Embed Size (px)
Citation preview

The speaker has no financial relationship or off-label usage to disclose

Overview
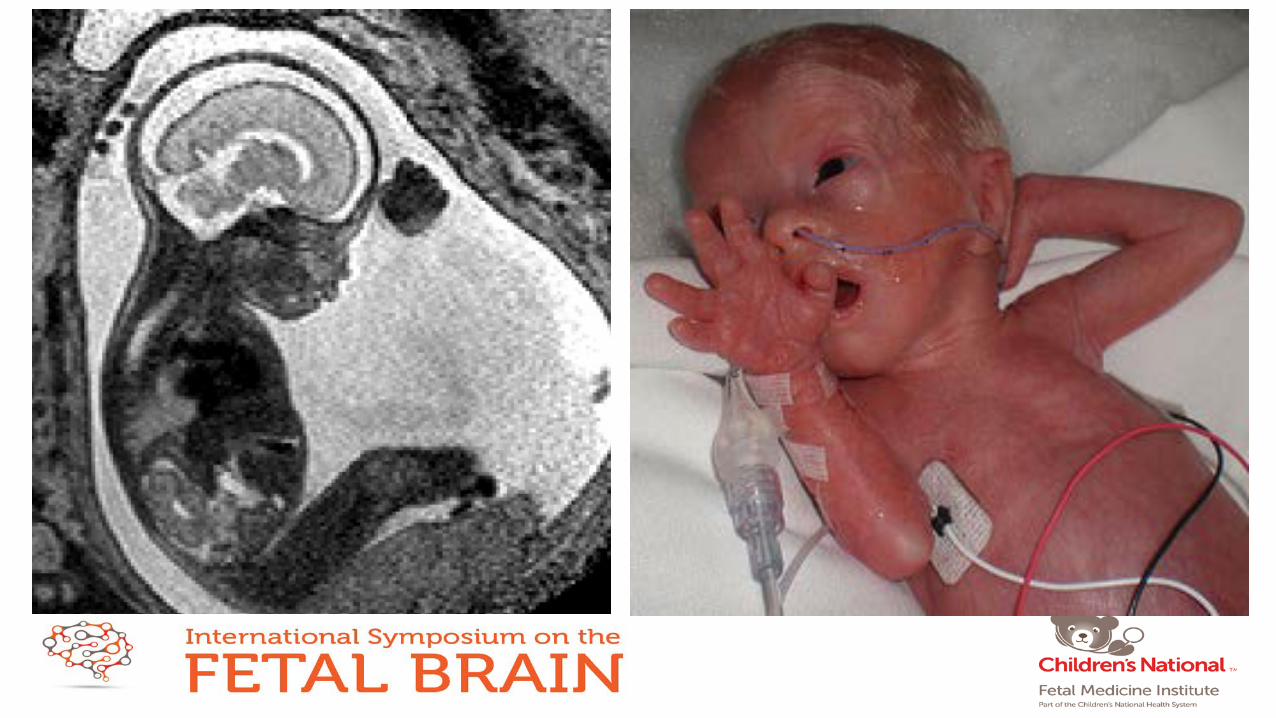
• Static encephalopathy in the immature human is an oxymoron; developmental disturbances in one brain system disrupt development in other remote brain regions
• The third trimester is a critical period in development of the autonomic nervous system
• Autonomic development is critically linked to healthy social engagement and self regulation
• Psycho-affective disorders are the next frontier in the neurology of prematurity • Disturbed autonomic development plays a major role in the psycho-affective and psychiatric
sequelae of prematurity, and may be a target for intervention
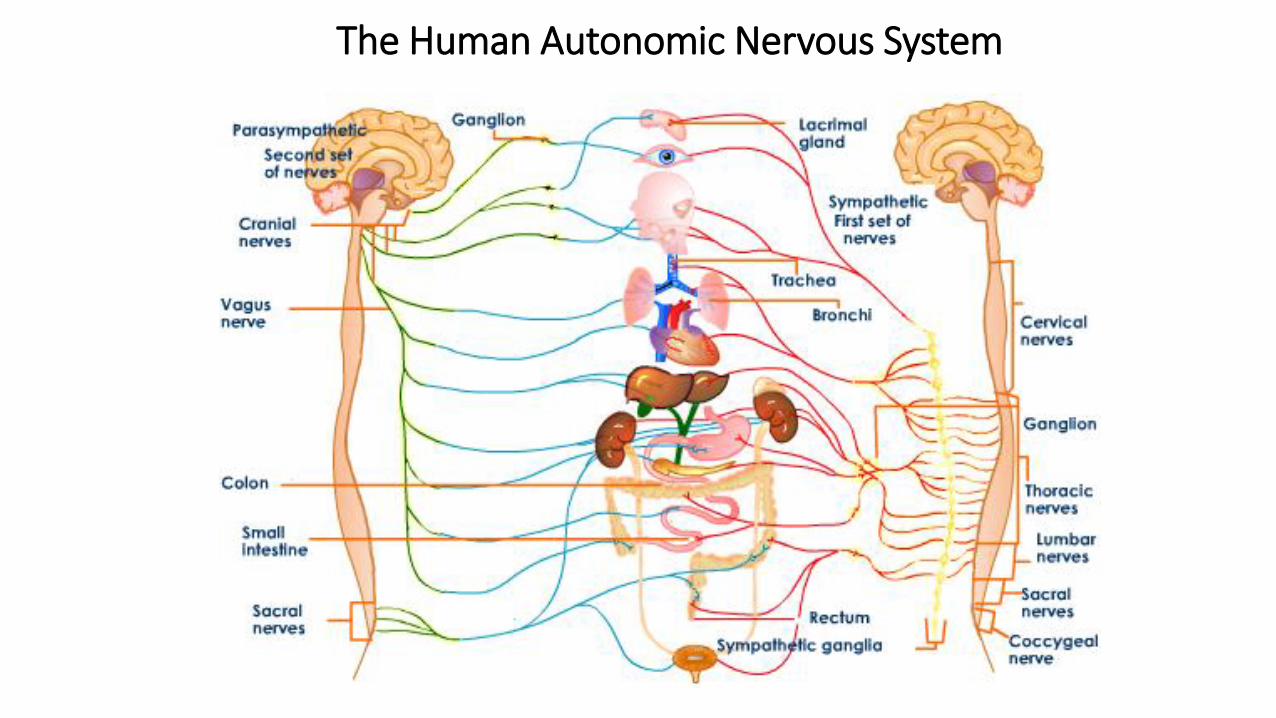
The Human Autonomic Nervous System
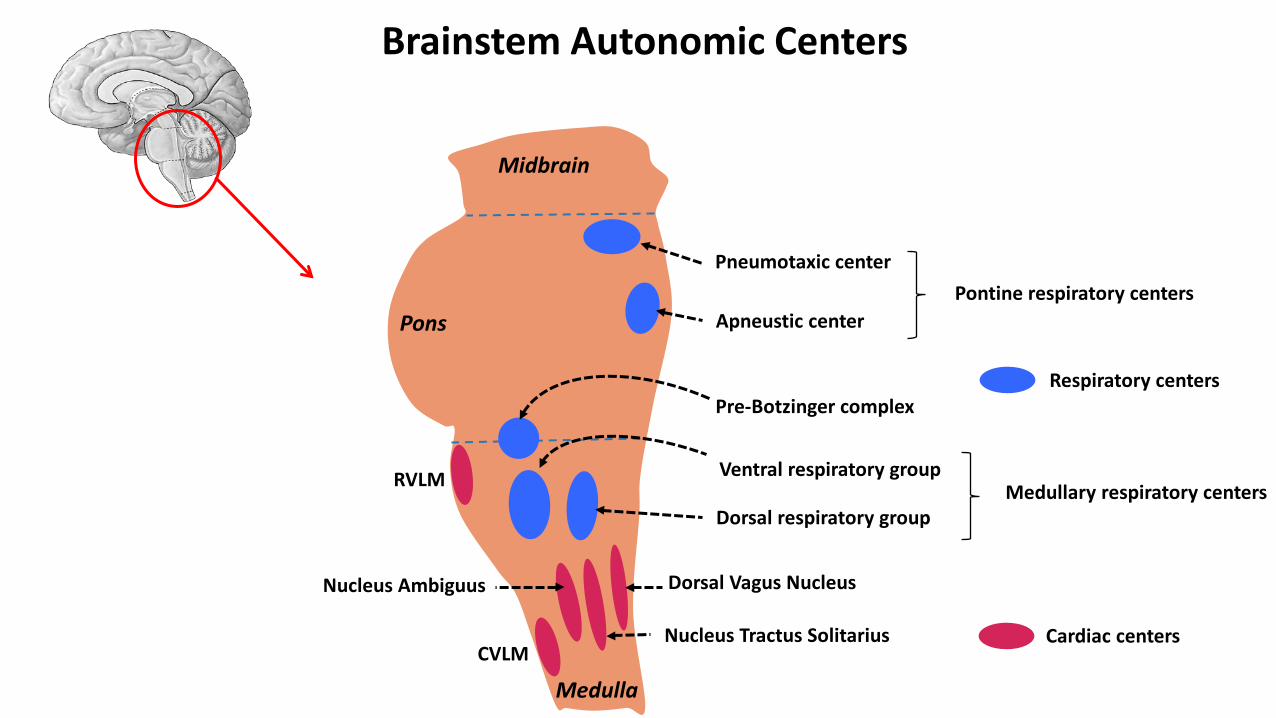
Brainstem Autonomic Centers
RVLM
CVLM Nucleus Tractus Solitarius
Nucleus Ambiguus Dorsal Vagus Nucleus
Pneumotaxic center
Apneustic center
Pre-Botzinger complex
Ventral respiratory group
Dorsal respiratory group
Pontine respiratory centers
Medullary respiratory centers
Cardiac centers
Respiratory centers
Midbrain
Pons
Medulla
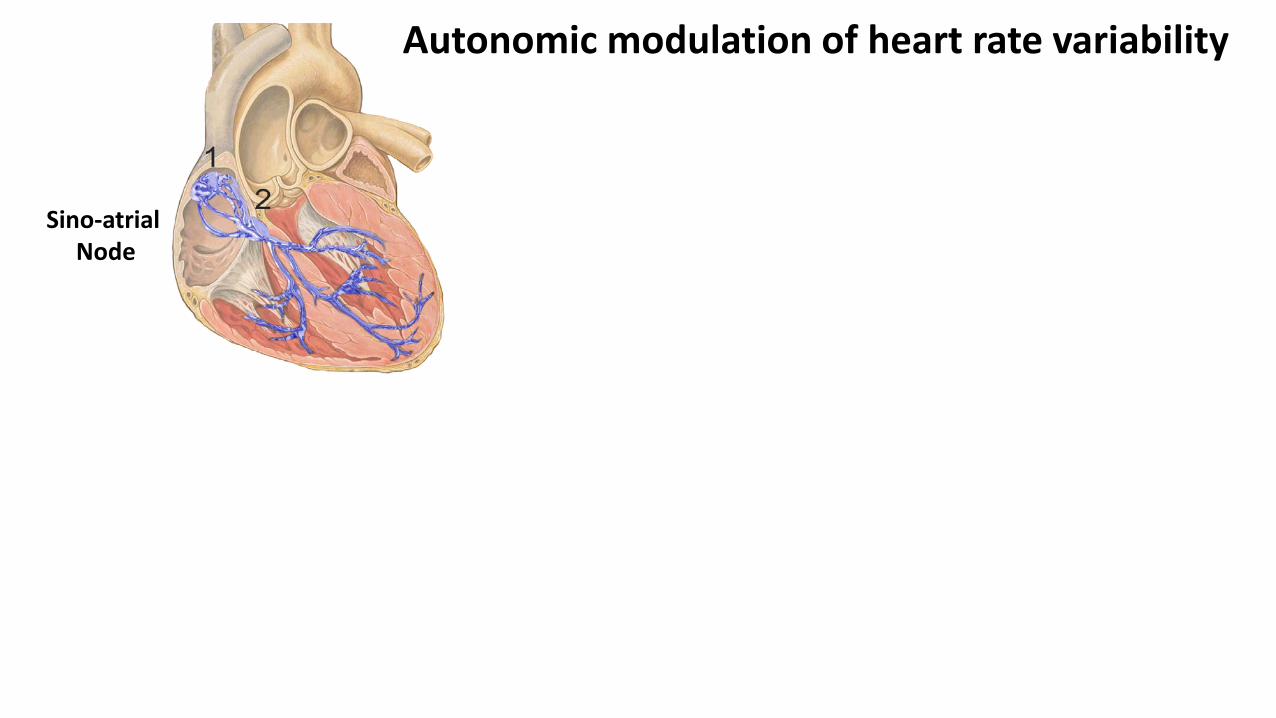
Autonomic modulation of heart rate variability
Sino-atrial Node

