Embed Size (px)
Citation preview

Pergamon
J. Behov. The,. & Exp. Psychlot. Vol. 24, No. 4, pp. 2X9-299.1993. Elsevier Saence Ltd
Printed in Great Britain OCO-7916l93 $6.00 + 0.00
00057916(93)EOOlO-5
THE STRUCTURE OF FUNDAMENTAL FEARS
STEVEN TAYLOR
Department of Psychiatry, University of British Columbia
Summary - Reiss’s expectancy theory states that panic attacks, phobias, and other fear reactions arise from three fundamental fears (sensitivities): anxiety sensitivity, fear of negative evaluation, and injury/illness sensitivity. The present study examined two central aspects of the theory: (1) the assumption that fundamental fears are factorially distinct, and (2) the proposition that fundamental fears account for variance in other forms of fear and in trait anxiety. Measures of fundamental fears, common fears, and trait anxiety were administered to 100 community volunteers. The results supported Reiss’s theory; the fundamental fears were factorially distinct, minimally intercorrelated, and accounted for significant proportions of variance in measures of other fears and trait anxiety. Specific and conceptually meaningful links were found between fundamental fears and common fears.
In an effort to develop a comprehensive yet parsimonious theory of individual differences in fear, Reiss (1987, 1991; Reiss & McNally, 1985) proposed that panic attacks, phobias, and other fear reactions arise from three fundamental fears (sensitivities): anxiety sensitivity, fear of negative evaluation, and injury/illness sensitivity. Anxiety sensitivity is the fear of anxiety symptoms arising from beliefs that anxiety has harmful somatic, psychological, or social consequences. Fear of negative evaluation is a concept drawn from the work of Watson and Friend (1969), and refers to apprehension and distress about receiving negative evaluations from others, expectations that others evaluate oneself negatively, and avoidance of evaluative situations. Injury/illness sensitivity refers to fears of injury, illness, and death.
Reiss (199 1, and personal communication, June, 1991) used two criteria to define these fears as fundamental; (1) they are fears of inherently noxious stimuli, and (2) other, “common” fears can be logically reduced to them. Reiss (1991)
provided the following account of the logical relationship between fundamental fears and common fears:
The distinction is suggested by an analysis of the rational relationships among different fears. Fundamental fears provide reasons for fearing a wide range of stimuli, whereas ordinary fears do not have this characteristic. For example, consider the rational relationships among three different fears: (a) the fear of snakes; (b) the fear of heights; and (c) the fear of anxiety. Fears of snakes and heights are rationally unrelated to one another in the sense that having one of the fears is not a reason for having the other fear. It makes no sense for a person to say, ‘I am afraid of heights because I am afraid of snakes.’ On the other hand, the fear of anxiety is rationally related to the fear of snakes and heights. A rational person might say, ‘I am afraid of snakes and heights because I am afraid I would have a panic attack if I encountered those stimuli.’ A person who is unusually afraid of. the possibility of a panic attack [i.e., has high anxiety sensitivity] holds a reason for potentially fearing snakes, heights, or any other situation that might be expected to lead to panic (p. 147, emphases in original).
In support of Reiss’s theory, studies have shown that simple phobics and agoraphobics often report they are frightened of stimuli such as harmless animals or air travel because of fears of
Requests for reprints should be addressed to Steven Taylor, Department of Psychiatry, 2255 Wesbrook Mall, University of British Columbia, Vancouver, B.C., Canada, V6T 2Al.
289

290 STEVEN TAYLOR
anxiety, illness/injury, or negative evaluation (Gursky & Reiss, 1987; McNally & Louro, 1992; McNally & Steketee, 1985).
By postulating three fundamental fears, Reiss’s theory assumes that these fears are distinct from one another; if they were not distinct then it would be more parsimonious to postulate a smaller set of fundamental fears. As described above, the theory also states that fundamental fears contribute to other, “common” fears. A related deduction is that the fundamental fears can account for variance in trait anxiety. Trait anxiety (anxiety proneness) is the tendency for stimuli to evoke anxiety in an individual (Spielberger, 1983). Reiss’s theory states that the intensity of fundamental fears will increase the likelihood of acquiring common fears:
People who are afraid of anxiety should develop a fear of any situation in which there is even a small chance/expectation of becoming anxious; because there are many such situations, people who are extremely sensitive to anxiety should develop fears of many situations. A similar analysis holds for injury sensitivity and sensitivity to negative evaluation (Reiss, 1991, p. 147).
Thus, people with intense fundamental fears will be made anxious by a variety of stimuli, and will tend to display high levels of anxiety proneness or trait anxiety.
The purpose of the present study is to evaluate these central aspects of Reiss’s theory. Two questions will be addressed: (1) Are the fundamental fears factorially distinct? (2) Can they account for significant proportions of variance in common fears and in trait anxiety? In the remainder of this article I review the relevant published literature and then report an empirical study designed to address these questions.
