Embed Size (px)
Citation preview
The Syndemic of Hepatitis C in Opioid Use Disorder
MACS WebinarApril 12, 2021
Sarah Kattakuzhy, MDAssistant Professor
Institute of Human Virology at the University of Maryland School of Medicine

1-855-337-MACS (6227) • www.marylandMACS.org
Provides support to prescribers and their practices in addressing the needs of their patients with substance use disorders and chronic pain management.
All Services are FREE
• Phone consultation for clinical questions
• Education and training opportunities related to substance use disorders and chronic pain management
• Assistance with addiction and behavioral health resources and referrals
• Technical assistance to practices implementing or expanding office-based addiction treatment services
• MACS TeleECHO™ Clinics: collaborative medical education through didactic presentations and case-based learning
Maryland Addiction Consultation Service (MACS)
Disclosures
• Dr. Kattakuzhy was the PI on a grant for investigator-sponsored research from Gilead Sciences paid to the institution (2016)

Why Syndemic?
Epidemic of Hepatitis C
Syndemic of Hepatitis C and
Opioid Use Disorder
What Is A Syndemic?
“A syndemic, or synergistic epidemic, is more than a convenient portmanteau or a synonym for comorbidity. The hallmark of a syndemic is the presence of two or more disease states that adversely interact with each other, negatively affecting the mutual course of each disease trajectory, enhancing vulnerability, and which are made more
deleterious by experienced inequities.”
Lancet Editorial, 2017
Outline
Viral Characteristics and Epidemiology
Challenges and Strategies
Diagnosis, Treatment, and Monitoring

Viral Characteristics and Epidemiology
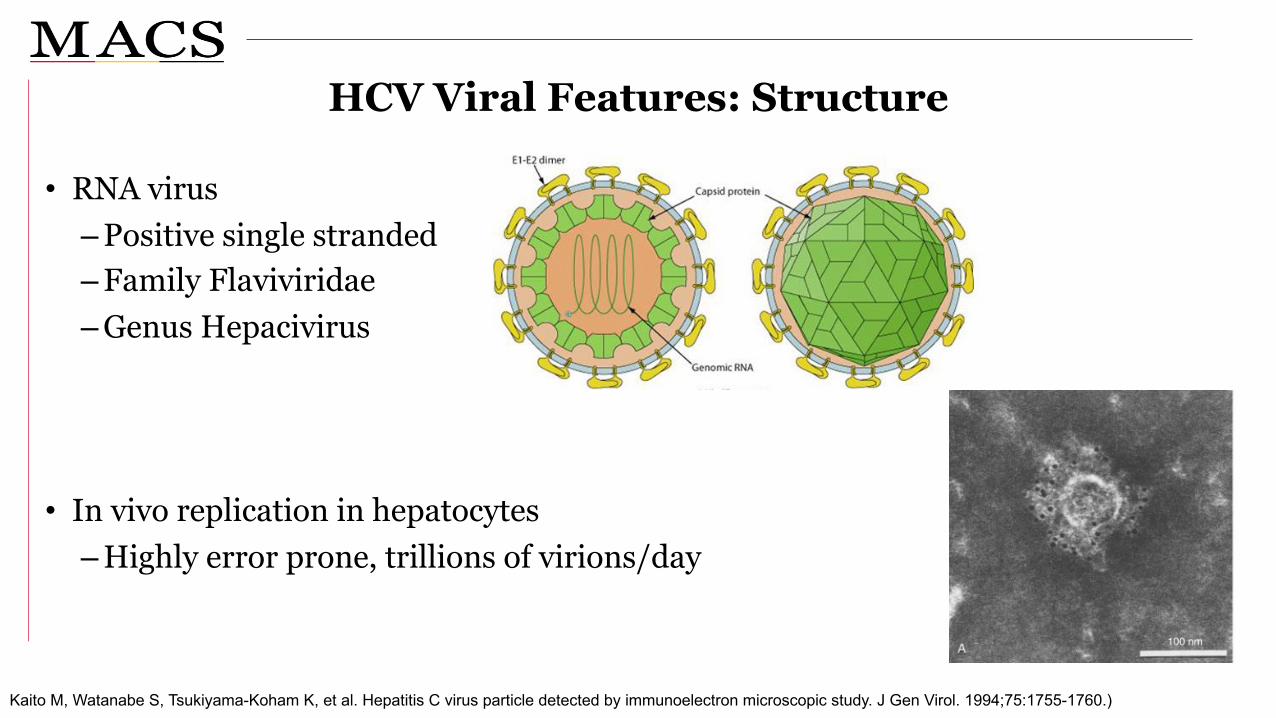
Kaito M, Watanabe S, Tsukiyama-Koham K, et al. Hepatitis C virus particle detected by immunoelectron microscopic study. J Gen Virol. 1994;75:1755-1760.)
HCV Viral Features: Structure
• RNA virus–Positive single stranded–Family Flaviviridae–Genus Hepacivirus
• In vivo replication in hepatocytes–Highly error prone, trillions of virions/day
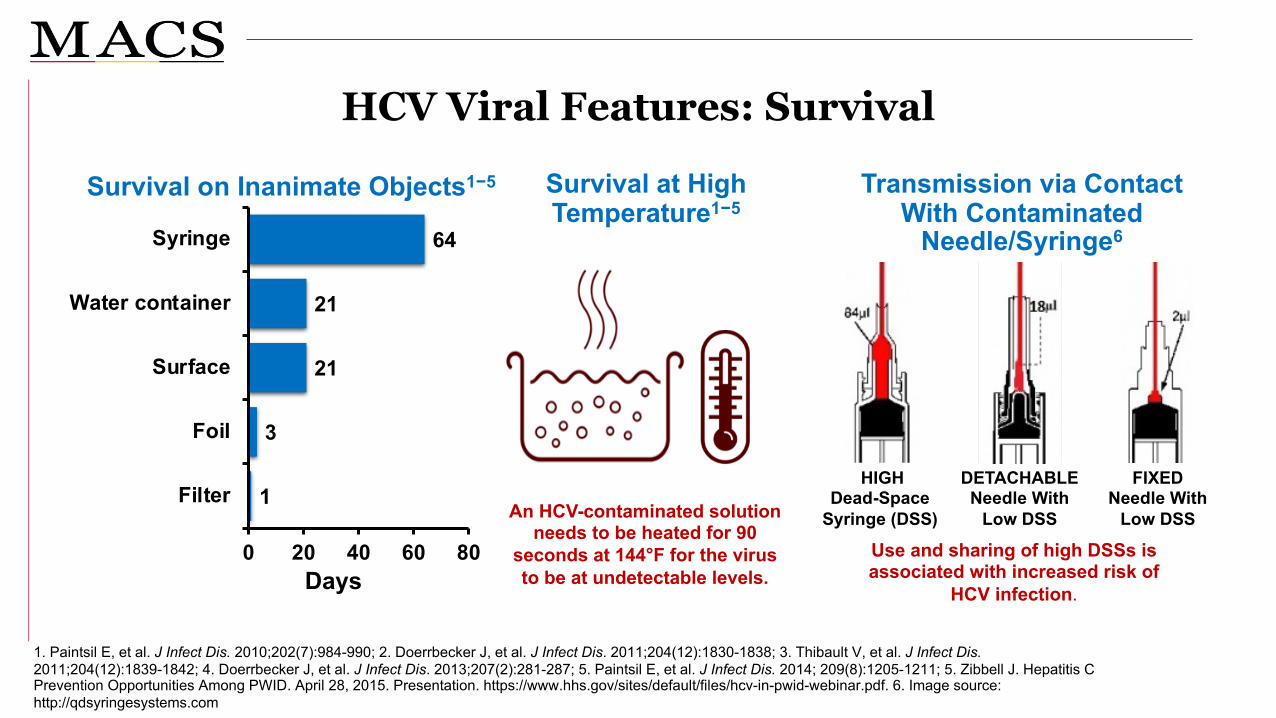
HCV Viral Features: Survival
1. Paintsil E, et al. J Infect Dis. 2010;202(7):984-990; 2. Doerrbecker J, et al. J Infect Dis. 2011;204(12):1830-1838; 3. Thibault V, et al. J Infect Dis. 2011;204(12):1839-1842; 4. Doerrbecker J, et al. J Infect Dis. 2013;207(2):281-287; 5. Paintsil E, et al. J Infect Dis. 2014; 209(8):1205-1211; 5. Zibbell J. Hepatitis C Prevention Opportunities Among PWID. April 28, 2015. Presentation. https://www.hhs.gov/sites/default/files/hcv-in-pwid-webinar.pdf. 6. Image source: http://qdsyringesystems.com
Survival on Inanimate Objects1−5
Days
Survival at High Temperature1−5
An HCV-contaminated solution needs to be heated for 90
seconds at 144°F for the virus to be at undetectable levels.
Transmission via Contact With Contaminated
Needle/Syringe6
HIGHDead-Space
Syringe (DSS)
DETACHABLENeedle With
Low DSS
FIXEDNeedle With
Low DSS
Use and sharing of high DSSs isassociated with increased risk of
HCV infection.
1
3
21
21
64
0 20 40 60 80
Filter
Foil
Surface
Water container
Syringe

