Embed Size (px)
Citation preview

THE VAGINAL PESSARY
Bernie BrennerGynaecologistClinical Director – Pelvic Floor ClinicMilfordAuckland [email protected]
Presentation modified from H Carcio “Bioteque – The Vaginal Pessary”

THE VAGINAL PESSARY

PELVIC ORGAN PROLAPSE QUANTIFICATION EXAM
Measures the descent of the anterior, apical and/or posterior portions of the vagina
Records vaginal length and width of the introitus. Uses centimeters with reference to the hymen
when performing the Valsalva Negative numbers: Distance above the hymen Positive numbers: Distance of prolpase protruding
beyond hymen May simply grade the prolapse from 1 to 3

PURPOSES Supports the vaginal musculature/bladder base in
physiologic alignment Can provide a solution to incontinence in women
unable or unwilling to have surgical correction May unmask Stress Urinary Incontinence Provides a diagnostic means of predicting which
patients would be helped with surgical correction

ADVANTAGESMay reduce the symptoms of incontinence
Supports and corrects retro-displacement of the uterus in early pregnancy
Relieves the discomfort of a pelvic organ prolapse
Repositions pelvic structures during pelvic floor rehabilitation (decreases post op adhesions)

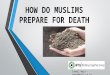
PESSARY CAN SUPPORT A POP
A. Cystocele B. Rectocele C. Enterocele

CAUSES OF PROLAPSE
Constipation Exercise Pregnancy and Childbirth Abnormal collagen/connective tissue Hormonal factors Previous pelvic surgery

STRESS INCONTINECE: Causes Weakened pelvic floor musculature Intrinsic sphincter deficiency Increased intraabdominal pressure Reduced strength of urethral sphincter

HISTORICAL PERSPECTIVES Appears in both Latin
and Greek literature Many different types
of materials and shapes
Over 2000 used throughout history
Fell into disfavour 10-20 years ago
Today offers a viable alternative to surgery

PESSARY FEATURES Silicone
Non-toxic, medical-grade silicone Biologically inert - does not absorb vaginal odor Pliable Can be autoclaved or soaked in Cidex
A few pessaries are made of latex rubber Must assess and document any latex allergy
Available in a variety of sizes and shapes The outside diameter is measured in inches
with a range of one to four inches

SEXUAL ACTIVITY
Intercourse is possible with pessaries that are not vaginally occlusive
Must have the dexterity and know-how to insert and remove as necessary
Note: Always ask about sexual activity – never assume

CONTRAINDICATIONS
Severe untreated vaginal atrophism Vaginal bleeding of unknown origin Pelvic inflammatory disease Abnormal cervical smear Dementia without possibility of
dependable follow-up care Expected non-compliance with follow-up

THE EVALUATION
Pelvic Examination Determine the extent of the
pelvic support problem POP-Q Assess degree of incontinence Rule out any pathology
Cervical smear Assess oestrogen status

Some possible predictors of pessary failure Short vaginal length Wide introitus Posterior-wall defects Patients who desire surgery

FITTING A PESSARY The pubic bone is an important landmark.
The pessary should fit snugly behind it. There is less chance of expulsion if thus anchored
Uterine Prolapse (if present) Insert two fingers in the vagina to push any
uterine prolapse back into place Place opposite hand on abdomen and push on the
fundus (if present) to hold in place Reduce any cystocoele or rectocoele prior to
fitting Put in largest size that will fit comfortably, or
simply tuck a smaller pessary well behind the pubic bone

MEASURING THE WIDTH
Insert first two fingers of dominant hand deep to the posterior fornix
Approximate size by using the fingers to determine the width
Spread fingers wide to measure
Remove fingers and compare to pessary sample or fitting kit

MEASURING THE LENGTH
Reinsert fingers deep into the posterior fornix
Make note of where the hand comes into contact with the pubic bone
Compare to pessary.
Iden

VAGINAL OESTROGEN
The majority of older women with a pessary need vaginal oestrogen
The Estring works nicely since it also needs to be changed every 3 months
Oestrogen use keeps the vagina healthy Oestrogen thickens the layer of the vaginal
mucosa allowing for more support of the pelvic organs.

COMPLICATIONS Increase in vaginal discharge Odor Ulcerations Pelvic discomfort Incarceration
Scar/granulation tissue may form around pessary
Complications are rare in the properly fitted and well maintained pessary

DONUT
The Donut Hole
Description: soft silicone, donut shaped.
Indications: Occludes upper vagina
and supports a uterine prolapse
Useful for cystocoele or rectocoele
Good for prolapse of the vagina after a hysterectomy
Adequate integrity of the introitus is necessary for the pessary to remain in place

CUBEIndications: Third-degree
prolapse, cystocele or rectocele, with or without good vaginal tone.
Often this is the only satisfactory support for women with a complete prolapse, complicated by a cystourethrocoele.
Excellent for vaginal wall prolapse in that it keeps the vaginal wall from collapsing from its six pressure points.
Maybe used by an athlete and removed after exercise.
Mucosa molds to the concavities creating a negative pressure
Description: Each side of the cube has concave suction cups that adhere to the vaginal walls, helping to restore anatomical support to the pelvic organs.
Drainage holes

INCONTINENCE DISH
Description: Dish-shaped pessary with holes to allow for drainage. The flexible membrane of the dish supports and elevates a mild cystocele.
Indications: SUI in conjunction with a 1st or 2nd degree prolapse, or a mild cystocele.
The knob
Membrane support

SHAATZ
Description:A circular pessary with
holes for drainage of secretions.
Indications: For the support of a first or mild second-degree prolapse.

GEHRUNGDescription:U-shaped device that provides
support to the anterior vaginal wall. The arms or heels rest flat on the vaginal floor
It avoids pressure on the rectum while supporting the anterior wall
Arclike – malleable-can be shaped to suit the shape of the vagina
Shape can be expanded once inserted, a distinct advantage
Creates a “bladder bridge”
May be underutilized
HeelArch

GELLHORN Description: Most commonly
used pessary for uterine prolapse, also helpful with SUI. Fits superiorly and anteriorly.
Indications: Provides support for third-degree uterine prolapse and procidentia.
Provides less support for a rectocele since there is less support of the posterior segment.
Holes for drainage

HODGE
Description: The anterior notch prevents
urethral impingement and obstruction.
Available with support for the bladder in patients with stress incontinence.
If properly fitted sexual intercourse is possible
Malleable
Notch
Support for cystocele

RING - with and without support
Description:Round flexible ring.Helps support the urethra and
bladder neck.Membrane provides
additional support for a cystocele.
Indications:Useful for a first or mild
second-degree uterine prolapse associated with a mild cystocele.
Support