Embed Size (px)
Citation preview
A O R N J O U R N A L APRIL 1984. VOL 39, NO 5
The Tunable Dye Laser PHOTORADLATION OF MALIGNANCIES
Pat Niessner Palmer, RN
W hat's it like to be involved in an in- vestigation team in cancer treat- ment? I asked the interdisciplinary
laser team at Grant Hospital of Columbus, Ohio, that question. They work with James S McCaughan, Jr, MD, and Robert Bruce, Jr, MD, principal investigators, in using 'an argon laser-pumped tunable dye laser in conjunction with hematoporphyrin (HpD) derivative to photoradiate certain malignant tumors.
Beth Olson, RN, MS, oncology clinical nurse specialist, said her staff was enthusiastic about their role in the experimental treatment. Nurses usually react negatively to investigational treat- ments for cancer, she said, but because this treatment does not have the toxic effects so common in anticancer modalities they are less disturbed by the investigation. The patients are well informed so they can decide if they want the treatment.
Carolyn J Mackety, RN, BS, director of oper- ating room services at Grant Hospital, has de- veloped a position for a clinical laser nurse. As a clinical laser nurse, Peggy J Nowell, RN, will teach staff and coordinate perioperative patient care. Laser technicians Bill Janssen and Deborah McMahon are responsible for the instrumenta- tion and the laser equipment used for each patient,
The idea that photoradiation might be therapeutic treatment for malignancies origi- nated in the 1920s when scientists observed a red-orange fluorescence from some types of tumor cells when exposed to near ultraviolet light. The light was caused by endogenous por- phyrins contained in hemoglobin. Experiments
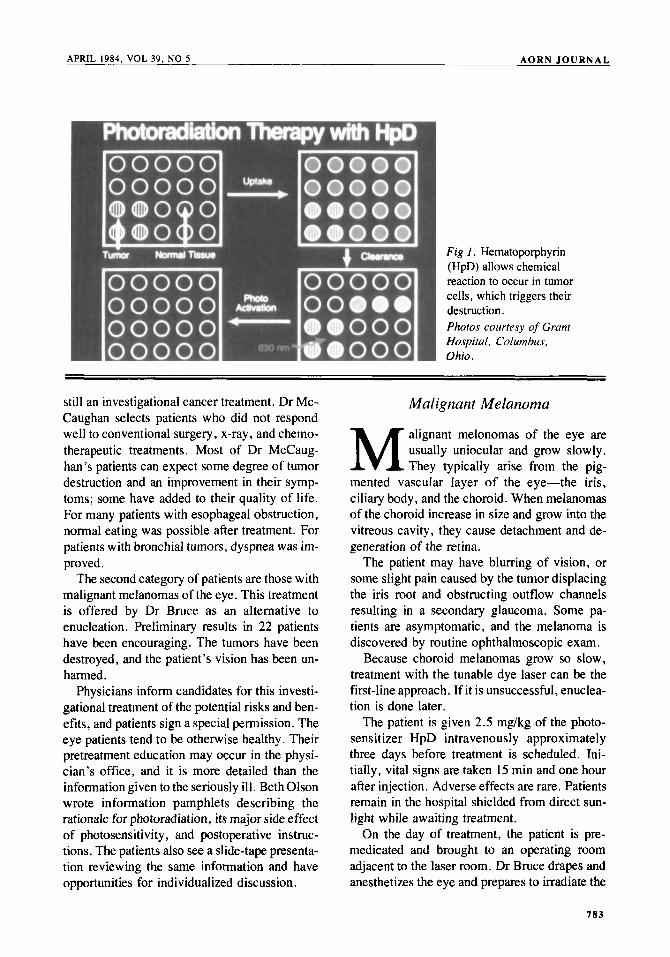
showed that an artificial porphyrin could be made from hemoglobin, and it could make cells extremely sensitive to light. When the HpD de- rivative was injected into animals, it rapidly cleared out normal cells and remained longer in tumor and reticular endothelial cells. When the tumors, which contained HpD, were exposed to near ultraviolet light, the HpD absorbed the light causing a photochemical reaction. The reaction produced singlet oxygen, which triggers tumor cell destruction.' Because HpD cleared from normal cells, the reaction was absent in non- malignant surrounding tissues (Fig 1 ) .
