Embed Size (px)
Citation preview

National Coordinating Centre for the UK Ambulance Services Clinical Practice Guidelines, The University of Warwick, Coventry, CV4 7AL www.warwick.ac.uk/go/jrcalcguidelines
Resuscitation Supplement (2010)
The UK Ambulance Service Clinical Practice Guidelines Resuscitation Supplement (2010)
- For use ONLY until publication of the UK Ambulance Service Clinical
Practice Guidelines (2011)
Contents: Disclaimer
Basic Life Support in adults Foreign Body Airway Obstruction in adults Advanced Life Support in adults Traumatic Cardiac Arrest Maternal Resuscitation Implantable Cardioverter Defibrillator
Basic Life Support in children Foreign Body Airway Obstruction in children Advanced Life Support in children Atropine Newborn Life Support
Cardiac Rhythm Disturbance
Recognition of Life Extinct

Disclaimer – Resuscitation Supplement
Resuscitation Supplement 2010 Page 1 of 1
The Joint Royal Colleges Ambulance Liaison Committee has made every effort to ensure that the information, tables, drawings and diagrams contained in this Resuscitation Supplement (2010) is accurate at the time of publication. However, the JRCALC guidance is advisory and has been developed to assist healthcare professionals, together with patients, to make decisions about the management of the patient’s health, including treatments. It is intended to support the decision making process and is not a substitute for sound clinical judgement. Guidelines cannot always contain all the information necessary for determining appropriate care and cannot address all individual situations; therefore individuals using these guidelines must ensure they have the appropriate knowledge and skills to enable appropriate interpretation.
The JRCALC does not guarantee, and accepts no legal liability of whatever nature arising from or connected to, the accuracy, reliability, currency or completeness of the content of this Resuscitation Supplement.
Users of the Resuscitation Supplement must always be aware that such innovations or alterations after the date of publication may not be incorporated in the content. As part of its commitment to defining national standards, the committee will periodically issue updates to the content and users should ensure they are using the most up-to-date version of the guidelines: http://www.jrcalc.org.uk
Although some modification of the guidelines may be required by individual ambulance services, and approved by relevant local clinical committees, to ensure they respond to the health requirements of the local community, the majority of the guidance is universally applicable to NHS ambulance services. Modification of the guidelines may also occur when undertaking research sanctioned by a research ethics committee.
Whilst these guidelines cover the full range of paramedic treatments available across the UK they will also provide a valuable tool for ambulance technicians and other pre-hospital care providers. Many of the assessment skills and general principles will remain the same. Those not qualified to Paramedic level must practise only within their level of training and competence.

Basic Life Support (Adult) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 1 of 4
1. INTRODUCTION Basic life support refers to maintaining airway
patency, and supporting breathing and circulation without the use of equipment other than a protective device, usually a facemask or shield. In the pre-hospital environment, BLS includes the use of a bag-mask and oropharyngeal airway.
BLS is undertaken as a prelude to
defibrillation, often with an automated external defibrillator (AED).
2. ASSESSMENT and MANAGEMENT For the assessment and management of
adult basic life support see below and refer to the adult basic life support sequence detailed in Figure 1.
Assess safety Ensure that you, the patient
and any bystanders are safe. Check Responsiveness: Gently shake the
patient by the shoulders and ask loudly: “Are you alright?”
The responsive patient - Take history and
make assessment of what is wrong, with further action determined accordingly.
The unresponsive patient Summon help if necessary. Turn the patient onto their back and then
open the airway using head tilt and chin lift. Look in the mouth. If a foreign body or debris is visible attempt to remove it with a finger sweep, forceps or suction as appropriate.
When there is a risk of back or neck injury,
establish a clear upper airway by using jaw thrust or chin lift in combination with manual in-line stabilisation of the head and neck by an assistant (if available). If life threatening airway obstruction persists despite effective application of jaw thrust or chin lift, add head tilt a small amount at a time until the
airway is open; establishing a patent airway takes priority over concerns about a potential back or neck injury.
Keeping the airway open Look, listen and feel for normal breathing,
taking no more than 10 seconds to determine if the patient is breathing normally. If you have any doubt whether breathing is normal, act as if it is NOT normal.
Agonal breathing (occasional gasps, slow,
laboured noisy breathing) is common in the early stages of cardiac arrest. It is a sign of cardiac arrest and should not be confused as a sign of life / circulation.
If the patient is breathing normally Turn into the recovery position.
Undertake assessment, monitoring and
transport accordingly.
Re-assess regularly. If the patient is not breathing normally It may be difficult to be certain that there is
no pulse. If there are no signs of life (lack of
movement, normal breathing, or coughing), or there is doubt, start chest compressions at a rate of 100-120 compressions per minute.
Compression depth should be 5–6cm. Allow
the chest to recoil completely after each compression. Take approximately the same amount of time for each compression and recoil. Minimise interruptions to chest compression. Do not rely on a palpable pulse (carotid, femoral, or radial) as a gauge of effective blood flow.
Combine chest compression with rescue
breaths.

Basic Life Support (Adult) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 2 of 4
After 30 compressions, open the airway
again and provide two ventilations with the most appropriate equipment available, using an inspiratory time of one second with adequate volume to produce normal chest expansion. Each time compressions are resumed the ambulance clinician should place their hands without delay in the centre of the chest.
Add supplemental oxygen as soon as
possible.
Continue chest compressions and ventilation in a ratio of 30:2.
Stop to recheck only if he starts breathing
normally; otherwise do not interrupt chest compressions and ventilation.
Performing chest compressions is tiring; try
to change the person doing chest compressions every two minutes; ensure the minimum of delay during the changeover. Once the airway is secure (for example after supraglottic airway insertion) continue chest compressions uninterrupted at a rate of 100-120 per minute (except for defibrillation or further assessment as indicated). Ventilate 8-10 times per minute. Avoid hyperventilation.
If attempts at ventilation do not make the
chest rise as in normal breathing, then before the next attempt at ventilation: o check the patient’s mouth and remove
any obstruction o recheck that the airway position is
optimal with adequate head tilt / chin lift or jaw thrust
o do not attempt more than two breaths each time before returning to chest compressions.
ADDTIONAL INFORMATION
CPR in confined spaces - Over the head CPR and straddle CPR may be considered for resuscitation in confined spaces.
THE RECOVERY POSITION - There are several variations of the recovery position each with its own advantages. No single position is perfect for all patients. The position should be stable, near a true lateral position with the head dependent, and with no pressure on the chest to impair breathing. If the patient has to be kept in the recovery position for more than 30 minutes, turn the patient to the opposite side to relieve pressure on the lower arm.
Use of the Automated External Defibrillator (AED)
1. Make sure you, the patient and any bystanders are safe.
2. If you do not have an AED with you, perform CPR until an AED arrives.
3. As soon as an AED is available: o switch on the defibrillator and attach
the electrode pads. If more than one ambulance clinician is present, CPR should be continued whilst this is done
o follow the spoken / visual directions o ensure nobody touches the patient
whilst the AED is analysing the rhythm.
4a. If a shock is indicated:
o ensure nobody touches the patient o push the shock button as directed o continue as directed by the voice/visual
prompts.
4b. If no shock is indicated:
o immediately resume CPR using a ratio of 30 compressions to 2 rescue breaths
o continue as directed by voice / visual prompts.
5. Continue to follow AED prompts until:
o the patient starts to breathe normally o you are exhausted o the resuscitation attempt is abandoned.

Basic Life Support (Adult) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 3 of 4
Key Points – Adult Basic Life Support
Agonal breathing is common in the early stages of cardiac arrest and should not be confused as a sign of life/circulation.
If there are no signs of life, start chest compressions at a rate of 100-120 per minute using a ratio of 30 compressions to 2 breaths.
Once the airway is secure, chest compressions should be uninterrupted with ventilations 8-10 times per minute; avoid hyperventilation.
As soon as an AED is available switch on the defibrillator and attach the electrode pads and follow voice/visual prompts.
To relieve pressure on the lower arm, whilst in the recovery position, turn the patient to the opposite side every 30 minutes.
REFERENCES1 2
1. Koster RW, Baubin MA, Bossaert LL, Caballero A, Cassan P, Castrén M, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 2. Adult basic life support and use of automated external defibrillators. Resuscitation 2010;81(10):1277-92.
2. Nolan JP, Soar J, Zideman DA, Biarent D,
Bossaert LL, Deakin C, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 1. Executive summary. Resuscitation 2010;81(10):1219-76.

Basic Life Support (Adult) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 4 of 4
Figure 1 - Adult Basic Life Support Sequence – Modified from the Resuscitation Council (UK) Guidelines 2010 algorithm for the JRCALC Resuscitation Supplement 2010 (www.resus.org.uk).
UNRESPONSIVE?
Shout for help
Open airway
NOT BREATHING NORMALLY?
30 chest compressions
2 rescue breaths
30 compressions

Foreign Body Airway Obstruction (Adult) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 1 of 2
1. INTRODUCTION
Foreign body airway obstruction is an uncommon but potentially treatable cause of accidental death.
In adults, food, usually fish, meat or poultry
is the commonest cause of obstruction. Most cases occur when eating and are
therefore usually witnessed. The signs and symptoms vary, depending on the degree of airway obstruction (Table 1).
Table 1 – General Signs of Foreign Body Airway Obstruction
ASSESSMENT and MANAGEMENT Assess for severity of obstruction (Table 1).
Mild airway obstruction.
Encourage the patient to cough but do nothing else.
Monitor carefully.
Rapid transport to hospital.
Severe airway obstruction-conscious patient.
Give up to five back blows - after each back blow check to see if the obstruction has been relieved.
If the obstruction has not been relieved undertake a further back blow.
If five back blows do not relieve the airway obstruction, give up to five abdominal thrusts.
If five abdominal thrusts do not relieve the obstruction, continue alternating five back blows with five abdominal thrusts.
Severe airway obstruction-unconscious patient. If the patient is unconscious or becomes
unconscious, begin basic life support - refer to adult BLS guidance-section 4.
During CPR, the patient’s mouth should be quickly checked for any foreign body that has been partly expelled, each time the airway is opened.
If these measures fail and the airway remains obstructed:
Attempt to visualise the vocal cords with a laryngoscope.
Remove any visible foreign material with forceps or suction.
If this fails or is not possible, and you are trained in the technique, perform needle cricothyroidotomy.
Additional Information:
Chest thrusts/compressions generate a higher airway pressure than back blows and finger sweeps.
Avoid blind finger sweeps. Manually remove solid material in the airway only if it can be seen.
Following successful treatment for FBAO, foreign material may remain in the upper or lower respiratory tract and cause complications later. Patients with a persistent cough, difficulty swallowing or the sensation of an object being stuck in the throat must be assessed further.
Abdominal thrusts can cause serious internal injuries and all patients so treated must be assessed for injury in hospital.
Attack usually occurs while eating Patient may clutch his neck
Mild airway obstruction
In response to question - “Are you choking?”
The patient speaks and answers “yes”.
Other signs - the patient is able to: speak cough breathe.
Signs of severe airway obstruction
In response to question - “Are you choking?”
The patient is unable to speak and may respond by nodding.
Other signs: patient unable to breathe breathing sounds wheezy attempts at coughing are silent patient may be unconscious.

Foreign Body Airway Obstruction (Adult) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 2 of 2
Figure 1 – Adult Foreign Body Airway Obstruction Algorithm - Modified from the Resuscitation Council (UK) Guidelines 2010 algorithm for the JRCALC Resuscitation Supplement 2010 (www.resus.org.uk).
Key Points – Adult Foreign Body Airway Obstruction (FBAO)
Potentially treatable cause of death; often occurs whilst eating.
Asking the patient “Are you choking?” can aid diagnosis.
Back blows and abdominal thrusts may relieve the obstruction; check after each manoeuvre to see if obstruction is relieved.
Abdominal thrusts can cause internal injuries and patients should be assessed in hospital.
Avoid blind finger sweeps; manually remove solid material in the airway ONLY if it can be seen.
REFERENCES1 2 1. Nolan JP, Soar J, Zideman DA, Biarent D,
Bossaert LL, Deakin C, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 1. Executive summary. Resuscitation 2010;81(10):1219-76.
2. Koster RW, Baubin MA, Bossaert LL, Caballero A, Cassan P, Castrén M, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 2. Adult basic life support and use of automated external defibrillators. Resuscitation 2010;81(10):1277-92.

Advanced Life Support (Adult) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 1 of 7
1. INTRODUCTION The heart rhythms associated with cardiac arrest are divided into two groups:
1. shockable rhythms – ventricular fibrillation and pulseless ventricular tachycardia (VF/VT) 2. non-shockable rhythms – asystole and pulseless electrical activity (PEA).
The principal difference in the
management of these two groups is the need for attempted defibrillation in VF/VT. Subsequent actions including chest compressions, airway management and ventilation, venous access, administration of adrenaline and the management of reversible factors, are common to both groups.
The interventions that unequivocally
improve survival are early defibrillation and effective basic life support. Attention should focus therefore on early defibrillation and high quality, uninterrupted cardio-pulmonary resuscitation (CPR).
A solo responder should not interrupt
chest compressions for any reason other than to deliver two breaths or defibrillate the patient. IV access, drug delivery and advanced airway management require two or more responders. While these procedures are performed, interruptions to chest compressions must be kept to an absolute minimum.
High quality, uninterrupted chest
compressions are crucial in achieving return of spontaneous circulation. Chest compressions of correct rate (100-120 min-1) and depth (5-6 cm) with complete recoil should commence immediately and continue while the defibrillator is charging only pausing to assess the rhythm or
deliver the shock (as appropriate) before recommencing the compressions.
Intravenous access should be
established as soon as an appropriately trained responder is able to do so. If IV access is not possible intraosseous access should be considered.
2. ASSESSMENT and MANAGEMENT For assessment and management of cardiac arrest see below and refer to Figure 1.
Having confirmed cardiac arrest:
Summon help if appropriate.
Start CPR beginning with chest compressions. Ventilate with high concentration oxygen.
As soon as the defibrillator arrives, diagnose the rhythm by applying self-adhesive pads to the chest and attempt defibrillation as appropriate.
1. SHOCKABLE RHYTHMS (VF/PULSELESS VT)
Attempt defibrillation (one shock – 150-200 Joules biphasic or 360 Joules monophasic).
Immediately resume chest compressions (30:2) without re-assessing the rhythm or feeling for a pulse.
Continue CPR for 2 minutes, and then pause briefly to check the monitor,
If VF/VT persists:
Give a further (2nd) shock (150-360 Joules biphasic or 360 Joules monophasic).
Resume CPR immediately and continue for 2 minutes.

