-
The use of the simplified International Index of Erectile
Function(IIEF-5) as a diagnostic tool to study the prevalence of
erectiledysfunction
EL Rhoden1*, C Teloken1, PR Sogari1 and CA Vargas Souto1
1Department of Urology, Andrology Division, Santa Casa Hospital
and Fundacao Faculdade Federal de Ciencias Medicas,Porto Alegre,
Brazil
The purpose of this research was to determine the prevalence of
erectile dysfunction (ED) in a non-selected population using the
abridged 5-item version of the International Index of
ErectileFunction (IIEF-5) as a diagnostic tool. In a
non-institutionalized population and during a freescreening program
for prostate cancer (Prostate Cancer Awareness Week of Santa Casa
Hospital,Porto Alegre, Brazil), from 26 to 30 July 1998, all men
who were attending were invited tocomplete a sexual activity
questionnaire (the abridged 5-item version of the International
Index ofErectile Function-IIEF-5) as a diagnostic tool for ED. The
possible scores for the IIEF-5 range from5 to 25, and ED was
classified into five categories based on the scores: severe (5 7),
moderate (8 11), mild to moderate (12 16), mild (17 21), and no ED
(22 25). Of the 1071 men whoparticipated in the program, 965
(90.1%) were included in this study. Of the responding men 850were
Caucasian (88%) and 115 were black (12%). The mean age of the men
was 60.7 y, rangingfrom 40 to 90 y old. In this sample the
prevalence of all degrees of ED was estimated as 53.9%. Inthis
group of men, the degree of ED was mild in 21.5%, mild to moderate
in 14.1%, moderate in6.3%, and severe in 11.9%. According to age
the rates of ED were: 40 49 (36.4%); 50 59 (42.5%);60 69 (58.1%);
70 79 (79.4%), and over 80 y (100%) showed ED (P< 0.05). The
Pearsoncoefficients between the variables age and IIEF-5 showed a
statistically significant inverse(negative) relation (r 70.3449;
P< 0.05). ED is highly prevalent in men over 40 and
thiscondition showed a clear relationship to aging, as demonstrated
in other studies published. Thesimplified IIEF-5, as a diagnostic
tool, showed to be an easy method, which can be used to
evaluatethis condition in studies with a great number of
men.International Journal of Impotence Research (2002) 14, 245250.
doi:10.1038=sj.ijir.3900859
Keywords: erectile dysfunction; aging; erectile function;
diagnostic tests; IIEF; epidemiology oferectile dysfunction
Introduction
Erectile dysfunction (ED) is defined as the persistentinability
to achieve and maintain an erectionsufficient to permit
satisfactory sexual inter-course.1 3
Incidence and prevalence of ED are considerableand awareness is
growing that the condition istreatable.1,4 Despite the increasing
demand forclinical services and the potential impact of EDand other
sexual disorders, on interpersonal rela-
tionships and quality of life, epidemiological dataare
relatively scarce.5 7
The prevalence of ED depends on the populationstudied and the
definition and methods used. SinceED often accompanies aging and is
associated withchronic illness, such as diabetes mellitus,
heartdisease, hypertension, and a variety of neurologicaldiseases,
very few studies have been carried out toestablish the incidence
and prevalence of thiscondition in a healthy population.8 In a
commu-nity-based survey of men between the ages of 40 and70 y, 52%
of the respondents reported some degreeof erectile difficulty.
Based on these data it isestimated that ED affects 20 30 million
men inthe USA.2
Although laboratory-based diagnostic proceduresare available, it
has been proposed that sexualfunction is best assessed in a
naturalistic settingwith patient self-report techniques,
particularly in
*Correspondence: EL Rhoden, Rua Jaragua 370 apto. 302,90450-140
Porto Alegre, Brazil.E-mail: [email protected] 3
October 2001; revised 26 December 2001; accepted16 Janaury 2002
International Journal of Impotence Research (2002) 14, 245250
2002 Nature Publishing Group All rights reserved 0955-9930/02
$25.00www.nature.com/ijir
-
multicenter, multinational and epidemiologicalclinical
trials.9
The objective of the present study is to use theabridged 5-item
version of the International Index ofErectile Function (IIEF-5)10
as a diagnostic tool forestablishing the prevalence of ED in a
normalhealthy population.
Materials and methods
The ethics committee at our hospital approved thisstudy.
