Embed Size (px)
Citation preview

The Strength-Duration Curve and Its Importancein Pacing Efficiency: A Study of 325 Pacing Leadsin 229 PatientsSTEPHEN COATES and BARNABY THWAITESFrom the Department of Cardiology, Wansbeck Ceneral Hospital, Ashington, Northumberland,the United Kingdom
COATES, S., ET AL.: The Strength-Duration Curve and its Importance in Pacing Efficiency: A Study of 325Pacing Leads in 229 Patients. Pacemaker battery life is dependant on programmable parameters, princi-pally pulse amplitude and puise duration. Higb factory default settings cause excessive current drain. Thestrength-duration curve relates pacing threshold to pulse duration. The most energy efficient pacing oc-curs at chronaxie, a value of pulse duration derived from the curve. Strength-duration curves were calcu-lated for 325 acutely implanted pacing leads. Chronaxie and rheobase were compared for atrial and ven-tricular leads. Chronaxie was compared with actual programmed pulse duration. There were 101 atrialand 224 ventricular leads, all passive fixation. The curve fit was good, (mean error ± SD) 0.024 ± 0.06 Vfor atrial curves and 0.008 ± 0.034 V for ventricular curves. Mean (± SD) atrial and ventricular chronax-ies were 0.24 ± 0.07 ms and 0.25 ± 0.07 ms. respectively. A "Z" value of 1.4 indicated that chronaxiesmight have been from tbe same population. Mean (± SD) atrial and ventricular rheoboses were 0.51 ± 0.2VandO.35 ±0.13 V, respectively. A "Z" valueof7.1 (P < 0.001) suggested atrial and ventricular rheobaseswere from differing populations. AU patients had factory defauU pulse durations ofO.45msorO.5ms, ex-ceeding acute chronaxie by a factor of two, thus, demonstrating suboptimal pacing. We conclude that un-derstanding the strength-duration curve is critical Sensible programming of other pacing functions opti-mizes longevity. Battery drain is reduced by programming pulse duration to cbronaxie with a doubling ofvoltage threshold at this point to achieve a safety margin. Further study of chronaxie drift with time is re-quired. (PACE 2000; 23:1273-1277)
pacing, pacemaker, strength-duration curve
IntroductionIt is probable that maximal pacemaker battery
life is not realized in the majority of paced pa-tients. This study illustrates the key position of thestrength-duration curve in pacing practice. Exces-sive energy drain from pacemakers leads to short-ened battery life with a consequent reduction intime to replacement of the pulse generator. Twoprincipal pacing waveform parameters, voltageand tlie pulse duration for which that voltage is ap-plied, account for a large proportion of that energydrain, longevity being inversely proportional tolead currnnt. These parameters are programmablein all modern pacemakers allowing for optimiza-tion of their settings. Factory defaults in those set-tings are high to provide safety margins for the risein threshold after implantation and are usually leftunchanged.^ The energy required for cardiac stim-ulation varies wilh pulse duration as a U-shaped
Address for reprints: Mr. Steve Coates, Medical School, Fram-lington Place. Newcastle upcjn Tyne NE2 4HH. UK. Fax: 44 (0)1B70 529452; e-mail: coates steve((f hotmail.com
Received July 27, 1999; revised December 20, 1999: acceptedlanuary 26. 2000.
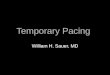
curve. The minimum of this curve is at chronaxie,which indicates the most efficient pulse durationfor stimulation. Chronaxie is defined as the pulseduration at twice the rheohase. Rheobase is thestimulation threshold at infinite pulse duration;that is, as pulse duration is increased there comesa value of voltage (or current) below which thresh-old will not fall. Lapique" in 1909 was the first todescribe the hyperbolic correlation between pulseduration and mean stimulus. Figure 1 shows an ex-ample of this hyperbolic strength-duration curvewith rheobase and chronaxie highlighted and theenergy curve superimposed.
