Embed Size (px)
Citation preview
COMMON LEARNING OUTCOMES / COMPETENCES FOR THE BACHELOR OF
MEDICINE IN EUROPE
THE MEDINE2 BOLOGNA FIRST CYCLE
TUNING PROJECT
Prepared with the support of a Grant from the European Commission
No. 155731-LLP-1-2009-1-UK-ERASMUS-ENWA

2
Michael Ross, Allan Cumming
On behalf of the WP4 Working Group of the
MEDINE2 Thematic Network
Dr Michael T Ross
WP4 Leader. Senior Clinical Lecturer, Centre for Medical Education, College of Medicine and Veterinary Medicine, The University of Edinburgh
Professor Allan D Cumming
MEDINE2 Chair. Professor of Medical Education and Dean of Students, College of Medicine and Veterinary Medicine, University of Edinburgh

3
INDEX
Executive summary 4
Background 5
The Bologna Process 5
Implementing the Bachelor of Medicine 5
The Tuning Project (Medicine) 6
Terminology 7
Methods 8
Research process 8
Questionnaire design 8
Data analysis 9
Results 10
Respondent demographics 10
Quantitative data 10
Level 1 learning outcomes (table) 11
Level 2 learning outcomes (table) 13
Learning outcomes in medical professionalism (table) 23
Subgroup analysis 27
Qualitative data 27
Comment 28
Key findings of this research 28
Conclusions and implications 29
References 30
Contributors to Workpackage 4 31
Acknowledgements 31
4
EXECUTIVE SUMMARY
The Bologna Process requires European Higher Education institutions to adopt a three-
cycle system of Bachelor, Master and Doctor degrees. A research-based approach to
gain consensus on core learning outcomes for these was developed by the Tuning Project,
and previously used by Tuning (Medicine) for primary medical degrees (Master of
Medicine) across Europe. The Bachelor of Medicine remained controversial, however,
with differing opinions on whether core learning outcomes could or should be defined. This
booklet reports the findings of the MEDINE2 (www.medine2.com) Workpackage 4 study
on common learning outcomes / competences for the Bachelor of Medicine in Europe. An
online survey, based on Tuning (Medicine) results, was developed and widely
disseminated to stakeholders. Respondents indicated, on a Likert scale, to what extent
they thought students should have achieved each learning outcome on successful
completion of the first three years (180 ECTS) of university education in medicine. There
were 560 responses, representing medical students, academics, graduates, employers
and patients from virtually all EU countries. Respondents broadly agreed that all learning
outcomes defined by the Tuning (Medicine) project for primary medical degrees should be
achieved to some extent in the First Cycle. Free text comments suggested some
additional learning outcomes, and reinforced the importance of early patient contact and
practical clinical experience. Broad consensus was achieved from a range of key
stakeholders across Europe on core learning outcomes for a Bachelor of Medicine degree.
Defining the Bachelor of Medicine degree in this way promotes early patient contact and
clinical experience, and thus promotes integration in the undergraduate medical curriculum
and may also facilitate mobility.
5
BACKGROUND
The Bologna Process
The Bologna Process requires all European Higher Education institutions to adopt a three-
cycle system of Bachelor, Master and Doctor degrees (www.ehea.com). These three
‘cycles’ are defined for all academic disciplines by the ‘Dublin Descriptors’ (Joint Quality
Initiative 2004). The Bologna Process, and the Bachelor of Medicine in particular, has
been controversial in medicine, and is strongly debated in the literature (Christensen 2004;
AMEE et al. 2005; Rigby 2007; AMEE et al. 2010; Cumming 2010; Davies 2010; Patrício
and Harden 2010). Potential benefits reported include enhanced transparency (with easily
readable and comparable degrees); mobility and choice (with transferable degrees and
additional exit points); and enhanced patient safety (since medical graduates can already
freely move around Europe, but may have very different competences). Potential
concerns reported include loss of integration of medical curricula; standardisation and
lowering of quality; competitive entry to Masters degree programmes so some students
are unable to continue their medical studies or find a suitable job; Bachelor of Medicine
graduates being employed as a cheaper alternative to trained doctors; risks to patient
safety; and increasing outside interference with medical training.
Implementing the Bachelor of Medicine
Many countries have been slow to adopt the three-cycle system (Patrício et al. 2008). A
recent survey only 32 of the 442 medical schools in Bologna signatory countries had
adopted the Bachelor-Master two cycle medical curriculum, with most of the others
retaining a single undergraduate primary medical degree (Patrício et al. 2012). Medical
schools which had adopted the two cycles in Belgium, the Netherlands, Denmark,
Switzerland, Armenia, Portugal and Iceland, reported no significant problems in
implementation or any significant interference with curriculum integration (Patrício et al.
2012). One medical school studied the impact on student career choices and found no
increase in students interrupting, discontinuing or transferring their medical studies after
the Bachelor phase (van den Broek et al. 2010)

