Embed Size (px)
Citation preview

THE TREATMENT OF COMPOSITE DEFECT OF BONE AND SOFTTISSUES WITH A COMBINED LATISSIMUS DORSI AND SERRATUSANTERIOR AND RIB FREE FLAP
EMILIO TRIGNANO, M.D., Ph.D.,1,2,3 NEFER FALLICO, M.D.,2* AGNESE NITTO, M.D.,1 and HUNG-CHI CHEN, M.D., M.H.A., F.A.C.S.1
Background: Composite defects of bone and soft tissues represent a reconstructive challenge. Several techniques have been described inthe medical literature; however, extensive composite defects should be reconstructed with microvascular free tissue transfer. The purposeof this report is to present the use of a composite latissimus dorsi and serratus anterior and rib free flap (LD-SA/rib) as an alternative pro-cedure in patients who cannot undergo more commonly used vascularized bone-containing free flap reconstruction. Methods: Since Janu-ary 2009, 12 patients have undergone bone and soft tissues reconstruction with a composite LD-SA/rib flap. In this case series, indicationsfor LD-SA/rib reconstruction were large mandibular defects after oral cancer ablation, scalp defects, and lower extremity defects. Results:All flaps survived entirely. With reference to postoperative complications, haematoma occurred in four patients, scar contractures in threecases, lower lip incontinence in one patient, and local infection in one patient. Skin graft revision was performed in two cases and second-ary debulking procedure in three patients. Flap viability was consistent during the 2-year follow-up. Conclusions: LD-SA/rib free flap shouldbe regarded as an effective procedure for reconstruction of composite tissue defects in patients who are not candidates for morecommonly used vascularized bone-containing free flaps. VVC 2013 Wiley Periodicals, Inc. Microsurgery 33:173–183, 2013.
Composite defects of bone and soft tissues resultingfrom tumor ablation, radiation treatment, infection, ortrauma represent a reconstructive challenge.
Several techniques for the reconstruction of bonedefects have been described in the medical literature,including direct nonvascularized cancellous bone grafts,1,2
vascularized bone grafts,3,4 bone transport using the Ili-zarov bone lengthening technique.5
However, composite defects also need an adequatesoft tissue covering. Extensive composite defects cannotbe reconstructed with local muscular flaps or conven-tional bone grafts but need composite bone and soft tis-sue transfer instead. Microvascular free tissue transferallows early definitive reconstruction of combined boneand soft tissues defects.6
In this report, we present our results in the treatment ofcombined bone and soft tissues defects with a composite latis-simus dorsi and serratus anterior and rib free flap (LD-SA/rib).
PATIENTS AND METHODS
Since January 2009, 12 patients have undergone boneand soft tissues reconstruction with a composite LD-SA/rib
osteomuscular free flap (Table 1). The age of the patientsranged from 29 to 71 years (average age 50.3 years).Thegroup consisted of 10 male (83.3%) and 2 female (16.7%)patients.
In this case series, indications for LD-SA/rib recon-struction were large mandibular defects after oral cancerablation in 5 cases, scalp defects in three cases, andlower extremity defects in four cases (two involving themetatarsal bones and the other two the calcaneus).
All procedures were performed at the China MedicalUniversity Hospital of Taichung (Taiwan) by the samesurgical team.
SURGICAL TECHNIQUE
An elliptical-shaped skin island was designed alongthe medial border of the latissimus dorsi muscle. The in-ferior border of the flap was identified, and the dissectionwas performed with an inferior-to-superior direction untilthe desired rib was reached.
A patent musculo-periosteal perforator vessel was iden-tified and isolated to transfer the rib based on the periostealblood supply. The rib bone was harvested along with the an-terior rib periosteum while the posterior rib periosteum wasleft adherent to the parietal pleura through a meticulous dis-section over the undersurface of the rib, in the attempt toprevent the perforation of the parietal pleura.
The desired segment of the rib was then osteotomizedfirst laterally and then medially, leaving 3–4 cm of rib ateach side.
To prevent scapular winging, the SA muscle was notentirely harvested, but indeed it was coronally split as toobtain two halves of all serratus muscle slips, one ofwhich is left at the donor site and the other is transferredto the recipient site.
1Department of Plastic and Reconstructive Surgery, China Medical UniversityHospital, 2 Yuh-Der Road, Taichung 40447, Republic of China, Taiwan2Department of Plastic and Reconstructive Surgery, ‘‘Sapienza’’ University ofRome, Viale del Policlinico 151, 00161 Rome, Italy3Department of Plastic and Reconstructive Surgery, University of Sassari,Viale San Pietro 43b, 07100 Sassari, Italy
*Correspondence to: Nefer Fallico, M.D., Via Val Savio 3, 00141, Rome, Italy.E-mail: [email protected]
Received 11 June 2012; Revision accepted 17 October 2012; Accepted 22October 2012
Published online 25 February 2013 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/micr.22067
VVC 2013 Wiley Periodicals, Inc.

