Embed Size (px)
Citation preview

Research ArticleThe SIESTA Trial: A Randomized Study Investigatingthe Efficacy, Safety, and Tolerability of Acupressure versusSham Therapy for Improving Sleep Quality in Patients withEnd-Stage Kidney Disease on Hemodialysis
Kunyu Shen,1,2,3,4 Yeoungjee Cho,1,2 Elaine M. Pascoe,2
Carmel M. Hawley,1,2 Veronica Oliver,1 Kathryn M. Hughes,5
Richard Baer,5,6 Jeremy Frazier,5,6 Elizabeth Jarvis,5 Ken-Soon Tan,5,6,7
Xusheng Liu,3,4 Glenda Gobe,8 and David W. Johnson1,2,8
1Department of Nephrology, Princess Alexandra Hospital, Brisbane, QLD, Australia2Australasian Kidney Trials Network, The University of Queensland, Brisbane, QLD, Australia3Department of Nephrology, Guangdong Provincial Hospital of Chinese Medicine, Guangzhou, China4Second School of Clinical Medicine, Guangzhou University of Chinese Medicine, Guangzhou, China5Department of Nephrology, Logan Hospital, Logan, QLD, Australia6School of Medicine, Griffith University, Brisbane, QLD, Australia7School of Medicine, The University of Queensland, Brisbane, QLD, Australia8Centre for Kidney Disease Research, School of Medicine, The University of Queensland,Translational Research Institute, Woolloongabba, Brisbane, QLD, Australia
Correspondence should be addressed to David W. Johnson; [email protected]
Received 25 November 2016; Accepted 26 January 2017; Published 21 February 2017
Academic Editor: Evan P. Cherniack
Copyright © 2017 Kunyu Shen et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Objectives. To compare the effectiveness of real acupressure versus sham acupressure therapy in improving sleep quality in patientsreceiving hemodialysis (HD) or hemodiafiltration (HDF). Methods. A multicenter, single-blind, randomized controlled trial wasconducted in two Australian dialysis units located in Princess Alexandra Hospital and Logan Hospital, respectively. Forty-twosubjects with self-reported poor sleep quality were randomly assigned to real (𝑛 = 21) or sham (𝑛 = 21) acupressure therapydelivered thrice weekly for four consecutive weeks during routine dialysis sessions. The primary outcome was the PittsburghSleep Quality Index (PSQI) score measured at week four adjusted for baseline PSQI measurements. Secondary outcomes werequality of life (QOL) (SF-8), adverse events, and patient acceptability (treatment acceptability questionnaire, TAQ). Results. Thetwo groups were comparable on global PSQI scores (difference 0.19, 95% confidence interval [CI] −1.32 to 1.70) and on the subscalescores. Similar results were observed for QOL both in the mental (difference −3.88, 95% CI −8.63 to 0.87) and the physical scores(difference 2.45, 95% CI −1.69 to 6.58). There were no treatment-related adverse events and acupressure was perceived favorablyby participants. Conclusion. Acupressure is a safe, well-tolerated, and highly acceptable therapy in adult hemodialysis patients in aWestern healthcare setting with uncertain implications for therapeutic efficacy.
1. Introduction
Self-reported poor sleep quality is exceedingly commonin patients with chronic kidney disease, particularly inthose with end-stage kidney disease requiring maintenance
hemodialysis where reported prevalence rates are as highas 80% [1–8]. The high frequency of poor sleep qualityin hemodialysis patients has been attributed to a lack ofnocturnal endogenous melatonin surge [9], increased corebody temperature from exposure to warm dialysate [10], and
HindawiEvidence-Based Complementary and Alternative MedicineVolume 2017, Article ID 7570352, 10 pageshttps://doi.org/10.1155/2017/7570352

2 Evidence-Based Complementary and Alternative Medicine
possibly cerebral edema in the context of dialysis disequilib-rium syndrome [11]. Other risk factors for poor sleep qualityreported by theDialysis Outcomes and Practice Pattern study(DOPPS) include the use of certain types of medications(e.g., antihistamine, antidepressant, anti-inflammatory, anti-asthmatic, narcotic, gastrointestinal, or hypnotics), femalegender, higher bodymass index (BMI), presence of body painor pruritus, comorbidities (e.g., depression, lung disease, andperipheral arterial disease), high serum phosphorus levels,and unfavorable lifestyle behaviors (e.g., lack of exerciseand smoking) [12]. Poor sleep quality is in turn associatedwith heightened risk of hypertension [13], chronic kidneydisease progression [14, 15], impaired glucose tolerance [16],diabetes mellitus [17], cardiovascular events [18], depression[19], increased healthcare utilization [20], impaired quality oflife (QOL), and mortality [12].
Current therapeutic interventions purported to improvesleep quality in dialysis patients include pharmacotherapywith hypnotic agents [21] and melatonin [22], cognitive-behavioral therapy [23] (e.g., sleep hygiene [24], relaxation[25], mindfulness meditation [26], and stationary cycling[27]), nocturnal hemodialysis conversion [28], and cooled(35∘C) dialysate use [29]. These interventions have beenlimited by poor quality evidence base, a lack of demonstrationof consistent or sustainable benefit, frequent side effects(particularly for pharmacologic agents in the setting ofimpaired renal function exposed to polypharmacy), and ahigh cost burden.
Alternatively, acupressure applied at specific meridiansor acupoints has been employed in Traditional ChineseMedicine to improve sleep quality by restoring the yinand yang harmony and balancing life energy (qi) [30].Several studies have demonstrated its safety and efficacyin various patient populations, including the elderly [31–34], postmenopausal women [35], and cancer patients [36].Acupressure is a noninvasive therapy, which is likely tobe associated with a low risk of side effect profile, whencompared to therapies such as hypnotics.