Are Fundamental Feurs Factorially Distinct?
There has yet to be a published study to directly address this question. However, a study by Reiss, Peterson, and Gursky (1988), although intended for other purposes, provides suggestive results. These investigators analyzed a pool of items from the Anxiety Sensitivity Index (ASI: Peterson & Reiss, 1987; Reiss, Peterson, Gursky, & McNally, 1986) and the Fear Survey Schedule-II (FSS-II:
Geer, 1965). The AS1 is a 16-item self-report measure of the fear of anxiety (anxiety sensitivity) (Peterson & Reiss, 1987). The FSS-II is a 5 1 -item self-report inventory assessing a range of fears, such as fears of harmless animals, fears of illness and injury, social fears, fears of agoraphobic situations, and so forth.
Reiss et al.‘s (1988) factor analysis yielded three factors, corresponding to each of the fundamental fears. While this result offers some support for the distinction among fundamental fears, there are problems with Reiss et al.‘s analysis. Of the 51 FSS-II items and 16 AS1 items, only 28 (42%) had salient loadings on any factor. A total of 39% of FSS-II items and 50% of ASI items failed to load on any factor. This indicates that the factor analysis was performed incorrectly in that an insufficient number of factors were extracted (Gorsuch, 1983; Harman, 1976). With the extraction and rotation of a greater number of factors, the pattern of loadings of the first three factors may change (Velicer & Jackson, 1990). Thus, it cannot be concluded that the results of Reiss et al. (1988) unequivocally support the distinction among the fundamental fears.
Even if the pool of AS1 and FSS-II items were appropriately factored, the results still would pose problems for evaluating the distinction among fundamental fears. Reiss’s (199 1) theory proposes that fundamental fears account for ,var+iance in common fears. This suggests that fears are factorially organized in a hierarchic manner, with fundamental fears forming a set of first-order factors, and common fears forming a set of second-order factors. The AS1 is a measure of a fundamental fear, whereas the FSS-II assesses common fears and fundamental fears. Thus, the joint factoring of the AS1 and FSS-II items may yield factors consisting of a mix of common fears and fundamental fears.
Comrey (1978) argued that a factor analytic investigation is most appropriate when one has reasonably pure measures of the hypothesized factors. If the postulated factor structure exists in the data, then this method provides the best way of revealing it. Thus, the question of whether fundamental fears are factorially distinct is best

Fundamental Fears 291
addressed by factoring items that only assess the fundamental fears. One approach is to construct internally consistent scales for each fundamental fear, and then pool and factor the items from these scales. It is an empirical question as to whether or not the scales correspond to distinct factors. It may be that some fears are not distinct. For example, anxiety sensitivity and illness/injury sensitivity both pertain to fears of interoceptive stimuli, and so they may form a single factor.
Accounting for Variance in Common Fears and in
Trait Anxiety
Factor analytic investigations by Arrindell and colleagues have shown that there are four main dimensions of common fears: (1) social fears, (2) fears of injury, illness, blood, and surgical procedures, (3) animal fears, and (4) agoraphobia (Arrindell, Emmelkamp, & van der Ende, 1984; Arrindell, Pickersgill, Merkelbach, Ardon, & Cornet, 1991; Arrindell & van der Ende, 1986). These findings are robust; they have been replicated across gender, assessment instruments, and nationalities, and have been replicated with different statistical methods (i.e., exploratory and confirmatory factor analyses). The utility of Reiss’s theory depends on its ability to account for the variance in these dimensions of fear. To date, there has yet to be a comprehensive evaluation of the extent that fundamental fears can account for variance in common fears, although several studies have partly addressed this issue.
Reiss et al. (1986) administered the AS1 to two samples of college students and found that it accounted for 35-50% of variance in FSS-II total scores. Reiss et al. (1988, Study 2) reanalyzed these data and found that the AS1 and a measure of injury/illness sensitivity accounted for 21% and 34% of the variance, respectively, in responses to a short fear schedule. The latter assessed a variety of different fears. The sum of the sensitivity
measures accounted for 42% of the total variance.
McNally and Lorenz (1987) found that the AS1 accounted for 41% of the variance in the FSS-II total score in a sample of agoraphobics.
Few studies have examined whether the fundamental fears can account for specific dimensions of common fears. Watson and Friend (1969) found the fear of negative evaluation accounted for lO-26% in variance of social fears, such as fears of writing or eating in public.* Similar results were reported by Leary (1983). McNally and Lorenz (1987) found the ASI accounted for only 4% of variance in responses to the agoraphobia subscale of the Fear Questionnaire (Marks & Mathews, 1979). However, this is likely to be an underestimation due to severe range restriction (all subjects were agoraphobic).
In summary, there is some evidence that the three fundamental fears can account for significant proportions of variance in common fears. However, there has yet to be a comprehensive study of the joint contribution of the fundamental fears to each of the major dimensions of common fears. This was addressed in the present study. In addition, the predictive power of the fundamental fears was assessed by determining the amount of variance they can account for in trait anxiety (anxiety proneness), since Reiss’s theory predicts that fundamental fears should contribute to anxiety proneness.