HCV Viral Features: Genotype
Messina, Hepatology, 2015

HCV Transmission
6015
10
4
10
Injection Drug UseSexualTransfusion before 1985OccupationalUnknown
https://www.cdc.gov/hepatitis/hcv/hcvfaq.htm.
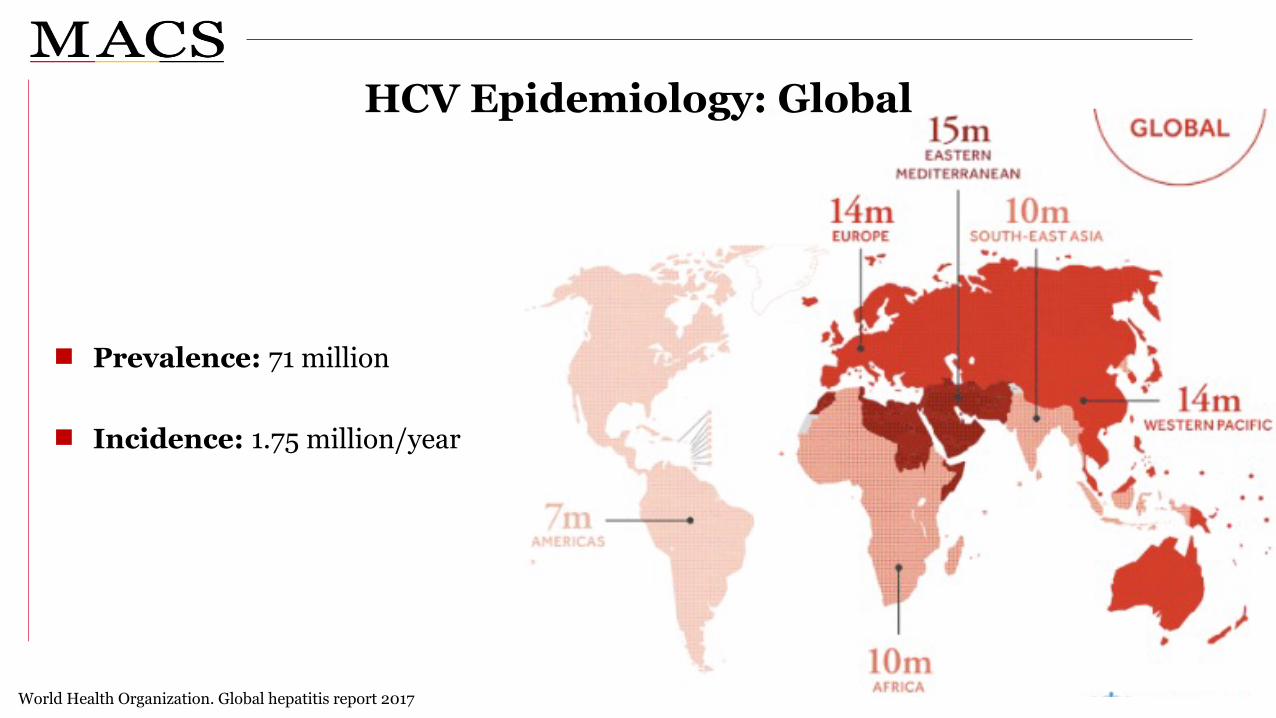
World Health Organization. Global hepatitis report 2017
HCV Epidemiology: Global
Prevalence: 71 million
Incidence: 1.75 million/year

HCV Epidemiology: US
3.7 million people HCV Ab+
Hep Vu

Incidence of Acute Hepatitis C by Year in the United States, 2006-2016
https://www.cdc.gov/hepatitis/statistics/2016surveillance/index.htm

Changing Epidemiology of HCV in the US
Male
Female
Mostly baby boomers
New
ly R
epor
ted
HC
V C
ases
, %
5
0 10 20 30 40
Age, Years
4
3
2
1
050 60 70 80 90 100
2007 (N = 41,037)
New
ly R
epor
ted
HC
V C
ases
, %
5
0 10 20 30 40
Age, Years
4
3
2
1
050 60 70 80 90 100
Male
Female
PWIDs: 20-40 years of age
2015 (N = 33,454)
https://www.cdph.ca.gov/Programs/CID/DCDC/CDPH%20Document%20Library/Converted_ChronicHCV_SurvRpt_Graphs.pdf.

Opioid Use Disorder Is Driving Acute HCV
HCV prevalence among PWID is estimated to be 70%−77%1
1. CDC. Surveillance for Viral Hepatitis—United States, 2015. https://www.cdc.gov/hepatitis/statistics/2015surveillance/pdfs/2015HepSurveillanceRpt.pdf. 2. Hagan H, et al. Am J Epidemiol.2008;168(10):1099-1109.
1 in 3 people who inject drugs acquires HCV infection in the first year of injecting2

HCV Cases Reported in Maryland by County
Hepatitis C Strategic Plan, Maryland Department of Health, 2019
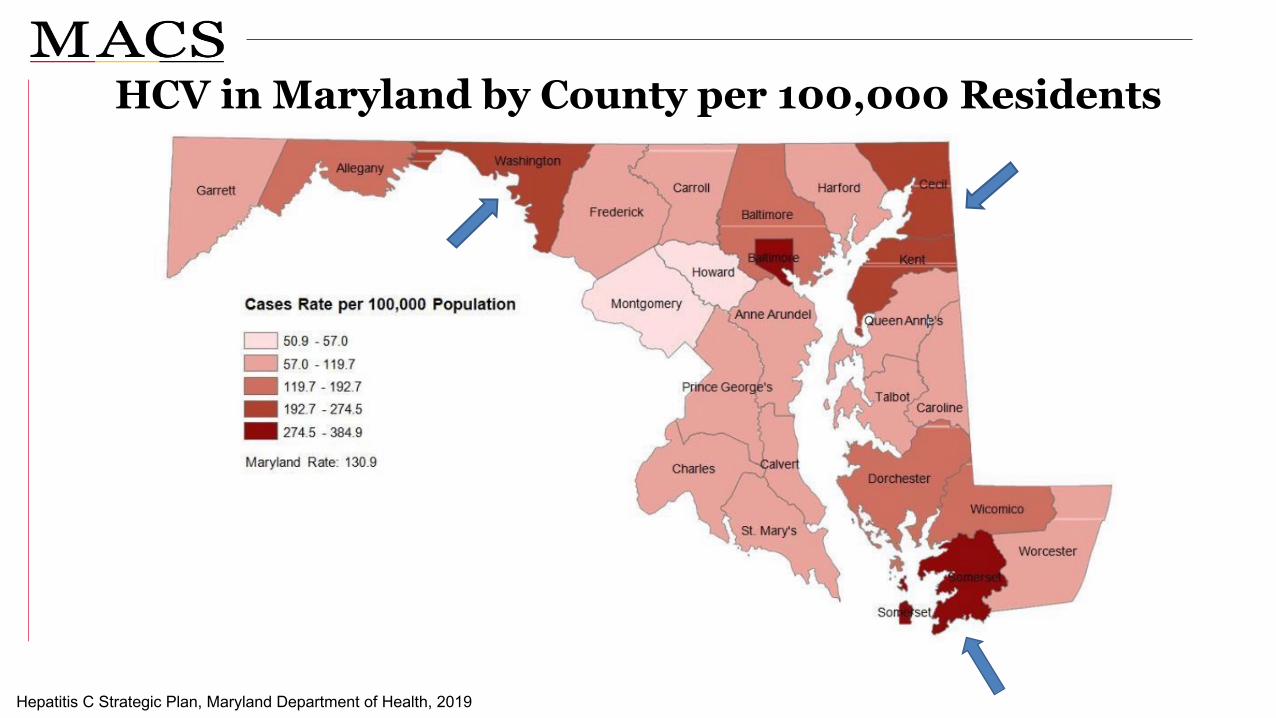
HCV in Maryland by County per 100,000 Residents
Hepatitis C Strategic Plan, Maryland Department of Health, 2019
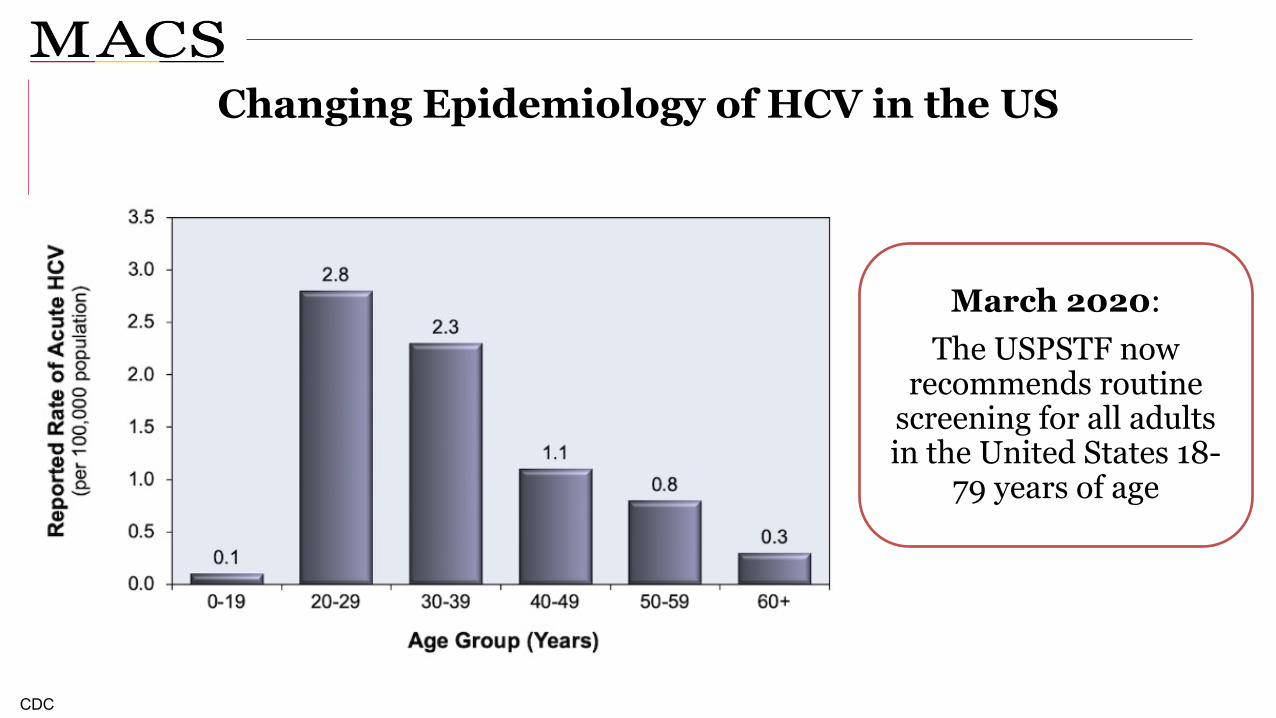
Changing Epidemiology of HCV in the US
CDC
March 2020: The USPSTF now
recommends routine screening for all adults in the United States 18-
79 years of age
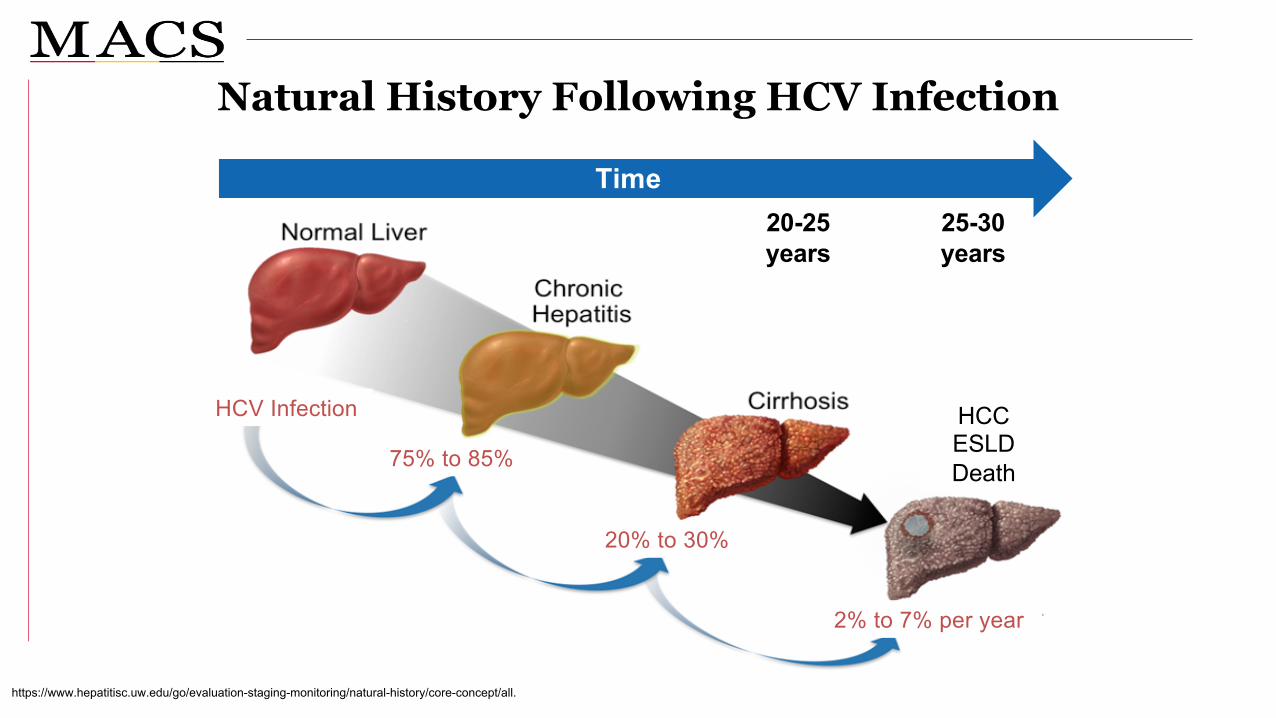
Natural History Following HCV Infection
https://www.hepatitisc.uw.edu/go/evaluation-staging-monitoring/natural-history/core-concept/all.
Time20-25 years
25-30 years
HCCESLDDeath75% to 85%
20% to 30%
2% to 7% per year
HCV Infection

