Embed Size (px)
Citation preview

447
THE SURGERY OF THE THYROID GLANDVICTOR H. RIDDELL, M.A., M.D., F.R.C.S.
St. George's Hospital, London, S. W. I
The surgery of the thyroid gland is describedas it applies to simple goitre, toxic goitre andmalignant goitre. Particular attention is paid tothe contraindications for surgery.
SURGERY IN SIMPLE GOITREThe Solitary NoduleThe apparently solitary swelling, clinically and
colloquially referred to as a ' simple adenoma,'may histologically be a hyperplastic nodule (due tocompensatory hyperplasia) or a neoplastic nodule(innocent or malignant).The management of the solitary nodule is
influenced in some hands by the availability ornot of 131I facilities for investigation.131I Facilities Not Available
It is impossible to distinguish with certainty, byclinical methods alone, the hyperplastic nodulefrom the neoplastic. It is for this reason that-given these circumstances-the removal of anysolitary symptomless swelling in the thyroid isadvised.
It is generally agreed that the solitary noduleshould not be treated by simple enucleation butby resection of the affected lobe. There is lessgeneral agreement about the management of thecontralateral lobe. It is known that a large hyper-plastic nodule is rarely, if ever, truly solitary, butthat there are numerous minute areas of focalhyperplasia scattered throughout both lobes.'0Removal of the affected lobe only is followed in aproportion-a small proportion-by the appear-ance of a nodule on the opposite side. It isagreed that the incidence of this occurrence canbe reduced by performing a subtotal thyroidec-tomy in all cases of apparently unilateral simplegoitre. A contrary point of view, which I believeto be the more reasonable practice, is to performlobectomy on the side of the swelling, to palpatethe opposite side to exclude a palpable nodule ornodules and to do no more surgically if thecontralateral lobe feels normal.
If it is true that a low level of circulating thyroidhormone is responsible for triggering off themechanism of anterior pituitary stimulation, in-creased TSH production, thyroid focal hyper-
plasia-then it is illogical further to reduce thy-roxin production by removing a substantial part ofthe remaining lobe. Strong additional support isgiven to this restricted surgical attack in the caseof the solitary nodule (i) by the low rate of sub-sequent nodular involvement of the contralaterallobe, (2) by the greater morbidity of the bilateralas compared with the unilateral operation, and(3) by the experience that postoperatively thecontinued growth of any remaining impalpablethyroid nodules may be discouraged by the ad-ministration of thyroid extract (I20 mg. daily)or of 1-thyroxine sodium (0.3 mg. daily).
131I Facilities Are AvailableAttempts have been made to determine the
innocence or malignancy of a nodule by 131Iuptake examinations. If the nodule fails to takeup the isotope-the so-called ' cold' nodulethere is a strong probability that it is a carcinomaor other tumour. Immediate surgery must becarried out and the nodule pathologically identi-fied. If the nodule takes up 131I in greateramount than the rest of the gland-the so-called' hot' nodule-it is unlikely to be a carcinoma.In these circumstances it is probably justifiable towithhold surgery temporarily. A test course ofthyroxin should be given for a period not exceed-ing three months: if at the end of this time thenodule has not disappeared or become appre-ciably smaller, removal and pathological identi-fication must be advised. The possibility of adeeply placed carcinoma surrounded by a thicklayer of normal thyroid tissue giving rise to afalse interpretation must be borne in mind.
Smooth Diffuse GoitreThe smooth diffuse type of goitre occurs in
two forms: (a) As a physiological response to alack of iodine-puberty goitre-this is a reversibleprocess in which the gland may return to normalwhen the stress passes; and (b) as a pathologicalresponse to a lack of iodine such as occurs inendemic goitrous areas where the process tendsto be progressive.The puberty goitre should not be operated
E I
copyright. on July 13, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.417.447 on 1 July 1960. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
upon but treated with thyroid medication. Theendemic variety of smooth diffuse goitre shouldbe similarly treated while it remains small andshould only be operated upon for reasons of sizeor pressure.
Nodular Diffuse GoitreBilateral nodular goitres with marked bossing,
or if causing pressure symptoms or trachealdeviation or compression, should be treated bysubtotal thyroidectomy followed post-operativelyby the administration of thyroid either in theform of the dried extract or as 1-thyroxine sodium.When there are advanced degenerative changes inthe gland it is my practice to leave the inferiorthyroid artery untied on the side exhibiting mostnormal thyroid tissue.When the ' nodularity' is not marked and
amounts to no more than a mild asymmetry ofthe lobes-if there are no pressure symptoms, nohistory of recent increase in size and no trachealdeviation or compression, the patient should betreated conservatively with 1-thyroxine, particu-larly if elderly. The possibility of this type ofgland being in fact the site of carcinoma orlymphadenoid goitre must always be borne inmind, and if there is any doubt biopsy should becarried out, preferably with a fast-moving drillmotivated by compressed air.
Recurrent Nodular Goitre (Non-toxic)Regeneration of thyroid tissue may occur after
the subtotal operation. If this regrowth occurs onone side only scanning may show that it is theonly remaining functioning thyroid tissue in theneck so that its preservation and not its removalshould be the clinician's concern. In all cases ofrecurrent non-toxic nodular goitre, even if theregrowth is considerable, re-operation should beentertained with the greatest caution and onlythen after checking the integrity of the recurrentlaryngeal nerves by laryngoscopy.
The Recurrent Laryngeal NervesThe recurrent laryngeal nerves are most liable
to injury in the operation for bilateral nodulargoitre. Outlying nodules may burrow beneaththe recurrent laryngeal nerve so that in this typeof case its identification is essential-if it is to bepreserved.
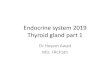
Pre-operative LaryngoscopyPre-operative laryngoscopy occasionally reveals
unsuspected paralysis of a vocal cord (Fig. i).Such a discovery may influence the surgeon'sdecision to operate and exonerate him if symp-toms develop post-operatively. The examinationis of particular importance in patients who have
FIG. i -Pre-operative laryngoscopy. This has revealedan abductor paralysis of the right vocal cord;patient had a normal speaking voice at conver-sational distance.
had a previous operation on the thyroid gland, orif thyroid carcinoma, chronic thyroiditis, or myx-oedema is suspected.
Preferential Abductor ParalysisThe abductor fibres seem to be more prone to
paralysis than the adductor. The view that theabductor fibres occupy a circumferential super-ficial position in the recurrent laryngeal nerve orthat the abductor fibres are separately groupedin one of the two terminal branches of the nerve hasbeen disproved in man by Sunderland and Swaney,9and their paper should be studied as a model ofthis type of intraneural topographical research.
There seems to be no purely anatomical basisupon which a satisfactory explanation of thepreferential paralysis of the abductors can bebased. It only remains to postulate that theabductor elements have a lower resistance toinjury, or that an unknown factor operates peri-pherally within the muscles. The evolutionarytheory of Negus5 seems the most rational. Hepoints out that the larynx is guarded by twogroups of muscles: a primitive protective sphinc-teric group (the adductors) and a dilator group(the abductors) essentially associated with themuch more recently developed vocal function ofthe larynx. He believes that it is reasonable to
UY-lyI 960448copyright.
on July 13, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.36.417.447 on 1 July 1960. D
ownloaded from

RIDDELL: The Surgerv of the Tzyroid Gland
expect that the vital protective function of thesphincteric group should give this group a greatervitality and the ability to survive over the morerecently evolved dilator group.
