Embed Size (px)
Citation preview

Naval Health Research Center
The U.S. Department of Defense Millennium Cohort Study: Career Span and Beyond Longitudinal Follow-up
T. C. Smith
For the Millennium Cohort Study Team
Report No. 08-38
. Approved for Public Release; Distribution Unlimited.
Naval Health Research Center 140 Sylvester Road
San Diego, California 92106

The US Department of Defense MillenniumCohort Study: Career Span and BeyondLongitudinal Follow-Up
Tyler C. Smith, MS, PhD; for the Millennium CohortStudy Team
Objective: To describe current and future career-span health researchin the US Department of Defense Millennium Cohort Study. Methods:Collaborating with all military service branches and the Department ofVeterans Affairs, the Millennium Cohort Study launched in 2001, beforeSeptember 11 and the start of deployments in Afghanistan and Iraq, toconduct coordinated strategic research to determine any effects ofmilitary occupational and deployment-related exposures, on long-termhealth. Results: More than 150,000 consenting members represent demo-graphic, occupational, military, and health characteristics of the USmilitary. More than 70% of the first two panels have submitted follow-upquestionnaires and �50% have deployed since 2001. Conclusions:Prospective cohort data have identified subgroups of military populations athigher risk or more resilient to decrements in mental and physical health.Continued career span and beyond follow-up will answer long-term healthquestions related to military service. (J Occup Environ Med. 2009;51:1193–1201)
C ross-sectional and retrospective stud-ies of exposures and health outcomesare capable of establishing associa-tions but lack a more robust ability todistinguish exposure contribution indisease pathways. Causative roles ofexposure to disease are better de-scribed through prospective analyseswith appropriate comparison popula-tions where subjects are disease freeat baseline and followed over time todocument exposure and diseasethrough temporal sequence. Well-designed prospective cohort studiesmay have inferential leverage overcross-sectional and retrospectivestudies through the minimization ofrecall and selection biases that areoften influenced by exposure and/ordisease in retrospective or cross-sectional assessment of study pop-ulations. Well-known prospectivecohort studies, such as the Framing-ham Heart Study, the British Physi-cians Study, and others, have madesignificant contributions toward im-proving public health.1–3
Occupational cohort studies areoften defined by a group of workersin a given occupation classified bycertain exposures encountered on thejob. Occupational cohort studieshave been instrumental in identifyingincreased risk of cancer in workersexposed to gas,4 dyestuff,5 and asbes-tos6 and increased risk of mortality ormorbidity from other occupationalexposures.7–11 Prospective or histor-ical prospective military cohort stud-ies have also been conducted withsome success in the past but havelargely focused on single exposures.
From the Department of Defense Center for Deployment Health Research, Naval Health ResearchCenter, San Diego, Calif.
Address correspondence to: Tyler C. Smith, MS, PhD, Department of Defense Center forDeployment Health Research, Naval Health Research Center, 140 Sylvester Road, San Diego, CA92106-3521; E-mail: [email protected].
Copyright © 2009 by American College of Occupational and Environmental Medicine
DOI: 10.1097/JOM.0b013e3181b73146
JOEM • Volume 51, Number 10, October 2009 1193

These studies have been designedpost exposure, combat deployment,or conflict and have often lackedrepresentativeness.6–9
The Millennium Cohort Study wasenvisioned to mitigate these limita-tions and construct a longitudinalheterogeneous cohort for compari-sons of disease experience acrosssubgroups defined by military ser-vice-related exposures.10,11 Thislarge population-based cohort de-signed in the late 1990s was initiatedin the aftermath of the 1991 GulfWar after the Department of Defense(DoD), Congress, and the Institute ofMedicine recommended coordinatedstrategic research to determine howmilitary service, including deploy-ment-related exposures, affect long-term health.12,13 In collaborationwith all military service branchesand the Department of Veterans Af-fairs (VA), the Millennium CohortStudy was launched in 2001, beforeSeptember 11 and the start of thewars in Afghanistan and Iraq.10,11
The Cohort includes military servicemembers from all components (ac-tive duty, Reservists, National Guardmembers) and all services (Army,Air Force, Navy, Marine Corps, andCoast Guard). The objective of thisreport is to describe this DoD study,which follows service members forthe span of their careers and beyond,and discuss strategic research goalsthat will answer health questions per-taining to military service for yearsto come.
Materials and Methods
Design and ObjectivesThe Millennium Cohort Study was
designed in the wake of the 1991Gulf War to complement many ofthe large electronic data that werebeginning to become available toresearchers. This Cohort was con-structed to prospectively assess long-term health in all components andservice branches of the US militaryand to follow them even after sepa-ration from military service withseven designed 3-year questionnaire
interval assessment periods. Theoriginal objectives of the MillenniumCohort Study included building acohort of �150,000 and assessingchronic diagnosed and subjectivehealth problems, including hyperten-sion, diabetes, heart disease, andchronic multisymptom illnessesamong military members, in relation-ship to exposures of military con-cern. The average age of the cohortat baseline was 28.9 years. Thenewer military accessions that wereinvited in 2004 and 2007 were ran-domly selected (oversampling forwomen and Marine Corps members)and designed to complement thepopulation-based random sample.More than 150,000 service membershave voluntarily consented and com-pleted baseline questionnaires sincethe first wave of invitations in 2001(July 2001 to June 2003; n �77,047), 2004 (Panel 2 enrolled be-tween June 2004 and February 2006;n � 31,110), and 2007 (Panel 3enrolled between June 2007 and De-cember 2008; n � 43,440), resultingin a 34% cumulative baseline re-sponse rate. More than 70% of thefirst two panels have submitted atleast one follow-up questionnaire.
Study PopulationCohort composition and survey in-
struments were designed in 2000. Aninitial random sample of active-duty,Reserve, and National Guard membersfrom all services was constructed bythe Department of Defense ManpowerData Center (DMDC) from all USmilitary personnel serving in Octo-ber 2000. The study team spent theremainder of 2000 and the first partof 2001 conducting a pilot test,which represented 1% of the originalsample.10,11 The instrument andmethods for conducting the studywere further refined, and the Millen-nium Cohort Study officially beganenrollment on July 1, 2001. The in-vited Millennium Cohort Study par-ticipants were randomly selected;however, oversampling of those whohad been previously deployed toBosnia, Southwest Asia, or Kosovo
(1998 to 2000), Reserve and NationalGuard members, and women was con-ducted to ensure sufficient power todetect statistical differences in smallersubgroups of the population.