Method
Subjects
The aims of this study were addressed by factor analytic, correlational, and regression analyses, and so it was necessary to obtain a wide range of responses to the various measures. To this end, 100 subjects were recruited by advertisements in a
*These results indicate that fear of negative evaluation is not equivalent to fears of social stimuli. Fear of negative evaluation is a general tendency to catastrophically appraise negative evaluation, and, consequently, to become anxious at the prospect of negative evaluation. Social fears, by comparison, are fears of situations or activities in which the individual is under social scrutiny. See Watson and Friend (1969) for further details on the conceptual and empirical distinction between fear of negative evaluation and social fears.

292 STEVEN TAYLOR
local newspaper and advertisements placed on campus of the University of British Columbia. The sample was 65% female with a mean age of 28 years (SD = 10 years; range 18-65 years). Most (87%) were single and 75% were Caucasian. With regard to education, 5% had less than Grade 12, 20% completed Grade 12, and 75% had partial or completed university education. Half were students. 18% were unemployed, 32% were in full or part-time employment.
Anxiety .sensitivity index. Anxiety sensitivity was measured by the AS1 (Peterson & Reiss, 1987) which contains 16 items. Subjects rate the extent that they agree with each item by selecting one of 5 points on a Likert scale (0 = very little and 4 = very much).
Fear qf negatitle evaluation. Subjects completed a 12-item version of the Fear of Negative Evaluation Scale (FNE: Leary, 1983). This was used in place of the original 30-item version (Watson & Friend, 1969) because the former is more efficient, has almost identical psychometric properties to the original, and is highly correlated with the original (r = .96: Leary, 1983). To maintain consistency with the other sensitivity measures, subjects rated the extent that they agreed with each FNE item. This represents a minor departure from Leary’s (1983) response format, which required subjects to rate the self-descriptiveness of each item. This modification also required some minor changes in item wording in order to improve comprehension, and required that all items were scored in the same direction (i.e., reverse-scored items were reworded).
Illness/injury sensitivity index. In the only previous study to attempt to measure illness/injury sensitivity, Reiss et al. (1988) used the blood- injury items from the FSS-II. This approach confounds the fear of injury/illness with stimuli that may be secondary to this fear (e.g., fears of hospitals, doctors, or medical odours). This
problem was avoided in the present study by developing an Illness/injury Index (ISI) that assesses the fear and catastrophic appraisal of illness or injury (e.g., “I am frightened of being injured, ” “I get scared when I think I’m coming down with an illness”). The IS1 contains six items pertaining to the fear of illness and five items referring to the fear of injury. The items are rated on the same 5-point scale as the AS1 and FNE. The IS1 does not assess the fear of stimuli that are likely to be secondary to illness/injury sensitivity, such as fears of doctors, cemeteries, hypodermic needles, and the like.
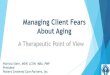
Items of the ISI, FNE, and AS1 are presented in Table 1. The items from these scales were pooled to create a single scale, called the Sensitivity Index. The items were prefaced by instructions for subjects to rate the extent they agreed with each item.
The ASI, FNE, and IS1 each had acceptable internal consistencies (CLS > .80). It is important to note that this does not mean that they are necessarily distinct from one another; i.e., internal consistency does not imply discriminative validity. The scales were developed as face valid measures of the constructs of interest. In the process of scale development, items were not selected so that they were correlated with one fundamental fear and not with others. That is, the ASI, FNE, and IS1 were not forced to be uncorrelated with one another. Thus, the items from these scales are appropriate for the factor analysis used in the present study.