To date, there have only been three randomized con-trolled trials examining the effect of acupressure therapyin HD patients with demonstrated benefit in improvingquality of sleep. First, Shariati and colleagues reported asignificant reduction in PSQI scores in hemodialysis patientswho received thrice weekly acupressure treatment comparedto those who received routine therapy in their 4-week studyinvolving 48 end-stage kidney disease patients (𝑝 < 0.001)[37]. Although the investigators described this study as adouble-blind randomized controlled trial, the control groupreceived no treatment beyond their routine care; thereforethe participants would have known their treatment allocationstatus, which raises concern for “placebo” effect. Similarly,a significant reduction in the PSQI scores was observedin a multicenter randomized controlled trial from Taiwanwhen acupressure therapy was superior compared to routinecare (𝑝 < 0.01), with comparable results between real andsham acupressure treatment groups [38]. Although this studyrandomized 105 participants, there was no description ofnumber of patients allocated to each treatment group nor thereasons for those who did not complete the study (𝑛 = 7)
or safety data. Neither of these studies adequately describedthe methods of randomization nor allocation concealment,which places them at a high risk of bias from subopti-mal methodological quality. The most recent randomizedcontrolled trial, conducted by Arab and colleagues in 108prevalent hemodialysis patients from 3 Iranian hemodialysisunits, reported significantly lower total PSQI scores at 4weeks in patients treated with acupressure compared withsham acupressure or no treatment (𝑝 < 0.001) [39]. Nonethe-less, the study recruited patients with PSQI scores greaterthan 5, which may have limited generalization of theirfindings. In fact, all the above-mentioned studies excludedpatients with an entry PSQI score less than 5, whichmay havelimited the generalizability of their findings to patients withself-reported poor sleep qualitywhomayhave recorded lowerPSQI scores. Moreover, all studies were conducted in Asiancountries, such that the generalizability of their findings andacceptability of such treatmentmodality toWestern countriesremain unclear.
2. Objects
The aims of this multicenter, single-blind, parallel designrandomized controlled trial were to (1) investigate the effectof acupressure on the sleep quality of prevalent hemodialysispatients and (2) establish the feasibility and safety of acupres-sure treatment in a Western healthcare setting.
3. Methods
3.1. Study Oversight. The SIESTA (Study Investigating theEfficacy, Safety, and Tolerability of Acupressure versus shamtherapy for improving sleep quality in patients with end-stagekidney disease on hemodialysis) study was an investigator-initiated, multicenter, prospective, 1 : 1 randomized, single-blind, sham-controlled, parallel design trial. Participantswere recruited from the dialysis units at Princess AlexandraHospital and Logan Hospital, Australia. This study wasregistered with the Australian New Zealand Clinical TrialsRegistry (ACTRN 12615000989549) and the study protocolwas approved by ethics committees at both participatingcenters. All patients providedwritten participant informationand consent form (PICF) before trial participation and thetrial was conducted in accordance with the principles of theInternational Conference on Harmonization Good ClinicalPractice Guidelines [40].
3.2. Participants. The study included adult patients (age >18years) with end-stage kidney disease and self-reported poorsleep quality who were receiving thrice weekly hemodialysisor hemodiafiltration for at least 3 months prior to studyenrolment and had no plans to change their renal replace-ment modality within the study period. All patients had tohave sufficient knowledge of English to be able to completequestionnaires independently. English language proficiencyof participants who were nonnative English speakers wasassessed by clinical staff. Exclusion criteria included thosewith a history of amputation (precluding ability to applyacupressure treatment on limbs), serious skin diseases (e.g.,

Evidence-Based Complementary and Alternative Medicine 3
dermatitis and burn) near the location of acupoints, andprevious knowledge of the Traditional Chinese Medicine tominimize the risk of participants being able to distinguishthe real acupoints from the sham or the nonspecific acupoint.Recruitment occurred between 23rd September 2015 and 2ndDecember 2015.
3.3. Study Treatment. After enrolment, participants wereasked to keep a sleep diary for oneweek to collect informationon sleep duration, quality, reasons for sleep disturbance,and habits that may influence sleep quality (e.g., caffeineconsumption; Supplementary Appendix 1 in Supplemen-tary Material available online at https://doi.org/10.1155/2017/7570352). At the baseline visit prior to commencementof study treatment, patients were asked to independentlycomplete the PSQI (Supplementary Appendix 2) [41] andshort form-8 (SF-8)Health Survey (SupplementaryAppendix3) [42]. Patients were randomized 1 : 1 to receive either acu-pressure therapy (intervention) or sham acupressure therapy(control) delivered thrice weekly for four consecutive weeksduring their routine dialysis sessions (morning, afternoon,or evening). Participants in the intervention group receivedacupressure therapy on Shen Men (HT7) and Yongquan(K11); participants in the control group received sham acu-pressure therapy on a nonspecific acupoint, Zhongquan (EX-EU3), and a sham acupoint (S) (Supplementary Appendix4). All selected acupoints were stimulated bilaterally. Oneaccredited Traditional Chinese Medicine health practitionerapplied acupressure treatment in all participants of thestudy.
To ensure adequate concealment of allocation, acomputer-generated randomization schedule was kept insequentially numbered, sealed opaque envelopes. Studyparticipants, care providers working in the dialysis units,an outcome assessor, and study statistician were blinded tothe participant’s allocation to minimize the potential forperformance bias. Only the Traditional Chinese Medicinehealth practitioner delivering acupressure was unblindedand was prohibited from revealing the treatment allocationstatus.
The therapy was applied at each acupoint for 3 minutesand the applied intensity was adjusted according to thepatient’s level of tolerance. At the conclusion of the 4th studyweek, all participants were asked to complete a sleep diary,SF-8, PSQI, and treatment acceptability questionnaire (TAQ)(Supplementary Appendix 5) [43]. During the study period,participants were instructed to not make any adjustments topreexisting sleeping aides (e.g., doses of hypnotics, yoga, andtai chi).
3.4. Study Outcomes. The primary outcome was PSQI globaland subscale scores at four weeks. Prespecified secondaryoutcomes were QOL measured using the SF-8 at four weeks,patient acceptability, and adverse events. The SF-8 HealthSurvey includes a total of eight questionnaire items andincorporates two dimensions: (i) a mental component sum-mary (MCS) which reflects mental health, role emotional,and social function and (ii) a physical component summary
(PCS) which reflects physical function and health (licensenumber: QM 034204) [42].