Advanced Life Support (Adult) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 2 of 7
Pause briefly to check the monitor.
If VF/VT persists, give a further (3rd) shock (150-360 Joules biphasic or 360 Joules monophasic).
As soon as CPR has resumed, give adrenaline 1 milligram IV and amiodarone 300 milligrams IV while continuing CPR for a further 2 minutes.
Pause briefly to check the monitor.
If VF/VT persists, give a further (4th) shock (150-360 Joules biphasic or 360 Joules monophasic).
Resume CPR immediately and continue for 2 minutes.
Pause briefly to check the monitor.
If VF/VT persists give a (5th) shock (150-360 Joules biphasic or 360 Joules monophasic).
Resume CPR immediately and give adrenaline 1 mg IV while continuing CPR for a further 2 minutes.
Give adrenaline 1 milligram IV immediately after alternate shocks (i.e. approximately every 3-5 minutes).
Give further shocks after each 2 minute period of CPR and after confirming that VF/VT persists.
If organised electrical activity is seen, check for a pulse.
If a pulse is present, start post-resuscitation care.
If no pulse is present, continue CPR and switch to the non-shockable algorithm.
If asystole is seen
Continue CPR and switch to the non-shockable algorithm.
2. NON-SHOCKABLE RHYTHMS (ASYSTOLE AND PEA)
If these rhythms are identified:
Start CPR 30:2 and give adrenaline 1 milligram as soon as intravascular access is achieved.
If asystole is displayed, without stopping
CPR, check the leads are attached correctly.
Secure the airway as soon as possible to enable continuous chest compressions without pausing for ventilation.
After two minutes CPR 30:2, recheck the rhythm. If asystole is present or there has been no change in ECG appearance resume CPR immediately.
If VF / VT present, change to the shockable rhythm algorithm.
If an organised rhythm is present, attempt to palpate a pulse.
If a pulse is present begin post resuscitation care.
If no pulse is present (or there is any doubt) continue CPR. Give adrenaline 1 milligram IV every 3–5 minutes (alternate loops).
If signs of life return during CPR, check the rhythm and attempt to palpate a pulse.

Advanced Life Support (Adult) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 3 of 7
POTENTIALLY REVERSIBLE CAUSES
Potential causes or aggravating factors for which specific treatment exists must be considered during any cardiac arrest. For ease of memory these are presented Assess the 4H’s and 4T’s according to their initial letter. Those amenable to treatment include:
4 H’s
1. Hypoxia – ensure adequate ventilation, adequate chest expansion and breath sounds. Verify tracheal tube placement, preferably using capnography.
2. Hypovolaemia – PEA caused by hypovolaemia is usually due to haemorrhage from trauma, gastrointestinal bleeding or rupture of an aortic aneurysm. Intravascular volume should be restored rapidly with IV fluid. Rapid transport to definitive surgical care is essential.
3. Hypothermia – refer to hypothermia and immersion incident guidelines.
4. Hyperkalaemia - and other electrolyte disorders are unlikely to be apparent in the pre-hospital arena or amenable to treatment. 4T’s 1. Tension Pneumothorax – the diagnosis is made clinically; decompress as soon as possible by needle thoracocentesis.
2. Cardiac Tamponade is difficult to diagnose as the typical signs (high venous pressure, hypotension) disappear after cardiac arrest occurs. Cardiac arrest after penetrating chest trauma is highly suggestive of cardiac tamponade. These patients should be transported to hospital immediately without any delay on scene as pericardiocentesis or thoracotomy cannot usually be performed outside hospital.
3. Toxins – only rarely will an antidote be available outside hospital, and in most cases supportive treatment will be the priority.
4. Thromboembolism – massive pulmonary embolism is the commonest cause but
diagnosis in the field is difficult once arrest has occurred. Specific treatments (like thrombolytic drugs) are not available to ambulance personnel in the UK at present.
THE WITNESSED, MONITORED ARREST
If a patient who is being monitored has a witnessed arrest:
Confirm cardiac arrest, summon help if appropriate.
If the rhythm is VF/VT and a defibrillator is not immediately available consider a precordial thump.
If the rhythm is VF/VT and a defibrillator is immediately available, give a shock first. Treat any recurrence of VF.
When the arrest is witnessed but unmonitored, using self-adhesive hands free defibrillation pads will allow assessment of the rhythm more quickly than attaching ECG electrodes.
Return Of Spontaneous Circulation (ROSC) For the care of patients following ROSC see below and Figure 2.
Return of spontaneous circulation (ROSC) is an important first step on the pathway to recovery from cardiac arrest. Following ROSC some patients may suffer post-cardiac-arrest syndrome, the severity of which will depend on the duration and cause of the cardiac arrest. Post-cardiac-arrest syndrome often complicates the post-resuscitation phase and comprises:
Brain injury: coma, seizures, myoclonus, varying degrees of neurocognitive dysfunction and brain death; this may be exacerbated by microcirculatory failure, impaired autoregulation, hypercarbia, hyperoxia, pyrexia, hyperglycaemia and seizures.

Advanced Life Support (Adult) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 4 of 7
Myocardial dysfunction: this is common after cardiac arrest but usually improves in the following weeks.
The systemic ischaemia / reperfusion response: The whole body ischaemia/reperfusion that occurs with resuscitation from cardiac arrest activates immunological and coagulation pathways contributing to an inflammatory response and multiple organ failure.
Persistence of the precipitating pathology.
Management of Return of spontaneous circulation: Transfer the patient directly to the
nearest hospital capable of delivering PPCI in accordance with local protocols.
Early recurrence of VF is common, so ensure continuous monitoring in order to deliver further shocks if appropriate.
Continue patient management en-route-see below.
Provide an alert/information call. Undertake a 12-lead ECG. Oxygen Measure oxygen saturation. Maintain oxygen saturations between 94-
98%. Ventilation Use of an automatic ventilator is
preferable to manual ventilation. Monitor ventilation rate and volume. Monitor end-tidal C02 (N.B. Readings
may be low because of reduced cardiac output rather than hyperventilation. Normal range = 3.5-5.0 kPa).
Blood glucose level Measure blood glucose level. If the patient is hypoglycaemic (BM
<4.0mmol) refer to glycaemic emergencies guideline.
Cooling In cases of non-traumatic cardiac arrest,
in patients that have not regained consciousness, start active cooling as soon as possible, according to local protocols.
Key Points - Advanced Life Support (Adult)
Begin good quality, uninterrupted chest compressions immediately. Attempt defibrillation as soon as a defibrillator is available.
For shockable rhythms defibrillate and resume chest compressions (30:2) for 2 minutes without re-assessing the rhythm or feeling for a pulse; then check rhythm, if VF/VT persists follow ALS algorithm.
Give adrenaline 1 mg and amiodarone 300 mg immediately after the 3rd shock.
For non-shockable rhythms start CPR at a ratio of 30:2 and give adrenaline 1mg as soon as intravascular access is achieved.
Give adrenaline every second cycle (3-5 minutes).
Always consider reversible features (4Hs and 4Ts) and correct when possible.

Advanced Life Support (Adult) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 5 of 7
REFERENCES1-3 1. Deakin CD, Nolan JP, Soar J, Sunde K,
Koster RW, Smith GB, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 4. Adult advanced life support. Resuscitation 2010;81(10):1305-52.
2. Deakin CD, Nolan JP, Sunde K, Koster RW. European Resuscitation Council Guidelines for Resuscitation 2010 Section 3. Electrical therapies: Automated external defibrillators, defibrillation, cardioversion and pacing. Resuscitation 2010;81(10):1293-304.
3. Nolan JP, Soar J, Zideman DA, Biarent D, Bossaert LL, Deakin C, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 1. Executive summary. Resuscitation 2010;81(10):1219-76.

Advanced Life Support (Adult) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 6 of 7
Unresponsive?Not breathing or
only occasional gasps?
CPR 30:2Attach defibrillator / monitor
Minimise interruptions
Assessrhythm
Return of spontaneous circulation
Immediate post cardiac arrest treatment:
- Use ABCDE approach- Controlled oxygenation and ventilation- 12-lead ECG- Investigations- Treat precipitating cause- Temperature control- Therapeutic hypothermia
Shockable(VF / Pulseless VT)
1 Shock
Immediately resumeCPR for 2 min
Minimise interruptions
Non-Shockable(PEA / Asystole)
Immediately resumeCPR for 2 min
Minimise interruptions
Du
rin
g C
PR Ensure high-quality CPR: rate, depth,
recoil.
Plan actions before interrupting CPR.
Administer oxygen.
Consider advanced airway and capnography.
Continuous chest compressions when advanced airway in place.
Vascular access (intravenous,
intraosseous).
Administer adrenaline every 3-5 min.
Correct reversible causes.
Rev
ersi
ble
cau
ses
Hypoxia.
Hypovolaemia.
Hypo/hyperkalaemia/metabolic.
Hypothermia.
Thrombosis.
Tamponade – cardiac.
Toxins.
Tension pneumothorax.
Figure 1 – Advanced Life Support Algorithm - Modified from the Resuscitation Council (UK) Guidelines 2010 algorithm for the JRCALC Resuscitation Supplement 2010 (www.resus.org.uk)

Advanced Life Support (Adult) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 7 of 7
Figure 2 – Assessment and management of Return Of Spontaneous Circulation (ROSC)

Traumatic Cardiac Arrest – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 1 of 2
1. INTRODUCTION Traumatic cardiac arrest is a very
different condition from the more usual cardiac arrest which is often related to ischaemic heart disease. Management of traumatic cardiac arrest must be directed toward identifying and treating the underlying cause of the arrest or resuscitation is unlikely to be successful.
Traumatic cardiac arrest may develop as a result of:
1. Hypoxia caused by manageable issues such as obstruction of the airway (e.g. facial injury or decreased level of consciousness) or breathing problems (e.g. pneumo / haemothorax). 2. Hypoperfusion caused by compromise of the heart (e.g. stab wound causing cardiac tamponade) or hypovolaemia (either occult or revealed haemorrhage).
2. ASSESSMENT and MANAGEMENT Assess for potential causes. The potential causes should be addressed by applying standard trauma management principles (refer to trauma emergencies guideline). Any problem should be dealt with adequately before moving on to the next: <C> CATASTROPHIC HAEMORRHAGE (extreme bleeding likely to cause death in minutes) - assess for the presence LIFE-THREATENING EXTERNAL BLEEDING – refer to trauma emergencies overview. A – Airway obstruction; ensure the airway is open and clear. B – Impaired breathing; search for and manage a sucking chest wound or a tension pneumothorax (refer to thoracic trauma guideline). If not absolutely certain, then needle thoracocentesis should be performed on both sides. Support and assist ventilation.
C – Hypovolaemia as a result of major blood loss; apply external haemorrhage control and secure vascular access while transferring without delay to definitive treatment. D – Major head injury (refer to head trauma guideline) or spinal cord injury (refer to neck and back trauma guideline) impairing ventilation through CNS depression or loss of neuromuscular function. 2.1 Commencing Cardio-Pulmonary Resuscitation (CPR): Resuscitation should be commenced in
all patients, irrespective of whether the arrest was witnessed, unless the patient is clearly beyond help (Non-survivable injury, rigor mortis, decomposition etc.). Once resuscitation is commenced, full ALS-based resuscitation (refer to advanced life support guidelines) should be attempted for an appropriate duration (see below).
In paediatric traumatic cardiac arrest, CPR is
commenced in the vast majority of circumstances, unless it is clear that the child will not survive.
In penetrating traumatic cardiac arrest, patients must be transferred rapidly to hospital because surgical intervention is often needed to treat the cause of the arrest. In these patients, a ‘scoop and run’ policy is appropriate. Do not stay on scene to resuscitate a patient with penetrating injury.
If a patient has not responded after 20 minutes of advanced life support (ALS) then resuscitation can be terminated.

Traumatic Cardiac Arrest – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 2 of 2
2.2 Terminating Cardio-Pulmonary Resuscitation (CPR): Termination of resuscitation in a patient
who has suffered a traumatic cardiac arrest (blunt or penetrating) should be considered if the patient has not responded (i.e. the patient is apnoeic, pulseless, without organised cardiac electrical activity and without pupillary light reflexes) to 20 minutes of ALS, providing all reversible causes have been treated.
The only exceptions to this are pregnancy (when the patient should be rapidly transferred to hospital to deliver the infant), in the presence of hypothermia and with trauma involving children. In this latter case follow paediatric resuscitation guidelines and undertake a TIME CRITICAL transfer to a hospital Emergency Department with ongoing resuscitation.
After stopping resuscitation, the Recognition of Life Extinct by Ambulance Clinicians (ROLE) procedure should be followed (refer to ROLE guideline) and the Police informed.
Key Points – Traumatic cardiac arrest
Traumatic cardiac arrest is different from cardiac arrest due to primary cardiac disease.
Assessment and management should follow the trauma guideline, treating problems as they are found.
Once a decision to start resuscitation is taken, full ALS-based resuscitation for at least 20 minutes should be performed.
If there is no response to resuscitation after 20 minutes of ALS and all potentially reversible causes have been treated, further effort is futile. However, resuscitation of children should be continued to hospital.
The ROLE procedure should be followed if resuscitation is terminated.
REFERENCES1-4 1. Soar J, Perkins GD, Abbas G, Alfonzo A,
Barelli A, Bierens JJLM, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 8. Cardiac arrest in special circumstances: Electrolyte abnormalities, poisoning, drowning, accidental hypothermia, hyperthermia, asthma, anaphylaxis, cardiac surgery, trauma, pregnancy, electrocution. Resuscitation 2010;81(10):1400-33.
2. Deakin CD, Nolan JP, Soar J, Sunde K, Koster RW, Smith GB, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 4. Adult advanced life support. Resuscitation 2010;81(10):1305-52.
3. Deakin CD, Nolan JP, Sunde K, Koster RW. European Resuscitation Council Guidelines for Resuscitation 2010 Section 3. Electrical therapies: Automated external defibrillators, defibrillation, cardioversion and pacing. Resuscitation 2010;81(10):1293-304.
4. Biarent D, Bingham R, Eich C, López-Herce J, Maconochie I, Rodríguez-Núñez A, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 6. Paediatric life support. Resuscitation 2010;81(10):1364-88.