Diagnosis, Treatment, and Monitoring
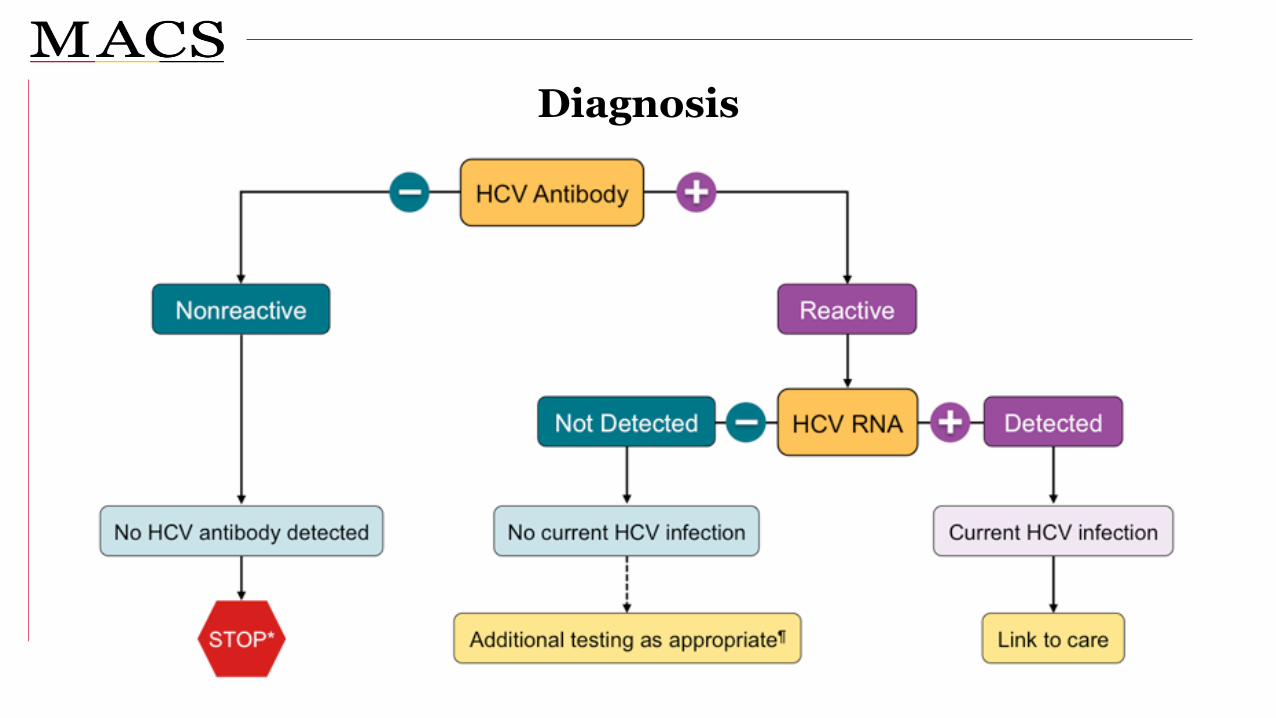
Diagnosis
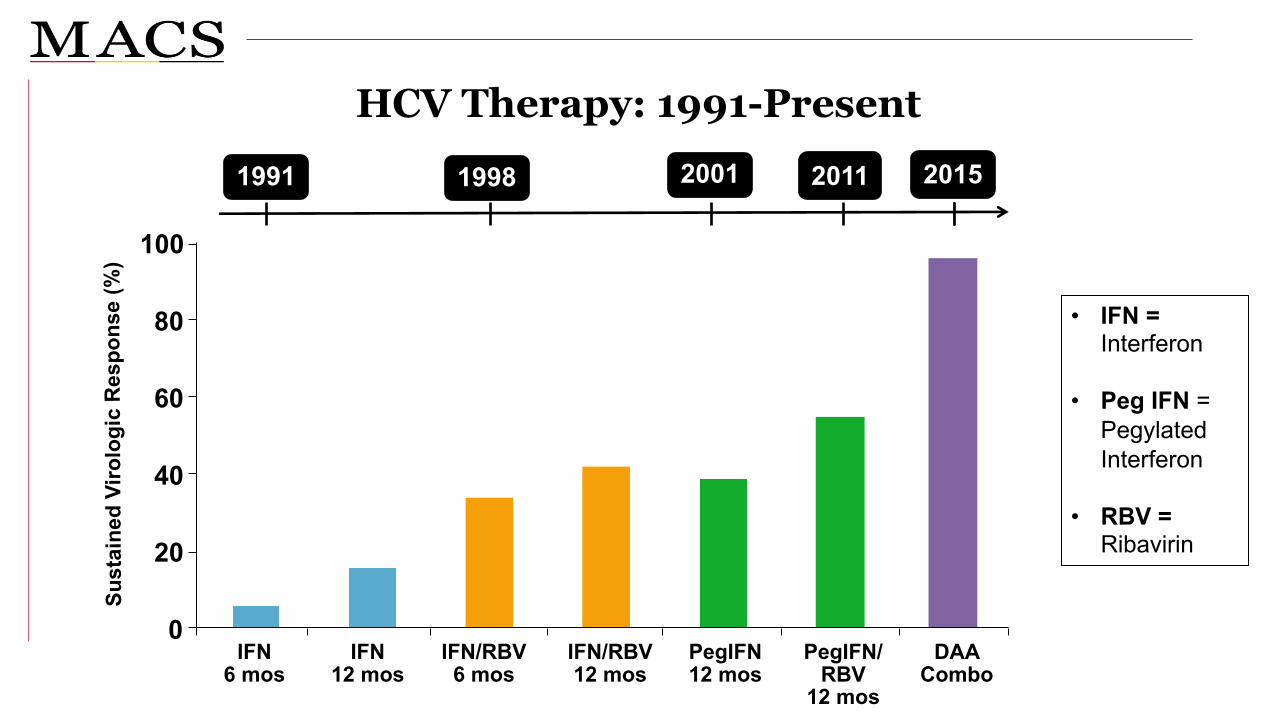
HCV Therapy: 1991-Present
• IFN = Interferon
• Peg IFN = Pegylated Interferon
• RBV =Ribavirin
Sust
aine
d Vi
rolo
gic
Res
pons
e (%
)
IFN6 mos
PegIFN/ RBV
12 mos
IFN12 mos
IFN/RBV12 mos
PegIFN12 mos
IFN/RBV6 mos
0
20
40
60
80
100
DAA Combo
200119981991 2011 2015
When and in Whom to Initiate HCV Therapy
https://www.hcvguidelines.org..
Treatment is recommended for all patients with chronic HCV infection
Rating: Class I, Level A

Rationale for HCV Treatment
Reduce decompensated liver disease/hepatocellular carcinoma
Reduce cirrhosis
Reduce transmission and progression
Cirrhosis
Intermediate stages of fibrosis
Early stages of fibrosis
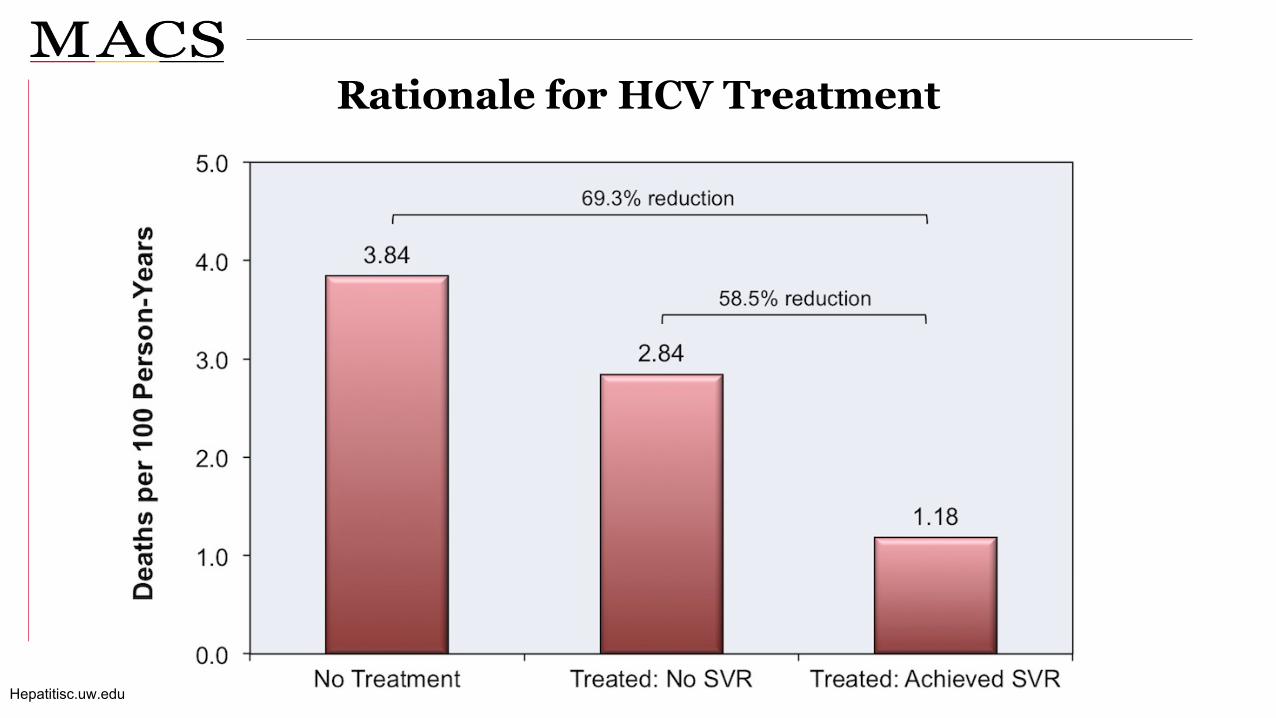
Rationale for HCV Treatment
Hepatitisc.uw.edu