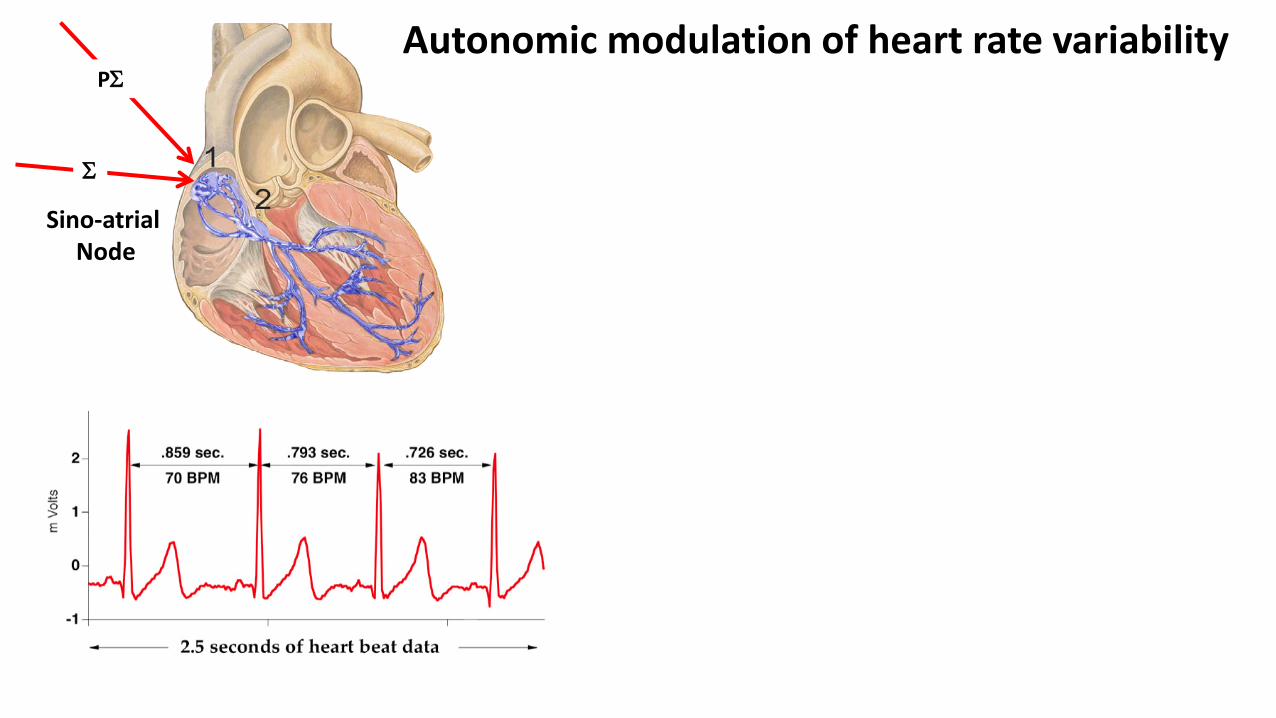
Autonomic modulation of heart rate variability
Sino-atrial Node
Σ
PΣ
Autonomic modulation of heart rate variability
Sino-atrial Node
Σ
PΣ

