Embed Size (px)
Citation preview
The TMJ and the MiddleEar: Structural and
Functional Correlates forAural SymptomsAssociated With
Temporomandibular |ointDysfunction
Carolyn M. Ash, DDSAdvanced Education in ProsthodonticsUniversity of Southern Californietos Angeles, California
Otympio F. Pinto, CO. MSProsthodontistRio De laneiro, Brazil
Several anatomic relationships existing between the ear andthe femporomandibular joint have been proposed to accountfor the presence of atjral symptoms that occur in somepafienfs with temporomandibular ¡oinf dysfunction. There area plethora of functional hypotheses for aural symptomsrelating to disturbed funcfions of the eusfachian tube (as wellas neuromuscular relationships and neurovascular functionsintegrating with fhese hypotheses). Investigators explain thepresence of aural symptoms relative to the anatomicrelationship of fhe middle ear fo fhe TMJ as hypotheticallydue in part to the "tiny ligament," the sphenomandibularligament, or the diskomalleolar ligament. This article reviewshypotheses, explanations, and current research on fhiscontroversial issue. Int I Prosthodont 1991;4:51-57.
A ural symptoms often complained of by patientswith temporomandibular joint dysfunction
(TMD) are otalgia, tinnitus, impaired hearing (inter-mittent or contintiotis), stuffy sensations in the ears,and vertigo.'-' The existence and cause of some ofthese symptoms remain controversial and are evenconsidered to be entirely subjective or unrelated toTMD. However, there is renewed interest in pos-sible structural or functional correlations betweenthe ear, joints, and associated muscles because ofthe influence that treatment of TMD has had ontinnitus in some patients.
Nature of the Problem
It is no longer appropriate to think of temporo-mandibular joint (TM)) and muscle dysfunction as acollective constellation of symptoms and proposedcauses known as Costen's Syndrome,' or as a com-plex of symptoms and multifactorial causesdescribed as a "TMj Syndrome." It is possible tocategorize TMD, but it is not always possible to
Reprint requests: Dr Carolyn M. Ash, I533S Pomerado Road,Suite 203, Poway, California 92064.
determine the cause of associated symptoms. Cer-tainly, muscle dysfunction associated with some dis-orders may be related to a number of sensory inputsto the brain stem. However, a particularly difficultproblem is the subjective nature of ear symptomsassociated with TMD and the absence of objectivetests for correlating aural symptoms and TMD.
Incidence
Otalgia appears to be the most frequent of auralsymptoms described by patients with TMD.' Thefrequency of other subjective aural symptoms inTMD has been reported to be about 4%,^' butmuch higher percentages (25%) may be given,°even with normal audiologic findings.'
The apparent disparity between reported fre-quencies of subjective symptoms may relate to thefailure to discriminate between patients with inter-mittent audiologic symptoms, failure to use audio-metric tests (eg, pure tone threshold, impedance),and inclusion of older patients with a reduction ofhearing acuity. Although tests of the eustachian tubemay be normal, in TMD patients a disturbance ofactive opening may occur frequently during swal-lowing/ Some symptoms of TMD are also commonin the general population, but, in the absence of
•21-ie4, Number 1, 1991 5 1 The International ]oiirnal of Prosthodontic
The TM| and tiie Middle Ea Aih/PintD
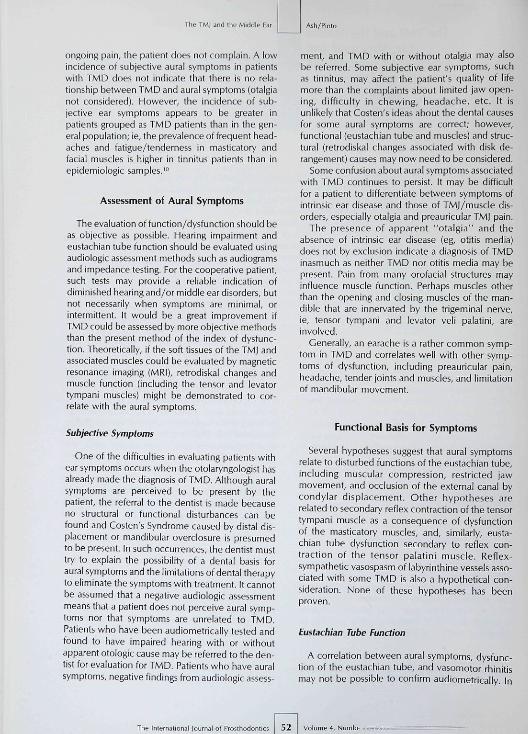
ongoing pain, the patient does not complain, A lowincidence of subjective aural symptoms in patientswith TMD does not indicate that there is no rela-tionship between TMD and aural symptoms (otalgianot considered). However, the incidence of sub-jective ear symptoms appears to be greater inpatients grouped as TMD patients than in the gen-eral population; ie, the prevalence of frequent head-aches and fatigue/tenderness in masticatory andfacial muscles is higher in tinnitus patients than inepidemiologic samples,^"