Demographic and military-specificdata were obtained from electronicpersonnel files maintained byDMDC, including sex, birth date,highest education level, marital sta-tus, race/ethnicity, deployment expe-rience in support of wars in Iraq andAfghanistan, pay grade (rank of theservice member), service component(active duty consisting of full-timemilitary members and Reserve/National Guard who are mostly citi-zen soldiers with often full-time em-ployment outside of the US military),service branch (Army, Air Force,Navy, Marine Corps, and CoastGuard), and occupation.
QuestionnaireThe questionnaire was designed to
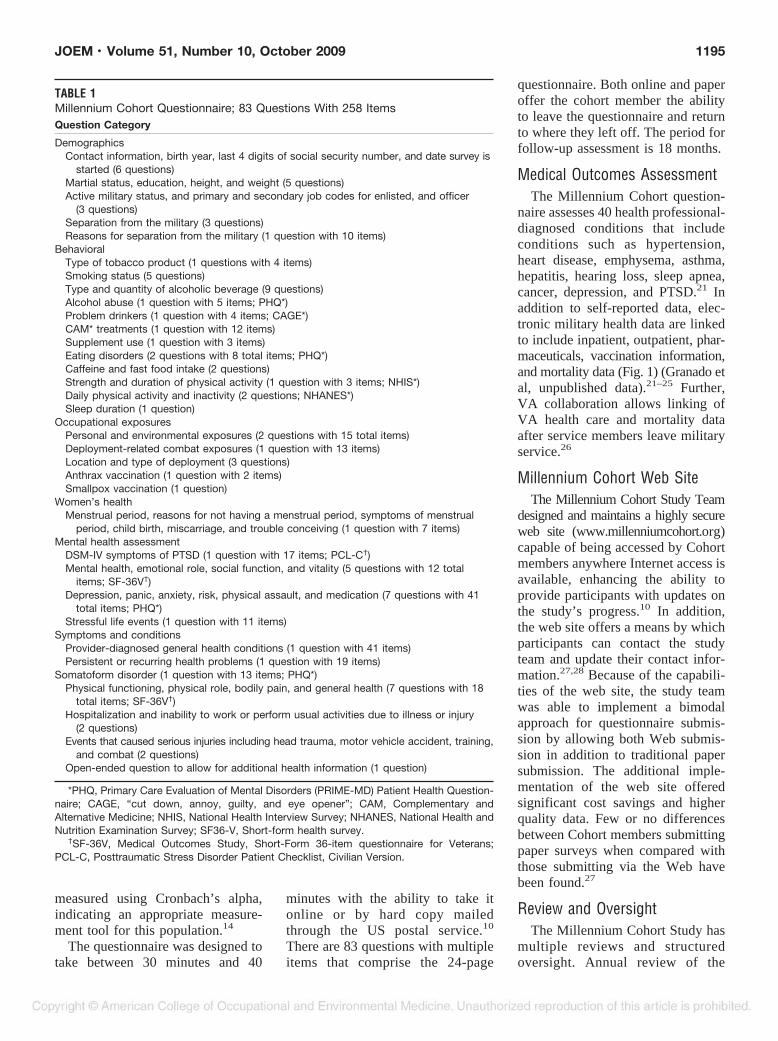
assess medical outcomes and symp-toms, chronic multisymptom illnesses,mental and physical health, physicalactivity, sleep, alcohol consumption,complementary and alternative healththerapies, tobacco use, physical activ-ity, weight change, energy supplemen-tation, family stressors, occupationalstressors, occupational exposures, de-ployment-specific locations and dates,deployment-specific exposures, injury,mild traumatic brain injury, duty andprimary occupation, and reasons forleaving military service (Table 1).
Multiple standardized instru-ments are included in the question-naire, including the posttraumaticstress disorder (PTSD) Checklist-Civilian Version14; the PatientHealth Questionnaire to assessdepression, panic, anxiety, eatingdisorders, and alcohol-relatedproblems15–18; the Medical Out-comes study Short Form 36-ItemHealth Survey for Veterans to assessfunctional health19; and potentialproblem drinking assessed using theCAGE questionnaire.20 These stan-dardized instruments included in thequestionnaire have been shown to beinternally consistent and reliable as
1194 Millennium Cohort Longitudinal Follow-Up • Smith
measured using Cronbach’s alpha,indicating an appropriate measure-ment tool for this population.14
The questionnaire was designed totake between 30 minutes and 40
minutes with the ability to take itonline or by hard copy mailedthrough the US postal service.10
There are 83 questions with multipleitems that comprise the 24-page
questionnaire. Both online and paperoffer the cohort member the abilityto leave the questionnaire and returnto where they left off. The period forfollow-up assessment is 18 months.