Maternal Resuscitation – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 1 of 3
GENERAL INTRODUCTION It is important to recognise that there are two
patients. Effective resuscitation of the mother will provide
effective resuscitation of the fetus. Resuscitation priority is the mother. 1. CARDIAC ARREST Undertake a TIME CRITICAL transfer as soon as ventilation is achieved and CPR commenced. 1.1 INTRODUCTION The approach to resuscitating an obstetric
patient is the same as that of any adult in cardiac arrest; but in the third trimester additional measures must be undertaken to maximise the efficacy of resuscitation.
Because fetuses can tolerate significant levels of hypoxia, resuscitation should be initiated immediately and NOT terminated in pre-hospital care, even in cases where the mother’s condition is, or appears non-survivable or unequivocally associated with death, as this will maximise the chances of both maternal and fetal survival.
1.2 RISK FACTORS There is an increased risk of maternal mortality for patients who are: socially disadvantaged from poor communities from minority ethnic groups late in booking for antenatal care or have poor
attendance obese the victims of domestic violence substance abusers.
1.3 PATHOPHYSIOLOGY Cardiorespiratory arrest in pregnancy is very
rarely due to a primary cardiac cause. Common causes of sudden maternal death include pulmonary or amniotic fluid embolus.
There are a number of physiological and anatomical changes during pregnancy that may influence the management of the obstetric patient (refer to obstetric and gynaecology overview guideline).
1.4 ASSESSMENT and MANAGEMENT of cardiac arrest during pregnancy.
Quickly scan the patient and scene as you approach. Undertake a primary survey ABCDEF.
Manage as per standard advanced life support (refer to ALS guideline).
Assess and exclude treatable causes including hypovolaemia, sepsis and anaphylactic shock.
Caution – ventilation with a bag-valve-mask may lead to regurgitation and aspiration. Consider early tracheal intubation which reduces the risk of gastric aspiration and may make ventilation of the lungs easier. A supraglottic airway is a suitable alternative.
Undertake a TIME CRITICAL transfer to
nearest suitable receiving hospital; provide an alert/information call – ask to have an OBSTETRICIAN ON STANDBY IN THE EMERGENCY DEPARTMENT for an emergency Caesarean section (in this situation delivering the fetus MAY facilitate maternal resuscitation).
Manually displace the uterus to the left to
remove compression of the inferior vena cava. Add left lateral tilt (15 - 30 degrees). N.B. the angle of tilt needs to allow good quality chest compressions (refer to obstetric and gynaecology overview).
Aim to establish intravascular access using
a LARGE BORE cannula without delay in transfer to hospital.
Attempt IO access if rapid IV cannulation is
not possible.

Maternal Resuscitation – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 2 of 3
2. SHOCK
2.1 PATHOPHYSIOLOGY The failure of perfusion of the tissues with oxygenated blood due to loss of circulating fluid volume may be due to: hypovolaemic shock - loss of circulating fluid
volume due to haemorrhage septic shock - movement of circulating fluid
volume into the interstitial spaces due to increased capillary permeability
cardiogenic shock - pump failure or obstruction in the circulatory system
anaphylactic shock - severe allergic reaction psychogenic shock - severe stress. 2.2 RISK FACTORS There are a number of associated risk factors including: intercurrent heart disease (cardiogenic shock) thromboembolism or amniotic fluid embolism
(cardiogenic shock) non-obstetric infections and genital tract sepsis
(septic shock) trauma (hypovolaemic shock) obstetric haemorrhage (hypovolaemic shock) inverted uterus (hypovolaemic shock) ruptured ectopic pregnancy (hypovolaemic
shock) incomplete miscarriage (hypovolaemic shock) opiate-induced histamine release or other drug
allergy (anaphylaxis). 2.3 PATHOPHYSIOLOGY The body’s main mechanism for maintaining
maternal circulation in the event of blood loss is to restrict blood flow to the uterus. This results in a reduction of placental perfusion and associated fetal hypoxia.
There are a number of other physiological and anatomical changes during pregnancy that may influence the management of the obstetric patient (refer to obstetric and gynaecology overview guideline).
2.4 ASSESSMENT and MANAGEMENT of shock Quickly scan the patient and scene as you
approach. Undertake a primary survey ABCDEF.
Cardiogenic / anaphylactic shock: Refer to specific resuscitation
guidelines. Refer to anaphylaxis / allergic reactions
guideline. Manually displace the uterus to the left to
remove compression of the inferior vena cava. Add left lateral tilt if this is feasible (15 - 30 degrees). The angle of tilt needs to allow good quality chest compressions (refer to obstetric and gynaecology overview).
Administer supplemental oxygen and aim
for a saturation of 94-98% (refer to oxygen guideline).
Undertake a TIME CRITICAL transfer to
nearest suitable receiving hospital; provide an alert/information. Ask to have an OBSTETRICIAN ON STANDBY IN THE EMERGENCY DEPARTMENT for an emergency Caesarean section if the mother has suffered cardiorespiratory collapse (in this situation delivering the fetus MAY facilitate maternal resuscitation).
Monitor blood pressure, ECG, and blood
glucose level. Treat the underlying condition. Insert at least one LARGE BORE IV
cannulae – do not delay transfer. In hypovolaemia, septic shock, and
anaphylactic shock administer IV sodium chloride 0.9% given in 250ml aliquots to maintain a systolic blood pressure of 90mmHg or if there is significant external haemorrhage >500ml, altered mental status, or dysrrhythmias.

Maternal Resuscitation – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 3 of 3
Key Points – Maternal resuscitation
Do not withhold or terminate maternal resuscitation.
ALWAYS manage patients >22 weeks gestation with manual displacement of the uterus to the left and a 15-30 degree lateral tilt to the left.
Gastric regurgitation is more likely; be ready with suction (consider early intubation or supraglottic airway insertion) to reduce gastric insufflation
Insert at least one LARGE BORE IV cannulae.
Cardiac arrest may be caused by pulmonary arrest or amniotic fluid embolism.
Due to physiological changes of pregnancy, patients may initially compensate for hypovolaemia.
If the patient is unstable, ask to have an OBSTETRICIAN ON STANDBY IN THE EMERGENCY DEPARTMENT.
REFERENCES1-5 1. Soar J, Perkins GD, Abbas G, Alfonzo A,
Barelli A, Bierens JJLM, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 8. Cardiac arrest in special circumstances: Electrolyte abnormalities, poisoning, drowning, accidental hypothermia, hyperthermia, asthma, anaphylaxis, cardiac surgery, trauma, pregnancy, electrocution. Resuscitation 2010;81(10):1400-33.
2. Woollard M, Hinshaw K, Simpson H, Wieteska S, editors. The Pre-hospital Obstetric Emergency Training (POET) India: Wiley-Blackwell, 2009.
3. Deakin CD, Nolan JP, Soar J, Sunde K, Koster RW, Smith GB, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 4. Adult advanced life support. Resuscitation 2010;81(10):1305-52.
4. Deakin CD, Nolan JP, Sunde K, Koster RW. European Resuscitation Council Guidelines for Resuscitation 2010 Section 3. Electrical therapies: Automated external defibrillators, defibrillation, cardioversion and pacing. Resuscitation 2010;81(10):1293-304.
5. Richmond S, Wyllie J. European Resuscitation Council Guidelines for Resuscitation 2010: Section 7. Resuscitation of babies at birth. Resuscitation 2010;81(10):1389-99.

The Implantable Cardioverter Defibrillator – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 1 of 6
1. INTRODUCTION The Implantable Cardioverter Defibrillator (ICD) has revolutionised the management of patients at risk of developing a life-threatening ventricular arrhythmia. Several clinical trials have testified to their effectiveness in reducing deaths from sudden cardiac arrest in selected patients, and the devices are implanted with increasing frequency. ICDs are used in both children and adults. ICD systems consist of a generator connected to electrodes placed transvenously into cardiac chambers (the ventricle, and sometimes the right atrium and / or the coronary sinus (Figure 1). The electrodes serve a dual function allowing the monitoring of cardiac rhythm and the administration of electrical pacing, defibrillation and cardioversion therapy. Modern ICDs are slightly larger than a pacemaker and are usually implanted in the left subclavicular area (Figure 1). The ICD generator contains the battery and sophisticated electronic circuitry that monitors the cardiac rhythm, determines the need for electrical therapy, delivers treatment, monitors the response and determines the need for further therapy.
Figure 1 – Usual Location of an ICD (used with the permission of medmovie.com).
The available therapies include: Conventional programmable pacing for
the treatment of bradycardia Anti-tachycardia pacing (ATP) for
ventricular tachycardia (VT) Delivery of biphasic shocks for the
treatment of ventricular tachycardia and ventricular fibrillation (VF)
Cardiac resynchronisation therapy (CRT) (biventricular pacing) for the treatment of heart failure.
These treatment modalities and specifications are programmable and capable of considerable sophistication to suit the requirements of individual patients. The implantation and programming of devices is carried out in specialised centres. The patient should carry a card or documentation which identifies their ICD centre and may also have been given emergency instructions. The personnel caring for such patients in emergency situations are not usually experts in arrhythmia management or familiar with the details of the sophisticated treatment regimes offered by modern ICDs. Moreover, the technology is complex and evolving rapidly. In an emergency, patients will often present to the ambulance service or Emergency Department (ED) and the purpose of this guidance is to help those responsible for the initial management of these patients. 2. GENERAL PRINCIPLES Some important points should be made at the outset: On detecting VF/VT the ICD will usually
discharge a maximum of eight times before shutting down. However, a new episode of VF/VT will result in the ICD recommencing its discharge sequence. A patient with a fractured ICD lead may suffer repeated internal defibrillation as the electrical noise is misinterpreted as a

The Implantable Cardioverter Defibrillator – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 2 of 6
shockable rhythm. These patients are likely to be conscious with a relatively normal ECG rate.
When confronted with a patient fitted with
an ICD who has a persistent or recurring arrhythmia, or where the ICD is firing, expert help should be summoned at the outset. Outside hospital this will normally be from the ambulance service, who should be summoned immediately by dialling 999.
When confronted with a patient in cardiac
arrest the usual management guidelines are still appropriate (refer to cardiac arrest and arrhythmia guidelines).If the ICD is not responding to VF or VT, or if shocks are ineffective, external defibrillation / cardioversion should be carried out. Avoid placing the defibrillator electrodes / pads / paddles close to or on top of the ICD; ensure a minimum distance of 8 cm between the edge of the defibrillator paddle pad/electrode and the ICD site. Most ICDs are implanted in the left sub-clavicular position (see Figure 1) and are usually readily apparent on examination; the conventional (apical / right subclavicular) electrode position will then be appropriate. The anterior / posterior position may also be used, particularly if the ICD is right sided.
Whenever possible, record a 12-lead
electrocardiogram (ECG) and record the patient‟s rhythm (with any shocks). Make sure this is printed out and stored electronically (where available) for future reference. Where an external defibrillator with an electronic memory is used (whether for monitoring or for therapy) ensure that the ECG report is printed and handed to appropriate staff. Again, whenever possible, ensure that the record is archived for future reference. Record the rhythm during any therapeutic measure (whether by drugs or electricity).
All these records may provide vital information for the ICD centre that may greatly influence the patient‟s subsequent management.
The energy levels of the shocks
administered by ICDs (up to 40 Joules) are much lower than those employed with external defibrillators (120 – 360J). Personnel in contact with the patient when an ICD discharges are unlikely to be harmed, but it is prudent to minimise contact with the patient while the ICD is firing. Chest compression and ventilation can be carried out as normal and protective examination gloves should be worn as usual.
Placing a ring magnet over the ICD
generator can temporarily disable the shock capability of an ICD. The magnet does not disable the pacing capability for treating bradycardia. The magnet may be kept in position with adhesive tape if required. Removing the magnet returns the ICD to the status present before application. The ECG rhythm should be monitored at all times when the device is disabled. An ICD should only be disabled when the rhythm for which shocks are being delivered has been recorded. If that rhythm is VT or VF, external cardioversion/defibrillation must be available. With some models it is possible to programme the ICD so that a magnet does not disable the shock capabilities of the device. This is usually done only in exceptional circumstances, and consequently, such patients are rare.
The manufacturers of the ICDs also
supply the ring magnets. Many implantation centres provide each patient with a ring magnet and stress that it should be readily available in case of emergency. With the increasing prevalence of ICDs in the community it

The Implantable Cardioverter Defibrillator – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 3 of 6
becomes increasingly important that emergency workers have this magnet available to them when attending these patients.
Decisions to apply a Do Not Attempt
Resuscitation (DNAR) order will not be made in the emergency situation by the personnel to whom this guidance is directed. Where such an order does exist it should not be necessary to disable an ICD to enable the implementation of such an order.
Many problems with ICDs can only be
dealt with permanently by using the programmer available at the ICD centre.
The guidelines should be read from the
perspective of your position and role in the management of such patients. For example, the recommendation to „arrange further assessment‟ will mean that ambulance clinicians should transport the patient to hospital. For ED staff however, this might mean referral to the medical admitting team or local ICD centre.
Coincident conditions that may contribute
to the development of arrhythmia (for example acute ischaemia, worsening heart failure) should be managed as appropriate according to usual practice.
Maintain oxygen saturations between 94-
98%. Receiving ICD therapy may be
unpleasant “like a firm kick in the chest”, and psychological consequences may also arise. It is important to be aware of these, and help should be available from implantation centres. An emergency telephone helpline may be available.
3. ASSESSMENT and MANAGEMENT This should be read in conjunction with the treatment algorithm (Figure 2). Approach and assess the patient and perform basic life support according to current BLS guidelines. Monitor the ECG. 3.1. If the patient is in cardiac arrest 3.1.1 Perform basic life support in accordance with current BLS guidelines. Standard airway management techniques and methods for gaining IV/IO access (as appropriate) should be established. 3.1.2 If a shockable rhythm is present (VF or pulseless VT) but the ICD is not detecting it, perform external defibrillation and other resuscitation procedures according to current resuscitation guidelines. 3.1.3 If the ICD is delivering therapy (whether by antitachycardia pacing or shocks) but is failing to convert the arrhythmia, then external defibrillation should be provided, as per current guidelines. 3.1.4 If a non-shockable rhythm is present manage the patient according to current guidelines. If the rhythm is converted to a shockable one, assess the response of the ICD, as in 1.2 above, performing external defibrillation as required. 3.1.5 If a shockable rhythm is converted to one associated with effective cardiac output (whether by the ICD or by external defibrillation), manage the patient as usual and arrange further treatment and assessment. 3.2. If the patient is not in cardiac arrest Determine whether an arrhythmia is present.