Fear survey schedule. Subjects completed a modified version of the Fear Survey Schedule-III (FSS-III: Wolpe & Lang, 1964). Previous studies (e.g., Arrindell et al., 1984, 1991) have shown that the FSS-III is composed of five factors: (1) agoraphobia (13 items), (2) social fears (13 items), (3) fears of bodily injury and illness (12 items), (4) fears of harmless animals (6 items), and (5) fears of sexual and aggressive stimuli (8 items). The fear of sexual/aggressive stimuli factor has a heterogeneous items content, and is the least replicable of the FSS-III factors (Arrindell et al., 1984; Taylor & Rachman, 1992). This scale was dropped from the present version of the FSS-III,

Table 1
Fundamental Fears
Factor Loadings and Communalities (h”) for the 3-Factor Solution
293
Factor
Scale Item I II III h’
FNE
FNE FNE FNE FNE
FNE FNE FNE FNE
FNE FNE FNE ASI AS1 IS1 IS1 IS1 ISI IS1 IS1 IS1 IS1 IS1 IS1 AS1 IS1 AS1 AS1 AS1 AS1 AS1
AS1 AS1 AS1 AS1 AS1 AS1 ASI AS1
Sometimes I think I am too concerned with what other people think of me .91* I worry about what kind of impression I make on people .87* I am afraid that people will find fault with me .a7* 1 am concerned about other people’s opinions of me .85* When I am talking to someone, I worry about what they may be thinking of me .85* I am afraid that others will not approve of me .84* I am usually worried about the kind of impression I make .84* I am frequently afraid of other people noticing my shortcomings .84* I worry what other people will think of me even when I know it doesn’ make any difference .83* It bothers me when people form an unfavourable impression of me .80* I often worry that I will say or do the wrong things .64* If I know that someone is judging me, it tends to bother me .64* It is important for me not to appear nervous .45* It is important to me to stay in control of my emotions .32* I am frightened of being injured .06 The thought of injury terrifies me .I1 I worry about becoming physically ill .oo The thought of physical illness scares me .I6 I worry about being injured .14 1 worry that I might get a serious physical illness in the future -.02 It would be awful to be injured in any way .06 It would be awful to have a serious physical illness .Ol I worry about my physical health -.06 I get scared if I think I am coming down with an illness .31* It scares me when I am nauseous .20 1 can’t stand the thought of being injured .29 It scares me when my heart beats rapidly -.24 It scares me when I feel faint -.08 It embarrasses me when my stomach growls .21 It scares me when I am unable to keep my mind on a task .I9 When I notice that my heart is beating rapidly, I worry I might have a heart attack -. 16 When my stomach is upset, I worry that I might be seriously ill -.03 When I cannot keep my mind on a task, I worry that I might be going crazy .29 Unusual body sensations scare me -.04 When I am nervous, I worry that I might be mentally ill .27 It scares me when I am nervous .31* It scares me when I become short of breath .04 Other people notice when I feel shaky .I8 I1 scares me when I feel “shaky” (trembling) .04
-.I2 -.Ol .78 .04 .07 .82 .04 -.02 .76 .02 .04 .75
-.12 .14 .I5 .04 .03 .75 .09 -.03 .75
-.07 .I0 .72
-.06 .05 .69 .21 -.14 .73 .12 .I2 .55 .I5 .06 .53 .09 -.03 .23 .I3 .04 .I6 .84* .03 .76 .76* -.08 .61 .16* .19 .68 .75* .04 .68 .69* .04 .58 .68* .19 .56 .67* -.20 .45 .58* -.29 .34 .55* .31* .52 .55* .08 .54 .54* .09 .45 .53* -.02 .45 .51* .32* .38 .47* .29 .35 .35* .I2 .26
-.I5 .68* .52
-.03 .66* .39 .29 .61* .54
-.13 .61* .5 1 .22 .59* .45
-.15 .57* .44 -.03 .55* .49
.I7 .49* .33
.03 .47* .32
.26 .46* .36
Note. FNE = Fear of Negative Evaluation, IS1 = Injury Sensitivity Index, AS1 = Anxiety Sensitivity Index. *Salient (2 .30).
and the remaining factors formed subscales of the the social and blood-injury subscales were further four major dimensions of common fears. modified to reduce the possible overlap with the Additional items were generated for the animal measures of fear of negative evaluation and and blood-injury subscales so that each subscale injury/illness sensitivity. This was done by contained 13 items. This was done in order to ensuring that the items pertained to external enhance subscale reliability. The item contents of stimuli rather than internal states or interpretations

294 STEVEN TAYLOR
of situations (e.g., items such as “feeling criticized” and “failure” were deleted, and items such as “writing in public” were added). The blood-injury scale was modified by including only those items that do not overlap with ISI. Thus, items pertaining to fears of personal illness or injury were deleted, and items pertaining to fears of hospitals, cemeteries, medical odours, doctors, etc. were retained or added.? The agoraphobia subscale was modified by deleting items with low loadings on this factor (as determined by previous studies: Arrindell et al., 1984; Taylor & Rachman, 1992), and deleting items that blurred the distinction between agoraphobia and social fears. To maintain the subscale at 13 items, additional items were taken from the Mobility Inventory for Agoraphobia (Chambless, Caputo, Jasin, Gracely, & Williams, 1985).
Finally, the FSS-III instructions were modified by asking subjects to rate how anxious or fearful they are of each stimuli, using a 5-point scale; 0 = not at all, 4 = very much. In the original FSS-III, subjects rated how disturbed they were by each stimulus. The original version may be lacking in sensitivity since one may obtain a high score on the blood-injury scale because the stimuli are disturbing without being fear-evoking (e.g., such stimuli may evoke faintness or nausea but not necessarily fear or anxiety).
Trait unxiety. This was assessed by the trait version of the State-Trait Anxiety Inventory (STAI-T: Spielberger, 1983), which is a 20-item scale where subjects rate how they generally feel on a 4-point scale (1 = almost never, 4 = almost
always).
Procedure
Subjects provided informed consent and then completed the STAI-T followed by the FSS-III, and finally the Sensitivity Index. As mentioned, the latter consisted of items from the ASI, FNE,
and ISI. After completing the scales, subjects were debriefed and received an honorarium for participation.