3.5. Statistical Analysis. Baseline characteristics are expressedas frequencies (percentages) for categorical variables, mean± SD for continuous normally distributed variables, andmedian (interquartile range) for continuous nonnormallydistributed variables. Analysis of covariance (ANCOVA)was used to examine the differences in treatment effectsbetween the intervention and control groups adjusted forbaseline measurements. Week four PSQI global scores, MCSand PCS of SF-8, and all the subscales of the PSQI wereanalyzed using ANCOVA. The normality assumption wasassessed by examining residuals from the ANCOVA models.The assumption of homogeneity of within-group regressioncoefficients was assessed by testing the significance of thetreatment group by baseline measurement interaction. Sen-sitivity analyses were performed by including as covariatesin the models two baseline characteristics on which the twogroups were statistically significantly different (duration ofdialysis and hours per dialysis session). Statistical analyseswere performed using Stata/MP 14 (College Station, TX,USA) statistical software. 𝑝 values of <0.05 were consideredto represent a statistically significant result.
3.6. Sample Size. The SIESTA study was a pilot study de-signed to examine the efficacy and acceptability of acu-pressure as a therapy in hemodialysis and hemodiafiltrationpatients in Australia. Therefore, no formal sample size calcu-lation was conducted. The study aimed to recruit at least 40patients, a feasible number considering patient numbers atthe dialysis units and the workload of the practitioner whowould deliver the therapy.
4. Results
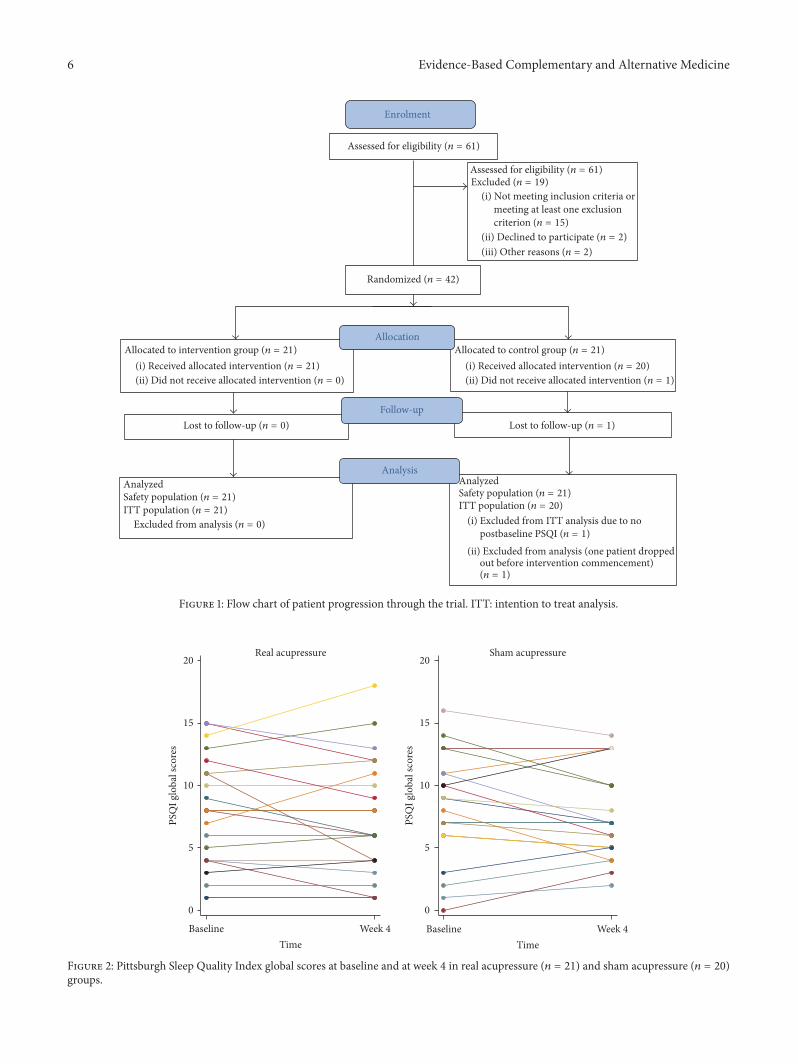
4.1. Patients. Forty-two patients were randomly assigned toreceive either real acupressure therapy (𝑛 = 21) or shamacupressure therapy (control: 𝑛 = 21; Figure 1). One partici-pant declined to participate after randomization but prior toreceiving any treatment. Overall, the groupswere comparableon baseline characteristics except for significantly longerdialysis duration (46 months versus 21.5 months, 𝑝 = 0.04)and duration of each dialysis session (5.2 ± 0.5 versus 4.7± 0.6 hours, 𝑝 = 0.01) in the intervention group (Table 1).At baseline, the intervention group patients reported asignificantly higher frequency of experiencing days with nochance of daytime somnolence compared to the controlgroup (median 4.5 versus 0.5, 𝑝 = 0.03; SupplementaryTable S1). Other parameters reported in the sleep diary werecomparable between the two groups (i.e., sleep duration,ability to fall asleep, mood, exercise, frequency of daytimenaps, and alcohol or caffeine consumption).
4.2. Pittsburg Sleep Quality Index. In general, both groupsdemonstrated a reduction in global PSQI scores frombaselineto week four (Figure 2, Table 2). However, these differenceswere not statistically significant (intervention: difference 0.52,95% CI −1.7 to 0.61, 𝑝 = 0.35; control: difference 0.74,

4 Evidence-Based Complementary and Alternative Medicine
Table 1: Baseline characteristics of treatment group.
