Embed Size (px)
Citation preview
Clinical Radiology (1986) 37,495-498 0009-9260/86/713495502.00 © 1986 Royal College of Radiologists
The Urographic Appearances of Ureteric Obstruction Secondary to Bladder Carcinoma SIMON ELLIOTT and PETER DAVIES
Department of Radiology, City Hospital, Nottingham NG5 1PB
It is usually assumed as a result of experiments that post-obstructive and hydronephrotic atrophy are due to raised intrapelvic pressure. In acute ureteric obstruc- tion raised intrapelvic pressure is associated with renal colic; the absence of pain in chronic obstruction has been a stumbling block to acceptance of the back pressure theory.
In ureteric obstruction due to bladder carcinoma the complete spectrum of nephrographic appearances ranging from those of high pressure obstruction to low pressure obstruction is seen in the absence of pain.
This shows that acute ureteric obstruction may be painless and therefore post-obstructive and hyd- ronephrotic atrophy may be preceded in man by a raised intrapelvic pressure. This removes the stumbling block.
The various urographic appearances due to ureteric obstruction have been previously described (Davies, 1982). It has also been reported that the dense nephrogram associated with acute obstruction may occur without pain, However this phenomenon has not been well documented. This is of considerable importance in supporting the hypothesis that post- obstructive atrophy is secondary to a previously high intrapelvic pressure (Hodson and Craven, 1966). In order to document painless acute ureteric obstruction, we reviewed cases of ureteric obstruction secondary to bladder carcinoma.
PATIENTS AND METHODS
From histopathology records, the names of all patients from whom transitional cell tumours had been excised in the previous two years were obtained. The films and notes were reviewed and cases showing ureteric obstruction were selected.
Intravenous urography (IVU) was performed by rapid injection of a bolus of 50ml of sodium iothala- mate 70% (Conray 420, May & Baker Ltd).
Classification of Urographic Appearances
Type 1. The increasingly dense nephrogram not followed by a pyelogram which we feel reflects a very high intrapelvic pressure.
Type 2. An increasingly dense nephrogram followed by a normal or dense pyelogram which is normal or minimally dilated - simple acute obstruction, as usu- ally seen in patients with renal colic due to stones causing a raised intrapelvic pressure.
Type 3. A nephrogram persisting with the same
density not followed by a pyelogram representing perhaps a post-acute state with a high intrapelvic pressure.
Type 4. A persistent nephrogram followed by a faint or normal pyelogram indicating a post-acute but low pressure state.
Type 5. The faint nephrogram with dilated pelvi- calyceal system of chronic obstruction.
Type 6. A combination of signs: increasingly dense nephrogram with a dilated pelvicalyceal system, i.e. acute-on-chronic obstruction. (Davies and Price, 1980).
RESULTS
The intravenous urograms of 36 patients with ureteric obstruction secondary to bladder carcinoma were analysed. Clinical records were available in 25 of these patients. There were 24 men (mean age 64 years, range 50-84 years) and 12 women (mean age 61 years, range 34-79 years).
Forty-five kidneys were obstructed; in 10 patients both kidneys were affected and in 25 only one was affected (Table 1). Follow-up urography was available on 16 kidneys in 13 patients (Table 2). Three patients had kidneys showing an increasingly dense nephro- gram which did not proceed to a pyelogram within the time of the examination (up to 4h). One of these patients had follow-up urography which showed the kidney was smaller with a nephrogram of normal density and a hydronephrotic calyceal system (hyd- ronephrotic post-obstructive atrophy).
Two patients had simple acute obstruction with an increasingly dense nephrogram and normal or mini- mally dilated pelvicalyceal system. Two months later, one patient had passed into a post-acute state with.a dilated pyelogram and faint nephrogram with no change in renal size; in the other patient the urogram had returned to normal.