In 1982, T J Dougherty, PhD, and his asso-. ciates at Roswell Park Memorial Institute in Buffalo, NY, began experimenting with hem-. atoporphyrin derivative and different light sources and wavelengths. They treated tumors in laboratory animals and tried to determine the most effective combination of HPD dye and light to produce the desired chemical reaction in tumor cells. Neither agent will work by itself.
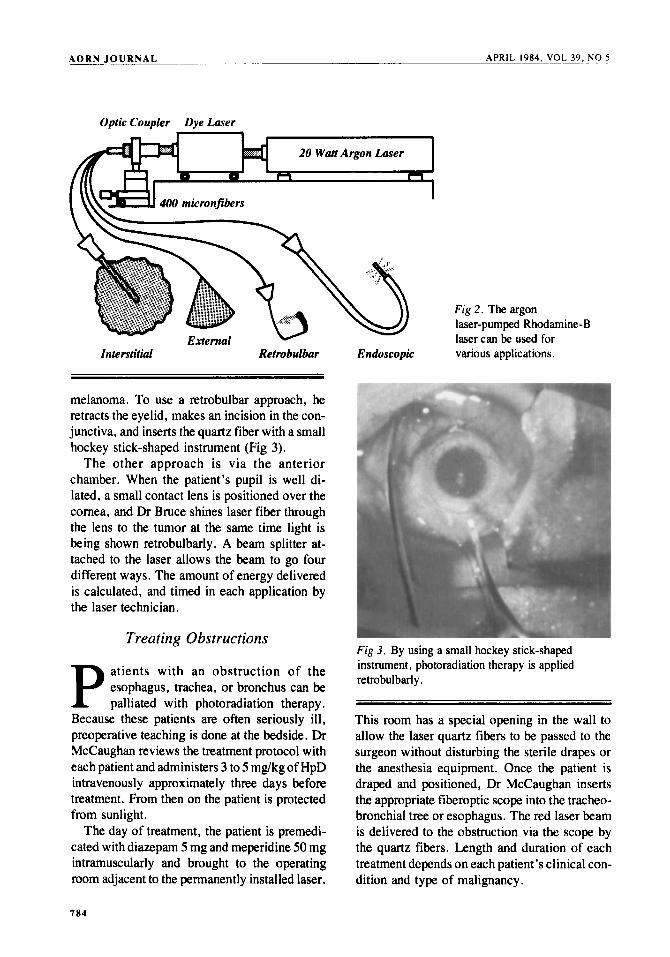
Dougherty 's group is credited with determin- ing that the 631 nonometer (nm) light from an argon laser-pumped Rhodamine-B laser pene- trates tissue best and produces the therapeutic singlet oxygen reaction. By 1978, they reported effective treatment of human malignancies. The HpD phototherapy is still under FDA investiga- tion and under Dougherty's direction. Figure 2 shows the four ways HpD can be administered: interstitially, externally, retrobulbarly, and en- doscopically .
At Grant Hospital, two categories of patients are treated with HpD phototherapy because it is
782
AORN JOURNAL APRIL 1984, VOL 39, NO 5
Fig 1. Hematoporphyrin (HpD) allows chemical reaction to occur in tumor cells, which triggers their destruction. Photos courresy of Grunt Hospitul, Columbus, Ohio.
still an investigational cancer treatment. Dr Mc- Caughan selects patients who did not respond well to conventional surgery, x-ray, and chemo- therapeutic treatments. Most of Dr McCaug- han’s patients can expect some degree of tumor destruction and an improvement in their symp- toms; some have added to their quality of life. For many patients with esophageal obstruction, normal eating was possible after treatment. For patients with bronchial tumors, dyspnea was im- proved.