Characteristics Intervention (𝑛 = 21) Control (𝑛 = 20)Age (years) 58.6 ± 11.9 51.6 ± 17.9Female 6 (28.6%) 9 (45%)Ethnicity
Caucasian 11 (52%) 13 (65%)Aboriginal and Torres 3 (14%) 1 (5%)Asian 1 (5%) 2 (10%)Maori and Pacific Islander 6 (29%) 4 (20%)
Marital statusMarried or living with a partner 10 (48%) 11 (55%)Single 11 (52%) 9 (45%)
Education statusLess than high school 5 (24%) 3 (15%)High school finished 16 (76%) 17 (85%)
Cause of end-stage kidney stageDiabetes 8 (38%) 7 (35%)Glomerulonephritis 2 (10%) 5 (25%)Hypertension 4 (19%) 1 (5%)Reflux nephropathy 2 (10%) 1 (5%)Polycystic kidneys 1 (5%) 1 (5%)Other 4 (19%) 5 (25%)
ComorbidityCoronary artery disease 10 (48%) 4 (20%)Diabetes 8 (38%) 12 (60%)Hypertension 13 (62%) 11 (55%)Congestive heart failure 2 (10%) 2 (10%)Peripheral vascular disease 6 (29%) 3 (15%)Cerebrovascular disease 3 (14%) 3 (15%)Chronic lung disease 12 (57%) 10 (50%)PLMD/RLS 9 (43%) 6 (30%)Insomnia 2 (10%) 1 (5%)Mood disorder 11 (52%) 6 (30%)Gastroduodenal ulcer or reflux 7 (33%) 10 (50%)
Treatment typeHD 2 (10%) 2 (10%)HDF 19 (90%) 18 (90%)
Dialysis duration (months) 46 [28, 116] 21.5 [13, 56.5]Time of day to have dialysis
Morning 15 (71%) 13 (65%)Afternoon 6 (29%) 6 (30%)Evening 0 (0%) 1 (5%)
Hours per dialysis session 5.2 ± 0.5 4.7 ± 0.6Medications
Antidepressants 5 (24%) 3 (15%)Hypnotics 3 (14%) 1 (5%)Bronchodilators 4 (19%) 1 (5%)Antihistamines 2 (10%) 1 (5%)Proton pump inhibitors 7 (33%) 7 (35%)
Evidence-Based Complementary and Alternative Medicine 5
Table 1: Continued.
Characteristics Intervention (𝑛 = 21) Control (𝑛 = 20)Nonpharmaceutical interventions to aid sleep
Exercise 0 (0%) 4 (20%)Massage 1 (5%) 0 (0%)CPAP machine 2 (10%) 0 (0%)None 18 (86%) 16 (80%)
BMI (kg/m2) 32.9 [26.5, 35.3] 29.65 [21.2, 34]Pre-SBP (mmHg) 148.6 ± 27.5 149.7 ± 23.0Post-DBP (mmHg) 79 ± 16.2 73.6 ± 22.3Hemoglobin (g/L) 116.3 ± 17.1 112.8 ± 10.5Phosphate (mmol/L) 2.0 ± 0.6 2.0 ± 0.6Urea reduction ratioa 0.8 ± 0.1 0.8 ± 0.1KT/Vb 1.4 [1.2, 1.5] 1.3 [1.2, 1.7]PSQI global score 8.1 ± 4.3 8.3 ± 4.4SF-8
Physical component summary (PCS) 43.3 ± 11.5 45.0 ± 10.6Mental component summary (MCS) 45.9 ± 13.6 48.5 ± 10.6
BMI, body mass index; DBP, diastolic blood pressure; HD, hemodialysis; HDF, hemodiafiltration; PSQI, Pittsburgh Sleep Quality Index; SBP, systolic bloodpressure; SF-8, Short Form-8 Health Survey; PMLD, periodic movement disorder; RLS, restless legs syndrome; CPAP, continuous positive airway pressure.Note. Values for categorical variables are given as number (percentage); values for continuous variables are given as mean ± SD if normally distributed or ifnonnormally as median [interquartile range]. aOne missing value in the control group at baseline. bOne missing value in the intervention group at baseline.
Table 2: Primary (PSQI) and secondary (QOL) outcomes at four weeks of treatment group (adjusted for baseline values).
Outcome Intervention (𝑁 = 21) Control (𝑁 = 19) Difference (intervention − control) [95% CI] 𝑝 valuePSQI global scores 7.62 7.42 0.19 [−1.32 to 1.70] 0.80∗PSQI subscalesSleep duration 1.06 1.08 −0.01 [−0.40 to 0.38] 0.95Habitual sleep efficiency 1.12 1.23 −0.11 [−0.72 to 0.50] 0.73Subjective sleep quality 0.84 0.80 0.04 [−0.33 to 0.42] 0.82Sleep latency 1.66 1.48 0.18 [−0.44 to 0.81] 0.55Daytime dysfunctions 0.95 0.95 0.00 [−0.50 to 0.49] 0.99Sleep disturbances 1.58 1.56 0.02 [−0.31 to 0.35] 0.90Use of sleep medicationQOLMCS 47.41 51.30 −3.88 [−8.63 to 0.87] 0.11PCS 44.39 41.94 2.45 [−1.69 to 6.58] 0.24PSQI, Pittsburgh Sleep Quality Index; QOL, quality of life; MCS, mental component summary; PCS, physical component summary.Note. ∗Results for subscale“use of sleep medication” were not included due to a lack of variability in the data.