After elevation of the SA-rib component, the remain-ing portion of the flap, i.e., the LD myocutaneous compo-nent, was harvested along with its thoraco-dorsal pediclewhich is followed superiorly up to the take-off of thesubscapular vessels from the axillary artery. Flap harvestwas completed by ligating and transecting the circumflexscapular artery. In this way, the pedicle can reach up to11 cm in length, compared with the thoraco-dorsal arterythat can only reach 4–5 cm.
The flap was then inset on the defect site, and micro-vascular anastomoses were performed.
After placing two drainage tubes, the donor site wasclosed by direct suture. To avoid seroma formation, thelateral part of the fascia was sutured with Vicryl 2/0.
RESULTS
Patients’ data and reconstructions performed are sum-marized in Table 1 along with the description of the flapcharacteristics and complications.
The incidence of flap complications in our case serieswas 50% (6/12 cases). (Table 2)
Four of 12 flaps (33.3%) presented a hematoma andtherefore needed a second procedure to drain it. Twocases (16.6%) needed a revision of the skin graft,
which did not take completely on. The reason for suchcomplication was probably due to the absence of acompressive dressing, which was not performed toavoid the compression of the pedicle. In two patientswith mandibular reconstruction (cases 1 and 4) and inone patient with calcaneal reconstruction (case 8; 25%),a secondary procedure was performed to reduce thebulk of the flap. In three cases of mandibular recon-struction (cases 1, 7, and 9; 25%), scar contractureswere released through z-plasties. Case 7 (7.7%) alsoneeded a tendon graft to correct lower lip incontinence.In a case of scalp reconstruction (case 11; 7.7%) localinfection was observed; however, it was successfullytreated with antibiotic therapy. Despite these complica-tions, all flaps were viable.
Table 2. Complications
Complications Number of cases Incidence
Hematoma 4 33.3%Skin graft partial necrosis 2 16.6%Excessive bulk 3 25Scar contracture 3 25Wound infection 1 7.7%Lower lipin continence 1 7.7%
Table 1. Patients’ Data and Description of the Flap Characteristics and Complications
CasesAge
and sexType ofdefect Type of flap Pedicles Recipient vessels Complications
1 45, M Mandible LD-SA/11th rib Subscapular artery and vein Superficial temporal artery þmandibular branch vein
Skin graft partialnecrosis; excessivebulk; scar contracture
2 36, F Scalp LD-SA/5th and7th ribs
Subscapular artery and vein Superficial temporal artery þmandibular branch vein
None
3 37, M Metatarsalbones
LD-SA/5th and7th ribs
Subscapular artery and veinand circumflex scapularartery and vein
Posterior tibial arteryand veins
Skin graft partialnecrosis, Hematoma
4 58, M Mandible LD-SA/11th rib Subscapular artery and vein Superficial temporal artery þmandibular branch vein
Excessive bulk,Hematoma
5 71, M Mandible LD-SA/11th rib Subscapular artery and vein Superior thyroid artery andexternal jugular vein
None
6 29, M Calcaneus LD-SA/5th and7th ribs
Subscapular artery and veinand circumflex scapularartery and vein
Posterior tibial arteryand veins
None
7 68, M Mandible LD-SA/11th rib Subscapular artery and vein Superficial temporal arteryþmandibular branch vein
Lower lip incontinence;scar contracture
8 43, M Calcaneus LD-SA/5th and7th ribs
Subscapular and circumflexscapular artery and vein
Posterior tibial arteryand veins
Excessive bulk,Hematoma
9 67, M Mandible LD-SA/11th rib Subscapular artery and vein Superficial temporal artery þmandibular branch vein
Scar contracture
10 34, M Metatarsalbones
LD-SA/5th and7th ribs
Subscapular artery andcircumflex scapularartery and vein
Posterior tibial artery veins None
11 51, F Scalp LD-SA/5th and7th ribs
Subscapular artery and vein Superficial temporal artery andmandibular branch vein
Wound infection,hematoma
12 65, M Scalp LD-SA/5th and7th ribs
Subscapular artery and vein Superficial temporal artery andmandibular branch vein
None
LD, latissimus dorsi; SA, serratusanterior.
174 Trignano et al.
Microsurgery DOI 10.1002/micr

As for donor site complications, neither pneumothoraxnor weakness or winging of the scapula has occurred.
The functional recovery after reconstruction of lowerextremity defects was evaluated in terms of the abilityto walk without support and wear shoes. All patientsunderwent multiple physiotherapy sessions to improveambulation throughout the 2-year follow-up time. Thetwo patients with metatarsal defects (case 3 and 10)achieved complete functional recovery, respectively, at18 and 3 months after surgery. As for the two patientswith calcanear defects, case 6 despite the uneventfulpostoperative course at 2-year follow-up still neededsupport for walking and complained of foot pain. Case 8was able to walk at 3 months after the reconstructiveprocedure; however, he complained of an excessive bulkwhich prevented him from wearing shoes comfortably.As such, the patient underwent a debulking procedure 6months later.
With reference to the bone union rate, all patients(100%) achieved primary bone union.
The bone union time in our series ranged from 2.5months for the metatarsal bones to 8 months for thescalp, with an average union time of 6.7 months.
