (p=0.01). This suggested that tumour ADC values should
not be considered absolute but that these values are influenced by “background” variation of
normal PZ tissue composition. Adding the information of normal PZ ADC, increased the AUC
from 0.91 to 0.96 (p<0.05) in separating low-grade from combined intermediate- and high-grade
prostate cancer. We therefore concluded that peripheral zone ADC shows a significant inter-
patient variation, which had a significant effect on the prediction of prostate cancer
aggressiveness. Correcting this effect on a per patient basis resulted in a significant increase in
diagnostic accuracy.
Chapter 12, being last but not least in the line, represented an important aspect to aid bringing
MR imaging of the prostate into routine clinical use. Despite the apparent “ease” and “value” of
MRI shown in this thesis, evaluation of the multi-parametric images is notoriously challenging
and often a reason why many a radiologist is reluctant and not willing to take up the challenge of
learning prostate MR interpretation. To aid radiologists, especially the unacquainted and
inexperienced ones in improving their confidence and accuracy when reporting on multi-
parametric MRI, we have developed a novel computer aided diagnosis (CAD) system which
utilizes quantitative pharmacokinetic parameters derived from DCE-MRI, in combination with
absolute ADC values from DWI to differentiate tumour from benign but tumour suspicious
regions on MRI. In this chapter we presented the results which indicated that such a CAD
technique could be developed and revealed a stand-alone AUC ROC performance of 0.92 for the
peripheral zone characterization and 0.87 for the transition zone. We then sought to determine
the effect of computer-aided diagnosis (CAD) on less-experienced and experienced observer
performance in differentiating benign and malignant prostate lesions on 3T multi-parametric
MRI (MP-MRI). The addition of CAD significantly improved lesion discriminating performance
for less- experienced radiologists both for the peripheral zone (p<0.001) as well as the transition
zone (p=0.01). After CAD, less-experienced radiologists (AUC=0.91) reached similar
performances as experienced radiologists (AUC=0.93). CAD methods that aid radiologists
especially those less experienced in prostate MRI, may expedite utilization of multi-parametric
MR imaging for accurate detection and localization of prostate cancer.
300
English Summary – Nederlandse Samenvatting – 14

In chapter 13 the previous ones are discussed. The general conclusion is that with multi-
parametric MRI and MR-biopsy, less needles are used with an increased yield and with the
added bonus (because of lesion targeting), a more accurate presentation of the true tumour
aggression (Gleason grades). With this technique, insignificant cancers can be differentiated
from significant ones. The MRI-technique is substantially superior to TRUS-biopsy for this
purpose.
Future perspectives:
1. Multi-parametric MRI should be implemented as fast as possible. Implementation
barriers should be defined and solved.
2. The value of multi-parametric MRI in screening should be investigated. This technique
in combination with PSA, potentially can lead to implementation of prostate screening.
3. Also the role of multi-parametric MRI in Active Surveillance should be evaluated
4. The same is true for MR-guided minimal invasive focal therapy, as the most aggressive
tumour part can be mapped.
5. CAD will enhance implementation of multi-parametric MRI, however, a substantial
amount of research in this regard is needed.
6. The potential, additional value of 7T MRI should be explored.
A final word of consideration:
According to the author, sufficient stones have been dislodged to aid in bringing about a
PARADIGM SHIFT in diagnosis and management of prostate cancer. The thunder sounds of the
“Battle of Anghiari” are audible. May this battle turn out to be a victorious one for patients, their
families and clinicians alike!
Let us as clinicians never forget the purpose of all our work and endeavor:
301
English Summary – Nederlandse Samenvatting – 14

Nederlandse Samenvatting
MRI bij de detectie en de bepaling van de aggressiviteit van
- Van Theorie tot Praktijk
SAMENVATTING VAN DE STELLINGEN OP BASIS VAN DIT
PROEFSCHRIFT:
Iedere man met de DIAGNOSE van prostaatkanker MOET een multi-
parametrische MRI ondergaan
Iedere man met een blijvende VERDENKING op het hebben van
prostaatkanker MOET een multi-parameterische MRI ondergaan
Iedere man bij wie een nauwkeurige bepaling van de AGRESSIVITEIT van
prostaatkanker nodig is MOET een multi-parametrische MRI ondergaan!
Prostaatkanker is een aanzienlijk maatschappelijk probleem geworden. Deze vorm van kanker
heeft longkanker van de eerste plaats van de meest voorkomende maligniteiten verdrongen.
Bovendien is het de 2e doodsoorzaak ten gevolge van kanker bij de man. In Nederland worden
er jaarlijks 9.000 nieuwe diagnoses gesteld. Naast een groot maatschappelijk probleem is dit een
aanzienlijke belasting voor patiënten en artsen, met aanzienlijke psychologische effecten en
hoge kosten van de zorg.
Ondanks het feit, dat prostaatkanker een ziekte van de “oude man” is, laten post-mortem studies
zien, dat deze vorm van kanker al bij 25% voorkomt bij mannen van 30-40 jaar, toenemend tot
>80% bij mannen van 80 jaar. Toch gaan meer mannen dood “met” dan “aan” prostaatkanker.
Bovendien treed 2/3de van de sterfte op bij de oudere patiënten (>75 jaar). Dit houdt in, dat
slechts 5% van de sterfte door prostaatkanker gezien wordt bij jonge mannen. Dit zijn er
302
English Summary – Nederlandse Samenvatting – 14

jaarlijks 450. Alhoewel de ziekte specifieke sterfte slechts 15% is, is de morbiditeit na therapie
(zoals impotentie, incontinentie, blaasontsteking, gezwollen benen en infectie) aanzienlijker.
Hier komen de gevolgen van een PSA-stijging na een radicale behandeling (zoals angst
onzekerheid, zorg, depressie) nog eens bij. Deze worden vaak niet voldoende herkend en
gewaardeerd.
De meeste prostaatkankers zijn laag agressief en veroorzaken geen klachten en de man gaat er
niet aan dood. Daarom worden deze kankers ook wel niet-significant genoemd. De agressie van
de kanker wordt tot nu toe bepaald door pathologisch onderzoek van tumorweefsel, verkregen
met een echografisch geleid biopt via de anus en uitgedrukt in de zogenaamde Gleason
gradering. De juiste bepaling hiervan is van zeer groot belang voor de bepaling van de juiste
therapie en de prognose. En dit is nu net de grootste valkuil! Met de tot nu toe gebruikelijke
rectale echogeleide biopsie (het wegnemen van stukjes weefsel via de anus) wordt niet alleen
een aanzienlijk aantal prostaatkankers gemist, maar wordt ook het meest agressieve deel van de
kanker in 40% gemist, hetgeen leidt tot het later ontdekken van de tumor of tot ondergradering
van de agressie ervan. Het behoeft geen uitleg, dat dit leidt tot onderbehandeling of inefficiënte
behandeling.
Op dit moment laat meer dan de helft van de mannen hun PSA testen. Helaas is niet alleen de
PSA verhoogd bij kanker, maar wordt dit ook vaak gezien bij goedaardige prostaataandoeningen
(specificiteit van de test is 63%). Wanneer het PSA niveau boven een bepaalde waarde komt,
wordt overgegaan tot de echografische biopten. Bij een drempelwaarde van 4 ng/ml wordt 15%
van de kankers gemist. Van de ontdekte tumoren is weer 15% agressief, en behoeven
behandeling. Daarentegen hebben de meeste mannen met een licht verhoogd PSA (4-10 ng/ml)
door de lage specificiteit van de PSA-test geen prostaatkanker, en ondergaan derhalve een
onnodig echo-biopt. Omdat met de echografie de kanker veelal niet zichtbaar is maar de prostaat
wel, wordt met het echografisch biopt op 10 tot 12 stelselmatige plekken uit de prostaat weefsel
weggegnomen. Deze “blinde” biopsie wordt alleen nog maar bij de prostaat gedaan. Zo
ondergaan bijvoorbeeld vrouwen met een mogelijke borstkanker gerichte weefselafname geleid
door goede beeldvorming.
De schrijver van dit proefschrift heeft zich daarom als doel gesteld, de huidige diagnostiek van
303
English Summary – Nederlandse Samenvatting – 14