Medical Outcomes AssessmentThe Millennium Cohort question-
naire assesses 40 health professional-diagnosed conditions that includeconditions such as hypertension,heart disease, emphysema, asthma,hepatitis, hearing loss, sleep apnea,cancer, depression, and PTSD.21 Inaddition to self-reported data, elec-tronic military health data are linkedto include inpatient, outpatient, phar-maceuticals, vaccination information,and mortality data (Fig. 1) (Granado etal, unpublished data).21–25 Further,VA collaboration allows linking ofVA health care and mortality dataafter service members leave militaryservice.26
Millennium Cohort Web SiteThe Millennium Cohort Study Team
designed and maintains a highly secureweb site (www.millenniumcohort.org)capable of being accessed by Cohortmembers anywhere Internet access isavailable, enhancing the ability toprovide participants with updates onthe study’s progress.10 In addition,the web site offers a means by whichparticipants can contact the studyteam and update their contact infor-mation.27,28 Because of the capabili-ties of the web site, the study teamwas able to implement a bimodalapproach for questionnaire submis-sion by allowing both Web submis-sion in addition to traditional papersubmission. The additional imple-mentation of the web site offeredsignificant cost savings and higherquality data. Few or no differencesbetween Cohort members submittingpaper surveys when compared withthose submitting via the Web havebeen found.27
Review and OversightThe Millennium Cohort Study has
multiple reviews and structuredoversight. Annual review of the
TABLE 1Millennium Cohort Questionnaire; 83 Questions With 258 ItemsQuestion Category
DemographicsContact information, birth year, last 4 digits of social security number, and date survey is
started (6 questions)Martial status, education, height, and weight (5 questions)Active military status, and primary and secondary job codes for enlisted, and officer
(3 questions)Separation from the military (3 questions)Reasons for separation from the military (1 question with 10 items)
BehavioralType of tobacco product (1 questions with 4 items)Smoking status (5 questions)Type and quantity of alcoholic beverage (9 questions)Alcohol abuse (1 question with 5 items; PHQ*)Problem drinkers (1 question with 4 items; CAGE*)CAM* treatments (1 question with 12 items)Supplement use (1 question with 3 items)Eating disorders (2 questions with 8 total items; PHQ*)Caffeine and fast food intake (2 questions)Strength and duration of physical activity (1 question with 3 items; NHIS*)Daily physical activity and inactivity (2 questions; NHANES*)Sleep duration (1 question)
Occupational exposuresPersonal and environmental exposures (2 questions with 15 total items)Deployment-related combat exposures (1 question with 13 items)Location and type of deployment (3 questions)Anthrax vaccination (1 question with 2 items)Smallpox vaccination (1 question)
Women’s healthMenstrual period, reasons for not having a menstrual period, symptoms of menstrual
period, child birth, miscarriage, and trouble conceiving (1 question with 7 items)Mental health assessment
DSM-IV symptoms of PTSD (1 question with 17 items; PCL-C†)Mental health, emotional role, social function, and vitality (5 questions with 12 total
items; SF-36V†)Depression, panic, anxiety, risk, physical assault, and medication (7 questions with 41
total items; PHQ*)Stressful life events (1 question with 11 items)
Symptoms and conditionsProvider-diagnosed general health conditions (1 question with 41 items)Persistent or recurring health problems (1 question with 19 items)
Somatoform disorder (1 question with 13 items; PHQ*)Physical functioning, physical role, bodily pain, and general health (7 questions with 18
total items; SF-36V†)Hospitalization and inability to work or perform usual activities due to illness or injury
(2 questions)Events that caused serious injuries including head trauma, motor vehicle accident, training,
and combat (2 questions)Open-ended question to allow for additional health information (1 question)
*PHQ, Primary Care Evaluation of Mental Disorders (PRIME-MD) Patient Health Question-naire; CAGE, “cut down, annoy, guilty, and eye opener”; CAM, Complementary andAlternative Medicine; NHIS, National Health Interview Survey; NHANES, National Health andNutrition Examination Survey; SF36-V, Short-form health survey.
†SF-36V, Medical Outcomes Study, Short-Form 36-item questionnaire for Veterans;PCL-C, Posttraumatic Stress Disorder Patient Checklist, Civilian Version.
JOEM • Volume 51, Number 10, October 2009 1195

study is conducted by the Institu-tional Review Board at the researchsite, the Naval Health Research Cen-ter (Protocol NHRC.2000.0007).Moreover, regular scientific peer-review by the American Institute ofBiological Sciences, DMDC reviewof survey content, Office of Manage-ment and Budget reviews of science,Defense Health Board review of sci-ence, and a yearly scientific steeringand advisory committee meeting ofleading academicians, veterans ser-vice organizations representatives,and military representatives help toguide the long-term study.10
SupportThe study is funded by the Depart-
ment of Defense through the USArmy Medical Research MaterielCommand (USAMRMC) MilitaryOperational Medicine Research Pro-gram (MOMRP). The MillenniumCohort Study requires considerablefinancial and logistical support thatmust be projected and maintainedover the lengthy period of observa-tion. This takes a large and dedicatedstaff of professionals who under-stand the complexities of conductinga cohort study of this size and who
continually strive to find ways tomake the process more efficient. Thestudy is conducted at the NavalHealth Research Center (NHRC) inSan Diego by a multidisciplinaryteam of epidemiologists, statisti-cians, physicians, research assistants,and data programmers.
Exposure MetricsExposure assessment is important
for hypothesis-driven research aswell as controlling for confoundingthat may affect research conclusions.In health-related studies, it is importantto assess and control for behavioralexposures. The Millennium Cohortsurvey assesses alcohol use, tobaccouse, complementary and alternativetherapies, body mass index, physicalactivity, and nutritional supplementuse. It is difficult to completely as-sess occupational exposures and todifferentiate between those occurringas a result of one’s occupation andthose occurring in conjunction withpersonal nonoccupational settings.The Millennium Cohort survey as-sesses personal and family stressorsthat include changes in residence, jobchanges, suffering sexual or physicalassaults, and death or severe illness
of family members. In addition toassessing changes in job descriptionthrough military occupational spe-cialty codes as well as self-reportedjob codes, occupational exposuresassessed include jobs requiring pro-tective equipment, routine skin con-tact with paint and/or solvents,microwaves, and pesticides. Military-specific exposures assessed includewitnessing a person’s death due towar, disaster, or tragic event; wit-nessing instances of physical abuse;seeing dead or decomposing bodiesor prisoners of war; or being exposedto or provided with countermeasuresfor chemical/biological/radiological(CBR) warfare agents or depleteduranium. Assessment of exposuresspecific to military deployment in-clude feeling in danger of beingkilled, being attacked or ambushed,receiving small-arms fire, clearinghomes or buildings, having an im-provised explosive devise explodenearby, being wounded or injured,seeing or handling human remains,knowing someone seriously injuredor killed, having members in unitseriously injured or killed, and beingdirectly responsible for death of non-combatants or enemy combatants.