At 2-year follow-up stable results were observed inall patients. The scars at the donor and recipient areawere acceptable.
CASE REPORTS
Case 1
A 45-year-old businessman was diagnosed with leftoral cancer at Taichung Chung-San Hospital. After cancerablation, the resulting mandibular defect was recon-structed with a free fibula flap from the left leg. Subse-quently, the patient received radiotherapy and chemother-apy. After the radiation therapy, his reconstructed mandi-ble became exposed and grew necrotic, requiring asegmental resection of the left mandible. Subsequently,reconstruction with a free fibular osteocutaneous flapfrom the right leg was performed. It failed, though. Post-operative necrosis of the flap required debridement, whichcaused a 10 3 4 cm defect in the oral mucosa and a4-cm bone defect at the left submandibular area. Themandibular bone became exposed and developed asequestrum (Fig. 1A), and it was in contact with foodand saliva, which constantly leaked from the oral cavity.
Figure 1. A: deteriorated aspect of previous reconstructive procedures; B: intraoperative view of the mandibular defect; C: left LD-SA with 11thrib free flap; D: final result 2 years after the surgery. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Latissimus Dorsi þ Serratus Anterior and Rib Free Flap for Reconstruction of Composite Tissue Defects 175
Microsurgery DOI 10.1002/micr

The patient needed a new reconstruction and wastransferred in our department. A composite left LD-SAwith left 11th rib free flap was performed to reconstructthe left cheek, oral mucosa, and bone segment (Figs. 1B
and 1C). The skin paddle of the flap replaced the oralmucosa and a skin graft covered the muscle. A subscapu-lar pedicle was used to perform the anastomosis with thecontralateral superficial temporal artery. The skin graftdid not take completely on. So, 1 month later, theremaining skin defects were covered with split thicknessskin grafts. After 6 months, the patient underwent debulk-ing of the flap and release of scar contracture at the chinand neck through multiple Z-plasties.
The final result at 2 years from surgery was goodboth from an aesthetical and functional point of view(Figs. 1D and 2) as the patient was able to open andclose his mouth, to talk, to eat, and to swallow. No sali-vary incontinence was observed.
Case 2
A 36-year-old housewife affected by meningiomaunderwent a craniotomy for the removal of the tumorand, subsequently, a Gamma Knife surgery to remove theresidual tumor. The wound underwent chronic ulcerationwith bone exposure and subsequent Pseudomonas aerugi-nosa infection of the scalp. The patient was admitted toour department, where she underwent antibiotic therapyand extensive debridement. The resulting defect was 193 10 cm area at the occipital temporal region involvingthe dura mater, the calvarial bone, and the overlyingscalp (Fig. 3A). The defect was reconstructed with an ar-
Figure 2. Postoperative radiologic image of the mandibular recon-struction with LD-SA/rib flap.
Figure 3. A: preoperative aspect of the scalp defect; B: combined LD-SA/fifth and seventh ribs flap; C: final result 2 years after the sur-gery. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
176 Trignano et al.
Microsurgery DOI 10.1002/micr

tificial dura mater and a microsurgical combined flapcomposed of LD-SA with fifth and seventh ribs (Fig.3B). The ribs were fixed to the calvarial bone withscrews and Kirschner wires. The LD and SA musclescovered the artificial dura mater and the rest of thedefect. A wide skin paddle allowed the primary closureof the wound. After 12 hours, some bleeding wasobserved at the wound site. The patient was taken backto the operating room, and an hematoma was removed.
Two years after surgery, the flap presented a goodcolor and the residual scars, at the recipient and donorsites, were acceptable (Fig. 3C). Two years postoperativeradiologic images showing the stability of the scalpreconstruction both at a CT scan (Fig. 4A) and at an X-ray (Fig. 4B).
Case 3
A 37-year-old businessman suffered a severe crushinjury of the right lower limb, for which he received pri-mary treatment in a different hospital 4 years before. Inthat occasion, his right outer four toes were amputatedbecause of their devascularization. The hallux had sur-vived because the lateral digital artery was not injured.The resulting defect was covered with a free fibularosteocutaneous flap and crossleg flap. After surgery, thepatient was able to walk but still presented a chronic dis-charge from necrotic tissue around the metatarsal bones.As a consequence, he underwent several debridement pro-cedures, which, however, did not resolve the problem. Asswab cultures from the wound grew Methicillin-resistantStaphylococcus aureus, Vancomycin was administered.However, no improvement was observed. He was admit-ted to our department with necrotic tissue and sequestrum
at distal tibia after free flap reconstruction. As the patientunderwent extensive debridement, a composite bone andsoft tissue defect was observed in the metatarsal area.(Fig. 5A) A combined free flap composed of LD-SA withfifth and seventh ribs was performed for metatarsal recon-struction (Fig. 5B). The skin defect was covered withsplit thickness skin grafts. The posterior tibial artery waschosen as recipient vessel. As the anterior tibial arteryhad been damaged at the time of the crush injury, it wasnot possible to perform an end-to-end anastomosis to theposterior tibial artery (Fig. 5C). As a consequence, wedecided to perform two end-to-end anastomoses: the firstone between the subscapulary artery and the proximalpart of the posterior tibial artery and the second onebetween the circumflex scapular artery and the distal partof the posterior tibial artery. This allowed us to preservethe integrity of the posterior tibial artery, which was theonly source of blood supply for the inferior extremity ofthe patient. The metatarsus was replaced by one rib,which was fixed to the tarsal bones and the proximalphalanx of the hallux with Kirschner wires. The other ribwas positioned between the second and third metatarsalbones to give stability to the deambulation. The mainte-nance of the arch structure of the foot and the separatereconstruction of metatarsal bones allowed us to preservethe shock absorber function of the foot.