The second category of patients are those with malignant melanomas of the eye. This treatment is offered by Dr Bruce as an alternative to enucleation. Preliminary results in 22 patients have been encouraging. The tumors have been destroyed, and the patient’s vision has been un- harmed.
Physicians inform candidates for this investi- gational treatment of the potential risks and ben- efits, and patients sign a special permission. The eye patients tend to be otherwise healthy. Their pretreatment education may occur in the physi- cian’s office, and it is more detailed than the information given to the seriously ill. Beth Olson wrote information pamphlets describing the rationale for photoradiation, its major side effect of photosensitivity, and postoperative instruc- tions. The patients also see a slide-tape presenta- tion reviewing the same information and have opportunities for individualized discussion.
Malignant Melanoma
M alignant melonomas of the eye are usually uniocular and grow slowly. They typically arise from the pig-
mented vascular layer of the eye-the iris, ciliary body, and the choroid. When melanomas of the choroid increase in size and grow into the vitreous cavity, they cause detachment and de- generation of the retina.
The patient may have blurring of vision, or some slight pain caused by the tumor displacing the iris root and obstructing outflow channels resulting in a secondary glaucoma. Some pa- tients are asymptomatic, and the melanoma is discovered by routine ophthalmoscopic exam.
Because choroid melanomas grow so slow, treatment with the tunable dye laser can be the first-line approach. If it is unsuccessful, enuclea- tion is done later.
The patient is given 2.5 mg/kg of the photo- sensitizer HpD intravenously approximately three days before treatment is scheduled. Ini- tially, vital signs are taken 15 min and one hour after injection. Adverse effects are rare. Patients remain in the hospital shielded from direct sun- light while awaiting treatment.
On the day of treatment, the patient is pre- medicated and brought to an operating room adjacent to the laser room. Dr Bruce drapes and anesthetizes the eye and prepares to irradiate the
783
A O R N J O U R N A L APRIL 1984, VOL 39, NO 5
Optic Coupler Dye Laser
Fig 2. The argon laser-pumped Rhodamine-B laser can be used for
Interstitial Retrobulhr Endoscopic various applications.
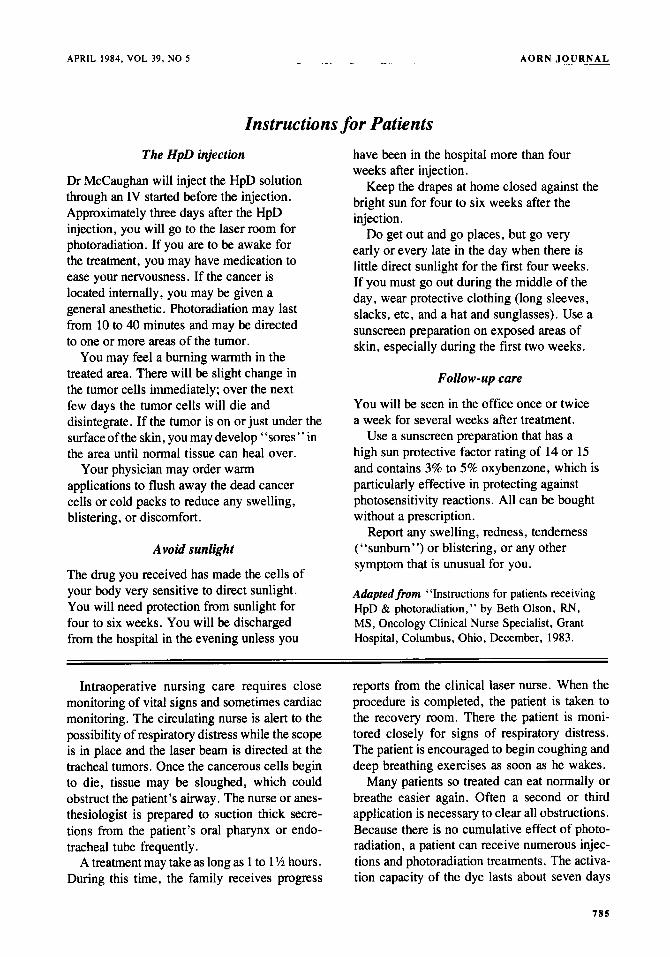
melanoma. To use a retrobulbar approach, he retracts the eyelid, makes an incision in the con- junctiva, and inserts the quartz fiber with a small hockey stick-shaped instrument (Fig 3).