Results
Items from the ASI, FNE, and IS1 were submitted to a principal components analysis with oblique rotation. The number of factors was selected according to two rules; the scree test (Cattell, 1966) and parallel analysis (Horn, 1965; Longman, Cota, Holden, & Fekken, 1989). These are among the most accurate factor-extraction rules (Zwick & Velicer, 1986). Following the recommendations of Longman et al. (1989), the mean and 95th percentile eigenvalues were used for the parallel analysis. Both extraction rules indicated a 3-factor solution, accounting for 54% of the variance. The factors had low correlations among one another, with rs ranging from .26 to .32. Table 1 shows the factor loadings and communalities (h2) for the 3-factor solution.
To facilitate interpretation, items in Table 1 are ordered according to the size of loading. Taking salient loadings as those 2 .30 (Gorsuch, 1983), the Table shows that each factor corresponds to one of the fundamental fears postulated by Reiss (1991). Each scale corresponds to a separate factor, with the exception of six AS1 items, which loaded on other factors. This is consistent with previous studies that have found that some AS1 items are questionable measures of anxiety sensitivity (Taylor, Koch, & Crockett, 1991: Taylor, Koch, McNally, & Crockett, 1992).
The magnitude of communalities (Table 1) indicates that the factors accounted for a substantial proportion of variance in most of the items. The magnitude of loadings shows that, in general, the salient items provided excellent measures of their respective factors. With regard to the stability (replicability) of the factor structure, the results of a series of Monte Carlo
;The distinction between illness/injury sensitivity and blood-injury fears is similar to the distinction between fear of negative evaluation and social fears. Illness/injury sensitivity pertains to the catastrophic appraisal and fear of personal injury or illness. In comparison, blood-injury fears pertain to external stimuli that are associated with illness or injury. Illness/injury sensitivity and blood-injury fears are correlated, although they are not equivalent constructs.

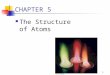
Table 2
Fundamental Fears 295
Zero-Order Correlations and Results of Regression Analyses
Predictors
Factor I Factor II Factor III (Fear of Negative Evaluation) (Illness/Injury Sensitivity) (Anxiety Sensitivity)
Dependent variable r P r P r P R’
Trait anxiety .44* .63* .lO .35* .23 .44* .41* Social fears .42* .61* .14 .31* .19 .40* .38* Agoraphobia .09 .28* .15 .31* .33* .45* .22* Animal fears .38* .57* .31* .51* .06 .28* .38* Blood-injury fears .I8 .40* .48* .62* .06 .27* .38*
*p < .Ol.
studies by Guadagnoli and Velicer (1988) indicate that if components possess four or more variables with loadings above .60, then the factor structure is likely to be stable, and is unlikely to change with an increase in sample size. The factors in Table 1 contain numerous loadings > .60, which suggests that the factor solution is likely to be stable.
To fully evaluate the relationship between fundamental fears and common fears, factor scores were computed and used in three types of analysis. First, the relationship between specific fundamental fears and specific common fears was assessed by zero-order (bivariate) Pearson correlations. Second, the relationship between specific fundamental fears and sets of common fears was examined by multiple regression analysis. Third, the relationship between sets of fundamental fears and sets of common fears was assessed by canonical correlation analysis. An alpha level of .Ol was adopted throughout these analyses to offset the increase in Type 1 error arising from the use of multiple significance tests.
Zero-order correlations (rs) and results for the regression analyses (l3s and R’s) are shown in Table 2. The regression analyses revealed that the fundamental fears were significant predictors of trait anxiety, F(3, 96) = 22.67, p < .OOOl, social fears, F(3, 96) = 19.71, p < .OOOl, agoraphobia, F(3, 96) = 9.04, p < .OOOl, animal fears, F(3,96) = 19.69, p < .OOOl, and blood-injury fears, F(3, 96) = 19.41, p < .OOOl. The fundamental fears accounted for significant proportions of variance
(22-41%), which supports Reiss’s theory. However, a substantial amount of variance was left unexplained, which suggests that other factors influence common fears and trait anxiety. This
issue will be taken up later. All l3 weights were significant (Table 2), which
indicates that all fundamental fears were significant predictors of all common fears and trait anxiety. However, as suggested by the pattern of significant zero-order correlations and magnitude of l3 weights, the fundamental fears differed considerably in their ability to account for variance in trait anxiety and common fears. Fear of negative evaluation (Factor I) was most strongly related to trait anxiety, social fears, and animal fears. Illness/injury sensitivity (Factor II) was most strongly related to animal fears and blood-injury fears. Anxiety sensitivity (Factor III) was most strongly related to agoraphobia. Table 2 further shows that illness/injury sensitivity is not synonymous with blood-injury fears, since a correlation of .48 indicates that the two types of fear have 23% of variance in common. Similarly, fear of negative evaluation is not synonymous with social fears, since the two had a correlation of .42, which indicates 18% of variance in common.