Post-operative LaryngoscopyPost-operative laryngoscopy is essential for a
true estimate of the frequency of vocal-corddamage due to thyroidectomy. Vocal-cord para-lysis following thyroidectomy is commoner thanis supposed. Existing statistics tend to be basedon the selective post-operative examination ofpatients who have some obvious symptom ofdamage to a recurrent laryngeal nerve, e.g. ahoarse voice. But this does not reveal those caseswhere compensatory readjustment of the unpara-lysed cord has produced a normal speaking voiceat conversational distance. Such cases are plentifuland may be wrongly assumed not to have sufferedany damage to a recurrent laryngeal nerve. More-over, an injury rate calculated on only a proportionof the patients operated on can be applied to thatproportion only.
Laryngoscopy within the theatre, immediatelyafter thyroidectomy while the patient is stillanaesthetized, can also be misleading. If thevocal cords are seen to abduct and adduct nor-mally it can be assumed that there has been noinjury to the recurrent laryngeal nerves; but, ifmovement is impaired, it should not be taken asproof that a nerve has been injured, because insome cases pressure on the vocal cords by theintratracheal tube may temporarily limit adduc-tion or abduction and in other cases the depth ofanaesthesia may prevent normal movement of thecords.
Post-operative laryngoscopy should not be donetoo soon after the operation or it will be uncom-fortable for the patient; furthermore, the findingscannot be accurately assessed at this early stage.Our practice is to do post-operative laryngoscopyon the day before the patient is due to be dis-charged. The throat is sprayed with 400 ligno-caine (this has not produced any unfavourablereactions in our experience) and after threeminutes the larynx is ready for examination.After the examination the patient is instructednot to eat anything for the next two hours, i.e.until laryngeal sensation has returned.
IdentificationSurgeons are either ' identifiers' or ' non-
identifiers.' The non-identifiers take the viewthat the deliberate exposure of the recurrentlaryngeal nerves by dissection is likely to producemore palsies from handling than if they are leftundisturbed and unidentified.The ' identifiers ' argue that modern anesthesia
and the antithyroid drugs have removed theurgency for speed in operating on the thyroidgland and so allow the operator time for an un-hurried search for the recurrent laryngeal nervesin a field which should be bloodless.A third course which lies between the two ex-
treme views is for the surgeon to improve hisknowledge of the local anatomy by exposing therecurrent laryngeal nerves on a limited number ofoccasions and thereafter to revert to the blindoperation with the added safety which his experi-ence will have given him.
Sites of InjuryThe sites of greatest vulnerability of the nerve
are as follows:(i) At the lower pole of the thyroid gland-the
nerve may be included in the ligature of theinferior thyroid veins. This accident can happenvery readily, particularly if a mass ligature isused for securing the veins.
(2) At the upper pole of the thyroid gland-justbefore the nerve enters the larynx, although Ibelieve this to be uncommon. Injury at this siteis most surely avoided by a clean exposure of thesuperior thyroid vessels, which should be tiedand divided as a pedicle and not through theglandular tissue of the superior pole by the clip-and-cut method.
(3) On the lateral surface of the thyroid gland-the nerve may be injured by marker forcepsplaced there before its resection or simply byexcessive traction or rough handling. It is prob-ably most liable of all to injury when the cutsurface of the gland is being resutured. Unlessspecial care is taken the nerve may be picked upand included in the suture if the needle is insertedinto the gland remnant too far posteriorly.
Haemorrhage is the agent which prepares theconditions most favourable to injury at all sites.
VZisual IdentificationThe identification of the recurrent laryngeal
nerve does not require its naked exposure as inan anatomical display specimen. It is wrong andunnecessary to dissect out or to strip the recurrentlaryngeal nerve of its ensheathing fascia. Byopening up the tissues lying to its outer side thenerve can be clearly demonstrated and identifiedwithout ever touching it with an instrument.The nerve is first sought for and is most readilyfound, where it comes into relation with theinferior thyroid artery. In other words, it shouldnot be looked for in the lower part of the wound-the root of the neck-where it bears away fromthe side of the trachea and oesophagus, or in theupper part of its course where it is covered andpartly obscured by strong fascia. It is recognized
7uly I 960 449copyright.
on July 13, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.36.417.447 on 1 July 1960. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
also by the minute vein which runs upon itssurface. The operation must be done gently,because the nerve is readily damaged by stretchingif too much traction is exerted on the thyroidgland, a mistake which is particularly likely to bemade when the thyroid lobe is unusually mobile.
Identification by PalpationThe visual method of exposure is not always
wise or expedient. In such cases, with experience,the nerve can be identified in a high proportionof patients by palpation. It feels like a cord or athrombosed vein which can be gently rolledagainst the trachea. Identification by touch cannot,however, for comparative statistical purposes, beaccepted as being as accurate a method of identi-fication as the visual.
Transient and Permanent ParalysisThe word 'transient '-to imply temporary
palsy of a recurrent nerve-should be used spar-ingly and only if full recovery of movement of thevocal cord is subsequently objectively confirmedby laryngoscopy as well as subjectively by areturn of the voice to normal tones. Fortunately,the palsy is more often transient than permanent-12 out of 22 cases of unilateral palsy.6
SummaryThe production of a bilateral abductor palsy of
the cords following thyroidectomy is a grave sur-gical injury. The young surgeon starting thyroidsurgery should arm himself and protect his patientby deliberately identifying the recurrent nerve inhis first 25 or 30 operations. It is a tediousapprenticeship, for it is easier not to do so, butthereafter with this solid anatomical experienceto draw upon he will automatically become asafer operator in the neck and can reasonablyrevert to the blind operation in uncomplicatedcases. It is wise to continue to identify the nerveon one side, by palpation or visually, in all bilateraloperations (total or subtotal thyroidectomy).
SURGERY IN TOXIC GOITREIf the surgeon is to be something more than a
technician who is called in to perform the opera-tive procedure two pre-requisites are necessary.
Firstly, the surgeon must make it his businessto be as familiar as is a physician with the medicalaspects of management, particularly with theeccentricities and potentialities of the antithyroiddrugs. These drugs, if properly used, can easethe achievement of a euthyroid state and by sodoing ensure that the patient is brought to a safeoperative level-if misused they can complicatethe pre-operative phase and make the operationitself one of the most difficult in surgery.
Secondly, the surgeon must make a point ofseeing the patient in her original thyrotoxic state,that is, at her worst, and before therapy isinitiated. If seen for the first time when an anti-thyroid effect has been obtained, an entirely falseassessment of the severity of the disease may bearrived at and a wrong decision made as to theneed or time for operative treatment.
Since 1311 is contraindicated in the treatment ofpatients under the age of 45 because of its un-known carcinogenic potential, it is convenient todescribe separately the choice of treatment as itapplies to patients below the age of 45.
Thyrotoxicosis Under the Age of 45It is helpful first to exclude those patients who
fall naturally into a medical category. Theseinclude the following:
(i) Young Patients and Those Subject to StressMcdical treatment-by sedation or chemo-
therapy-should be employed whenever possiblein young children and at times of exceptionalphysiological stress, such as puberty, pregnancyand the menopause, when antithyroid cover willgenerally be all that is necessary.