The flap had a smooth postoperative course. Only theskin grafts needed a revision.
At 2-year follow-up, the flap was stable and thepatient was able to walk and to wear shoes without prob-lems (Fig. 5D). The posterior tibial nerve being intact,both the function and the sensitivity of the heel was pre-served. Indeed, the patient referred pain elicited by me-
Figure 4. A: Postoperative CT 3D scan of the scalp reconstruction (frontal view); B: Postoperative radiologic image of the scalp recon-struction (lateral view). [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Latissimus Dorsi þ Serratus Anterior and Rib Free Flap for Reconstruction of Composite Tissue Defects 177
Microsurgery DOI 10.1002/micr

chanical stimulation. A 2 years postoperative radiologic
image shows the stability of the metatarsal reconstruction
(Fig. 6).
Case 8
A 43-year-old man with a history of severe crushinjury of the left leg was admitted to our department
Figure 5. A: preoperative aspect presenting necrotic tissue and composite bone and soft tissue defect in the metatarsal area; B: combinedLD-SA/fifth and seventh ribs free flap; C: intraoperative view of the metatarsal defect; D: final result 2 years after our surgery. [Color figurecan be viewed in the online issue, which is available at wileyonlinelibrary.com.]
178 Trignano et al.
Microsurgery DOI 10.1002/micr

with cicatricial outcomes of previous reconstruction withskin grafts (Figs. 7 and 8A). The patient underwent de-bridement and reconstruction with a combined LD-SAwith fifth and seventh ribs flap.
The two ribs were fixed together in a L-shape usingKirchner wires and were then fixed to the rest of the cal-caneus bone by means of plates and screws (Fig. 8B).The muscles were positioned to avoid empty spaces. Theanastomosis was performed to the posterior tibial artery,for also in this patient, the anterior tibial artery had beendamaged in the injury. As in case 3, the subscapulary ar-tery was anastomosed with the proximal part of the pos-terior tibial artery and the circumflex scapular artery withthe distal part of the posterior tibial artery. The skindefect was covered with split thickness skin grafts. Theflap had a smooth postoperative course. Only part of theskin grafts needed a revision.
Six months after surgery a debulking procedure wasperformed enabling the patient to walk and wear shoesmore comfortably.
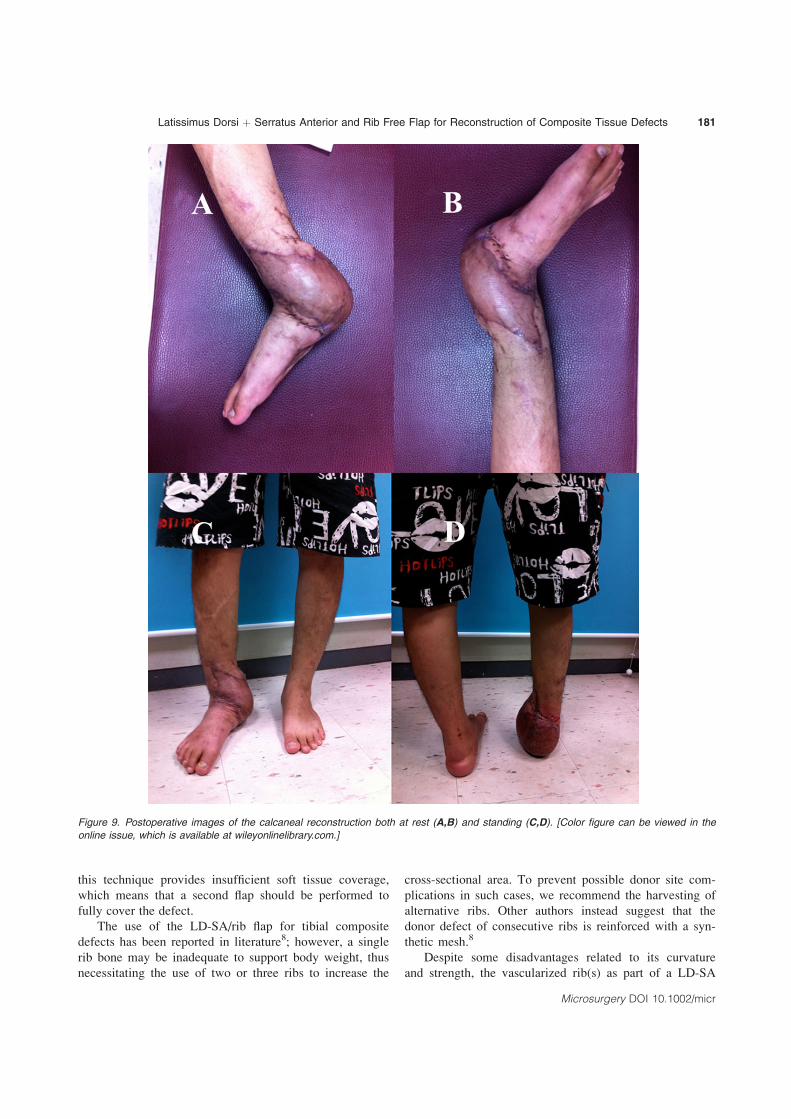
The final result at 2 years from surgery was goodboth from an aesthetical and functional point of view asthe patient was able to walk without support and wearshoes (Figs. 9A–9D). However, the patient occasionallycomplained of foot pain when standing or walking for along time.