prostaatkanker te verbeteren. Een “PARADIGMA SHIFT” creëren, is de enige weg vooruit!
Daarom wordt in dit proefschrift uitvoerig en nauwgezet ingegaan op de uitdagingen voor de
patiënt en hun artsen. Er wordt gezocht naar nieuwe technieken, deze worden gevalideerd en
vervolgens geïmplementeerd in de routine zorg. Het doel van dit proefschrift, was niet alleen om
te zien welke technieken leiden tot minder biopsie naalden met betere opbrengst maar ook een
verbetering in de representativiteit van meest agressieve component aangwezig in de tumor.
Dit proefschrift onderzoekt derhalve het pad van “van theorie tot praktijk”.
Samenvattend is het volgende gevonden:
In hoofdstuk 3 worden de haalbaarheid en de nauwkeurigheid van multi-parametrische MRI –
bestaande uit anatomische T2-gewogen beelden en functionele dynamische contrast en diffusie
MRI- onderzocht om voor tumor verdachte gebieden te identificeren. Er werd gebruik gemaakt
van een magneetveldsterkte van 3T en een 32-kanaals oppervlaktespoel. Ook werd gekeken of
deze biopten met een MR-compatibel biopsie apparaat genomen konden worden. Multi-
parametrische MRI bleek zeer nauwkeurig te zijn om prostaatkanker op te sporen. Bovendien
bleek de MR-geleide biopsie, gericht op de multi-parametrische MRI verdachte afwijking, goed
uitvoerbaar en waardevolle informatie op te leveren over de aanwezigheid van prostaatkanker.
Daarom zouden een aanzienlijk deel van de mannen met een verhoogd PSA een multi-
parametrisch onderzoek moeten ondergaan.
In hoofdstuk 4 wordt de in hoofdstuk 3 ontwikkelde techniek in een grotere patiëntengroep met
patiënten met een persisterend verhoogd PSA en minimaal 2 negatieve voorafgaande
echografische bioptie-sessies toegepast. Het doel was om te kijken bij hoeveel patiënten multi-
parametrische MRI en MR-biopsie, ondanks voorafgaande negatieve echo-biopsie, toch
prostaatkanker ontdekt kan worden. Bovendien werd gekeken, bij hoeveel patiënten er een
klinisch significante kanker aanwezig was (dat zijn kankers, die agressief zijn en dus behandeld
moet worden). Bij 40/ 68 (59%) patiënten werd prostaatkanker gevonden. Hiervan hadden er
37 (93%) een significant carcinoom. Ook werd gezien, dat de meeste tumoren buiten het gebied
van de echografisch biopsie lagen. Ook in een subgroep analyse –voor PSA waarde, prostaat
volume en PSA densiteit- bleek de MR-techniek significant betere resultaten op te leveren in
vergelijking met de echo-biopsie. Deze bevindingen onderstrepen de CBO-2007 richtlijn, dat
304
English Summary – Nederlandse Samenvatting – 14

patiënten met een blijvende klinisch verdenking op prostaatkanker na een negatieve echo-
biopsie een multi-parametrische MRI en MR-biopsie moeten ondergaan.
In hoofdstuk 5 werd de waarde van multi-parametrische MRI en MR-biopsie onderzocht bij
patiënten met een mogelijk recidief na een voorafgaande externe radiotherapiebehandeling.
Deze techniek had bij deze patiëntengroep een positief voorspellende waarde van 75% en bleek
ook hier succesvol te zijn.
Vooral het ontdekken en lokaliseren van kankers in de zogenaamde is een
uitdaging. Daarom werd in hoofdstuk 6 in een retrospectieve studie gekeken hoe nauwkeurig
multi-parametrische MRI is om de laaggradige (Gleason graad 2/3) en agressievere (Gleason
graad 4/5) kankers in de transitie zone op te kunnen sporen. Er werd gevonden dat de
anatomische T2-gewogen beelden het beste waren om dit te doen: de ervaren radioloog
ontdekte 86% van de agressieve carcinomen. Indien ook de functionele technieken (diffusie en
contrast) werden toegevoegd, nam de nauwkeurigheid maar weinig toe tot 91%. De laaggradige
tumoren werden echter met de T2-techniek slecht ontdekt (24%) en nam meer toe met de
functionele beeldvorming erbij (47%). De T2-gewogen techniek bleek dus een nauwkeurige
techniek te zijn om agressieve kankers in de transitie zone op te sporen.
De belangrijkste uitdaging is gelegen in het niet invasief nauwkeurig kunnen voorspellen of een
tumor niet significant of significant is. Tot nu toe blijkt dit met bestaande technieken niet goed
mogelijk. Daarom wordt in hoofdstuk 7 in de perifere zone van de prostaat de correlatie tussen
de apparent diffusion coefficient (ADC) waarden van 3T diffusie MRI met de Gleason gradering
in het operatiepreparaat onderzocht. Het bleek, dat de ADC waarden een omgekeerde correlatie
met de Gleason gradering vertoonde, en dat de ADC waarden van de laag-, intermediair- en de
hooggradige tumoren significant verschilden (p<0.001). Met de gemiddelde ADC waarde van een
bepaald gebied bleek het mogelijk te zijn, de laaggradige (niet significante) van de agressieve
(significante) tumoren te onderscheiden (AUC 0.90). Er werd daarom geconcludeerd, dat
diffusie MRI, gebruik makend van de ADC waarden een goede fenotypische biomarker is om niet
significante prostaatkaker van significante te onderscheiden.
In hoofdstuk 9 werd de waarde van een additionele functionele MRI-techniek, magnetic
305
English Summary – Nederlandse Samenvatting – 14

resonance spectroscopic imaging (MRSI) bij 3T onderzocht voor de differentiatie tussen laag en
hoger agressieve tumoren. Er werd een correlatie gevonden tussen de Gleason graad en de
Choline + Creatine over Citraat- en de Choline over Citraat ratio’s (AUC 0.70 en 0.74). De
correlatie tussen Cho+Cr/Cit en tumor agressie was significant. Ook werd de MRSI techniek
gestandaardiseerd teneinde deze in de praktijk beter te kunnen gebruiken. MRSI levert op grond
van dit onderzoek een extra mogelijkheid om de tumor agressie niet invasief met MRI te
bepalen.
Een belangrijk probleem is, dat de patiënten met een laaggradige tumor (Gleason 3+3) vaak
ondergegradeerd worden met het echo-biopt. Eigenlijk moeten deze patiënten een meer
agressieve behandeling ondergaan, echter de “fout lage” gradering leidt tot onderbehandeling.
Graag zouden we de “ware” Gleason 3+3 patiënten onderscheiden van die met een meer
agressieve tumor. Om de klinische waarde van diffusie MRI hiervoor te onderzoeken, zijn er 2
verschillende studies gedaan. De eerste studie, is een retrospectieve, beschreven in Hoofdstuk
8. De tweede in hoofdstuk 10. Bij 11/23 patiënten met op echo-biopsie uitslag van een
laaggradige tumor (Gleason score 3+3=6), liet het operatiepreparaat toch een agressievere
tumor zien. Deze patiënten (48%) hadden dus op de echo-biopsie een ondergradering. Diffusie
MRI liet een significant verschil zien in de groep van patiënten die met echografie
ondergradering toonden (11/23) versus die patiënten, die een terecht laag stadium hadden
(12/23). ROC analyse toonde een AUC van 0.88 voor de ADC waarde. Deze resultaten tonen aan,
dat diffusie MRI van grote klinische waarde is bij patiënten, bij wie de echo-biopsie een
laaggradige tumor (Gleason score ) aantoont. De ondergradering wordt dankzij multi-
parametrische MRI aanzienlijk gereduceerd. Daarom ZOU deze MRI techniek een onderdeel
MOETEN uitmaken bij patiënten met (de verdenking op ) prostaatkanker.
De bevindingen in hoofdstuk 10 vormen de kroon op dit proefschrift. Deze prospectieve studie
vergelijkt in 2 gelijkwaardige patiëntengroepen (matched-cohorts) de uitkomsten voor de
detectie van het meest agressieve tumor deel in het operatie preparaat met multi-parametrisch
MRI + MR-biopsie in de ene, en met echo-biopsie in de andere groep. Het bleek dat MR-biopsie
gericht op de meest afwijkende laesie op de multi-parametrische MRI superieur was. De MRI
methode liet in 95% een exacte overeenkomst zien met het operatiepreparaat voor wat betreft
het aantonen van de agressieve tumoren (hoogste Gleason graad). Bij het echo-biopt was dit
306
English Summary – Nederlandse Samenvatting – 14

slechts in 54% het geval. Bovendien waren met MRI slechts 3 naalden nodig voor de biopsie,
tegen 10 met het echo-biopt. Dit onderstreept, dat met MRI met minder naalden meer informatie
wordt verkregen, en daarom onderdeel moet uitmaken bij de diagnostiek van prostaatkanker.
In hoofdstuk 7 werd gezien, dat de gemiddelde waarde van de ADC voor de “normale” perifere
zone tussen patiënten variatie vertoont. Op grond daarvan kan verwacht worden, dat ook de
waarde van de tumor varieert. Deze inter-patiënt variatie kan nadelig werken op de voorspelling
van de tumor agressie. Daarom werd deze variatie in hoofdstuk 11 onderzocht. Inderdaad bleek
de ADC waarde voor normale perifere zone significant tussen patiënten te verschillen (p<0.001).
Dit is waarschijnlijk het gevolg van natuurlijke variatie in de fysiologie van de prostaat. Indien
voor deze “normale” variatie gecorrigeerd werd, bleek de voorspelling van de tumor agressie
significant te verbeteren (p=0.001). De ADC waarden moeten dus gezien worden tegen het licht
van de ”achtergrond” variatie van de “normale” prostaat.
In hoofdstuk 12 gaat in op het belangrijke aspect, hoe de multi-parametrische MRI bij de in de
radiologische praktijk algemeen geïmplementeerd kan worden. In dit proefschrift lijkt de multi-
parametrische MRI makkelijk toe te passen, maar de praktijk is weerbarstiger. Het kost de
beginnende radioloog moeite om de juiste beoordelingstechniek van de MRI-beelden te leren.
Om dit vergemakkelijken, en om de variatie tussen de radiologen bij de beoordeling te
reduceren is er een computer assisted diagnosis (CAD) techniek ontwikkeld en uitgetest. Deze
techniek maakt gebruik van de functionele parameters van contrast en diffusie MRI. Toevoeging
van CAD verbeterde de herkenning van prostaatkanker door de niet ervaren radioloog
significant voor zowel de perifere (p<0.001) als de transitie zone (p=0.001). Met gebruik van
CAD bereikte de niet ervaren radioloog (AUC 0.91) bijna het niveau van de expert radioloog.
(AUC 0.93).
In hoofdstuk 13 worden voorgaande hoofdstukken in verband gebracht en bediscussieerd. De
algehele conclusie is, dat met multi-parametrische MRI en MR-biopsie met minder naalden een
betere diagnose gesteld kan worden. Dat wil zeggen insignificante kanker kan worden
onderscheiden met deze techniek van de significante. De techniek is significant beter dan wat er
op dit moment –met de echo-biopsie- gedaan wordt.
307
English Summary – Nederlandse Samenvatting – 14