Autonomic modulation of heart rate variability
Power Spectral Density
Sino-atrial Node
PΣ
Σ Σ PΣ
PΣ
Autonomic Regulation of Heart Rate Variability
• Denervated heart has a ~ constant rate around 100/min
• HRV is driven by sympathetic (Σ) and parasympathetic (PΣ) innervation
• Baroreflex function (PΣ and Σ) 0.1 Hz (LF: 10 sec)
• Respiratory sinus arrhythmia (PΣ) 0.5 -1.5 Hz (HF: 0.5-2.0 sec)
• Sympathovagal balance is assessed by the HF/LF ratio

Normal Trajectories of ANS Branch Development
Σ tone
20 wk //
PΣ tone
// 6 mo post term 25wk 30wk
• Measuring Σ and PΣ tone, and sympathovagal balance
• Assessing sensitivity of homeostatic brainstem reflex loops (e.g., baroreflex loop)
• Integration of ANS into other systems • Fetal movements ~ 23 wks heart rate varies with fetal rest/activity • Sleep wake cycling - from 32 wks progressive synchronization of fetal state
variables (movements, behavioral patterns, respiration, eye movements • Feeding (non-nutritive to nutritive feeding) • (Social engagement)
• These indices are biomarkers of developmental integrity in the fetus and newborn
Assessing Autonomic Function in the Fetus and Newborn
Baroreflex Function in the Fetus and Newborn Studies in fetal sheep • Fetal BR is functional as early as 0.6 gestation • Fetal BR sensitivity starts low and increases through gestation • Fetal BR sensitivity increases primarily due to progressive brainstem integration,
more so than baroreceptor/baroeffector function Studies in premature humans • Sequential BR testing (tilt) in preterm infants shows initial weak HR response in
early gestation which increases to term • Increasing BR sensitivity is associated with increasing PΣ tone
Autonomic function is critical for successful transition
Successful transition from fetal to neonatal physiology requires • major hemodynamic changes - in heart rate, peripheral vascular resistance,
blood pressure, and redistribution of blood flow • marked surge in Σ activation
• increase in circulating catecholamines • RNSA increases by 250% (fetal sheep) • activated cutaneous thermoreceptors
• At term birth the surge in Σ outflow is controlled by the medulla, higher centers (e.g., hypothalamus), and forebrain-brainstem circuits

Autonomic development in an abnormal third trimester environment
The developing ANS is sensitive to a variety of stimuli including chronic hypoxia, acidosis, inflammation, hormones, medications, abnormal afferent (hemodynamic and respiratory) signals, many others Conditions that disrupt third trimester ANS maturation • In utero - placental failure, CHD, infection, maternal smoking and substance abuse, maternal
diabetes, maternal ‘stress’/depression • Ex utero - prematurity
Negative influences on third trimester autonomic development


Brainstem Centers for Autonomic Cardiovascular Control
NTS
DMNX NA
RVLM
CVLM
SPN
Afferent Input
Parasympathetic (Vagal) Efferents
Sympathetic Efferents
+
+
+
+
-
- -
Neurotransmitter Systems • Glutamate • GABA • Serotonin • Substance P • Angiotensin II • Neurotensin
+
Autonomic development in the ‘ex utero fetus’
Immature autonomic function (across all domains, especially PΣ)
Delayed autonomic development Autonomic dysmaturation of prematurity
Premature engagement of the ANS by the extra-uterine environment

Autonomic Maturational Delay in Prematurity
Domain Effect
Blood pressure at term/beyond 10-15 mmHg in premature infants until 6 months post term Especially low at 2-3 months in quiet sleep (peak risk for SIDS)
HRV-sleep coupling In term infants Σ tone increases from QS to AS In preterm infants coupling is delayed until ~ 6 mo post-term
Baroreflex testing (head-up tilt) Significantly delayed recovery of BP in preterm Premature infants with BPD, BRF is impaired until 12 wk post term

