Embed Size (px)
Citation preview

LABORATORY INVESTIGATIONVENTRICULAR PERFORMANCE
The superiority of maximum fiber elastance over
maximum stress-volume ratio as an index ofcontractile stateTHOMAS WISENBAUGH, M.D., GEORGE YU, M.S.M.E., AND JOYCE EVANS, M.S.
ABSTRACT The end-systolic pressure-volume relationship has been used as a load-independentmeasure of ventricular pump performance. Since comparisons of load between ventricles of differentsize and thickness may be more accurately made with measurements of wall stress than with those ofpressure, the end-systolic stress-volume relationship at one or more levels of end-systolic stress hasbeen used to estimate contractile function in hypertrophied ventricles. Linear regression of end-systolicstress against end-systolic volume for differently loaded beats has a slope termed maximum fiberelastance (fiber Emax) and a volume intercept termed Vo; the maximum stress-volume ratio (MSVR)for a single beat is an approximation of fiber Emax but assumes Vo 0. However, the influence ofpreload, afterload, and inotropic state on these indexes has not been examined. We therefore studiedthe stress-volume relationship in seven open-chest dogs instrumented with ultrasonic crystals andmicromanometers. Postextrasystolic potentiation (PESP) increased both the MSVR (5.7 + 1.83 vs4.85 -+- 1.43 at control, p < .05) and fiber Emax (13.93 + 3.24 vs 9.24 + 2.15 at control; p < .05).Augmentation of preload by infusion of dextran, with the use of nitroprusside to maintain afterloadrelatively constant. did not significantly influence either the MSVR or fiber Emax. Vo was notsignificantly influenced by PESP, but was shifted to higher values by augmentation of preload (17.514.8 vs 13.9 + 1 1.1 ml at control; p < .05). Augmentation of afterload by aortic constriction was usedto derive fiber Emax, and produced an increase in MSVR directly proportional to the increase in wallstress (6.03 ± 1.39 with end-systolic stress augmented by 93% vs 4.85 + 1.43 at control; p < .05).Thus, MSVR is a less reliable index of inotropic state than fiber Emax since it is afterload dependent.Circulation 72, No. 3, 648-653, 1985.
THE END-SYSTOLIC pressure-volume relationshiphas been used as a preload-independent measure ofventricular pump performance.'-3 Since the load onmyocardial fibers comprising the ventricle depends notonly on intraventricular pressure., but also on wallthickness and chamber dimensions, it has been pro-posed that in hypertrophied ventricles stress is a bettermeasure of load than is pressure.4 Several investiga-tors have therefore used either the end-systolic stress-volume relationship for differently loaded beats6 or theend-systolic stress-volume ratio from a single beat7-9 toestimate contractile function in chronically overloadedventricles. However, existing data are not sufficient toclearly define the sensitivity of either the stress-vol-
From the Veterans Administration and University of Kentucky Medi-cal Centers, Lexington.
Supported by a grant from the American Heart Association, Ken-tucky Affiliate.
Address for correspondence: Thomas Wisenbaugh, M.D., Cardiolo-gy Division, Room MN670, University of Kentucky Medical Center.800 Rose St., Lexington, KY 40536.
Received March 8, 1985; revision accepted May 23. 1985.
648
ume ratio or the slope of the stress-volume relationshipat end-systole to changes in contractile state. We there-fore examined the effects of postextrasystolic potentia-tion (PESP) of inotropic state and of altered ventricularvolume and load on the maximum stress-volume ratio(MSVR) and the slope of the end-systolic stress-vol-ume relationship (fiber Emax) in open-chest dogs in-strumented with sonomicrometer crystals and micro-manometer-tip pressure transducers.