Toekomst-persopectieven:
1. Multi-parametrische MRI moet zo snel mogelijk worden geïmplementeerd. De
implementatie barrières moeten worden geïdentificeerd en overwonnen.
2. Er moet worden onderzocht, wat de waarde is van deze MRI techniek bij prostaatkanker
screening. Op grond van de bewijzen uit dit proefschrift, lijkt het aannemelijk dat
invoering van screening met PSA+ multi-parametrische MRI mogelijk en wenselijk is.
3. De rol van multi-parametriche MRI bij active survellance moet eveneens worden
gevalueerd.
4. De rol van MRI bij lokale therapie is eveneens veelbelovend. Immers met multi-
parametrische MRI kan de agressieve tumor component in kaart worden gebracht.
5. CAD zal leiden tot snellere implementatie van Multi-parametrische MRI en de kwaliteit
van de beoordeling verbeteren, echter er moet nog veel aan CAD ontwikkeld worden,
voordat iedereen dit kan gaan gebruiken.
6. De potentiële meerwaarde van hogere veldsterkten (bijvoorbeeld 7T) zal moeten
worden onderzocht.
Enkele slotopmerkingen:
Er zijn voldoende stenen verplaatst om de PARADIGMA SHIFT in de diagnostiek en de daarop
volgende behandeling te laten plaatsvinden. Het gedonder van de “Battle of Anghiari” is
hoorbaar. Laat deze oorlog uitdraaien op overwinning voor de patiënt met prostaatkanker, zijn
familie en zijn behandelaar.
Clinici, vergeet echter nooit het doel van ons werk en inspanningen:
atiënt is onze grootste roeping!
308
English Summary – Nederlandse Samenvatting – 14

Toekomst-persopectieven:
1. Multi-parametrische MRI moet zo snel mogelijk worden geïmplementeerd. De
implementatie barrières moeten worden geïdentificeerd en overwonnen.
2. Er moet worden onderzocht, wat de waarde is van deze MRI techniek bij prostaatkanker
screening. Op grond van de bewijzen uit dit proefschrift, lijkt het aannemelijk dat
invoering van screening met PSA+ multi-parametrische MRI mogelijk en wenselijk is.
3. De rol van multi-parametriche MRI bij active survellance moet eveneens worden
gevalueerd.
4. De rol van MRI bij lokale therapie is eveneens veelbelovend. Immers met multi-
parametrische MRI kan de agressieve tumor component in kaart worden gebracht.
5. CAD zal leiden tot snellere implementatie van Multi-parametrische MRI en de kwaliteit
van de beoordeling verbeteren, echter er moet nog veel aan CAD ontwikkeld worden,
voordat iedereen dit kan gaan gebruiken.
6. De potentiële meerwaarde van hogere veldsterkten (bijvoorbeeld 7T) zal moeten
worden onderzocht.
Enkele slotopmerkingen:
Er zijn voldoende stenen verplaatst om de PARADIGMA SHIFT in de diagnostiek en de daarop
volgende behandeling te laten plaatsvinden. Het gedonder van de “Battle of Anghiari” is
hoorbaar. Laat deze oorlog uitdraaien op overwinning voor de patiënt met prostaatkanker, zijn
familie en zijn behandelaar.
Clinici, vergeet echter nooit het doel van ons werk en inspanningen:
atiënt is onze grootste roeping!
308
English Summary – Nederlandse Samenvatting – 14


PART SIX
POSTLUDE


Postlude
A. LIST OF PUBLICATIONS
2012
1. Value of 3T multiparametric MR Imaging and MR guided biopsy for early risk re-
stratification in active surveillance of low-risk prostate cancer: a prospective
multicentre cohort study. C. Hoeks, D. Somford, T. Hambrock, C. Hulsbergen-van de
Kaa, J.O. Barentsz (Submitted)
2. Differentiation of Prostatitis and Prostate Cancer using Diffusion Weighted Imaging
and MR-guided Biopsy at 3T. M. Schouten, K. Nagel, B ten Haken, C. Hoeks, G. Litjens T.
Hambrock, J.O. Barentsz, J.J. Fütterer. Radiology (Accepted awaiting publication)
3. Evaluation of Diffusion-Weighted MR Imaging (DWI) at Inclusion in an Active
Surveillance Protocol for Low-Risk Prostate Cancer. D.M. Somford, C. M. Hoeks, C.A.
Hulsbergen-van de Kaa, T. Hambrock, J.J. Futterer, J. A. Witjes, C. H. Bangma, H. Vergunst,
G.A. Smits, J. R. Oddens, I.M. van Oort , J.O. Barentsz. Invest Radiol (Accepted awaiting
publication)
4. Computer-aided diagnosis of prostate cancer using multiparametric 3T MR
imaging : Effect on Observer Performance. Hambrock T, Vos P, Hulsbergen-van de
Kaa C, Barentsz J, Huisman HJ Radiology (Accepted awaiting publication)
5. The effect of inter-patient normal peripheral zone Apparent Diffusion Coefficient
variation on the Prediction of Prostate Cancer Aggressiveness. Litjens G, Hambrock
T, Barentsz JO, Huisman HJ. Radiology 2012 Oct 265 (1):260-3
6. MR Spectroscopy and Diffusion Weighted Imaging at 3T for in vivo Assessment of
Prostate Cancer Aggressiveness. Kobus T, Vos P, Hambrock T, Hulsbergen-van de Kaa
C, Barentsz JO, Scheenen T. Radiology. 2012 Nov;265(2):457-67
7. Simulated required accuracy of image registration tools for targeting high-grade
cancer components with prostate biopsies". Van de Ven W, Hulsbergen-van de Kaa C,
Hambrock T, Barentsz JO, Huisman HJ Eur Radiol. (Accepted awaiting publication)
310311

Postlude
8. 3T Magnetic Resonance-Guided Prostate Biopsy in Men with Increased PSA and
Repeated Negative Random Systematic Transrectal Ultrasound Biopsies: Detection
of Clinically Significant Prostate Cancers. Hoeks C, Schouten MG, Bomers JG,
Hoogendoorn SP, Hulsbergen-van de Kaa CA, Hambrock T, Vergunst H, Sedelaar JP,
Fütterer JJ, Barentsz JO. Eur Urol. 2012 Nov;62(5):902-9
9. Initial Experience With Identifying High-Grade Prostate Cancer Using Diffusion-
W
Schematic TRUS-Guided Biopsy: A Radical Prostatectomy Correlated Series.
Somford DM, Hambrock T, Hulsbergen-van de Kaa CA, Fütterer JJ, van Oort IM, van
Basten JP, Karthaus HF, Witjes JA, Barentsz JO. Invest Radiol. 2012 Mar;47(3):153-8.
10. Functional MRI techniques demonstrate early vascular changes in renal cell cancer
patients treated with sunitinib: a pilot study. Desar IM, ter Voert EG, Hambrock T, van
Asten JJ, van Spronsen DJ, Mulders PF, Heerschap A, van der Graaf WT, van Laarhoven
HW, van Herpen CM.Cancer Imaging. 2012 Jan 12;11:259-65.
11. Prospective Assessment of Prostate Cancer Aggressiveness using 3 Tesla Diffusion
Weighted MR Imaging Guided Biopsies versus a systematic 10-core Transrectal
Ultrasound Prostate Biopsy Cohort. Hambrock T, Hoeks C, Hulsbergen-van de Kaa C,
Scheenen J, Oort I, Fütterer JJ, Huisman H, Barentsz J. Eur Urol. 2012 Jan;61(1):177-84.
2011
12. Value of 3 Tesla Endorectal Coil Magnetic Resonance Imaging in Local Staging of
Prostate Cancer. Hamoen E, Hambrock T, Witjes J, Barentsz J (Submitted)
13. High-risk prostate cancer: value of multi-modality 3T MRI-guided biopsies after
previous negative biopsies. Fütterer JJ, Verma S, Hambrock T, Yakar D, Barentsz JO.
Abdom Imaging. 2011 Oct 29.
14. Prostate cancer: multiparametric MR imaging for detection, localization, and
staging. Hoeks CM, Barentsz JO, Hambrock T, Yakar D, Somford DM, Heijmink SW,
Scheenen TW, Vos PC, Huisman H, van Oort IM, Witjes JA, Heerschap A, Fütterer JJ.
Radiology. 2011 Oct;261(1):46-66. Review.
311312