Canonical correlation analysis was conducted to identify links between sets of fundamental fears and sets of common fears. In this form of analysis, links between sets of variables are represented by a correlation between pairs of canonical variates. Each variate is a linear combination of variables within a given set. Statistical tests are used to

296
Table 3
STEVEN TAYLOR
Loudings md Cmonicnl Correlations for Canonical Vmiates
Loadings on Canonical Variate Pairs
Variable
Set I : Fundamental fears Factor I (Fear of negative evaluation) Factor II (Illness/injury sensitivity) Factor III (Anxiety sensitivity)
Set 2: Common fears Social fears Agoraphobia Animal fears Blood-injury fears
Canonical correlation between sets 1 and 2:
First Variate Pair Second Variate Pair
.53* -.56*
.49* .x7*
.20 -.40*
.82* -.46*
.57* -.I7
.85* .04
.81* .52*
.73 .40
Third Variate Pair
-.63* .07 .x9*
-.o I .X1”
-.25 .I0
.31
*Salient (2 .30).
determined the number of significant pairs of canonical variates. In the present analysis, each canonical variate is a linear combination of variables from either set 1 or set 2 (see Table 3 for the variables constituting each set). The first pair of canonical variates is a linear combination of variables from set 1 and a linear combination of variables from set 2. The variables are combined such that the correlation between sets is maximized (Hotelling, 1935). The second pair of canonical variates also is a linear combination of variables from set 1 and a linear combination of variables form set 2. The variables are combined such that the correlation between sets is maximized, providing the first variate pair is orthogonal to the second variate pair. Similarly, the third pair of canonical variates maximized the correlation between sets 1 and 2, providing the third variate pair is orthogonal to the first and second variate pairs. The loadings on variables in each variate pair (Table 3) indicate the importance of each variable in defining a given canonical variate. Thus, canonical variate pairs can be interpreted like factors. The major difference is that variate pairs do not represent a single dimension; they represent two linked dimen- sions.
The first pair of canonical variates was significant, F(12, 228) = 9.22, p < .0005, and so was the second pair of variates, F(6, 174) = 13.00,
p < .000.5. The third pair of canonical variates was marginally significant at the predetermined alpha level of .Ol: F(2, 88) = 4.65, p < .012. Table 3 shows the loadings for each variate pair, and the canonical correlation between the variates in each variate pair. These results replicate and extend the findings from the zero-order correlational analyses and multiple regression analyses, despite that fact they arose from different statistical procedures. The pattern of loadings for the first pair of variates indicates that fear of negative evaluation and illness/injury sensitivity are related to all common fears, suggesting a link between the two fundamental fears and general fearfulness. The loadings for the second variate pair indicate that illness/injury sensitivity, in the absence of other fundamental fears, is strongly associated with blood-injury fears. Loadings for the third variate pair shows that anxiety sensitivity, in the absence of fear of negative evaluation, is strongly associated with agoraphobia.
Discussion
This study used the ASI, FNE, and IS1 to examine the structure of fundamental fears. The scales are internally consistent and appear to be good measures of the constructs of interest. In the construction of the scales, they were not forced to

Fundamental Fears 297
be uncorrelated with one another, and so the factor analysis of their pooled items is an appropriate method for determining whether the fundamental fears are factorially distinct. The three fundamental fears were factorially distinct, which supports Reiss’s (1991) theory.
The fundamental fears accounted for significant proportions of variance in common fears and in trait anxiety. Fear of negative evaluation was related to social fears and animal fears. The latter finding is not unexpected since many animal phobics state that they are embarrassed about their “irrational” fears. Thus, the fear of negative evaluation appears to contribute to animal fears. Fear of negative evaluation also was related to general fearfulness and to trait anxiety, which suggests that fear of negative evaluation is the most important fundamental fear, at least in accounting for fears responses in our community sample.
Illness/injury sensitivity was related to animal fears, and particularly to blood-injury fears. The fact that illness/injury sensitivity was primarily related to blood-injury fears is not surprising, since fears of being injured or ill are likely to lead to the fear and avoidance of stimuli associated with illness or injury, such as hospitals, doctors, and cemeteries. Of greater interest is the finding that illness/injury sensitivity is related to animal fears. This provides empirical support for Reiss’s (1991) contention that fundamental fears are rationally related to common fears; e.g., if one is frightened of injury or illness, then it logically follows that one should also be frightened of potential sources of injury or illness, such as dogs, snakes, or spiders.
Anxiety sensitivity was specifically associated with agoraphobia. This is consistent with the fact that agoraphobic is often secondary to panic disorder, and panic disorder appears to arise from heightened anxiety sensitivity (McNally, 1990, 1993; Reiss, 1991; Taylor, Koch, & McNally, 1992). Lilienfeld, Jacob, and Turner (1989) suggested that anxiety sensitivity is simply a form of trait anxiety. This possibility was later refuted in several studies (see McNally, 1993, for a review). The present study found that trait anxiety
and anxiety sensitivity were weakly correlated, r = .23 (5% shared variance).