Strength-duration curves can also be plottedas a linear function where the y-axis representsthe product of mean voltage and pulse durationand the x-axis is the pulse duration. From thisgraph derived by Weiss^ in 1901, the slope givesthe rheobase and the chronaxie is calculated fromthe y-intercept divided by the slope.
To set the pacing output stimulus to a pulseduration equal to chronaxie would then conserveenergy and prolong pulse generator longevity. Anadequate safety margin can be provided by settinga pulse amplitude of twice voltage threshold asmeasured at chronaxie.
PACE, Vul. 23 August 2000 1273

COATES, ETAL.
ChronaxiePuJse Duration
Figure 1. Energy and stimulus strength versus pulseduration. The horizontal axis is the pulse duration. Thevertical axis is the energy or stimulus strength delivered.Hheobase is shown as the lower hashed line and theupper-hashed line represents voltage (or current) attwice rheobase. The intersection of this value with thecurve defines chronaxie. An energy curve at topillustrates a nadir at chronaxie.
0.1 02 03 0-1 05 as 07 08 09Pulu Ourslion (m*)
1 11 12 13 14 15
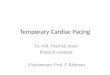
Figure2. Exampleofthe Weiss linear strength-durationcurve derived from data obtained from one of ourpatients. The crosses represent the four data pointscalculated as the product of mean threshold voltage andpulse duration. The slope of the curve gives the rheobase,and the chronaxie is derived from the value of the y-axisintersection divided by the slope.
The aims of this study were to (1) construct astrength-duration curve from four simple thresh-old measurements preoperatively and assess itsaccuracy, (2) derive the chronaxie and rheobasefor each lead, (3) compare actual pulse durationsettings with individual chronaxies for a set of pa-tients to see if pacing waveforms were optimizedfor energy, (4) consider the relationship of acutestrength-duration curves to the mature lead, and(5) consider other possibilities to prolong batterylife.
Patients and MethodsData were analyzed from 325 pacing leads
[101 atrial and 224 ventncular) in 229 consecutivepatients [141 men, 88 women; mean age 76 years,range 28-98 years) with pacemakers implanted atour hospital between December 1993 and January1999. Active fixation leads were excluded as theyhave different acute characteristics. Patients hadvoltages delivered at implantation using aBiotronic Pacing System Analyser ERA 300 atpulse durations of 0.1 ms, 0.3 ms, 0.5 ms, and 1ms. The mean output voltage was measured usinga Tektronix 2445A oscilloscope. Voltages were setto achieve capture and then decremented in 0.1-Vsteps until capture was lost. Threshold was takenas the voltage at 0.1 V ahove loss of capture. Eachthreshold voltage was multiplied by the pulse du-ration to give four data points. The Weiss linearmodel of the strength duration curve was thenadapted to the data points using "method of leastsquares." Figure 2 show.s an example of the linearstrength-duration curve from data obtained from
one of our patients. The quality of the fit of thecurve was determined by finding the average dif-ference between the measured points and thosepoints on the calculated curve at the same pulsedurations. Chronaxie and rheobase were then de-rived for each set of data points and their meansand standard deviations calculated. Z values wereused to see if atrial and ventricular data were fromthe same population. A P value < 0.01 was takenas significant.
ResultsThe 229 patients comprised 101 atrial leads
and 224 ventricular leads. All were passive fixa-tion in design, and tbe different leads are shownin Table J. Table II shows the indication for pacingin these patients.
Tbe curve fit gave a mean error ± SD of 0.024± 0.06 V for atrial curves and 0.008 ± 0.034 Vfor ventricular curves wben compared to mea-sured points. Tbis gave a good accuracy as thevoltage tbresbolds were measured to a resolutionof 0.1 V.
Comparison of atrial and ventricular chron-axies and rbeobases sbowed tbat while chronax-ies may bave come from tbe same population(Z = 1.4) tbe probability of rbeobases doing sowas exceedingly small [Z = 7.1, P < 0.001).Atrial and ventricular data were tberefore treatedseparately.