The Implantable Cardioverter Defibrillator – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 4 of 6
3.2.2 If no arrhythmia is present: If therapy from the ICD has been effective and the patient is in sinus rhythm or is paced, monitor the patient, give O2 and arrange further assessment to investigate possibility of new myocardial infarction (MI), heart failure, other acute illness or drug toxicity / electrolyte imbalance etc. An ICD may deliver inappropriate shocks (i.e. in the absence of arrhythmia) if there are problems with sensing the cardiac rhythm or there are problems with the leads. Record the rhythm (while shocks are delivered, if possible), disable the ICD with a magnet, monitor the patient and arrange further assessment with help from the ICD centre. Provide supportive treatment as required. 3.2.3 If an arrhythmia is present: If an arrhythmia is present and shocks are being delivered, record the arrhythmia (while ICD shocks are delivered if possible) on the ECG. Determine the nature of the arrhythmia. Transport rapidly to hospital in all cases. TACHYCARDIA 3.2.3.1 If the rhythm is a supraventricular tachycardia i.e. sinus tachycardia, atrial flutter, atrial fibrillation, junctional tachycardia, etc. and the patient is haemodynamically stable, and the patient is continuing to receive shocks, disable the ICD with a magnet. Consider possible causes, treat appropriately and arrange further assessment in hospital. 3.2.3.2 If the rhythm is ventricular tachycardia: Pulseless VT should be treated as
cardiac arrest (1.2 above). If the patient is haemodynamically stable,
monitor the patient and convey to the emergency department.
If the patient is haemodynamically unstable, and ICD shocks are ineffective treat as per VT guideline.
An ICD will not deliver anti-tachycardia pacing (ATP) or shocks if the rate of the VT is below the programmed detection
rate of the device (generally 150 beats/min). Conventional management may be undertaken according to the patient‟s haemodynamic status.
Recurring VT with appropriate shocks. Manage any underlying cause (acute ischaemia, heart failure etc.). Sedation may be of benefit.
INAPPROPRIATE /INEFFECTIVE ICD FIRING 3.2.3.3 A ring magnet placed over the ICD box will stop the ICD from firing and may be considered in conscious patients where the ICD shocks are ineffective and the patient is distressed. In ICDs that have a dual pacing function, the magnet will also usually change the pacing function to deliver a paced output of 50 beats/min.

The Implantable Cardioverter Defibrillator – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 5 of 6
Key Points – Implantable Cardioverter Defibrillators (ICD)
ICDs deliver therapy with bradycardia pacing, ATP and shocks for VT not responding to ATP or VF.
ECG records, especially at the time that shocks are given, can be vital in subsequent patient management. A recording should always be made if circumstances allow.
Cardiac arrest should be managed according to normal guidelines.
Avoid placing the defibrillator electrode over or within 8 cm of the ICD box.
A discharging ICD is unlikely to harm a rescuer touching the patient or performing CPR.
An inappropriately discharging ICD can be temporarily disabled by placing a ring magnet directly over the ICD box.
REFERENCES1-3 1. Nolan JP, Soar J, Zideman DA, Biarent D, Bossaert LL, Deakin C, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 1. Executive summary. Resuscitation 2010;81(10):1219-76. 2. Koster RW, Baubin MA, Bossaert LL, Caballero A, Cassan P, Castrén M, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 2. Adult basic life support and use of automated external defibrillators. Resuscitation 2010;81(10):1277-92. 3. Deakin CD, Nolan JP, Sunde K, Koster RW. European Resuscitation Council Guidelines for Resuscitation 2010 Section 3. Electrical therapies: Automated external defibrillators, defibrillation, cardioversion and pacing. Resuscitation 2010;81(10):1293-304.

The Implantable Cardioverter Defibrillator – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 6 of 6
Primary survey - ABCDMonitor ECG
Is the patient in cardiac arrest?
YES
Was the shock effective / appropriate?
YES
Assess patientMonitor 12-lead ECG
Monitor blood pressureTreat as per clinical guidelines
If blood pressure is low treat underlying cause(s), consider and treat arrhythmias e.g. VT
Transfer to further care Provide an alert/information call
YES
Is the ICD firing?
NO
Treat as per clinical guidelines (even if the ICD is firing)
N.B. avoid ICD site if external defibrillation is required
NO
Does the patient have an arrhythmia?
CONSIDER if the ICD is firing?
NO
If the ICD is ineffective or appropriate, disable the ICD
with a ring magnet (if available) and treat as appropriate
SAFETYIt is SAFE to touch a patient who has
an ICD fitted; even if it is firing.
Figure 2 - Implantable Cardioverter Defibrillator Algorithm

Basic Life Support (Child) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 1 of 6
1. INTRODUCTION The following sequence is that followed by those with a duty to respond to paediatric emergencies (also refer to Figure 1: Child Basic Life Support Sequence Algorithm). Age definitions: an infant is a child under one year old. a child is between one year and puberty. These guidelines are not intended to apply to the resuscitation of newborn (refer to neonatal resuscitation guideline). Assess safety - ensure that you, the child
and any bystanders are safe. Check responsiveness - Gently stimulate
the child and ask loudly “Are you all right?” - DO NOT shake infants, or children with suspected cervical spinal injuries.
If the child responds (by answering or moving): Leave the child in the position found
(provided the child is not in further danger).
Check the child’s condition.
Summon help if necessary.
Re-assess the child regularly.
If the child does not respond: Summon help if necessary.
Open the child’s airway by tilting the
head and lifting the chin:
o with the child in the position found, place your hand on the forehead and gently tilt the head back
o at the same time, with your fingertip(s) under the point of the child’s chin, lift the chin. Do not push on the soft
tissues under the chin as this may block the airway
o if you still have difficulty in opening the airway, try the jaw thrust method: place the first two fingers of each hand behind each side of the child’s mandible (jaw bone) and push the jaw forward. Both methods may be easier if the child is turned carefully onto their back.
When there is a risk of back or neck injury, establish a clear upper airway by using jaw thrust or chin lift alone in combination with manual in-line stabilisation of the head and neck by an assistant (if available).
If life-threatening airway obstruction
persists despite effective application of jaw thrust or chin lift, add head tilt a small amount at a time until the airway is open; establishing a patent airway takes priority over concerns about a potential back or neck injury.
Keeping the airway open Look, listen and feel for normal breathing by
putting your face close to the child’s face and looking along the chest:
o look for chest movements o listen at the child’s nose and mouth
for breath sounds o feel for air movement on your
cheek.
Look, listen and feel for no more than 10 seconds before deciding that breathing is absent.
a. If the child IS breathing normally Turn the child onto their side into the
recovery position (see below) taking appropriate precautions if there is any chance of injury to the neck or spine.
Check for continued breathing.

Basic Life Support (Child) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 2 of 6
If the child is NOT breathing or is making agonal gasps (infrequent, irregular breaths): Carefully remove any obvious airway
obstruction. Turn the child carefully on to their back
taking appropriate precautions if there is any chance of injury to the back or neck.
Give 5 initial rescue breaths.
While performing rescue breaths, note
any gasp or cough response to your action. These responses (or their absence), will form part of your assessment of “Signs of life”, which will be described later.
Rescue breaths for an INFANT: Ensure a neutral position of the head and
apply chin lift. Use a bag valve mask device if available
(with a mask appropriate to the size of the child) and inflate the chest steadily over 1–1½ seconds watching for chest rise.
Maintaining head tilt and chin lift, watch the
chest fall as air comes out. Repeat this sequence 5 times.
Identify effectiveness by observing the
child’s chest rise and fall in a similar fashion to the movement produced by a normal breath.
Rescue breaths for a CHILD > 1 year of age: Ensure head tilt and chin lift. Use a bag mask device if available, (with a
mask appropriate to the size of the child) and inflate the chest steadily over 1–1½ seconds watching for chest rise.
Maintaining head tilt and chin lift, watch the
chest fall as air comes out.
Repeat this sequence 5 times. Identify effectiveness by observing the
child’s chest rise and fall in a similar fashion to the movement produced by a normal breath.
Rescue breaths for an INFANT if no bag valve mask is available: Ensure a neutral position of the head and
apply chin lift. Take a breath and cover the mouth and
nose of the infant with your mouth, making sure you have a good seal. In an older infant, if the mouth and nose
cannot be covered, seal either the infant’s nose or mouth with your mouth (if the nose is used, close the lips to prevent air escape). Blow steadily into the child’s mouth and
nose over 1–1½ seconds, sufficient to make the chest visibly rise. Maintain head tilt and chin lift, take your
mouth away from the child and watch for the chest to fall as air comes out.
Take another breath and repeat this
sequence five times.
Identify effectiveness by seeing that the child’s chest has risen and fallen in a similar fashion to the movement produced by a normal breath.
Rescue breaths for a CHILD > 1 year of age if no bag valve mask is available: Ensure head tilt and chin lift. Pinch the soft part of the nose closed with
the index finger and thumb, with the hand on the forehead.

Basic Life Support (Child) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 3 of 6
Open the mouth a little, but maintain chin lift.
Take a breath and place your lips around
the mouth, making sure that you have a good seal.
Blow steadily into the mouth over 1–1½
seconds watching for chest rise. Maintain head tilt and chin lift, take your
mouth away from the child and watch for the chest fall as air comes out.
Take another breath and repeat this
sequence five times. Identify effectiveness by seeing that the
child’s chest has risen and fallen in a similar fashion to the movement produced by a normal breath.
If you have difficulty achieving an effective breath, the airway may be obstructed: Open the child’s mouth and remove any
visible obstruction.
DO NOT perform a blind finger sweep.
Ensure that there is adequate head tilt and chin lift but also that the neck is not over extended.
If head tilt and chin lift has not opened
the airway, try the jaw thrust method.
Make up to 5 attempts to achieve effective breaths.
If still unsuccessful, move on to chest
compressions. Assess the child’s circulation: Take no more than 10 seconds to look for
signs of life. This includes any movement, coughing, or normal breathing (not agonal gasps - these are infrequent, irregular breaths).
Check the pulse but ensure you take no more than 10 seconds to do this: o in a child over 1 year - feel for the
carotid pulse in the neck o in an infant - feel for the brachial pulse
on the inner aspect of the upper arm.
If you are not sure if there is a pulse, assume there is NO pulse.
If you are confident that you can detect signs of a circulation within 10 seconds: Continue rescue breathing, until the
child starts breathing effectively on their own.
If the child remains unconscious, turn
them on to their side (into the recovery position), taking appropriate precautions if there is any chance of injury to the neck or spine.
Re-assess the child frequently.
If there are:
no signs of a circulation OR no pulse OR a slow pulse (less than 60/min with poor perfusion)
OR you are not sure: Start chest compressions Combine rescue breathing and chest
compressions. For all children, compress the lower half of the sternum: Avoid compressing the upper abdomen
by locating the xiphisternum (i.e. find the angle where the lowest ribs join in the midline) and compressing the sternum one finger’s breadth above this point.
Compressions should be sufficient to
depress the sternum by at least 1/3rd of the depth of the chest.

Basic Life Support (Child) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 4 of 6
Release the pressure, and then repeat at a rate of 100-120 per minute.
After 15 compressions, tilt the head, lift the chin and give two effective breaths.
Continue compressions and breaths in a ratio of 15:2.
Lone rescuers may use a ratio of 30:2, particularly if they are having difficulty with the transition between compression and ventilation.
Although the rate of compressions is 100-120 per minute, the actual number of compressions delivered will be less than 100 per minute because of pauses to give breaths.
The best method for compression varies slightly between infants and children (below).
Chest compressions in infants The lone rescuer should compress the
sternum with the tips of 2 fingers. If there are 2 or more rescuers, use the
encircling technique.
Place both thumbs flat side by side on the lower half of the sternum (as above) with the tips pointing towards the infant’s head.
Spread the rest of both hands with the
fingers together to encircle the lower part of the infant’s rib cage with the tips of the fingers supporting the infant’s back.
Press down on the lower sternum with the
two thumbs to depress it at least one-third of the depth of the infant’s chest.
Chest compression in children >1 year of age Place the heel of one hand over the lower
half of the sternum (as above).
Lift the fingers to ensure that pressure is not applied over the child’s ribs. Position yourself vertically above the child’s
chest and, with your arm straight, compress the sternum to depress it by at least 1/3rd of the depth of the chest.
In larger children or for small rescuers, this
may be achieved most easily by using both hands with the fingers interlocked.
Continue resuscitation until: The child shows signs of life (spontaneous
respiration, pulse, movement). You become exhausted. Additional Information RECOVERY POSITION An unconscious child with a clear airway that is breathing spontaneously should be turned on their side into the recovery position: The child should be placed in as near a
true lateral position as possible with their mouth dependent to allow free drainage of fluid.
A small pillow or a rolled-up blanket placed behind their back may be used to maintain an infant/small child in a stable position.
It is important to avoid any pressure on
the chest that impairs breathing. It should be possible to turn a child onto
their side and to return them back easily and safely, taking into consideration the possibility of cervical spine injury.
The airway should be accessible and
easily observed. The adult recovery position is suitable for
use in children.