Autonomic Dysmaturation of Prematurity
Domain Effect
Infants developing later ALTE Paradoxical increase in PΣ tone and decrease in Σ tone at 36 wk
Opiate exposure in 3rd trimester Hyper-reactive increase in HRV (PΣ and Σ) from non-nutritive to nutritive sucking
Prolonged PDA exposure Paradoxical predominance of PΣ tone
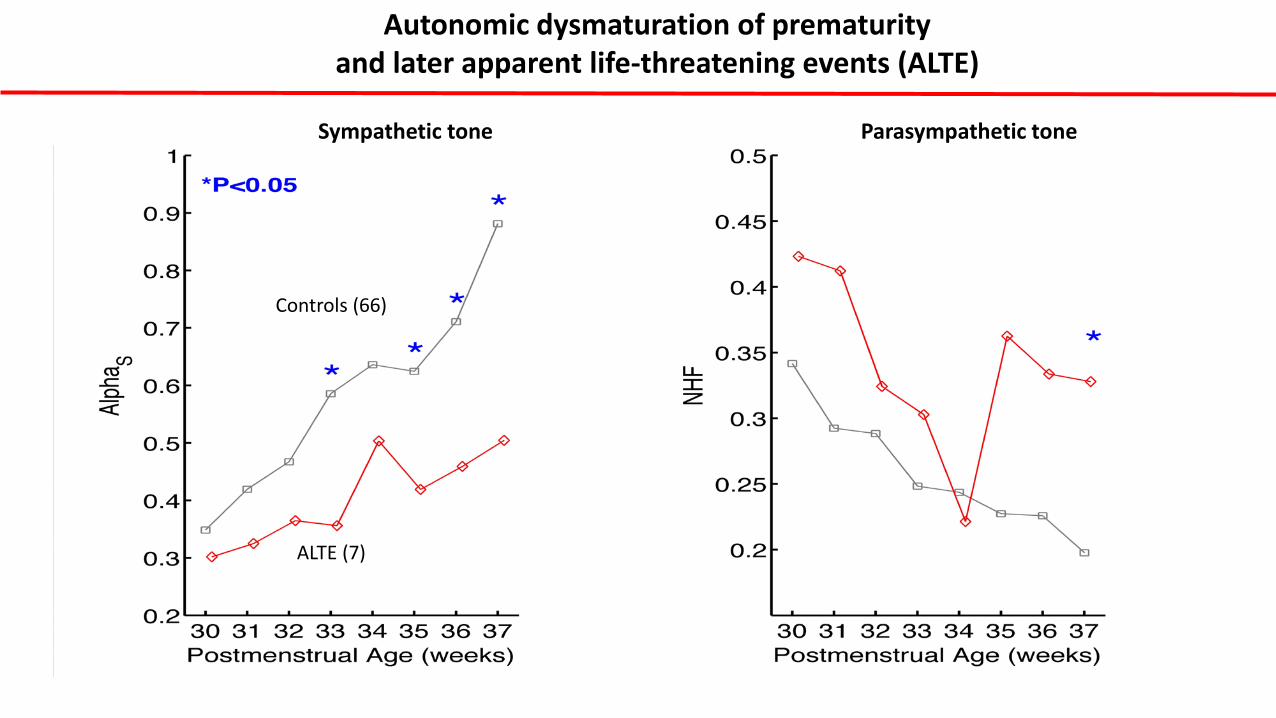
Sympathetic tone Parasympathetic tone
Controls (66)
ALTE (7)
Autonomic dysmaturation of prematurity and later apparent life-threatening events (ALTE)
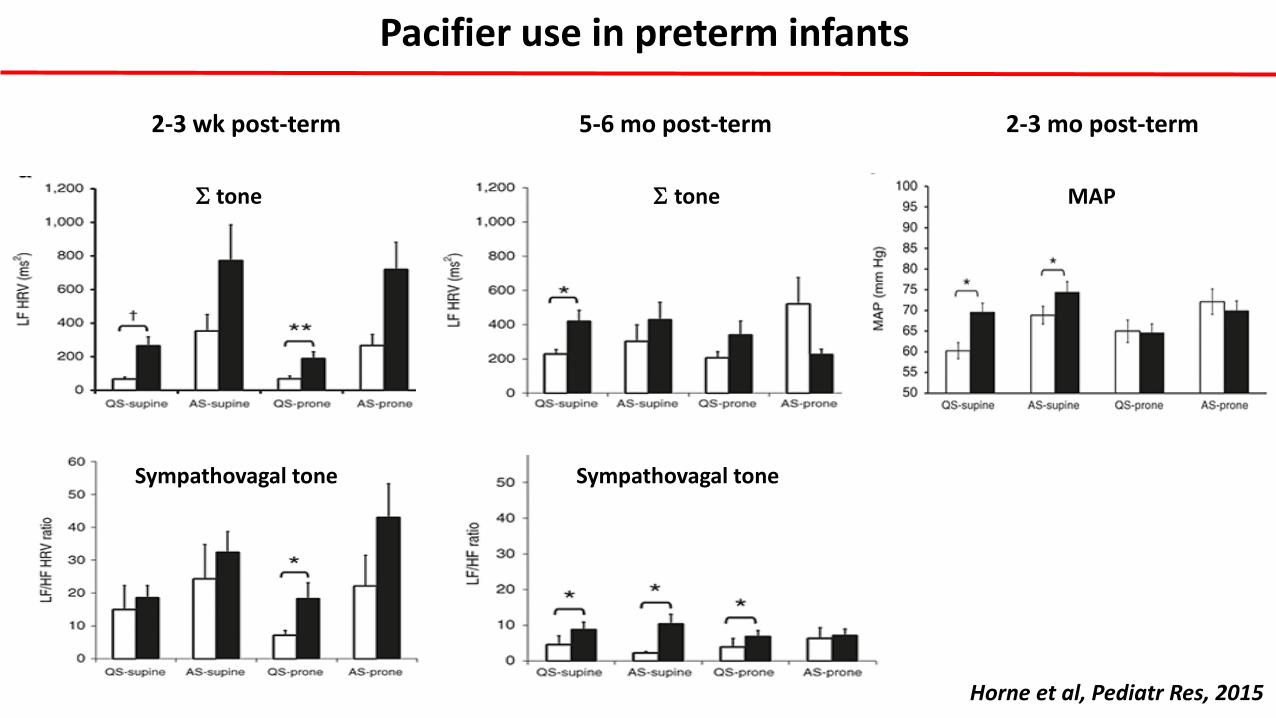
2-3 wk post-term 5-6 mo post-term
Horne et al, Pediatr Res, 2015
Σ tone
Σ tone
Sympathovagal tone Sympathovagal tone
Pacifier use in preterm infants
2-3 mo post-term
MAP
Static encephalopathy in the immature human is an oxymoron
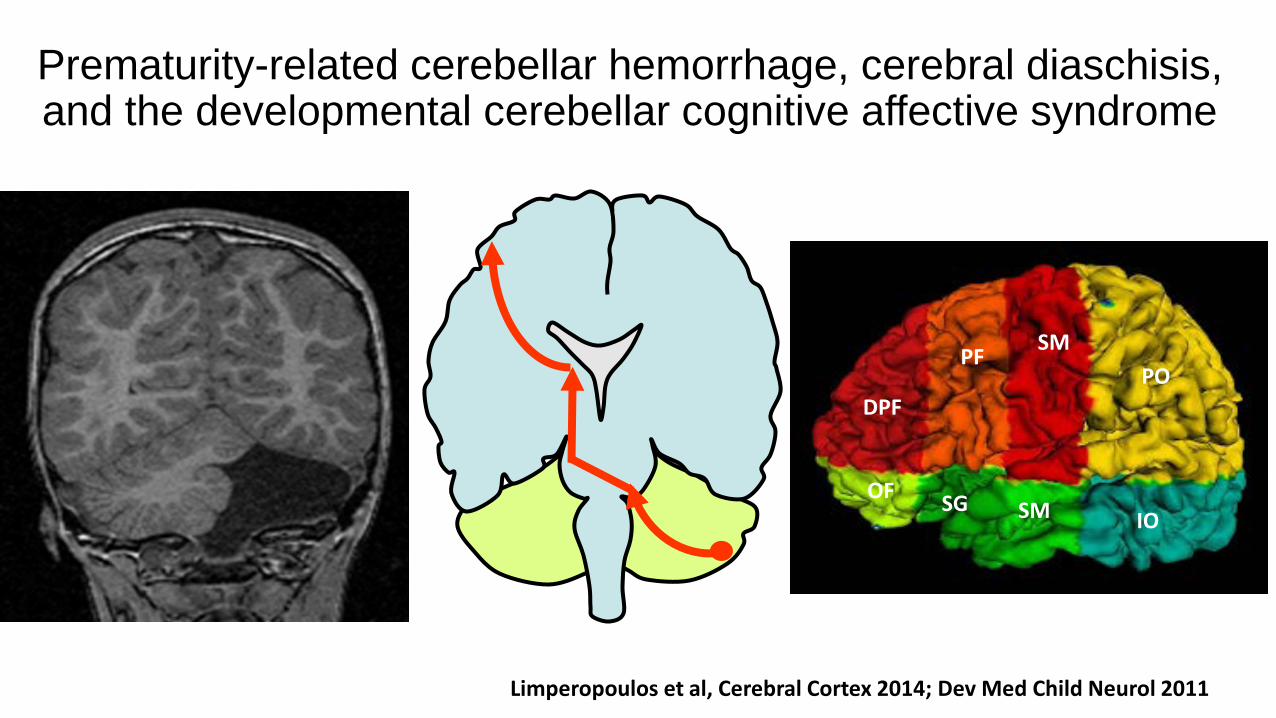
Prematurity-related cerebellar hemorrhage, cerebral diaschisis, and the developmental cerebellar cognitive affective syndrome
SM PF
DPF
OF
PO
SM IO SG
Limperopoulos et al, Cerebral Cortex 2014; Dev Med Child Neurol 2011