ResultsThere are more than 150,000 con-
senting Millennium Cohort memberswho represent the US military indemographic, occupational, military,and health-related characteristics.Enrollment and follow-up cycles forthe first panel have resulted in77,047 completing the initial base-line survey (2001 to 2003), with55,021 completing the first fol-low-up (2004 to 2006). Also, as orig-inally designed, the Cohort was lateraugmented with 31,110 new acces-sions (personnel with 1 years to 3years of service) who completed abaseline survey between 2004 and2006, and again with �40,000 newaccessions who completed a baselinesurvey between 2007 and 2008.More than 70% of Cohort memberswho submitted baseline data havesubmitted a follow-up questionnaire.
Fig. 1. The multiple complementary electronic data sources that are or that may be linked toMillennium Cohort self-reported data.
1196 Millennium Cohort Longitudinal Follow-Up • Smith

Demographic data for the Cohort arepresented in Table 2. For comparisonpurposes of the Cohort to the USmilitary in general, a snap shot of the
US Military in 2008 is presented inTable 2 stratified by active duty andReserve/National Guard status. Atbaseline, the active duty portion of
the Cohort (�60%) comprised�70% men, 80% younger than 34years, 70% with a high school di-ploma or equivalent, 50% married,
TABLE 2Characteristics of Millennium Cohort Study Participants and US Military Personnel at 2008
Characteristic
Active Dutya
Millennium CohortMembers (%)
Active Duty USMilitary Personnel
in 2008b (%)
Reserve or National Guarda
Millennium CohortMembers (%)
Reserve or National GuardUS Military Personnel in
2008b (%)
GenderMale 69.6 85.8 65.8 83.2Female 30.4 14.2 34.2 16.8
Age, yr17–24 47.8 33.9 29.9 19.325–34 34.8 40.8 30.3 34.335–44 15.1 20.8 25.0 20.1�44 2.3 4.5 14.8 26.3
EducationLess than high school diploma 4.5 8.8 15.8 19.6High school diploma diploma/
equivalent64.9 67.2 42.6 53.1
Some college 13.0 6.1 16.9 6.1Bachelor’s degree 12.3 11.9 18.1 14.9Advanced degree 5.3 6.0 6.6 6.3
Marital statusSingle 48.6 40.5 44.8 41.1Married 48.2 55.3 47.9 51.7Divorced 3.2 4.2 7.3 7.2
Race/ethnicityWhite non-Hispanic 67.5 62.8 76.3 66.4Black non-Hispanic 13.3 16.0 11.5 13.3Asian/Pacific Islander 8.5 4.8 3.4 3.3Hispanic 8.0 10.3 6.8 8.4Native American 1.5 1.8 1.0 1.3Other/unknown 1.2 4.3 1.0 7.3Operation Iraqi Freedom/
Operation Enduring Freedomdeployment statusc
Deployment experience 55.0 56.6 40.7 40.4No deployment experience 45.0 43.4 59.3 59.6
Military pay gradeEnlisted 84.6 84.2 79.1 82.5Officer 15.4 15.8 20.9 17.5
Branch of serviceArmy 34.6 37.1 59.7 54.6Air Force 30.5 23.1 27.0 21.9Navy/Coast Guard 22.8 26.3 10.2 14.3Marine Corps 12.1 13.5 3.1 9.2
Occupational categoryCombat specialists 18.3 22.4 16.6 17.9Electrical repair 10.3 8.8 6.7 5.2Communications/intelligence 9.7 8.8 5.6 5.8Health care specialists 10.0 8.2 12.1 7.8Other technical 3.3 2.9 2.7 3.1Functional support specialists 16.8 16.0 21.9 20.5Electrical/mechanic 17.0 17.2 12.1 13.1Craft workers 2.8 3.1 4.0 5.1Service support 8.6 9.6 11.2 13.1Students, trainees, other 3.2 3.0 7.1 8.4
aCharacteristic measured at the time of baseline invitation.bBased on US military rosters as of March 2008 with complete demographic data.cDeployment experience recorded as of March 2008.
JOEM • Volume 51, Number 10, October 2009 1197

90% enlisted, 35% Army personnel,15% combat specialists, and 10%health care specialists. At baseline,the Reserve and National Guard por-tion of the Cohort (�40%) com-prised �70% men, 60% youngerthan 34 years, 55% with a highschool diploma or equivalent, 50%married, 75% enlisted, 60% Armypersonnel, 15% combat specialists,and 10% health care specialists.These baseline military and demo-graphic characteristics reasonablyreflect the composition of the USmilitary in 2008. Although the Co-hort is a good reflection of the com-position of the US military, there arenoticeable differences in the activeduty Cohort members when com-pared with active duty in March2008 with the Cohort comprisingproportionately more women,younger, educated, single, whitenon-Hispanic, Air Force, and withsome deployment experience insupport of the wars in Iraq andAfghanistan when compared withthe military in general. Moreover,there are noticeable differences inthe Reserve/Guard Cohort mem-bers when compared with all Re-serve/Guard in March 2008 withthe Cohort comprising proportion-ately more women, educated, whitenon-Hispanic, and officers than inthe general military.
Investigations have focused onestablishing reliability and represen-tativeness of Cohort data, cross-sectional prevalence studies, andprospective analyses using two datapoints in time. Future analyses usingrepeated health and exposure assess-ments will yield a significant andexponential increase in inferentialcapability (Fig. 2). To date, �50% ofthe 150,000 Cohort members havedeployed in support of the wars inIraq or Afghanistan. Data analyseshave been performed using SAS sta-tistical software version 9.1 (SASInstitute, Inc., Cary, NC).
