Embed Size (px)
Citation preview

Ellen Buckley Lead Tissue Viability Clinical Nurse Specialist, Alder Hey Children’s NHS Foundation Trust, Liverpool Email: [email protected] Elizabeth Merlin-Manton Clinical Specialist, Urgo Medical. Email: [email protected]
INTRODUCTION
A neonate born at 25 weeks, weighing 707 grams presented with a range of specialist requirements at birth. The skin structure even for full term new born babies is fragile and full development is not completed until a few months after birth. The skin is our first defence system which protects and regulates effectively when it is fully developed and intact. Therefore choosing an effective suitable dressing to support healing is important, especially for a patient so young.
DISCUSSION
The fragility of the skin of a neonate and the holistic challenges that such a young patient can face, coupled with the emotional situation for the family, being able to demonstrate effective and progressive healing is imperative. The ease of application and atraumatic, pain free removal was excellent for this patient(2) .
CLINICAL SIGNIFICANCE
Pain at dressing change is not only distressing for the patient but can have significant psychological impact on the family. On a patient, with skin so fragile, where further surgery needs to be avoided, the selection of the correct wound dressing regime is paramount to be able to achieve the desired effect. Dressings which are marketed as pain free on removal also need to be able to meet the other desired outcomes such as absorbency and surrounding skin management, which in this case were successfully achieved.
RESULTS
The wound site continued to reduce in size throughout the treatment with the TLC healing matrix dressings and the excoriation to the peri wound edge resolved. One fistula required the placement of a catheter to aid fluid management. Full healing was achieved within a 5 week period with the highest percentage of wound surface area reduction achieved within a two week period.
*The TLC, silicone borded dressing was: UrgoTul Absorb Border * The desloughing TLC dressing was: UrgoClean
METHODS
The little girl underwent 3 Laparotomies for a twisted bowel and subsequent resection of necrotic bowel and she had suffered with sepsis. Following surgery she was left with only approximately 15cm of bowel. Post-operatively, her wound dehisced and she developed spontaneous fistulas which began leaking faecal matter onto her fragile skin which caused severe excoriation. On referral to the Tissue Viability Nurse, the wound measured 4cm x 1cm with a low level of exudate present. Advice around surrounding skin management and wound healing was provided by the tissue viability service and a dressing regime was created. Dressings with the Technology Lipido Colloid (TLC) healing matrix were selected to deslough the wound, protect the surrounding skin, manage the exudate, enhance the fibroblast proliferation(1) and ensure pain free, atraumatic removal. Dressings were changed 2 to 3 times weekly depending on fluid levels from either the fistulas or wound exudate.
The use of a Lipido-Colloid Dressing in the management of a dehisced wound in a neonate
REFERENCES [1] White, R., Cowan, T., Glover, D. Supporting evidence-based practice: a clinical review of TLC healing matrix (2nd edition). MA Healthcare Ltd, London, 2015 [2] Merlin-Manton E, Greenwood M, Linthwaite A. An observational evaluation of a new foam adhesive dressing. British Journal of Nursing (Tissue Viability Supplement), 2015, Vol 24, No 1
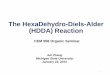
Prior to initiation of new dressing regime
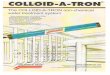
Week 3: Measuring 2cm x 1cm
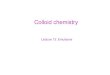
Week 5: Full Healing