(2) Mild Thyrotoxicosis (and Anxiety State)Medical treatment is indicated in all patients
with mild thyrotoxicosis. Surgery, the antithyroiddrugs and iodine are alike contraindicated, yetinstances of the use of each of these methods arenot uncommonly seen. Surgery is absolutelycontraindicated because it is unnecessary. Theantithyroid drugs should not be used in the firstinstance, but only resorted to if rest and sedationfails. Iodine also has no place in the purelymedical treatment of any form of thyrotoxicosis.Iodine is to the thyrotoxic patient what morphiais to the ' acute abdomen'-it masks symptomswithout curing the disease, it produces a rapidresponse which is misleading as the effect is onlytransient and is not maintained-but it may besignificant enough to induce a false belief in non-surgical measures, with the result that operativetreatment is postponed unwisely. Its use in thetreatment of toxic goitre should therefore berestricted to the immediate pre-operative phase.
(3) Recurrent Thyrotoxicosis (Post-operative)(a) No thyroid tissue palpable. Surgery is abso-
lutely contraindicated in those cases of post-operative recurrent thyrotoxicosis in whom thereis no palpable thyroid tissue in the neck. Treat-ment with the antithyroid drugs has its most aptand valuable application in these circumstances.
(b) Thyroid tissue palpable. In these patientsthe recurrence is usually nodular in type. The
Yuly I 960450copyright.
on July 13, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.36.417.447 on 1 July 1960. D
ownloaded from

J7uly I960 RIDDELL: The Surgery of the Thyroid Gland 45I
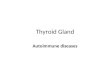
A BFIG. 2. Tarsorrhaphy.-(a) Patient developed a traumatic conjunctivitis as a result of contact with the
pillow during sleep. (b) Tarsorrhaphy is surprisingly well tolerated by these patients who rarelycomplain of their ' blinkers.'
choice as between surgery or medical methodswill be influenced by two considerations-thesize of the thyroid recurrence and the integrity ofthe recurrent nerves. Re-operation on thesepatients is always hazardous because of the riskof damaging a nerve. If the recurrence is bulky,and displacing the trachea, surgery may be forcedand should be carried out if laryngoscopy showsthat both inferior laryngeal nerves are intact. Ifthe recurrence is associated with an inferiorlaryngeal nerve palsy on the side opposite to therecurrence, re-operation incurs the risk of damag-ing the only remaining recurrent nerve so that anattempt should be made to control the thyro-toxicosis with antithyroid agents or radioiodine.The decision as to which of these methods isused will be influenced by the age of the patientand by whether she is sensitive or not to anti-thyroid drugs. If the recurrence takes place onthe same side as a nerve lesion, re-operation canbe considered with less anxiety as the underlyingnerve has already been damaged. If the recurrenceonly involves the pyramidal lobe then this shouldbe excised.
(4) Masked ThyrotoxicosisMost patients with masked hyperthyroidism-
often presenting with unexplained auricular fibril-lation-are found in the over-45 age group, butif occurring at a younger age they should betreated with the antithyroid drugs to which theyrespond well.
(5) Malignant ExophthalmosMedical treatment is advisable in the oph-
thalmic forms of thyrotoxicosis. It is importantto assess the degree of thyrotoxicosis withoutregard to the eye signs and to treat the toxicityon its own merits. It may not be severe.
Thyroidectomy, the antithyroid agents and1311 may increase the proptosis. If operation iscontemplated-possibly because of the large sizeof the goitre-it is advisable to give a preliminarytest course of antithyroid agent and observe itseffect upon the eyes. If the proptosis increases itwill be wise to avoid thyroidectomy. Whatevertreatment is employed it is reasonable to givethyroid extract at the same time with the intention
copyright. on July 13, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.417.447 on 1 July 1960. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
of reducing the amount of thyrotropic hormoneproduced by the anterior lobe of the pituitary.
Tarsorrhaphy should be carried out early insevere proptosis (Fig. 2). It is often recom-mended too late, when corneal ulceration, hypo-pyon and other ocular complications have de-veloped. Orbital decompression, whereby theorbit is unroofed, will be necessary in progressivecases to save the sight.
Toxic Nodular GoitreThyroidectomy is indicated in the treatment of
toxic nodular goitre-with a few exceptions. Ifthe patient is middle-aged or elderly and thenodularity amounts to no more than a smoothasymmetry in ' size ' of the two lateral lobes,good results can be obtained in carefully selectedcases from medical treatment only, as concomitantmalignant change is very rare.
Pressure symptoms. Thyroidectomy is indicatedwhen pressure symptoms are present or might beprecipitated by the use of antithyroid drugs as ina retrosternal or intrathoracic goitre, or whenthere is displacement or compression of thetrachea. The pressure symptoms vary from asense of pressure in the neck to choking sensationsor even a feeling of suffocation in more severecases. In non-malignant goitres dysphagia isstrangely rare even when the oesophagus is grosslydisplaced. A chronic cough, hoarseness of thevoice or inspiratory stridor may be a directpressure effect; in all these cases involvement ofthe recurrent nerves should be excluded bylaryngoscopy.
Failed medical treatment. By a process ofelimination thyroidectomy or radioactive iodinebecomes the only effective expedient in thosepatients in whom medical treatment with anti-thyroid drugs has failed, i.e. the thiouracil-sensitive, the thiouracil relapses and the thiouracil-resistant.
Social and economic factors. Thyroidectomymay also be the most desirable method of treat-ment in those who are unable or unwilling toattend regularly, in the unreliable and unco-operative patient, or for social or economicreasons.
Malignancy. Surgical treatment is indicated ifmalignancy cannot be excluded.
Size. Size alone can be a contraindication tomedical treatment. A large goitre often becomeseven larger with antithyroid treatment, and evenif it does not cause pressure symptoms requiringsurgical intervention its presence is uncomfort-able and is at meal times a constant reminder ofthe patient's disability. The cosmetic appearanceis unsightly and if the patient is a male he islikely to have to buy new shirts and collars.
Open Group: Surgery or Antithyroid Drugs ?The exclusion of those patients who sort them-
selves out naturally into a medical or surgicalcategory for treatment leaves a third group inwhom it is not at first obvious as to which methodof treatment will suit them best. It is the groupof patients under 45 with toxic diffuse goitre ofmoderate or severe degree (excluding mild thyro-toxicosis). A decision can be arrived at in thisopen, indeterminate group by reference to thepatient's age, the patient's preference and thefacilities available.
Younger Age Group (I8-40)Very broadly, surgery is indicated as the elective
method of treatment in those patients at theyounger end of the under-45 scale (I8-40) andchemotherapy in those at the older end of thescale (40-45).The disappointing long-term results of anti-
thyroid therapy have produced a swing of thependulum back towards surgical treatment, par-ticularly for the younger adult patients in whomradioiodine is contraindicated. Younger patientsdo not tolerate well the tedium of prolonged anti-thyroid therapy. They are impatient of resultsand inclined to find the repeated visits to hospitaltedious and continuous tablet medication irk-some, and for these reasons they may not progressfavourably. More important still, those in theyounger age group-because the gland reactsmaximally to the antithyroid agent-are moreliable to develop a thiouracil goitre and quitesuddenly slip over into myxoedema unless veryfrequent and time-consuming visits are made tohospital or practitioner for reassessment andsupervision. For these reasons in the ' underforties ' better results can be achieved by thy-roidectomy than by purely medical methods oftreatment.
Middle Age Group (40-45)In the older patient, that is those in the pre-
menopausal and menopausal age groups, forexactly the opposite reasons to those just setdown, there should be an inclination towardsmedical treatment as the initial method of choice.In these patients there is less likelihood of thedevelopment of a thiouracil goitre or myxoedema.