Assessment of Aural Symptoms
The evaluation of function/dysfunction should beas objective as possible. Hearing impairment andeustachian tube function should be evaluated usingaudiologic assessment methods such as audiogramsand impedance testing. For the cooperative patient,such tests may provide a reliable indication ofdiminished hearing and/or middle ear disorders, butnot necessarily when symptoms are minimal, orintermittent. It would be a great improvement ifTMD could be assessed by more objective methodsthan the present method of the index of dysfunc-tion. Theoretically, if the soft tissues of the TM| andassociated muscles could be evaluated by magneticresonance imaging (MRI), retrodiskal changes andmuscle function (including the tensor and levatortympani muscles) might be demonstrated to cor-relate with the aural symptoms.
Subjective Symptoms
One of the difficulties in evaluating patients withear symptoms occurs when the otoiaryngologist hasalready made the diagnosis of TMD. Although auralsymptoms are perceived to be present by thepatient, the referral to the dentist is made becauseno structural or functional disturbances can befound and Costen's Syndrome caused by distal dis-placement or mandibular overclosure is presumedto be present. In such occurrences, the dentist musttry to explain the possibility of a dental basis foraural symptoms and the limitations of dental therapyto eliminate the symptoms with treatment. It cannotbe assumed that a negative audiologic assessmentmeans that a patient does not perceive aural symp-toms nor that symptoms are unrelated to TMD.Patients who have been audiometrically tested andfound to have impaired hearing with or withoutapparent otoiogic cause may be referred to the den-tist for evaluation for TMD, Patients who have auralsymptoms, negative findings from audiologic assess-
ment, and TMD with or without otalgia may alsobe referred. Some subjective ear symptoms, suchas tinnitus, may affect the patient's quality of lifemore than the complaints about limited jaw open-ing, difficulty ¡n chewing, headache, etc. It isunlikely that Costen's ideas about the dental causesfor some aural symptoms are correct; however,functional (eustachian tube and muscles) and struc-tural (retrodiskal changes associated with disk de-rangement) causes may now need to be considered.
Some confusion about aural symptoms associatedwith TMD continues to persist. It may be difficultfor a patient to differentiate between symptoms ofintrinsic ear disease and those of TMJ/muscle dis-orders, especially otalgia and preauricular TM) pain.
The presence of apparent "otalgia" and theabsence of intrinsic ear disease (eg, otitis media)does not by exclusion indicate a diagnosis of TMDinasmuch as neither TMD nor otitis media may bepresent. Pain from many orofacial structures mayinfluence muscle function. Perhaps muscles otherthan the opening and closing muscles of the man-dible that are innervated by the trigeminal nerve,ie, tensor tympani and levator veli palatini, areinvolved.
Generally, an earache is a rather common symp-tom in TMD and correlates well with other symp-toms of dysfunction, including preauricular pain,headache, tender joints and muscles, and limitationof mandibular movement.
Functional Basis ior Symptoms
Several hypotheses suggest that aural symptomsrelate to disturbed functions of the eustachian tube,including muscular compression, restricted jawmovement, and occlusion of the external canal bycondylar displacement. Other hypotheses arerelated to secondary reflex contraction of the tensortympani muscle as a consequence of dysfunctionof the masticatory muscles, and, similarly, etista-chian tube dysfunction secondary to reflex con-traction of the tensor palatini muscle. Reflex-sympathetic vasospasm of labyrinthine vessels asso-ciated with some TMD is also a hypothetical con-sideration. None of these hypotheses has beenproven.