Table III shows the mean and standard devi-ations of rheobase and cbronaxie in tbe atrial andventricular leads as determined by the calculatedstrength-duration curves. It can be seen that atrial
1274 August 2000 PACE, Vol. 23

IMPORTANCE IN PACIING EFFIGIENCY OF THE STRENGTH-DURATION GURVE
Table I.
Lead Type and Electrode Surface Areas for Implanted Atrial and Ventricular Leads
Atrial Leads Total n = 101 Ventricular Leads Total n = 224
Surface area shown in brackets as (proximal electrode area, distal electrode area)1 Sorin S200 B62 Sorin S80 JB26 Biotronik TIJ 53 BP6BiotronikJP53BP5 Intermedics 438 051 Intermedics 430 05
(35,8)(35,6)(48,6)(48,6)(50,10)(50,10)
12 Sorin S80 (35,6)71 Sorin S80TB (35,6)80 Biotronik TIR 60 BP (48,6)58 Biotronik NP 60 BP (48,6)2 Pacesetter 1401 T (30,9)1 Pacesetter 1470 T (30,2.3)
Table II.
Indication for Pacing in the 325 Patients
Number ofReason for Pacemaker Implantation Patients
Sick sinus syndromeFirst-degree AV blockSeoond-degree AV block Type 1Second-degree AV block type 2Third-degree AV block (narrow QRS)Third-degree AV block (wide QRS)Bifascicular blockTrifascicular blockSlow atrial-fibrillationAF preventionVasovagal syncopeCarotid syncopeTachybradyJunctional bradyHypertrophic cardiomyopathyUnspecified
6927
23294077
222277122
and ventricular chronaxies are at approximately0.25 ms. This value is in keeping with otherchronaxie measurements with similar surfaceareas of distal electrodes.'*-'̂ Most of Ihe patientsin the study had a pulso duration set at 0.45 msor 0.5 ms (common factory defaults) from im-plantation suggesting that pulse durations were
Table III.
Means and Standard Deviations for the 101 Atrial and224 Ventricular Leads
Mean rheobase (V)Standard deviation (V)Mean chronaxie (ms)Standard deviation (ms)
AtrialData
0,510.20.240.07
VentricularData
0.3510.130.250.07
too long and wasteful of energy, even thoughvoltage pulse amplitudes are routinely reducedas possible at the 6-month postimplantation pac-ing check (to the available programmed sett-ing closest to twice voltage threshold). Pulsedurations set at chronaxie are at minimum en-ergy. If pulse durations are set higher than chron-axie, then more energy is being used than isrequired.
Figure 3 shows a plot of the energy wasted ifchronaxie is less than the factory pulse durationdefault sotting of 0.5 ms (Appendix A). With achronaxie of 0.25 ms (the mean chronaxie), 12.5%more energy was used than necessary. At lowchronaxies (2 SD below the mean] up to 73% moreenergy was being wasted.
250
0,05 0-1 0,15 0.25 0.35
ChronaxJe (ms)
0,45
Figure 3. Percentage energy used above the minimumrequired for given chronaxies and at a fixed pulseduration of 0.5 ms. If chronaxie is in fact 0.25 ms,actually pacing at a pulse duration of 0.5 ms represents12.5% excess energy usage. If the chronaxie is 2 SD <0.25 ms, there is 73% energy wastage.
PACE, Vol. 23 August 2000 1275

COATES, ET AL.
DiscussionIn our study, chronaxies were derived from
threshold values measured at four stimulationpulse durations at implantation. Since only fourdata points were used for the curve fit, a source oferror was introduced. Nevertheless, the closenessofthe fit was good, as suggested by the small meanerror and standard deviation of the error. Thechronaxie values obtained are likely to ho accu-rately representative of the acutely implantedlead.