6
The Tuning Project (Medicine)
A research-based approach to gain consensus on core learning outcomes / competences
was developed by the Tuning Project (http://www.unideusto.org/tuning/; ), and used by
Tuning (Medicine) to gain consensus on core learning outcomes for primary medical
degrees (Master of Medicine) across Europe (Cumming and Ross 2007, 2008). This
resulted in consensus on twelve broad ‘Level 1’ learning outcomes, each of which could be
divided into more detailed ‘Level 2’ learning outcomes, and also a series of learning
outcomes in medical professionalism.
The results have been widely accepted and influential. For example, ‘Outcomes’ section
of the third (2009) version of Tomorrow’s Doctors from the GMC, draws heavily on the
Tuning (Medicine) outcomes, which are also referenced in that document (GMC 2009).
The aim of the current research was to use Tuning methodology to explore stakeholder
opinions and, where possible, identify consensus on core learning outcomes for the
Bachelor of Medicine degree programmes across Europe. These would systematically link
with the previously identified Tuning (Medicine) outcomes for the primary medical degree,
in order to promote curriculum integration, transparency of graduate competences, and
transferability of teaching and learning materials, strategies, students and staff between
institutions.
7
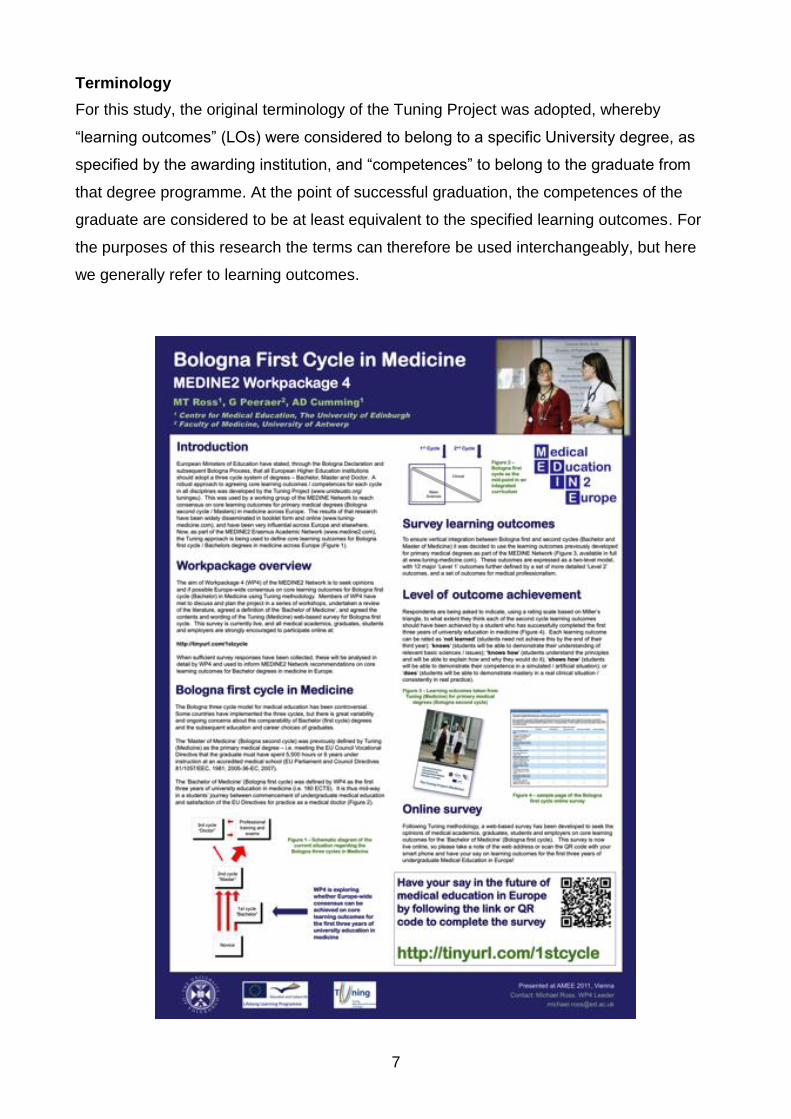
Terminology
For this study, the original terminology of the Tuning Project was adopted, whereby
“learning outcomes” (LOs) were considered to belong to a specific University degree, as
specified by the awarding institution, and “competences” to belong to the graduate from
that degree programme. At the point of successful graduation, the competences of the
graduate are considered to be at least equivalent to the specified learning outcomes. For
the purposes of this research the terms can therefore be used interchangeably, but here
we generally refer to learning outcomes.
8
METHODS
Research process
Members of the MEDINE2 Thematic Network from all across Europe met in a series of
workshops to review the Tuning (Medicine) learning outcomes for primary medical
degrees, and how these related to existing literature on the Bologna First Cycle in
Medicine. They also considered and discussed the ethical and political implications of the
research. On the basis of these discussions, the group formalised a questionnaire and
process for data collection, which was reviewed and approved by the wider MEDINE2
Network before being translated into English, German, French and Spanish. The
questionnaire was made available using an online survey tool (www.surveymonkey.com)
from June 2011 to June 2012. Invitations to participate were disseminated by members of
the MEDINE2 Network, posted on the Network website, distributed by various international
and national medical education organisations and at conferences, and sent to
undergraduate teaching Deans across Europe. Results were compiled and analysed by a
small international working group, before being presented and critiqued by a specially
invited group of experts in a ‘consensus conference’ and then by all members of the wider
MEDINE2 Network.
Questionnaire design
For each of the Level 1 and Level 2 learning outcomes / competences arising from the