The fundamental fears accounted for 22-41% of the variance, leaving much variance unexplained. Unexplained variance may be due to other fundamental fears that have yet to be identified, although it is difficult to say what these might be. A more likely explanation is that unexplained variance was due to idiosyncratic factors in fear acquisition. That is, the individual’s particular learning history, including the frequency and intensity of aversive or traumatic experiences, plays a role in fear acquisition (Rachman, 1990). Thus, for example, fear of social stimuli may arise from fundamental fears and from one’s history of aversive social experiences.
Apart from the main effects of fundamental fears and learning history, it also may be that the intensity of common fears are strongly influenced by the interactions among fundamental fears and environmental events. That is, fundamental fears may be most likely to exert their effects in the context of a history of aversive life experiences. Aversive experiences with a given class of stimuli would facilitate the establishment of links between fundamental fears and these stimuli. To illustrate, intense illness/injury sensitivity is unlikely to contribute to fear of dogs in a person with a history of entirely pleasant experiences with dogs. Conversely, a person who has a history of aversive experiences with dogs may acquire a dog phobia, and this phobia will be inflated by illness/injury sensitivity because the aversive experiences with dogs will forge a powerful link between injury and dogs. In other words, intense illness/injury sensitivity (and other fundamental fears) amplify the fear-inducing effects of aversive life experiences.
These considerations suggest that the prevalence and intensity of common fears may be best predicted by three sets of variables; (1) fundamental fears, (2) aversive life experiences, and (3) internations between 1 and 2. This hypothesis merits future investigation.
It remains to be determined whether the present findings generalize to other samples. Given the logical nature of the links found between

298 STEVEN
fundamental fears and common fears, it seems likely that the pattern of results should generalize not only to other community samples, but also to clinical samples. Several studies (e.g., Arrindell et al., 1984, 1991) have shown that the factor structures of fear inventories generalize across clinical and normal populations. Our previous work (Taylor et al., 1991, 1992) demonstrates that the factorial structure of anxiety sensitivity is stable across clinical and nonclinical samples. Taken together, these results suggest that the factor structure in Table 1 also should generalize across samples.
Perhaps the most important issues for further investigation concern the definition and identification of “fundamental” fears, and the hierarchic organization of fears. Although the results support Reiss’s rationally-derived set of fundamental fears, it may be possible to generate other sets of fears that are even more fundamental. For example, anxiety sensitivity and illness/injury sensitivity may arise from fear of suffering or fear of death. Anxiety sensitivity arises from beliefs that anxiety symptoms have harmful psychological consequences (Reiss, 1991), which raises the question of whether anxiety sensitivity is secondary to fears of insanity or mental incapacitation. In future studies it would be useful to investigate the relationships among the fundamental fears and other possible basic fears, such as fears of suffering, death, and mental incapacitation.
Ackr~~~~lrdgements - This study was supported by grants from British Columbia Health Research Foundation and from the UBC Humanities and Social Sciences Program. The author would like to thank Eleny Goritsas for her assistance.
References
Arrindell, W. A., Emmelkamp, P. M. G., & van der Ende, J. (1984). Phobic dimensions: I. Reliability across samples, gender, and nations. Advances in Behaviour Research and Therapy, 6,207-254.
Arrindell, W. A., Pickersgill, M. J., Merckelbach, H., Ardon, A. M., & Cornet, F. C. (1991). Phobic dimensions: III. Factor analytic approaches to the study of common phobic fears; an updated review of findings obtained with adult
TAYLOR
subjects. Advances in Behaviour Research and Therapy, 13. 73-l 30.
Arrindell, W. A., & van der Ende, J. (1986). Further evidence for cross-sample invariance of phobic factors: Psychiatric inpatient ratings on the Fear Survey Schedule-III. Behaviour Research and Therapy, 24,289-297.
Cattell, R. B. (1966). The scree test for the number of factors. Multivariate Behavioral Research, I, 245-276.
Chambless, D. L., Caputo, Cl. C., Jasin, S. E., Gracely, E. J., & Williams, C. (1985). The Mobility Inventory for agoraphobia. Behaviour Research and Therapy, 23, 35- 44.
Comrey, A. L. (1978). Common methodological problems in factor analytic studies, Journal of Consulting and Clinical Psychology, 46,648-659.
Geer, J. H. (1965). The development of a scale to measure fear. Behaviour Research and Therapy, 3,45-53.
Gorsuch, R. (1983). Factor an&.&. Hillsdale, NJ: Erlbaum. Guadagnoli, E., & Velicer, W. F. (1988). Relation of samole
size to the stability of component patterns. Psychological Bulletin, 103, 265-275.