Patients were previously informed of theresearch details and they
agreed to participate in thestudy. Informed consent was obtained at
the inter-view.
All the men attending a screening program forprostate cancer
(Prostate Cancer Awareness Week ofSanta Casa Hospital-Porto Alegre,
Brazil) from 26 to30 July 1998 were asked to answer the
5-itemversion of the IIEF10 to determine the prevalenceof ED. This
was a non-institutionalized populationand included 1071 men.
As previously described this questionnaire con-sists of only
five questions and each IIEF-5 item isscored on a five-point
ordinal scale where lowervalues represent poorer sexual function.10
Thus, aresponse of 0 for a question was considered the
leastfunctional, whereas a response of 5 was consideredthe most
functional. The possible scores for the IIEF-5 range from 1 to 25
(one question has scores of 1 5), and a score above 21 was
considered as normalerectile function and at or below this cutoff,
ED.According to this scale, ED is classified into four
categories based on IIEF-5 scores: severe (1 7),moderate (8 11),
mild to moderate (12 16), mild(17 21), and no ED (22 25). Trained
physiciansfrom the urology staff interviewed each of the menin an
individual room with a total guarantee ofconfidentiality.
The screening was advertised in print andelectronic mass media
and participants were self-selected, according to order of arrival
at the evalua-tion site, after responding to media publicity.
Themedia was only directed to prostate evaluation. Allmen who were
patients of the hospital InstitutionalDivision of Urology or
Andrology, as well as, thosewho were using intracavernous
pharmacology ther-apy, oral drugs for ED, penile prothesis and
patientswith major psychiatric disorders or penile anatomi-cal
disorders or who reported no sexual activityduring the last 6
months were excluded from thestudy analysis. Men who did not speak
Portuguesewere excluded from the study.
The Chi-square test was used for statisticalanalysis as well as
the Pearson correlation whichwas calculated for the variables age
and IIEF-5 in thestudy. A value of P< 0.05 was considered
statisti-cally significant.
Results
Of the 1071 individuals seen, 965 (90.1%) wereincluded in the
present study. One hundred and sixmen were excluded (9.9%) because
of failure tocomplete all of the criteria in the protocol.
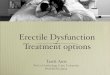
Thefrequency distribution of the men according to the
Figure 1 Distribution of the subjects according to the age
groups included in the study of erectile function.
The use of simplified IIEF-5 to study the prevalence of EDEL
Rhoden et al
246
International Journal of Impotence Research
-
different age groups is shown in Figure 1. Of theresponding men
850 were Caucasian (88%) and 115were black (12%).The mean age was
60.7 y, rangingfrom 45 to 90.
In this sample the prevalence of all degrees of EDwas estimated
at 53.9%. In this group of men, thedegree of ED was mild in 21.5%,
mild to moderate in14.1%, moderate in 6.3%, and severe in
11.9%(Table 1). According to age the ED rates were: 40 49(36.4%);
50 59 (42.5%); 60 69 (58.1%); 70 79(79.4%), and over 80 y (100%)
showed ED, whichwas statistically different among all the age
groups(P< 0.05), except between 40 49 and 50 59 y(P> 0.05;
Table 2).
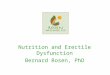
The relationship between different degrees of EDprobabilities
and age of the subjects studied isillustrated in Figure 2. We can
observe that thenormal erectile function declines with advancingage
and ED, mainly severe, was progressively morelikely in the aging
male. Subjects aged 70 have morethan double the ED when compared
with men aged40 y. An estimated 63.6% of the men have no ED atthe
age of 40, with a decrease to 20.6% at 70 y and0% at age 80. Mild
and intermediate degrees of EDhave a similar prevalence in the
different agegroups.
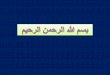
The Pearson coefficient between age and inci-dence of ED showed
a significant inverse correlation(r 7 0.3449; P< 0.05) (Figure
3).
Discussion
The present study was based on a cross-sectionedoutline of
non-institutionalized men with agesdistributed between 40 and 90 y,
from a centerdesignated for the treatment of urological
diseases.These men were invited to participate in a freescreening
program for prostate cancer. Completing asexual activity
questionnaire was only mentionedduring the interview at the
office.