DiscussionThe Millennium Cohort Study was
created after lessons learned from the
1991 Gulf War, which made itapparent that a well-designed pro-spective cohort study was critical toadequately investigate long-termhealth consequences associated withmilitary service. The Cohort allowsfor robust comparisons of deployedand nondeployed, active-duty andReserve and National Guard mem-bers across all services. Using datafrom the Millennium Cohort Study,recent research has uniquely in-cluded active duty, Reserve, andNational Guard members from allservices and focused on comparisonsof populations including deployedwithout reported combat exposures,deployed with reported combat ex-posures, and nondeployed. Prospec-tive analyses of those deployed insupport of the wars in Iraq and Af-ghanistan and those not deployedhave answered questions regardingnewly reported respiratory symp-toms and conditions (Smith et al,unpublished data, 2008), hyperten-sion,29 PTSD symptoms,30,31 depres-sion,32 disordered eating,33 newlyreported cigarette smoking,34 andnewly reported problem alcoholdrinking.35
Never before has such a large pop-ulation-based cohort had the abilityto link to a multitude of electronicdata including inpatient and outpa-tient health care21,36 pharmaceuticalprescriptions (Granado et al, unpub-lished data), vaccinations,22–25,37,38
the DoD Birth and Infant HealthRegistry,39 the DoD Serum Reposi-
tory,40 mortality while in service andpost service,41 exposure data col-lected and maintained by the USArmy Center for Health Promotionand Preventive Medicine,42–44 con-tingency/deployment data,45 and VAhealth and mortality data26 after sep-aration from military service. Theseelectronic DoD and VA data allowfor the observation of a full spectrumof health exposures and outcomesand significantly strengthens the ca-pability of this longitudinal cohortstudy (Fig. 1).
At baseline, the Millennium Co-hort Study enrolled and consented36% of those invited to participatein the 21-year study.10 Understand-ing the limitations or potential biasesof this cohort is paramount to long-term inferential capabilities. Concernsover generalizability, reliability ofself-reported data, and loss to fol-low-up are inherent in longitudinalcohort studies caused by these limi-tations. The Millennium Cohortstudy Team has made great efforts toinvestigate potential biases. Weightshave been created and employed forthe inverse of the sampling schemeas well as for the inverse of responsedifferences with minimal differencesin results.46,47 Analyses have shownno differential in responder healthwith respect to hospitalization andoutpatient encounters in the yearprior to enrollment, suggesting thatprior health did not effect enroll-ment.36 Reliability of reporting as-sessed using both test-retest analyses
Fig. 2. The planned longitudinal design of the US DoD Millennium Cohort Study until 2022and the potential temporal increase of research benefit.
1198 Millennium Cohort Longitudinal Follow-Up • Smith

and internal consistency investiga-tion of standardized scores,14 andsimilar reporting in comparisons ofself-report to electronic vaccinationdata,23,24 occupational data,48 anddeployment data has been estab-lished.49 Additional analyses haveshown minimal differences betweenparticipants choosing Web submis-sion versus paper submission,27 andstrategies for retention are providingpositive results.28 Although the Mil-lennium Cohort study Team hasworked hard to maximize retention,which has resulted in a follow-uprate of �70%, analyses of responsein separated and nonseparated per-sonnel as well as potential responderbias to follow-up are ongoing.
Current areas of research includeinvestigations differentiated by de-ployment focusing on diabetes, weightchange, hearing loss, migraine head-aches, unit cohesion, complementaryand alternative medicine and healthcare use, complementary and alterna-tive medicine use and mental healthsymptoms and diagnoses, physical ac-tivity and PTSD symptoms, profes-sional care provider occupations andPTSD and depression symptoms,chronic multisymptom illnesses andassociated comorbidities, motor vehi-cle accidents among deployers, andmortality.
Future strategic research plans in-clude conducting augmented contactand focused surveys; neurocognitivetesting of select subsamples of theCohort; neuroimaging of select sub-samples of the Cohort; biologicalsampling using blood/DNA/RNA;linking to accession data in the Re-cruit Assessment Program; continu-ing investigations of biases and lossto follow-up; longitudinal investiga-tion of effects of multiple deploy-ments on mental and functionalhealth; longitudinal investigation ofresolution and new onset of mentalhealth morbidity including PTSD;longitudinal investigation of resolu-tion and new onset of alcohol use/misuse; longitudinal evaluation ofnew, reuptake, or varied use of to-bacco (smoking cigarettes or cigars,
or using smokeless tobacco); longi-tudinal investigation of mild trau-matic brain injury; longitudinalinvestigation of respiratory condi-tions and illnesses; chronic sleepingdeficiencies and mental symptoms;physical activity and persistence orresolution of mental health disorders;investigation of long-term chronicillnesses, such as diabetes and hyper-tension, and their impact on militaryservice; chronic conjunctivitis andtrachoma among deployed servicemembers; longitudinal assessment ofmortality; parental stress associatedwith deployment and birth-relatedoutcomes; and family unit stress; andhealth effects associated with mili-tary-unique occupational exposures.
Although the cohort design offerssuperior inferential capability overother observational studies, there arelimitations and strengths that shouldbe discussed. Limitations to cohortstudies include how generalizablethe responders are to the rest of themilitary, self-reporting of symptomsand reporting of exposures, loss tofollow-up, and rare outcomes thatwould not allow the statistical powerto establish exposure to outcome in-ferences. Strengths to this cohort de-sign include the ability to temporallyinvestigate an exposure and healthoutcome, to detect outcomes withlonger latency, and to ascertainsymptom duration, resolution, andchronicity of the symptoms and ill-nesses being measured. Unique tothe Millennium Cohort Study is theadditional strength of being able tolink these data to a wealth of DoDand VA electronic data that includepersonnel files, birth and infanthealth, inpatient and outpatienthealth care use, pharmaceutical use,vaccination experience, deploymentexperience, exposures, and mortality(Fig. 1).
Funded by the DoD through theUSAMRMC MOMRP and con-ducted at NHRC with coinvestiga-tors from all services and the VA,this large study symbolizes triserviceand VA cooperation needed to effec-tively assess career-span health out-
comes now and beyond militaryservice. The uniqueness of thisstudy’s temporal inception, which al-lowed launching before September11, 2001, and the beginning of com-bat deployments in Afghanistan andIraq with continued assessment, willyield answers to leadership for yearsto come. The sustained high opera-tional tempo since September 2001has been marked by significant com-bat operations, multiple and oftenlengthy deployments, and higherrates of postdeployment mentalhealth morbidity associated withcombat deployment.30,50,51 US fight-ing personnel have never been betterequipped with advanced weaponryand body armor on the battlefield,nor has a better strategic long-termcohort study been implemented toanswer health concerns after servicemembers return and long after de-ployments conclude. PTSD, mildtraumatic brain injuries (concus-sions), and mental health morbidityremain a significant challenge forboth the service member and themedical community, potentially foryears to come. The Millennium Co-hort Study, currently in its eighthyear, will continue to answer healthconcerns now and into the future.