DISCUSSION
The management of bone defects associated with softtissue loss is challenging and requires a composite tissuereconstruction.
A two-stage reconstruction in composite bone andsoft tissue defects brings about more difficulties becauseof increased scarring and lack of available, healthy recipi-ent vessels. For these reasons, most authors believe thatthese composite defects can be better managed in a one-stage procedure.7–11
The most commonly used flaps in composite defectreconstruction are the vascularized fibula osteoseptocuta-neous flap,3,12–15 the vascularized iliac osteocutaneousflap,13,16 and the vascularized muscular rib flap.8,11,17,18
The free fibula flap is considered the most suitableamong these vascularized bone grafts. However, some-times it is not available because it has been previouslyused, as in cases 1 and 3, or because of severe peripheralvascular disease of the leg. Moreover, this flap is notindicated in case of large tissue loss requiring musclecover.
Regarding the vascularized iliac bone, its curvature,length, and skin paddle do not generally correspond tothe reconstruction of large bone and soft tissue defects. Itprovides a limited quantity of bone and muscle, and itspedicle is short. Moreover, the iliac crest free flappresents a high incidence of donor site morbidity, such aspostoperative pain and gait disturbance.
Alternative bone-containing free flaps, such as theosteo-cutaneous radial forearm flap, can be complicatedby pathologic fractures of the radius after flap harvest.Moreover, it provides a limited quantity of bone tissue.19
The free flaps based on the circumflex scapular arterycontaining the lateral border of the scapula require a longduration of surgery due to impossible simultaneous flap
Figure 6. Postoperative radiologic image of the metatarsal recon-struction with LD-SA/rib flap. [Color figure can be viewed in theonline issue, which is available at wileyonlinelibrary.com.]
Figure 7. Cicatricial outcomes of previous calcaneal reconstructionwith skin grafts. [Color figure can be viewed in the online issue,which is available at wileyonlinelibrary.com.]
Latissimus Dorsi þ Serratus Anterior and Rib Free Flap for Reconstruction of Composite Tissue Defects 179
Microsurgery DOI 10.1002/micr

harvest and tumor resection in case of oral cancer (simul-taneous two-team surgery). Moreover, bone stock fromthe lateral scapular border may not be sufficient for largedefects (larger than 10 cm).18
Furthermore, all these bone-containing free flap,except for the LD-SA/rib flap, only include a limitedamount of muscle. As a consequence, in case of large tis-sue loss requiring extensive muscle cover they appearinsufficient.
LD-SA/rib osteomusculocutaneous free flap is effec-tive for reconstruction of composite tissue defects inpatients who are not candidates for more commonly usedvascularized bone-containing free flaps, and in cases inwhich a muscular component is required as the defectcannot be covered only by bone and skin. This flap isuseful for small to large bone defects accompanied bylarge soft tissue defects. The rib bone offers reconstruc-tive advantages over other bone sources in specificpatients.6 In addition, the size of the myocutaneous com-ponent of the flap can be tailored according to the vol-ume of the soft tissue defect. Furthermore, its pedicle islong, and its vessels are of large caliber and are not com-monly involved in peripheral vascular diseases.6,20–22 Thedonor site morbidity is limited in terms of functional andaesthetic sequelae. The donor site defect can be closedprimarily with a scar that is easily disguisable because ofits location on the axillary line, which can only be seenwhen the patient elevates the arms. A two-team approachis possible, and there is no need of intraoperative reposi-tioning.23
Another advantage of this combined flap is the inde-pendent vascular pedicle of its components, which allowsfreedom in orienting the various tissue segments.6
In contrast with the description of the LD-SA/rib flapgiven by Kim and Blackwell,23 we prefer to use lowerribs, i.e., ninth or 11th, because of the possibility to har-vest a longer flap. Moreover, the rib bone was harvestedalong with the anterior rib periosteum while the posteriorrib periosteum was left adherent to the parietal pleuraproceeding to a subperiosteal dissection on the posteriorborder of the rib, as described in previous reports,24,25 toprevent the opening of the parietal pleura. In fact, con-trary to their results, in our case series, no secondarypneumothorax has occurred.