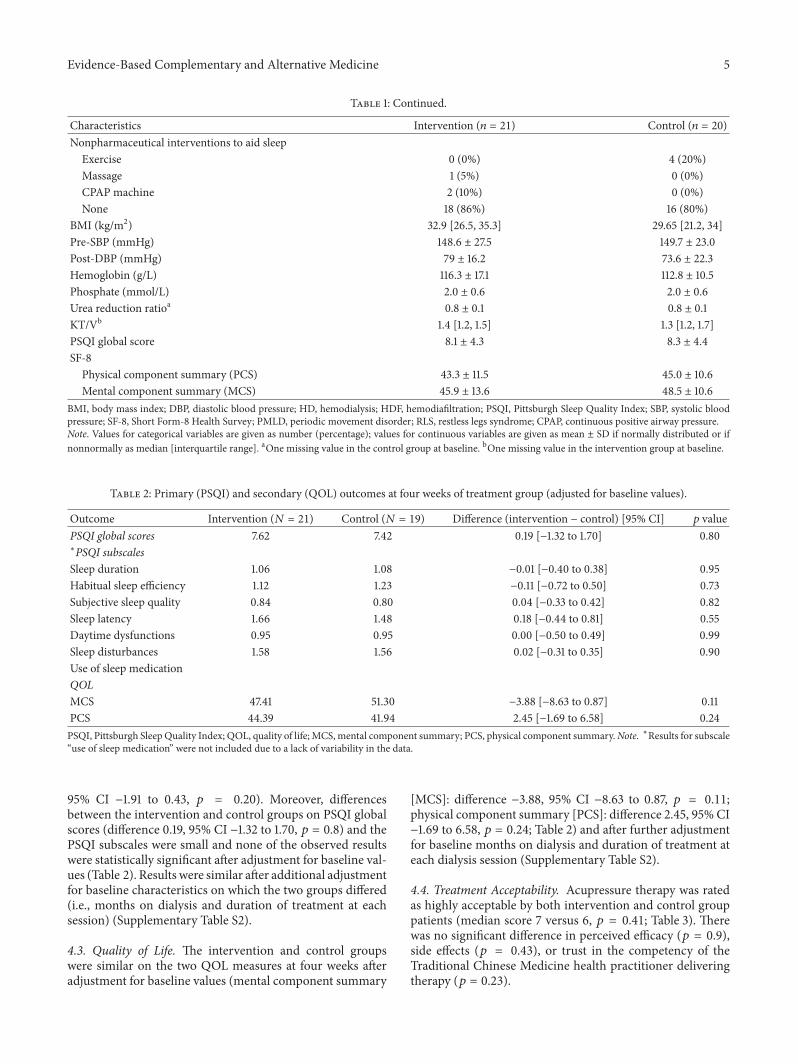
95% CI −1.91 to 0.43, 𝑝 = 0.20). Moreover, differencesbetween the intervention and control groups on PSQI globalscores (difference 0.19, 95% CI −1.32 to 1.70, 𝑝 = 0.8) and thePSQI subscales were small and none of the observed resultswere statistically significant after adjustment for baseline val-ues (Table 2). Results were similar after additional adjustmentfor baseline characteristics on which the two groups differed(i.e., months on dialysis and duration of treatment at eachsession) (Supplementary Table S2).
4.3. Quality of Life. The intervention and control groupswere similar on the two QOL measures at four weeks afteradjustment for baseline values (mental component summary
[MCS]: difference −3.88, 95% CI −8.63 to 0.87, 𝑝 = 0.11;physical component summary [PCS]: difference 2.45, 95% CI−1.69 to 6.58, 𝑝 = 0.24; Table 2) and after further adjustmentfor baseline months on dialysis and duration of treatment ateach dialysis session (Supplementary Table S2).
4.4. Treatment Acceptability. Acupressure therapy was ratedas highly acceptable by both intervention and control grouppatients (median score 7 versus 6, 𝑝 = 0.41; Table 3). Therewas no significant difference in perceived efficacy (𝑝 = 0.9),side effects (𝑝 = 0.43), or trust in the competency of theTraditional Chinese Medicine health practitioner deliveringtherapy (𝑝 = 0.23).
6 Evidence-Based Complementary and Alternative Medicine
Analysis
Allocation
meeting at least one exclusion(i) Not meeting inclusion criteria or
(i) Excluded from ITT analysis due to no
(ii) Excluded from analysis (one patient droppedout before intervention commencement)
Enrolment
Follow-up
Excluded (n = 19)
Randomized (n = 42)
(iii) Other reasons (n = 2)(ii) Declined to participate (n = 2)
criterion (n = 15)
Assessed for eligibility (n = 61)
Assessed for eligibility (n = 61)
(ii) Did not receive allocated intervention (n = 1)(i) Received allocated intervention (n = 20)
Allocated to control group (n = 21)
(ii) Did not receive allocated intervention (n = 0)(i) Received allocated intervention (n = 21)
Lost to follow-up (n = 1)Lost to follow-up (n = 0)
Safety population (n = 21)ITT population (n = 21)
Excluded from analysis (n = 0)
ITT population (n = 20)
postbaseline PSQI (n = 1)
n = 1)(
Allocated to intervention group (n = 21)
AnalyzedSafety population (n = 21)Analyzed
Figure 1: Flow chart of patient progression through the trial. ITT: intention to treat analysis.
0
5
10
15
20
TimeWeek 4
Real acupressure Sham acupressure
PSQ
I glo
bal s
core
s
0
5
10
15
20
PSQ
I glo
bal s
core
s
BaselineTime
Week 4Baseline
Figure 2: Pittsburgh Sleep Quality Index global scores at baseline and at week 4 in real acupressure (𝑛 = 21) and sham acupressure (𝑛 = 20)groups.

Evidence-Based Complementary and Alternative Medicine 7
Table 3: Individual scales of TAQ at four weeks.
Individual scales of TAQ Intervention (𝑛 = 21) Control (𝑛 = 19) 𝑝 valuesQuestion 1: acceptability 7 [6, 7] 6 [6, 7] 0.41Question 2: efficacy 6 [5, 7] 6 [4, 7] 0.90Question 3: side effects 1 [1, 1] 1 [1, 1] 0.43Question 4: trust rank of the therapist 7 [7, 7] 7 [7, 7] 0.23TAQ: treatment acceptability questionnaire.Note: values are given as median [interquartile range].For Question 1, 1 represents “very unacceptable” and 7 represents “very acceptable”; for Question 2, 1 represents “very ineffective” and 7 represents “veryeffective”; for Question 3, 1 represents “very unlikely” and 7 represents “very likely”; for Question 4, 1 represents “very untrustworthy” and 7 represents “verytrustworthy.”
Table 4: Listing of SAEs.
SAEs Treatment group Body system for SAEFluid overload Intervention CardiovascularEye haemorrhage Intervention CardiovascularNecrotising Fasciitis Control MusculoskeletalPhysical trauma Control MusculoskeletalArteriovenous graft failure Control MusculoskeletalChest muscle pain Control OtherSAE: serious adverse event.
4.5. Adverse Events. There were six adverse events (6 par-ticipants) recorded during the study (Table 4), all of whichwere rated as serious adverse events (SAEs) as they led tohospitalization. Two SAEs occurred in the intervention group(fluid overload and ocular hemorrhage) and the remainingfour SAEs occurred in the control group (necrotizing fasciitis,physical trauma, chest muscle pain, and arteriovenous graftfailure). No adverse event was considered by investigatorsto be causally related to the study intervention. No localskin reaction (e.g., bruise) from repeated acupressure wasreported during the study.