MethodsAnimal studies were conducted in accordance with the guide-
lines of the American Physiologic Society. Adult mongrel dogsanesthetized with 1 mg/kg im morphine, 350 mg/kg iv urethane,and 45 mg/kg iv a-chloralose were ventilated on a respiratorthrough an endotracheal tube. Through a left lateral thoracot-omy, the pericardium was opened and two orthogonal pairs of 5MHz piezoelectrical crystals 5 mm in diameter were sutured atthe major and minor axes, as previously described.6 A snare wasplaced around the descending thoracic aorta. Through branchesof the femoral artery, No. 7F micromanometer-tip catheterswere introduced into the left ventricle and proximal aorta. Alarge-bore cannula was inserted into the inferior vena cavathrough a femoral vein. Bipolar epicardial electrodes were su-
CIRCULATION
by guest on April 17, 2017
http://circ.ahajournals.org/D
ownloaded from

LABORATORY INVESTIGATION-VENTRICULAR PERFORMANCE
tured to both the left atrium and left ventricle. Autonomic block-ade was produced with 0. 1 mg/kg atropine and 2 mg/kg iv
propanolol; adequacy of fl-blockade was assessed by determin-ing the dose of isoproterenol required to produce a 25% increasein heart rate both before and after administration of propranolol.Heart rate was maintained just above intrinsic rate (120 to 150beats/min) by atrial pacing. Left ventricular dimensions were
measured with a sonomicrometer (Triton Industries) and record-ed on a strip-chart recorder and on 16-channel magnetic tape
simultaneously with aortic pressure, left ventricular pressure,
left ventricular dP/dT, and the electrocardiogram. Measure-ments were made at four to five different levels of aortic pres-
sure, each produced by tightening the snare during an 8 to 10 sec
interruption of ventilation.PESP was produced by premature ventricular stimuli deliv-
ered at a coupling interval of 200 msec by a programmable pacer
(Medtronics) every eighth beat at each level of pressure. Myo-cardial length (or preload), measured as left ventricular end-diastolic dimensions, was increased by rapid infusion of 250 mldextran. Intravenous nitroprusside was used to maintain con-
stant aortic pressure. Measurements were again made at this andthree to four higher levels of aortic pressure produced by tight-ening the aortic snare. Each experiment was terminated byinducing fibrillation of the heart, which was then removed. Theleft ventricle, including the septum, was weighed after it wasseparated from the right ventricle and atria. Data were digitizedat 5 msec intervals and transferred to floppy disks with an
analog-to-digital converter (Data Acquisition Systems) and mi-crocomputer (IBM PC). Beats just before and after the pro-
grammed premature stimulus at each level of varied loadingwere chosen for analysis.
Ventricular volume was calculated with the equation of Ran-kin et al.'0 as follows:
Vi = (Pi/6)(a- 1. I h)(b - 2h)2 (1)
where Vi is the dynamic internal volume of a prolate ellipsoidalshell in which b is the external diameter of the minor axis, a isthe external diameter of the major axis, and h is the equatorialwall thickness.The external shell volume (Ve) was calculated from the equa-
tion
Ve = (Pi/6)(ab2) (2)
Since the myocardial volume (Vm = Ve - Vi) can becomputed from the measured postmortem mass of the left ven-
tricle and the specific gravity of the myocardium (1.06 g/cm3),wall thickness can be determined from simultaneous solution of
equations 1 and 2. This is done by computer iteration with theNewton Raphson method." Briefly, iteration of the three fol-lowing computations is performed until convergence on thesolution for h:
g(h) 1. 1 h3 - (a + 1. 1 b)h2+ (ab + 1.1b/4)h -3Vm/2Pi
g'(h) = 3.3h2- 2(a + l.lb)h + (ab + l.lb/4)h (4)
h = lh - g(h)/g'(h) (5)
where g(h) is a function of h, g'(h) is the first derivative of thefunction, and lh represents the value of h from the precedingiteration. This is the method used by Hugenholz et a].'2 forcomputing dynamic thickness from left ventriculograms in hu-mans. Mean circumferential wall stress is then computed at 5
Vol. 72, No. 3, September 1985
msec intervals throughout the cardiac cycle with Mirsky's equa-
tion for a thick wall ellipse4 as follows:
S = 1.33(Pb/2h)(1 - b2/(2a2) - h/b) (6)
The end-systolic stress-volume relationship was derived fromeach series of stress-volume loops with the iterative method ofKono et al. 13 that first locates the end-systolic stress-volumecoordinate on each loop and then performs a linear regression onthese points. Since we used stress rather than pressure as ameasure of afterload in this study, we have referred to the slopeof this relationship as fiber Emax to differentiate this quantityfrom chamber Emax, as used by Sagawa and his colleagues. 1 2The MSVR within each loop, which assumes an intercept of Vo= 0, was also determined by the computer, which then plottedeach loop. Comparisons of MSVR for single beats were madeunder control conditions, both for a regular atrial and a poten-tiated beat, with afterload (end-systolic stress) augmented byapproximately 100% of control, and with preload augmentedwhile afterload was held constant.