The LD-SA/rib flap remains one of the best indica-tions in reconstruction of metatarsal bones, as the archstructure of the foot is well reconstructed using the curveof the ribs.26,27 In fact, the shock absorber function ofthe foot was well preserved in case 3 because of themaintenance of the arch structure of the foot and to theseparate reconstruction of each metatarsal bone. A recon-struction with a single lump of bone would not havebeen so resistant to external forces, and the foot wouldnot have been able to stand torsional stress.
For other defects in the lower limbs, ipsilateral vascu-larized fibular transposition is a plausible option especiallyfor tibial reconstruction as described by Chung et al.28
Unfortunately, it does not seem appropriate for compositedefects of the bone and soft tissue as it is not long enoughto reach either the calcaneus or the metatarsus. Moreover,
Figure 8. A: preoperative (at time of admission) radiologic image of the metatarsal defect; B: 3-month postoperative radiologic image ofthe metatarsal reconstruction with LD-SA/rib flap.
180 Trignano et al.
Microsurgery DOI 10.1002/micr
this technique provides insufficient soft tissue coverage,which means that a second flap should be performed tofully cover the defect.
The use of the LD-SA/rib flap for tibial compositedefects has been reported in literature8; however, a singlerib bone may be inadequate to support body weight, thusnecessitating the use of two or three ribs to increase the
cross-sectional area. To prevent possible donor site com-plications in such cases, we recommend the harvesting ofalternative ribs. Other authors instead suggest that thedonor defect of consecutive ribs is reinforced with a syn-thetic mesh.8
Despite some disadvantages related to its curvatureand strength, the vascularized rib(s) as part of a LD-SA
Figure 9. Postoperative images of the calcaneal reconstruction both at rest (A,B) and standing (C,D). [Color figure can be viewed in theonline issue, which is available at wileyonlinelibrary.com.]
Latissimus Dorsi þ Serratus Anterior and Rib Free Flap for Reconstruction of Composite Tissue Defects 181
Microsurgery DOI 10.1002/micr

osteomuscular flap also proves to be a reliable flap in cal-caneal bone and soft tissue reconstruction.29 The calca-neum is a cortical bone while the rib is a cortico-cancel-lous bone that may not tolerate well to the weight bear-ing heel area. As a consequence, patients may experiencepainful heel while walking and rib fracture can developin time. However, to avoid excessive pressure on the ribsthe LD and SA muscles have been wrapped around theribs as a cushion. According to our experience, thepatients are able to walk without problems although theymight develop complications in time.
The LD-SA/rib composite free flap is also useful in avariety of head and neck reconstructive situations. Iliaccrest and fibula are reported to provide a better qualitybone for osseointegrated dentition. In fact, the little corti-cal bone of the rib is not appropriate for the placementof osteointegrated dental implants.23 The rib, however,contours easily and can, in contrast to the iliac crest, pro-vide sufficient material for total mandibular reconstruc-tion. Moreover, the temporo-mandibular joint can bereconstructed using the cartilaginous portion of the rib.30
The long thoraco-dorsal vascular pedicle allowed vesselanastomosis in the lower part of the neck and by-passedprevious vascular anastomoses and area of postoperativescarring without requiring vein grafts. Because of thelarge amount of muscle, in case of radiation therapy therib flap has the advantage of preventing bone exposure.Moreover, in case of flap revision, this accounts for a re-markable pliability.
This flap is very useful also in skull reconstruction.31
In fact, the rib bone ideally fits the calvarium as the ribbone is slender and easily contoured. Although someauthors maintain that skull reconstruction can be per-formed without using bony component,32 in their report,the defect was localized at the base of the skull while incase of calvarial defect bony material plays a key role giv-ing further stability to the reconstructed area. Calvarialreconstruction is usually performed using nonvascularizedbone grafts,33 however, there are instances in which theshortage of protective soft tissue coverage makes the freevascularized bone graft the preferred choice.34 In case 2,which presented extensive skull and dura mater defectswith sepsis, an artificial dura mater was used together witha combined LD-SA/rib flap as a triple-layered mantle toprotect the brain, similarly to the report by Lee et al.34
A further option for reconstructing large calvarialdefects consists in splitting the two ribs into four nonvas-cularized ribs. However, the ribs are a very fragile struc-ture and if longitudinally split they can break while if cuthorizontally they might not be long enough to beattached at the borders of the skull. Therefore, thisapproach was not used in our case series.
The limitations of the LD-SA/rib flap are the rib bonecurvature which may not always be appropriate, its limited
cross-sectional area to withstand body weight load and thehigher morbidity rate compared with other vascularizedbone transfers.
Main donor site complications associated with this flapare secondary pneumothorax and scapular winging. Toprevent pleural perforation, we used the subperiosteal dis-section of the rib. The scapular winging can be preventedor minimized by harvesting the lowest two or three slipsof the SA muscle or by anchoring the remaining slips tothe periosteum of the superjacent and subjacent ribs.35,36
We decided to split the SA muscle in a coronal plane toleave all serratus muscle slips at the donor site.