Gursky, D. M., & Reiss, S. (1987). Identifying danger and anxiety expectancies as components of common fears. Journal ff Behavior Therapy arzd Experimental Psvchiutr\: I& 3 17-324.
Harman, H. H. (1976). Modern factor analysis (3rd ed., rev.). Chicago: University of Chicago Press.
Horn, J. L. (1965). A rationale and test for the number of factors in factor analysis. Psyrhometrika, 30, 179-I 85.
Hotelling, H. (I 935). The most predictable criterion. Jourrml oq Educationul Psychology, 26, 139-142.
Leary, M. R. (1983). A brief version of the Fear of Negative Evaluation Scale. Personality and Social Psycholog) Bulletin, 9, 371-375.
Lilienfeld, S. O., Jacob, R. G., Turner, S. M. (1989). Comment on Holloway and McNally’s (1987) “Effects of anxiety sensitivity on the response to hyperventilation.” Journal of Abnormal Psychology, 98, 1 OO- 102.
Longman, R. S.. Cota, A. A., Holden, R. R., & Fekken, G. C. (1989). A regression equation for the parallel analysis criterion in principal components analysis: mean and 95th percentile eigenvalues. Multirtrriatr Behaviorcrl Rrsectrch, 24,59-69.
Marks, I. M., & Mathews, A. M. (1979). Brief standard self- rating for phobic patients. Behuviour Resecrrch cmd Therapy, 17,263-267.
McNally, R. J. (1990). Psychological approaches IO panic disorder: a review. Psychological Bulletin, 108. 403419.
McNally, R. J. (1993). Anxiety sensitivity is distinguishable from trait anxiety. In R. M. Rapee (Ed.), Current controversies in anxiet.v disorder reseccrch. New York: Guilford.
McNally, R. J.. & Lorenz, M. (1987). Anxiety sensitivity in agoraphobics. Journal of Behavior Therapy crtld E.xperimental Ps~chiutr~, 18, 3-l I
McNally, R. J., & Louro. C. E. (1992). Fear of flying in agoraphobia and simple phobia: Distinguishing features. Journal of Anxiety Disorders, 6, 3 19-324.
McNally, R. J., & Steketee, G. S. (1985). The etiology and maintenance of severe animal phobias. Behaviour Research and Therapy, 23,43lL435.
Peterson, R. A., & Reiss, S. (1987). Anxieq Sensitivit! hzdu

Fundamental Fears 299
manual. Palos Heights, IL: International Diagnostic Systems.
Rachman, S. (1990). Fear and courage. New York: Freeman. Reiss, S. (1987). Theoretical perspectives on the fear of
anxiety. Clinical Psychology Review, 7, 141-153. Reiss, S. (1991). Expectancy theory of fear, anxiety, and panic.
Clinical Psychology Review, 11, 141-153. Reiss, S., & McNally, R. .I. (1985). The expectancy model of
fear. In S. Reiss & R. R. Bootzin (Eds.), Theoretical issues in behavior therapy (pp. 107-121). New York: Academic Press.
Reiss, S., Peterson, R. A., Gursky, M., & McNally, R. J. (1986). Anxiety sensitivity, anxiety frequency, and the prediction of fearfulness. Behaviour Research and Therapy, 24, l-8.
Reiss, S., Peterson, R. A., & Gursky, M. (1988). Anxiety sensitivity, injury sensitivity, and individual differences in fearfulness. Behaviour Research and Therapy, 24, l-8.
Spielberger, C. D. (1983). Manual for the State-Trait Anxiery Inventory (Form Y). Palo Alto, CA: Consulting Psychologists Press.
Taylor, S., Koch, W. J., & Crockett, D. .I. (1991). Anxiety sensitivity, trait anxiety, and the anxiety disorders. Journal
of Anxiety Disorders, 5,293-3 11. Taylor, S., Koch, W. J., & McNally, R. J. (1992). How does
anxiety sensitivity vary across the anxiety disorders? Journal of Anxiety Disorders, 6, 249-259.
Taylor, S., Koch, W. J., McNally, R. J., & Crockett, D. J. (1992). Conceptualizations of anxiety sensitivity. Psychological Assessment, 4, 245-250.
Taylor, S., & Rachman, S. (1992). Fear and avoidance of aversive affective states: Dimensions and causal relations. Journal of Anxiety Disorders, 6, 15-26.
Velicer, W. F., & Jackson, D. N. (1990). Component analysis vs. common factor analysis: Some issues in selecting an appropriate procedure. Multivariate Behavioral Research, 25, l-28.
Watson, D., & Friend, R. (1969). Measurement of social- evaluative anxiety. Journal of Consulting and Clinical Psychology, 33.448457.
Wolpe, J., & Lang, P. J. (1964). A fear survey schedule for use in behavior therapy. Behaviour Research and Therapy, 2, 27-30.
Zwick, W. R. & Velicer, W. F. (1986). Comparison of five rules for determining the number of components to retain. Psychological Bulletin, 99,432442.