Ten patients had evidence of post-acute obstruction with a persistent nephrogram and a dilated pelvicaly- ceal system which filled slowly. A further nine kidneys had persistent nephrograms which did not proceed to pyelograms. Those kidneys with persistent nephro- grams and opacified pelvicalyceal systems showed a varying degree of calyceal dilatation. Three were minimally dilated, three moderately dilated and four markedly hydronephrotic. Follow-up urography showed one returning to normal from a grossly hydronephrotic state, one proceeding to post- obstructive atrophy with a normal pelvicalyceal sys- tem, two appearing unchanged after 20 months and one proceeding to chronic obstruction.
Three patients had evidence of preceding chronic
496
Table 1 - Type of obstruction on presentation
CLINICAL RADIOLOGY
Type Description No. of cases
'High pressure acute' 3 Acute (raised pressure) 3 Raised pressure post-acute 9 Low pressure post-acute 10 Chronic (low pressure) 17 Acute-on-chronic (raised pressure) 3
Type 1 Type 2 Type 3 Type 4 Type 5 Type 6
dence of post-obstructive atrophy. Clinical informa- tion was available in five patients.
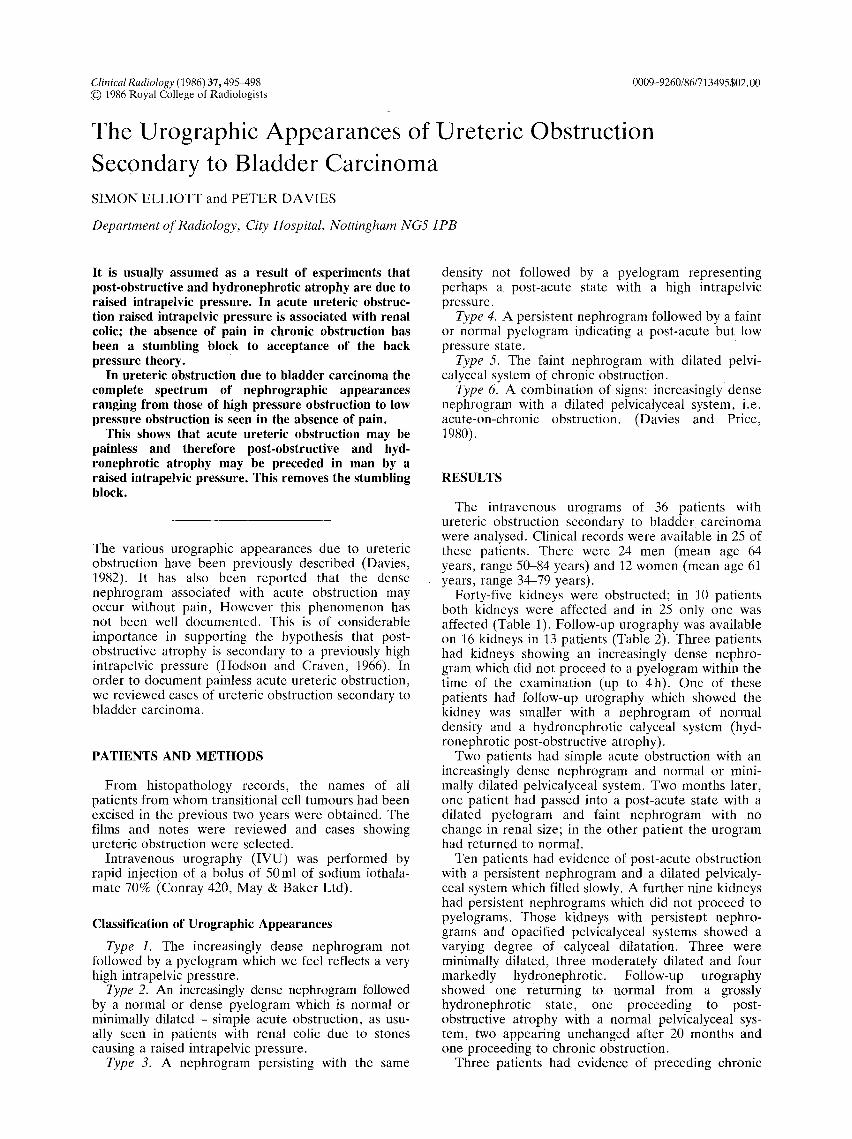
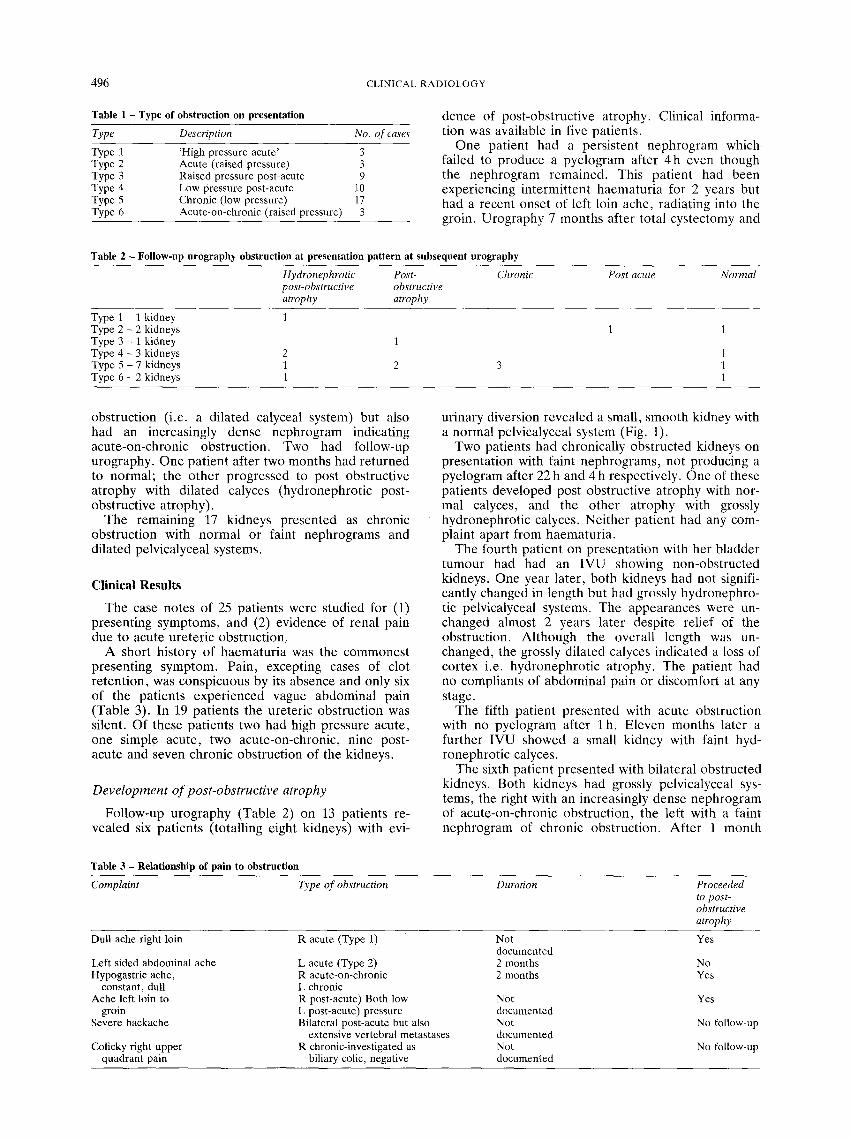
One patient had a persistent nephrogram which failed to produce a pyelogram after 4h even though the nephrogram remained. This patient had been experiencing intermittent haematuria for 2 years but had a recent onset of left loin ache, radiating into the groin. Urography 7 months after total cystectomy and
Table 2 - Follow-up urography obstruction at presentation pattern at subsequent urography
Hydronephrotic Post- Chronic Post acute Normal post-obstructive obstructive atrophy atrophy
Type 1 - 1 kidney 1 Type 2 - 2 kidneys 1 1 Type 3 - 1 kidney 1 Type 4 - 3 kidneys 2 1 Type 5 - 7 kidneys 1 2 3 1 Type 6 - 2 kidneys 1 1
obstruction (i.e. a dilated calyceal system) but also had an increasingly dense nephrogram indicating acute-on-chronic obstruction. Two had follow-up urography. One patient after two months had returned to normal; the other progressed to post obstructive atrophy with dilated calyces (hydronephrotic post- obstructive atrophy).