The other approach is via the anterior chamber. When the patient’s pupil is well di- lated, a small contact lens is positioned over the cornea, and Dr Bruce shines laser fiber through the lens to the tumor at the same time light is being shown retrobulbarly. A beam splitter at- tached to the laser allows the beam to go four different ways. The amount of energy delivered is calculated, and timed in each application by the laser technician.
Treating 0 bstructions
atients with an obstruction of the esophagus, trachea, or bronchus can be P palliated with photoradiation therapy.
Because these patients are often seriously ill, preoperative teaching is done at the bedside. Dr McCaughan reviews the treatment protocol with each patient and administers 3 to 5 mg/kg of HpD intravenously approximately three days before treatment. From then on the patient is protected from sunlight.
The day of treatment, the patient is premedi- cated with diazepam 5 mg and meperidine 50 mg intramuscularly and brought to the operating room adjacent to the permanently installed laser.
Fig 3. By using a small hockey stick-shaped instrument, photoradiation therapy is applied retrobulbarly .
This room has a special opening in the wall to allow the laser quartz fibers to be passed to the surgeon without disturbing the sterile drapes or the anesthesia equipment. Once the patient is draped and positioned, Dr McCaughan inserts the appropriate fiberoptic scope into the tracheo- bronchial tree or esophagus. The red laser beam is delivered to the obstruction via the scope by the quartz fibers. Length and duration of each treatment depends on each patient’s clinical con- dition and type of malignancy.
184
APRIL 1984, VOL 39, NO 5 A O R N JOURNAL
Instructions for Patients The HpD injection
Dr McCaughan will inject the HpD solution through an IV started before the injection. Approximately three days after the HpD injection, you will go to the laser room for photoradiation. If you are to be awake for the treatment, you may have medication to ease your nervousness. If the cancer is located internally, you may be given a general anesthetic. Photoradiation may last from 10 to 40 minutes and may be directed to one or more areas of the tumor.
You may feel a burning warmth in the treated area. There will be slight change in the tumor cells immediately; over the next few days the tumor cells will die and disintegrate. If the tumor is on or just under the surface of the skin, you may develop “sores” in the area until normal tissue can heal over.
applications to flush away the dead cancer cells or cold packs to reduce any swelling, blistering, or discomfort.
Your physician may order warm
Avoid sunlight
The drug you received has made the cells of your body very sensitive to direct sunlight. You will need protection from sunlight for four to six weeks. You will be discharged from the hospital in the evening unless you
have been in the hospital more than four weeks after injection.
bright sun for four to six weeks after the injection.
Do get out and go places, but go very early or every late in the day when there is little direct sunlight for the first four weeks. If you must go out during the middle of the day, wear protective clothing (long sleeves, slacks, etc, and a hat and sunglasses). Use a sunscreen preparation on exposed areas of skin, especially during the first two weeks.
Keep the drapes at home closed against the
Follow-up care
You will be seen in the office once or twice a week for several weeks after treatment.
Use a sunscreen preparation that has a high sun protective factor rating of 14 or 15 and contains 3% to 5% oxybenzone, which is particularly effective in protecting against photosensitivity reactions. All can be bought without a prescription.
Report any swelling, redness, tenderness (“sunburn”) or blistering, or any other symptom that is unusual for you.
Adapted from “Instructions for patients receiving HpD & photoradiation,” by Beth Olson, RN, MS, Oncology Clinical Nurse Specialist, Grant Hospital, Columbus, Ohio, December, 1983.