Tuning (Medicine) Project (Cumming and Ross 2008), participants were asked to “Please
rate the following learning outcomes / competences on the extent to which you think they
should have been achieved by a student who has successfully completed the first three
years of university education in medicine” on the following Likert scale, which is based on
Miller’s triangle (Miller 1990):
Not Learned
Knows (about it)
Knows How (to do it)
Shows How (in simulation)
Does (in real practice)
9
For each of the learning outcomes / Competences in Medical Professionalism arising from
the Tuning (Medicine) Project, participants were asked to “Please rate the following
learning outcomes / competences relating to medical professionalism on the extent to
which you think they should have been achieved by a student who has successfully
completed the first three years of university education in medicine”:
Not Learned
Knows (aware of issues)
Knows How (understands principles)
Shows How (in artificial scenarios)
Does (consistently in real practice)
Free text responses were sought on any additional LO they thought were important for
students to have achieved at the end of the first three years, respondent demographic
information, and any other comments about the questionnaire, the Bachelor of Medicine,
or the Tuning process.
Data analysis
Demographic data were collated, and qualitative data were analysed thematically.
Quantitative data from all four language versions of the survey were combined into a
single Excel spread-sheet for analysis. All responses for each Level-1, Level-2 and
Medical Professionalism learning outcomes item were charted as bar graphs and the
mean and median values calculated. The Leik measure of ordinal consensus was
calculated for each item and group of items (Leik 1966), and Intra-class Correlation
Coefficients (ICC) were used for sub-groups analysis.
10
RESULTS
Respondent demographics
There were 560 responses to the survey in total, representing all EU countries except
Bulgaria, Cyprus and Luxembourg. Respondents represented medical students,
academics, graduates, employers and patients / members of the public, most of whom
were associated with a university medical school within the EU.
Quantitative data
Seven Level-1 LOs had a median rating of 3 (Knows How), three of 4 (Shows How), and
two of 2 (Knows). Thirty-six Level-2 LOs had a median rating of 3 (Knows How), fourteen
of 4 (Shows How), twelve of 2 (Knows), and seven of 5 (Does). Seventeen LOs for
Medical Professionalism had a median rating of 4 (Shows How), and nine of 3 (Knows
How). None of the LOs had a median rating of 1 (Not Learned). Respondents therefore
considered that all of the learning outcomes/ competences defined by the Tuning
(Medicine) Project for the primary medical degree (Bologna Second Cycle) should be
achieved to some degree by the end of the first three years of study (Bologna First Cycle).
Leik measures of consensus for each of the LOs were calculated as ‘moderate’ (0.41-0.60)
for ninety-six, ‘substantial’ (0.61-0.80) for nine, ‘good’ (>0.80) for one (‘Measure blood
pressure’), and ‘fair’ for one (‘Communicate by telephone’). No LOs had ‘poor’ (<0.20)
consensus. Consensus was generally highest for Level-1 LOs, followed by Level-2 and
then Medical Professionalism LOs.