Virologic Targets of Treatment
Hadgan, JAMA, 2011

HCV Treatment Regimens
https://www.hcvguidelines.org.
RegimenGenotype
1a 1b 2 3 4 5 6
Elbasvir/grazoprevir ü ü ü
Ledipasvir/sofosbuvir ü ü ü ü ü
Sofosbuvir/velpatasvir ü ü ü ü ü ü ü
Glecaprevir/pibrentasvir ü ü ü ü ü ü ü
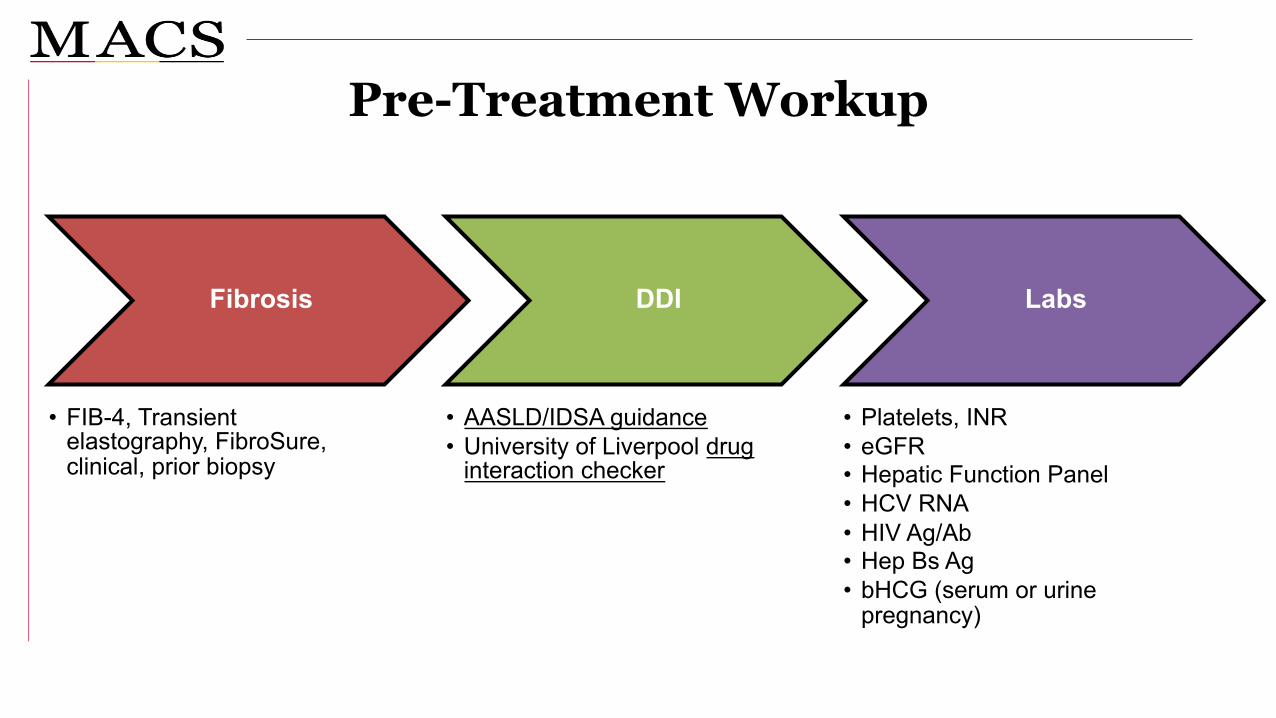
Pre-Treatment Workup
Fibrosis
• FIB-4, Transient elastography, FibroSure, clinical, prior biopsy
DDI
• AASLD/IDSA guidance• University of Liverpool drug
interaction checker
Labs
• Platelets, INR• eGFR• Hepatic Function Panel• HCV RNA• HIV Ag/Ab• Hep Bs Ag• bHCG (serum or urine
pregnancy)

“Simplified Treatment”
Do use in:• Treatment naïve• Non cirrhotic patients
Do not use in: • Known or suspected hepatocellular carcinoma• Prior liver transplantation• HBsAg positive• Current pregnancy• HIV positive

“Simplified Treatment” First-Line Agents
Glecaprevir (300mg)/Pibrentasvir (120mg)
Mavyret
Sofosbuvir (400mg)/Velpatasvir (100mg)
Epclusa
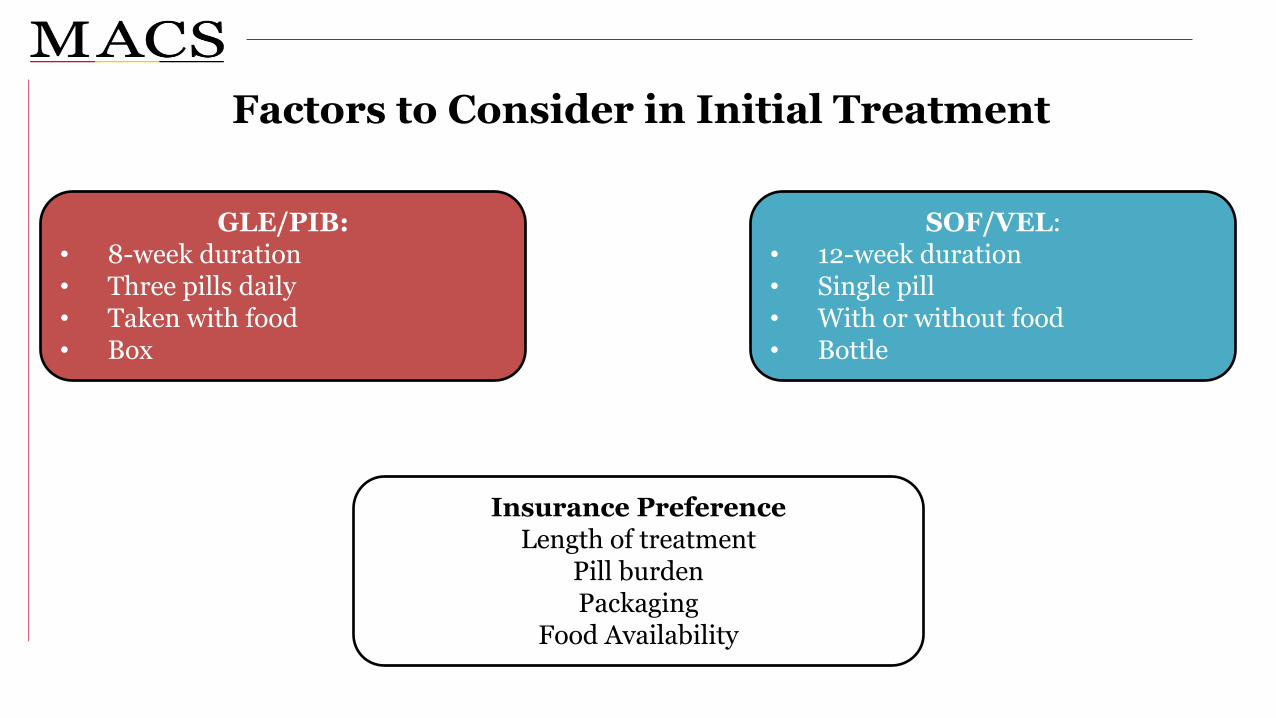
Factors to Consider in Initial Treatment
SOF/VEL: • 12-week duration• Single pill• With or without food• Bottle
GLE/PIB: • 8-week duration• Three pills daily• Taken with food• Box
Insurance PreferenceLength of treatment
Pill burdenPackaging
Food Availability