Basic Life Support (Child) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 5 of 6
Key Points – Paediatric Basic Life Support
If the child is not breathing, carefully remove any obvious airway obstruction but DO NOT perform blind finger sweeps.
Give 5 initial rescue breaths.
Blow steadily into the mouth over 1–1½ seconds watching for chest rise.
If there are: o no signs of life, or o no or a slow pulse (<60 bpm with
poor perfusion) or o you are not sure,
start chest compressions at a rate of 100-120 per minute.
Continue alternating compressions and breaths in a ratio of 15:2.
REFERENCES1 2 1. Biarent D, Bingham R, Eich C, López-Herce J,
Maconochie I, Rodríguez-Núñez A, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 6. Paediatric life support. Resuscitation 2010;81(10):1364-88.
2. Nolan JP, Soar J, Zideman DA, Biarent D, Bossaert LL, Deakin C, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 1. Executive summary. Resuscitation 2010;81(10):1219-76.

Basic Life Support (Child) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 6 of 6
Figure 1 - Child Basic Life Support Sequence Algorithm - Modified from the Resuscitation Council (UK) Guidelines 2010 algorithm for the JRCALC Resuscitation Supplement 2010 (www.resus.org.uk)

Foreign Body Airway Obstruction (Child) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 1 of 4
1. INTRODUCTION The majority of choking events in infants and children occur during play or whilst eating, when a carer is usually present. Events are frequently witnessed and interventions are usually initiated when the child is conscious. Foreign body airway obstruction (FBAO) is characterised by the sudden onset of respiratory distress associated with coughing, gagging or stridor (Table 1).
Similar signs and symptoms may also be associated with other causes of airway obstruction such as laryngitis or epiglottitis, which require different management. Recognition of FBAO When a foreign body enters the airway, the child reacts immediately by coughing in an attempt to expel it.
A spontaneous cough is likely to be more effective and safer than any manoeuvre a rescuer might perform. If coughing is absent or ineffective and the object completely obstructs the airway the child will rapidly become asphyxiated. Active interventions to relieve FBAO are only required when coughing becomes ineffective, but when required they should be commenced confidently and rapidly. Suspect FBAO if: the onset was very sudden there were no other signs of illness there are other clues to alert the rescuer,
e.g. a history of eating or playing with small items immediately prior to the onset of symptoms.
2. ASSESSMENT and MANAGEMENT Assess safety - Do not place yourself in
danger and consider the safest action to manage the choking child.
Assess for the severity of obstruction
refer to Table 1. Effective coughing:
Encourage the child to cough but do nothing else.
Monitor continuously.
Transport rapidly to hospital.
Ineffective coughing or cough becoming ineffective: Summon help if appropriate. Determine the child’s conscious level
CONCIOUS CHILD
Conscious child with ineffective coughing or cough becoming ineffective: Give back blows.
Table 1 - GENERAL SIGNS OF FOREIGN BODY AIRWAY OBSTRUCTION
Witnessed episode
Coughing or choking
Sudden onset
Recent history of playing with or eating small objects
Ineffective coughing
Unable to vocalise Quiet or silent cough Unable to breathe Cyanosis Decreasing level of consciousness
Effective coughing
Crying or verbal response to questions Loud cough Able to breathe before coughing Fully responsive

Foreign Body Airway Obstruction (Child) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 2 of 4
If back blows do not relieve the FBAO, give chest thrusts (infants) or abdominal thrusts (children).
These manoeuvers increase intrathoracic
pressure and may dislodge the foreign body.
Alternate these until the obstruction is relieved or the child loses consciousness.
UNCONCIOUS CHILD
If the child is or becomes unconscious:
Place him/her on a firm, flat surface.
Open the Airway - Open the mouth and look for any obvious object. If one is seen and you think you can grasp it easily, make an attempt to remove it with a single finger sweep.
DO NOT attempt blind or repeated finger
sweeps - these can cause injury and impact the object more deeply into the pharynx.
Attempt ventilation
Open the airway and make 5 attempts to ventilate the lungs.
Assess the effectiveness of each ventilation.
If the chest does not rise, reposition the
head before making the next attempt.
Perform chest compression and CPR if there is no response to 5 attempts at ventilation (moving, coughing, spontaneous breaths).
Proceed to chest compressions without
further assessment of the circulation.
Perform chest compression and CPR Follow the sequence for single rescuer
CPR for approximately 1 minute.
Start with compressions.
When the airway is opened for attempted ventilation, look to see if the foreign body can be seen in the mouth.
If an object is seen, attempt to remove it
with a single finger sweep.
If it appears that the obstruction has been relieved, open and check the airway as above.
Perform ventilation if the child is not
breathing.
If the child regains consciousness and exhibits spontaneous effective breathing, place them in the recovery position. Monitor breathing and conscious level and transfer to hospital.
NOTES ON TECHNIQUES BACK BLOWS - infant: Support the infant in a head-down, prone
position, to allow gravity to assist the removal of the foreign body.
A seated or kneeling rescuer should be
able to support the infant safely across their lap.
Support the infant’s head by placing the
thumb of one hand at the angle of the lower jaw, with one or two fingers from the same hand at the same point on the other side of the jaw.
Do not compress the soft tissues under the
infant’s jaw, as this will exacerbate the airway obstruction.

Foreign Body Airway Obstruction (Child) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 3 of 4
Deliver up to 5 sharp back blows with the heel of one hand in the middle of the back between the shoulder blades, aiming to relieve the obstruction with each blow rather than to give all five.
BACK BLOWS - child over 1 year of age: Back blows are more effective if the child is
positioned head down. A small child may be placed across the
rescuer’s lap as with an infant. If this is not possible, support the child in a forward-leaning position and deliver the back blows from behind.
CHEST and ABDOMINAL THRUSTS If back blows fail to dislodge the object and the child is still conscious, use chest thrusts for infants or abdominal thrusts in older children. Abdominal thrusts (Heimlich manoeuvre) must not be used in infants. Chest thrusts for infants: Turn the infant into a head-down supine
position (this can be safely achieved by placing the free arm along the infant’s back and encircling the occiput with the hand).
Support the infant down your arm, which is
placed down (or across) your thigh.
Identify the landmark for chest compression (lower sternum, approximately a finger’s breadth above the xiphisternum).
Deliver 5 chest thrusts (if required). These
are similar to external chest compressions but sharper in nature and delivered at a slower rate.
Abdominal thrusts for children over 1 year: Stand or kneel behind the child. Place your
arms under the child’s arms and encircle their torso. Clench your fist and place it between the umbilicus and the xiphisternum. Grasp this hand with the other hand and pull sharply inwards and upwards.
Repeat up to 5 times (if required). Ensure that pressure is not applied to the
xiphoid process or the lower rib cage as this may result in abdominal trauma.
REASSESSMENT Following the chest or abdominal thrusts, reassess the child: If the object has not been expelled and
the victim is still conscious, continue the sequence of back blows and chest (for infant) or abdominal (for children) thrusts.
Do not leave the child at this stage.
Arrange transfer to hospital.
If the object is expelled successfully assess the child’s clinical condition. It is possible that part of the object may remain in the respiratory tract and cause complications.
Abdominal thrusts may cause internal
injuries and all victims so treated should be assessed further.

Foreign Body Airway Obstruction (Child) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 4 of 4
Key Points – Foreign Body Airway Obstruction
REFERENCES1 2
1. Nolan JP, Soar J, Zideman DA, Biarent D, Bossaert LL, Deakin C, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 1. Executive summary. Resuscitation 2010;81(10):1219-76.
2. Biarent D, Bingham R, Eich C, López-Herce J, Maconochie I, Rodríguez-Núñez A, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 6. Paediatric life support. Resuscitation 2010;81(10):1364-88.
FBAO is a potentially treatable cause of death that often occurs whilst playing or eating.
It is characterised by the sudden onset of respiratory distress.
If the child is coughing effectively, encourage them to continue to cough.
If coughing is ineffective, back blows should initially be given.
If coughing is ineffective and back blows have failed to relieve the FBAO, use chest thrusts in infants and abdominal thrusts in children.
Abdominal thrusts may cause serious internal bleeding – such patients require further hospital assessment.
Avoid blind finger sweeps.
Figure 1 - Foreign Body Airway Obstruction in Children - Modified from the Resuscitation Council (UK) Guidelines 2010 algorithm for the JRCALC Resuscitation Supplement 2010 (www.resus.org.uk).

Advanced Life Support (Child) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 1 of 4
1. INTRODUCTION Most of the changes in the paediatric guidelines for 2011 have been made to simplify and minimise the differences between adult and paediatric guidelines. Age definitions: an infant is a child under one year old. a child is between one year and puberty. These guidelines are not intended to apply to the resuscitation of newborn (refer to neonatal resuscitation guideline). 2. ASSESSMENT and MANAGEMENT For children requiring advanced life support follow the assessment and management guidance below and refer to Figure 1. Establish basic life support - refer to Basic
Life Support (Child) Guideline. Oxygenate, ventilate, and start chest compression Ensure a patent airway by using an airway
manoeuvre as described in the child basic life support guideline. An adjunct such as an oropharyngeal airway may be needed.
Provide positive pressure ventilation
delivering high flow oxygen.
Provide ventilation initially by bag and mask.
Provide compressions and ventilation at a ratio of 15 compressions to 2 ventilations (The compression rate should be 100 - 120 per minute and the ventilation rate about 10 per minute).
If bag valve mask ventilation is impossible or
impractical, and if the clinician is trained, a laryngeal mask or possibly another supraglottic airway can be used.
In most circumstances, tracheal intubation
should be avoided in children. The technique
is difficult and used only rarely as the skill is very difficult to acquire and maintain.
If intubation has been performed, continuous
compressions are recommended.
Take care to ensure that ventilation remains effective.
Attach a defibrillator or monitor Assess and monitor the cardiac rhythm. Place one defibrillator pad/paddle on the
chest wall just below the right clavicle and the other in the left anterior axillary line.
Use paediatric pads for children <1 year of
age and adult pads ≥1 year of age. For infants, if there are only large pads or paddles available, then it may be more appropriate to apply them to both the front and back of the chest.
Monitoring electrodes should be placed in the
conventional positions. Check for signs of circulation and assess rhythm. Look for signs of life e.g. moving,
responsiveness, coughing, and normal breathing.
Assess the rhythm on the monitor: Non-shockable (i.e. Asystole or Pulseless
Electrical Activity (PEA)). Shockable (Ventricular Fibrillation (VF) or
Pulseless Ventricular Tachycardia (VT). Non-shockable (Asystole, Pulseless Electrical Activity (PEA)) Asystole and PEA are the commonest
paediatric cardiac arrest rhythms. Perform continuous CPR:
o ventilate with high concentration oxygen.

Advanced Life Support (Child) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 2 of 4
o if ventilating with a bag-mask device, give 15 chest compressions to 2 ventilations for all ages.
NOTE: Once there is return of spontaneous circulation (ROSC), gently (as over inflation of the lungs can cause increased intrathoracic pressure, which has a detrimental effect on venous return and hence cardiac output) ventilate at a rate of 12–20 per minute. Administer adrenaline Obtain circulatory access.
Insert a peripheral venous cannula. If
venous access is not readily attainable, give early consideration to intraosseous access.
Give adrenaline 10 micrograms/kg
(0.1ml/kg of 1 in 10,000 solution) IV/IO (see adrenaline guideline).
Continue CPR Repeat the cycle Give 10 micrograms/kg of adrenaline (see
adrenaline guideline) every 3 to 5 minutes (10 micrograms/kg is the dose for all subsequent doses i.e. “high-dose” adrenaline is no longer used).
Continue effective chest compressions and
ventilation without interruption, at a ventilatory rate of approximately 10 per minute and a compression rate of 100 – 120 per minute.
If the airway is protected by tracheal
intubation, chest compressions should be provided without pausing for ventilation.
When circulation is restored, ventilate the
child at a rate of 12 to 20 breaths per minute. Consider and correct reversible causes: 4Hs
1. Hypoxia
2. Hypovolaemia
3. Hyper/hypokalaemia
4. Hypothermia 4Ts
1. Tension pneumothorax
2. Tamponade
3. Toxic/therapeutic disturbance
4. Thromboembolism Shockable (VF/Pulseless VT) These rhythms are less common in paediatric practice but more likely when there has been a witnessed and sudden collapse or in children with underlying cardiac disease. Defibrillate the heart: Give 1 shock of 4 Joules/kg if using a manual
defibrillator, rounding the shock up as necessary to the machine settings. (This energy level is appropriate for both biphasic and the older monophasic defibrillators).
If using an AED in a child over the age of 8
years, use the adult shock energy – paediatric attenuation is not required. If using an AED in a child under the age of 8 years, use a machine with paediatric attenuation (according to the manufacturer’s instructions) when available.
An AED should not routinely be attached to
infants unless they have a history of cardiac problems.
Where an infant is found to have a shockable
rhythm, use a manual defibrillator to administer 4 Joules/kg. (In infants, if a manual defibrillator is not available a paediatric attenuated AED may be used).
If no paediatric attenuated AED is available,
use the adult shock energy at all ages.
Resume CPR: without reassessing the rhythm or feeling for a pulse, resume CPR