5. Discussion
This study demonstrated that, when compared with shamtherapy, four weeks of acupressure did not significantlyimprove sleep quality or quality of life in patients on mainte-nance hemodialysis or hemodiafiltration. Nevertheless, acu-pressure was found to be a safe, well-tolerated, and acceptableform of treatment by study participants.
These findings are in keeping with the outcome of a ran-domized controlled trial conducted in 105 adult hemodialysispatients from four Taiwanese centers where acupressure didnot significantly decrease PSQI scores compared with shamtherapy after 4 weeks [38]. A lack of benefit in improvingsleep quality measured using PSQI from acupressure ther-apy compared to sham therapy was again observed in thepresent study. These results contrast with findings from Araband colleagues, who conducted a single-blind randomizedcontrolled trial in 108 prevalent hemodialysis patients inIran [39]. Participants were randomized to three groups(acupressure, sham acupressure, and a control group who
received routine care only). Total PSQI scores at the end of4 weeks were significantly lower in the acupressure groupcompared to the other two groups.Unfortunately, the analysiswas conducted on a per-protocol basis; the dropout rate wasmoderate (14%), and the statistical methods employed didnot adjust for baseline differences in PSQI global scores [44,45]. Other previous studies have reported beneficial effectsof acupressure on insomnia in patients without chronickidney disease, including the elderly [31, 33], postmenopausalwomen [35], and cancer patients [36].The apparent disparityin findings compared with the present study may relate tothe limitations of the previous studies, including suboptimalmethodologic quality, for example, lacking of placebo control[35, 36], selective outcome reporting [31], and inclusion ofpredominantly Asian patient populations [31, 33, 35, 36].
FromaTraditional ChineseMedicine perspective, insom-nia may arise in end-stage kidney disease patients because ofa dynamic disequilibrium between the kidney (yin or water)andheart (yang or fire), such that the exhaustion of the kidneyyin leads to a failure of the kidney water to restrict the heartfire [46]. Acupressure applied to the HT7 (heart meridian)and K11 (kidney meridian) is thought to restore yin andyang harmony (important for normal sleep-wake rhythm) byadjusting the disturbance of the kidney and heart. However,the mechanism of insomnia is likely to be different betweenindividuals from a Traditional ChineseMedicine perspective.For instance, besides the yin-yang disequilibriumwhich is theholistic mechanism of insomnia, there are other conditionsknown to promote insomnia, such as the deficiency of the“Qi and blood” of the heart and spleen, and the internaldisturbance of pyrophlegm [47]. For each patient diagnosedwith specific conditions, the optimal acupoints, intensity, andfrequency of stimulation are different. However, in order tostandardize the delivery of treatment, all patients receivedtreatments at the same acupoints based on their treatmentallocation status in the present study. Therefore, this “onesize fits all” approach could have potentially blunted thereal general effects of the individualized acupressure therapy,which is utilized in a real-world setting.
From a Western medicine perspective, the mechanismunderpinning any beneficial effects of acupressure is uncer-tain but may relate to an effect of massage on relaxation [48].Alternatively, acupressure applied to acupoints may promoterelaxation through the stimulation of neurotransmitters, suchas serotonin [49].

8 Evidence-Based Complementary and Alternative Medicine
The strengths of this study include concealed randomallocation of treatments, involvement of two centers, use ofa sham therapy control, examination of safety and treatmentacceptability, blinding of outcome assessors, broad inclusioncriteria (i.e., patients with self-reported poor sleep qual-ity independent of PSQI scores were eligible), and robuststatistical adjustment for baseline values. These strengthsshould be balanced against the trial’s limitations, includinga lack of blinding of the therapist delivering treatment,which could have introduced the risk of performance bias.However, the therapist was prohibited from disclosing thetreatment allocation status, and data from questionnaireswere independently assessed by a blinded outcome assessor(YC), to further reduce the risk of bias. As this was apilot study, the sample size was small which could haveintroduced the risk of type 2 statistical error. However, theobserved effect size between the two treatment groups wassmall (mean difference 0.19; Table 2) and unlikely to beconsidered a clinically meaningful improvement. Nonethe-less, therapy was delivered thrice weekly during dialysissessions for four weeks, and it remains unknown whetheran increase in therapy frequency (e.g., daily) or duration(e.g., eight weeks) or nocturnal treatment would result inclinically significant benefit. Indeed, there is limited, lowquality evidence suggesting that the use of overnight wristcompression with acupressure devices has beneficial effectson sleep quality in patients without kidney disease [50].The acupressure points chosen for the intervention groupmay also not have been the most appropriate point to helpimprove insomnia at an individual level, and sham acupres-sure points could have had a positive impact on insomnia. Inaddition, decreasing global PSQI scores in both interventionand sham groups were observed, which is consistent withthe placebo effect from receiving “therapy.” Finally, indi-vidualized therapy is a major characteristic of TraditionalChinese Medicine. However, it is difficult to incorporatethis level of individualization of therapy into practice in arandomized controlled trial which evaluates the response ofa group of individuals to a “one size fits all” therapeuticapproach.
6. Conclusion
In conclusion, the present pilot study identified that acupres-sure is a safe, well-tolerated, and highly acceptable therapy inadult hemodialysis patients in a Western healthcare settingbut did not result in any clinically meaningful improvementin sleep quality or quality of life compared with shamtherapy.
Competing Interests
The authors have no conflict of interests to declare.
Authors’ Contributions
Kunyu Shen and Yeoungjee Cho contributed equally to thepaper.
Acknowledgments
The authors would like to thank Liza Vergara for producingthe sealed envelopes and Donna Riedlinger for assistancewith obtaining a license for the SF-8 Survey.
References
[1] A. V. Lindner, M. Novak, M. Bohra, and I. Mucsi, “Insomnia inpatients with chronic kidney disease,” Seminars in Nephrology,vol. 35, no. 4, pp. 359–372, 2015.
[2] F. B. Brekke, A. Amro, T. B. H. Osthus, T. Dammen, B.Waldum,and I. Os, “Sleep complaints, depression and quality of life inNorwegian dialysis patients,” Clinical Nephrology, vol. 80, no. 2,pp. 88–97, 2013.