On Treatment Monitoring
• Check in in some way (phone, telemedicine, in person) at least once
• Ask about adherence
• Ask about common adverse events
• NO LABS NEEDED if everything is going smoothly
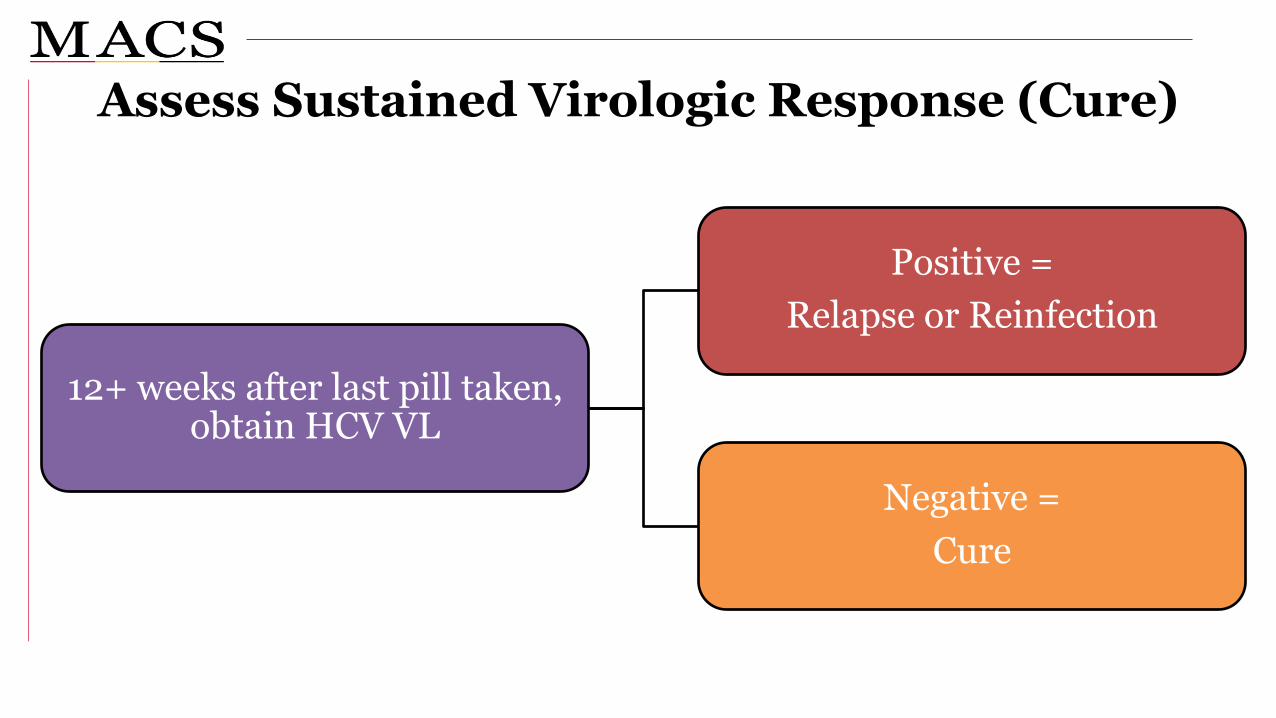
Assess Sustained Virologic Response (Cure)
12+ weeks after last pill taken, obtain HCV VL
Positive = Relapse or Reinfection
Negative = Cure
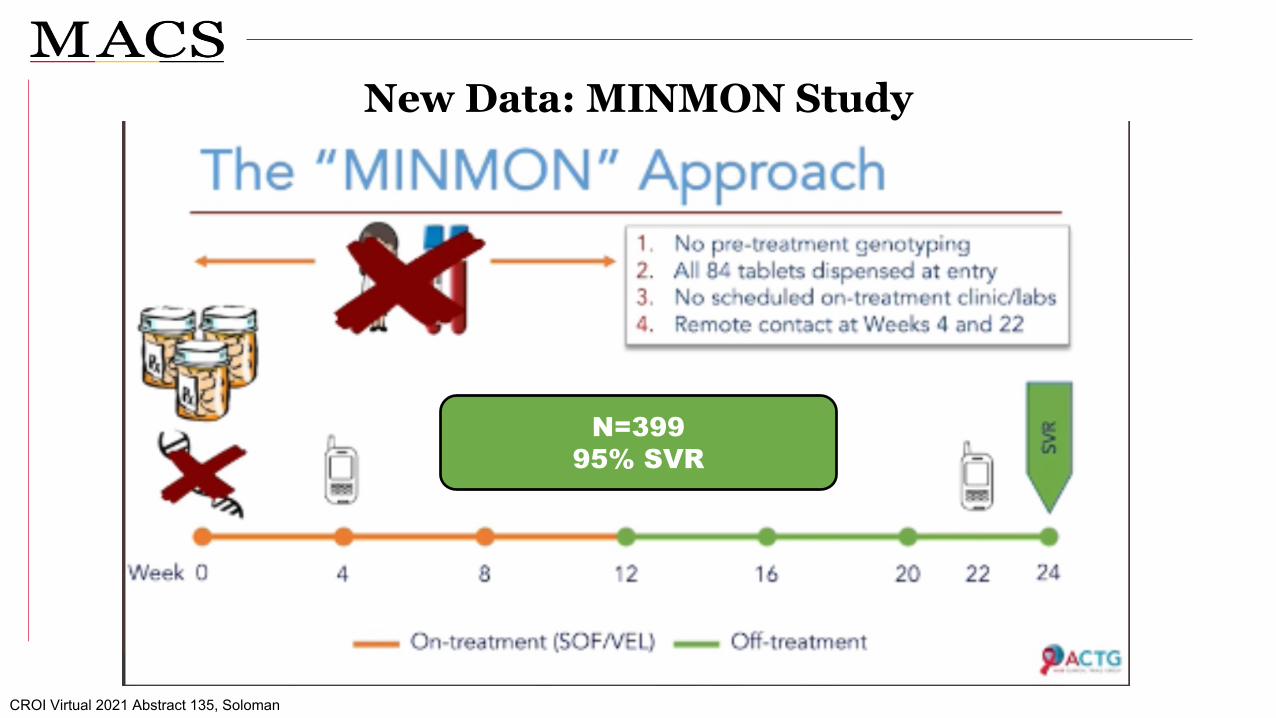
New Data: MINMON Study
N=39995% SVR
CROI Virtual 2021 Abstract 135, Soloman
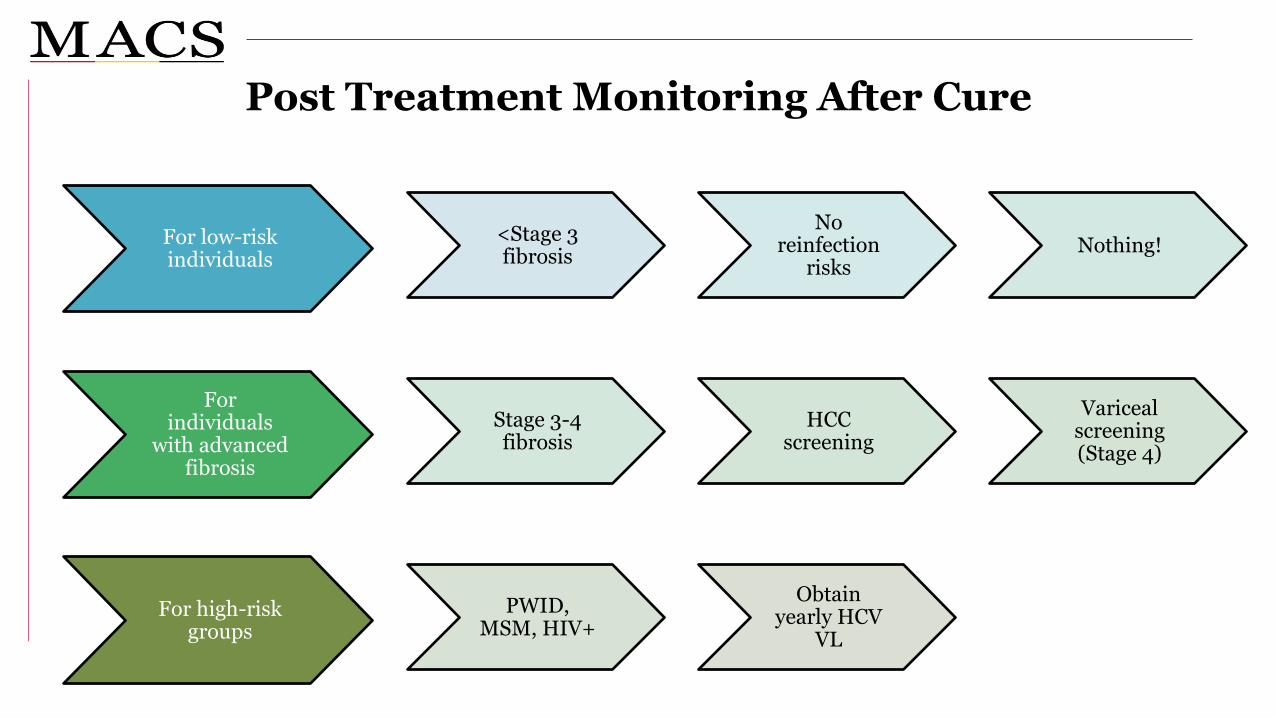
Post Treatment Monitoring After Cure
For low-risk individuals
<Stage 3 fibrosis
No reinfection
risksNothing!
For individuals
with advanced fibrosis
Stage 3-4 fibrosis
HCC screening
Variceal screening (Stage 4)
For high-risk groups
PWID, MSM, HIV+
Obtain yearly HCV
VL
Non-Cure: Definitions
Treatment Failure (Relapse)
• Detectable VL at SVR, of same genotype• Can be re-treated with alternative regimens
Reinfection
• Identified by a genotype switch• Can be treated as if initial infection
Non-Cure: Don’t Worry!
• >90% efficacy with re-treatment regimens• Address the initial cause of relapse
• Drug-drug interactions• Adherence• Life instability/challenges
Viral relapse will occur!
• Sign you are in the right population• Harm reduction is the key
Reinfection will occur!