Supplementary Factors Influencing, SelectionApart from the patient's age the decision as to
whether the treatment should te along medicalor surgical lines will be influenced by the patient'sown preference, and by the presence or absence ofa causal agent, such as domestic worry, housingdifficulties or an uncongenial occupation and by
452 3ruly I 960copyright.
on July 13, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.36.417.447 on 1 July 1960. D
ownloaded from

RIDDELL: The Surgery of the Thyroid Gland
the standard of medical and surgical facilitiesavailable, both of which can vary greatly.
Thyrotoxicosis Over the Age of 45The methods of treatment in patients with
thyrotoxicosis over the age of 45 are extended bythe possibility of using 1311 so that the choice inthe over-45 age group lies between chemotherapy,surgery and radioiodine. In most cases, chemo-therapy or l3lI should be the initial elective methodof choice rather than surgery; the decision be-tween these two methods will usually be decidedby the availability or not of 131I and the necessaryfacilities for its administration and control. Inthe main a case suitable for treatment with anantithyroid drug is suitable for treatment with131I; an exception is the patient with a small im-palpable thyroid who is best treated with anantithyroid drug owing to the difficulty of judgingthe correct dose of 1311 when the gland size issmall. Thyroidectomy will, however, continue tobe the method of choice in this group for casesof established toxic nodular goitre-unilateral orbilateral-and for all cases in which long-termtherapy or radioiodine seems likely to be unsuitedto the patient in question. Meticulous surgerystill has much to offer at all ages as an alternativeto the slower-acting antithyroid drugs and 1311.
The Thyrocardiac PatientThe thyrocardiac patient is usually found in the
over-45 age group. There is a double lesion-thethyrotoxicosis and the fibrillation-and it is im-portant that the severity of each of these com-ponents should be separately assessed, and ifnecessary separately treated.
The thyrotoxic component. The thyrotoxicosisin this group is much more commonly relativelymild or, at the most, of moderate severity only.The problem in fact is usually more cardiac thanthyrotoxic. If the thyrotoxicosis is severe thenan antithyroid drug should be prescribed in itsusual dosage, to overcome the toxicity.
If the thyrotoxicosis is not severe and the patientis being prepared for operation, the use of iodineis all that is necessary to bring the patient to asafe pre-operative level. In the milder case thepre-operative use of an antithyroid drug as wellmerely adds difficulty without adding safety tothe operation.
The cardiac component. If there is no heartfailure a patient with slow fibrillation can safelybe operated upon as soon as the toxicity has beencontrolled.
If the patient is in heart failure and this isrelieved by treatment, thyroidectomy can be under-taken as soon as the patient has become euthyroid,or more probably it will be decided to continue
treatment with antithyroid drugs or radioiodine.If the heart failure remains unrelieved, althoughthe thyrotoxicosis is controlled, surgery will haveto be abandoned permanently as the definitiveform of treatment for the thyrotoxicosis. Thistype of case remains more a cardiac than a thyro-toxic problem.
Pre-operative PreparationPre-operative Preparation for Second DegreeThyrotoxicosis (Sleeping Pulse 90-I i0)
Patients with thyrotoxicosis of intermediateseverity can be brought, with a few exceptions,to a safe operative level with iodine alone. Manyfall into this category. It is necessary to stressthis fact because in recent years there has been atendency to advise the use of antithyroid agents-' just for safety '-in the preparation of allpatients undergoing thyroidectomy for toxic goitreregardless of the initial severity of the disease.This is unsound. Antithyroid agents should beused only for the pre-operative preparation ofpatients with severe thyrotoxicosis (third degree).
It is satisfactory to give iodine in aqueous solu-tion as Lugol's iodine (5% iodine, io% potassiumiodide in water), io minims t.d.s. in milk, althoughall soluble compounds of iodine are equally effec-tive and sodium and potassium iodide particu-larly more efficient. Potassium or sodium iodide,250 mg., are approximately equivalent to 30minims Lugol's solution. Dosage in excess ofthis is valueless as the excess iodine is not utilizedby the gland. The practice of giving graduallyincreasing doses has no advantage and is onlyconfusing to dispenser and patient alike; a constantdaily dose should be prescribed.
Operation is carried out at the moment ofminimum risk, that is when the maximum lower-ing of the pulse rate has been obtained. This isusually ten days after starting the course, but asthis point may be reached earlier, e.g. eighth dayor later-twelfth day-no rule of thumb shouldbe followed or some cases will be operated uponprematurely and others after the iodine effect hasbegun to wear off. In calculating the optimumday for operation it is important not to forget totake into consideration the date of onset of thenext menstrual period so that this may be avoided.
Post-operatively iodine should be continued forone week and then stopped.
Pre-operative Preparation for Third DegreeThyrotoxicosis (Sleeping Pulse i io and above)
Patients with severe thyrotoxicosis cannot bebrought to. a safe operative level without a pre-liminary course of an antithyroid drug. Adminis-tration of the antithyroid agent selected con-tinues in its initial dosage until the patient is
3tuly I 96o 453copyright.
on July 13, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.36.417.447 on 1 July 1960. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
symptom-free, or ideally just short of this point,when the drug is stopped altogether. The sur-geon's aim is to keep the course as short as possiblein order to reduce haemorrhage at operation andto avoid operating on a hypothyroid patient. Aplanned pre-operative course of antithyroid agentshould rarely exceed four weeks and can often bediscontinued with safety after two or three weeks.A post-therapy pre-operative white cell countshould be carried out on the day before operationto exclude a delayed thiouracil leucopenic reaction.
Pre-operative iodine in a patient already de-toxicated by an antithyroid drug is not an essential.If the iodine is being used for its alleged devascu-larizing effect the questionable advantage obtainedhas to be balanced against the increased hardnessand rigidity it produces in the gland.
OvertreatmentIt is almost true to say that the misapplication
of the antithyroid drugs is causing surgeons moreanxiety and difficulties than the disease itself.Overtreatment is the main error. It producesboth local and general effects.
Local Effects-Thiouracil GoitreOvertreatment with antithyroid drugs results in
a hyperplastic gland-a thiouracil goitre.This is a huge, throbbing vascular goitre over
which a bruit may be heard on auscultation. Thismistake arises as a result of a failure in the systemof supervision. Either the patient is seen tooseldom and slips over into myxoedema in theinterval between visits, or she is seen regularlybut by a different clinician on each occasion, whorepeats unaltered a dosage which should bereduced.The reversal of the original thyrotoxic state
and its replacement by myxoedema from over-dosage with antithyroid drugs not only is theunnecessary replacement of one disease by anotherbut greatly delays the patient's return to normalhealth. A hypothyroid state can be avoided onlyby repeated examinations of the patient by thesame clinician throughout the period of anti-thyroid therapy and by the simultaneous adminis-tration of thyroxine. If myxoedema or a goitredevelops the treatment is to stop the drug as soonas the evidence of overdosage is detected.A thiouracil goitre may be associated with
pressure symptoms; increased vascularity: tachy-cardia.
Pressure SymptomsIt is very undesirable that overdosage with
antithyroid agent should occur. The resultantthiouracil goitre, by producing tracheal compression,may cause pressure symptoms and force surgery
when the gland is at its most intractable and thepatient verging on myxoedema. The antithyroidagents produce effects upon the gland of primarytoxic goitre which occur only minimally or not atall in the nodular thyroid of the older patient.They increase the size of the gland, render itsconsistence hard and rigid, and so seriously restrictits mobility at operation and increase its vascu-larity many times.
