Embed Size (px)
Citation preview

International Orthopaedics (SICOT) (1991) 15:265-271 International Orthopaedics
© Springer Verlag 1991
Current concepts
The treatment of spinal kyphosis*
R. Winter
Minnesota Spine Centre, Minneapolis and St Paul, 606, 24th Ave. South, Minneapolis, MN 55454, USA
Summary. The modern management of kyphosis depends on the diagnosb, but there are common factors on which rational treatment can be based. An understanding of the biomechanics is very im- portant, especially in planning operations on the spine. The greatest single advance has been the anterior approach. Scheuermann's disease in chil- dren is best treated by bracing, but most other de- formities need anterior and posterior fusion. Mod- ern instrumentation benefits both the patient and the surgeon.
R/~sum& Le traitement moderne des cyphoses varie beaucoup selon le diagnostic. II existe cependant des facteurs communs qui permettent un traitement rationnel. La comprbhension de la biombcanique est cruciale, tout particuli&ement en ce qui concerne les indications chirurgicales. Le principal progr& dans ce domaine a btb apportO par l'abord du rachis par voie ant&ieure. La maladie de Scheuermann est correctement traitbe par corset de Milwaukee, chez l'adolescent, mais la plupart des cyphoses sbv&es n~cessitent une fusion vertbbrale d la lois ant&ieure et post&ieure. Les chirurgiens et les malades ont bgalement bbnbficib de l'ambliora- tion de l'instrumentation.
Introduction
There are many causes which can produce a spi- nal kyphotic deformity, ranging from benign pos-
* Current trends lecture at SICOT meeting in Montreal 10 September 1990
tural kyphosis to the severe deformities produced by congenital and tuberculous disease. Although there are general principles of treatment, the or- thopaedic surgeon should know the variations of natural history associated with different diag- noses. It is also important to understand when ei- ther bracing or operation is needed.
Classification and aetiology
The Scoliosis Research Society has established a systematic classification for spinal deformities [1] with a classification for kyphosis as follows:
(1) Postural (7) Post-irradiation (2) Scheuermann's (8) Metabolic
disease (9) Dwarfing disorders (3) Congenital (10) Collagen disease (4) Neuromuscular (1 1) Yumour (5) Traumatic (12) Infection (6) Post-traumatic (13) Neurofibromatosis
The biomechanics of kyphosis
Kyphosis occurs in a single plane so its biomech- anics are easier to understand than those of scoli- osis. In the standing orsit t ing posture, the spine is subject to the force of gravity. The amount of stress on any one mobile vertebral segment is re- lated to the weight of the individual and the level of the spine; for example, the 5th thoracic verte- bra carries less load than the 5th lumbar.
Other factors have to be added to this simple concept, namely motion stresses, muscular forces, and the relative position of any one vertebra to the axis of the centre of gravity of the body. The 8th thoracic vertebra lies most posterior to this central sagittal axis; its position is precarious as the extensor muscles are close to it and there is a

266 R. Winter: The treatment of spinal kyphosis
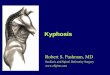
Fig. l. A 13 year old boy who had Scheuermann's disease with a 56 ° kyphosis. There is marked wedging of the apical verte- bra, disc space narrowing and irregularity of the end plates
very short moment arm. In contrast, the flexor muscles lie far in front of the 8th thoracic vertebra so there is a strong moment arm of action. It is thus not surprising that the most commonly in- volved vertebra in Scheuermann's disease is the 8th thoracic, or that a laminectomy for a spinal tumour in this area in a growing child can pro- duce a devastating deformity.
In the thoracic spine, the factors increasing kyphosis are gravity, muscle imbalance, loss of bony integrity due to tumour, burst fracture, in- fection or osteoporosis, and loss of ligamentous stability due to laminectomy or trauma. Factors which counteract this natural tendency are use of the extensor muscles, the supraspinous and inter- spinous ligaments, the capsule of the facet joints, and the ligamentum flavum. In the thoracic spine the supraspinous and interspinous ligaments are very small, there being really no interspinous liga- ments [2].
The capsular ligaments are important and this has been shown in studies of children who had a laminectomy for spinal cord tumours. The in- cidence and severity of the postoperative kyphosis was much higher in those who had facet resection, especially when bilateral, compared with those in whom only the ligamentum flavum was removed.
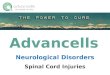
Fig. 2.a A 14 year old girl with an 81 ° progressive kyphosis due to Scheuermann's disease. Her deformity was significant, but corrected to 35 ° on a hyperextension supine radiograph. A considerable amount of growth remained, so she was fitted immedi- ately with a brace, b This radiograph in her Milwaukee brace shows correction to 35 °. e This is the outcome at the age of 16 years and 9 months when she had been out of her brace for 6 months and had a 40 ° deformity