The remaining 17 kidneys presented as chronic obstruction with normal or faint nephrograms and dilated pelvicalyceal systems.
C l i n i c a l R e s u l t s
The case notes of 25 patients were studied for (1) presenting symptoms, and (2) evidence of renal pain due to acute ureteric obstruction,
A short history of haematuria was the commonest presenting symptom. Pain, excepting cases of clot retention, was conspicuous by its absence and only six of the patients experienced vague abdominal pain (Table 3). In 19 patients the ureteric obstruction was silent. Of these patients two had high pressure acute, one simple acute, two acute-on-chronic, nine post- acute and seven chronic obstruction of the kidneys.
Deve lopmen t o f post-obstructive atrophy
Follow-up urography (Table 2) on 13 patients re- vealed six patients (totalling eight kidneys) with evi-
urinary diversion revealed a small, smooth kidney with a normal pelvicalyceal system (Fig. 1).
Two patients had chronically obstructed kidneys on presentation with faint nephrograms, not producing a pyelogram after 22 h and 4 h respectively. One of these patients developed post obstructive atrophy with nor- mal calyces, and the other atrophy with grossly hydronephrotic calyces. Neither patient had any com- plaint apart from haematuria.
The fourth patient on presentation with her bladder tumour had had an IVU showing non-obstructed kidneys. One year later, both kidneys had not signifi- cantly changed in length but had grossly hydronephro- tic pelvicalyceal systems. The appearances were un- changed almost 2 years later despite relief of the obstruction. Although the overall length was un- changed, the grossly dilated calyces indicated a loss of cortex i.e. hydronephrotic atrophy. The patient had no compliants of abdominal pain or discomfort at any stage.
The fifth patient presented with acute obstruction with no pyelogram after l h . Eleven months later a further IVU showed a small kidney with faint hyd- ronephrotic calyces.
The sixth patient presented with bilateral obstructed kidneys. Both kidneys had grossly pelvicalyceal sys- tems, the right with an increasingly dense nephrogram of acute-on-chronic obstruction, the left with a faint nephrogram of chronic obstruction. After 1 month
Table 3 - Relationship of pain to obstruction
Complaint Type of obstruction Duration Proceeded to post- obstructive atrophy
Dull ache right loin
Left sided abdominal ache Hypogastric ache,
constant, dull Ache left loin to
groin Severe backache
Colicky right upper quadrant pain
R acute (Type 1)
L acute (Type 2) R acute-on-chronic L chronic R post-acute) Both low L post-acute) pressure Bilateral post-acute but also
extensive vertebral metastases R chronic-investigated as
biliary colic, negative
Not documented 2 months 2 months
Not documented Not documented Not documented
Yes
No Yes
Yes
No follow-up
No follow-up
URETERIC OBSTRUCTION DUE TO BLADDER CANCER 497
(b)
(a)
Fig. 1 - (a) IVU showing obstruction to the left ureter producing a persistent nephrogram which subsequently failed to produce, i.e. a post acute state. (b) After cystectomy and urinary diversion there has been reduction in renal size with a non-dilated pelvicalyceal system, demonstrating the development of post-obstructive atrophy.
both kidneys had undergone significant reduction in renal length, but retained the dilated calyces.