Postlude
15. F-18 FDG PET/CT as a Crucial Guide Toward Optimal Treatmet Planning in a Case
of Postirradiation Sarcoma 10 Years after Primary Bone Lymphoma of the Pelvis.
de Rooy, JW, Hambrock T, Vriends D, Flucke UE, van der Geest IC, van de Luijtgaarden AC,
Schreuder BW, de Geus-Oei LF. Clin Nucl Med 2011 Jul; 36 (7): 565-7.
16. Relationship between apparent diffusion coeeffcients at 3.0-T MR imaging and
Gleason Grade in Peripheral Zone Prostate Cancer. . Hambrock T, Somford D,
Hoeks C, Hulsbergen-vandeKaa C, Scheenen T, Huisman HJ, van Oort I, Witjes JA,
Barentsz J. Radiology 2011 May; 259(2):453-61
17. In Vivo Assessment of Prostate Cancer Aggressiveness Using Magnetic Resonance
Spectroscopic Imaging at 3T with an Endorectal Coil. Kobus T, Hambrock T,
Hulsbergen-van de Kaa CA, Wrigth AJ, Barentsz JO, Heerschap A, Scheenen TW. Eur Urol.
2011 Nov;60(5):1074-80
18. Prostate cancer detection and dutasteride: utility and limitations of prostate-
specific antigen in men with previuos negative biopsies. Van Leeuwen PJ, Kölbe K,
Huland H, Hambrock T, Barentsz J, Schröder FH. Eur Urol 2011 Feb; 59(2): 183-190.
2010:
19. Magnetic Resonance Imaging guided prostate biopsy in men with repeat negative
biopsies and increased prostate specific antigen. Hambrock T, Somford DM, Hoeks C,
Bouwense SA, Huisman HJ, Yakar D, van Oort IM, Witjes JA, Fütterer JJ, Barentsz JO.
J Urol 2010 Feb;183(2):520-7.
20. Relationship of Apparent Diffusion Coefficient Values at 3T and prostate cancer
Gleason grades in the peripheral zone. Hambrock T, Somford D, Hoeks C, Hulsbergen-
vandeKaa C, Scheenen T, Huisman HJ, van Oort I, Witjes JA, Barentsz J. Radiology. 2011
May;259(2):453-61
21. Feasibility of 3T Dynamic Contrast-Enhanced Magnetic Resonance-Guided Biopsy
in Localizing Local Recurrence of Prostate Cancer after External Beam Radiation
Therapy. Yakar D, Hambrock T, Huisman H, Hulsbergen-van de Kaa CA, van Lin E,
Vergunst H, Hoeks CM, van Oort IM, Witjes JA, Barentsz JO, Fütterer JJ. Invest Radiol. 2010
Mar ;45(3):121-5.
312313

Postlude
2009:
22. Automated calibration for computerized analysis of prostate lesions using
pharmacokinetic magnetic resonance images. Vos P, Hambrock T, Barentsz J,
Huisman HJ. MICCAI 2009, September 20-24, 2009, Proceedings, Part II, Volume
5761/2009, p 836-843
2008:
23. Magnetic Resonance Imaging guided biopsies of the prostate: Technique,
feasibility and clinical applications. Yakar D, Hambrock T, Hoeks C, Barentsz JO,
Fütterer JJ. Top Magn Reson Imag. 2008 Dec;19(6):291-5
24. Diffusion and Perfusion MR imaging of the Prostate. Somford DM, Futterer JJ,
Hambrock T, Barentsz JO. Magn Reson Imaging Clin N Am. 2008 Nov;16(4):685-95.
25. MR-Guided Biopsy of the Prostate: An Overview of Techniques and a Systematic
Review. Pondman KM, Fütterer JJ, Ten Haken B, Schultze Kool LJ, Witjes JA, Hambrock T,
Macura KJ, Barentsz JO. Eur Urol. 2008 Sep;54(3):517-27
26. 32-Channel Coil 3T MR Guided Biopsies of Prostate Tumor Suspicious Regions
Identified on Multi-Modality 3T MR Imaging Technique and Feasibility.
Hambrock T, Futterer J, Huisman H, Oort I, Witjes J, Van Basten J,Barentsz J; Invest
Radiology 2008 Oct;43(10):686-94.
27. Computerized analysis of prostate lesions in the peripheral zone using dynamic
contrast enhanced MRI. Vos P, Hambrock T, Hulsbergen-vandeKaa C, Futterer J,
Barentsz J, Huisman J; Med Phys. 2008 Mar;35(3):888-99
2007:
28. Local Staging of Prostate Cancer using Endorectal Coil MR Imaging. Hambrock T,
Barentsz JO, Futterer JJ. Cancer Imaging Vol. II : Instrumentation and Applications,
H.M. Hayat (Editor), Acad. Press, Ch. 46 p.641 655
313314

Postlude
29. Prostate cancer: body-array versus endorectal coil MR imaging at 3T
comparison of image quality, localization and staging performance. Heijmink SW,
Futterer JJ, Hambrock T, Huisman HJ, Hulsbergen-Van deKaa CA, Knipscheer BC,
Kiemeney LA, Witjes JA, Barentsz JO. Radiology 2007 Jul;244(1):184- 95.
2006:
30. Dynamic Contrast Enhanced MR Imaging in the Diagnosis and Management of \
Prostate Cancer. Hambrock T, Padhani A, Tofts P, Vos P, Huisman H, Barentsz JO.
Categorical Course in Genitourinary Imaging, RSNA 2006.
2002:
31. Screening for Chilhood Anemia using Coppersulfate Densitometry. Funk M,
Hambrock T, van Niekerk GC, Wittenberg DF. S Afr Med J 2002. Dec;92(12):978-82.
314315

Postlude
B. LIST OF PRESENTATIONS SCIENTIFIC PAPER PRESENTATIONS
1. 2011 Oct International Cancer Imaging Society Kopenhagen, Denmark:
"The Value of MR guided Biopsies in Prostate Cancer”
2. 2010 Mar Society of Computed Body Tomography and MR San Diego, U.S.A
"Correlation between 3T DWI-ADC and tumor Gleason score in Prostatectomy Specimens”
3. 2010 Mar European Society of Radiology Vienna, Austria:
"Concordance between MR-guided biopsy determined Gleason Score and Prostatectomy GS”
4. 2010 Mar European Society of Radiology Vienna, Austria:
"Correlation between 3T DWI-ADC and tumor Gleason score in Prostatectomy Specimens”
5. 2008 Dec Radiological Society of North America annual meeting Chicago, U.S.A :
The Value of 3 Tesla Magnetic Resonance Imaging Guided Prostate Biopsies in Men with
Repetitive Negative Biopsies an elevated PSA
6. 2008 Oct Nederlandse Radiologendagen Rotterdam, Netherlands:
Effect van Computer-Aided Diagnosis op de Karakterisatie van Prostaat Laesies op Dynamische
Contrast MRI
7. 2008 Oct Nederlandse Radiologendagen Rotterdam, Netherlands :
Waarde van MR Geleide Bioptie van de Prostaat op 3 Tesla
8. 2008 Oct International Cancer Imaging Society annual meeting Bath, England :
Correlation between 3T DWI-ADC and tumor Gleason Score in Prostatectomy specimens
9. 2008 Oct International Cancer Imaging Society annual meeting Bath, England :
Effect of Computer Assisted Diagnosis to characterized prostate tumor suspicious regions on
DCE-MRI
10. 2008 Oct International Cancer Imaging Society annual meeting Bath, England:
DCE-MRI & MR Guided Biopsy for Detection of Prostate Cancer Recurrence following
Radiotherapy”
315316

Postlude
11. 2008 Oct International Cancer Imaging Society annual meeting Bath, England:
The Value of 3 Tesla Magnetic Resonance Imaging Guided Prostate Biopsies in Men with
Repetitive Negative Biopsies an elevated PSA
12. 2008 Sep European Society of Uroradiology annual meeting Munic, Germany:
The Value of 3 Tesla Magnetic Resonance Imaging Guided Prostate Biopsies in Men with
Repetitive Negative Biopsies an elevated PSA
13. 2008 Sep European Society of Uroradiology annual meeting Munic, Germany:
Correlation between 3T MRI Apparent Diffusion Coefficient Values and Prostate Cancer Gleason
Score in Prostatectomy Specimen
14. 2007 Jun International Society of Magnetic Resonance in Medicine / European
Society of Magnetic Resonance in Medicine and Biology joint meeting Berlin, Germany
“32-Ch MR Guided Biopsy of tumor suspicious regions on multi-modality 3T MRI of the prostate
– Initial Experience”
15. 2007 Apr European Society of Uroradiology (ESUR) / Society of Uroradiology
(SUR) joint annual meeting Bonita Springs, U.S.A.
“32-Channel MR Guided Biopsy of tumor suspicious regions on multi-modality 3T MR imaging of
the prostate – Initial Experience”
16. 2006 Nov Radiological Society of North America (RSNA) meeting Chicago, U.S.A
-mapping vs T2* mapping of prostate cancer lesions : Elektronic poster presentation
316317

Postlude
C. LIST OF PRESENTATIONS PRESENTATIONS ON INVITATION
1. 2012 Oct Radiologendagen
“MRI van de prostaat: Pro en contra”
2. 2012 May Oncology 2.0 Apeldoorn, Netherlands:
“The Value of MRI prior to Radical Prostatatcomy”
3. Feb 2012 Pathologie Onderwijs St. Radboud, Nijmegen
“De waarde MRI bij prostaatkanker diagnostiek”
4. Sept 2011 Kernspintomografie Fortbildung – Münster, Germany
5. Jul 2011 Radiologen Fortbildungscongress Düsseldorf, Germany
6. Jun 2011 Urologen Fortbildungscongress Zürich, Switserland
7. Okt 2010 - Patient Prostata Krebs Selbshifegruppe Düsseldorf, Germany
“The value of MRI in screening and detection of prostate cancer“
8. 2008 Jan - Abteilung Radiologie/Urologie/Radiotherapie Vienna, Austria
“The value of MRI in screening and detection of prostate cancer“
9. 2007 Nov - Afdeling Radiologie/Urologie Hirslanden Hospital, Zürich, Zwitserland
“The role of Magnetic Resonance Imaging in the diagnosis and management of prostate cancer”
10. 2007 Aug Afdeling Urologie UMCN St. Radboud Nijmegen
"De rol van MRI in de diagnostiek en behandeling van prostaatkanker”
317318