Eustacbian Tube Function
A correlation between aural symptoms, dysfunc-tion of the eustachian tube, and vasomotor rhinitismay not be possible to confirm audiometrically. In
The Intemational Journal of Prosthodontif 52 • 4, Numbt..-.—Vi;z=
As h/Pinto The TM| and Ihe Middle Ear
some patients with vasomotor rhinitis and TMD,auditory symptoms improve with occlusal splinttherapy and repositioning devices but return wbenthese are not used. FHowever, objective studiesusing appropriate audiometric tests and use/nonusesplint therapy have not been reported. It is possiblethat only audiometric impedance tests would beaffecfed.
Some patients who complain of transient auralsymptoms have difficulty in yawning and swallowingbecause of pain or restricted jaw movement,"Although the symptoms may subside with effectivetreatment of tbe associated TMD, fhe relationshipto the function of fhe eustacbian tube is not clear.Studies of such dysfunction and active and passivetests of tensor palatini and levator palatini musclesare difficult to conduct. Even so, in some instances,disturbances may relate to TMD. '^"
The normal function of the eustacbian tubeequalizes intratympanic pressure and environmen-tal air pressure. Disturbances in its function maycause a decrease in perception of bigher tones.'^ Itis unlikely that direct condylar pressure causes dys-function of the tube, but an anatomic relationshipexists in which mandibtilar position could indirectlyinduce symptom acuity.'" Occasional functionaltubal disturbances could relate to aural symptoms,although tympanometric evidence suggests other-wise,'^ Occlusion of tbe external auditory canal anderosion of the tympanic plate are highly unlikely tooccur,'" even though fenestration of the plate is notuncommon in dry skull material.
Neuromuscular Relationships
Muscle dysfunction may be caused by central andperipheral influences. Because there is a commonnerve supply for tbe masticatory muscles as well asfor the tensor tympani and veli palatini muscles, ithas been suggested that disturbances in tbe mas-ticatory muscles, joints, and/or other orofacial tis-sues may cause a secondary reflex confraction ofthe tensor tympani muscle and hence aural symp-toms.'*'
If bruxism, clenching, and associated muscle dis-order causes dysfunction of the tensor tympani, asobserved in tympanotomy procedures,'<• if is diffi-ctilt to accept the premise that such tensor tympanihyperactivity is tbe reflection of a generalized stateof muscle hyperactivity and the coincidental effecfof a central cause,' Bioieedback training is seldomhighly effective unless the hyperactive muscle(s)and the source of pain are identified and the mus-cle(s) subsequently "retrained." The activity of the
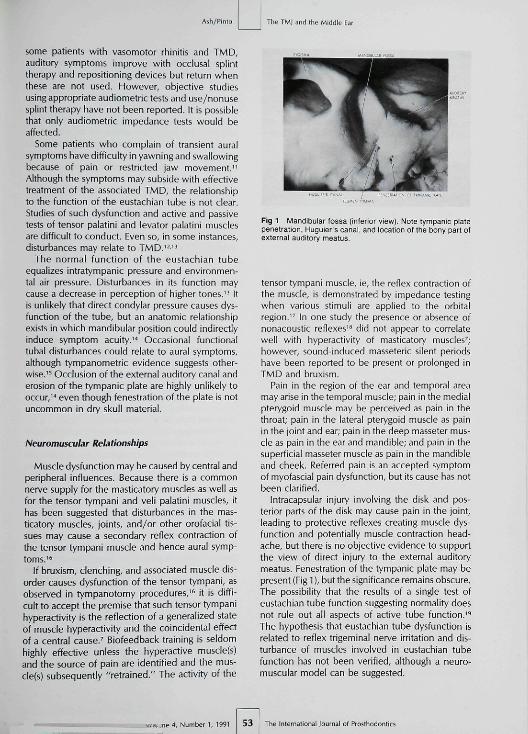
Fig 1 Mandibular fossa ¡inferior view]. Note tympanic platepenetration, Huguier's canal, and location of ttie bony part otexternal auditory meatus.
tensor tympani muscle, ie, the reflex contraction ofthe muscle, is demonstrated by impedance testingwhen various stimuli are applied to the orbitalregion." In one study the presence or absence ofnonacoustic reflexes'" did not appear to correlatewell with hyperactivity of masticatory muscles^;however, sound-induced masseteric silent periodshave been reported to be present or prolonged inTMD and bruxism.