R. Winter : The t r ea tmen t o f spinal kyphos i s 267
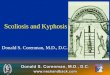
Fig. 3 . a A girl aged 16 years and 3 m o n t h s who had a 70 ° kyphos i s s econda ry to S c h e u e r m a n n ' s disease. T rea t men t with a Mi lwaukee brace was a t t empted , bu t she was a l ready ma tu re a n d we did not achieve p e r m a n e n t corect ion, b At the age o f 34 years, she still h ad a 70 ° de formi ty an d increas ing ly severe pa in ; she asked for surgical t rea tment , c She u n d e r w e n t , u n d e r one anaes- thetic, an anter ior d i scec tomy f rom T4 to T11, a l i gamen tous release and fus ion ; then a poste- rior fus ion was carr ied out with Co t r e l -Dubousse t i n s t rumen ta t ion . Correc t ion was to 44 °. No cast or brace was used after the opera t ion , d One year later her kyphos i s was solidly fused at 48 °, She had no pa in and was h a p p y
Resection of the ligamentum flavum alone has a profound effect. Adults who have had Luque in- strumentation for Scheuermann's disease have shown a marked tendency to develop a kyphosis at the ends of the system, this being the place
where the ligament is resected to allow the pas- sage of the last set of Luque wires.
An understanding of the biomechanics of ky- phosis allows an appreciation of the mechanics of its treatment. Since the apical vertebra in a typical

268 R. Winter: The treatment of spinal kyphosis
case of Scheuermann's disease is the 8th thoracic, we can understand why an underarm orthosis has such a minimal effect and why the Milwaukee brace (CTLSO) has had such a great success [3].
Loss of the anterior column can be produced by tuberculosis, congenital malformations, tu- mours and severe burst fractures, and results in collapse of the spine. Successful restoration of spinal integrity can only be achieved by recon- struction of the anterior bony column by anterior surgery.
Scheuermann's disease
This condition is very common and occurs all over the world. It can present in different ways, one of which is adolescent kyphosis that may or may not be painful. If the deformity is significant, and particularly if it is progressive, orthotic treat- ment is appropriate.
The Milwaukee brace is the treatment of choice for thoracic Scheuermann's disease. For 10% of the patients with disease at the thoracol- umbar junction a TLSO is adequate. The brace should be worn till growth stops, and then the child is slowly weaned from it. Excellent results can expected provided the diagnosis has been made promptly, the brace fits well and is worn faithfully, and treatment is continued for an ade- quate length of time. The definitive paper on the subject is by Sachs et al. [4]; their results were ex- cellent, except where a rigid structural deformity was present before treatment was started.
Since flexible Scheuermann's disease in grow- ing adolescents responds well to bracing, surgery is not needed in this group of patients, but is indi- cated in late adolescents and young adults who have both pain and a significant deformity. An anterior multilevel ligament release is required with discectomy and interbody fusion with rib chip grafts. A posterior fusion, of adequate length and with instrumentation, is carried out either on the same day or a week later [5]. We previously used heavy Harrington compression rods, but we now believe that Cotrel-Dubousset rods are better (Figs. 1, 2 and 3).
Congenital kyphosis
Paraplegia can occur if congenital kyphosis is not treated. Bracing is useless and should never be used. Operation is the treatment of choice.
If the curve is less than 60 ° and the child is under 3 years old, posterior fusion only can be excellent treatment. The fusion must be explored and augmented at 6 months after the original
fusion, and an external support used for one year [6].
If the diagnosis is made later, then both ante- rior and posterior fusion must be done. Ante- riorly, the short ligaments, the discs and all the cartilage remnants must be resected. The spine is then distracted anteriorly and a rigid strut graft of autogenous fibula inserted; the entire anterior angle must be grafted. No internal fixation is used. Posteriorly, a fusion of adequate length is carried out. Rigid external support in a full Risser cast is used until the fusion is completely solid which may take from 12 to 18 months.
In adolescents and adults, posterior in- strumentation can be used with bilateral com- pression rods for a pure kyphosis, but for a kyphoscoliosis, a convex compression rod is in- serted first and a concave distraction rod second.
Halo or halo-femoral traction should be avoided as the cord may be tethered, and traction pulls it against the gibbus causing paraplegia.
A patient with a paraparesis will usually need anterior cord decompression, anterior fusion and the posterior fusion. Laminectomy is contraindi- cated [8] (Fig. 4).
Tuberculous kyphosis
Tuberculosis is now rare in well developed coun- tries, but is still prevalent throughout the world. With the rapid movement of people between countries, surgeons in developed countries c a n expect to see patients with Pott's disease.
Early active disease affecting only one or two segments can be treated by antibiotics, and sur- gery is not necessary; more advanced disease will need operation. The best plan then is to start anti- biotics and ensure good nutrition with bed rest. Then radical anterior debridement of all necrotic and infected material is carried out with immedi- ate anterior autogenous bone grafting. Later pos- terior spinal fusion is undertaken and an hyperex- tension cast worn until the fusion is solid [11].
This programme will eliminate the infection in most cases and will virtually guarantee against a late kyphosis. Failure to take each logical step will often result in disaster.
Post-laminectomy kyphosis
Neurosurgeons often have to perform a laminec- tomy to treat or remove a tumour in the spinal cord or canal; in growing children this will nearly always result in a progressive kyphosis. The long- er the laminectomy, and especially if the facets have to be removed, the worse the deformity [12].