Postlude
D. LIST OF AWARDS
2010:
1. Lauterbur Award from the Society of Computed Body Tomography and Magnetic Resonance (SCBT-MR), San Diego, U.S.A for best MR paper entitled:
"Scientific presentation on Correlation of 3T DWI-ADC and prostate cancer Gleason Score”
2008 :
2. First Prize Award from the International Cancer Imaging Society (ICIS) Bath, United Kingdom for best paper entitled:
"Scientific presentation on Correlation of 3T DWI-ADC and prostate cancer Gleason Score”
3. Cum Laude Award from the Society of Computed Body Tomography and Magnetic
Resonance (SCBT-MR), Charleston, U.S.A (presented by Prof.dr.J.O.Barentsz) for:
"Scientific Presentation on MR imaging guided biopsy of the prostate at 3T using a 32- channel phased array coil"
2007 :
4. First Prize Award from the Society of Urogenital Radiology and European Society of Urogenital Radiology, Bonita Springs, U.SA. for best scientific paper entitled: "Scientific Presentation on MR imaging guided biopsy of the prostate at 3T using a 32- channel
phased array coil"
318319

Postlude
E. CURRICULUM VITAE
Thomas Hambrock werd geboren onder heldere Afrika zon op de eerste dag van lente in het
zuidelijke halfrond. Dit was op 1 september 1978 in Pretoria, Zuid-Afrika. Hij groeide in een
bijzonder liefdevolle gezin op en woonde met zijn ouders Eckehard en Karin alsook zijn twee
broers Norbert en Bernard in het dorp Vereeniging. Met 5 jarige leeftijd besloot hij arts te
worden. Zijn interesses in de wetenschap, onderzoek en avontuur zijn op verscheidene
manieren door zijn liefdevolle ouders gestimuleerd. Achter zijn Zeiss microscoop, zijn
chemie experiment set, zijn edelgesteente, munt, postzegel en fossiel verzameling alsook
jagen met zijn luchtgeweer heeft hij veel uren van zijn jongen leven verbracht. Zijn latere
leven was gekenmerkt door wandeltochten met rugsak, tent en slaapzak in de
Drakensbergen van Zuid-Afrika. Zijn grootste hobby is en blijft het intensief bestuderen van
de geschiedenis en genealogie van zijn familie. Zowel zijn basisschool opleiding (bij
Laerskool Vryheidsmonument) alsook zijn middelbare schoolopleiding (bij Hoërskool
Vereeniging) werd in Vereeniging met succes afgerond. Vanaf 1997-2002 studeerde hij
geneeskunde aan de Universiteit van Pretoria, Zuid-Afrika waar hij ook zijn artsen beul, Cum
Laude heeft behaald. Dezelfde rusteloosheid en zin in avontuur die ooit zijn 72 voorouders
heeft gedreven om hun tuiste in Europa achter te laten, heeft hem weer terug naar Europa
gebracht. Hij werkte in totaal 3 jaar als arts in de Verenigde Koninkrijken, eerst binnen de
heelkunde in Stoke-on-Trent (Engeland), dan interne geneeskunde in Bangor (Wales).
Vervolgens werkte hij in Kirckaldy en Dunfermline (Schotland), eerste binnen de
kindergeneeskunde en dan binnen de spoedeisende hulp. In 2005 verhuisde hij opnieuw, dit
keer naar Nederland waar hij een bijzondere PhD onderzoek bij de gerenommeerde prostaat
centrum in Nijmegen, onder leiding van Prof. Barentsz, kon beginnen. Vanaf oktober 2009 is
hij in opleiding tot radioloog bij het Universitair Medisch Centrum St. Radboud, Nijmegen,
Nederland. Op 29 maart 2012 trouwde hij in Zwitserland met de vrouw van zijn dromen,
Nadia.
319
E. CURRICULUM VITAE
Thomas Hambrock werd geboren onder de heldere Afrika zon, op de eerste dag van lente in het
zuidelijke halfrond. Dit was op 1 september 1978 in Pretoria, Zuid-Afrika. Hij groeide in een
bijzonder liefdevolle gezin op en woonde met zijn ouders Eckehard en Karin alsook zijn twee
broers Norbert en Bernard in het dorp Vereeniging. Met 5 jarige leeftijd besloot hij arts te
worden. Zijn interesses in de wetenschap, onderzoek en avontuur zijn op verscheidene
manieren door zijn liefdevolle ouders gestimuleerd. Achter zijn Zeiss microscoop, zijn chemie
experiment set, zijn edelgesteente, munt, postzegel en fossiel verzameling alsook jagen met zijn
luchtgeweer heeft hij veel uren van zijn jongen leven verbracht. Zijn latere leven was
gekenmerkt door wandeltochten met rugsak, tent en slaapzak in de Drakensbergen van Zuid-
Afrika. Zijn grootste hobby is en blijft het intensief bestuderen van de geschiedenis en genealogie
van zijn familie. Zowel zijn basisschool opleiding (bij Laerskool Vryheidsmonument) alsook zijn
middelbare schoolopleiding (bij Hoërskool Vereeniging) werd in Vereeniging met succes
afgerond. Vanaf 1997-2002 studeerde hij geneeskunde aan de Universiteit van Pretoria, Zuid-
Afrika waar hij ook zijn artsen beul, cum laude heeft behaald. Dezelfde rusteloosheid en zin in
avontuur die ooit zijn 72 voorouders hebben gedreven om hun tuiste in Europa achter te laten,
hebben hem weer terug naar Europa gebracht. Hij werkte in totaal 3 jaar als arts in de Verenigde
Koninkrijken, eerst binnen de heelkunde in Stoke-on-Trent (Engeland), dan interne
geneeskunde in Bangor (Wales). Vervolgens werkte hij in Kirckaldy en Dunfermline (Schotland),
eerst binnen de kindergeneeskunde en dan binnen de spoedeisende hulp. In 2005 verhuisde hij
opnieuw, dit keer naar Nederland waar hij een bijzondere PhD onderzoek bij het gerenommeerd
prostaat centrum in Nijmegen, onder leiding van Prof. Barentsz, kon beginnen. Vanaf oktober
2009 is hij in opleiding tot radioloog bij het Universitair Medisch Centrum St. Radboud,
Nijmegen, Nederland. Op 29 maart 2012 trouwde hij in Zwitserland met de vrouw van zijn
dromen, Nadia.
320
E. CURRICULUM VITAE
Thomas Hambrock werd geboren onder de helder Afrika zon, op de eerste dag van lente in het
zuidelijke halfrond. Dit was op 1 september 1978 in Pretoria, Zuid-Afrika. Hij groeide op in een
bijzonder liefdevolle gezin en woonde met zijn vader Eckehard en moeder Karin alsook zijn twee
broers: Norbert en Bernard, in het dorp Vereeniging. Met 5 jarige leeftijd besloot hij arts te
worden. Zijn interesses in de wetenschap, onderzoek en avontuur zijn op verschillende wijzen
door zijn ouders gestimuleerd. Achter zijn Zeiss microscoop, zijn chemie experiment set, zijn
edelgesteente, munt, postzegel en fossiel verzameling alsook jagen met zijn luchtgeweer, heeft
hij veel uren van zijn jongen leven verbracht. Zijn latere leven was gekenmerkt door
wandeltochten met rugzak, tent en slaapzak in de Drakensbergen van Zuid-Afrika. Zijn grootste
hobby is en blijft het intensief bestuderen van de geschiedenis en genealogie van zijn familie.
Zowel zijn basisschool opleiding (aan de Laerskool Vryheidsmonument) alsook zijn
middelbare schoolopleiding (aan de Hoërskool Vereeniging) werd met succes afgerond. Vanaf
1997-2002 studeerde hij geneeskunde aan de Universiteit van Pretoria, Zuid-Afrika waar hij ook
zijn artsen beul, cum laude heeft behaald. Dezelfde rusteloosheid en zin in avontuur die ooit zijn
72 voorouders hebben gedreven om hun tuiste in Europa achter te laten, hebben hem weer
terug naar Europa gebracht. Hij werkte in totaal 3 jaar als arts in de Verenigde Koninkrijken.
Eerst binnen de heelkunde in Stoke-on-Trent (Engeland), dan interne geneeskunde in Bangor
(Wales). Vervolgens werkte hij in Kirckaldy en Dunfermline (Schotland), eerst binnen de
kindergeneeskunde en dan binnen de spoedeisende hulp. In 2005 verhuisde hij opnieuw, dit
keer naar Nederland, waar hij een bijzondere PhD onderzoek kreeg bij het gerenommeerd
prostaat centrum in Nijmegen, onder leiding van Prof. Barentsz. Vanaf oktober 2009 is hij in
opleiding tot radioloog aan het Universitair Medisch Centrum St. Radboud, Nijmegen, Nederland.
Op 29 maart 2012 trouwde hij in Zwitserland met de vrouw van zijn dromen, Nadia.