Pain in the region of the ear and temporal areamay arise in the temporal muscle; pain in the medialpterygoid muscle may be perceived as pain in thethroat; pain in the lateral pterygoid muscle as painin the joint and ear; pain in the deep masseter mus-cle as pain in the ear and mandible; and pain in tbesuperficial masseter muscle as pain in the mandibleand cheek. Referred pain is an accepted symptomof myofascial pain dysfunction, but its cause has notbeen clarified,
¡ntracapsular injury involving the disk and pos-terior parts of the disk may cause pain in the joint,leading to protective reflexes creating muscle dys-function and potentially muscle contraction head-ache, but there is no objective evidence to supportthe view of direct injury to the external auditorymeatus. Fenestration of the tympanic plate may bepresent (Fig 1), butthe significance remains obscure.The possibility that the results of a single test ofeustachian tube function suggesting normality doesnot rule out all aspects of active tube function.'^The hypothesis that eustachian tube dysfunction isrelated to reflex trigeminal nerve irritation and dis-turbance of muscles involved in eustachian tubefunction has not been verified, although a neuro-muscular model can be suggested.
DaiCijne4, Number I, 1991 53 The International lournal of Prosthodontics
The TM| and ihe Middle Ea Ash/Pinto
Seurovascular Function
There is evidence that some autonomie nervefibers from the otic ganglion reach the TMJ^" andthat reflex-sympathetic vasospasm of the labyrin-thine vessels could hypothetically occur secondaryto abnormal stimulation of autonomie nerves sup-plying the TM],' However, it is difficult to objec-
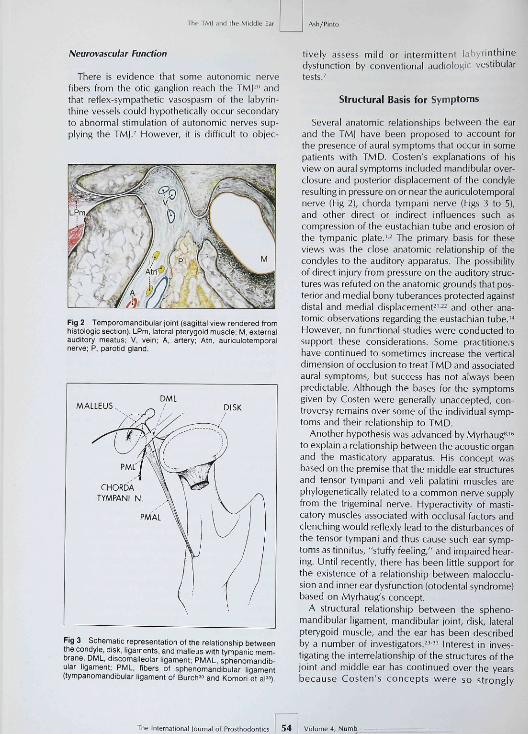
Fig 2 Temporomandibular joint (sagittal view rendered fromhistologie section). LPm, lateral pterygoid muscle: M, externalauditory meatus; V, vein; A, artery; Atn, auriculotemporalnerve; P, parotid gland.
MALLEUSDML
DISK
CHORDATYMPANI N
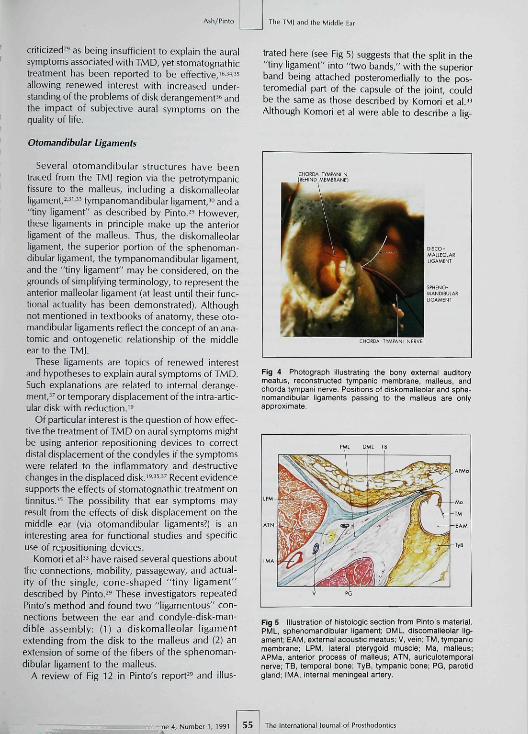
Fig 3 Schematic representation of the relationship betweenthe condyle, disk, ligaments, and malleus with tympanic mem-brane, DML, discomaileolar iigament; PMAL, sphenomandib-uiar ligament; PML, fibers of sphenomandibular ligament(tymparomandibular ligament ot Burch^» and Komori et al")
tively asses5 mild or intermittent labyrinthinedysfunction by conventional audiologic vestibulartests,'
Structural Basis for Symptoms
Several anatomic relationships between the earand the TMJ have been proposed to account forthe presence of aural symptoms that occur in somepatients with TMD, Costen's explanations of hisview on aural symptoms included mandibular over-closure and posterior displacement of the condyleresulting in pressure on or near the auriculotemporalnerve (Fig 2), chorda tympani nerve (Figs 3 to 5),and other direct or indirect influences such ascompression of the eustachian tube and erosion ofthe tympanic plate,'-^ The primary basis for theseviews was the close anatomic relationship of thecondyles to the auditory apparatus. The possibilityof direct injury from pressure on the auditory struc-tures was refuted on the anatomic grounds that pos-terior and medial bony tuberances protected againstdistal and medial displacement^'" and other ana-tomic observations regarding the eustachian tube,'"However, no functional studies were conducted tosupport these considerations. Some practitione,shave continued to sometimes increase the verticaldimension of occlusion to treat TMD and associatedaural symptoms, but success bas not always beenpredictable. Although the bases for the symptomsgiven by Costen were generally unaccepted, con-troversy remains over some of the indivitjual symp-toms and their relationship to TMD.