11
Level 1
Outcomes Responses Mean
Median Leik Measure
of Consensus
Carry out a
consultation with a
patient
3.38
0.490
Assess clinical
presentations, order
investigations, make
differential
diagnoses, and
negotiate a
management plan
2.62
0.563
Provide immediate
care of medical
emergencies,
including First Aid
and resuscitation
3.50
0.514
Prescribe drugs
2.18
0.658
Carry out practical
procedures
3.01
0.490
Communicate
effectively in a
medical context
3.68
0.528
Ability to apply
ethical and legal
principles in medical
practice
3.14
0.492

12
Assess psychological
and social aspects of
a patient's illness
3.23
0.559
Apply the principles,
skills and knowledge
of evidence-based
medicine
3.18
0.555
Use information and
information
techology effectively
in a medical context
3.60
0.492
Apply scientific
principles, method
and knowledge to
medical practice and
research
3.30
0.536
Promote health,
engage with
population health
issues and work
effectively in a
health care system
3.17
0.506

13
Level 2
Outcomes
Responses
Mean
Median Leik Measure
of Consensus
Take a history
4.19
0.617
Carry out physical
examination
4.08
0.640
Make clinical
judgements and
decisions
2.87
0.573
Provide explanation
and advice
3.15
0.545
Provide reassurance
and support
3.26
0.500
Assess the patient's
mental state
2.95
0.509
Recognise and assess
the severity of
clinical presentations
3.04
0.568

14
Order appropriate
investigations and
interpret the results
2.71
0.541
Make differential
diagnoses
2.87
0.538
Negotiate an
appropriate
management plan
with patients and
carers
2.41
0.582
Provide care of the
dying and their
families
2.20
0.619
Manage chronic
illness
2.32
0.619
Recognise and assess
acute medical
emergencies
3.30
0.503
Treat acute medical
emergencies
2.82
0.522

15
Provide basic First
Aid
3.99
0.580
Provide basic life
support and cardio-
pulmonary
resuscitation
according to current
European guidelines
3.81
0.568
Provide advanced
life support
according to current
European guidelines
2.69
0.471
Provide trauma care
according to current
European guidelines
2.53
0.492
Prescribe clearly and
accurately
2.33
0.597
Match appropriate
drugs and other
therapies to the
clinical context
2.40
0.599
Review the
appropriateness of
drug and other
therapies and
evaluate potential
benefits and risks
2.42
0.598
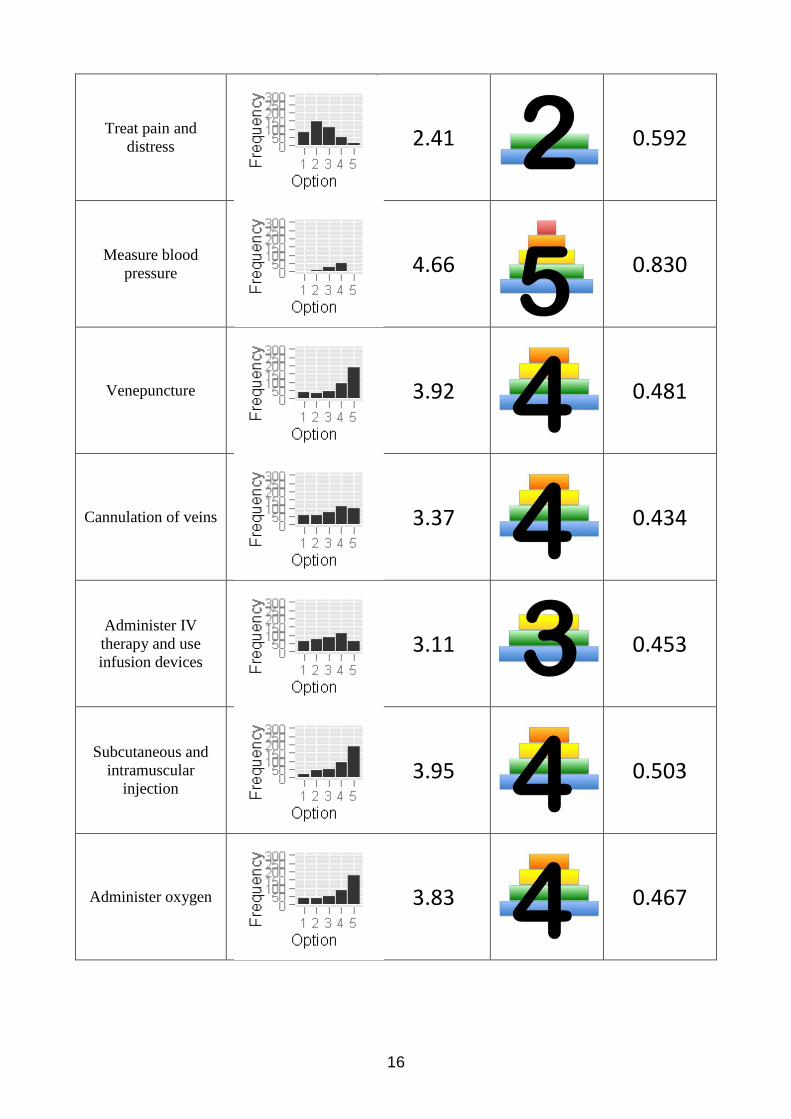
16
Treat pain and
distress
2.41
0.592
Measure blood
pressure
4.66
0.830
Venepuncture
3.92
0.481
Cannulation of veins
3.37
0.434
Administer IV
therapy and use
infusion devices
3.11
0.453
Subcutaneous and
intramuscular
injection
3.95
0.503
Administer oxygen
3.83
0.467