Autonomic Dysmaturation of Prematurity and its relation to
Psycho-Affective and Social Outcome

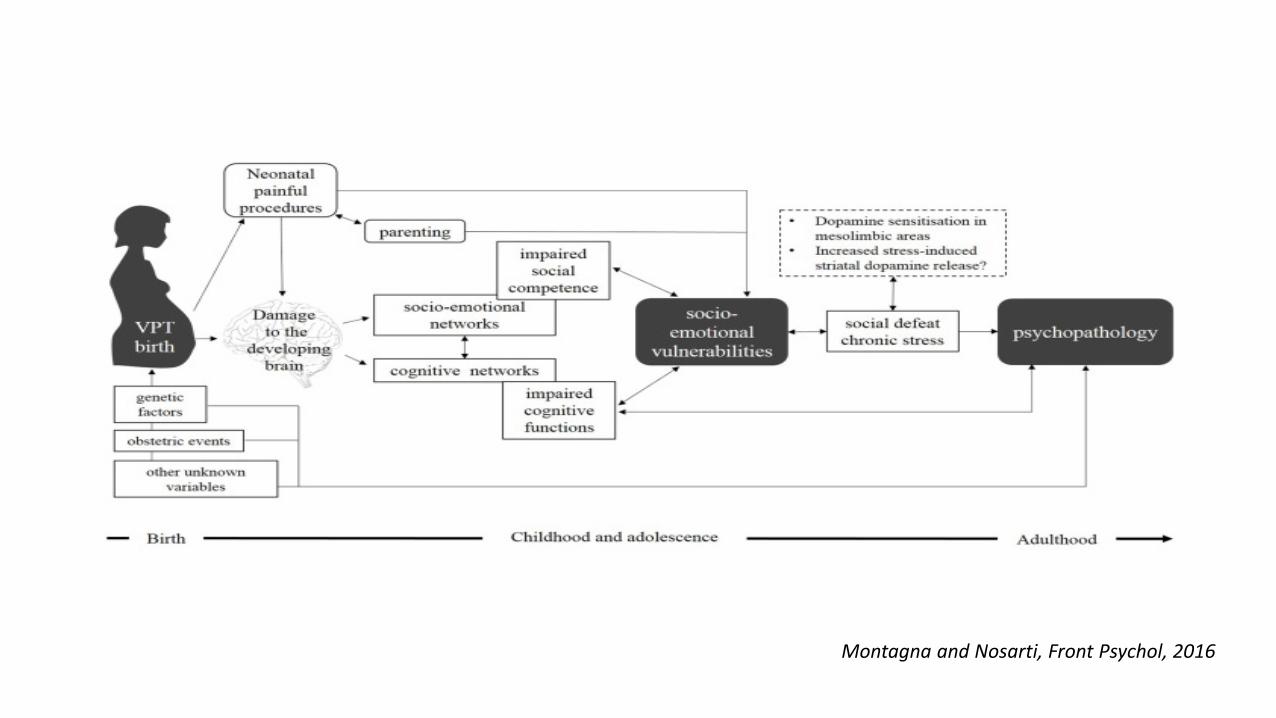
Psycho-affective disorders among prematurity survivors
• 25% premature infants (<32 weeks GA) develop later psycho-affective dysfunction
• Phenotype is relatively consistent - inattention, anxiety, internalizing issues, and socio-emotional dysregulation
• Early-life disturbances in socio-emotional processing may progress to frank psychiatric conditions (ASD, depression, non-affective psychosis, eating disorders, bipolar disorders)
• Social dysfunction (social defeat, social exclusion) is a major mediator (and potential therapeutic target) in the causal pathway from prematurity to socio-emotional vulnerability and psychopathology

xxx
XXX

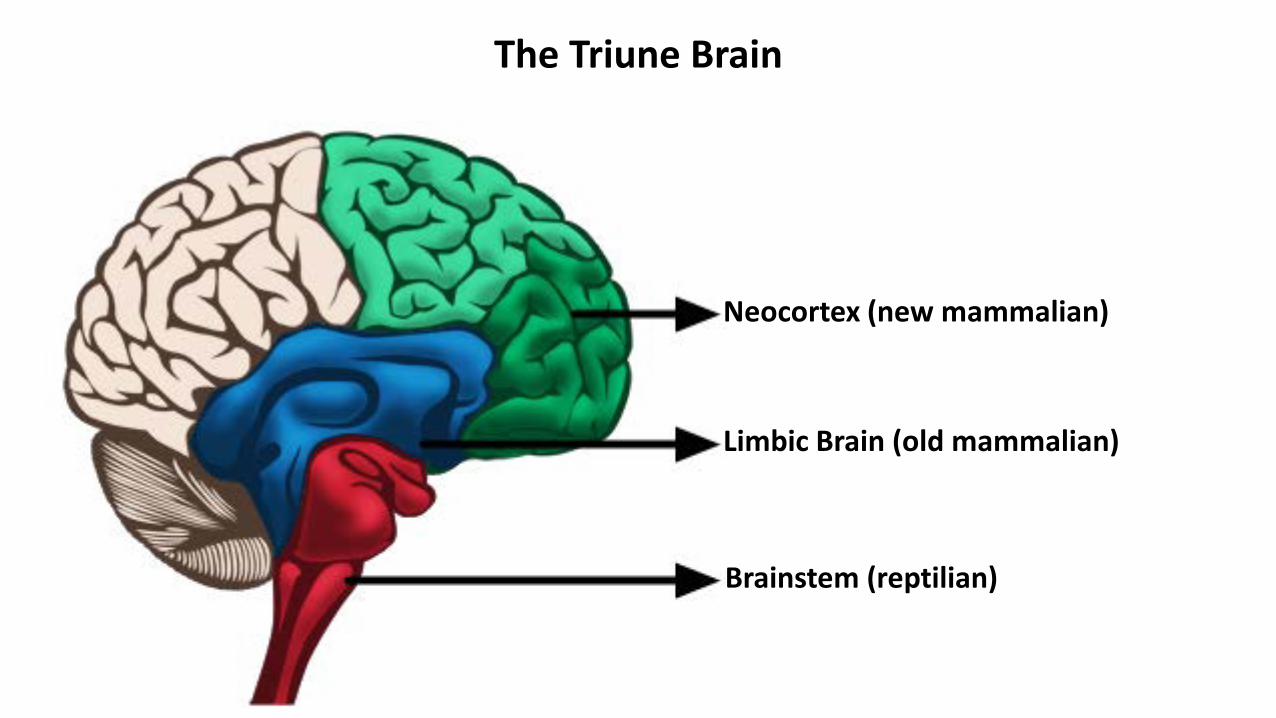
The Triune Brain
Neocortex (new mammalian)
Limbic Brain (old mammalian)
Brainstem (reptilian)