Statistical analysis. Analysis of covariance was used to es-tablish whether or not significant differences in the Emax wereproduced in each dog by PESP (SYSTAT, Inc.). Comparisonsof values for fiber Emax and other parameters under differentstates were made by analysis of variance for repeated measuresand the multiple-comparison test of Dunnett.
ResultsThe morphologic and baseline hemodynamic char-
acteristics of the dogs are listed in table 1. The hemo-dynamic responses to PESP, volume loading, andpressure loading are shown in table 2.
Fiber Emax was significantly increased by PESP ineach dog, with a mean increase of 51% for the group (p< .05). Fiber Emax was not significantly altered byaugmentation of preload with infusion of dextran-ni-troprusside. The volume intercept, Vo, was not alteredby inotropic stimulation with PESP, but was shifted toa larger value by dextran-nitroprusside. An exampleof the influence of PESP on fiber Emax and Vo isillustrated in figure 1, and the data are summarized intable 3.
TABLE 1Morphologic and hemodynamic data
Body LVweight weight HR LVSP LVEDP
Dog (kg) (g) (bpm) (mm Hg) (mm Hg)
437 22.5 107 150 106 7344 22.4 82 160 108 5438 17.5 64 150 103 6567 20.5 82 150 78 8608 20.5 103 120 135 8614 20.0 73 150 110 8663 24.5 106 130 153 8Mean 21.1 90 144 113 7SD +2.2 +18 +14 +24 +1
LV = left ventricular; HR = heart rate; LVSP = LV systolicpressure; LVEDP = LV end-diastolic pressure.
649
(3)
by guest on April 17, 2017
http://circ.ahajournals.org/D
ownloaded from
WISENBAUGH et at.
TABLE 2Hemodynamic response to intervention (mean + SD)
Volume PressureControl PESP loading loading
LVSP 113 24 135 30A 1 13 + 25 160 ± 38ALVEDP 7+1 9+3 9+2 10±3Maximum
dP/dt 1874 560 3182+2909 2396 + 470A 2083 + 458
Hemodynamic conditions listed in the pressure loading column arethose under which MSVR volume ratio was analyzed. Abbreviationsand units are as in table 1.
ASignificant (p < .05) difference from control by ANOVA.
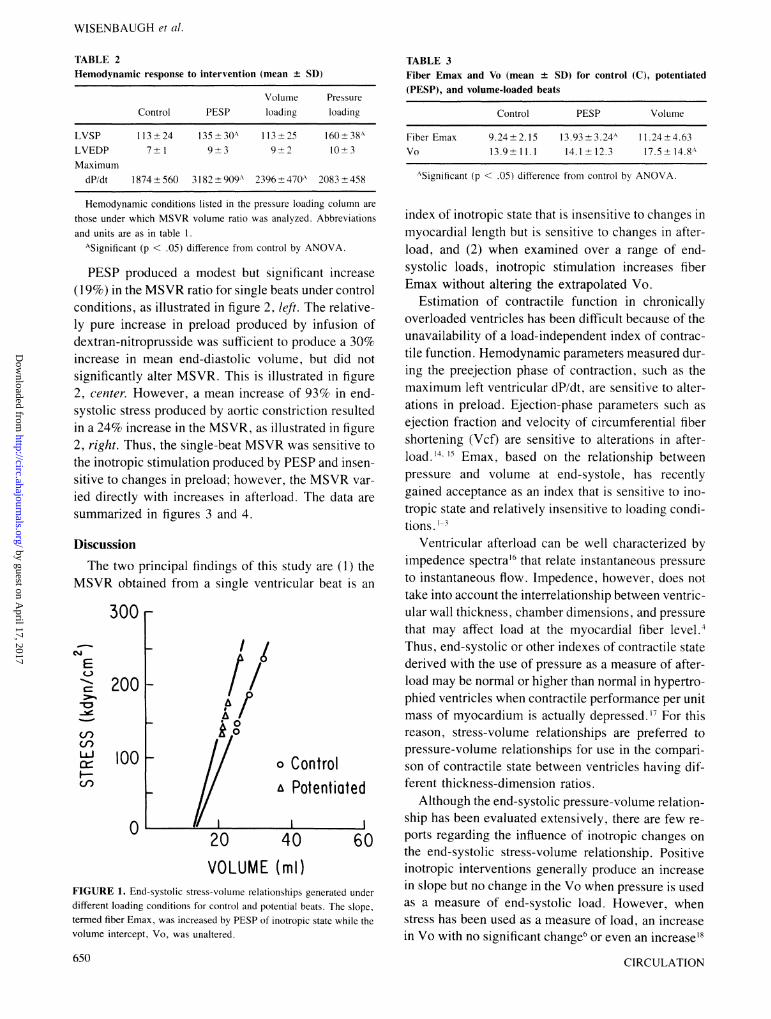
PESP produced a modest but significant increase(19%) in the MSVR ratio for single beats under controlconditions, as illustrated in figure 2, left. The relative-ly pure increase in preload produced by infusion ofdextran-nitroprusside was sufficient to produce a 30%increase in mean end-diastolic volume, but did notsignificantly alter MSVR. This is illustrated in figure2, center. However, a mean increase of 93% in end-systolic stress produced by aortic constriction resultedin a 24% increase in the MSVR, as illustrated in figure2, right. Thus, the single-beat MSVR was sensitive tothe inotropic stimulation produced by PESP and insen-sitive to changes in preload; however, the MSVR var-ied directly with increases in afterload. The data aresummarized in figures 3 and 4.
DiscussionThe two principal findings of this study are (1) the