Another hypothesis was advanced by Myrhaug"''^to explain a relationship between the acoustic organand the masticatory apparatus. His concept wasbased on the premise that the middle ear structuresand tensor tympani and veli palatini muscles arephylogenetically related to a common nerve supplyfrom the trigeminal nerve. Hyperactivity of masti-catory muscles associated with occlusal factors andclenching would reflexly lead to the disttirbances ofthe tensor tympani and thus cause such ear symp-toms as tinnitus, "stuffy feeling," and impaired hear-ing. Until recently, there has been little support forthe existence of a relationship between malocclu-sion and inner ear dysfunction (otodental syndrome)based on Myrhaug's concept,
A structural relationship between the spheno-mandibular ligament, mandibular joint, disk, lateralpterygoid muscle, and the ear has been describedby a number of investigators,"" Interest in inves-tigating the interrelationship of the structures of thejoint and middle ear has continued over the yearsbecause Costen's concepts were so strongly
The Intemationai lournal ol Prosthodontii 54 '. 4, Numb
Ash/Pinto
criticized'^ as being insufficient to explain the auralsymptoms associated witb TMD, yet stomatognatbictreatment bas been reported to be effective, "̂ •̂"'̂allowing renewed interest with increased under-standing of tbe problems of disk derangement'*- andthe impact of subjective aural symptoms on thequality of life.
Otomandibular Ligaments
Several otomandibular structures have beentraced from the TMI region via the petrotympanicfissure to the malleus, including a diskomalleolarligament,^^'" tympanomandibular ligament,^" and a"tiny ligament" as described by Pinto." However,these ligaments in principle make up tbe anteriorligament of tbe malleus. Thus, tbe diskomalleolarligament, the superior portion of the sphenoman-dibular ligament, tbe tympanomandibular ligament,and the "tiny ligament" may be considered, on thegrounds of simplifying terminology, to represent theanterior malleolar ligament (at least until their func-tional actuality has been demonstrated). Althoughnot mentioned in textbooks of anatomy, these oto-mandibuiar ligaments reflect tbe concept of an ana-tomic and ontogenetic relationship of tbe middleear to tbe TMJ.
These ligaments are topics of renewed interestand hypotheses to explain aural symptoms of TMD.Such explanations are related to internal derange-ment,'' or temporary displacement of the intra-artic-ular disk with reduction.'^
Of particular interest is the question of how effec-tive the treatment ofTMD on aural symptoms mightbe using anterior repositioning devices to correctdistal displacement of the condyles if tbe symptomswere related to tbe inflammatory and destructivechanges in the displaced disk.'^^^-'^ Recent evidencesupports the effects of stomatognathic treatment ontinnitus.^^ The possibility that ear symptoms mayresult from the effects of disk displacement on themiddle ear (via otomandibular ligaments?) is aninteresting area for functional studies and specificuse of repositioning devices.
Komori et a l " have raised several questions aboutthe connections, mobility, passageway, and actual-ity of tbe single, cone-shaped "tiny ligament"described by Pinto." Tbese investigators repeatedPinto's metbod and found two "ligamentous" con-nections between the ear and condyle-disk-man-dible assembly: (1) a diskomalleolar ligamentextending from tbe disk to tbe malleus and (2) anextension of some of tbe fibers of the sphenoman-dibular ligament to the malleus.