HaemorrhageOperation on a thiouracil goitre is an operation
on an arteriovenous fistula. It is important to beaware of the increased vascularity and so beprepared for the very severe bleeding which canoccur at operation. If this comes as a surprise itmay well extend the most experienced surgeon.There is little doubt that isolated experiences ofthis kind, usually in overtreated glands, have donemuch to prejudice some surgeons against the anti-thyroid agents.Much can be done to diminish the technical
difficulties associated with the use of the anti-thyroid drugs: (i) By avoiding pre-operative over-dosage with antithyroid agent; (2) by adminis-tering 1-thyroxine sodium synchronously with thechosen antithyroid drug; and (3) by not adminis-tering Lugol's iodine in cases satisfactorily con-trolled by the antithyroid agent alone.
But despite observing these precautions therewill be occasional cases calling for all the opera-tor's skill if bleeding is to be controlled, anadequate amount of gland removed and nodamage inflicted upon either of the recurrentlaryngeal nerves.
Vocal Cord ThickeningThickening of the vocal cords takes place when
myxoedema is induced by overtreatment and thisconstitutes a very real post-operative danger fromoedema of the glottis. If surgery is forced inthese circumstances a very careful watch will benecessary post-operatively, and it will be wise tohave a tracheotomy set in readiness.
General EffectsMyxoedema. If myxoedema is produced by
antithyroid agents an irreversible state may beset up, or at least a state which takes a long timeto adjust itself. If the patient is referred forsurgery at this stage of overpreparation operationshould be refused. Thyroidectomy is stronglycontraindicated in the hypothyroid phase, becauseof the danger from haemorrhage and oedema ofthe glottis, and must be resisted unless it isrequired to relieve urgent pressure symptoms.A long delay must follow before operation cansafely be undertaken-to allow the patient time
_7uly I 960454copyright.
on July 13, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.36.417.447 on 1 July 1960. D
ownloaded from

RIDDELL: The Surgery of the Thyroid Gland
to revert to a euthyroid state. In short, the netresult of overtreatment is seriously to slow up thepatient's return to normal health and thyroidbalance.
TECHNIQUE OF SUBTOTALTHYROIDECTOMY
This is not a treatise on the surgical techniqueof thyroidectomy, which is now well established,so that only a few points of interest to surgeonswill be summarized. In the modern operationall the main arteries to the gland are secured-' the clip and cut' method is obsolete. The firststep taken is the mobilization of the lateral lobeand the identification and division of the lateralthyroid veins. This is followed by division of thesuperior thyroid vessels, the division or ligationin continuity of the inferior thyroid artery, theidentification of the recurrent laryngeal nerve andthe division of the inferior thyroid veins. Thisprocedure is then repeated on the other side.
The Superior and Inferior Thyroid ArteriesWhen the subtotal operation is performed for
thyrotoxicosis the superior thyroid arteries shouldbe tied and divided and the inferior thyroid arterytied in continuity on each side. There is anabundant blood supply left to the gland by wayof the paratracheal and paraoesophageal branchesof the ascending pharangeal and bronchial arteries.Ligation of the inferior arteries-as far awayfrom the gland as possible to avoid injury to therecurrent nerve-has two great advantages: itreduces the incidence of recurrent thyrotoxicosis,and it reduces the bleeding from the cut surfaceof the gland when this is resected.
In patients who before preparation for operationwere very severely toxic, the inferior arteries, asis the usual practice with the superior arteries,should be tied and divided or recanalization islikely. One must beware of tying one of the mainterminal divisions in mistake for the main trunk,which may bifurcate far out.
In thiouracil-prepared cases it is dangerous toattempt the resection of the gland until all thenamed arteries have been secured or an uncon-trollable fatal haemorrhage may result from thecut surface.
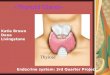
Multiple-stage Operations (Fig. 3)It is difficult to visualize the circumstances in
which the preliminary ligation of arteries couldarise today unless the toxicity is quite uncon-trollable by the medical methods which are nowavailable. On the other hand, it may occasionallybe both prudent and necessary to stop the opera-tion after resecting one lobe and to operate on thesecond side at a later date. The need for such a
FIG. 3.-Multiple-stage operations. At the first stage it isoccasionally wise to remove one lobe only, tyingand dividing superior and inferior thyroid arteries,together with ligating in continuity the oppositesuperior thyroid artery.
two-stage thyroidectomy is most likelv to arisewhen operating on a very vascular hyperplasticgland in a young person who has received toolong a pre-operative course of antithyroid agentor who has relapsed after long-term therapy.The operation under these conditions can be oneof the most testing in surgery and if the haemor-rhage is unusually heavy or if the pulse rateshould rise to I40 or above it would be foolishto proceed to the resection of the second lobe.
The Infrahyoid (Strap) MusclesThe infrahyoid muscles should be divided in all
cases in which the improved exposure would addsafety to the operation. Division of the musclesis indicated more often in bilateral than unilateraloperations. It should be carried out in all opera-tions upon glands which have been prepared withan antithyroid agent unless the surgeon is excep-tionally experienced; it is usually unnecessary inpartial thyroidectomy (hemithyroidectomy) for asolitary adenoma.
,7uly I 960 455copyright.
on July 13, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.36.417.447 on 1 July 1960. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
SURGERY IN MALIGNANT GOITREIn malignant goitre-if operable-surgery holds
undisputed priority over all other methods oftreatment.
ContraindicationsThere are no local contraindications to opera-
tion in cancer of the thyroid-except inoperability.Operability can often only be assessed after
surgical exposure of the thyroid gland. Clinicalfindings suggestive of inoperability are: Dys-phagia; limitation of the excursion of the thyroidon swallowing; recurrent laryngeal nerve involve-ment; cervical sympathetic chain involvement;and fixed cervical lymph nodes.
Dysphagia. Dysphagia is curiously rare even inthe largest of non-malignant goitres associatedwith gross displacement of the gullet. Thissymptom, if it develops, should therefore alwaysbe regarded with suspicion.
Limitation of excursion of the thyroid on swallow-ing. This is due to fixation of the gland by trans-capsular spread. It has to be remembered that asimilar restriction of movement of the thyroid isfound (i) in true retrosternal goitre where theintrathoracic extension wedges the trachea in thethoracic inlet, and (2) when there has been ahaemorrhage into a thyroid cyst, the outer surfaceof the cyst becoming coated with a sticky,fibrinous exudate which temporarily adheres tosurrounding structures. (In Hashimoto's diseasemovement of the gland is full and normal and themargins of the thyroid are usually well definedand easily palpable.)
Involvement of a recurrent laryngeal nerve. Thiswill produce a partial or complete paralysis of avocal cord, but is not always associated with ahoarse voice. This is because compensation bythe normal cord may be very complete so that apalsy may not be suspected unless the cords areexamined routinely by laryngoscopy before everyoperation upon the thyroid.
Involvement of the cervical sympathetic chain.This will produce enophthalmos, ptosis and acontracted pupil on the affected side (Horner'ssyndrome).Enlarged cervical lymph nodes. The neck and
both axillae should be palpated. A fixed mass ofnodes is a warning that operation will be difficultor impossible. A mobile lymph node offersreadily accessible material for excision and patho-logical identification.
Metastases. Paradoxically in cancer of thethyroid alone, the presence of distant metastasesis not necessarily a contraindication but in somecircumstances is an indication for radical thyroidsurgery, notably in follicular adenocarcinoma.