Higher-order cortical systems socio-emotional self-regulation, inhibitory control, cognitive processing (social engagement system) Limbic system integration of brainstem and limbic systems regulates emotion and attention Brainstem autonomic systems homeostatic cyclic processes and sensory integration (vagal, circadian)
Hierarchical model for cognitive, affective and behavioral regulation
The Social Engagement System
• The social engagement system plays a critical role in the ability • to interact and communicate successfully in a social context • to deal appropriately with emotions
• The social brain is an ‘anatomically distributed network’ involving the temporal lobe, amygdala, insula, orbitofrontal cortex and prefrontal cortex
• Specific developmental abnormalities have been detected in ex preterm subjects by volumetric MRI in regions of socio-emotional processing
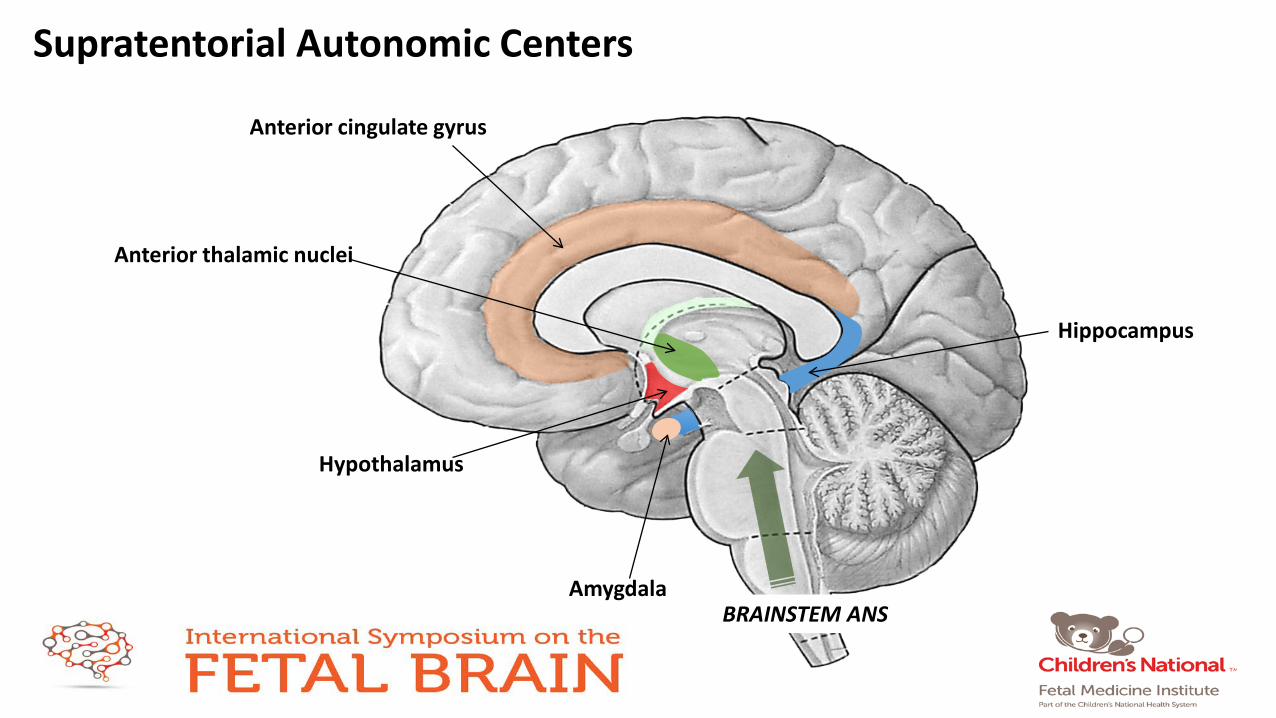
Anterior cingulate gyrus
Anterior thalamic nuclei
Hypothalamus
Amygdala
Hippocampus
BRAINSTEM ANS
Supratentorial Autonomic Centers

Structural alterations in the ‘social brain’ of ex-preterm infants
Montagna and Nosarti, Front Psychol, 2016
Graphic summary of brain regions involved in processing socio-emotional stimuli
Hierarchical model for cognitive, affective and behavioral regulation
• Transition to self-regulatory behaviors during the second year of life depends on higher control systems, reflecting the integration of the anterior cingulate gyrus that is implicated in the coordination of distress and attention
• Activation of the social engagement system dampens the neural circuits that trigger fight, flight, or freeze, including the limbic circuits
• Even transitory dysfunction of brainstem structures during brain development may disrupt maturation of the entire system that supports behavior and emotion regulation.
Concluding remarks • Mechanisms and manifestations of motor, cognitive, learning sequelae of prematurity have
been an major investigative focus for years. The origins of (potentially crippling) psycho-affective disturbances in the ex-premature population are relatively unexplored
• Neurologic dysfunction in the preterm has focused more on destructive insults to the supratentorial brain. The role of developmental disruption mediated by impaired activation and trophic support from remote sights is underexplored
• During the 3rd trimester, the immature ANS is in an accelerated developmental phase (critical period) and thus vulnerable to aberrant programming by abnormal influences
• Autonomic dysmaturation of prematurity may play a critical role in shorter-term (SIDS, ALTE) and longer-term (psycho-affective) sequelae increasingly recognized in prematurity survivors
• The remarkable plastic potential of the ANS may make it amenable to behavioral interventions

Autonomic predictors of longterm outcome
• In preterm neonates • HRV in the newborn period predicted cognitive development at 3 years (Huffman et al., 1998). • Vagal tone predicted cognitive and social emotional development from birth to 5 years of age (Feldman &
Eidelman, in press) • Sleep–wake cycling predicted sustained exploration at 6 months (Feldman et al., 2002).
• These data point to bi-directional relations between the cycling of arousal, attention orientation, and circadian rhythmicity, functions mediated by brainstem-related systems, which contribute to information processing and cognitive competencies among premature infants.
• sustained heart rate lowering during visual fixation marks voluntary, sustained attention in infants (Richards & Cronise, 2000). Respiratory sinus arrhythmia is related to an increase in vagal firing during sustained attention and to its inhibition at attention termination.

The Polyvagal Theory (PVT) • Biobehavioral model relating autonomic function to self-regulation and social engagement. • Mammalian autonomic development goes through three phylogenetic stages with distinct
subsystems. • These autonomic subsystems are linked to specific behaviors
• Immobilization system • most primitive – freezing behavior with apnea/bradycardia • operates through the dorsal vagal nucleus and the unmyelinated (‘vegetative’) vagus
• Mobilization • fight or flight behaviors • operates through the sympathetic nervous system
• Social engagement system • facial expression, vocalization – fosters calm behavior • dependent on the nucleus ambiguus and the myelinated vagus • inhibits the sympathetic system and dampens the HPA axis

Disturbances in Autonomic Function and Cognitive-affective Regulation
Disturbances in autonomic brainstem development are may disrupt development of social-emotional self-regulatory function, Leading to impaired attention to external stimuli, modulation of arousal, and reactivity to stressors, management of negative emotions Deficits in inhibitory control may result in perseverative, impulsive, distractible behavior, and later attention deficit/hyperactivity, conduct or antisocial disorders
The social engagement system and the ANS
• Muscles of the head and face are controlled by brainstem nuclei that communicate directly with an inhibitory neural system that lowers HR and BP, reduces arousal, and promotes calm states. Direct corticobulbar pathways from the frontal areas of the cortex influence the system. Afferent feedback through the vagus to the medullary nuclei (eg, NTS) in turn influence forebrain areas. These centers of the social engagement system are influenced by the HPA axis, oxytocin, and vasopressin.
• The neural regulation of the myelinated vagus is integrated into the Social Engagement System (SES) • When SES is compromised the effects are both behavioral and autonomic, with decreased myelinated vagal influence on
the heart, which in turn potentiates the the expression of two older systems, the sympathetic nervous system and the dorsal vagal complex (including DMV) which in turn foster the mobilization behaviors of fight-flight (SNS), and the immobilization behavior of freezing/feigned death/behavioral shutdown (DMV).
(SW Porges, 2003)