Table 1 Prevalence of erectile dysfunction in the
populationstudied
Population
Condition of erectile function (IIEF-5) n %
Normal erectile function 445 46.1Erectile dysfunction 520
53.9
Mild 208 21.5Mild to moderate 136 14.1Moderate 61 6.3Severe 115
11.9
IIEF-5 (abridged 5-item version of the International Index
ofErectile Function).
Table 2 Prevalence of erectile dysfunction (ED), in the
differentage groups
Prevalence of erectiledysfunction (ED)
Age groups n n (%)
40 49 11 4 36.450 59 470 200 42.560 69 334 194 58.170 79 131 103
79.4 80 19 19 100
IIEF-5 (abridged 5-item version of International Index of
ErectileFunction).Statistically difference among all the age
groups, except between40 49 and 50 59 y Analysis of Variance
(ANOVA), followed bythe Bonferroni test.P
-
The data in this study do not represent arandomly selected
population from within a com-munity but are from men seeking
medical attentionin a free screening program. It is possible,
therefore,that these data might not represent the country oreven
regional status. People seeking medical atten-tion in a screening
program may be more concernedwith their own health that the general
populationbut, on the other hand, patients with co-morbidityand low
quality of life might have no interest inparticipating in this type
of program.
The erectile function in this study was based onsubject
responses to a privately administered ques-tionnaire by a
physician. Recently, Lehmann et al.11
demonstrated that ED could not be defined bypharmacostimulated
erection but relevant ED washonestly reported. As referred by Rosen
et al.10 theIIEF-5 is intended to complement, not supplant,clinical
judgment and useful diagnostic assess-ments. It may be particularly
useful as an initialscreening instrument in the general practice
setting,mainly when we consider the progressive advent ofrecently
available oral therapeutics for the treatmentof ED. In
epidemiological studies, when manypeople are assessed, a simple,
practical and validquestionnaire is essential.
The IIEF is a multidimensional validated ques-tionnaire with 15
questions in the five domains ofsexual function (erectile and
orgasmic functions,sexual desire, satisfaction with intercourse
andoverall sexual satisfaction) approved by the NationalInstitutes
of Health (NIH).1 Its purpose to unify thelanguage used in studies
with the intention ofdefining the prevalence of ED in different
popula-tions and countries.9 More recently, to simplify theIIEF an
abridged 5-item version of this (IIEF-5) wasdeveloped as a
diagnostic tool for ED.10 It consists offive selected items to
clearly discriminate betweensubjects with and without ED, as well
as address the
NIH1 definition of this condition. This simplifiedversion,
proved to be a valid specific and sensitivescale for use in the
clinical setting.10,12
ED has been described as an important publichealth problem by
the NIH Consensus Panel,1 whichidentified an urgent need for
population-based dataconcerning the prevalence, determinants, and
con-sequences of this disorder.6
As previously observed, the prevalence of EDdepends on the
population studied and the defini-tion of this condition and
methods used.5,13 15
These aspects can explain the varied data of the 52%prevalence
from a study in the USA,2 32% from astudy in the UK, 26% in Japan
and 19% from astudy in Denmark.10
Studies performed in a select population withpathological
conditions such as diabetes mellitus,heart disease or in
institutions which provideattention for patients with specific
andrologic dis-eases do not represent the true prevalence of ED
inthe general population. Another aspect is the factthat many
studies using different questionnaires anddefinitions of ED have
significant influence on thedata obtained.
Potency, defined as satisfactory functional capa-city for
erection, may coexist with some degree ofED in the sense of
submaximal rigidity or submax-imal capability to sustain the
erection.16 18 There-fore, erectile function is best defined by
theindividual as assessment of his own situation insimple terms of
minimal, moderate or complete aspresented to a physician for
treatment.9,17
Although ED can be primarily psychogenic inorigin, most patients
have an organic disorder(vascular, neurologic, endocrine
disorders), com-monly with some psychogenic overlay.19 21 Somemen
assume that erectile failure is a natural part ofthe aging process
and tolerate it; for others it is adevastating condition.
Withdrawal from sexual
Figure 3 Correlation between erectile function and age of the
population studied.
The use of simplified IIEF-5 to study the prevalence of EDEL
Rhoden et al
248
International Journal of Impotence Research
-
intimacy because of fear of failure can damagerelationships and
have a profound effect on theoverall relationship of the couple.