Advanced Life Support (Child) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 3 of 4
immediately, starting with chest compressions - continue CPR for 2 minutes:
Then pause briefly to check the monitor If still VF/pulseless VT: give a 2nd shock at 4 Joules/kg as for the 1st
shock (see start of step 6) - resume CPR immediately after the second shock.
Consider and correct reversible causes 4Hs 4Ts (see above). Continue CPR for 2 minutes Pause briefly to check the monitor: If still VF/pulseless VT: give a 3rd shock followed by adrenaline 10
micrograms/kg PLUS an intravenous or intraosseous bolus of Amiodarone 5 milligrams/kg (refer to Amiodarone guideline for further information).
resume CPR immediately and continue for
another 2 minutes. Pause briefly to check the monitor If still VF / pulseless VT give a 4th shock, resume CPR, and continue giving shocks
every 2 minutes, minimising the breaks in chest compressions as much as possible.
give adrenaline after every other shock (i.e.
every 3-5 minutes) until ROSC. After each 2 minutes of uninterrupted CPR, pause briefly to assess the rhythm. If still in VF/VT continue CPR with the shockable rhythm
(VF/VT) sequence. If asystole continue CPR and switch to the non-
shockable (asystole / PEA) sequence as above.
If an organised rhythm appears at any time, check for a central pulse: if there is return of a spontaneous circulation
(ROSC) begin post-resuscitation care. if there is NO pulse, and there are no other
signs of life, or you are not sure, continue CPR as for the non-shockable sequence as above.
Key Points – Advanced Life Support (Child)
Changes in the guidelines have been made to simplify and minimise the differences between adult and paediatric protocols.
One defibrillating shock rather than three stacked shocks should be used.
Intubation is rarely indicated and should only be undertaken by those with appropriate skills.
Automated External Defibrillators (AEDs) If using an AED in a child < 8 years, paediatric
attenuation should be used whenever possible. An unmodified AED may be used in children
older than one year. If an infant is known to have a shockable
rhythm or underlying cardiac problem, a paediatric attenuated AED may be used. If an unmodified AED is the only machine
available, it may be used at all ages or the child/infant will die.
REFERENCES1-3 1. Biarent D, Bingham R, Eich C, López-Herce J,
Maconochie I, Rodríguez-Núñez A, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 6. Paediatric life support. Resuscitation 2010;81(10):1364-88.
2. Nolan JP, Soar J, Zideman DA, Biarent D, Bossaert LL, Deakin C, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 1. Executive summary. Resuscitation 2010;81(10):1219-76.
3. Deakin CD, Nolan JP, Sunde K, Koster RW. European Resuscitation Council Guidelines for Resuscitation 2010 Section 3. Electrical therapies: Automated external defibrillators, defibrillation, cardioversion and pacing. Resuscitation 2010;81(10):1293-304.

Advanced Life Support (Child) – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 4 of 4
Unresponsive?Not breathing or
only occasional gasps?
CPR (5 initial breaths then 15:2)Attach defibrillator / monitor
Minimise interruptions
Assessrhythm
Return of spontaneous circulation
Immediate post cardiac arrest treatment:
- Use ABCDE approach- Controlled oxygenation and ventilation- Investigations- Treat precipitating cause- Temperature control- Therapeutic hypothermia
Shockable(VF / Pulseless VT)
1 Shock 4j/Kg
Immediately resumeCPR for 2 min
Minimise interruptions
Non-Shockable(PEA / Asystole)
Immediately resumeCPR for 2 min
Minimise interruptions
Du
rin
g C
PR Ensure high-quality CPR: rate, depth,
recoil.
Plan actions before interrupting CPR.
Administer oxygen.
Vascular access (intravenous, intraosseous).
Administer adrenaline every 3-5 min.
Consider advanced airway and capnography.
Continuous chest compressions when advanced airway in place
Correct reversible causes.
Rev
ersi
ble
cau
ses
Hypoxia.
Hypovolaemia.
Hypo/hyperkalaemia/metabolic.
Hypothermia.
Tension pneumothorax.
Toxins.
Tamponade – cardiac.
Thromboembolism.
Figure 1 – Advanced Life Support Algorithm - Modified from the Resuscitation Council (UK) Guidelines 2010 algorithm for the JRCALC Resuscitation Supplement 2010 (www.resus.org.uk).

Atropine – Resuscitation Supplement 2010 ATR
Resuscitation Supplement 2010 Page 1 of 2
PRESENTATION Pre-filled syringe containing 1-milligram atropine in 10ml. Pre-filled syringe containing 1-milligram atropine in 5ml. Pre-filled syringe containing 3-milligrams atropine in 10ml. An ampoule containing 600 micrograms in 1ml.
INDICATIONS Symptomatic bradycardia in the presence of ANY of these adverse signs: absolute bradycardia (pulse <40 beats per
minute) systolic blood pressure below expected for
age (refer to page for age guideline for age related blood pressure readings in children)
paroxysmal ventricular arrhythmias requiring suppression
inadequate perfusion causing, for example, confusion etc.
N.B. Hypoxia is the most common cause of bradycardia in children, therefore interventions to support ABC and oxygen therapy should be the first line therapy.
ACTIONS May reverse effects of vagal overdrive. May increase heart rate by blocking vagal activity in sinus bradycardia, second or third degree heart block. Enhances A-V conduction.
CONTRA-INDICATIONS Should NOT be given to treat bradycardia in suspected hypothermia.
SIDE EFFECTS
Dry mouth, visual blurring and pupil dilation. Confusion and occasional hallucinations. Tachycardia, and in the elderly, retention of urine may occur. Do not use small (<100 micrograms) doses as they may cause paradoxical bradycardia.
ADDITIONAL INFORMATION May induce tachycardia when used after myocardial infarction, which will increase myocardial oxygen demand and worsen ischaemia. Hence, bradycardia in a patient with an MI should ONLY be treated if the low heart rate is causing problems with perfusion, such as hypotension.

Atropine – Resuscitation Supplement 2010 ATR
Resuscitation Supplement 2010 Page 2 of 2
DOSAGE AND ADMINISTRATION
SYMPTOMATIC BRADYCARDIA
Route: Intravenous / Intraosseous administer as a rapid bolus
N.B. BRADYCARDIA in children is most commonly caused by HYPOXIA, requiring immediate ABC care, NOT drug therapy; therefore ONLY administer atropine in cases of bradycardia caused by vagal stimulation (e.g. suction).
CONCENTRATION
100 micrograms per ml 200 micrograms per ml 300 micrograms per ml 600 micrograms per ml
AGE INITIAL DOSE VOLUME VOLUME VOLUME VOLUME
≥12 years 600 micrograms 6.0 ml 3.0 ml 2.0 ml 1.0 ml
11 years 600 micrograms 6.0 ml 3.0 ml 2.0 ml 1.0 ml
10 years 600 micrograms 6.0 ml 3.0 ml 2.0 ml 1.0 ml
9 years 500 micrograms 5.0 ml 2.5 ml 1.7 ml 0.8 ml
8 years 500 micrograms 5.0 ml 2.5 ml 1.7 ml 0.8 ml
7 years 400 micrograms 4.0 ml 2.0 ml 1.3 ml 0.7 ml
6 years 400 micrograms 4.0 ml 2.0 ml 1.3 ml 0.7 ml
5 years 300 micrograms 3.0 ml 1.5 ml 1.0 ml 0.5 ml
4 years 300 micrograms 3.0 ml 1.5 ml 1.0 ml 0.5 ml
3 years 240 micrograms 2.4 ml 1.2 ml 0.8 ml 0.4 ml
2 years 240 micrograms 2.4 ml 1.2 ml 0.8 ml 0.4 ml
18 months 200 micrograms 2.0 ml 1.0 ml 0.7 ml 0.3 ml
12 months 200 micrograms 2.0 ml 1.0 ml 0.7 ml 0.3 ml
9 months 120 micrograms 1.2 ml 0.6 ml 0.4 ml 0.2 ml
6 months 120 micrograms 1.2 ml 0.6 ml 0.4 ml 0.2 ml
3 months 120 micrograms 1.2 ml 0.6 ml 0.4 ml 0.2 ml
1 month 100 micrograms 1.0 ml 0.5 ml 0.3 ml 0.2 ml
Birth 100 micrograms 1.0 ml 0.5 ml 0.3 ml 0.2 ml
ADULTS If no improvement administer a repeat dose every 3-5 minutes up to a maximum dose of 3 milligrams
CHILDREN If no improvement administer a repeat dose every 3-5 minutes up to a maximum dose of 600micrograms

Newborn Life Support – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 1 of 4
1. INTRODUCTION Passage through the birth canal is a hypoxic
experience for the fetus since placental respiratory exchange is prevented for the 50–75 seconds duration of the average contraction. Most babies tolerate this well, but those few that do not may require help to establish normal breathing at delivery.
Newborn life support provides this help and
comprises the following elements: 1. drying and covering the baby to conserve
heat 2. assessing the need for any intervention 3. opening the airway 4. lung aeration 5. rescue breathing 6. chest compression.
2. PHYSIOLOGY In the face of in utero hypoxia, the breathing
centres in the fetal brain become depressed and spontaneous breathing ceases. The fetus can maintain an effective circulation in the face of hypoxia, so the most urgent requirement for any asphyxiated baby at birth is aeration of the lungs. Then, provided the circulation has remained intact, oxygenated blood will be conveyed from the lungs to the heart and onwards to the brain. The centres responsible for breathing should recover and the baby will breathe spontaneously.
Merely aerating the lungs is sufficient in the
majority of cases. Where cardiac function has deteriorated to an extent that the circulation is inadequate, a brief period of chest compression may be needed.
In a very small number of cases, lung
aeration and chest compression will not be sufficient - the outlook in this group is poor.
3. SEQUENCE OF ACTIONS (refer to Figure 1) Keep the baby warm and assess Babies are small and born wet. They become
cold very easily, particularly if they are allowed to remain wet and exposed.
A healthy baby will be born blue but will have
a good tone, will cry within a few seconds of delivery, will have a good heart rate (normally 120 – 150 per minute), and will become pink within the first 90 seconds or so.
A less healthy baby will be blue, will have
less good tone, may have a slow heart rate (less than 100 per minute) and may not establish adequate breathing by 90–120 seconds.
An ill (very hypoxic) baby will be born pale
and floppy, not breathing and with a very slow heart rate.
4. ASSESSMENT and MANAGEMENT Whatever the problem: Ensure the ambient temperature is as high as
possible. Reduce drafts. Clamp and cut the cord. Dry the baby. Remove wet towels and cover the baby with
dry towels. Assess: Colour Tone Breathing rate Heart rate: o assess heart rate by listening with a
stethoscope (feeling for a peripheral pulse is not reliable)
o in noisy or very cold environments, palpating the pulse at the umbilical cord may be an alternative and may save unwrapping the baby (This is only reliable when the pulse is >100bpm).
Reassess breathing and heart rate, every 30
seconds. An increase in heart rate is usually the first clinical sign of improvement.
Decide whether help is required (and likely to
be available) or whether rapid evacuation to hospital is indicated. If transferring to hospital follow pre-alert procedure.

Newborn Life Support – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 2 of 4
Once the baby is in the ambulance, the
patient compartment should be kept as warm as can be tolerated (especially if pre-term) even if uncomfortable for the mother and attendant.
Airway The airway must be open for a baby to breathe effectively: Place the baby on their back with the head in
a neutral position i.e. neither flexed nor extended.
If the baby is very floppy, a chin lift or jaw thrust may be necessary.
Breathing If the baby is not breathing adequately by about 90 seconds: Give 5 inflation breaths – use a 500 ml bag
valve mask device. N.B. Until birth the baby’s lungs have been filled with fluid; aeration of the lungs in these circumstances is likely to require sustained application of pressures of about 30 centimetres of water for 2–3 seconds. These are known as inflation breaths. Bag–valve-mask devices should incorporate a safety device that allows this pressure to be generated yet prevents higher pressures that might damage the lungs.
Heart Rate If the heart rate increases: Assume that lung aeration has been successful. If the heart rate increases but the baby does not start breathing: Continue to provide regular breaths
(ventilation breaths) at a rate of about 30–40 per minute until the baby starts to breathe on their own. N.B. Ventilation breaths do not need as long an inspiratory time as inflation breaths (~ 1 second).
Continue to monitor the heart rate. If the rate
should drop <100 bpm it suggests insufficient ventilation. In this situation, increase the rate of inflation or use a longer inspiratory time.
If the heart rate does not increase following inflation breaths: Either lung aeration has not been adequate or
the baby requires more than lung aeration alone.
It is most likely that you have not aerated the
lungs effectively.
If the heart rate does not increase and the chest does not move with each inflation you have not aerated the lungs; in this situation consider: 1. Is the head in the neutral position? 2. Do you need jaw thrust? 3. Do you need a longer inflation time? 4. Do you need help with the airway from a
second person? 5. Is there obstruction in the oropharynx
(laryngoscope and suction)? 6. Do you need an oropharyngeal airway?
Check the baby’s head is in the neutral
position; that breaths are at the correct pressure and applied for the correct time and the chest moves with each breath.
If the chest still does not move, consider an
obstruction in the oropharynx that may be removable under direct vision.
If after 5 inflation breaths the heart rate remains
slow (<60bpm), or the heart beat is absent despite good passive chest movements in response to inflations. Start chest compressions.
If the baby is not vigorous at birth or does not
respond very rapidly to bag-valve-mask ventilation undertake a TIME CRITICAL transfer. Provide an alert/information call.
If the mother has received morphine or any
other opiate within the previous four hours and the baby does not breathe adequately: o administer naloxone intramuscularly (refer
to naloxone drug guideline) o provide respiratory support until it takes
effect.