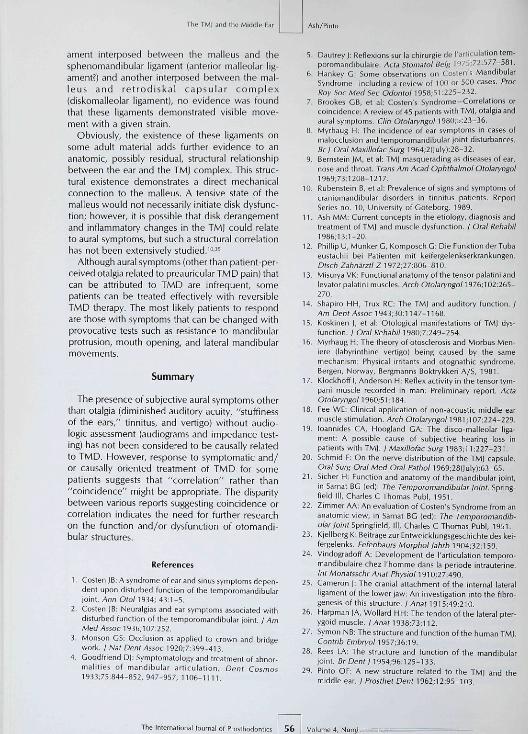
A review of Fig 12 in Pinto's report^^ and illus-
The TM| and tlie Middle Ear
trated here (see Fig 5) suggests that the split in the"tiny ligament" into "two bands," witb the superiorband being attached posteromedially to the pos-teromedial part of tbe capsule of the joint, couldbe tbe same as those described by Komori et al ."Although Komori et al were able to describe a lig-
CHOtCA(EEHINE
TIMMNI NMlfMBRAME}
ÉÉMCHOBDA lY
ÉíT^^^^Ê DISCO-
— ^ ^ ^ ^ H Í̂AILEOLAC^ ^ ^ ^ ^ H LIGAMENT
^ ^ ^ ^ ^ 1 SPHEFJO-• ^ ^ ^ H MANDIBUIAR• ^ ^ ^ H LIGAMÍMT
HWPANL NfBVE
Fig 4 Photograph illustrating the bony external auditorymeatus, reconstructed tympanic membrane, malleus, andchorda tympani nerve. Positions of aiskomalieolar and Sphe-nomanûibular ligaments passing to the malleus are onlyapproximate.
Fig 5 Illustration of histoiogic section from Pinto's material,PML. sphenomandibular ligament; DML, discomalleolar lig-ament; EAM, external acoustic meatus; V. vein; TM, tympanicmembrane; LPM, lateral pterygoid muscle; Ma, malleus;APMa, anterior process ot malleus; ATN, auriculotemporalnerve; TB, temporal bone; TyB. tympanic bone; PG, parotidgland; IMA. internal meningeal artery.
-ne 4, Number l . 1991 55 The Interrutional Icurnal of Prosthodontics
The TM| and the Middle Ea Ash/Pinto
ament interposed between the malleus and thesphenomandibular ligament (anterior malleolar lig-ament?) and another interposed between the mal-leus and retrodiskal capsular complex(diskomalieolar ligament), no evidence was foundthat these ligaments demonstrated visible move-ment with a given strain.
Obviously, the existence of these ligaments onsome adult material adds further evidence to ananatomic, possibly residual, structural relationshipbetween the ear and the TMj complex. This struc-tural existence demonstrates a direct mechanicalconnection to the malleus, A tensive state of themalleus would not necessarily initiate disk dysfunc-tion; however, it is possible that disk derangementand inflammatory changes in the TMJ could relateto aural symptoms, but such a structural correlationhas not been extensively studied.'""
Although aural symptoms ¡other than patient-per-ceived otalgia related to preauricular TMD pain) thatcan be attributed to TMD are infrequent, somepatients can be treated effectively with reversibleTMD therapy. The most likely patients to respondare those with symptoms that can be changed withprovocative tests such as resistance to mandibularprotrusion, mouth opening, and lateral mandibularmovements.