MSVR obtained from a single ventricular beat is an
300r
200 F
17/AO
U1look
0
o Controla Potentiated
20 40VOLUME (ml)
FIGURE 1. End-systolic stress-volume relationships generated underdifferent loading conditions for control and potential beats. The slope.termed fiber Emax, was increased by PESP of inotropic state while thevolume intercept, Vo, was unaltered.
TABLE 3Fiber Emax and Vo (mean + SD) for control (C), potentiated(PESP), and volume-loaded beats
Control PESP Volume
Fiber Emax 9.24 + 2.15 13.93 + 3.24A 1 1.24 + 4.63Vo 13.9± 1 1.1 14.1 ± 12.3 17.5 + 14.8A
ASignificant (p < .05) difference from control by ANOVA.
index of inotropic state that is insensitive to changes inmyocardial length but is sensitive to changes in after-load, and (2) when examined over a range of end-systolic loads, inotropic stimulation increases fiberEmax without altering the extrapolated Vo.
Estimation of contractile function in chronicallyoverloaded ventricles has been difficult because of theunavailability of a load-independent index of contrac-tile function. Hemodynamic parameters measured dur-ing the preejection phase of contraction, such as themaximum left ventricular dP/dt, are sensitive to alter-ations in preload. Ejection-phase parameters such asejection fraction and velocity of circumferential fibershortening (Vcf) are sensitive to alterations in after-load.1455Emax, based on the relationship betweenpressure and volume at end-systole, has recentlygained acceptance as an index that is sensitive to ino-tropic state and relatively insensitive to loading condi-tions. ]-3
Ventricular afterload can be well characterized byimpedence spectra'6 that relate instantaneous pressureto instantaneous flow. Impedence, however, does nottake into account the interrelationship between ventric-ular wall thickness, chamber dimensions, and pressurethat may affect load at the myocardial fiber level.4Thus, end-systolic or other indexes of contractile statederived with the use of pressure as a measure of after-load may be normal or higher than normal in hypertro-phied ventricles when contractile performance per unitmass of myocardium is actually depressed.'7 For thisreason, stress-volume relationships are preferred topressure-volume relationships for use in the compari-son of contractile state between ventricles having dif-ferent thickness-dimension ratios.
Although the end-systolic pressure-volume relation-ship has been evaluated extensively, there are few re-ports regarding the influence of inotropic changes onthe end-systolic stress-volume relationship. Positiveinotropic interventions generally produce an increasein slope but no change in the Vo when pressure is usedas a measure of end-systolic load. However, whenstress has been used as a measure of load, an increasein Vo with no significant change6 or even an increase"
650
EC-)
CQ1-.