Newborn Life Support – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 3 of 4
Circulation If chest compressions are necessary: Ensure that the lungs have been successfully
aerated. In newborns, encircle the lower chest with both
hands in such a way that the two thumbs can compress the lower 1/3
rd of the sternum, at a
point just below an imaginary line joining the nipples, with the fingers over the spine at the back.
Compress the chest quickly and firmly in such
a way as to reduce the antero-posterior diameter of the chest by 1/3
rd.
The ratio of compressions to inflations in
newborn resuscitation is 3:1 Meconium Attempting to aspirate meconium from a
baby’s mouth and nose while their head is still on the perineum does not prevent meconium aspiration and is not recommended.
Also, attempts to aspirate meconium from a
vigorous baby’s airway after birth will not prevent meconium aspiration and therefore is no longer recommended.
If a baby is born through thick meconium and is
unresponsive at birth, the oropharynx should be inspected and cleared of meconium. The larynx and trachea should also be cleared if a suitable laryngoscope is available. This should not however unduly delay initial attempts to inflate the lungs.
ADDITIONAL INFORMATION There is no evidence to suggest that any one
concentration of oxygen is better than another when starting resuscitation. Air has also been shown to be equally effective. Whenever possible, additional oxygen should be available if there is not a rapid improvement in the baby’s condition.
Key Points – Newborn Life Support
Passage through the birth canal is a hypoxic experience and some babies may require help to establish normal breathing at delivery.
Babies become cold very easily. Dry the baby, remove any wet towels and replace with dry ones. Once in the ambulance keep the compartment as warm as possible.
Ensure the airway is open by placing the baby on their back with the head in a neutral position. If the baby is very floppy it may be necessary to apply a chin lift or jaw thrust.
If the baby is not breathing adequately by about 90 seconds give 5 inflation breaths.
If chest compressions are necessary compress the chest quickly and firmly at a ratio of 3:1 compressions to inflations. Use a two thumbs encircling technique.
REFERENCES
1 2
1. Nolan JP, Soar J, Zideman DA, Biarent D, Bossaert LL, Deakin C, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 1. Executive summary. Resuscitation 2010;81(10):1219-76.
2. Richmond S, Wyllie J. European Resuscitation Council Guidelines for Resuscitation 2010: Section 7. Resuscitation of babies at birth. Resuscitation 2010;81(10):1389-99.

Newborn Life Support – Resuscitation Supplement
Resuscitation Supplement 2010 Page 4 of 4
Figure 1 – Newborn Life Support Algorithm - Modified from the Resuscitation Council (UK) Guidelines 2010 algorithm for the JRCALC Resuscitation Supplement 2010 (www.resus.org.uk)
Dry the babyRemove any wet towels and cover
Start the clock or note the time
Assess (tone)breathing and heart rate
If gasping or not breathing:Open the airway
Give 5 inflation breaths
Consider Sp02
Re-assess
If no increase in heart rateLook for chest movement
If chest not moving:Recheck head position
Consider 2-person airway control and other airway manoeuvers
Repeat inflation breaths
Consider Sp02
Look for a response
If no increase in heart rate
look for chest movement
When the chest is moving:
If heart rate is not detectable or slow (<60) Start chest compressions -
3 compressions to each breath
Re-assess heart rate every 30 seconds.
Undertake a TIME CRITICAL transfer immediately.
Provide a pre-alert/information message.
AT
AL
L S
TA
GE
S A
SK
: D
O I
NE
ED
HE
LP
?
Acceptable Sp02
2 min 60%3 min 70%4min 80%5 min 85%10 min 90%
60 sec
Birth
30 sec

Cardiac Rhythm Disturbance – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 1 of 5
1. INTRODUCTION Cardiac arrhythmia is a common
complication of acute myocardial ischaemia or infarction and may precede cardiac arrest or complicate the early post-resuscitation period.
Rhythm disturbance may also present in
many other ways and be unrelated to coronary heart disease.
The management of disorders of cardiac
rhythm is a specialised subject, often requiring detailed investigation and management strategies that are not available outside hospital.
Diagnosis of the precise rhythm
disturbance may be complicated and the selection of optimal treatment difficult. Very often expert advice will be required, yet this expertise is rarely immediately available in the emergency situation.
2. PRINCIPLES OF TREATMENT Management is determined by the
condition of the patient as well as the nature of the rhythm. Manage the patient using the standard ABCDE approach.
In all cases give high concentration
oxygen and aim for a target saturation within the range of 94-98%.
Gain venous access. Always take a defibrillator to any patient
with suspected cardiac rhythm disturbance.
Establish cardiac rhythm monitoring as
soon as possible.
Document the arrhythmia. This should be done with a 12 lead ECG whenever possible. If only a 3-lead ECG is available, lead II provides the best waveform for arrhythmia analysis.
Provide a printout for the hospital and if possible archive the record electronically so that further copies can be available at a later time if needed. Repeat the recording if the rhythm should change at any time. Record the ECG rhythm during any intervention (vagotonic procedures or the administration of drugs).
If patients are not acutely ill there may be
time to seek appropriate advice. The presence of adverse signs or
symptoms will dictate the need for urgent treatment. The following adverse factors indicate a patient who is unstable because of the arrhythmia:
o evidence of low cardiac output: pallor,
sweating, cold clammy extremities, impaired consciousness or hypotension (SBP <90mmHg)
o excessive tachycardia, defined as a
heart rate of >150bpm
o excessive bradycardia, defined as a heart rate of <40bpm
o heart failure implies the arrhythmia is
compromising left ventricular function. This may cause breathlessness, confusion and hypotension or other features of reduced cardiac output
o ischaemic chest pain implies that the
arrhythmia (particularly tachyarrhythmia) is producing myocardial ischaemia. It is particularly important if there is underlying coronary disease or structural heart disease in which ischaemia is likely to lead to life threatening complications including cardiac arrest.

Cardiac Rhythm Disturbance – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 2 of 5
3. BRADYCARDIA Introduction A bradycardia is defined as a ventricular
rate below 60bpm, but it is important to recognise patients with a relative bradycardia in whom the rate is inappropriately slow for their haemodynamic state.
4. Risk of ASYSTOLE ASSESSMENT and MANAGEMENT For the assessment and management of bradycardia and risk of asystole see below.
Bradycardia
A ventricular rate below 60 bpm, but it is important to recognise patients with a relative bradycardia in whom the rate is inappropriately slow for their haemodynamic state.
Assess to determine if one or more adverse signs are present:
Systolic blood pressure <90mmHg.
Ventricular rate <40bpm.
Ventricular arrhythmias compromising BP requiring treatment.
Heart failure.
If one or more signs are present:
Administer high levels of supplemental oxygen – aim for target saturation within the range 94-98%.
Gain IV access. Administer atropinea (refer to atropine
guideline) and repeat after 3–5 minutes if necessary or transcutaneous pacing.
Undertake an ECG. Transfer to further care.
a Caution
- Doses of atropine lower than 500mcg may
paradoxically cause further slowing of ventricular rate. Use atropine cautiously in acute myocardial ischaemia or infarction; an increased rate may worsen ischaemia.
Risk of Asystole
If the patient is initially stable (i.e. no adverse signs are present) or a satisfactory response is achieved with atropine, next determine the risk of asystole.
Assess for risk of asytole - This is indicated by: Previous episode of asystole. Möbitz II AV block. Complete (third degree) AV block,
especially with a broad QRS complex or an initial ventricular rate <40bpm.
Ventricular standstill >3 seconds. If there is a risk of asytole (i.e. one or more signs are present) or the patient shows adverse signs and has not responded satisfactorily to atropine, transvenous pacing is likely to be required. One or more of the following interventions may improve the patient’s condition during transport: a. transcutaneous pacing should be
undertaken if available. If transcutaneous pacing is not available: b. fist pacing may produce ventricular
contraction - give serial rhythmic blows with the closed fist over the lower left sternal edge to pace the heart at a rate of 50–70bpm.
NOTES:
Do not give atropine to patients with cardiac transplants; paradoxical high degree AV block or sinus arrest may result.
Complete heart block with a narrow QRS complex escape rhythm may not require pacing. The ectopic pacemaker (which is situated in the atrioventricular junction) may provide a stable rhythm at an adequate rate.
Initiate transcutaneous pacing (if equipment is available):

Cardiac Rhythm Disturbance – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 3 of 5
o if there is no response to atropine o patient is severely symptomatic,
particularly when high degree block (Möbitz type II or third degree AV block) is present.
N.B. Transcutaneous pacing may be painful; use analgesia. Verify mechanical capture. Monitor the patient carefully; try to identify the cause of the bradycardia.
5. TACHYCARDIA Introduction These guidelines are intended for the
treatment of patients who maintain a cardiac output in the presence of the tachycardia.
Pulseless tachycardia is treated
according to the cardiac arrest algorithm for the treatment of pulseless VT/VF.
BROAD COMPLEX TACHYCARDIA
NARROW COMPLEX TACHYCARDIA ASSESSMENT and MANAGEMENT For the assessment and management of tachycardia, broad complex tachycardia, and narrow complex tachycardia see below. Tachycardia: These guidelines are intended for the
treatment of patients who maintain a cardiac output in the presence of the tachycardia.
Pulseless tachycardia is treated with
immediate attempts at cardioversion following the algorithm for the treatment of pulseless VT/VF.
a. Support the ABCs. b. Administer high levels of
supplemental oxygen – aim for target saturation 94-98%.
c. Gain IV access.
d. Establish cardiac rhythm monitoring. e. Record and monitor BP and SpO2. f. Record a 12-lead ECG if possible, if
not, record a rhythm strip. g. If the rhythm changes at any time,
make a further recording. h. Make a continuous record of the
rhythm during any therapeutic intervention (whether a drug or physical manoeuvre such as carotid sinus massage).
i. The response to treatment can provide important additional information about the arrhythmia.
j. Identify and treat reversible causes; give analgesia if indicated.
k. Try to define the cardiac rhythm from the ECG. Determine the QRS duration and determine whether the rhythm is regular or irregular. If the QRS duration is 120msec or more the rhythm is a broad complex tachycardia. If less than 120msec, the rhythm is a narrow complex tachycardia.
Broad Complex Tachycardia:
The rhythm is likely to be ventricular tachycardia, particularly in the context of ischaemic heart disease in patients showing adverse signs (reduced consciousness, SBP <90mmHg, chest pain or heart failure), or in the peri-arrest situation.
In all cases, maintain the supportive
measures above and monitor the patient during transport.
Provide a pre-alert message according to
local protocols.
Atrial fibrillation conducted aberrantly may produce an irregular broad complex tachycardia, but the diagnosis is difficult to make with certainty and often requires expert examination of the ECG. This emphasises the importance of recording

Cardiac Rhythm Disturbance – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 4 of 5
the ECG when the arrhythmia is present. Ambulance personnel may greatly assist the subsequent diagnosis and management of patients by obtaining good quality ECG recordings. It is advantageous if these can also be archived electronically so that additional copies are available in the future. It is frustratingly common for paper copies of ECGs to be lost after admission to hospital.
Narrow Complex Tachycardia: If the rhythm is narrow complex (QRS
<120 msec) AND REGULAR, it is likely to be either:
o sinus tachycardia. This is a physiological response, for example, to pain, fever, blood loss or heart failure. Treatment is directed towards the cause. Trying to slow the rate is likely to make the situation worse
o supraventricular tachycardia (SVT).
This is often seen in patients without other forms of heart disease. There may be a history of previous attacks
o atrial flutter with regular AV
conduction (often 2:1 and a rate of 150bpm).
If sinus tachycardia is absent, start with
vagal manoeuvres. In some cases the patient may be aware of techniques that have terminated previous episodes. The Valsalva manoeuvre (forced expiration against a closed glottis) may be effective and is conveniently achieved (especially in supine patients) by asking the patient to blow into a 20ml syringe with sufficient force to push back the plunger. If this fails, perform carotid sinus massage provided no carotid bruit is heard on auscultation. A bruit may indicate the presence of atheromatous plaque, rupture of which may cause cerebral embolism and stroke.
Record the ECG (preferably multi-lead) during each manoeuvre. If the arrhythmia is successfully terminated by vagal procedures, it is very likely to have been SVT. If the rhythm is atrial flutter, slowing of ventricular rate may occur and allow the identification of flutter waves on the ECG.
Maintain the supportive measures above
and monitor the patient during transport.
AN IRREGULAR narrow complex rhythm is most commonly atrial fibrillation, less commonly atrial flutter with variable block. Maintain the supportive measures above and monitor the patient during transport.
In all cases, ensure the patient is received
into a suitable high dependency unit maintaining cardiac monitoring throughout. Ensure detailed hand-over to appropriate staff and that ECGs are safely handed over.
Key Points – Cardiac Rhythm Disturbance
In all cases give high concentration oxygen.
Gain venous access. Always take a defibrillator to any patient
with suspected cardiac rhythm disturbance.
Establish cardiac rhythm monitoring as soon as possible preferably with a 12-lead ECG.
Record the ECG rhythm during any intervention and archive. Ensure all ECGs are safely handed over to receiving staff and archive so further copies can be retrieved if necessary.