Differential DiagnosisConditions simulating cancer of the thyroid
should, if possible, be excluded. They includenon-toxic nodular goitre, lymphadenoid goitreand the other rare forms of thyroiditis, metastatictumour tissue in the thyroid (the primary lesionhas been most frequently in the breast, lung orkidney), calcification, and haemorrhage into acyst. All these misleading conditions, so long asthey are remembered, can be excluded by takinga careful history supported by obtaining materialfor histological confirmation.To formulate a plan of treatment the clinician
must be able to answer the following questions:Is the tumour malignant or non-malignant ?Is the tumour operable or inoperable ?Is the tumour differentiated or undifferentiated ?Is the tumour radioactive-iodine-concentrating ?
InvestigationsSpecial investigations include radiography,
laryngoscopy, tracheoscopy, 1311 investigation,blood examination, biopsy and the exclusion ofmetastatic conditions simulating primary carci-noma of the thyroid.
RadiographyA lateral and antero-posterior radiological
examination of the neck and thoracic inlet isrequired to exclude deviation or compression ofthe trachea, and retrosternal or intrathoracic ex-tension of the thyroid. Radiography will occa-sionally show that a nodule suspected of malig-nancy because of its hardness is the site of calci-fication. The chest is also examined to excludemetastases and any site of bone pain should besimilarly investigated for the same reason.
LaryngoscopyPre-operative laryngoscopy may reveal an un-
suspected recurrent laryngeal nerve palsy. Thediscovery of a paralysed vocal cord in a patientwith no change of voice is important before theoperation is carried out, for obvious medico-legalprotection reasons; in addition, if complete, it willencourage the surgeon to do a more radicaloperation on the side of the nerve involvementand, by forewarning him, will make him morecautious in exposing the opposite normal nerve.
TracheoscopyTracheoscopy is important to exclude malignant
infiltration or ulceration of the trachea. If thesedevelopments are encountered unexpectedly inthe course of the operation the surgeon is likelyto be unprepared to deal with them and an incom-plete operation will result. If he is forewarnedhe can plan an extirpative procedure and be
7uly i 960456copyright.
on July 13, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.36.417.447 on 1 July 1960. D
ownloaded from

RIDDELL: The Surgery of the Thyroid Gland
prepared to resect and reconstruct a part or thewhole of the trachea.
BiopsyThe histology of the tumour has an important
bearing upon its surgical and radiation manage-ment. Three basic cell types are recognizable:the papillary (62%), the follicular (20%), and theundifferentiated (anaplastic) (i8%). Some tu-mours contain elements-of all three patterns, andif sufficient sections are examined few differ-entiated tumours will be found to be exclusivelypapillary or exclusively follicular. It is this ten-dency for elements of each to be present in mostdifferentiated and even in some undifferentiatedtumours that has encouraged 131J workers to tryto induce pick-up in tumours in which thepredominant histological picture would seem tobe against success.
Experience has shown that the differentiatedtumours are more likely to concentrate radio-active iodine than the undifferentiated ones, andthat the follicular carcinoma is considerably morelikely to pick up radioactive iodine than thepapillary type. The clinical behaviour of thesetwo varieties is also different; the slow-growingpapillary variety tends to metastasize to locallymph nodes, whereas the follicular type is morerapidly growing and tends to metastasize by theblood stream to the lungs or bones. These dif-ferences must be remembered as they influencethe approach to treatment.The histology can be determined pre-operatively
if an enlarged lymph node is available for ex-cision; at the time of operation by the frozensection method, post-operatively in the usual wayby examination of the operation specimen, and inthe inoperable case by a preliminary pre-radiationdrill biopsy.
Frozen Section ExaminationAn immediate diagnosis at operation may save
the patient a second operation or it may preventan unnecessary one. It is of most value in thedoubtful case, and in thyroid carcinoma presentingunilaterally. In the doubtful case the malignancyor innocence of the section will determine therestriction (if non-malignant) or extension (ifmalignant) of the operation. In the unilateralcase, by revealing the predominant histologicalpattern, it will aid the surgeon in his decision toremove (in follicular carcinoma) or not to remove(in anaplastic carcinoma) the contralateral normallobe.
In addition, by supplying the surgeon with theinformation that the tumour is malignant it willenable him to do a complete lobectomy instead ofan incomplete one. This, in turn, will obviate a
further operation to remove the thyroid remnantwhich, if left untreated (and if papillary or ana-plastic it is unlikely to respond to radioactiveiodine) will later lead to a stump recurrencewhich in turn may progress to a fatal issue.
Nevertheless, a frozen section examination witha reliable opinion remains a counsel of perfectionin the majority of clinics. The rapid interpreta-tion of the appearances of thyroid material requiresa pathologist of exceptional experience and wis-dom. The differences between certain benignpapillary adenomas and a papillary carcinomaand the difference between the thiouracil-preparedthyrotoxic gland and the papillary carcinoma arenotoriously difficult. Only a strong positive asser-tion of malignancy should be acted upon. Inmany instances it will therefore be wiser to allowthe extra time necessary for the preparation andexamination of paraffin-embedded sections.
It cannot be too often repeated that surgicalremoval offers the best chance of controllingthyroid cancer. ' Operable cases should first beoperated upon.'7 This is an obvious statement,yet the insistence of surgical priority in themanagement of operable cases cannot be toostrongly emphasized. Radiation methods are aptto bemuse the clinician, but it needs to be saidthat they are only supplementary and secondaryin importance when the tumour is removable.
Unilateral Operable CancerUnilateral operable thyroid cancer may present
in three clinical forms:(i) It may present as a solitary, symptomless
swelling of recent appearance. The initial diag-nosis is benign 'adenoma' from which this formis clinically indistinguishable, and it is this typeof ' unsuspected' carcinoma which is discoveredaccidentally when the 'adenoma' is cut across inthe theatre at the end of the operation. Thisvariety, which is the commonest of all and isalso the most favourable, is the one most liableto be left alone for the reason that it is symptom-less. It often occurs in young women and isusually of the papilliferous type.A solitary swelling in the thyroid must be
regarded as malignant until proved otherwise.It should be treated like a solitary swelling in thebreast by removal and histological examination.It should be excised not because it may becomemalignant, but because it may already bemalignant.
(2) It may present as a solitary-swelling not ofrecent appearance but with a history of recentincrease in size of a pre-existing unilateral goitre.
(3) It may present as a palpable cervical lymphnode or nodes-formerly misnamed a lateral
,7uly I960 457copyright.
on July 13, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.36.417.447 on 1 July 1960. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
aberrant thyroid-the primary tumour beingoccult in the thyroid.
This is the rarest type of carcinoma of thethyroid. It is comparable to occult carcinoma ofthe breast. The primary tumour in the thyroid istoo minute to be palpable, but at operation it isfound to be in the lobe on the same side as theenlarged cervical lumph nodes. A total lobec-tomy on the side on which the nodes are enlarged,together with removal of the palpable cervicalnodes on that side, is the treatment.
-Surgical ManagementThe surgical management of apparently uni-
lateral thyroid cancer must be considered as itconcerns (a) the. affected lobe, (b) the homolaterallymph nodes, and (c) the contralateral lobe.