Intraoperative nursing care requires close monitoring of vital signs and sometimes cardiac monitoring. The circulating nurse is alert to the possibility of respiratory distress while the scope is in place and the laser beam is directed at the tracheal tumors. Once the cancerous cells begin to die, tissue may be sloughed, which could obstruct the patient’s airway. The nurse or anes- thesiologist is prepared to suction thick secre- tions from the patient’s oral pharynx or endo- tracheal tube frequently.
A treatment may take as long as 1 to 1 ‘/z hours. During this time, the family receives progress
reports from the clinical laser nurse. When the procedure is completed, the patient is taken to the recovery room. There the patient is moni- tored closely for signs of respiratory distress. The patient is encouraged to begin coughing and deep breathing exercises as soon as he wakes.
Many patients so treated can eat normally or breathe easier again. Often a second or third application is necessary to clear all obstructions. Because there is no cumulative effect of photo- radiation, a patient can receive numerous injec- tions and photoradiation treatments. The activa- tion capacity of the dye lasts about seven days
785
A O R N J O U R N A L - . ~ _ _ _ ~ _ _ _ _ _ APRIL 1984, VOL 3 9 . 0 2
after each injection. Injections can be repeated in to use this technique for diagnosis. [I Note
1 . James S McCaughan, Jr, “Photoradiation treatment of cancer following administration of HpD,” Lusar Focus (May 1983).
Pat Niessner Palmer, RN, M S , is the wrse editor o j the AORN Journal.
six to eight weeks if necessary. Although this new form of cancer treatment is
still under investigation, physicians hope it can eventually be used to treat bladder carcinomas, nasopharyngeal tumors, and to debulk abdomi- nal and brain tumors. Because the HpD dye makes tumor cells fluorescent, it may be possible
-
Film Review: The Sterile Environment Maintaining A Sterile Environment is a flexible learning tool combining a film strip (or slidehape), a student activities guide, and an instructor’s guide. It can be used as a self-learning program for individual student instruction, or as an introduction to group activities in a classroom presentation. The audience should know general aseptic terms (ie, antiseptic agent, microorganism, contamination) because the film presents basic aseptic techniques for handling sterile items during routine patient care.
a sterile environment by using correct methods to open a sterile tray, open and add separately packaged items to the tray, and pour liquids into a sterile container. The program also discusses methods of sterilization and provides a guide to determine the length of time required for sterilization of an article at various altitudes using an autoclave.
This program is available from Medical Electronic Educational Services, Inc (MEES), PO Box 50700, Tucson, Ariz 85703. The film strip sells for $80, and the slidehape format for $1 10. A free 21-day preview of the film strip is available, but does not include the student activities guide.
The program demonstrates how to maintain
PATRICIA BALL, RN, CNOR AUDIOVISUAL COMMITTEE
Self-medic at ion Would Ease Pain A physician at Vanderbilt University Medical Center in Nashville, Tenn, has developed a plan he hopes can ameliorate poor pain management. Hematologist John M Flexner, American Cancer Society professor of clinical oncology, advocates patient self-medication as the keystone to pain management.
He believes suffering must be divided into two categories-acute pain and chronic pain. “Acute pain has biological value. It can save your life,” he notes. “Chronic pain, on the other hand, has no biological value, no use whatsoever. ”
For chronic pain sufferers, especially the terminally ill, Dr Flexner advocates around-the-clock self-medication, to break the torturous cycle of pain and relief. He normally prescribes a morphine-sulfate solution, more powerful and effective than the “Brompton’s Cocktail,” whose primary ingredient was cocaine. The solution is kept by patients’ beds so they can decide when and how much to take.
of addiction with this method, because chronic pain sufferers require less and less narcotic rather than more. Also, these patients do not develop tolerances or become addicted because they take the drug only to relieve pain, not to get high.
Dr Flexnor asserts that there is no danger
786