DISCUSSION
The natural history of complete ureteric obstruction is of an acute stage with high intrapelvic pressure progressing over the next seven to 21 days to a chronic stage with a return to a normal intrapelvic pressure (Schweitzer, 1973). Some kidneys may develop ob- structive atrophy which is defined as a loss of renal cortex following a period of ureteric obstruction. The cortical loss may be seen in three basic forms: (1) a normal calibre pelvicalyceal system but with a reduc- tion in overall kidney length, (2) a small kidney with clubbed calyces and (3) maintenance of the overall kidney length but with dilatation of the pelvicalyceal system. It is not uncommon to find gross hyd- ronephrosis from pelvi-ureteric junction obstruction with no history of pain.
The mechanism of development of post-obstructive atrophy is uncertain but is most likely due to renal ischaemia secondary to the high intrapelvic pressure (Hodson and Craven, 1966). If, therefore, it can be shown that a high intrapelvic pressure can occur in the absence of pain, there is no bar to accepting the hypothesis that post-obstructive atrophy is due to the
high pressure. The raised pressure need not be con- tinuous.
One of the authors has previously seen (a) a dense nephrogram which was not followed by a pyelogram in calculous obstruction, (b) an increasingly dense nephrogram in calculous disease and primary pelvic hydronephrosis without pain and (c) a dense nephro- gram in bladder carcinoma without pain.
Although Bretland (1972) stated that the dense nephrogram reflecting the high intrapelvic pressure was invariably painful, this was in patients presenting with renal colic due to stones.
Patients presenting with ureters obstructed by blad- der carcinoma show the complete spectrum of uro- graphic changes secondary to the obstruction (Davies, 1982).
In our series, of the 25 patients with clinical details, 19 were asymptomatic and of these, five had indirect evidence of raised intrapelvic pressure in the absence of pain. Of the six patients complaining of some form of discomfort, none presented with renal colic and in none was the pain sufficient to require hospital attention. Three of the six had evidence of raised intrapelvic pressure.
We have documented the urographic signs of acute obstruction in the absence of renal colic and in most cases without any pain. This supports the hypothesis that post-obstructive and hydronephrotic atrophy is

498 CLINICAL RADIOLOGY
due to a p e r i o d of high in t rape lv ic p ressure . The type of pos t -obs t ruc t i ve a t r o p h y may be r e l a t ed to the deg ree or ra te of p r e s s u r e rise. Pe rhaps a small k idney with n o r m a l m o r p h o l o g y resul ts f rom a r a p i d rise to a very high p re s su re whi le h y d r o n e p h r o t i c a t r ophy is the resul t when the r ise is s lower and m o r e ins id ious a l lowing a d a p t a t i o n of the calyces.
Acknowledgements We are grateful for the help of Karen Kelly for typing the manuscript, and Janet Scothern for research assist- ance.
REFERENCES
Bretland, P. M. (1972). Acute Ureteric Obstruction. Butterworth, London.
Davies, P. (1982). Urographic appearances in renal failure due to intraluminal ureteric obstruction. Journal of the Royal Society of Medicine, 75, 768-771.
Davies, P. & Price H. (1980). Urographic signs of acute on chronic obstruction of the kidney. Clinical Radiology, 31,205-213.
Hodson, C. J. and Craven, J. O. (1966). The radiology of obstructive atrophy of the kidney, Clinical Radiology, 17, 305-320.
Schweitzer F. A, W. (1973) Intrapelvic pressure and renal function studies in experimental chronic partial ureteric obstruction. British Journal of Urology, 45, 2-7.
![The molecular biology of pelvi-ureteric junction obstruction · Intrinsic obstruction due to an adynamic stenotic segment at the PUJ is the most common aetiology (75% of cases) [4],](https://img.pdfslide.us/doc/110x75/6051d63dad763b5a0a72603a/the-molecular-biology-of-pelvi-ureteric-junction-obstruction-intrinsic-obstruction.jpg)




