Postlude
E. DANKWOORD
Hoewel het dankwoord vaak de eerste en ook enige is wat mensen ooit in een proefschrift
lezen, zo heeft het dankwoord to grote belang. Een proefschrift is nooit het werk van een
mens. Veel, veel mensen hebben direct of indirect hiertoe bijgedragen. Het is dus van cruciaal
belang erkenning te geven aan die wie erkenning toekomt.
Indien ik moet terugkijken op mijn tijd als onderzoeker en ja, zelf terug op het leven zo kan ik
niet anders dan dezelfde woorden gebruiken die mijn betovergrootvader, H.W. Stumpf
(1841-1920) ooit schreef over zijn eigen leven:
“An mir und meinem Leben ist nichts auf dieser Erd. Was Christus mir gegeben, das ist des Dankes wert!”
Ein ganz besonderen Dank richte ich euch mein lieber Vater und Mutter. Eure besondere
Fürsorge, Liebe, Geduld und Unterstützung durch die Jahre hindurch haben mich mein Leben
begleitet. Wäre ist nicht für euer Einsatz und vor allem die Motivation um das Beste aus uns
heraus zu fordern, wäre es mir niemals gelungen zu erreichen was ich hab. In gute und
schlechte Zeiten wart ihr immer da als Stützen. Ein ewiger Dank.
An meine Brüdern, Norbert und Bernard. Ihr seid die Säulen in meinem Leben. Ich konnte
immer auf eure Hilfe und Unterstützung rechnen. Vor allem haben eure Gebete mich stets
wieder neue Kraft verliehen. Ihr seid nicht nur meine Brüder, ihr seid auch meine besten
Freunde. Unser unerschütterlicher Glaube in Gott ist ein weiterer Band der unsere Familie
zusammen hält.
Geachte Prof. Barentsz, beste Jelle. Het is uiterst moeilijk te beginnen om mijn dank aan jou
uit te spreken. Jij bent de grootste inspiratie voor mijn proefschrift geweest. Jouw passievolle
liefde voor jouw prostaatkanker werk en je buitengewone gave om met mensen om te gaan
zijn voor vele een bijzondere motivatie. Je hebt niet alleen de ziekte voor ogen maar je ziet
telkens de mens achter de ziekte. Zonder jouw motivatie zou dit proefschrift nooit tot stand
gekomen zijn. Dank, dat ik je niet alleen als hoogleraar, promotor maar ook als vriend mag
waarderen. In de donkerste tijden was jij altijd een helpende hand. Ik zie er na uit, dat wij in
de toekomst nog een lange weg samen zullen volgen in de grote strijd om prostaatkanker.
Beste Henkjan, van dag een, toen ik nog geen Nederlands sprak tot aan het einde was je er
altijd geweest. Jouw perfectionisme, kritische en vooral scherpe ideeën zijn in al mijn
320
E. DANKWOORD
Hoewel het dankwoord vaak de eerste en ook enige is wat mensen ooit in een proefschrift lezen,
zo heeft het dankwoord toch grote belang. Een proefschrift is nooit het werk van een mens.
Bijzonder veel mensen hebben direct of indirect hieraan bijgedragen. Het is dus van cruciaal
belang erkenning te geven aan die wie erkenning toekomt. Indien ik moet terugkijken op mijn
tijd als onderzoeker en ja, zelf terug op het leven, zo kan ik niet anders dan dezelfde woorden
uitspreken die mijn betovergrootvader, H.W. Stumpf (1841-1920) ooit schreef over zijn eigen
leven:
“An mir und meinem Leben ist nichts auf dieser Erd. Was Christus mir gegeben, das ist des Dankes
wert!”
Ein ganz besonderen Dank sage ich euch, mein lieber Vater und meine Mutter. Eure besondere
Fürsorge, Liebe, Geduld und Unterstützung durch die Jahre hindurch, haben mir in meinem Leben
eine besondere Stärke verliehen. Wäre ist nicht für euer Einsatz und vor allem die Motivation um
das Beste aus uns heraus zu fordern, wäre es mir niemals gelungen zu erreichen was ich hab. In
guten und schlechten Zeiten wart ihr immer da, als Stützen. Ein ewiger Dank.
An meinen Brüdern, Norbert und Bernard. Ihr seid die Säulen in meinem Leben. Ich konnte immer
auf eure Hilfe und Unterstützung rechnen. Vor allem haben eure Gebete mich stets wieder neue
Kraft verliehen wenn diese Doktorarbeit, sich lange hinaus gezögert hat. Ihr seid nicht nur meine
Brüder, ihr seid auch meine besten Freunde. Unser unerschütterlicher Glaube in Gott ist ein
wichtiger Band der unsere Familie zusammen hält.
Geachte Prof. Barentsz, beste Jelle. Het is uiterst moeilijk te beginnen om mijn dank aan jou uit te
spreken. Jij bent de grootste inspiratie voor mijn proefschrift geweest. Jouw passievolle liefde
voor jouw prostaatkanker werk en je buitengewone gave om met mensen om te gaan, zijn voor
vele een bijzondere motivatie. Je hebt niet alleen de ziekte voor ogen maar je ziet telkens de
mens achter de ziekte. Zonder jouw motivatie zou dit proefschrift nooit tot stand gekomen zijn.
Dank, dat ik je niet alleen als hoogleraar, promotor maar ook als vriend mag waarderen. In de
donkerste tijden was jij altijd een helpende hand. Ik zie er na uit, dat wij in de toekomst nog een
lange weg samen zullen volgen in de grote strijd tegen prostaatkanker.
Beste Henkjan, van dag een, toen ik nog geen Nederlands sprak tot aan het einde was je er altijd
geweest. Jouw perfectionisme, kritische en vooral scherpe ideeën zijn in al mijn artikelen terug
te vinden. De wereld heeft te weinig onderzoekers van jouw kwaliteit. Ik kan zonder twijfel
toegeven dat mijn proefschrift veel, veel magerder en oninteressanter geweest zou zijn, had jij
321
E. DANKWOORD
Hoewel het dankwoord vaak de eerste en ook de enige is wat mensen ooit in een proefschrift
lezen, zo heeft het dankwoord toch grote belang. Een proefschrift is nooit het werk van een
mens. Bijzonder veel mensen hebben direct of indirect hieraan bijgedragen. Het is dus van
cruciaal belang, erkenning te geven aan die wie erkenning toekomt. Indien ik moet terugkijken
op mijn tijd als onderzoeker en ja, zelf terug op het leven, zo kan ik niet anders dan dezelfde
woorden uitspreken die mijn betovergrootvader, H.W. Stumpf (1841-1920) ooit schreef over
zijn eigen leven:
“An mir und meinem Leben ist nichts auf dieser Erd. Was Christus mir gegeben, das ist des Dankes
wert!”
Ein ganz großen Dank sage ich euch, mein lieber Vater und meine Mutter. Eure besondere
Fürsorge, Liebe, Geduld und Unterstützung durch die Jahre hindurch, haben mir in meinem Leben
eine besondere Stärke verliehen. Wäre ist nicht für euer Einsatz und vor allem die Motivation um
das Beste aus uns heraus zu fordern, wäre es mir niemals gelungen zu erreichen was ich hab. In
guten und schlechten Zeiten wart ihr immer da, als Stützen. Ein ewiger Dank.
An meinen Brüdern, Norbert und Bernard. Ihr seid die Säulen in meinem Leben. Ich konnte immer
auf eure Hilfe und Unterstützung rechnen. Vor allem haben eure Gebete mich stets wieder neue
Kraft verliehen wenn diese Doktorarbeit, sich lange hinaus gezögert hat. Ihr seid nicht nur meine
Brüder, ihr seid auch meine besten Freunde. Unser unerschütterlicher Glaube hält uns zusammen.
Geachte Prof. Barentsz, beste Jelle. Het is uiterst moeilijk te beginnen om mijn dank aan jou uit te
spreken. Jij bent de grootste inspiratie voor mijn proefschrift geweest. Jouw passievolle liefde
voor prostaatkanker diagnostiek en je buitengewone gave om met mensen om te gaan, zijn voor
vele een echte motivatie. Je hebt niet alleen de ziekte voor ogen maar je ziet telkens de mens
achter de ziekte en wat je altijd deed was voor de patiënt en niet voor jezelf. Zonder jouw
inspiratie zou dit proefschrift nooit tot stand gekomen zijn. Dank, dat ik je niet alleen als
hoogleraar, promotor, maar ook als vriend mag waarderen. In de donkerste tijden was jij altijd
een helpende hand. Ik zie er na uit, dat wij in de toekomst nog een lange weg samen zullen
volgen in de grote strijd tegen prostaatkanker.
Beste Henkjan, van dag een, toen ik nog geen Nederlands sprak tot aan het einde was je er altijd
geweest en door jouw verdiensten, was de KWF aanvraag waarop ik kon promoveren, tot stand
gekomen. Jouw perfectionisme, kritische en vooral scherpe ideeën zijn in al mijn artikelen terug
te vinden. De wereld heeft te weinig onderzoekers van jouw kwaliteit. Ik kan zonder twijfel
toegeven dat mijn proefschrift veel, veel magerder en oninteressanter geweest zou zijn, had jij