R. Winter: The treatment of spinal kyphosis 269
Fig. 4.a This girl was first seen in 1967, aged 13 years, when she had a rigid congenital kyphosis of 92 °. There was no neurological abnormality, b An anterior trans- thoracic retroperitoneal section of the spine was done with anterior ligament release, discectomy and the in- sertion of a short rib graft (arrows) and autogenous bone chips. Two weeks later, posterior instrumentation with Harrington compression rods was done. c A stand- ing lateral radiograph at the age of 15 years show solid fusion with correction to 60 °. d The most recent follow up was when she was 33 years old, 20 years after the operation. Her correction had been maintained and she has had no difficulties of any kind
Fig. 5. A woman aged 30 years with a severe 120 ° ky- phosis secondary to a laminectomy as a child for an ependymoma. She had progressive deformity and pain. A multilevel (T3-T12) anterior ligament release, ante- rior discectomy, correction with an anterior distractor (SLOT) and fixation with multiple rib grafts and an autogenous rib graft was carried out. She also had a posterior spinal fusion; instrumentation was not used because of the large posterior defect. She was immo- bilised in a halo cast for one year and a Milwaukee brace for one year. This radiograph was taken 3 years after operation and showed a solid fusion at 82°; the rib and fibular grafts can be seen.

270 R. Winter: The treatment of spinal kyphosis
Such children should be carefully watched with preoperative and then serial postoperative lateral radiographs. Treatment should begin if there are signs of progression. A Milwaukee brace can be used as a temporizing measure, but the only de- finitive treatment is anterior and posterior fusion. The posterior fusion is difficult because of the ab- sent laminae and must be done in the area of the facets and transverse processes. Instrumentation is either difficult or impossible. Halo casts are often necessary for both correction and to hold the spine until the fusion is solid. Failure to use a halo is the commonest error in patients referred to our clinic. The second error is failure to do an adequate anterior fusion, and the third is the re- moval of the external support too early [13] (Fig. 5).
Neurofibromatous kyphosis
Spinal deformity is the commonest skeletal prob- lem in patients with neurofibromatosis. They may have a lordoscoliosis or pure scoliosis, but a large number have a kyphoscoliosis which may be either a rotational kyphosing scoliosis or a true kyphosis. These patients often develop paraplegia [14].
The treatment of these severe kyphoses is a real test of the spinal surgeon's ability. Preopera- tive halo traction can be very helpful and must be followed by anterior fusion with multiple strut grafts and then a posterior fusion with autogenous bone. These procedures demand a highly skilled technique. Instrumentation should be used, but often the deformity is so severe that this is im- possible. Halo casts are the answer to this difficult challenge. Of all spinal deformities these heal most slowly, and they must be immobilised until they are absolutely solid [15].
Traumatic kyphosis
Patients with vertical load injuries may have a classical burst fracture with severe disruption of the anterior column of the spine. If only a cast is used there is nothing to prevent anterior shorten- ing and a residual kyphosis.
In the past we have used posterior rods with 2 below and 3 above instrumentation in order to achieve adequate leverage forces. But is it really necessary to operate on 6 vertebrae when only 2 or 3 are injured? Pedicle screws produce good early reduction, but late failure is common be- cause there is no anterior bony strut. It is there- fore logical to operate anteriorly at the site of the damage; bony fragments can be removed and a