Autonomic changes in psycho-affective disorders
• When defense (fight/flight) systems are not appropriately inhibited in safe circumstances anxiety disorders and reactive affective disorders may emerge
• Reactive affective disorders are a well known complication of prematurity and include two clinical patterns, (i) inhibited
(emotionally withdrawn, absence of attachment behaviors) and (ii) uninhibited (indiscriminate attachment).
• In conditions such as autism, schizophrenia where there is an inability to activate normal social engagement, there appears to be limited activation of pathways from the temporal cortex that inhibit the limbic defense reactions.
• Clinical populations such as anxiety or depression (compromised social behavior) have difficulties regulating visceral state
(lower vagal regulation of the heart) and SES behaviors (reduced facial expressiveness)

Social engagement and attachment – A phylogenetic perspective (4) (SW Porges, 2003)
• In safe situations projections from the cerebral cortex especially the prefrontal and temporal cortex (fusiform gyrus and
superior temporal sulcus) • activate the central amygdaloid nucleus to inhibit the limbic defense systems • activate the corticobulbar pathways that regulate social engagement behaviors
Dysmaturation Socio-emotional vulnerability Psychopathology
Chronic stress Social defeat
Geva • Brainstem dysfunction in the newborn • 1 month of age showed poorer attention regulation as a function of arousal states (Gardner et
al., 2003); • 4 months over-responsive attentional responses to increased endogenous arousal (Karmel et
al., 1996); • 3 years less regulated inhibitory control on rapid automatized naming tasks (Geva, 1995; Geva,
Gardner, & Karmel, 2004).

Geva • Brainstem-related developmental impairment is likely to impact on the development of self-
regulation across childhood and beyond. • Brainstem centers mature early preceding development of the limbic system and cortex. • Dysmaturation of brainstem systems during the third trimester in preterm and high-risk
infants predict later neuropsychologic deficits. • Specific prenatal and perinatal risks that interfere with myelination and synaptic functions in
the brainstem may affect the development of adaptive self-regulation.

Geva • Difficulties in the regulation of basic physiological functions such as sleep, feeding, or self-
soothing may disrupt the management of negative emotions, the • development of inhibitory control (conduct or antisocial problems), • lead to later attention deficit/hyperactivity disorders. • premature infants at highest risk are those with
• intra-uterine growth restriction (Geva, Eshel, Leitner, Fattal-Valevski, & Harel, 2005) • very low birth weight infants with periventricular leucomalacia (Skranes et al., 2007).
• Later maturation of top-down fronto-limbic connections, often in the right prefrontal cortex, is described as the apex of the proposed hierarchy (Schore, 1997) and enables adaptive coping responses to stress (Ellenbogen, Schwartzman, Stewart, & Walker, 2006).
• development of higher functions, such as inhibitory control and social-emotional self-regulation, is hypothesized to be compromised (Dennis, 2006).
• Mechanisms of arousal and attention are mediated by sub-cortical brainstem-related structures, especially prior to 2–3 months of age (Gardner & Karmel, 1995; Geva, Gardner, Karmel, Feldman, & Freedland, 1999a; Geva, Gardner, & Karmel, 1999b).
Geva • Disruptions in the ability to shift arousal or maintain equilibrium impact on later cognitive,
behavioral, and emotion-regulation capacities (Sigman, Cohen, & Beckwith, 1997). • During this period, through mediation of norepinephrine and dopamine, modulation of
attention affords the adaptive coordination of vigilance and distress during information processing (Eckerman, Oehler, Hannan, & Molitor, 1995).
• The second relevant milestone is the connectivity to the limbic system. Tucker and colleagues (2005) proposed that two midbrain structures, the hypothalamus and thalamus, are pivotal in organizing internal and external influences to ensure homeostasis of complex vertebrates. The hypothal- amus is central in securing visceral regulation of internal states
Geva • transition to self-regulatory behaviors during the second year of life often draws upon higher
control systems, reflecting the integration of the anterior cingulate gyrus that is implicated in the coordination of distress and attention
• even transitory dysfunction of brainstem structures at the newborn period may disrupt the maturation of the entire system that supports behavior and emotion regulation.

Geva • three hierarchical and nested levels, originating in the assessment of brainstem functions. The
first level includes physio- logical regulation of cyclic processes and sensory integration processes; the second level relates to further integration of three aspects of emotion and attention regulation; and the final level includes an integration of higher-level complex behavioral outputs.
• biological clocks and the cyclic autonomic changes regarding state, sati- ety, temperature, and heart rate (Porges, 1997; Geva & Feldman, in press).
• Porges’ (1997) polyvagal evolutionary theory pro- poses that the nucleus ambiguus moderates the control of respiratory sinus arrhythmia, a function unique to the mammalian brainstem organization and related to processes of attention, emotion, and communication in humans.
• Cardiac vagal-tone, a measure of respiratory sinus arrhythmia, provides an index of attention regula- tion in newborns (Arditi, Feldman, & Eidelman, 2006), orientation in neonates (Feldman, 2006), and information processing during the first months of life (Bornstein & Suess, 2000).
Geva • sustained heart rate lowering during visual fixation marks voluntary, sustained attention in
infants (Richards & Cronise, 2000). Respiratory sinus arrhythmia is re- lated to an increase in vagal firing during sustained attention and to its inhibition at attention termina- tion. Heart rate variability in the newborn period was found to predict cognitive development at 3 years in premature infants (Huffman et al., 1998).
Geva • Cardiac vagal-tone in preterm neonates was found to deter- mine the trajectories of cognitive
and social emo- tional development from birth to 5 years of age (Feldman & Eidelman, in press) and sleep–wake cyclicity predicted sustained exploration at 6 months in premature infants (Feldman et al., 2002). These data point to bi-directional relations between the cyclicity of arousal, attention orienta- tion, and circadian rhythmicity, functions mediated by brainstem-related systems, which contribute to information processing and cognitive competencies among premature infants.
• (b) Arousal-modulated attention (AMA). when less aroused and following feeding, full-term neonates look at more stimulating and novel events, and when more aroused, such as during the period before feeding, they look at less stimulating and familiar events.
• This pattern of neonatal arousal- modulated attention differentiates normal neonates from infants with compromised brainstem func- tioning (CBSF; Karmel et al., 1996).
• infants are able to prefer novel stimuli when less aroused (Geva et al., 1999a, 1999b)

Geva • The development of higher levels of output regu- lation requires inhibitory control capacities
that would allow for stopping, reflecting, and considering options prior to the execution of output. Deficits in inhibitory control and executive attention may be reflected in the child’s difficulties in making mental or behavioral shifts, which result in perseverative, impulsive, or distractible behavior (Diamond, 1990; Feldman, Gardner, Karmel, & Freedland, 1999a).
• over the long term CBSF may affect the development of regulatory capacities by inter- fering with the development of inhibitory control and cognitive self-regulation.
• he second path, which focuses on the mother’s role in the development of self-regulation, • Maternal milk, touch, smell, body heat, and biological rhythms provide a set of bio-behav-
ioral regulators to the infant’s autonomic, thermo- regulation, feeding, and stress-management systems, most of which are mediated by the brain- stem.
• brainstem dysfunction in preterm infants or in affected neo- nates, with its ensuing regulatory deficits, is thus likely to have a negative impact on the development of social-emotional regulatory skills.