17
Move and handle
patients
3.82
0.454
Suturing
3.23
0.423
Blood transfusion
2.52
0.504
Bladder
catheterisation
2.95
0.420
Urinalysis
3.15
0.435
Electrocardiography
3.55
0.485
Basic respiratory
function tests
3.29
0.495

18
Communicate with
patients
4.30
0.649
Communicate with
colleagues
4.29
0.643
Communicate in
breaking bad news
3.13
0.541
Communicate with
relatives
3.30
0.503
Communicate with
disabled people
3.20
0.440
Communicate in
seeking informed
consent
3.26
0.474
Communicate in
writing (including
medical records)
3.30
0.472
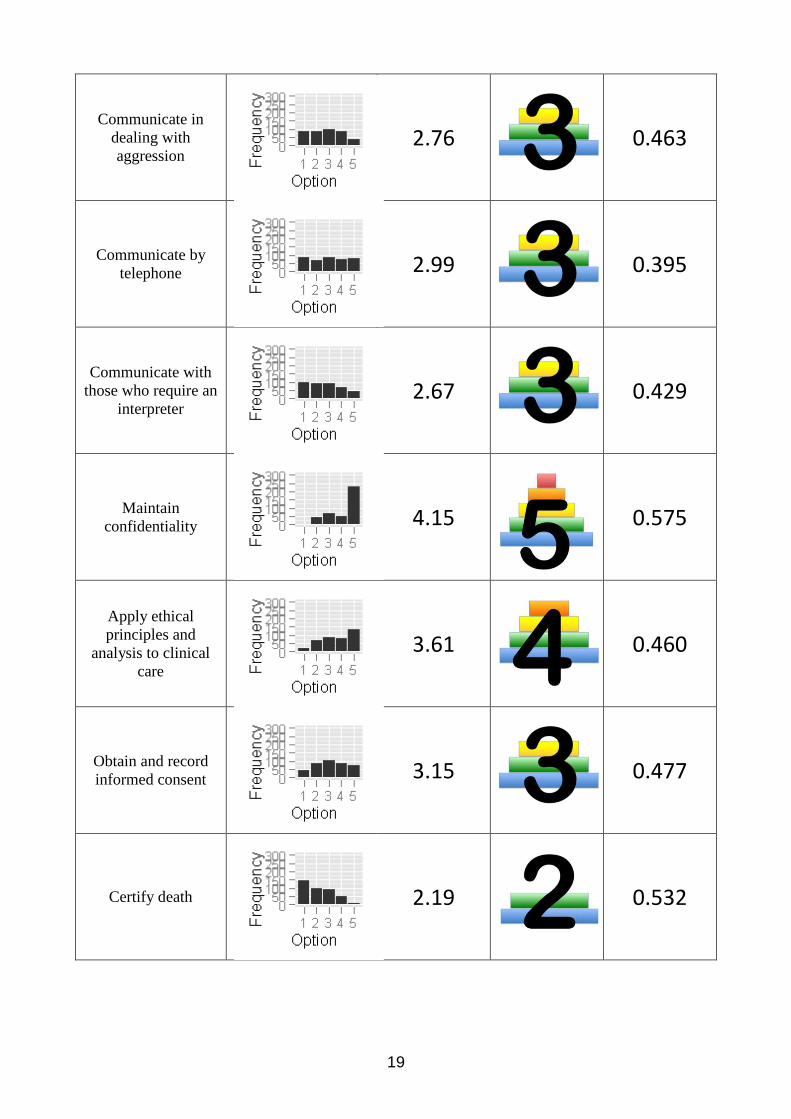
19
Communicate in
dealing with
aggression
2.76
0.463
Communicate by
telephone
2.99
0.395
Communicate with
those who require an
interpreter
2.67
0.429
Maintain
confidentiality
4.15
0.575
Apply ethical
principles and
analysis to clinical
care
3.61
0.460
Obtain and record
informed consent
3.15
0.477
Certify death
2.19
0.532