-W
cncn
U-)
__j
CIRCULATION
by guest on April 17, 2017
http://circ.ahajournals.org/D
ownloaded from
LABORATORY INVESTIGATION-VENTRICULAR PERFORMANCE
o Control (MSVR = 5.43) 300a Potentioted (MSVR '6.43) 250
60 20 40 60 0 20 40VOLUME (ml) VOLUME (ml)
FIGURE 2. MSVR was increased by PESP (left), but was also sensitive to increased afterload (right). Augmentation of preload,
with afterload held constant, did not alter MSVR (center).
in slope has been noted in ventricles in which there ischronic overload hypertrophy, suggesting a shift in thestress-volume relationship to larger volumes with de-pression of the inotropic state. Borow et al.'9 havelikewise shown a parallel shift in the end-systolicstress-dimension relationship, with a decrease in end-systolic diameter, for any stress, after short-term ino-tropic intervention in humans. Weber et al.20 demon-strated alteration of the slope of the force-lengthrelationship in the isolated dog heart with an indetermi-nate change in the length intercept. The present dataindicate that the stress-volume relationship responds to
inotropic stimulation, as does the pressure-volume'-'relationship, with an increase in fiber Emax and no
significant change in Vo.
LU.
-J
C>C -
crLU'
C),Cf)
LLJ
cncn
cc
F--<Dcn E
H-->Co
er)LU
40
30
20
10
0
200
150
' 100
50
0
The significance of the increase in Vo that occurredafter infusion of dextran-nitroprusside in our study isuncertain, but may be related to the inverse correlationof Vo with resistance noted by Maughan et al.',2 whostudied pressure-volume relationships in excised ca-
nine ventricles connected to a servopump system.These investigators observed deficits in pressure forany given end-systolic volume (i.e., a parallel shift tothe right) for beats with large end-diastolic volumesand low resistances compared with those with smallerend-diastolic volumes at higher resistances. The vis-coelastic property of muscle, termed creep, may possi-bly account for such parallel shifts at a constant ino-tropic state in their study2' and in ours.
Determination of Emax requires repeated measure-
ments of end-systolic ventricular volume over a widerange of systolic pressures. This is difficult in patientsin whom hemodynamics are already abnormal, par-
ticularly those with critical aortic stenosis.22 Someinvestigators have therefore used either ventricularpressure or wall stress and ventricular volume at end-systole under basal conditions as a practical alternative
8
7
c>
C PESP VL PL
FIGURE 3. Preload was measured as end-diastolic volume (top) andafterload was measured as end-systolic stress (bottom). *p < .05.
Vol. 72, No. 3, September 1985
6
4
3
2
\0.
I. ~~~~~~0~
I p<0.05 I pNS IC PESP C VL
/
0-
p< 0.05
C PL
FIGURE 4. MSVR was increased by PESP and pressure loading (PL),but not by volume loading (VL).
651
E
c-a
V)LaccI-
300 -
250 -
200
150 _
100 _
50 _
000
.
5 F
by guest on April 17, 2017
http://circ.ahajournals.org/D
ownloaded from
WISENBAUGH et al.
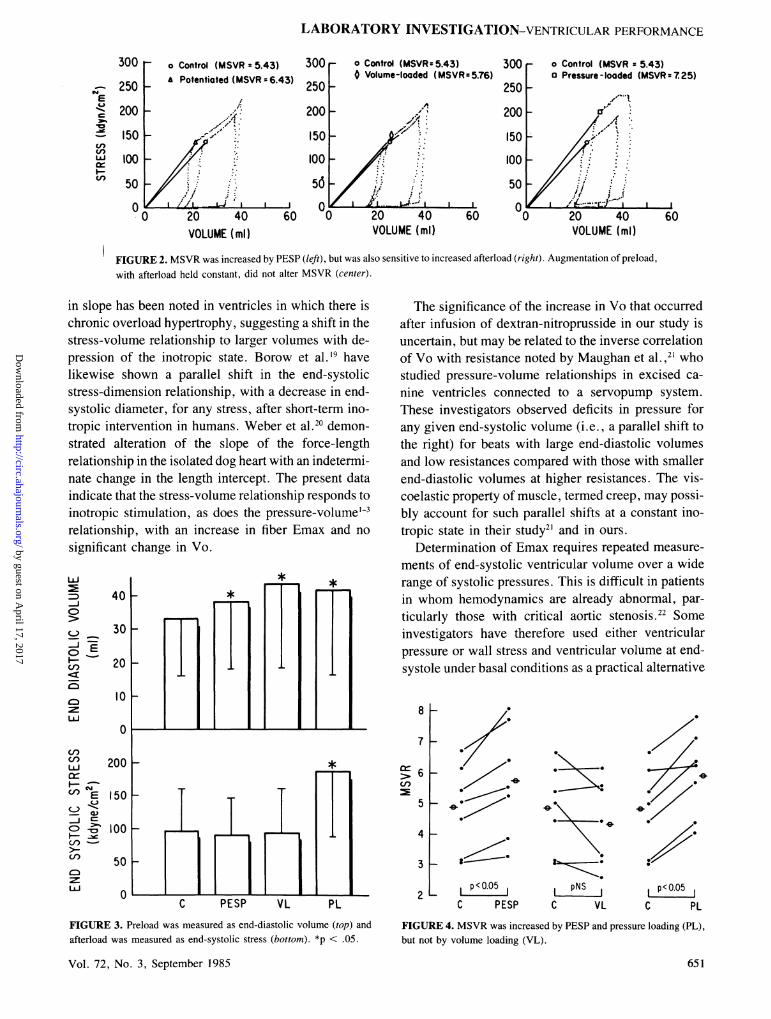