Postlude
artikelen terug te vinden. De wereld heeft te weinig onderzoekers van jouw kwaliteit. Ik kan
zonder twijfel toegeven dat mijn proefschrift veel, veel magerder en oninteressanter geweest
zou zijn, had jij niet de kwaliteit omhoog gedreven. Jij moest vaak achter mij aanzetten om
mijn artikelen uiteindelijk af te ronden. Ik denk dat jij trots kunt zijn. Het is uiteindelijk
allemaal goed gelukt.
Beste Christina. Wij hebben vele, vele uren samen achter de microscoop gezeten om
prostaten te bekijken. Hoewel je veel moeite en tijd heb geofferd hiervoor, had je dit altijd
met grote bereidwilligheid en vreugde gedaan. Bedankt hiervoor. Zonder aarzelen kan ik
zeggen dat jij de beste prostaat patholoog bent die ik ken. Helaas is klonen nog geen
mogelijkheid. Jouw enthousiasme voor de pathologie heeft mij ook geraakt. Ik kan eerlijk
zeggen dat indien de mooiste richting binnen de geneeskunde (radiologie natuurlijk) niet
bestond en ik ook niet kleurblind was, was ik direct patholoog geworden.
Beste Tom, alias Tomaso. Onze wegen kruisten al vroeg. Eerst in Praag en toen als buur
kamergenoten in het F.C. Donders instituut. Jij bent een onuitputbaar kennis van MRI
techniek en Fysica. Jij hebt mij bijna alles geleerd wat ik over MRI weet. Ik besef dat het
dagelijkse lastig vallen met mijn vragen over dit en dat, zeer zeker uitputbaar voor jou was.
Het was onontbeerlijk voor mij en daardoor kon ik zelf achter the scanner aan de slag. Dus
indirect heb jij vele patiënten geholpen.
Beste Pieter, alias Pietro. Dit proefschrift was absoluut niet gelukt zonder jou vele, vele uren
werk in MRCAD. Wij hebben samen duizenden uren verbracht om alles goed te krijgen. De
kroon van onze harde werk is zonder meer onze laatste artikel in Radiology (hoofdstuk 12).
Hier komt alle eer jou ook toe. Bedankt voor alle gezellige tijden en grappen. Hoop dat wij nog
in de toekomst samen kunnen werken aan projecten en ook buiten werk verband kunnen
blijven verkeren.
Beste Ritse. Ik moet eerlijk toegeven dat mijn Nederlandse woordenschat voor 80% van jouw
afkomstig is. Als (gezellige) kamergenoot moest je vele onderbrekeningen en vragen vanuit
mijn kant verdragen zodat ik de Nederlandse taal wat onder beheer kon krijgen. Wij hebben
vele leuke gesprekken: van de samenstelling van het atoom, beklimmen van Mount Everest,
tot de zin van het leven, bij een glaasje bier in de Esculaaf gehad. Ik verlang naar deze tijden.
Beste Monique. Jij was de derde persoon in onze onderzoekers kamer. Jij bent een echt
bijzonder mens en jouw uitgesproken vermogen tot efficiënte multi-tasking heeft mij sterk
321
niet de kwaliteit omhoog gedreven. Jij moest vaak achter mij aanzetten om mijn artikelen
uiteindelijk af te ronden. Ik denk dat jij trots kunt zijn. Het is uiteindelijk allemaal goed gelukt.
Beste Christina. Wij hebben vele, vele uren samen achter de microscoop gezeten om prostaten te
bekijken. Hoewel je veel moeite en tijd heb geofferd hiervoor, had je dit altijd met grote
bereidwilligheid en vreugde gedaan. Bedankt hiervoor. Zonder aarzelen kan ik zeggen dat jij de
beste prostaat patholoog bent die ik ken. Helaas is klonen nog geen mogelijkheid. Jouw
enthousiasme voor de pathologie heeft mij ook geraakt. Ik kan eerlijk zeggen dat indien de
mooiste richting binnen de geneeskunde (radiologie natuurlijk) niet bestond en ik ook niet
kleurblind was, was ik wel patholoog geworden.
Beste Tom, alias Tomaso. Onze wegen kruisten al vroeg. Eerst in Praag en toen als buurmannen
in het F.C. Donders instituut. Jij bent een onuitputbaar kennis van MRI techniek en fysica. Jij hebt
mij bijna alles geleerd wat ik over MRI weet. Ik besef dat het dagelijkse lastig vallen met mijn
vragen over dit en dat, zeer zeker uitputbaar voor jou was geweest. Het was onontbeerlijk voor
mij en daardoor kon ik zelf makkelijker achter the scanner aan de slag. Dus indirect heb jij vele
patiënten geholpen.
Beste Pieter, alias Pietro. Dit proefschrift was absoluut niet gelukt zonder jou vele, vele uren
werk in MRCAD. Wij hebben samen duizenden uren verbracht om alles goed te krijgen. De kroon
van onze harde werk is zonder meer onze laatste artikel in Radiology (hoofdstuk 12). Hier komt
alle eer jou ook toe. Bedankt voor alle gezellige tijden en grappen. Hoop dat wij nog in de
toekomst samen kunnen werken aan projecten en ook buiten werk verband, kunnen blijven
verkeren.
Beste Ritse. Ik moet eerlijk toegeven dat mijn Nederlandse woordenschat voor 80% van jouw
afkomstig is. Als (gezellige) kamergenoot moest je vele onderbrekingen en vragen vanuit mijn
kant verduren zodat ik de Nederlandse taal wat onder beheer kon krijgen. Wij hebben vele
leuke gesprekken bij een glaasje bier in de Esculaaf gehad: van de samenstelling van het atoom,
beklimmen van Mount Everest, tot de zin van het leven. Ik verlang naar deze tijden.
Beste Monique. Jij was de derde persoon in onze onderzoekers kamer. Jij bent een echt bijzonder
mens en jouw uitgesproken vermogen tot efficiënte multi-tasking heeft mij sterk onder de
indruk gebracht. Ik denk dat jij een van de weinige uitstekende arts-onderzoeker-moeder
combinaties maakt. Je zult zonder twijfel een succes van je toekomstige leven maken.
Beste Caroline. Jij kwam wat later in mijn onderzoekers tijd erbij. Van alle prostaat onderzoekers
is jij beslist de meest enthousiaste en kundige op dit gebied. Jouw creativiteit en kennis bij het
322
niet de kwaliteit omhoog gedreven. Jij moest vaak achter mij aanzetten om mijn artikelen
uiteindelijk af te ronden. Ik denk dat jij trots kunt zijn. Het is uiteindelijk allemaal goed gelukt.
Beste Christina. Wij hebben vele, vele uren samen achter de microscoop gezeten om prostaten te
bekijken. Hoewel je veel moeite en tijd heb geofferd hiervoor, had je dit altijd met grote
bereidwilligheid en vreugde gedaan. Bedankt hiervoor. Zonder aarzelen kan ik zeggen dat jij de
beste prostaat patholoog bent die ik ken. Helaas is klonen nog geen mogelijkheid. Jouw
enthousiasme voor de pathologie heeft mij ook geraakt. Ik kan eerlijk zeggen dat indien de
mooiste richting binnen de geneeskunde (radiologie natuurlijk) niet bestond en ik ook niet
kleurblind was, was ik wel patholoog geworden.
Beste Tom, alias Tomaso. Onze wegen kruisten al vroeg. Eerst in Praag en toen als buurmannen
in het F.C. Donders instituut. Jij bent een onuitputbaar bron van kennis: van MRI techniek en
fysica. Jij hebt mij bijna alles geleerd wat ik over MRI weet. Ik besef dat het dagelijks lastig vallen
met mijn vragen over dit en dat, zeer zeker uitputtend voor jou was geweest. Het was
onontbeerlijk voor mij en daardoor kon ik zelf makkelijker achter the scanner aan de slag. Dus
indirect heb jij vele patiënten geholpen.
Beste Pieter, alias Pietro. Dit proefschrift was absoluut niet gelukt zonder jou vele, vele uren
werk in MRCAD. Wij hebben samen honderden uren verbracht om alles goed te krijgen. De
kroon van onze harde werk is zonder meer onze laatste artikel in Radiology (hoofdstuk 12). Hier
komt alle eer jou ook toe. Bedankt voor alle gezellige tijden en grappen. Hoop dat wij nog in de
toekomst samen kunnen werken aan projecten en ook buiten werk verband, kunnen blijven
ontmoeten.
Beste Ritse. Ik geef toe dat mijn Nederlandse woordenschat voor 80% van jouw afkomstig is. Als
(gezellige) kamergenoot moest je vele onderbrekingen en vragen vanuit mijn kant verduren
zodat ik de Nederlandse taal wat onder beheer kon krijgen. Wij hebben vele leuke gesprekken
bij een glaasje bier in de Esculaaf gehad: van de samenstelling van het atoom, beklimmen van
Mount Everest, tot de zin van het leven. Ik zal deze tijden zeer zeker missen.
Beste Monique. Jij was de derde persoon in onze onderzoekers kamer. Jij bent een echt
inspirerend mens en jouw uitgesproken vermogen tot efficiënte multi-tasking heeft mij sterk
onder de indruk gebracht. Ik denk dat jij een van de weinige uitstekende arts-onderzoeker-
moeder combinaties maakt. Je zult zonder twijfel een succes van je toekomstige leven maken.
Beste Caroline. Jij kwam wat later in mijn onderzoekers tijd erbij. Van alle prostaat onderzoekers
ben jij beslist de meest enthousiaste en kundige op dit gebied. Jouw creativiteit en kennis bij het