Since optimization of stimulation settingsrefers to the chronic stable lead that pertains after6-12 weeks, the behavior of chronaxie after im-plantation is important. This is to some extent un-clear. Some authors state that after an initial in-crease, chronaxies fall to 8n%-100% of theiroriginal value."''' Others suggest that chronicchronaxies are the same as acute values or slightlylarger.^" If the former occurs, using acute chron-axie to optimize the chronic settings would besafe. However, a significant increase would lead tounsafe pacing if the acnto chronaxie was used.
Crossley et al.'* found that optimizing pulseparameters in terms of safety margins gave a po-tential extension of time to reimplantation of 4.25± 2.14 years. A better method of lead energy opti-mization may, therefore, be to measure chronicchronaxies. This would require a pacemaker toprovide fine 0.1-V steps in programmable valuesand several programmable pulse durations.
In general, the pacemakers of tbe patientsforming this study group underwent simple en-ergy conservation 6 months after implantation bymeasuring tbe voltage stimulation threshold at de-fault pulse durations (0.45 ms or 0.5 ms) and dou-hling the voltage threshold. This was repeated ateach 6-month follow-up. This leaves untappedfurther energy saving potential as default pulsedurations arc clearly well above the averagechronaxies [0.25 ms) obtained at implantation.
Although energy is optimized at pnlse dura-tions set to chronaxie, a high threshold value atthis point may mean that the pulse generator maynot have the capability to produce a pulse largeenough to satisfy amplitude safety margins, or thevoltage required may stimulate the pectoral mus-cles [in unipolar pacing) or the diaphragm [in ei-ther a unipolar or a bipolar system), hi this case alimited reduction in required pulse amplitudemay he achieved hy increasing pulse duration be-yond chronaxie at the expense of energy.
Battery longevity is related to other importantfactors. High impedance leads [> 1,000 il) can re-duce lead current thus maximizing battery life.Sensible programming of lower rate and atrioven-tricular delay can reduce the frequency of pacedcomplexes and minimize the occurrence of ven-
tricular pseudofusion (coincident ventricular pac-ing impulse with intrinsic atrioventricnlar con-duction). The use ofthe atrial pacing [AAI) modein patients with intact atrioventricular conductionsaves all ventricular circuitry. Minimal effectiveuse ofthe rate response mode is also important.
Battery longevity is given as L =̂ [C/D] X114.2, where L = longevity in years, C = batterycapacity ampere-hours (Ah), and D = currentdrain (|JLA) [114.2 constant to convert Ah to micro-ampere-years). Thus, a 0.2 = Ah battery with 2-ti.Acurrent drain results in an 11.4-year longevity.The largest longevity savings are elicited in prac-tice with the greatest voltage output reductionspossible, and this should he done at the chronaxiepulse width.
ConclusionWe have shown that an accurate strength-du-
ration curve can be derived at implantation fromfour data points. Also, with a sufficiently pro-grammable pulse generator, it can he teiemetri-cally derived at any time thereafter. The dataclearly demonstrated that factory default pnlsedurations (around 0.5 ms) are too long and energyinefficient. The balance of evidence suggests thatthe acute chronaxie is a reliahle guide to chronicvalues, and so setting the chronic pulse durationto acute chronaxie and setting pulse amplitude todouble voltage threshold at chronaxie will resultin substantial energy savings. Put another way, thecost per year of pacing can he reduced. However,a clearer definition of chronaxie drift with time infuture studies is desirable. Understanding of thestrength-duration curve is highly rewarding in en-hancing everyday pacing practice.
Acknnwledgmonts: The authors thank Shelly Thwaites,Jenny Lewis, and Gloria Wilson (cardiac technicians) forrecording data points during implantation and Dr. P.D. Higham,Consultant Cardiologist, ibr sindy of patients under his care.