Summary
The presence of subjective aural symptoms otherthan otalgia (diminished auditory acuity, "stuffinessof the ears," tinnitus, and vertigo) without audio-logic assessment (audiograms and impedance test-ing) has not been considered to be causally relatedto TMD. However, response to symptomatic and/or causally oriented treatment of TMD for somepatients suggests that "correlation" rather than"coincidence" might be appropriate. The disparitybetween various reports suggesting coincidence orcorrelation indicates the need for further researchon the function and/or dysfunction of otomandi-bular structures.
References
1. C05ten IB: Asyndrorneof ear and sinus symptoms depen-dent upon drsturbed function of Ihe lemporomandibularjoin!. Ann 0(0/1934: 4i:1-5.
2. Costen ]B: Neuralgias and ear sympioms associated wilhdisturbed i'unclion of the temporomandibylar joint. ; AmMed Assoc ^33(,:^ 07.252.
3. Monson GS: Occlusion as applied lo crown and bridgework, j Nat Dent Assoc 1930;7:399-41 3.
4. Coodfriend D|: Symptomatology and trealment of abnor-malities of mandibular articulation. Dent Cosmos1933;75:844-e52, 947-957, 1106-1111.
Dautrey J: Reflexions sur la chirurgie de I'artic ulation tem-poiomandibulaire. Acta Stomatol Beig 197S;72:577-581.Hankey G: Some observations on Custen's MandibularSyndrome-including a review of 100 or 500 cases. PfocRoy Soc Med Sec Odontol 1958:51:225-232.Brookes Gß, et al: Costen's Syndrome-Correlations orcoincidence: A review of 45 patients with TM|, otalgia andaural symptoms. Clin Otolaryngons80;5.23-3b.Myrhaug H: The incidence of ear symptoms in cases ofmalocclusion and temporomandibular ¡oint disturbances.Brj Oral Maxiilofac Surg 1964;2(luly):2B-32.Bernstein |M, et al: TM| masquerading as diseases of ear,nose and throat. Trans Am Acad Ophthalmol Otolaryngol1969,73:1208-1217.Rubenstein B, et al: Prevalence of signs and symptoms ofcraniomandibular disorders in tinnitus patients. ReportSeries no. 10, University of Göteborg, 1989.Ash MM: Current concepts in the etiology, diagnosis andtreatment of TM| and muscle dysfunction. J Oral Rehabii1986;I3:1-2Q,Phillip U, Munker G, Komposch G: Die Funktion der Tubaeustachii bei Patienten mit keifergelenkserkrankungen.Dtsch Zahnarzt! Z 1972:27:006-310.Miíurya VK: Functional anatomy of the tensor palatini andlevator palatini muscles. Arch Otolaryngol ]97(>:}02:2f>5-270.Shapiro HH, Trux RC: The TMJ and auditory function. /Am DentAssoc 1943,30:1147-1168.Koskinen J, et al: Otological manifestations of TM] dys-function. / Oral Reiiab/7 1980;7:249-254.Myrhaug H: The theory of otosclerosis and Morbus Men-iere (labyrinthine vertigo) being caused by the samemechanism: Physical irritants and otognathic syndrome.Bergen, Norway, Bergmanns Boktrykkeri A/S, I98I.Klockhoff I, Anderson H: Reflex activity in the tensor tym-pani muscle recorded in man: Preliminary report. ActaOtolaryngol I96O;5I:184.Fee WE, Clinical application of non-acoustic middle earmuscle stimulation. Arch Olo/aryngoM961 ;107:224-229.loannides CA, Hoogland GA: The disco-malleolar liga-ment: A possible cause of subjective hearing loss inpatienti with TMJ. / Mí;<j//o/ác 5urg 1983;11:227-231.Schmid F: On thp nerve distribution of the TM| capsule.Oral Surg Oral Med Oral Pathol 1969;28(|uly|:63-65,Sicher H: Function and anatomy of the mandibular joint,in Sarnat BG (ed): The Temporomandibular joint. Spring-field HI, Charles C Thomas Publ, 1951.Zimmer AA: An evaluation of Costen's Syndrome from ananatomic view, in Sarnat BG (ed]: The Temporomandib-ular ¡oint Ipimgmd, ll[, Charles C Thomas Publ, 1951.Kjellberg K: Beitrage zur Entweicklungsgeschichte des kei-fergelenks, Fefenbaurs Morpho! ¡ahrb 1904;32:159.Vindogradoff A: Development de l'articulation temporo-mandibulaire chez l'homme dans la période intrauterine.Int Monatsschr Anat PhysiohS^0,2?.430.Cameron |: The cranial attachment of the internal lateralligament of the lower jaw: An investigation into the fibro-genesis of this structure. ; ,Anai 1915,49:210.Harpman |A, Wollard HH. The tendon of the lateral pter-ygoid muscle, I Anat I938;73:112.