strong strut graft inserted. Although this might seem to be adequate fixation, collapse can occur [16]. Posterior pedicle fixation is quite satisfac- tory, but needs a second exposure and has the risks of pedicle screws. Anterior fixation is more satisfactory and recently we have used the Kaneda device or Armstrong plates; our experi- ence with this technique has been excellent and biomechanical testing has demonstrated the high quality of the fixation [17].
Discussion
Some of the many causes of structural kyphosis have been reviewed in this paper and the aetio- logical factors should be appreciated by ortho- paedic surgeons who treat these conditions.
It is a great advantage to be able to do both anterior and posterior fusions, and several sys- tems of instrumentation are available to meet the requirements of each patient. We have been able to learn from the successes and failures of our predecessors. The greatest single advance was the development of transthoracic anterior spinal sur- gery. Although Hodgson [9] is usually given credit for this, the method was first published by Ito et al. in 1934 [10].
References
Classification 1. Terminology Committee, Scoliosis Research Society, A
glossary of scoliosis terms (1976) Spine 1 : 57-58
Biomechanics 2. Panjabi M, Brand R, White A (1976) Mechanical proper-
ties of the human thoracic spine. J Bone Joint Surg [Am] 58 : 642
3. White A, Panjabi M (1978) Clinical biomechanics of the spine. Lippincott, Philadelphia
Seheuerrnann's disease 4. Sachs B, Bradford D, Winter R et al. (1987) Scheuer-
mann's kyphosis: follow-up of Milwaukee brace treat- ment. J Bone Joint Surg [Am] 69:50-57
5. Bradford D, Khalid B, Moe J et al. (1980) The surgical treatment of patients with Scheuermann's disease. A re- view of 24 cases managed by anterior and posterior fu- sion. J Bone Joint Surg [Am] 62:705
Congenital kyphosis 6. Winter R, Moe J (1982) The results of spinal arthrodesis
for congenital spine deformity in patients younger than 5 years old. J Bone Joint Surg [Am] 64:419-432
7. Winter R, Moe J, Lonstein J (1985) The surgical treatment of congenital kyphosis: A review of 94 patients aged 5 years or older. Spine 10:224-231
8. Lonstein J, Winter R, Moe J e t al. (1980) Neurologic defi- cits secondary to spinal deformity: A review of the litera- ture and report of 43 cases. Spine 5:331-355
Tuberculosis 9. Hodgson A, Stock F (1956) Anterior spinal fusion. A pre-
liminary communication on the radical treatment of Pott's disease. Brit J Surg 44:266-275

R. Winter: The treatment of spinal kyphosis
10. Ito H, Tsuchiya J, Asami G (1934) A new radical opera- tion for Pott's disease. J Bone Joint Surg 16:499
11. Medical Research Council Working Party on Tubercu- losis of the Spine (1982) A ten year assessment of a con- trolled trial comparing debridement and anterior spine fu- sion in Hong Kong. J Bone Joint Surg 64B: 393-398
Post-Larninectorny Kyphosis 12. Lonstein J, Winter R et al. (1976) Post-laminectomy spine
deformity. J Bone Joint Surg 58A: 727 13. Lonstein J (1987) Post laminectomy spine deformity.
Pp 513-522 in Moe's Textbook of Scoliosis, Saunders Co., Philadelphia
Neurofibrornatosis Kyphosis 14. Winter R, Moe J, Bradford D, et al. (1979) Spine defor-
mity in neurofibromatosis. J Bone Joint Surg 61A: 677-694
271
15. Winter R, Lonstein J, Anderson M (1988) Neurofibroma- tosis hyperkyphosis: A review of 33 patients with kyphosis of 80 ° or greater. J Spinal Disorders 1 : 39-49
Traumatic Kyphosis 16. Kaneda K, Abumi K, Fujiya M (1984) Burst fractures
with neurologic deficits of the thoracolumbar and lumbar spine: Results of anterior decompression and stabilization with anterior instrumentation. Spine 9:788-795
17. Gurr K, McAfee P, Shih CM (1988) Biomechanical analy- sis of anterior and posterior instrumentation systems after corpectomy: A calf spine model. J Bone Joint Surg [Am] 70:1182-1191






![Apoptosis of endplate chondrocytes in cervical kyphosis is ...deformity in the cervical spine [1]. If cervical kyphosis (CK) has a progression with damage to the spinal cord, surgical](https://img.pdfslide.us/doc/110x75/60de786243c0f812a85e37cd/apoptosis-of-endplate-chondrocytes-in-cervical-kyphosis-is-deformity-in-the.jpg)