Appendix AEnergy Equations
Energy E is the time integral over the productof voltage and current. For modern constant volt-age generators, at constant impedance, the equa-tion for energy E approximates to the product ofthe mean voltage , mean current and pulse dura-tion d''\
E = Viri (lA)
The mean voltage and current necessary toachieve capture is related to the chronaxie and therheobase.^ The voltage and current curves maydiffer in shape and so have different values ofchronaxie and rheobase. The relationship he-
1276 August 2000 PACE. Vol. 23

tMI'ORTANCE IN PACING EFFICIENCY OF THE STRENCTH-DURATION CURVE
tween energy E and voltage and current rheohasesis given by:
E = V^Udil + Tic/d)(l + T,Jd) (2A)
Where
V» = voltage rheohase
I^ = current rbeobase
Tit = current chronaxie
Tvc = voltage chronaxie
To find the energy minimum this equation isdifferentiated and equated to zero. This gives anenergy minimum at d = V(Tic Tvc). We have as-sumed that current and voltage chronaxies arecomparable. This is a safe assumption if elec-trodes are made of nonpolarizable material'* [mod-ern day electrodes have minimized polarization").
When Tic = Tvt then Equation A2 reduces to
E - V^I.c/[l + T^Jd]'-" (3A)
This has an energy minimum (Emin) at rf = Tvc-When this is suhstituted into Equation A3:
Emin = 4V.kT, , [4A)
Dividing Equation A3 by Equation A4 givesthe proportional change in energy above minimumdue to variation in pulse duration or chronaxie:
With a pulse duration set at the manufactur-ers default setting of 0.5 ms, E/Emin varies onlywith chronaxie:
- 0.125(1 (6D)
With Tvc ^ 0.5 ms and therefore with pulseduration at minimum energy. E/En,jn = 1- If chron-axie is < 0.5 ms then E/Emi,, will rise proportion-ally. This may be expressed as a percentage andshows the excess energy [Eexcess) used due to alower than optimum chronaxie:
" l ) X (7A)
This curve is shown in Figure 3.
References1, IriiK:!i VV. Kramor E, Mullor R. Tin? programming of cardiLic; pace-
makers; Wish and reality- DuLitchc Med Wnchenscihr 19yi:n6:t)01-605.
2. Lapiqut! L. Doiiriititiii (.ixporinifintallo dft rexcitablilite. Froc SncBinl 1909; 77:280-285,
3. Weiss CJ. Siir la possibilite rie rendur comparabli; cnire eiix les ap-pareils corvynl a I'nxcitation electriqiitt. Artili Hal Biol 1901;:JS;44(),
4, Irninli VV. 'I'lie cbronaxiu time and it.s practic:al importance. PAC:E
5. Furman S, (;ar\'py ), llurzoh^r P. Pulse duration variation and di'c-troiie size as a factor ill pacemaker iongevity. I Thorac CarcliovascSurg 1975: 59:382-389.
6. Smyth NHU, Tarjan PP, Chornoff E, et al. The significance of elec-trode surface arou and stimulating thresholds in permanent cardiacpacing, J Thorac flardiovasc Surg 1976: 71;55!>-f)B5.
7. Barold S, Modern C;ardiac Pacing, Armonk, NY, Futura PuhlishingCa.. 1985, p. 43.
a. Hynes JK, Holmes DR, Meridelh I, ct al. Ail evalualion of long-termstimulation Ihre.sholds by moasuremeiit of chronic strength dura-lion curves. PACE 19B1; 4:376-379.
9. Crossley CH, Gayle DD, Simmons TW, et al, Reprogramming pace-makes enhances longevity and is cost-effective. Circulation 1996;94(Suppl, 2):245-247,
10. Barold S, Modern Cardiac Pacing. Armonk. NY, Futura PvihlishingCo,, 1985, p, 3ri,
11, Ellenhogen KA, Cardiac Pai:iiig, 2nd edition. Maiden, MA. Black-well Science, 1997.
PACE. Vol. 23 August 2000 1277