20
Request autopsy
2.01
0.546
Apply national and
European law to
clinical care
2.24
0.543
Assess psychological
factors in
presentations and
impact of illness
3.17
0.506
Assess social factors
in presentations and
impact of illness
3.20
0.519
Detect stress in
relation to illness
3.14
0.490
Detect alcohol and
substance abuse,
dependency
3.04
0.515
Apply evidence to
practice
3.22
0.526

21
Define and carry out
an appropriate
literature search
3.86
0.500
Critically appraise
published medical
literature
3.46
0.464
Keep accurate and
complete clinical
records
3.29
0.480
Use computers
4.28
0.638
Access information
sources
4.28
0.642
Store and retrieve
information
4.04
0.519
Provide patient care
which minimises the
risk of harm to
patients
3.15
0.469

22
Apply measures to
prevent the spread of
infection
3.60
0.458
Recognise own
health needs and
ensure
own health does not
interfere with
professional
responsibilities
3.45
0.417
Conform with
professional
regulation and
certification to
practise
2.97
0.445
Receive and provide
professional
appraisal
2.82
0.435
Make informed
career choices
2.77
0.445
Engage in health
promotion at
individual and
population levels
3.09
0.467

23
Outcomes in
Medical
Professionalism
Responses Mean
Median Leik Measure
of Consensus
Probity, honesty,
ethical commitment
4.02
0.514
Commitment to
maintaining good
practice, concern for
quality
3.80
0.496
Critical and self-
critical abilities,
reflective practice
3.81
0.503
Empathy
4.08
0.550
Creativity
3.60
0.466
Initiative, will to
succeed
3.81
0.505
Interpersonal skills
4.00
0.540

24
Ability to recognise
limits and ask for
help
3.88
0.477
Capacity to deal with
uncertainty and
adapt to new
situations
3.54
0.466
Ability to lead others
2.98
0.510
Ability to work
autonomously when
necessary
3.34
0.466
Ability to solve
problems
3.54
0.506
Ability to make
decisions
3.41
0.492
Ability to work in a
multidisciplinary
team
3.54
0.459

25
Ability to
communicate with
experts in other
disciplines
3.35
0.469
Capacity for
organisation and
planning (including
time management)
3.33
0.469
Capacity for analysis
and synthesis
3.51
0.486
Capacity to learn
(including lifelong
self-directed
learning)
3.92
0.503
Capacity for
applying knowledge
in practice
3.68
0.528
Ability to teach
others
3.09
0.463
Research skills
3.29
0.500

26
Appreciation of
diversity and
multiculturality
3.70
0.439
Understanding of
cultures and customs
of other countries
3.45
0.430
Ability to work in an
international context
3.14
0.443
Knowledge of a
second language
3.86
0.431
General knowledge
outside medicine
3.68
0.422