AcknowledgmentsThis work represents report 08–38, sup-
ported by the Department of Defense, underwork unit no. 60002. The views expressed inthis article are those of the authors and do notreflect the official policy or position of theDepartment of the Navy, Department of theArmy, Department of the Air Force, Depart-ment of Defense, Department of VeteransAffairs, or the US Government. This re-search has been conducted in compliance withall applicable federal regulations governing theprotection of human subjects in research (Pro-tocol NHRC.2000.007).
We are indebted to the Millennium CohortStudy participants, without whom these anal-yses would not be possible. In addition to theauthors, the Millennium Cohort Study Teamincludes Paul J. Amoroso, MD, MPH, fromthe Madigan Army Medical Center, Tacoma,WA; Edward J. Boyko, MD, MPH, from theSeattle Epidemiologic Research and Informa-tion Center, Veterans Affairs Puget SoundHealth Care System, Seattle, WA; Gary D.
JOEM • Volume 51, Number 10, October 2009 1199

Gackstetter, DVM, MPH, PhD, from AnalyticServices, Inc. (ANSER), Arlington, VA;Gregory C. Gray, MD, MPH, from the Col-lege of Public Health, University of Iowa,Iowa City, IA; Tomoko I. Hooper, MD, MPH,from the Department of Preventive Medicineand Biometrics, Uniformed Services Univer-sity of the Health Sciences, Bethesda, MD;James R. Riddle, DVM, MPH, from the AirForce Research Laboratory, Wright-PattersonAir Force Base, OH; Timothy S. Wells,DVM, MPH, PhD from the Air Force Re-search Laboratory, Wright-Patterson AirForce Base, OH; Margaret A. K. Ryan, MD,MPH, Naval Hospital Camp Pendleton, Oc-cupational Health Department; Lacy Farnell;Gia Gumbs, MPH; Nisara Granado, MPH,PhD; Jaime Horton; Isabel Jacobson, MPH;Kelly Jones; Molly Kelton, MS; CynthiaLeardMann, MPH; Travis Leleu; JamieMcGrew; Besa Smith, MPH, PhD; DonaldSandweiss, MD; Amber Seelig, MPH;Katherine Snell; Steven Speigle; Kari Welch,MA; Martin White, MPH; James Whitmer;and Charlene Wong, MPH; from the Depart-ment of Defense Center for DeploymentHealth Research, Naval Health Research Cen-ter, San Diego, CA.
We thank Scott L. Seggerman and Greg D.Boyd from the Management Information Di-vision, Defense Manpower Data Center, Sea-side, CA. Additionally we thank MichelleStoia from the Naval Health Research Center.We also thank all the professionals from theUS Army Medical Research and MaterielCommand, especially those from the MilitaryOperational Medicine Research Program,Fort Detrick, MD. We appreciate the supportof the Henry M. Jackson Foundation for theAdvancement of Military Medicine, Rock-ville, MD.
References1. Dawber TR, Meadors GF, Moore FE.
Epidemiological approaches to heart dis-ease: the Framingham Study. Am J Pub-lic Health. 1951;41:279–286.
2. Doll R, Hill HB. The mortality of doctorsin relation to their smoking habits: a pre-liminary report. BMJ. 1954;1:1451–1455.
3. Willett WC, Hennekens CH, Bain C, Ros-ner B, Speizer FE. Cigarette smoking andnon-fatal myocardial infarction in women.Am J Epidemiol. 1981;113:575–582.
4. Doll R. The causes of death among gas-workers with special reference to cancer ofthe lung. Br J Ind Med. 1952;9:180–185.
5. Case RA, Pearson JT. Tumours of theurinary bladder in workmen engaged inthe manufacture and use of certain dye-stuff intermediates in the British chemi-cal industry. II. Further consideration of
the role of aniline and of the manufactureof auramine and magenta (fuchsine) aspossible causative agents. Br J Ind Med.1954;11:213–216.
6. Eisen SA, Kang HK, Murphy FM, et al.Gulf War veterans’ health: medical eval-uation of a US cohort. Ann Intern Med.2005;142:881–890.
7. McDiarmid MA, Engelhardt SM, OliverM, et al. Health surveillance of Gulf WarI veterans exposed to depleted uranium:updating the cohort. Health Phys. 2007;93:60–73.
8. Hotopf M, David AS, Hull L, NikalaouV, Unwin C, Wessely S. Gulf War ill-ness—better, worse, or just the same? Acohort study. BMJ. 2003;327:1370.
9. Wolfe WH, Michalek JE, Miner JC, et al.Health status of Air Force veterans occu-pationally exposed to herbicides in Viet-nam. I. Physical health. JAMA. 1990;264:1824–1831.
10. Ryan MA, Smith TC, Smith B, et al.Millennium Cohort: enrollment begins a21-year contribution to understanding theimpact of military service. J Clin Epide-miol. 2007;60:181–191.
11. Gray GC, Chesbrough KB, Ryan MAK,et al. The Millennium Cohort Study: a21-year prospective cohort study of140,000 military personnel. Mil Med.2002;167:483–488.
12. Secretary of Defense. Report to the Com-mittee on National Security, House ofRepresentatives, and the Armed ServicesCommittee, U.S. Senate, on Effectivenessof Medical Research Initiatives Regard-ing Gulf War Illnesses. Washington, DC:Department of Defense; 1998.
13. Committee on Measuring the Health ofGulf War Veterans IoM. Gulf War Vet-erans: Measuring Health. Washington,DC: National Academy Press; 1999.
14. Smith TC, Smith B, Jacobson IG, CorbeilTE, Ryan MA; for the Millennium Co-hort Study Team. Reliability of standardhealth assessment instruments in a large,population-based cohort study. Ann Epi-demiol. 2007;17:271–284.
15. Kroenke K, Spitzer RL. The PHQ-9: anew depression diagnostic and severitymeasure. Psychiatr Ann. 2002;32:509–521.
16. Spitzer RL, Williams JB, Kroenke K, etal. Utility of a new procedure for diag-nosing mental disorders in primary care.The PRIME-MD 1000 Study. JAMA.1994;272:1749–1756.