Geva • First, the model incorporates multidimensional regulatory expressions of the CBSF
phenomenon: biochemical (e.g., melatonin, cortisol), autonomic (vagal-tone; sleep; feeding), attentional-cognitive (e.g., arousal-modulated attention, inhibitory con- trol); emotional reactivity to stress; and co-regulation of emotional responsivity. These interdependent expressions are proposed to set the foundation for the development of higher-order complex cognitive and emotional processes.
• assessing dysfunctions related to lower levels of CNS functioning, particularly of brainstem dysfunctions, already at the NICU. Disruptions to the development of these lower-level systems can serve as important indicators of risk for the emer- gence of self-regulatory capacities.
Autonomic Nervous System Control of Cardiorespiratory Function
• The autonomic nervous system (ANS) has two branches – sympathetic and parasympathetic – with opposing physiologic effects
• The heart has a basic pacemaker that fires at around …./min
• The ANS modulates changes on this basic rhythm through the sympathetic (LF)/parasympathetic (HF) arms
• By analyzing the HRV at these two frequencies we can assess the strength of S/PS tone
• The autonomic nervous system controls BP by adapting heart rate and total peripheral resistance
• Multiple physiologic mechanisms cause fluctuations in HR and BP • Respiration • Baroreflex • Thermoregulation
• Power spectral analysis of the RRi time series show • LF peak (0.1Hz) at BR peak (Mayer waves) (PΣ and Σ systems) • HF peak (at resp frequency) (PΣ system) • VLF peak (0.03Hz) for thermoregulation

Fetal heart rate variability reveals differential dynamics in the intrauterine development of the sympathetic and parasympathetic branches of the autonomic nervous system. Schneider U1, Schleussner E, Fiedler A, Jaekel S, Liehr M, Haueisen J, Hoyer D. Physiol Meas. 2009 Feb;30(2):215-26.
• fHRV pattrens are determined by GA, pathology, and fetal activity state • Generally, HRV increases with GA, while mHR decreases • Rest/activity cycles in FHR have been described from 23 wks GA • From the 32nd GA on there is a progressive synchronization of fetal state variables (fHR, movements, eye movements) and this becomes a marker of developmental integrity of the fetus. • The sympathetic predominance becomes progressively reduced between 30 wk and term GA ((Ohta, 1999) • Hypothesis was that fHRV shows different time scales of sympathovagal development before and after 32 weeks • Magnetocardiology in 92 singleton pregnancies between 24.1 and 41.6 wk. Divided them into 2 groups • FHR patterns were either
• quiet/non-accelerative (fHRV-1) or active/accelerative (fHRV-2) • Characteristic feature of type 2 FHR is presence of accelerations
• They show a more rapidly progressive acceleration of PS influence prior to 32 weeks GA. • Non-accelerative fHRP are indicative of parasympathetic dominance >32 wks GA. • In contrast, the sympathetic accentuation during accelerative fHRP is displayed in the interrelations between mHR, SDNN and SDNN/RMSSD. • Prior to 32 wks GA, fHRV reveals the increasing activity of the respective ANS branches differentiating the types of fHRP
Montagna and Nosarti, Front Psychol, 2016

BR in Human Neonate In preterm and term newborns, head-up tilting produces marked increases in HR and the magnitude of change is proportional to the degree of tilting.(Finley JP, Biol Neo, 1984; Picton-Warlow CG, Arch Dis Child, 1970; Thoresen M, Early Hum Dev, 1991) Maturational changes in power spectra of HRV show a progressive decline in the LF/HF ratio associated with increasing GA and PNA, indicating an increase in PΣ tone (Chatow U, Pediatr Res, 1995; Clairambault J, Early Hum Devel, 1992) Clairambault found that changes in the HF band were greater at 37-38 wk suggesting a steep increase in vagal tone at this age. (Clairambault J, Early Hum Devel, 1992) Infants in the 28-30 GA range did not change their LF/HF ratio with head-up tilt, but with increasing PNA the LF component increases with head-up tilt.(Mazursky JE, Pediatr Res, 1995)
Autonomic function in the newborn
Premature Infants and HRV Heart rate variability during sleep in healthy term newborns in the early postnatal period.
Doyle OM, Korotchikova I, Lightbody G, Marnane W, Kerins D, Boylan GB; Physiol Meas. 2009
Normative time- and frequency-domain heart rate variability (HRV) measures were extracted during quiet sleep (QS) and active sleep (AS) periods in 30 healthy babies. All newborn infants studied were less than 12 h old and the sleep state was classified using multi-channel video EEG. Three bands were extracted from the heart rate (HR) spectrum: very low frequency (VLF), 0.01–0.04 Hz; low frequency (LF), 0.04–0.2 Hz, and high frequency (HF), >0.2 Hz. All metrics were averaged across all patients and per sleep state to produce a table of normative values. A noticeable peak corresponding to activity in the RSA band was found in 80% patients during QS and 0% of patients during AS, although some broadband activity was observed. The majority of HRV metrics showed a statistically significant separation between QS and AS. It can be concluded that (i) activity in the RSA band is present during QS in the healthy newborn, in the first 12 h of life, (ii) HRV measures are affected by sleep state and (iii) the averaged HRV metrics reported here could assist the interpretation of HRV data from newborns with neonatal illnesses.

Autonomic development in the ‘ex utero fetus’ at term corrected age
At term corrected age, premature and term infants have substantial differences in ANS function • Blood pressure in premature born
• 10-15 mm Hg lower than term infants until 6 months post-term, without a difference in HR • is especially low at 2-3 months during quiet sleep, without compensatory increase in HR
• In term infants HRV is coupled to sleep state (increased Σ tone from QS to AS); in preterm infants coupling is delayed until ~ 6 mo post-term
• Baroreflex function (head-up tilt test) - premature infants had significantly delayed BP recovery compared to term born infants
• 2-3 years there was a significant increase in all HRV parameters in premie group (Landrot, 2007, Autonomic Neurosci)
Forebrain Centers of the Autonomic Nervous System • Central sites with ANS functions include
• insular cortex, hypothalamic, ventral medullary, and cerebellar regions. • Amygdala,
• Insular cortices : Right insular cortex mainly related to sympathetic regulation; Left insular cortex mainly parasympathetic. (Oppenheimer SM Arch Neurol 1990; Cechetto DF Am J Physiol 1990) •Stimulation of the anterior right insular cortex greatly diminishes the baroreflex, whereas posterior right insular cortex stimulation leads to arrhythmia.(Oppenheimer SM Brain Res 1991)

Autonomic system is linked to the Social Engagement System
• Immobilization is a primitive defense system associated with decreased metabolic demands, increased pain threshold, apnea and bradycardia.
• Activation of this primitive system may be lethal in mammals because of their oxygen dependence. • Because mammals are so O2 dependent the freezing response with apnea and bradycardia may be lethal. • Certain mammalian behaviors (reproduction, nursing, pair bonding) may require immobilization without fear; for this
purpose structures that regulate immobilization and pain thresholds have been co-opted by mammals to serve social bonding needs, a process that is facilitated by oxytocin, a neuropeptide that promotes social bonding.
• With evolution the ANS has become linked to the social engagement system of affective experience, emotional expression, facial gestures, vocal communication, and contingent social behavior. These systems are dysfunctional in conditions such as autism and schizophrenia.
• Activation of the social engagement system dampens the neural circuits that trigger fight, flight, or freeze, including the limbic circuits.
Autonomic development in the ‘ex utero fetus’
Found that infants who developed ALTE events after discharge had paradoxically increased PS and decreased S tone at 36 weeks GA S (Nino G, 2016) SIDS victims have significant abnormalities in serotonergic brainstem pathways responsible for cardiorespiratory control
xxx
XXX