27
Subgroup analysis
Overall, no large subgroups were found to have an undue impact on the rankings of the
whole sample (n=560), with high or very high Intra-Class Correlation. Mean responses
from large subgroups in Portugal (n=104) and Belgium (n=68) differed by a full Likert point
on only six items, all of which were Level-2 practical procedures. Mean ratings by
Academics (n=144) and Students (n=193) were not separated by a point on any item.
Qualitative data
A number of themes emerged from analysis of the free text responses. Several
respondents voiced concerns about defining a Bachelor of Medicine, suggesting that the
3-Cycle system may not work in certain countries, that defining a Bachelor may lead to a
loss of integration in the undergraduate medical curriculum, and that Bachelor graduates
may work as “Semi-literate doctors” and put patients at risk. One respondent wrote that it
would “Need a clear protocol for what first cycle graduates are and are not allowed to do,
with safety checks and monitoring”. Others highlighted that the Bachelor of Medicine
should itself be a useful qualification, more than just half way to a medical degree, and that
we should think about the employability of graduates, who may require more skills in
lifelong learning, creativity, managing and critically evaluating information if they do not go
on to do the Masters of Medicine. Some also emphasised the need for early patient
contact and practical experience, commenting that students “Need patient contact from
start of Year 1”, and “Medicine is very practical so need to gain practical experience”. A
few raised philosophical concerns about defining core learning outcomes, for example
writing, “Education should stimulate diversity of opinion and competences rather than
trying to create a uniform group of doctors”, and “LOs may mean different things to
different people – particularly when translated”. A number of respondents suggested
additional or more detailed learning outcomes, which can be explored in subsequent
research.
28
COMMENT
Key findings of this research
Mean ratings for each of the learning outcomes were greater than 1 (Not Learned), and
therefore collectively respondents felt that all of the LO for the Masters of Medicine
(primary medical degree) should be achieved to some extent in the Bachelor cycle (first
three years). Most individual respondents attributed some importance to all of the LOs for
the Bachelor phase, including many clinical LOs. As reiterated in the free text comments,
this would therefore require the Bachelor of Medicine to include early clinical experience,
and supports the idea of a vertically integrated curriculum, rather than the more traditional
curriculum design with a preclinical/clinical divide. The seven LOs with a mean rating of 5
(which survey respondents considered students should be able to do in real practice after
3 years at medical school) were considered by all participants in the final MEDINE2
meeting to have face validity. They were also considered to be consistent with
competences which medical schools who do not award the Bachelor of Medicine degree
would expect a student to demonstrate on successful completion of their third year. Being
able to communicate with colleagues and patients, maintain confidentiality, use computers
and information sources, and undertake a simple clinical procedure such as measuring
blood pressure, together with less well-developed competences in all other areas, define
accurately what a Bachelor of Medicine graduate can, and importantly cannot, do. Whilst
potentially enhancing employability, it is also very clear that such graduates would not be
able to practise as medical doctors without further training.
29
Conclusions and implications
The most powerful impression given by the results is that there is promotion of a fully
integrated curriculum, with the same learning outcomes being sequentially achieved during
both the Bachelor and Master phases of medical education. The results support an
integrated approach to curriculum design and early clinical experience and skills
acquisition, rather than a split of undergraduate medical curricula as had been feared by
some. The LOs match well with the Dublin Descriptors for Bachelor degrees and thus will
be easily readable and comparable with degrees in other disciplines, and they appear to
have face validity.
The results emphasise that Bachelor of Medicine graduates would not be ready to practise
as ‘cut-price doctors’. This may be useful to regulatory bodies and licensing authorities in
considering roles and boundaries. They do, however, present a helpful, clear indication of
the sort of competences that could be expected of a student after the first three years of
undergraduate medical education in Europe. For those students who decide against
completion of their medical studies or are unable to continue, who can be considerable in
number,(Arulampalam et al. 2004) this could also be very helpful in terms of their
employability and mobility.
The results do not suggest that there should be rigid uniformity across medical school
curricula, but indicate that a degree of harmonisation, based on consensus, is achievable.
Differences in detailed learning outcomes will continue to exist between programmes, but
for the first time this research offers an ‘image’ of a European Bachelor of Medicine. Since
Bachelor of Medicine degrees are currently being awarded after 3 years of study in many
countries and institutions in Europe, without prior discussion or agreement at European
level as to what these graduates have learned or are able to do, we hope that these
findings will stimulate further consideration and collaboration in this area of practice.
30
REFERENCES
AMEE, EMSA, IFMSA (2010) The Bologna Process and its implications for medical education. The Association for Medical Education in Europe, European Medical Students' Association, International Federation of Medical Students' Associations. Medical Teacher 32: 302-304. AMEE, WFME, ASMSE, WHO-Euro (2005) Statement on the Bologna process and medical education. Prepared by the Asssociation for Medical Education in Europe, and the World Federation for Medical Education, in association with the Association of Medical Schools in Europe, and the World Health Organisation, Europe. Copenhagen, Denmark: World Federation for Medical Education. Arulampalam W, Naylor RA, Smith JP (2004) A hazard model of the probability of medical school drop-out in the United Kingdom. Journal of the Royal Statistical Society: Series A (Statistics in Society) 167(1): 157-178. Christensen L (2004) The Bologna Process and medical education. Medical Teacher 26(7): 625-629. Cumming AD (2010) The Bologna process, medical education and integrated learning. Medical Teacher 32: 316-318. Cumming AD, Ross MT (2007) The Tuning Project for medicine – learning outcomes for undergraduate medical education in Europe. Medical Teacher 29(7): 636-641. Cumming AD, Ross MT (2008) The Tuning Project (medicine) – learning outcomes / competences for undergraduate medical education in Europe. Edinburgh: The University of Edinburgh. Available online: http://www.tuning-medicine.com. Accessed 25th January 2013. Davies H (2010) A chance too good to miss. Medical Teacher 32: 284-287. GMC (2009) Tomorrow's Doctors: outcomes and standards for undergraduate medical education. London: General Medical Council. GMC (2009) Tomorrow’s Doctors. London, General Medical Council. Online: http://www.gmc-uk.org/education/undergraduate/tomorrows_doctors_2009.asp Joint Quality Initiative (2004) Shared 'Dublin' descriptors for Short Cycle, First Cycle, Second Cycle and Third Cycle awards. Online: http://www.jointquality.nl/content/descriptors/CompletesetDublinDescriptors.doc. Leik RK (1966) A measure of ordinal consensus. The Pacific Sociological Review 9(2): 85-90. Miller GE (1990) The assessment of clinical skills / competence / performance. Academic Medicine 65(9 Supplement): S63-67. Patrício M, Harden RM (2010) The Bologna Process - a global vision for the future of medical education. Medical Teacher 32: 305-315.