In this report, we have reviewed the use of the com-bined LD-SA/rib as an alternative to the often used fibulaor iliac crest in patients in whom such flaps are not avail-able. The results of vascularized bone grafting are basedon bone union rate, the occurrence of complications, andflap viability at final 2-year follow-up.
Our results regarding primary bone union rate (100%)are more encouraging than those reported in other stud-ies. In the series by Lin et al.,8 three out of eight patients(62.5%) did not achieve primary bone union. In the seriesby Kim and Blackwell,23 the primary bone union ratewas of 86%. In fact, four of 29 patients experienceddelayed wound healing related to hardware infection orextrusion, which did not occur in our case series, and onepatient showed partial bone resorption probably due tothe underlying condition of osteogenesis imperfecta.Georgescu et al.25 had a primary bone union rate of97.7% with only one of 44 patients showing a nonunionthat was ascribed to the recurrence of osteitis. However,they finally obtain the union in this case in 15 months.
With reference to bone union time, our findings aresimilar to those reported by Lin et al.8 (6.8 months) andGeorgescu et al.25 (6.6 months) in terms of average uniontime. However, some differences have been recorded at therecipients sites with shorter time to bone union at the meta-tarsal bones, in accordance with data by Georgescu et al.25
In this series of 12 reconstructions with LD-SA/ribflap, there were no complete flap failure but 6 patients(50%) experienced postoperative complications. Compli-cations associated with the flap include hematoma, partialnecrosis of the skin graft, excessive bulk, and scar con-tracture. Indeed, this procedure presents a high percentageof wound site complications in accordance with datafrom similar studies. The overall complication rate wasof 66.7% (6/9 patients) for Lin et al.8 and of 48% (14/29patients) for Kim and Blackwell.23
The limitations of this report are the small number ofcases in our series and the lack of a statistical analysis ofthe complications.
Our series was composed of extremely rare cases forwhich we do not have clear guidelines. As in thesepatients we could not perform more commonly used
182 Trignano et al.
Microsurgery DOI 10.1002/micr

vascularized bone-containing free flaps, the alternativeoption was the amputation. In such patients, theLD-SA/rib flap has proved to be a useful alternativeprocedure providing a reliable vascularized reconstructivecombination of bone and muscle.
REFERENCES
1. Chan KM, Leung YK, Cheng JC, Leung PC. The management oftype III open tibial fractures. Injury 1984;16:157–165.
2. Christian EP, Bosse MJ, Robb G. Reconstruction of large diaphysealdefects without free fibular transfer in grade IIIB tibial fractures. JBone Joint Surg Am 1989;71:994–1004.
3. Minami A, Kasashima T, Iwasaki N, Kato H, Kaneda K. Vascular-ized fibular grafts: An experience of 102 patients. J Bone Joint SurgBr 2000;82:1022–1025.
4. Brown KL. Limb reconstruction with vascularized fibular grafts afterbone tumor resection. Clin Orthop Relat Res 1991;262:64–73.
5. Dagher F, Roukoz S. Compound tibial fractures with bone losstreated with Ilizarov technique. J Bone Joint Surg Br 1991;73:316–321.
6. Netscher D, Alford EL, Wigoda P, Cohen V. Free composite myo-osseous flap with serratus anterior and rib: Indications in head andneck reconstruction. Head Neck 1998;20:106–112.
7. Yasar S, Lin CH, Wei FC. One stage reconstruction of compositebone and soft-tissue defects in traumatic lower extremities. PlastReconstr Surg 2004;114:1457–1466.
8. Lin CH, Wei FC, Levin LS, Su JI, Fan KF, Yeh WL, Hsu DT. Freecomposite serratus anterior and rib flaps for tibial composite boneand soft tissue defect. Plast Reconstr Surg 1997;99:1656–1665.
9. Swartz WM, Mears DC. Management of difficult lower extremityfractures and nonunions. Clin Plast Surg 1986;13:633–644.
10. Doi K, Kawakami F, Hiura Y, Oda T, Sakai K, Kawai S. One-stagetreatment of infected bone defects of the tibia with skin loss by freevascularized osteocutaneous grafts. Microsurgery 1995;16:704–712.
11. Weiland AJ, Moore JR, Daniel RK. The efficacy of free tissue transfer inthe treatment of osteomyelitis. J Bone Joint Surg Am 1984;66:181–193.
12. Arai K, Toh S, Tsubo K, Nishikawa S, Narita S, Miura H. Compli-cations of vascularized fibula grafts for reconstruction of long bones.Plast Reconstr Surg 2002;109:2301–2306.
13. Lin CH, Wei FC, Chen HC, Chuang DCC. Outcome comparison intraumatic lower extremity reconstruction by using various compositevascularized bone transplantation. Plast Reconstr Surg 1999;104:984–992.
14. Wei FC, El-Gammal TA, Lin CH, Ueng WN. Free fibula osteosepto-cutaneous graft for reconstruction of segmental femoral shaft defects.J Trauma 1997;43:784–792.