Symon NB: The structure and function of the human TM|.Contrib Embryofi357;3i..}g.Rees LA: The structure and function of the mandibular¡oint. Br Dent! 1954;96:I25-133.Pinto OF: A new structure related to the TMJ and themiddle ear. ; Prosthet Dent 1962:12:95-103.
The Internationa I of Prosthodontics 56

Ash/Pinto The TMI and the Middle Ear
30, Burch |C: The cranial attachment of the sphenomandib-ular ( tympanomandibular) l igament, Anat Rec1966:156:433-437.
31, Colemen RD: Ternporomandibular joint: Relation of theretrodiskal zone to Meckel's cartilage and lateral pterygoidmuscle, J Dent Res 1970:49:626-630.
32, Couly F, Hureau |: Les relations otomeniscale de I'artit-ulation temporo-mandibulaire du noveau. Arch Anat His-tol Embryo/1976;59;143,
33, Kortiori E, et al. Discomalleolar ligament in the adulthuman. / Craniomand Pract 1986:4:299-305,
34, Draf W, et al: Costensyndrom und Schellperzeptronssch-werhorigkeit. HNO 1971:19:179,
J5. Rubenstein B, Carlsson GE: Effects of stomatognathicIreatment on linnttus: A retrospective study. / CraniomandPract 19fi7:5:254-259,
36. Dolwick MF, Sanders B: TMI Internal Derangement andArthrosis. St Louis, CV Mosby, 1985,
37, Williams EH: The interrelationships of internal derange-ment of the TMI, headache, vertigo and tinnitus: A studyof 25 patients. Facial Orthop Temporomand Arthrol1086:3:13-17,
Literature Abstracts _
Congenital Heart Anomalies in Patients With Clefts ofthe Up and/or Palate
Ttie spectrum and severity of congenital heart disease in association with clefting were evaiuated in aretrospective study involving 78 patients. The prevalence of clefting in congenital heart diseasepatients was found to be a minimum of three times that of patients with a normal heart. The cardiacdefects observed were predominantly conotruncal, Faliot's tetraiogy was noted in 24% of the patiants,Additionaliy, the incidence of transposition, atrioventricuiar septal defects, and truncus arteriosus wasfound to be disproportionateiy high in these patients. Anomalies of other systems were observed inB7% ot the patients.
WyaeRKH, Mars M, Al-Mahdawi S, Russell-Eggitt IM, Blake KD, C'en Pa/als J 1990:27(3)258-264. Reterences: 51.Rapriiits: Dr Hicfiard K.H. Wyss. Senior Lecturer in Paediatric Cardiology, Institute ot Chiio Health, 30 GuiHord Street,London WCINtEH, Unjtaa Kingdom.—Sie l'en P, Haug. DDS. indiana University Sctiool oí Dentistry, tnaianapotis.indiana
Tooth Exfoliation and Necrosis of the Mandible—A RareComplication Following Trigeminal Herpes Zoster
Herpes zoster is an acute viral infection cfiaracterized by the appearance ot vesicles that occur on theskin and mucous membranes aiong the pathway of the involved nerve. Involvement of the trigeminalnerve often causes a pos therapeutic neuraigia. Pain ¡which may inciude tooth pain) is the initialsymptom, followed by vesicles 3 to 4 days later. Twenty-three patients having bone unilaterailyinvolyed in the distribution of the trigeminal nerve are described in the literature. Most of theindividuáis were healthy; however, seveh tiad been treated for malignant disease. One patientsuccumOed to oral mucosal lesions, necrosis of the underlying mandible, and subsequent exfoliation ofthree teeth. It is postulated that a vasculitis occurs as a result of «irai invasion of blood vessels
from adjacent peripheral nerves within the alveolus, leading to avascular necrosis.
Muto T, Tsuchiya H, Sato K, Kanazawa M, J Orai Maxi/tóOc Surg 1990:48:t000-1003 References: 32. Reprints: DrMuto, Departmerl of Oral and Maxiilofacial Surgery, School of Dentistry, Hokkaido, Japan,-fl/ionöa F, Jacob. DDS.MS. M.D. Anderson Cancer Center, htouston. Texas
" -«4, Number l , 1991 57 The International lournal of Prosthodontics