17. Spitzer RL, Kroenke K, Williams JB.Validation and utility of a self-reportversion of PRIME-MD: the PHQ PrimaryCare Study. Primary care evaluation ofmental disorders. Patient Health Ques-tionnaire. JAMA. 1999;282:1737–1744.
18. Spitzer RL, Williams JB, Kroenke K,Hornyak R, McMurray J. Validity andutility of the PRIME-MD Patient HealthQuestionnaire in assessment of 3000 ob-stetric-gynecologic patients: thePRIME-MD Patient Health Question-naire Obstetrics-Gynecology Study. Am JObstet Gynecol. 2000;183:759–769.
19. Kazis LE, Ren XS, Lee A, et al. Healthstatus in VA patients: results from theVeterans Health Study. Am J Med Qual.1999;14:28–38.
20. Ewing JA. Detecting alcoholism. TheCAGE questionnaire. JAMA. 1984;252:1905–1907.
21. Smith B, Chu LK, Smith TC, et al.Challenges of self-reported medicalconditions and electronic medicalrecords among members of a largemilitary cohort. BMC Med Res Meth-odol. 2008;8:37.
22. Wells TS, Sato PA, Smith TC, Wang LZ,Reed RJ, Ryan MA. Military hospitaliza-tions among deployed US service mem-bers following anthrax vaccination,1998–2001. Hum Vaccin. 2006;2:54–59.
23. LeardMann CA, Smith B, Smith TC,Wells TS, Ryan MA; for the MillenniumCohort Study Team. Smallpox vaccina-tion: comparison of self-reported andelectronic vaccine records in the Millen-nium Cohort Study. Hum Vaccin. 2007;3:245–251.
24. Smith B, Leard CA, Smith TC, Reed RJ,Ryan MA; for the Millennium CohortStudy Team. Anthrax vaccination in theMillennium Cohort: validation and mea-sures of health. Am J Prev Med. 2007;32:347–353.
25. Wells TS, LeardMann CA, Smith TC, etal. Self-reported adverse health eventsfollowing smallpox vaccination in a largeprospective study of US military servicemembers. Hum Vaccin. 2008;4:127–133.
26. Boyko EJ, Koepsell TD, Gaziano JM,Horner RD, Feussner JR. US Departmentof Veterans Affairs medical care systemas a resource to epidemiologists. Am JEpidemiol. 2000;151:307–314.
27. Smith B, Smith TC, Gray GC, Ryan MA;for the Millennium Cohort Study Team.When epidemiology meets the Internet:web-based surveys in the MillenniumCohort Study. Am J Epidemiol. 2007;166:1345–1354.
28. Welch KE, LeardMann CA, Jacobson IG,et al. Postcards encourage participant up-dates. Epidemiology. 2009;20:313–314.
29. Granado NS, Smith TC, Swanson GM, etal. Newly-reported hypertension aftermilitary combat deployment in a largepopulation-based study. Hypertension.2009; In press.
1200 Millennium Cohort Longitudinal Follow-Up • Smith

30. Smith TC, Wingard DL, Ryan MA,Kritz-Silverstein D, Slymen DJ, Sallis JF;Millennium Cohort Study Team. Priorassault and posttraumatic stress disorderafter combat deployment. Epidemiology.2008;19:505–512.
31. Smith TC, Ryan MA, Wingard DL, Sly-men DJ, Sallis JF, Kritz-Silverstein D;Millennium Cohort Study Team. Newonset and persistent symptoms of post-traumatic stress disorder self reportedafter deployment and combat exposures:prospective population based US militarycohort study. BMJ. 2008;336:366–371.
32. Wells TS, LeardMann CA, Fortuna SO,et al, for the Millennium Cohort StudyTeam. A prospective study of depressionfollowing combat deployment in supportof the wars in Iraq and Afghanistan. Am JPublic Health. 2009; In press.
33. Jacobson IG, Smith TC, Smith B, et al,for the Millennium Cohort Study Team.Disorderd eating and weight changes af-ter deployment: longitudinal assessmentof a large US military cohort. Am JEpidemiol. 2009;169:415–427.
34. Smith B, Ryan MA, Wingard DL, Patter-son TL, Slymen DJ, Macera CA; Millen-nium Cohort Study Team. Cigarettesmoking and military deployment: a pro-spective evaluation. Am J Prev Med.2008;35:539–546.
35. Jacobson IG, Ryan MA, Hooper TI, et al.Alcohol use and alcohol-related problemsbefore and after military combat deploy-ment. JAMA. 2008;300:663–675.
36. Wells TS, Jacobson IG, Smith TC, et al;Millennium Cohort Study Team. Priorhealth care utilization as a potential de-terminant of enrollment in a 21-year pro-spective study, the Millennium CohortStudy. Eur J Epidemiol. 2008;23:79–87.
37. Sato PA, Reed RJ, Smith TC, Wang L.Monitoring anthrax vaccine safety in USmilitary service members on active duty:surveillance of 1998 hospitalizations intemporal association with anthrax immu-nization. Vaccine. 2002;20:2369–2374.
38. Ryan MA, Smith TC, Sevick CJ, et al.Birth defects among infants born towomen who received anthrax vaccine inpregnancy. Am J Epidemiol. 2008;168:434–442.
39. Ryan MA, Pershyn-Kisor MA, HonnerWK, Smith TC, Reed RJ, Gray GC. TheDepartment of Defense Birth Defect Reg-istry: overview of a new surveillancesystem. Teratology. 2001;64:S26–S29.
40. Rubertone MV, Brundage JF. The De-fense Medical Surveillance System andthe Department of Defense serum repos-itory: glimpses of the future of publichealth surveillance. Am J Public Health.2002;92:1900–1904.
41. Gardner JW, Cozzini CB, Kelley PW, etal. The Department of Defense MedicalMortality Registry. Mil Med. 2000;165(7, Suppl 2):57–61.