15. Wei FC, Chen HC, Chuang CC, Noordhoff MS. Fibular osteosepto-cutaneous flap: Anatomical study and clinical applications. PlastReconstr Surg 1986;78:191–200.
16. Hierner R, Wood MB. Comparison of vascularized iliac crest andvascularized fibula transfer for reconstruction of segmental and par-tial bone defects in long bones of the lower extremities. Microsur-gery 1995;16:818–826.
17. Guelinckx PJ, Sinsel NK. The ‘‘Eve’’ procedure: The transfer of vas-cularized seventh rib, fascia, cartilage, and serratus muscle to recon-struct difficult defects. Plast Reconstr Surg 1996;97:527–535.
18. Thomas WO, Harris CN, Moline S, Harper LL, Prker JA. Versatilityof the microvascular serratus anterior muscle vascularized rib flap(SARIB) for multifaceted requirements reconstructions. Ann PlastSurg 1999;42:132–136.
19. Sinclair CF, Gleysteen JP, Zimmermann TM, Wax MK, Givi B,Schneider D, Rosenthal EL. Assessment of donor site morbidity forfree radial forearm osteocutaneous flaps. Microsurgery 2012;32:255–260.
20. Tobin GR, Moberg A, Ringberg A, Netscher D. Mandibular-facialreconstruction with segmentally split serratus anterior compositeflaps. Clin Plast Surg 1990;17:663–672.
21. Schlenker JD. Incorporating vascularized ribs in a latissimus dorsimyocutaneous flap. Plast Reconstr Surg 1991;88:920–921.
22. Yamamoto Y, Sugihara T, Kawashima K, Qi F. An anatomic studyof the latissimus dorsi-rib flap: An extension of the subscapular com-bined flap. Plast Reconstr Surg 1996;98:811–816.
23. Kim PD, Blackwell KE. Latissimus-serratus-rib free flap for oroman-dibular and maxillary reconstruction. Arch Otolaryngol Head NeckSurg 2007;133:791–795.
24. Chang DW, Miller MJ. A subperiosteal approach to harvesting thefree serratus anterior and rib myo-osseous composite flap. PlastReconstr Surg 2001;108:1300–1304.
25. Georgescu AV, Ignatiadis I, Ileana M, Irina C, Filip A, Olariu R.Long term results after muscle-rib flap transfer for reconstruction ofcomposite limb defects. Microsurgery 2011;31:218–222.
26. Kurokawa M, Muneuchi G, Hamagami H, Fujita H. Reconstructionof four metatarsal bone and soft-tissue defects using a serratus ante-rior muscle rib osteomyocutaneous free flap. Plast Reconstr Surg1998;101:1616–1619.
27. Kurokowa M, Yamada N, Suzuki S, Muneuchi G. Long-term followup of reconstruction of four metatarsal bone and soft tissue defectsusing a serratus anterior muscle rib osteomyocutaneous free flap.Plast Reconstr Surg 2004;114:1553–1555.
28. Chung DW, Han CS, Lee JH. Reconstruction of composite tibialdefect with free flaps and ipsilateral vascularized fibular transposi-tion. Microsurgery 2011;31:340–346.
29. Brenner P, Zwipp H, Rammelt S. Vascularized double barrel ribscombined with free serratus anterior muscle transfer for homologousrestoration of the hindfoot after calcaneotomy. J Trauma 2000;49:331–335.
30. Munro IR. One stage reconstruction of temporomandibular joint inhemifacial microsomia. Plast Reconstr Surg 1980;66:669–710.
31. Steuber K, Salcman M, Spence RJ. The combined use of the latissi-mus dorsi musculocutaneous free flap and split rib grafts for cranialvault reconstruction. Ann Plast Surg 1985;15:155–160.
32. Lo KC, Jeng CH, Lin HC, Hsieh CH, Chen CL. A free compositede-epithelialized anterolateral thigh and the vastus lateralis muscleflap for the reconstruction of a large defect of the anterior skullbase: A case report. Microsurgery 2011;31:568–571.
33. Chang V, Hartzfeld P, Langlois M, Mahmood A, Seyfried D. Out-comes of cranial repair after craniectomy. J Neurosurg 2010;112:1120–1124.
34. Lee JW, Hsueh YY, Lee JS. Composite skull and dura defect recon-struction using combined latissimus dorsi musculocutaneous and ser-ratus anterior muscle-rib free flap coupled with vascularized galeatransfer: A case report. Microsurgery 2010;8:632–635.
35. Georgescu AV, Ivan O. Serratus anterior-rib free flap in limb bonereconstruction. Microsurgery 2003;23:217–225.
36. Derby LD, Barlett SP, Low DW. Serratus anterior free tissue trans-fer: Harvest related morbidity in 34 consecutive cases and a reviewof literature. J Reconstr Microsurg 1997;13:397–403.
Latissimus Dorsi þ Serratus Anterior and Rib Free Flap for Reconstruction of Composite Tissue Defects 183
Microsurgery DOI 10.1002/micr





