Surgical Management of the Affected LobeIn all these clinical types of thyroid carcinoma
the ideal primary measure is total unilaterallobectomy (and in certain cases total thyroidec-tomy). Total unilateral lobectomy will includeall the thyroid tissue on the affected side, togetherwith any enlarged lymph nodes and the isthmusand the pyramidal lobe, so that the trachea is leftbare anteriorly. The completeness of the lobec-tomy will depend upon whether pathologicalidentification of the tumour by frozen sectionduring the operation has been possible or not.If the result of a frozen section examination is notavailable or is inconclusive, a hemithyroidectomy,leaving a strip of thyroid behind, is likely to bethe operation performed. Because the time intervalbetween the incomplete removal of the originaltumour and a recurrence may sometimes be 5-10years, it has led to a laissez-faire attitude towardsincomplete lobectomy. This is more than unfor-tunate. The totality of the lobectomy probablyinfluences the subsequent course of the diseasemore than any other single measure. Incompleteremoval invites stump recurrence, that is recurrentcarcinoma in the fragment of gland remainingafter incomplete lobectomy. Stump recurrencekills by local invasion of the trachea and oeso-phagus, a commoner cause of death in thyroidcancer than distant metastases.8 Medial extensionoccurs between the cartilaginous rings of thetrachea and then spreads submucously up anddown the trachea where the intraluminal tumourmay produce obstruction, ulceration and haemor-rhage.
Surgical Management of the Homolateral LymphNodesThe problem of dissection of the regional
lymph nodes. There are two views-the con-servative and the radical-regarding the question
of block dissection of the neck. The radical viewis that an aggressive attitude should be taken inall types of thyroid cancer, including the papillary,not only towards the thyroid gland but alsotowards the cervical lymph nodes, and a homo-lateral block dissection should be performedwhether lymph nodes are palpable or not. Thiscontention is supported by the fact that a highproportion of clinically impalpable nodes containmetastases on histological examination2 and bythe essentially local tendency to recurrence andspread which is characteristic of the papillarytumour.'2 It is contended that a resolute localattack upon the thyroid gland and the area of itslymphatic drainage has more positive life-savingpotentialities than what is regarded as the piece-meal conservative approach.Those who hold the conservative view place
their faith in the thoroughness and completenessof the primary surgery upon the malignant lobeor lobes of the thyroid gland (total lobectomy ortotal thyroidectomy) and its juxtathyroid lymphnodes. At this operation a special point is madeof meticulously removing all lymph nodes lyingnfear the thyroid (primary zone metastases).These juxtathyroid lymph nodes are found lyingabove and below the isthmus in front of thetrachea (pretracheal) and in the tracheo-oesopha-geal groove (para-oesophageal). They are distin-guished from the lateral cervical lymph nodes(secondary zone metastases) which lie alongsideand around the great vessels and are usuallyinvaded only at a later stage of the disease. Upto this point the conservative school and theradical school practise the same operation. There-after only do they diverge in their policy. Theradical school proceed to a block dissection; theconservative confine further surgery to the localremoval of visible lymph nodes in the operationfield. From this point the conservative schoolrely on close supervision and follow-up examina-tions to detect and deal with recurrence. Insupport of their attitude the conservative schoolquote: (a) The slow rate of growth of mostpapillary cancers; (b) the fact that patients withpapillary cancer do not die from uncontrolledlateral cervical metastases but from central inva-sion of the trachea, oesophagus and mediastinumby the primary tumour and its centrally placedmetastases.
' The battle' of the thyroid is won or lost in thecentral area of the mediastinum and neck. It isthis vital area that the classical block dissectiondisregards."
In contemplating the radical approach, whichis supported or condemned by surgeons experi-enced in thyroid surgery in almost equal numbers,the individual clinician responsible must try with
458 'Ylvl I 966copyright.
on July 13, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.36.417.447 on 1 July 1960. D
ownloaded from

RIDDELL: The Surgery of the Thyroid Gland
each individual patient-with such evidence as isavailable-to balance the possible prolongation oflife on the one hand against the tragic mutilationproduced, sometimes in a very young life, on theother. Statistics should provide the answer andgive him the factual guidance he seeks, but theyare sadly deficient because of the comparativerarity of the disease. Until pooling of materialand its statistical analysis is carried out on amuch larger scale, the present uncertainty is likelyto continue for some time to come. In the mean-time the writer's practice is to concentrate andpursue the surgical attack upon the thyroid andits juxtathyroid lymph nodes with determinationand vigour but to refrain from block dissection-particularly in the young-except in exceptionalcircumstances.
The Problem of the Contralateral LobeThe conflict of opinion here concerns the
advisability or not of destroying by radioactiveiodine or removing by surgery the contralateral or' normal' lobe of the thyroid in patients present-ing with clinically unilateral cancer.
Should the contralateral lobe be ablated ? Ifit is believed, even when the histological patternis unfavourable and when a complete lobectomyhas been performed, that every effort should bemade to induce radioactive iodine uptake, all thesepatients with apparently unilateral thyroid cancerwill be treated in the same way, namely, by totalthyroid suppression, regardless of the histology ofthe tumour, the natural history of the disease orthe presence or absence of distant metastases.
If it is believed that we should, and can, bemore selective in our treatment of this group, wewill consider the natural history as well as thehistology of the tumour. If the histology is pre-dominantly follicular there is general agreementthat suppression or removal of the contralateralnormal lobe should be carried out and radio-active iodine treatment instituted if there is anysuspicion of extracervical metastases being present.
There are two good reasons for this: First, theclinical course of follicular carcinoma is morerapid than the papillary variety, and there is atendency to earlier and more frequent distantmetastases; secondly, there is a better chance ofinducing uptake in the follicular type of carcinomathan in any other variety, provided the normaladjacent thyroid tissue which competes for theiodine has been removed.
If, on the other hand, the carcinoma is papillaryor anaplastic, the more conservative clinicianswill leave the normal lobe undisturbed in theabsence of demonstrable distant metastases, or atleast will seriously debate the advisability ofablation, the reason for this attitude being that
anaplastic tumours can almost never be inducedto pick up radioactive iodine and pure papillarytumours but rarely, even when ablation has beencarried out. Ablation, therefore, in unilateralcases of papillary or anaplastic cancer, must beregarded as a procedure which carries with it npabsolute guarantee that it will induce any remain-ing tumour tissue to take up radioactive iodine.Furthermore, it must be remembered that radio-active iodine treatment cannot be given withoutfirst making the patient myxoedematous, an effectthat must be given some consideration when it isremembered that the papillary cancer is thecommonest type, with the slowest and mostfavourable clinical course, and most often seen inyoung persons.
Choice of Re-operation or Radioactive IodineAblation of the Contralateral Lobe
If the histology of the tumour is not availableuntil some time after the operation has been con-cluded, and removal of the contralateral lobe isdecided upon, re-operation should be carried outas soon as possible. Operation, when it is possible,is preferred to radioactive iodine treatmentbecause it is quick and avoids using up valuableradiation tolerance. The final choice betweenoperative or radioactive iodine ablation will bedecided by such factors as the time available onthe one hand, and the patient's age and generalcondition on the other. If the time factor isurgent the bias will be towards operation, as thedevelopment of full myxoedema following an abla-tion dose of radioactive iodine takes up to 12weeks, a delay which may be difficult to justify ifmetastases are present or the tumour is rapidlygrowing. Ill-health, infirmity, a history of multiplethyroid operations, the presence of a -recurrentlaryngeal nerve palsy or a history of a previouscourse of irradiation to the neck will bias theclinician towards radioactive iodine ablation.
Following the ablation dose of radioactiveiodine the surgeon must be prepared to carry outtracheotomy, and sometimes it will be wise to doso before the dose is given if there is evidence ofnarrowing of the trachea, as the reaction followingradioactive iodine may be severe and may besudden.