Treatment in “Special” Populations
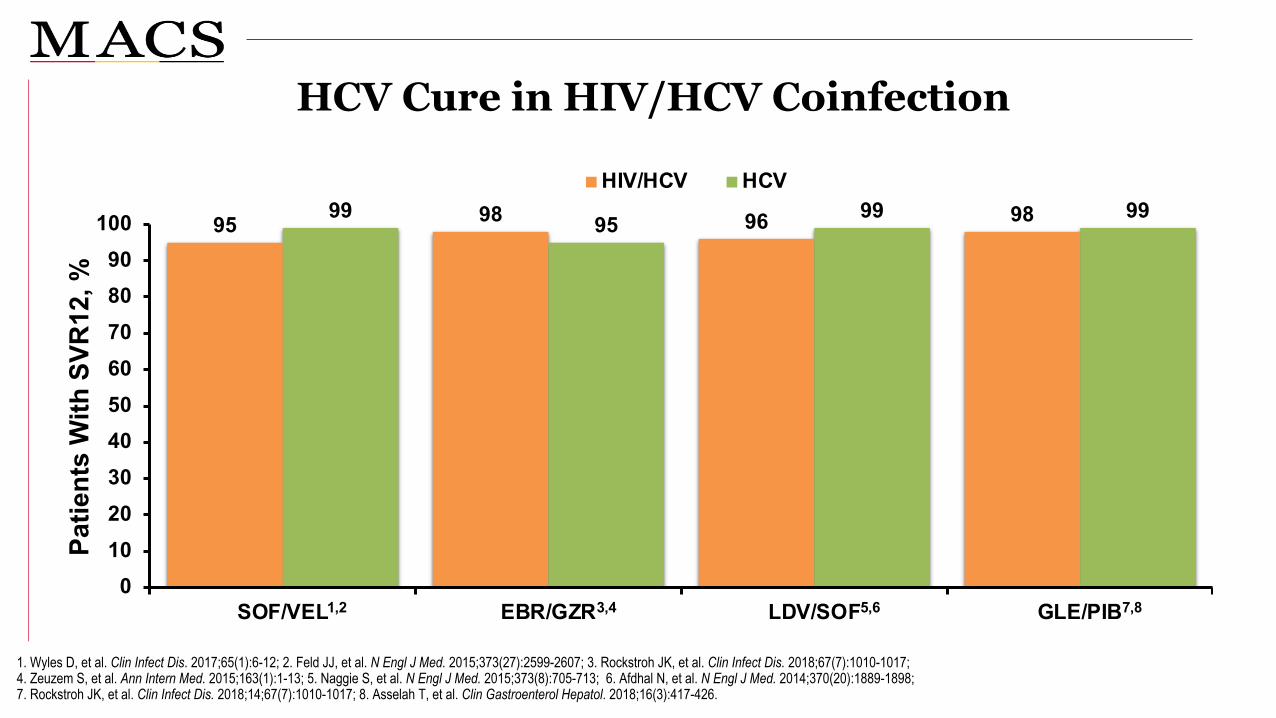
95 98 96 9899 95 99 99
0102030405060708090
100
SOF/VEL EBR/GZR LDV/SOF GLE/PIB
HIV/HCV HCV
Patie
nts
With
SVR
12, %
HCV Cure in HIV/HCV Coinfection
1. Wyles D, et al. Clin Infect Dis. 2017;65(1):6-12; 2. Feld JJ, et al. N Engl J Med. 2015;373(27):2599-2607; 3. Rockstroh JK, et al. Clin Infect Dis. 2018;67(7):1010-1017;4. Zeuzem S, et al. Ann Intern Med. 2015;163(1):1-13; 5. Naggie S, et al. N Engl J Med. 2015;373(8):705-713; 6. Afdhal N, et al. N Engl J Med. 2014;370(20):1889-1898; 7. Rockstroh JK, et al. Clin Infect Dis. 2018;14;67(7):1010-1017; 8. Asselah T, et al. Clin Gastroenterol Hepatol. 2018;16(3):417-426.
1,2 3,4 5,6 7,8
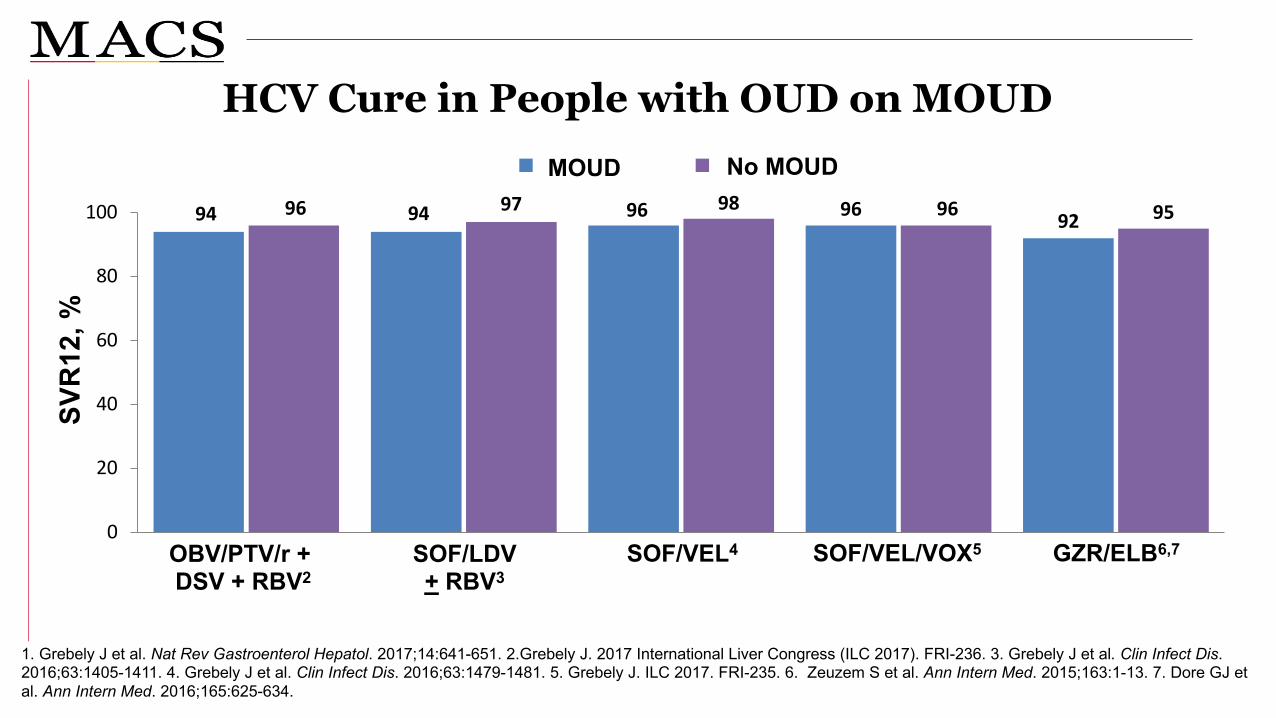
HCV Cure in People with OUD on MOUD
94 94 96 96 9296 97 98 96 95
0
20
40
60
80
100
OST no OST
OBV/PTV/r + DSV + RBV2
SOF/VEL/VOX5SOF/VEL4 GZR/ELB6,7SOF/LDV + RBV3
SVR
12, %
1. Grebely J et al. Nat Rev Gastroenterol Hepatol. 2017;14:641-651. 2.Grebely J. 2017 International Liver Congress (ILC 2017). FRI-236. 3. Grebely J et al. Clin Infect Dis. 2016;63:1405-1411. 4. Grebely J et al. Clin Infect Dis. 2016;63:1479-1481. 5. Grebely J. ILC 2017. FRI-235. 6. Zeuzem S et al. Ann Intern Med. 2015;163:1-13. 7. Dore GJ et al. Ann Intern Med. 2016;165:625-634.
MOUD No MOUD
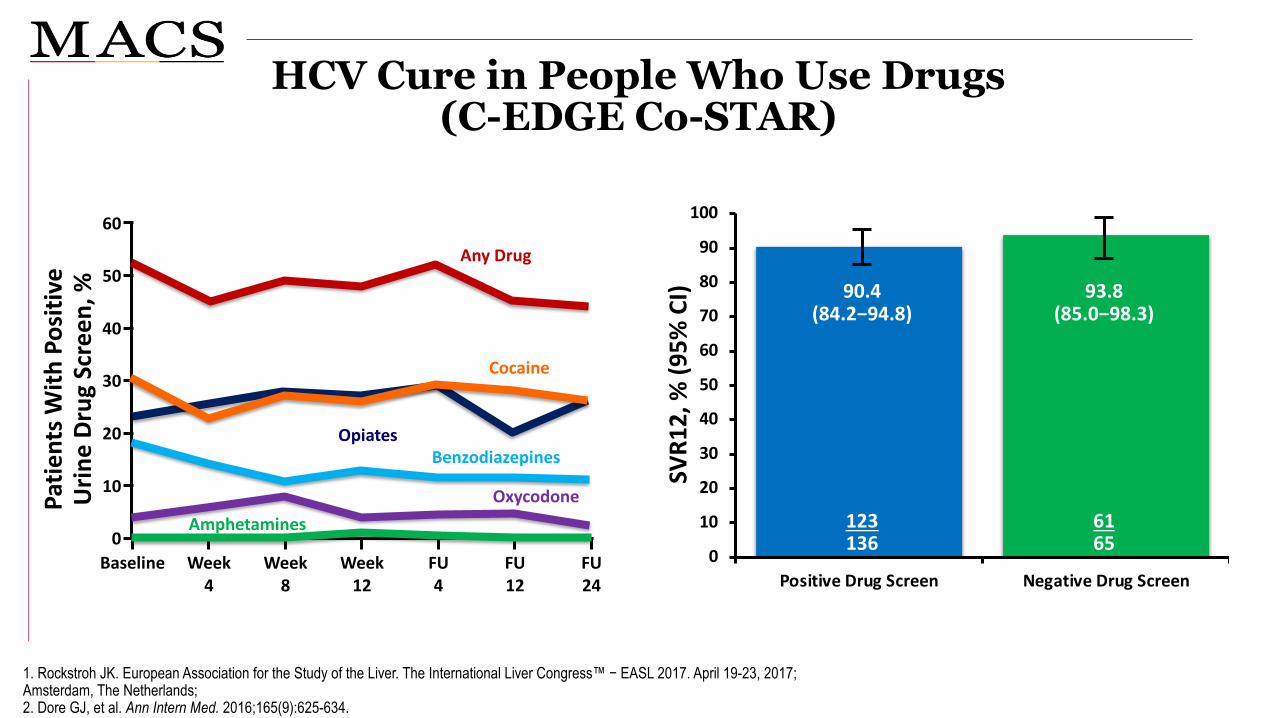
0
10
20
30
40
50
60
70
80
90
100
Positive Drug Screen Negative Drug Screen
SVR1
2, %
(95%
CI)
123136
6165
90.4(84.2−94.8)
93.8(85.0−98.3)
HCV Cure in People Who Use Drugs (C-EDGE Co-STAR)
1. Rockstroh JK. European Association for the Study of the Liver. The International Liver Congress™ − EASL 2017. April 19-23, 2017; Amsterdam, The Netherlands; 2. Dore GJ, et al. Ann Intern Med. 2016;165(9):625-634.
Patie
nts W
ith P
ositi
ve
Urin
e Dr
ug S
cree
n, %
60
Baseline
Any Drug50
40
30
20
10
0Week
4Week
8Week
12FU4
FU12
FU24
Cocaine
OpiatesBenzodiazepines
OxycodoneAmphetamines
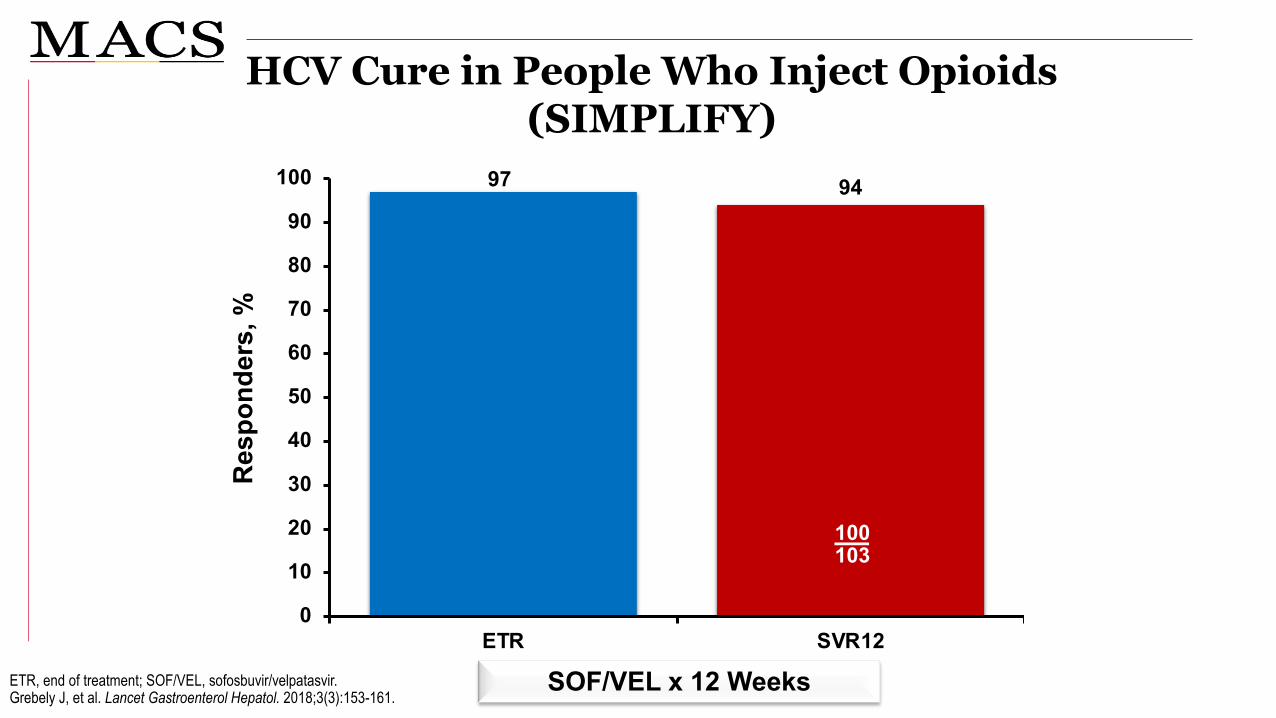
Res
pond
ers,
%
97 94
0
10
20
30
40
50
60
70
80
90
100
ETR SVR12
HCV Cure in People Who Inject Opioids(SIMPLIFY)
ETR, end of treatment; SOF/VEL, sofosbuvir/velpatasvir. Grebely J, et al. Lancet Gastroenterol Hepatol. 2018;3(3):153-161.
100103
97103
SOF/VEL x 12 Weeks