The decrease ofsexual activity has been frequently associated
withthe aging process.22 24 Normally, several causes hadassociated
ED with aging, which include, vascularinsufficiency, hormonal
disturbances, neuropathies,diabetes mellitus, psychological factors
and sideeffects of drugs usually used more by this
popula-tion.25
Sexual function progressively declines in healthyaging men. For
example, the latent period betweensexual stimulation and erection
increases, erectionsare less turgid, ejaculation is less forceful,
theejaculatory volume decreases, and the refractoryperiod between
erections lengthens.26 There is alsoa decrease in penile
sensitivity to tactile stimula-tion, a decrease in the serum
testosterone concen-trations, and an increase in cavernous
muscletone.26
In this cross-section study, with men who wereinvited to
participate in a screening program forprostate cancer, and who were
not informed pre-viously that their sex life would be assessed,
theprevalence of all degrees of ED was 54.5%, similar tothe results
obtained by Feldman et al.2 in theMassachusetts Male Aging Study
(MMAS), whichwas 52%, although several considerations have to
bemade regarding methodological aspects.
As demonstrated in Table 2, the mean values ofthe IIEF-5 scores,
in all age groups, decreasedprogressively with age.
We can observe that the rates of ED were 37.5% inthe group aged
40 49, 43.3% in the 50 59 group,60% in the 60 69 group, 81% in the
group aged70 79 y and 100% of the men had been classifiedwith ED
(all degrees) when ages over 80 y wereconsidered. The absence of a
statistical differencebetween the groups aged 40 49 and 50 59 can
beattributed to the small number of subjects in thefourth decade of
life evaluated in the present study.This aspect is explained by the
fact that in the mediacampaign men over 50 y were invited to
participateof the screening program.
Although, again data very similar to ours wereobserved by
Feldman et al2 in the epidemiologicalstudy of MMAS, in which the
rate of ED was 39% inthe age group 40 49 y, 48% in those aged 50 y,
57%in those aged 60 and 67% in the 70-y group. Veryfew studies
evaluated ED in men over 70. Someauthors, such as Morley,3 referred
to a 75% rate ofED in men 80 or over.
In the present study an interesting aspect is thehigh prevalence
of ED in men over 70 y old. Thisaspect is very important because
very few studies inthe literature have reported the erectile
condition inthis select aged population.
Another significantly relevant aspect observed inthe present
study showed a high rate of severedegree and decrease in frequency
of mild degree of
ED with aging. This aspect can be best explainedwhen we observe,
for instance, that in the age group40 49, nearly 90% have a mild
degree of ED, but70% have a severe degree of ED when we select
thepopulation over 80 y old. On the other hand, in thesesame groups
62.5% of the men mentioned normalerectile function in the fourth
decade, although thisrate fell to 19% and 0% in the ages groups 70
79 yand over 80 y, respectively.
The characteristic relationship between the prob-ability of
complete ED and the age of the individualscould also be observed in
the MMAS,2 so between40 and 70 y it increases 3-fold, from 5.1 to
15%, andthe moderate degree of ED increased 2-fold, 17 to34%,
although, the mild degree of ED was similar,17%, presented the two
extremes. Around 60% ofmen have normal erectile function at 40 y
but only33% presented the same condition when men ofaged 70 were
considered.
In our experience, the simplified 5-item IIEF-5used in this
study was shown to be a simple andeasy method for the evaluation of
ED mainly whenwe consider epidemiological studies with a
greatnumber of individuals. This aspect is reinforcedwhen we
observe the low number of men excluded(9%) from the study, as well
as, the characteristics ofthe results obtained. Another relevant
aspect is thefact that the erectile condition or the severity of
EDcould be established when we used the question-naire and probably
easier than other methods. Theevaluation of the erectile function
with this methodand the investigation of the association with
riskfactors for ED in others studies can establish healthstrategies
and medical orientations to change thefactors associated with this
clinical condition andwhich will result in significant improvement
for thedifficult problems related to the aging process.
Conclusions
In conclusion, we and other authors observed thatED is more
common with advancing age, data onprevalence being similar to those
found in othercountries.
From the data obtained in this population we canobserve that ED
is a condition highly prevalent inmen over the age of 40, and that
it is clearly relatedto advancing age in the different
stratificationsconsidered. Furthermore, age is thought to be
thefactor which has the strongest influence on erectilefunction
and, therefore, can be considered to be animportant risk factor for
ED. Finally, the IIEF-5 wasshown to be a useful instrument to
evaluate theprevalence of ED and its degree in this
unselectedpopulation and we agree that this method can beused in
the future to establish the prevalence of thiscondition in
epidemiological features with moreuniform language.