Postlude
onder de indruk gebracht. Ik denk dat jij een van de weinige uitstekende arts-onderzoeker-
moeder combinaties maakt. Je zult zonder twijfel een succes van je toekomstige leven maken.
Beste Caroline. Jij kwam wat later in mijn onderzoekers tijd bij. Van alle prostaat
onderzoekers is jij beslist de meest enthousiaste en kundige op dit gebied. Jouw creativiteit
en kennis bij het aanpakken van onderzoek heeft mij ook veel geholpen. De aantal
wederzijdse mede-auteurschappen getuigt van een goede spanpoging. Dank hiervoor.
Aan de kinderen van de prostaat team (jonge onderzoekers): Mathijn, Joyce, Thiele, Geert en
Wendy met wie ik enigszins heb samengewerkt. Jullie zijn beslist de beste kandidaten om het
belangrijke werk op prostaat kanker beeldvorming over te nemen. Succes ermee.
Jurgen en Stijn. Van jullie heb ik geleerd om een MRI scanner te gebruiken en zelf te kunnen
scannen. Dit was een essentieel onderdeel van mijn onderzoek. Jullie hebben ook het
baanbrekende voorwerk van MRI bij prostaatkanker gedaan. Zonder dit voorwerk was geen
van mijn eigen onderzoek mogelijk.
Beste Solange. Een echte perfectionistische secretaresse. Streng, exact en je doet je werk met
absolute overgave. De menigte VIP patiënten zijn jou in het bijzonder dankbaar voor de
excellente service die zij hebben gehad. Je vriendelijkheid en de glimlach iedere dag op jouw
gezicht betoverd iedereen. Mocht Jelle eendaags aftreden, zou ik jou (mocht ik in een
dergelijke positie verkeren) graag als mijn secretaresse willen aanstellen.
Beste M&M (Manita en Marijke). Wie van jullie de gele pinda en wie de rode een is, kunnen
jullie zelf uitvechten. Jullie harde werk was onontbeerlijk voor mijn onderzoek. De duizenden
patiënten die jullie voor mij hebben ingepland was vaak tijdrovend. Bedankt in ieder geval.
Bedankt ook dat ik altijd jullie kamer kon binnenlopen en een gezellig gesprekje kon maken.
Last but not least. My liewe vrou. Nadi, jy het ongelukkig eers teen die einde van my
navorsingsteit in my lewe weer gekom. Jammer dat dit nie eerder was nie. Ons kan ons daaraan
troos dat die lewe veel eensamer was gewees as jy aand vir aand wat ek moes scan alleen tuis
sou gesit het. Jy het my weer moet, lus en sin vir die lewe voorentoe gegee. Ek is God innig
dankbaar dat hy ons paaie weer laat kruis het. Hoewel die afgelope jaar een met vele stene in
die weg was, weet ek dat ons 2013 jaar die mooiste van ons lewe sal wees. Van jou het ek geleer:
“Carpe Diem”, gryp die dag. Laat ons mekaar motiveer om meer volluit te lewe. Jy is die
waardevolste wat ek het!
322
aanpakken van onderzoek heeft mij ook veel geholpen. De aantal wederzijdse
medeauteurschappen getuigt van een goede spanpoging. Dank hiervoor.
Aan de kinderen van de prostaat team (jonge onderzoekers): Mathijn, Joyce, Thiele, Geert en
Wendy met wie ik enigszins heb samengewerkt. Jullie zijn beslist de beste kandidaten om het
belangrijke werk op prostaat kanker beeldvorming over te nemen. Succes ermee.
Jurgen en Stijn. Van jullie heb ik geleerd om een MRI scanner te gebruiken en zelf te kunnen
scannen. Dit was een essentieel onderdeel van mijn onderzoek. Jullie hebben ook het
baanbrekende voorwerk van MRI bij prostaatkanker gedaan. Zonder dit voorwerk was geen van
mijn eigen onderzoek mogelijk.
Beste Solange. Een echte perfectionistische secretaresse. Streng, exact en je doet je werk met
absolute overgave. De menigte VIP patiënten zijn jou in het bijzonder dankbaar voor de
excellente service die zij hebben gehad. Je vriendelijkheid en de glimlach iedere dag op
jouwgezicht betoverd iedereen. Mocht Jelle eendaags aftreden, zou ik jou (mocht ik in een
dergelijke positie verkeren) graag als mijn secretaresse willen aanstellen.
Beste M&M (Manita en Marijke). Wie van jullie de gele pinda en wie de rode een is, kunnen jullie
zelf uitvechten. Jullie harde werk was onontbeerlijk voor mijn onderzoek. De duizenden
patiënten die jullie voor mij hebben ingepland was vaak tijdrovend. Bedankt in ieder geval.
Bedankt ook dat ik altijd jullie kamer kon binnenlopen en een gezellig gesprekje kon maken.
Last but not least. My liewe vrou. Nadi, jy het ongelukkig eers teen die einde van my navorsingsteit
in my lewe teruggekeer. Jammer dat dit nie eerder was nie. Ons kan ons daaraan troos dat die lewe
veel eensamer was gewees as jy aand vir aand wat ek moes scan alleen tuis sou gesit het. Jy het my
weer moet, lus en sin vir die lewe voorentoe gegee. Ek is God innig dankbaar dat hy ons paaie weer
laat kruis het. Hoewel die afgelope jaar een met vele stene in die weg was, weet ek dat ons 2013
jaar die mooiste van ons lewe sal wees. Van jou het ek geleer: “Carpe Diem”, gryp die dag. Laat ons
mekaar motiveer om meer voluit te lewe. Jy is diewaardevolste wat ek het!
323
aanpakken van onderzoek heeft mij ook veel geholpen. De aantal wederzijdse
medeauteurschappen getuigen van een goede spanpoging. Dank hiervoor.
Beste Rik, de enige uroloog waarmee ik direct heb samengewerkt. Wij hebben menigte avonden
achter het computer programma gezeten om het mysterie van prostaat
kanker agressiviteit op MRI te ontrafelen. Vaak wilden wij de handdoek in de strijd gooiden,
omdat het zo traag en moeizaam verliep. Maar Perseverance mooie artikelen
zijn het uiteindelijk geworden. Bedankt voor jou enorme inzet in dit verband.
Aan de kinderen van de prostaat team (jonge onderzoekers): Martijn, Joyce, Thiele, Geert, Esther
en Wendy met wie ik enigszins heb samengewerkt. Jullie zijn beslist de beste kandidaten om het
belangrijke werk van prostaat kanker beeldvorming over te nemen. Succes ermee.
Jurgen en Stijn. Van jullie heb ik geleerd om een MRI scanner te gebruiken en zelf te kunnen
scannen. Dit was een essentieel onderdeel van mijn onderzoek. Jullie hebben ook het
baanbrekende voorwerk van MRI bij prostaatkanker gedaan. Zonder dit voorwerk was geen van
mijn eigen onderzoek mogelijk.
Beste Solange. Een echte perfectionistische secretaresse. Streng, exact en je doet je werk met
absolute overgave. De menigte VIP patiënten zijn jou in het bijzonder dankbaar voor de
excellente service die zij hebben gehad. Je vriendelijkheid en de glimlach iedere dag op jouw
gezicht betoverd iedereen. Mocht Jelle eendaags aftreden, zou ik jou (mocht ik in een dergelijke
positie verkeren) graag als mijn secretaresse willen aanstellen.
Beste M&M (Manita en Marijke). Wie van jullie de gele pinda en wie de rode een is, kunnen jullie
zelf uitvechten. Jullie harde werk was onontbeerlijk voor mijn onderzoek. De duizenden
patiënten die jullie voor mij hebben ingepland was vaak tijdrovend. Bedankt in ieder geval.
Bedankt ook dat ik altijd jullie kamer kon binnenlopen en een gezellig gesprekje kon maken.
Last but not least. My liewe vrou. Nadi, jy het ongelukkig eers teen die einde van my navorsingstyd
in my lewe teruggekeer. Jammer dat dit nie eerder was nie. Ons kan ons daaraan troos dat die lewe
vir jou veel eensamer was gewees as jy aand vir aand wanneer ik tot laat moes werk om te scan
alleen tuis sou gesit het. Jy het my weer moet, lus en sin vir die lewe voorentoe gegee. Ek is God innig
dankbaar dat hy ons paaie weer laat kruis het. Hoewel die afgelope jaar een met vele stene in die
weg was, weet ek dat ons 2013 jaar die mooiste van ons lewe sal wees. Van jou het ek geleer: “Carpe
Diem”, gryp die dag. Laat ons mekaar motiveer om meer voluit te lewe. Jy is die waardevolste wat
ek het!

Sir Bertrand Russels (1872-1970)
323

The Author
324




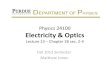





![Physics 102: Magnetic Fields - UNIVERSE OF ALI OVGUN€¦ · October 31, 2007 q Magnetic field: q SI unit of magnetic field: tesla (T) n 1T = 1 N/[Cm/s] = 1 N/[Am] = 104 gauss q Magnetic](https://img.pdfslide.us/doc/110x75/5f0523357e708231d4117499/physics-102-magnetic-fields-universe-of-ali-ovgun-october-31-2007-q-magnetic.jpg)