42. May LM, Weese C, Ashley DL, TrumpDH, Bowling CM, Lee AP. The recom-mended role of exposure biomarkers forthe surveillance of environmental andoccupational chemical exposures in mil-itary deployments: policy considerations.Mil Med. 2004;169:761–767.
43. Smith TC, Gray GC, Weir JC, Heller JM,Ryan MA. Gulf War veterans and Iraqinerve agents at Khamisiyah: postwar hos-pitalization data revisited. Am J Epide-miol. 2003;158:456–467.
44. Smith TC, Heller JM, Hooper TI, Gack-stetter GD, Gray GC. Are veterans of theGulf War experiencing illness from ex-posure to Kuwaiti oil well fire smoke?Department of Defense hospitalization
data examined. Am J Epidemiol. 2002;155:908–917.
45. Smith B, Wingard DL, Ryan MA, MaceraCA, Patterson TL, Slymen DJ. US militarydeployment during 2001–2006: compari-son of subjective and objective data sourcesin a large prospective health study. AnnEpidemiol. 2007;17:976–982.
46. Smith TC, Zamorski M, Smith B, et al;Millennium Cohort Study Team. Thephysical and mental health of a largemilitary cohort: baseline functionalhealth status of the Millennium Cohort.BMC Public Health. 2007;7:340.
47. Riddle JR, Smith TC, Smith B, et al; forthe Millennium Cohort Study Team. Mil-lennium Cohort: the 2001–2003 baselineprevalence of mental disorders in the USmilitary. J Clin Epidemiol. 2007;60:192–201.
48. Smith TC, Jacobson IG, Smith B, HooperTI, Ryan MA; for the Millennium CohortStudy Team. The occupational role ofwomen in military service: validation ofoccupation and prevalence of exposuresin the Millennium Cohort Study. Int JEnviron Health Res. 2007;17:271–284.
49. Davidson J, Smith R, Kudler H. Validityand reliability of the DSM-III criteria forposttraumatic stress disorder. Experiencewith a structured interview. J Nerv MentDis. 1989;177:336–341.
50. Milliken CS, Auchterlonie JL, Hoge CW.Longitudinal assessment of mental healthproblems among active and reserve com-ponent soldiers returning from the IraqWar. JAMA. 2007;298:2141–2148.
51. Hoge CW, Auchterlonie JL, Milliken CS.Mental health problems, use of mentalhealth services, and attrition from mili-tary service after returning from deploy-ment to Iraq or Afghanistan. JAMA.2006;295:1023–1032.
JOEM • Volume 51, Number 10, October 2009 1201

REPORT DOCUMENTATION PAGE
The public reporting burden for this collection of information is estimated to average 1 hour per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing the burden, to Washington Headquarters Services, Directorate for Information Operations and Reports, 1215 Jefferson Davis Highway, Suite 1204, Arlington, VA 22202-4302, Respondents should be aware that notwithstanding any other provision of law, no person shall be subject to any penalty for failing to comply with a collection of information if it does not display a currently valid OMB Control number. PLEASE DO NOT RETURN YOUR FORM TO THE ABOVE ADDRESS.
1. REPORT DATE (DD MM YY) 01 09 08
2. REPORT TYPE Journal submission
3. DATES COVERED (from – to) 1 January2001 to 30 Dec2008
4. TITLE AND SUBTITLE The U.S. Department of Defense Millennium Cohort Study: Career Span and Beyond Longitudinal Follow-Up
6. AUTHORS Tyler C. Smith, MS, PhD; for the Millennium Cohort Team
5a. Contract Number: 5b. Grant Number: 5c. Program Element Number: 5d. Project Number: 5e. Task Number: 5f. Work Unit Number: 60002 7. PERFORMING ORGANIZATION NAME(S) AND ADDRESS(ES)
Commanding Officer Naval Health Research Center 140 Sylvester Rd San Diego, CA 92106-3521
8. PERFORMING ORGANIZATION REPORT NUMBER
Report No. 08-38
10. SPONSOR/MONITOR’S ACRONYM(S) NMRC/NMSC
8. SPONSORING/MONITORING AGENCY NAMES(S) AND ADDRESS(ES) Commanding Officer Commander Naval Medical Research Center Navy Medicine Support Command 503 Robert Grant Ave P.O. Box 140 Silver Spring, MD 20910-7500 Jacksonville, FL 32212-0140 11. SPONSOR/MONITOR’S REPORT
NUMBER(s)
12. DISTRIBUTION/AVAILABILITY STATEMENT Approved for public release; distribution is unlimited.
13. SUPPLEMENTARY NOTES
14. ABSTRACT Objective To describe current and future career-span strategic health research in the US Department of Defense (DoD) Millennium Cohort Study. Methods In response to concerns after the 1991 Gulf War, the Millennium Cohort Study was launched in the late 1990s. Based on recommendations by the US DoD, US Congress, and the Institute of Medicine, the study involves coordinated strategic research to determine the effect of military occupational exposures, including deployment-related exposures, on long-term health. In collaboration with all military service branches and the Department of Veterans Affairs, the Millennium Cohort Study was launched in 2001, prior to September 11 and the start of the wars in Afghanistan and Iraq. Results More than 150,000 consenting Millennium Cohort members represent the US military demographic, occupational, military, and health characteristics. Over 75% of Cohort members have submitted a follow-up questionnaire with nearly 50% deploying in support of the wars in Iraq and Afghanistan. Conclusions Cohort data have prospectively yielded insight into vulnerability and resiliency of mental and physical health morbidity. Continued follow-up of this cohort, career span and beyond, will answer long-term health questions related to military service.
15. SUBJECT TERMS military personnel, prospective cohort, deployment health
16. SECURITY CLASSIFICATION OF: 18a. NAME OF RESPONSIBLE PERSON Commanding Officer a. REPORT
UNCL b. ABSTRACT
UNCL c. THIS PAGE
UNCL
17. LIMITATION OF ABSTRACT
UNCL
18. NUMBER OF PAGES
9 18b. TELEPHONE NUMBER (INCLUDING AREA CODE)
COMM/DSN: (619) 553-8429
Standard Form 298 (Rev. 8-98)Prescribed by ANSI Std. Z39-18





