The use of simplified IIEF-5 to study the prevalence of EDEL
Rhoden et al
249
International Journal of Impotence Research
-
References
1 NIH Consensus Development Panel on Impotence. Impotence.JAMA
1993; 270: 83 90.
2 Feldman HA et al. Impotence and its medical and psychoso-cial
correlates: results of the Massachusetts Male Aging Study.J Urol
1994; 151: 54 61.
3 Morley JE. Impotence. Am J Med 1986; 80: 897 905.4 Goldstein I
et al. Oral sildenafil in the treatment of erectile
dysfunction. New Engl J Med 1998; 338: 1397 1404.5 Jonler M et
al. The effect of age, ethnicity and geographical
location on impotence and quality of life. Br J Urol 1995;
75:651 655.
6 Laumann EO, Paik A, Rosen RC. Sexual dysfunction in theUnited
States. Prevalence and predictors. JAMA 1999; 281:537 544.
7 Kirby RS. Impotence: diagnosis and management of maleerectile
dysfunction. Br Med J 1994; 308: 957 961.
8 Wagner G, Saenz de Tejada I. Update on male
erectiledysfunction. Br Med J 1998; 316: 678 682.
9 Rosen RC et al. The International Index of Erectile
Function(IIEF): a multidimensional scale for assessment of
erectiledysfunction. Urology 1997; 49: 822 830.
10 Rosen RC et al. Development and evaluation of an abridged,
5-item version of the International Index of Erectile
Function(IIEF-5) as a diagnostic tool for erectile dysfunction. Int
J ImpotRes 1999; 11: 319 326.
11 Lehmann K, Eichlisberger R, Gasser TC. Lack of
diagnostictools to prove erectile dysfunction: consequences for
reimbur-sement? J Urol 2000; 163: 91 94.
12 Cappelleri JC, Rosen RC. Reply to The sexual health
inventoryfor men (IIEF-5) by Ja Vroege. Int J Impot Res 1999; 11:
353 354.
13 Benet AE, Melman A. The epidemiology of erectile
dysfunc-tion. Urol Clin North Am 1995; 22: 699 709.
14 Rubin A, Babbott D. Impotence in diabetes mellitus. JAMA1958;
168: 498 500.
15 Kolodny RC, Kahn CB, Goldstein HH, Burnett DM.
Sexualdysfunction in diabetic men. Diabetes 1973; 23: 306 309.
16 Hanash KA. Comparative results of goal oriented therapy
forerectile dysfunction. J Urol 1997; 157: 2135 2140.
17 Nickel JC et al. Endocrine dysfunction in impotence,
sig-nificance and cost-effective screening. J Urol 1984; 132: 40
43.
18 Krane RJ, Goldstein I, Saenz De Tejada I. Medical
progress:impotence. New Engl J Med 1989; 321: 1648 1659.
19 Andersson KE, Wagner G. Physiology of penile erection.Physiol
Rev 1995; 75: 191 196.
20 Lerner SE, Melman A, Christ GJ. A review of
erectiledysfunction: new insights and more questions. J Urol
1993;149: 1246 1256.
21 Taub HC, Lerner SE, Melman A, Christ GJ. Relationshipbetween
contraction and relaxation in human and rabbitcorpus cavernosum.
Urology 1993; 42: 698 704.
22 Kaiser FE et al. Impotence and aging: clinical and
hormonalfactors. J Am Geriatr Soc 1988; 36: 511 516.
23 Diokno AC, Brown MR, Herzog AR. Sexual dysfunction in
theeldery. Arch Intern Med 1990; 150: 197 200.
24 Panser LA et al. Sexual function of men ages 40 to 79 y:
theOlmsted county study of urinary symptoms and health statusamong
men. J Am Geriatr Soc 1995; 43: 1107 1111.
25 Rundles RW. Diabetic neuropathy. Medicine 1945; 24: 111
160.
26 Lue T. Erectile dysfunction. New Engl J Med 2000; 342: 1802
1813.
The use of simplified IIEF-5 to study the prevalence of EDEL
Rhoden et al
250
International Journal of Impotence Research