Challenges and Strategies in HCV Treatment
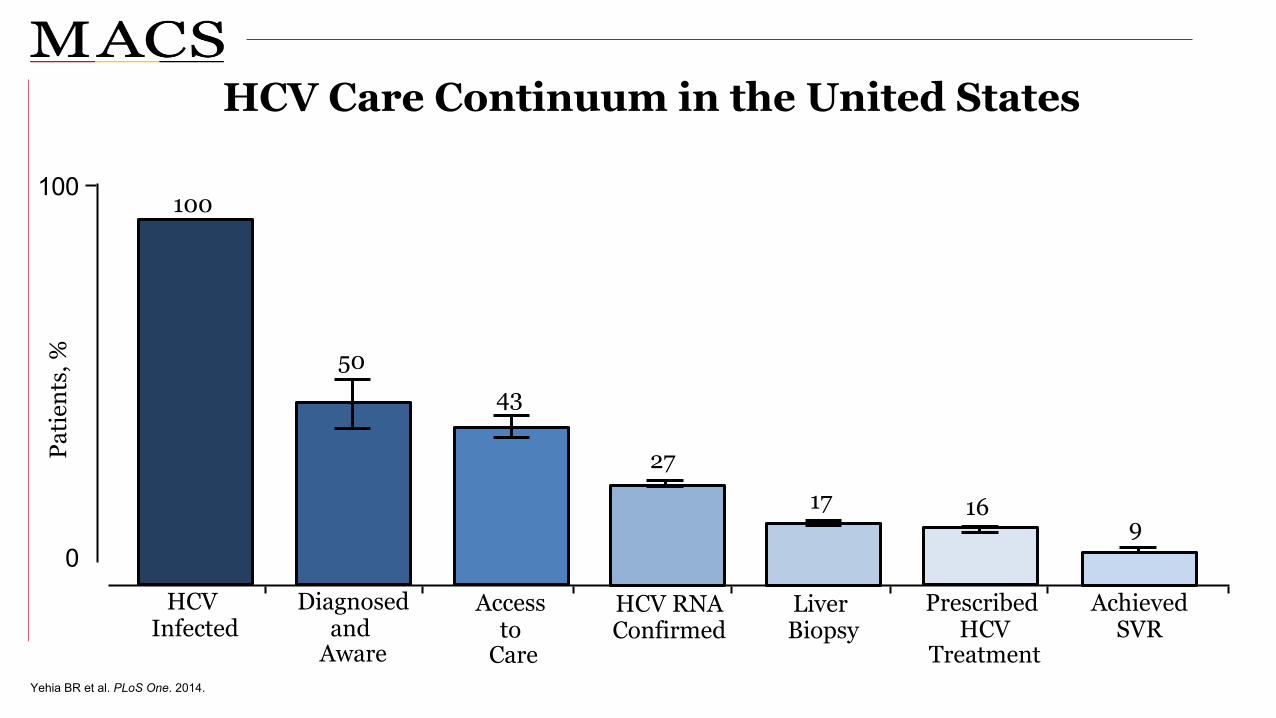
HCV Care Continuum in the United States
Yehia BR et al. PLoS One. 2014.
TimeTime
Patie
nts,
%
0
100
HCV Infected
Diagnosedand
Aware
Access to
Care
HCV RNAConfirmed
Liver Biopsy
Prescribed HCV
Treatment
AchievedSVR
100
5043
2717 16
9

• Insufficient number of providers who can treat HCV•Insufficient resources for case managers/social workers•Segregated service delivery•Cost of medications
Structural
•Provider knowledge of treatment guidelines•Provider knowledge of harm reduction•Patient–provider interactions•Provider reticence to treat PWID
Provider
•Limited knowledge about long-term consequences of HCV•Asymptomatic disease•Fear of side effects•Competing health and social priorities
Patient
HCV Treatment Barriers
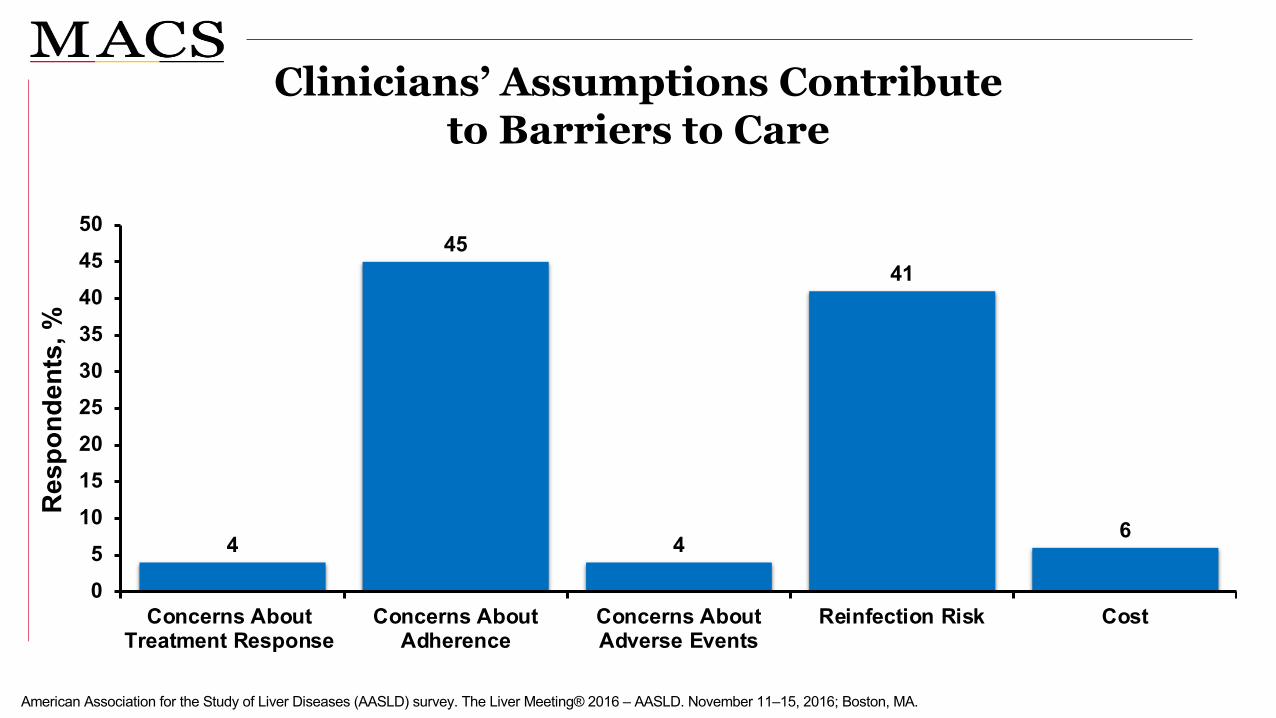
Clinicians’ Assumptions Contribute to Barriers to Care
American Association for the Study of Liver Diseases (AASLD) survey. The Liver Meeting® 2016 – AASLD. November 11‒15, 2016; Boston, MA.
4
45
4
41
6
05
101520253035404550
Concerns AboutTreatment Response
Concerns AboutAdherence
Concerns AboutAdverse Events
Reinfection Risk Cost
Res
pond
ents
, %

Principles to Improve the HCV Care Continuum
Incorporate Harm
Reduction Framework
Collocate Services
Decentralize Services
Disregard for the disease model of addiction
Misconceptions about MOUD
Criminalization of substance use disorder
Addressing Stigma and Discrimination

Harm Reduction Framework
Slide courtesy of PeerView/Rachel McClean MPH
Streets, encampments,and freeway overpasses
Shelters and residential drug treatment programs
Methadone clinics/opiate treatment programs
Syringe services programs
Harm Reduction Framework
Multiple phone numbers(cell, friends, family)
Social media accounts (if OK to contact)
Programs, shelters, food pantries
Hangouts, sleeping spots