to measuring Emax in disease states associated withabnormal ventricular size and loading conditions.7-9The ratios of pressure to volume23 or stress to volume24at end-systole have been presumed, but not proven, tobe sensitive to contractile state and independent ofpreload and afterload. Others25 have used the slope ofthe relationship of stress to volume during late systolefor a single beat to estimate contractile state, but thisrelationship is affected by afterload.'6 The results ofour animal studies demonstrate that, although MSVRis unaltered by short-term changes in preload and issensitive to short-term inotropic interventions, this ra-tio also changes in direct proportion to short-termchanges in afterload. This is illustrated in figure 5,which also illustrates that the magnitude by whichMSVR underestimates fiber Emax depends both on thevalue of afterload and the magnitude of Vo, sinceMSVR assumes Vo to be zero.Thus, a reduced MSVR could be the result of either
a depressed inotropic state or reduced afterload. Forexample, in patients with conditions such as acute mi-tral regurgitation, MSVR could be depressed as a re-sult of reduced afterload despite the presence of a nor-mal iniotropic state. Conversely, increased afterload inpatients with decompensated aortic stenosis or regurgi-tation could partially mask the effects of impaired ino-tropic state on the MSVR ratio. However, because thecomputation of ventricular stress provides a means tonormalize for abnormal wall thickness and chamberdimensions, this preload-independent index may moreaccurately assess contractile state in subjects withchronically overloaded ventricles than do traditionalindexes of contractility, providing that afterload is notsignificantly altered from normal.
Limitations of the study. A potential pitfall in the use
of the stress-volume relationship to estimate contrac-tile function is related to selection of the time in thecardiac cycle during which it is measured. Severaldefinitions of end-systole have been proposed. Thetime at which ventricular volume reaches a minimumhas been traditionally used; however, Sagawa' andMaughan et al.21 have noted that coincidence of end-ejection, as indicated by minimum ventricular volumeor dicrotic notch, with maximal elastance is circum-stantial. These investigators have recently derivedEmax using the point in each cardiac cycle at which thepressure-volume ratio reaches maximum" as an alter-native to searching pressure-volume regression lines atfrequent intervals during the cardiac cycle for themaximum value. ' Computer analysis of stress-volumeloops in our dogs usually showed that this point in eachcardiac cycle very nearly coincided in time with thetime of fiber Emax for the series of loops. However, ina few animals it was noted that, when impedence toejection was markedly reduced by nitroprusside, theMSVR for the loops with the lowest load occurredmore near the onset of ejection than the end of ejection.As can be seen in figure 5, the rapid decrease in stressduring ejection produced by nitroprusside caused thestress-volume ratio to be slightly greater at a time earli-er in the loop than at the time of Emax or end-ejection.In this situation, the stress-volume ratio at end-ejec-tion8 would be lower, and underestimate fiber Emax bya greater amount, than would MSVR.
Pure alterations in myocardial length, which hasbeen termed preload, are difficult to produce in situbecause of the alterations in stroke volume and load (orafterload) that result. We attempted to minimize in-creases in afterload that accompany increases in pre-load by using nitroprusside so that the influence of a
NCVEC-L
-C
U)LU.W:F-
150
100
50
20VOLUME (ml)
Dog 438
MSVRo 5.53o 7.46
20VOLUME (ml)
FIGURE 5. Fiber Emax and Vo as described in the methods section. MSVR for each loop fell very close to the regression line.