Post-operative External Radiation TherapyThe post-operative so-called prophylactic use
of external irradiation should probably be aban-doned if there has been apparently complete, ornearly complete, removal of a differentiatedtumour.12 'The uneasy suspicion that microscopicmalignant foci may have been left may persuadethe surgeon to prescribe a course of high-voltageX-ray treatment just ' for safety.' The result
,7uly I 960 459copyright.
on July 13, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.36.417.447 on 1 July 1960. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
may be far from what was intended. Papillaryand follicular carcinoma is relatively insensitiveto high-voltage X-rays; the trachea and pharynxinevitably receive a heavy dose which may causegreat and prolonged discomfort to the patient;the skin may develop telangiectases, serious scar-ring and even necrosis may occur, and the recentoperation wound may break down with the inter-mittent discharge of suture material.8
In the main, external radiotherapy should bereserved for the treatment of stump recurrencewhen radioactive iodine has failed, or is contra-indicated, and for the treatment of the inoperableanaplastic tumour.
Bilateral Operable CancerBilateral operable thyroid cancer may present
in two clinical forms:(i) Diffuse carcinoma (de novo). In this variety
the carcinoma arises in a previously normal gland.It is diffuse throughout both lobes. In appearancethe thyroid has no particularly striking featureapart from its enlargement-which may not bemarked; on palpation, however, it is usually muchharder than normal, and the gland is smoothrather than nodular. There may or may not beassociated enlarged cervical lymph nodes.
(2) Diffuse carcinoma (pre-existing multi-nodular goitre). In this variety the carcinomaarises in a previous multinodular goitre (whichmay or may not have been malignant from itsinception). In appearance the gland resemblesany other multinodular goitre; it is usually largerthan the diffuse smooth type and the bossingmay be very marked. Deviation or compressionof the trachea is common; large dilated veinsmay overlie the surface of the gland.The same three histological patterns are found
as in the unilateral group.Surgical management- total thyroidectomy.
In bilateral operable thyroid cancer the problemof the contralateral normal lobe does not arise sothat total thyroidectomy in one stage is the objec-tive. The operation should be confined to theremoval of the thyroid gland and associatedenlarged lymph nodes. The completeness withwhich this can be achieved is more important thanany subsequent form of radiation therapy. Preserva-tion of the recurrent laryngeal nerves, unless theyare hopelessly involved in the tumour, should bemeticulously attempted. The loss of one nervemay be unavoidable, but the sacrifice of both willadd a miserable complication to the patient'sconvalescence. Two at least of the parathyroidglands should also be deliberately identified andpreserved.
Radiation management. Following thyroidec-tomy the patient has a radioactive iodine tracer
investigation of the neck (and later profile count-ing of any remaining areas of iodine uptake inthe body). More often than not uptake of iodinecan be demonstrated even in cases where thesurgeon feels confident that a total thyroidectomywas carried out.3 The explanation is that a stripor islands of tissue may be left adherent to thetrachea or in the region of the parathyroid glandsand recurrent laryngeal nerves or attached to thepedicles of the superior thyroid vessels.The radiation management of patients who
have undergone total thyroidectomy is, on thewhole, decided by whether the primary tumourwas differentiated or undifferentiated.
Differentiated TumoursIn histologically favourable cases radioactive
iodine ablation of this remaining tissue should becarried out. The gland should then be retestedfor uptake with a tracer dose of radioactive iodine.If any can be demonstrated it is presumed thattumour is still present; in this event radioactiveiodine in therapeutic dosage should be given untilno further uptake is demonstrated.
Undifferentiated TumoursIn histologically unfavourable cases, notably
the anaplastic carcinoma, conventional wide-fieldexternal radiotherapy should be started imme-diately.
Inoperable CancerPre-irradiation biopsy. In cases of inoperable
thyroid cancer a preliminary pre-irradiation drillbiopsy should be carried out with the object ofdetermining the degree of differentiation of thetumour and, synchronously, to confirm its thyroidorigin and malignant nature. Advantage shouldbe taken, if an open biopsy by incision has beencarried out, to reduce at the same time the bulkof the thyroid tumour surgically if this is at all'possible, as the smaller the physical mass to betreated the more likely are radiation methods tobe successful. Removal of the isthmus alone may,by breaking the ring of malignant tissue encirclingthe trachea, postpone for some time trachealobstruction and therefore tracheotomy.
TracheotomyTracheotomy is sometimes necessary when
respiratory obstruction is present. In these cir-cumstances it is essential to use a rubber tube ifthe area is being, or is to be, irradiated.
MetastasesLocal metastases in cervical lymph nodes are
best treated by surgical excision-at the time ofthe first operation if they are then present-or by
460 Y- -y I960
copyright. on July 13, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.417.447 on 1 July 1960. Dow
nloaded from

J3uly I960 RIDDELL: The Surgery of the Thyroid Gland 46I-
separate local excision if they develop later. Arecurrence of thyroid gland tissue is excised ifthis is possible; if the mass is irremovable but canbe shown to take up radioactive iodine an ablationdose should be given in the histologically favour-able categories.
Thyroid AdministrationIt seems reasonable to administer thyroid ex-
tract, to patients with thyroid cancer, after thedefinitive treatment has been concluded, with theobject of inhibiting activity in any remainingnormal thyroid tissue.4' 11
REFERENCES
I. CRILE, G., Jnr. (0997), Ann. Surg., 143, 317.
2. FRAZELLE, E. L., and FOOTE, F. W. (xgSS), Cancer, 8, I I64.3. HILTON, G. (I956), Brit. J. Radiol., 29, 297.4. JAMES, A. G. (i9s8), Scot. med. J., 43, 423.s. NEGUS, V. (I94),' The Comparative Anatomy and Physiology
of the Larynx,' London, p. 242.6. RIDDELL, V. H. (1956, Brit. _7. Surg., 44, 25.7. RIDDELL, V. H. ("9S8), Lancet, iI, 638.8. RUNDLE, F. F., and BASSER, A. G. (I956), Cancer, 9, 692.9. SUNDERLAND, S., and SWANEY, W. (1952), Anat. Rec.,
114, 411.
IO. TAYLOR, S. (x958), Lancet, i, 75I.xi. THOMAS, C. G. (I9S7), Y. clin. Endocr., 17, 232.12. WINDEYER, B. W. (1954), Brit. .7. Radiol, 27, 537.
| Patilent's preference. o
W0Nhy bas Lucozade avery special attraction for Lucozade is lighdy car O
Othe patient ? The answer lies in its remarkably boae i0a trcie°Ogolden colour and a pleasant O
Orefreshing flavour and firagrance, qualities that citrus flavour. It contain 0
Obaffle precise description. The colour, the 23.5% w/vLiquid Glucose El
[1sparkle and the glucose content ensure equally an t eeg vleis2aCalories per fluid ounce. O
Oits recommenclation by the doctor and its ready It is supplied in 6 oz. and g
9 cceptance by the patient. 26 oz. bottdes. O
gOOOOOOOOUOOOOOLLLLLLiiiOLiLiLiOLiLiLiLiLiiLiLiLiLiLiLiL1L
CL
CLCLEl
Eli
A Clinic for the diagnosis and treatment of Internal Diseases (except Mental or Infectious Diseases). TheClinic is provided with a staff of doctors, nurses, technicians, m:3de,rn Radiological and Physiotherapydepartments.
The surroundings are beautiful. The climate is mild. There is cientral heating throughout. The annualWin hl is 30.S inchos,that is l vesthan the averagefor England.
The F are inclusive and vary according to the roomoccuaied.For particulasc apply to THE SECRETARYh Ruthin Castle, North Wales.
Teagrame:Cgtle, Ruthin Teyphone: Ruthl i
copyright. on July 13, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.36.417.447 on 1 July 1960. Dow
nloaded from