Cardiac Rhythm Disturbance – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 5 of 5
REFERENCES1-6 1. Deakin CD, Nolan JP, Soar J, Sunde K,
Koster RW, Smith GB, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 4. Adult advanced life support. Resuscitation 2010;81(10):1305-52.
2. Nolan JP, Soar J, Zideman DA, Biarent D, Bossaert LL, Deakin C, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 1. Executive summary. Resuscitation 2010;81(10):1219-76.
3. Koster RW, Baubin MA, Bossaert LL, Caballero A, Cassan P, Castrén M, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 2. Adult basic life support and use of automated external defibrillators. Resuscitation 2010;81(10):1277-92.
4. Deakin CD, Nolan JP, Sunde K, Koster RW. European Resuscitation Council Guidelines for Resuscitation 2010 Section 3. Electrical therapies: Automated external defibrillators, defibrillation, cardioversion and pacing. Resuscitation 2010;81(10):1293-304.
5. Biarent D, Bingham R, Eich C, López-Herce J, Maconochie I, Rodríguez-Núñez A, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 6. Paediatric life support. Resuscitation 2010;81(10):1364-88.
6. Soar J, Perkins GD, Abbas G, Alfonzo A, Barelli A, Bierens JJLM, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 8. Cardiac arrest in special circumstances: Electrolyte abnormalities, poisoning, drowning, accidental hypothermia, hyperthermia, asthma, anaphylaxis, cardiac surgery, trauma, pregnancy, electrocution. Resuscitation 2010;81(10):1400-33.

Recognition of Life Extinct by Ambulance Clinicians – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 1 of 6
1. INTRODUCTION In patients with cardio-pulmonary arrest, vigorous resuscitation attempts must be undertaken whenever there is a chance of survival, however remote. Nevertheless, it is possible to identify patients in whom there is absolutely no chance of survival, and where resuscitation would be both futile and distressing for relatives, friends and healthcare personnel and where time and resources would be wasted undertaking such measures. The views of an attending General Practitioner (GP), ambulance doctor or relevant third party should be considered. CONDITIONS UNEQUIVOCALLY ASSOCIATED WITH DEATH WHERE RESUSCITATION SHOULD NOT BE ATTEMPTED All the conditions, listed below, are unequivocally associated with death in ALL age groups (see below for further details): 1. massive cranial and cerebral destruction 2. hemicorporectomy or similar massive
injury 3. decomposition/putrefaction 4. incineration 5. hypostasis 6. rigor mortis In the newborn, fetal maceration is a contraindication to attempted resuscitation. FURTHER DETAILS Decapitation: Self evidently incompatible with life. Massive cranial and cerebral destruction: Where the injuries are considered by the ambulance clinician to be incompatible with life.
Hemicorporectomy (or similar massive injury): Where the injuries are considered by the ambulance clinician to be incompatible with life. Decomposition/putrefaction: Where tissue damage indicates that the patient has been dead for some hours, days or longer. Incineration: The presence of full thickness burns with charring of greater than 95% of the body surface. Hypostasis: The pooling of blood in congested vessels in the dependent part of the body in the position in which it lies after death (See Guidance Note 1). Rigor mortis: The stiffness occurring after death from the post mortem breakdown of enzymes in the muscle fibres (See Guidance Note 2). In all other cases resuscitation must be commenced and the facts pertaining to the arrest must be established. Following arrival and the recognition of an absent pulse and apnoea (in the presence of a patent airway), chest compression and ventilations should be commenced whilst the facts of the collapse are ascertained. IN THE FOLLOWING CONDITIONS, RESUSCITATION CAN BE DISCONTINUED The presence of a DNAR (Do Not
Attempt Resuscitation) order or an Advanced Decision (Living Will) that states the wish of the patient not to undergo attempted resuscitation (see 3b).
“A patient in the final stages of a terminal illness where death is imminent and unavoidable and CPR would not be successful, but for whom no formal DNAR decision has been made”1.

Recognition of Life Extinct by Ambulance Clinicians – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 2 of 6
There would be no realistic chance that
CPR would be successful if ALL the following exist together:
o 30 minutes since the onset of collapse
o no bystander CPR prior to arrival of the ambulance
o the absence of any of the exclusion factors on the flowchart (Figure 1)
o asystole (flat line) for >30 seconds on the ECG monitor screen.
Submersion for longer than 1.5 hours (N.B. submersion NOT immersion) (See Guidance Note 3).
Whenever possible a confirmatory ECG, demonstrating asystole, should be documented as evidence of death. In this situation a 3 or 4 electrode system using limbs alone will cause minimum disturbance to the deceased. If a paper ECG trace cannot be taken it is permissible to make a diagnosis of asystole from the screen alone (N.B. due caution must be applied in respect of electrode contact, gain and, where possible, using more than one ECG lead). The use of the flow chart shown in Figure 1 is recommended. If there is a realistic chance that CPR could be successful then resuscitation must continue to establish the patients’ response to Advanced Life Support interventions. If the patient does not respond despite full ALS intervention and remains asystolic for >20 minutes then the resuscitation attempt may be discontinued. Removal of tracheal tubes and/or indwelling cannulae should be in accordance with local protocol.
DO NOT ATTEMPT RESUSCITATION (DNAR) / ADVANCED DECISION TO REFUSE TREATMENT (LIVING WILL) Ambulance clinicians should initiate resuscitation unless: 1. A formal DNAR order is in place, either written and handed to the ambulance crew or verbally received and recorded by Ambulance Control from the patient‟s attendant requesting the ambulance providing that:
a. the order is seen and corroborated by the ambulance crew on arrival b. the decision to resuscitate relates to the condition for which the DNAR order is in force: resuscitation should not be withheld for coincidental conditions.
2. The patient is in the final stages of a terminal illness where death is imminent and unavoidable and CPR would not be successful, but for whom no formal DNAR decision has been made”.1 3. An Advanced Decision (Living Will) has been accepted by the treating physician (patient‟s GP or Hospital Consultant) as a DNAR order. This should be communicated to Ambulance Control and logged against the patient‟s address.
a. Patients may have an Advanced Decision (Living Will) although it is not legally necessary for the refusal to be made in writing or formally witnessed. This specifies how they would like to be treated in the case of future incapacity. Case law is now clear that an advance refusal of treatment that is valid, and applicable to subsequent circumstances in which the patient lacks capacity, is legally binding. An advance refusal is valid if made voluntarily by an appropriately informed person with capacity. Staff should respect the wishes stated in such a document. b. In an out of hospital emergency environment, there may be situations

Recognition of Life Extinct by Ambulance Clinicians – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 3 of 6
where there is doubt about the validity of an advance refusal or DNAR order. If staff are NOT satisfied that the patient had made a prior and specific request to refuse treatment, they should continue to provide all clinical care in the normal way.
ACTION TO BE TAKEN AFTER DEATH HAS BEEN ESTABLISHED For guidance on the actions to be taken following verification of death refer to Figure 2. Complete documentation – including all decisions regarding do not attempt resuscitation (DNAR) / advanced decision to refuse treatment. In light of the fact that earlier guidelines have been in use by a number of Services for almost 10 years, we no longer believe that it is necessary for a medical practitioner to attend to confirm the fact of death. Moreover, the new GP Contract contains no obligation for a GP to do so when requested to attend by Ambulance Control. Services should be encouraged, in conjunction with their coroner‟s service (or Procurator Fiscal in Scotland), to develop a local procedure for handling the body once death has been verified by ambulance personnel. We further propose the adoption of a locally approved leaflet for handing to bereaved relatives. GUIDANCE NOTE 1 Initially, hypostatic staining may appear as small round patches looking rather like bruises, but later these coalesce to merge as the familiar pattern. Above the hypostatic engorgement there is obvious pallor of the skin. The presence of hypostasis is diagnostic of death – the appearance is not
present in a live patient. In extremely cold conditions hypostasis may be bright red in colour, and in carbon monoxide poisoning it is characteristically „cherry red‟ in appearance. GUIDANCE NOTE 2 Rigor mortis occurs first in the small muscles of the face, next in the arms, then in the legs (30 minutes to 3 hours). Children will show a more rapid onset of rigor because of their large surface area/body mass ratio. The recognition of rigor mortis can be made difficult where, rarely, death has occurred from tetanus or strychnine poisoning. It is stated that the diagnosis of rigor mortis can be confirmed by firmly pressing on a joint such as the knee, when the rigor mortis will be abolished and the joint becomes flaccid. In some, rigidity never develops (infants, cachectic individuals and the aged) whilst in others it may become apparent more rapidly (in conditions in which muscle glycogen is depleted): exertion (which includes struggling), strychnine poisoning, local heat (from a fire, hot room or direct sunlight). Rigor should not be confused with cadaveric spasm (sometimes referred to as instant rigor mortis) which develops immediately after death without preceding flaccidity following intense physical and/or emotional activity. Examples include: death by drowning or a fall from a height. In contrast with true rigor mortis only one group of muscles is affected and NOT the whole body. Rigor mortis will develop subsequently. GUIDANCE NOTE 3 Submersion victims Attempting to predict criteria for commencing resuscitative efforts on victims found in water is fraught with danger because of many interacting factors that may contribute to extending accepted anoxic survival times.

Recognition of Life Extinct by Ambulance Clinicians – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 4 of 6
Chief among these is the heat exchange that occurs in the lungs following aspiration of water. Should the water temperature be very cold, it will rapidly cool the blood in the pulmonary circulation, which in turn selectively cools the brain for as long as a viable cardiac output continues. Should brain temperature be rapidly cooled to a degree where protection from hypoxia/anoxia is possible (circa 20°C) in the 70 seconds or thereabouts before cardiac failure occurs, then the chances of successful resuscitation are considerably enhanced even if cardio-respiratory arrest has been present for an hour or more. For this outcome to be likely, the water temperature has to be near freezing, and usually, but not necessarily, the body mass relatively small. Hence the majority of the accounts of successful resuscitation after submersion pertain to small children being rescued from „ice water‟. It would seem prudent that resuscitative efforts should be made on: 1. Those with a witnessed submersion
time of 1.5 hours or less, even though they appear to be dead on rescue.
2. All those where there is a possibility of their being able to breathe from a pocket of air while underwater.
3. Anyone showing any signs of life on initial rescue.
4. Those whose airway has been only intermittently submerged for the duration of their immersion, e.g. those wearing lifejackets but in whom the airway is being intermittently submerged, provided the body still has a reasonably fresh appearance.
5. Resuscitative efforts are unlikely to be successful in those submerged for periods exceeding 1.5 hours with the exception of those in categories 2-4 above.
Key Points – Recognition of Life Extinct by Ambulance Clinicians
Ambulance clinicians are increasingly called upon to diagnose death and initiate the appropriate responses to death.
In patients with cardio-pulmonary arrest, vigorous resuscitation efforts must be made whenever there is a chance of survival however remote.
Some conditions are incompatible with recovery and in these cases resuscitation need not be attempted.
In some situations, once the facts of the patient/situation/etc are known, resuscitation efforts can be discontinued.
Patients can and do make anticipatory decisions NOT to be resuscitated. An Advanced Decision (Living Will), if verifiable, must be respected.
These guidelines should be read in conjunction with local policies and procedures.
REFERENCES2 3 4 1. BMA, Resuscitation Council (UK), Royal
College of Nursing. Decisions Relating to Cardio-Pulmonary Resuscitation: a joint statement. London: Available from: http://www.rcn.org.uk/__data/assets/pdf_file/0004/108337/003206.pdf, 2007.
2. Nolan JP, Soar J, Zideman DA, Biarent D, Bossaert LL, Deakin C, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 1. Executive summary. Resuscitation 2010;81(10):1219-76.
3. Richmond S, Wyllie J. European Resuscitation Council Guidelines for Resuscitation 2010: Section 7. Resuscitation of babies at birth. Resuscitation 2010;81(10):1389-99.
4. Lippert FK, Raffay V, Georgiou M, Steen PA, Bossaert L. European Resuscitation Council Guidelines for Resuscitation 2010 Section 10. The ethics of resuscitation and end-of-life decisions. Resuscitation 2010;81(10):1445-51.

Recognition of Life Extinct by Ambulance Clinicians – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 5 of 6
Cardiac Arrest
Condition unequivocally associated with death? DNAR, final stages of terminal illness, prolonged (>1.5 hours) submersion?
NO
Start ventilations and
chest compressions
Attach defibrillator and analyse rhythm – is
a shock advised?
YES
Follow full resuscitation protocol
If the patient is in asystoledespite 20 minutes of ALS
cease resuscitation -
EXCEPT in cases of drowning and hypothermia
NO
Evidence of CPR in
past 30 minutes?
YES or Don’t know
NO
Any suspicion of:Drowning?
Hypothermia?
Poisoning or overdosePregnancy?
Asystole >30 seconds?
Cease resuscitation
YES
Cease resuscitation
Pulseless/Apnoeic
with open airway
YES
NO
1. massive cranial and cerebral destruction2. hemicorporectomy or similar massive injury3. decomposition/putrefaction4. incineration5. hypostasis6. rigor mortis.
Pregnancy is an indication for rapid transfer to hospital to deliver the infant, if necessary by emergency Caesarean section in order to resuscitate the infant.
NO
YES
Figure 1 – Recognition of Life Extinct by Ambulance Clinicians Algorithm

Recognition of Life Extinct by Ambulance Clinicians – Resuscitation Supplement 2010
Resuscitation Supplement 2010 Page 6 of 6
Diagnose death
Are there any suspicious
circumstances
NO
Are relatives present?
YESOffer condolences
Leave leaflet with relatives
Notify control – if death expected contact GP/OOH– if death unexpected pass to Coroner as per local pathway
Complete documentation
NOSeek contact details (control may have some)
Where none ask control to contact Police.
Remain on scene until police or other person arrivesComplete documentation
Death at home or place
of normal residence?Death in public place?
YES
Take steps to preserve the scene.Ask control to contact the
Police – if indicated by local pathway agreed by Coroner. Remain on scene.Complete documentation.
Handle the body as per local procedure. Request control to inform the Police of the details of the case and if the body has been removed, the destination. Leave the documentation with the body.
Figure 2 – Action to be taken after verification of fact of death




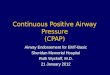
















![EVALUATION OF UPPER AIRWAY PATENCY DURING ......2012/05/16 · obstructive and central apneas in CSR-CHF [7, 8], that CSR can be affected by posture, [9, 10] and may be suppressed](https://img.pdfslide.us/doc/110x75/5f9965829dd89a11cb7dc845/evaluation-of-upper-airway-patency-during-20120516-obstructive-and.jpg)