With nitroprusside-induced reduction in afterload, stress fell rapidly during ejection so that for some beats, such as the one
designated by the open circle, the MSVR was found earlier during systole.
200r Dog 4380N-E
1-o
LiiW:I-
150
100
50
652 CIRCULATION
by guest on April 17, 2017
http://circ.ahajournals.org/D
ownloaded from

LABORATORY INVESTIGATION-VENTRICULAR PERFORMANCE
relatively pure length alteration on MSVR could beexamined. Likewise, an increase in afterload results inan increase in end-diastolic length if preload reserve28has not already been exhausted. Thus, we were unableto produce pure alterations in afterload, but since rela-tively pure changes in preload had no significant effecton MSVR, it can be assumed that the increase inMSVR with aortic constriction was a result of aug-mented afterload.A variety of methods have been used for measuring
ventricular volume. Isolated heart preparations'-'probably allow the most accurate determination ofventricular volume. Area-length methods of analysisof radiographic images and minor-axis measurementsfrom M mode echocardiograms have been used exten-sively in humans. Although the technique based onsonomicrometric measurement of left ventricular ma-jor and minor axes used in the present study has beenrecently validated,' l0 29 the computation of volume withan elliptical model is probably less accurate than meth-ods in which the excised heart is used, since the latterdoes not require such geometric assumptions. Howev-er, ultrasonic techniques have the advantage of allow-ing continuous measurements of cardiac dimensions insitu without the undesirable effects of contrast agents.
In summary, the MSVR measured from a singleventricular beat is sensitive to the inotropic state and isinsensitive to preload; however, the sensitivity of thisindex to afterload limits its usefulness as a practicalindex of contractile function. The slope of the end-systolic stress-volume relationship, or fiber Emax,which is increased by inotropic stimulation, accounts
for varied afterload over multiple beats, and is there-fore a more reliable measure of contractile functionthan the MSVR when myocardial load is abnormal.
The secretarial assistance of Lynne Cornish is gratefully ac-knowledged, as are the thoughtful comments of Dr. Blase Cara-bello during preparation of the manuscript.
References1. Sagawa K: The end-systolic pressure-volume relation of the ventri-
cle: definition, modifications and clinical use. Am J Cardiol 40:748, 1977 (editorial)
2. Sagawa K, Suga H, Shoukas AA, Bakalar KM: End-systolic pres-sure/volume ratio: a new index of ventricular contractility. Circula-tion 63: 1223, 1981
3. Suga H, Sagawa K, Shoukas A: Load independence of the instanta-neous pressure-volume ratio of the canine left ventricle and effectsof epinephrine and heart rate on the ratio. Circ Res 32: 314, 1973
4. Mirsky I: Left ventricular stresses in the intact human heart.Biophys J 9: 189, 1969
5. Hood WP, Rackley CE, Rolett EL: Wall stress in the normal andhypertrophied human left ventricle. Am J Cardiol 22: 550, 1968
6. Wisenbaugh T, Allen P, Cooper G, Holzgrefe H, Beller G, Cara-bello B: Contractile function, myosin ATPase activity and isoen-
zymes in the hyprtrophied pig left ventricle after a chronic progres-sive pressure overload. Circ Res 53: 332, 1983
7. Carabello BA, Spann JF: The uses and limitations of end-systolicindexes of left ventricular function. Circulation 69: 1058, 1984
8. Carabello BA, Nolan SP, McGuire LB: Assessment of preoper-ative left ventricular function in patients with mitral regurgitation:value of the end-systolic wall stress-end-systolic volume ratio.Circulation 64: 1212, 1981
9. Osbakken M, Bove AA, Spann JF: Left ventricular function inchronic aortic regurgitation with reference to end-systolic pressure,volume and stress relations. Am J Cardiol 47: 193, 1981
10. Rankin JS, McHale PA, Arentzen CE, Ling D, Greenfield JC,Anderson RW: The three-dimensional dynamic geometry of the leftventricle in the conscious dog. Circ Res 39: 306, 1976