31
Patrício M, den Engelsen C, Tseng D, ten Cate O (2008) Implementation of the Bologna two-cycle system in medical education: where do we stand in 2007? - Results of an AMEE-MEDINE survey. Medical Teacher 30: 597-605. Patrício M, de Burbure C, Costa MJ, Schirlo C, ten Cate O (2012) Bologna in medicine anno 2012: experiences of European medical schools that implemented a Bologna two-cycle curriculum - an AMEE-MEDINE2 survey. Medical Teacher 34(10): 821-832. Rigby E (2007) Taking forward aims of the Bologna Declaration: European core curriculum - the students' perspective. Medical Teacher 29: 83-84. Tuning Project website (Accessed April 2013): http://www.unideusto.org/tuning/
Van den Broek S, Muller B, Dekker N, Bootsma A, ten Cate O (2010) Effect of the new Bologna bachelor degree on career considerations of medical students in one medical school. Medical Teacher 32: 997-1001.

32
Contributors to Workpackage 4
Michael Ross Griet Peeraer Nebojša Nikolić
Ahmet Murt Juta Kroiča Melih Elcin
Allan Cumming Carol Telford David Hope
Birgitta Wallstedt Bernard Maillet Paola Arslan
Jorgen Nordenstrom Orla Hanratty Karen Pierer
Malgorzata Rejnik Matthius Dürst Lidia Przepiora-Dziewulska
Georges Casimir Miguel Angel Vizcaya Felicidad Rodríguez Sánchez
Juan Bosco Lopez Saez Suzana Manxhuka-Kerliu Elisabeth Hansson
Evelina Nystrom Nikolay Aryayev Kristjan Erlendsson
Michael Begg Helen Cameron Madalena Patrício
Ronald Harden

33
Acknowledgements
The study was conducted under the auspices of the MEDINE2 Erasmus Academic
Network for Medical Education in Europe, 2009-2013, coordinated by The University of
Edinburgh and supported by funding from the Life Long Learning Programme of the
European Commission: 155731-LLP-1-2009-1-UK-ERASMUS-ENWA. The authors would
like to thank all members of the MEDINE2 Thematic Network for their support, opinions
and collaboration, and the Project Officer, Carol Telford, for her invaluable support.
Particular thanks to those MEDINE2 members who participated actively in the work of
Workpackage 4. Special thanks to Ronald Harden, Helen Cameron and Madalena
Patrício for their invaluable contributions to the final consensus meeting, and to the many
survey respondents who contributed their valuable time and expertise.