[3] W.-C. Chen, P.-S. Lim, W.-C. Wu et al., “Sleep behaviordisorders in a large cohort of Chinese (Taiwanese) patientsmaintained by long-term hemodialysis,” American Journal ofKidney Diseases, vol. 48, no. 2, pp. 277–284, 2006.
[4] I. Mucsi, M. Z. Molnar, J. Rethelyi et al., “Sleep disorders andillness intrusiveness in patients on chronic dialysis,”NephrologyDialysis Transplantation, vol. 19, no. 7, pp. 1815–1822, 2004.
[5] F. E. M. Murtagh, J. Addington-Hall, and I. J. Higginson, “Theprevalence of symptoms in end-stage renal disease: a systematicreview,” Advances in Chronic Kidney Disease, vol. 14, no. 1, pp.82–99, 2007.
[6] S. Walker, A. Fine, and M. H. Kryger, “Sleep complaintsare common in a dialysis unit,” American Journal of KidneyDiseases, vol. 26, no. 5, pp. 751–756, 1995.
[7] M. L. Unruh, D. J. Buysse, M. A. Dew et al., “Sleep quality andits correlates in the first year of dialysis,” Clinical Journal of theAmerican Society of Nephrology, vol. 1, no. 4, pp. 802–810, 2006.
[8] G. Merlino, A. Piani, P. Dolso et al., “Sleep disorders in patientswith end-stage renal disease undergoing dialysis therapy,”Nephrology Dialysis Transplantation, vol. 21, no. 1, pp. 184–190,2006.
[9] M. Karasek, A. Szuflet, W. Chrzanowski, K. Zylinska, and J.Swietoslawski, “Decreased melatonin nocturnal concentrationsin hemodialyzed patients,” Neuroendocrinology Letters, vol. 26,no. 6, pp. 653–656, 2005.
[10] L. C. Lack,M. Gradisar, E. J.W. Van Someren, H. R.Wright, andK. Lushington, “The relationship between insomnia and bodytemperatures,” Sleep Medicine Reviews, vol. 12, no. 4, pp. 307–317, 2008.
[11] D. Zepeda-Orozco and R. Quigley, “Dialysis disequilibriumsyndrome,” Pediatric Nephrology, vol. 27, no. 12, pp. 2205–2211,2012.
[12] S. J. Elder, R. L. Pisoni, T. Akizawa et al., “Sleep quality predictsquality of life and mortality risk in haemodialysis patients:results from the dialysis outcomes and practice patterns study(DOPPS),” Nephrology Dialysis Transplantation, vol. 23, no. 3,pp. 998–1004, 2008.
[13] N. T. Vozoris, “The relationship between insomnia symptomsand hypertension using United States population-level data,”Journal of Hypertension, vol. 31, no. 4, pp. 663–671, 2013.
[14] X. Guo, S. Yu, Z. Li et al., “Self-reported sleep durationis associated with reduced glomerular filtration rate amongadults with hypertension: a population-based study from ruralnortheast China,” Journal of Sleep Research, vol. 24, no. 3, pp.351–358, 2015.
[15] R. Yamamoto, Y. Nagasawa, H. Iwatani et al., “Self-reportedsleep duration and prediction of proteinuria: a retrospective
Evidence-Based Complementary and Alternative Medicine 9
cohort study,” American Journal of Kidney Diseases, vol. 59, no.3, pp. 343–355, 2012.
[16] E. Van Cauter, “Sleep disturbances and insulin resistance,”Diabetic Medicine, vol. 28, no. 12, pp. 1455–1462, 2011.
[17] C. Meisinger, M. Heier, and H. Loewel, “Sleep disturbance as apredictor of type 2 diabetes mellitus in men and women fromthe general population,”Diabetologia, vol. 48, no. 2, pp. 235–241,2005.
[18] S. Schwartz, W. M. Anderson, S. R. Cole, J. Cornoni-Huntley, J.C. Hays, and D. Blazer, “Insomnia and heart disease: a review ofepidemiologic studies,” Journal of Psychosomatic Research, vol.47, no. 4, pp. 313–333, 1999.
[19] C. Baglioni, G. Battagliese, B. Feige et al., “Insomnia as a pre-dictor of depression: a meta-analytic evaluation of longitudinalepidemiological studies,” Journal of Affective Disorders, vol. 135,no. 1-3, pp. 10–19, 2011.
[20] M. Novak, I. Mucsi, C. M. Shapiro, J. Rethelyi, and M. S. Kopp,“Increased utilization of health services by insomniacs—an epi-demiological perspective,” Journal of Psychosomatic Research,vol. 56, no. 5, pp. 527–536, 2004.
[21] B. C. P. Koch, J. E. Nagtegaal, E. C. Hagen et al., “Subjective sleepefficiency of hemodialysis patients,”Clinical Nephrology, vol. 70,no. 5, pp. 411–418, 2008.
[22] B. C. P. Koch, J. E. Nagtegaal, E. C. Hagen et al., “The effectsof melatonin on sleep–wake rhythm of daytime haemodialysispatients: a randomized, placebo-controlled, cross-over study(EMSCAP study),” British Journal of Clinical Pharmacology, vol.67, no. 1, pp. 68–75, 2009.
[23] Y. Hou, P. Hu, Y. Liang, and Z. Mo, “Effects of cognitivebehavioral therapy on insomnia of maintenance hemodialysispatients,”Cell Biochemistry andBiophysics, vol. 69, no. 3, pp. 531–537, 2014.
[24] E. J. Stepanski and J. K. Wyatt, “Use of sleep hygiene in thetreatment of insomnia,” SleepMedicine Reviews, vol. 7, no. 3, pp.215–225, 2003.
[25] M. K. Means, K. L. Lichstein, M. T. Epperson, and C. T.Johnson, “Relaxation therapy for insomnia: nighttime and daytime effects,” Behaviour Research andTherapy, vol. 38, no. 7, pp.665–678, 2000.
[26] T. Heidenreich, I. Tuin, B. Pflug, M. Michal, and J. Michalak,“Mindfulness-based cognitive therapy for persistent insomnia:a pilot study,” Psychotherapy and Psychosomatics, vol. 75, no. 3,pp. 188–189, 2006.