11. Miller AR: Pascal programs for scientists and engineers. Berkeley,CA, 1981, Sybex
12. Hugenholtz PG, Kaplan E, Hull E: Determination of left ventricu-lar wall thickness by angiocardiography. Am Heart J 78: 513, 1969
13. Kono A, Maughan WL, Sunagawa K, Hamilton K, Sagawa K,Weisfeldt ML: The use of left ventricular end-ejection pressure andpeak pressure in the estimation of the end-systolic pressure-volumerelationship. Circulation 70: 1057, 1984
14. Mahler F, Ross J, O'Rourke RA, Covell JW: Effects of changes inpreload, afterload and inotropic state on ejection and isovolumicphase measures of contractility in the conscious dog. Am J Cardiol35: 626, 1975
15. Quinones MA, Gaasch WH, Alexander JK: Influence of acutechanges in preload, afterload, contractile state and heart rate onejection and isovolumic indices of myocardial contractility in man.Circulation 53: 293, 1976
16. Milnor WR: Arterial impedance as ventricular afterload. Circ Res36: 565, 1975
17. Huber D, Grimm J, Koch R, Krayenbuehl HP: Determinants ofejection performance in aortic stenosis. Circulation 64; 126, 1981
18. Reichek N, Laskey W, Fink L, Sutton MSJ, Unterecker W, Hirsh-feld: Relationships of left ventricular end-systolic mechanics toejection fraction. J Am Coll Cardiol 1: 664, 1983 (abst)
19. Borow KM, Green LH, Grossman W, Braunwald E: Left ventricu-lar end-systolic stress-shortening and stress-length relations in hu-mans. Am J Cardiol 50: 1301, 1982
20. Weber KT, Janicki JS, Hefner LL: Left ventricular force-lengthrelations of isovolumic and ejecting contractions. Am J Physiol231: 337, 1976
21. Maughan WL, Sunagawa D, Burkhoff D, Sagawa K: Effect ofarterial impedance changes on the end-systolic pressure-volumerelation. Circ Res 54: 595, 1984
22. Mehmel HC, Schwarz F, Ruffmann K, Manthey J, von OlshausenK, Kubler W: End-systolic pressure-volume and end-systolicstress-volume relationships in patients with aortic stenosis and withnormal valvular function. Basic Res Cardiol 78: 338, 1983
23. Ramanathan KB, Knowles J, Connor MJ, Tribble R, Kroetz FW,Sullivan JM, Mirvis DM: Natural history of chronic mitral insuffi-ciency: relation of peak systolic pressure/end-systolic volume ratioto morbidity and mortality. J Am Coll Cardiol 3: 1412, 1984
24. Gash AK, Carabello BA, Cepin D, Spann JF: Left ventricularejection performance and systolic muscle function in patients withmitral stenosis. Circulation 67: 148, 1983
25. Pouleur H, Rosseau MF, van Eyll C, Mechelen HV, Brasseur LA,Charlier AA: Assessment of left ventricular contractility from latesystolic stress-volume relations. Circulation 65: 1204, 1982
26. Colan SD, Borow KM, Gamble WJ, Sanders SP: Effects of en-
hanced afterload (methoxamine) and contractile state (dobutamine)on left ventricular late-systolic wall stress-dimension relation. AmJ Cardiol 52: 1304, 1983
27. Maughan WL, Shoukas AA, Sagawa K, Weisfeldt ML: Instanta-neous pressure-volume relationship of the canine right ventricle.Circ Res 44: 309, 1979
28. Ross J: Afterload mismatch and preload reserve: a conceptualframework for the analysis of ventricular function. Prog Cardio-vasc Dis 18: 255, 1976
29. Sodums MT, Badke FR, Starling MR, Little WC, O'Rourke RA:Evaluation of left ventricular contractile performance utilizing end-systolic pressure-volume relationships in conscious dogs. Circ Res54: 731, 1984
Vol. 72, No. 3, September 1985 653
by guest on April 17, 2017
http://circ.ahajournals.org/D
ownloaded from

T Wisenbaugh, G Yu and J Evansindex of contractile state.
The superiority of maximum fiber elastance over maximum stress-volume ratio as an
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1985 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.72.3.648
1985;72:648-653Circulation.
http://circ.ahajournals.org/content/72/3/648the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on April 17, 2017
http://circ.ahajournals.org/D
ownloaded from