Collocate Services: Linkage and Retention
Slide courtesy of PeerView/Rachel McClean MPH
Pay-as-you-go phones
Appointment reminders and multiple opportunities for reengagement
Transportation, accompaniment, and advocacy
Benefits and insurance enrollment
Help getting IDs
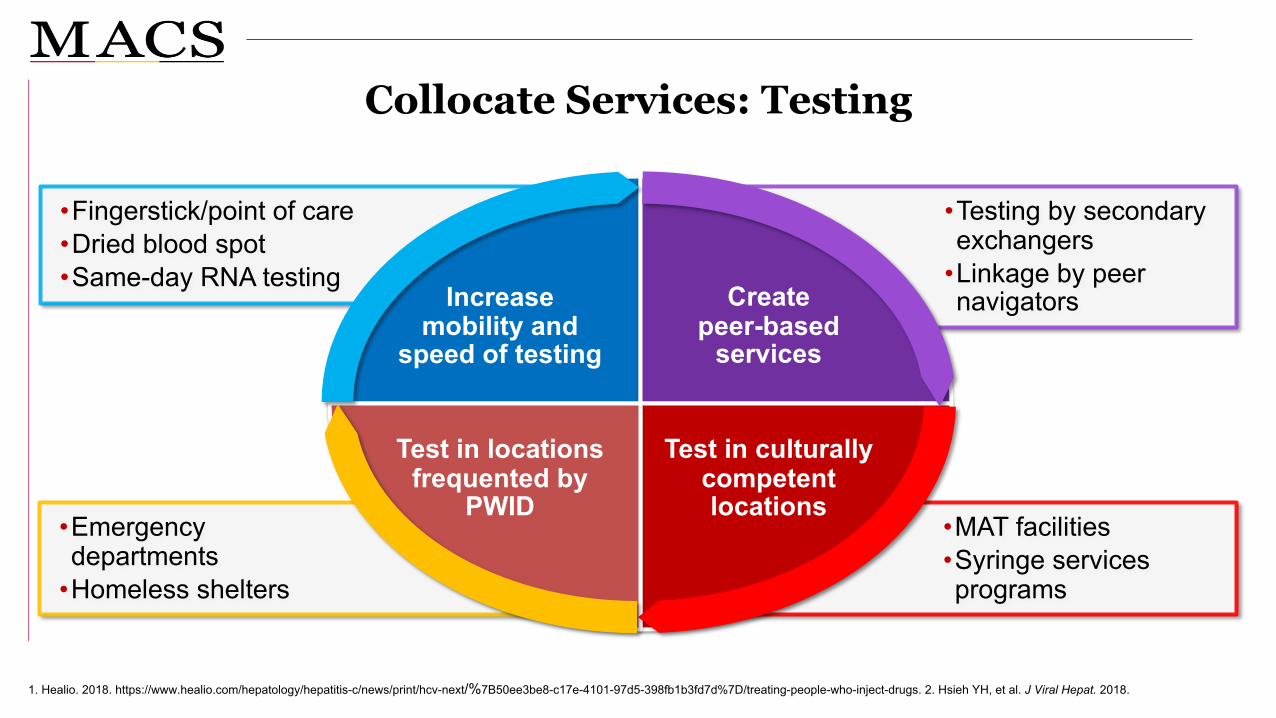
Collocate Services: Testing
1. Healio. 2018. https://www.healio.com/hepatology/hepatitis-c/news/print/hcv-next/%7B50ee3be8-c17e-4101-97d5-398fb1b3fd7d%7D/treating-people-who-inject-drugs. 2. Hsieh YH, et al. J Viral Hepat. 2018.
•MAT facilities•Syringe services programs
•Emergency departments
•Homeless shelters
•Testing by secondary exchangers
•Linkage by peer navigators
•Fingerstick/point of care•Dried blood spot•Same-day RNA testing
Increase mobility and
speed of testing
Createpeer-based
services
Test in culturally competent locations
Test in locations frequented by
PWID

Collocate Services: TreatmentANCHOR Study
D, day; HIV, human immunodeficiency virus; PrEP, HIV preexposure prophylaxis; OAT, opioid agonist therapy; PWID, people who inject drugs; SOF, sofosbuvir; SVR12, sustained virologic response at ≥12 weeks after end of treatment; VEL, velpatasvir; W, week.Rosenthal ES, et al. Clin Infect Dis. 2020 (Epub ahead of print).
SOF/VEL Monitor for HCV reinfection
Buprenorphine (optional)
Risk-taking behavior assessment
D0
W4 W12
W24
W48
W72
W96
PrEP (optional)
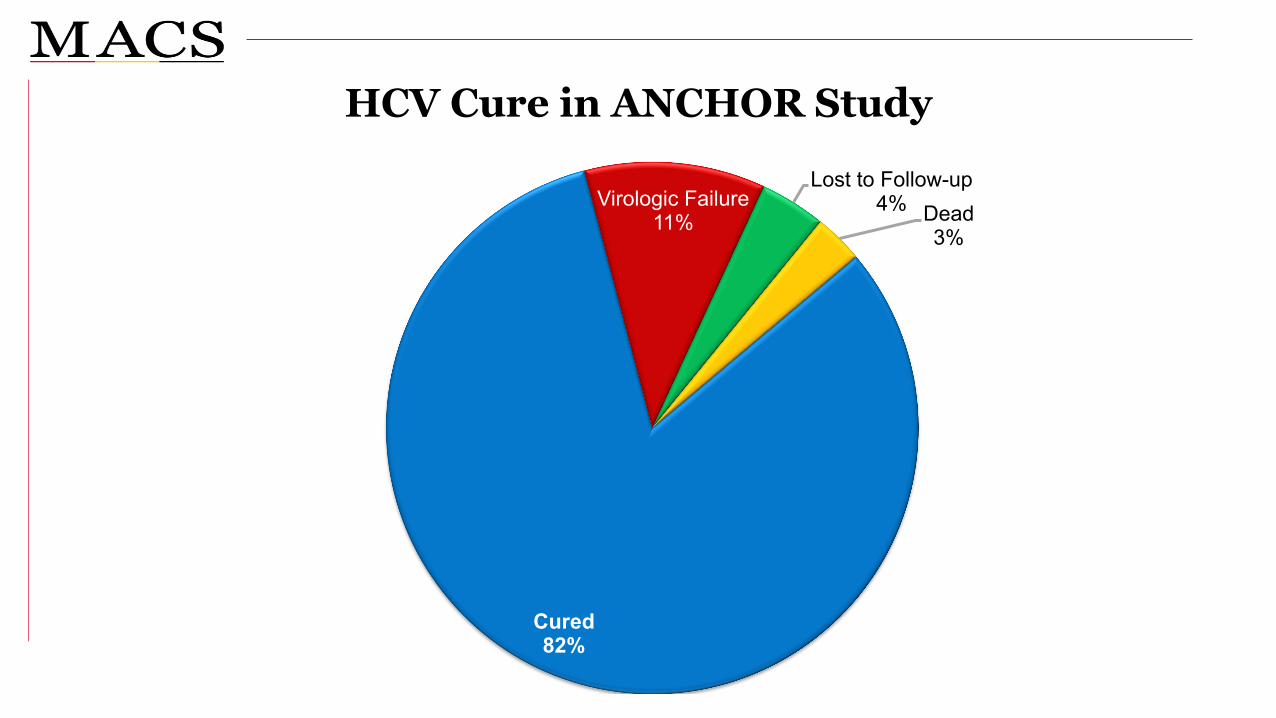
HCV Cure in ANCHOR Study
Cured82%
Virologic Failure11%
Lost to Follow-up4% Dead
3%
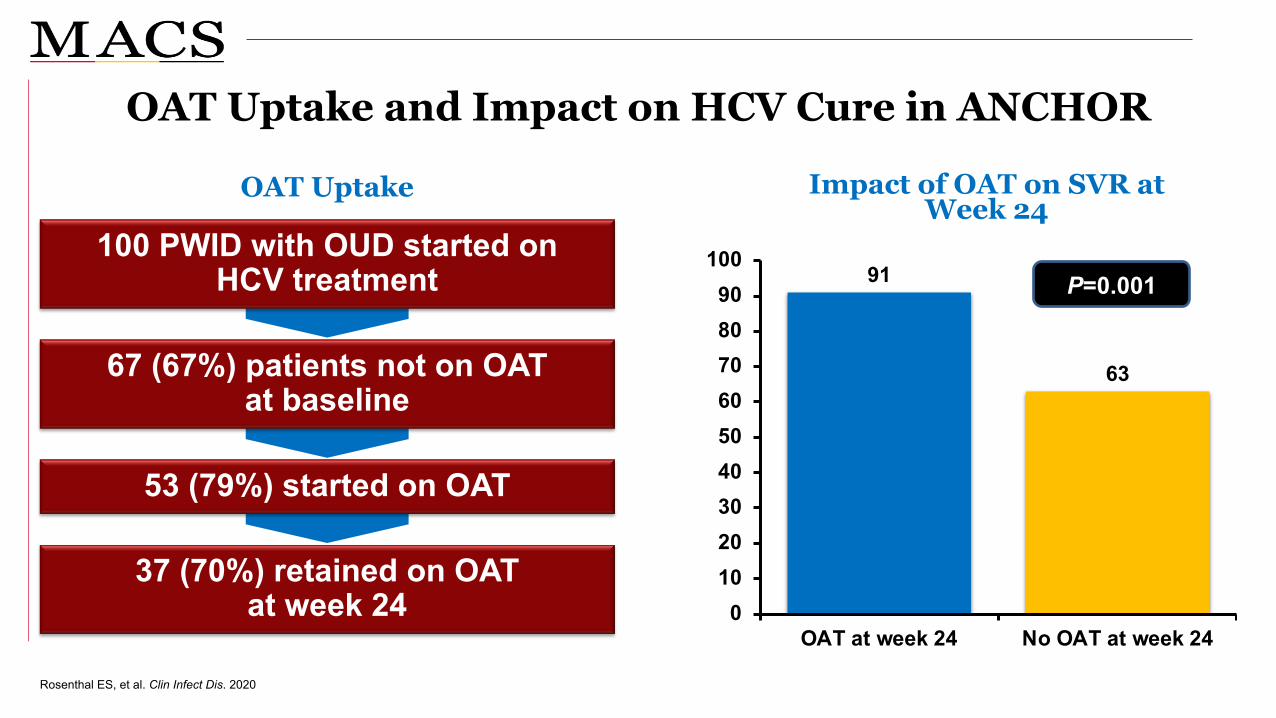
OAT Uptake and Impact on HCV Cure in ANCHOR
OAT Uptake Impact of OAT on SVR at Week 24
Rosenthal ES, et al. Clin Infect Dis. 2020
91
63
0102030405060708090
100
OAT at week 24 No OAT at week 24
P=0.001
37 (70%) retained on OAT at week 24
53 (79%) started on OAT
67 (67%) patients not on OAT at baseline
100 PWID with OUD started on HCV treatment

Providers
Task shifting to• Specialists• Drug and alcohol specialists• Primary care providers • Nurses• Pharmacists• Peer support workers• Others
Decentralize Treatment
1. Akiyama M, et al. Ann Intern Med. 2019;170(9):594-603; 2. Beste LA, et al. Am J Med. 2017;130(4):432-438 e3; 3. Morey S, et al. J Viral Hepat. 2019;26(1):101-108.
Settings
Drug andalcohol clinics
Primary care clinics
Prisons
FQHCsSSPSexual health clinics
Pharmacies

Decentralize Treatment: ASCEND Study
All patients, ITT (P=0.19) All patients, per protocol (P<0.49) Cirrhosis, per protocol (P=0.69)
0
20
40
60
80
10091%
87%92%
Overall
93%
NP PCP Specialist
92%94% 95% 95%86% 89% 86% 83%
513600
513548
99109
135151
135142
2630
138160
138146
2527
240289
240260
4852
SVR
12 (%
)
Kattakuzhy S, et al. Ann Intern Med. 2017;167:311-318.
No difference in SVR of HCV treatment provided by NP, PCP, and specialist providers after a targeted 3-hour training

Key Points
• Hepatis C incidence is rising due to the epidemic of opioid use disorder
• All adults 18+ should be screened for HCV
• Initial treatment of HCV in non-cirrhotic patients is straightforward
• Primary care providers can and should treat HCV
• Improving care for patients with OUD and HCV requires a harm reduction framework, collocation, and decentralization
• The syndemic framework of care will improve outcomes across diseases

Thank [email protected]