[27] R. Afshar, A. Emany, A. Saremi, N. Shavandi, and S. Sanavi,“Effects of intradialytic aerobic training on sleep quality inhemodialysis patients,” Iranian Journal of Kidney Diseases, vol.5, no. 2, pp. 119–123, 2011.
[28] B. C. P. Koch, E. C. Hagen, J. E. Nagtegaal, J. B. S. Boringa, G. A.Kerkhof, and P. M. Ter Wee, “Effects of nocturnal hemodialysisonmelatonin rhythmand sleep-wake behavior: an uncontrolledtrial,” American Journal of Kidney Diseases, vol. 53, no. 4, pp.658–664, 2009.
[29] K. P. Parker, J. L. Bailey, D. B. Rye, D. L. Bliwise, and E. J. W.Van Someren, “Lowering dialysate temperature improves sleepand alters nocturnal skin temperature in patients on chronichemodialysis,” Journal of Sleep Research, vol. 16, no. 1, pp. 42–50, 2007.
[30] H. Montakab, Acupuncture for Insomnia: Sleep and Dreams inChinese Medicine, GeorgThieme, Stuttgart, Germany, 2012.
[31] M.-L. Chen, L.-C. Lin, S.-C. Wu, and J.-G. Lin, “The effec-tiveness of acupressure in improving the quality of sleep of
institutionalized residents,” Journals of Gerontology—Series ABiological Sciences and Medical Sciences, vol. 54, no. 8, pp.M389–M394, 1999.
[32] N. S. Gooneratne, “Complementary and alternative medicinefor sleep disturbances in older adults,” Clinics in GeriatricMedicine, vol. 24, no. 1, pp. 121–138, 2008.
[33] H. Reza, N. Kian, Z. Pouresmail, K. Masood, M. Sadat SeyedBagher, and M. A. Cheraghi, “The effect of acupressure onquality of sleep in Iranian elderly nursing home residents,”Complementary Therapies in Clinical Practice, vol. 16, no. 2, pp.81–85, 2010.
[34] J.-L. Sun, M.-S. Sung, M.-Y. Huang, G.-C. Cheng, and C.-C.Lin, “Effectiveness of acupressure for residents of long-termcare facilities with insomnia: a randomized controlled trial,”International Journal of Nursing Studies, vol. 47, no. 7, pp. 798–805, 2010.
[35] Y.-Y. Kung, C. C. H. Yang, J.-H. Chiu, and T. B. J. Kuo, “Therelationship of subjective sleep quality and cardiac autonomicnervous system in postmenopausal women with insomniaunder auricular acupressure,”Menopause, vol. 18, no. 6, pp. 638–645, 2011.
[36] R. Cerrone, L. Giani, B. Galbiati et al., “Efficacy of HT 7 pointacupressure stimulation in the treatment of insomnia in cancerpatients and in patients suffering from disorders other thancancer,”Minerva Medica, vol. 99, no. 6, pp. 535–537, 2008.
[37] A. Shariati, S. Jahani, M. Hooshmand, and N. Khalili, “Theeffect of acupressure on sleep quality in hemodialysis patients,”Complementary Therapies in Medicine, vol. 20, no. 6, pp. 417–423, 2012.
[38] S.-L. Tsay and M.-L. Chen, “Acupressure and quality of sleep inpatients with end-stage renal disease—a randomized controlledtrial,” International Journal of Nursing Studies, vol. 40, no. 1, pp.1–7, 2003.
[39] Z. Arab, A. R. Shariati, H. Asayesh, M. A. Vakili, H. Bahrami-Taghanaki, and H. Azizi, “A sham-controlled trial of acupres-sure on the quality of sleep and life in haemodialysis patients,”Acupuncture in Medicine, vol. 34, no. 1, pp. 2–6, 2016.
[40] Good clinical practice in Australia, https://www.austral-ianclinicaltrials.gov.au/researchers/good-clinical-practice-gcp-australia.
[41] D. J. Buysse, C. F. Reynolds III, T.H.Monk, S. R. Berman, andD.J. Kupfer, “The Pittsburgh sleep quality index: a new instrumentfor psychiatric practice and research,” Psychiatry Research, vol.28, no. 2, pp. 193–213, 1989.
[42] J. E. Ware and GlaxoSmithKline, How to Score and InterpretSingle-Item Health Status Measures: A Manual for Users of theof the SF-8 Health Survey: (with a Supplement on the SF-6Health Survey), QualityMetric Inc, Lincoln, RI, USA; HealthAssessment Lab, Boston, Mass, USA, 2001.
[43] J. Hunsley, “Development of the treatment acceptability ques-tionnaire,” Journal of Psychopathology and Behavioral Assess-ment, vol. 14, no. 1, pp. 55–64, 1992.
[44] J. Dettori, “Loss to follow-up,” Evidence-Based Spine-Care Jour-nal, vol. 2, no. 1, pp. 7–10, 2011.
[45] H. J. Keselman, C. J. Huberty, R. A. Cribbie et al., “Sta-tistical practices of educational researchers: an analysis oftheir ANOVA, MANOVA, and ANCOVA analyses,” Review ofEducational Research, vol. 68, no. 3, pp. 350–386, 1998.
[46] “The kidney’s relationship with the heart,” http://www.shen-nong.com/eng/principles/affectheart.html.
10 Evidence-Based Complementary and Alternative Medicine
[47] L. Chen, S. Lili, X. Wang, and F. Zhang, “Literature studyon acupoint and prescription of acupuncture for treatment ofinsomnia,” Journal of Traditional Chinese Medicine, no. 53, pp.1051–1054, 2012 (Chinese).
[48] G. C. Goats, “Massage—the scientific basis of an ancient art:part 2—physiological and therapeutic effects,” British Journal ofSports Medicine, vol. 28, no. 3, pp. 153–156, 1994.
[49] A. Chen, “Effective acupuncture therapy for stroke and cere-brovascular diseases - Part III: prescription for prevention,”American Journal of Acupuncture, vol. 21, no. 4, pp. 305–318,1993.
[50] M. Nordio and F. Romanelli, “Efficacy of wrists overnightcompression (HT 7 point) on insomniacs: possible role ofmelatonin?”Minerva Medica, vol. 99, no. 6, pp. 539–547, 2008.
Submit your manuscripts athttps://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com