Embed Size (px)
Citation preview

The Science of Targeting and its Application in Health Care
Lisa A. Cooper, MD, MPH
April 8, 2010
Goal: To describe how we learn about group characteristics and develop skills that foster better delivery of health care

Objectives
1. Describe approaches to enhancing cultural sensitivity in health care
2. Provide examples of demographic, social, and cultural targeting in marketing messages and health care interventions
3. Identify effective strategies for demographic targeting that optimize positive images and minimize negative stereotypes and stigma
4. Explain how targeting and tailoring can be combined to acknowledge individual differences when designing population-level interventions

Targeting versus Tailoring
• Targeted interventions involve messages that are intended to reach population subgroups based on a specific set of shared characteristics
• Tailored interventions, involve messages that are intended to reach an individual based on specific characteristics of the individual as measured in a formal assessment process

Approaches to Enhancing Cultural Sensitivity in Health Care
• Early programs: cross-cultural medicine, cultural sensitivity, trans-cultural nursing, and multicultural counseling
• Focused on those “whose health beliefs may be at variance with biomedical models” – e.g. groups with limited English proficiency, non-Western
cultures, etc.
• Original approaches called for awareness and respect for different traditions, but recognized– detailed knowledge about all cultures was impractical– viewing patients as members of ethnic/cultural groups
might lead to stereotyping

Evolution of Cultural CompetenceEarly models recognized the need for “generic” attitudes not specific to a particular culture:
1) respecting the legitimacy of patients’ health beliefs 2) shifting from a paradigm of viewing patients’ complaints
as stemming from a disease to that of an illness occurring within a biopsychosocial context
3) eliciting patients’ explanatory model of illness 4) explaining the clinician’s explanatory model of illness in
language accessible to patients5) negotiating an understanding within which a safe,
effective, and mutually agreeable treatment plan could be implemented
Berlin & Fowkes (1983); Kleinman et al. (1978); Leininger (1978)
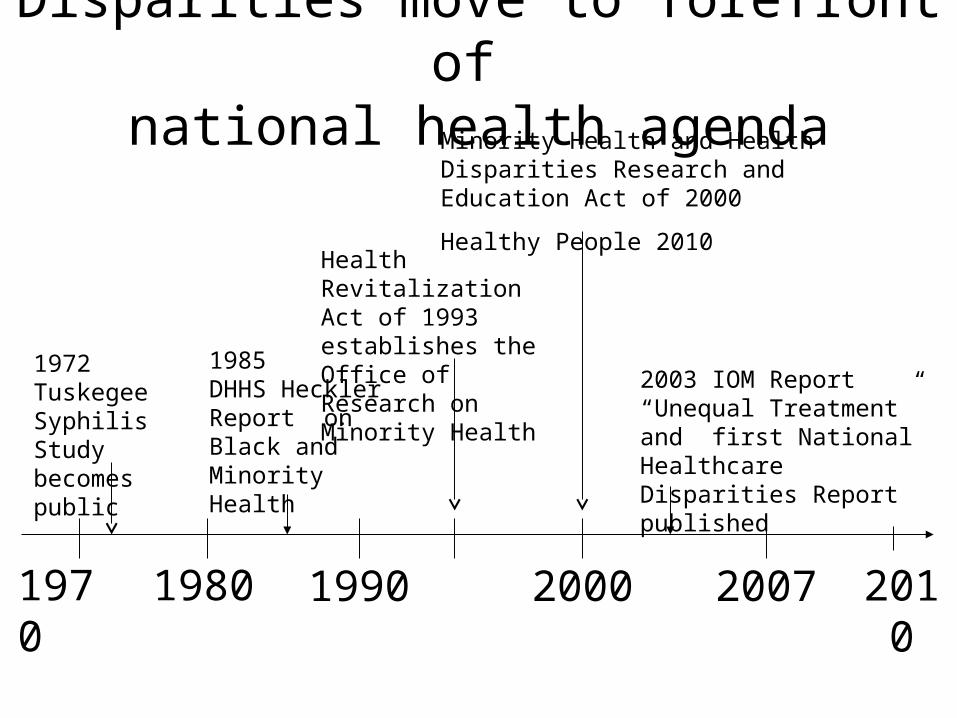
Disparities move to forefront of national health agenda
1970 20071990
1985 DHHS Heckler Report on Black and Minority Health
Minority Health and Health Disparities Research and Education Act of 2000
Healthy People 2010
2003 IOM Report “Unequal Treatment” and first National Healthcare Disparities Report published
1972Tuskegee Syphilis Study becomes public
1980
Health Revitalization Act of 1993 establishes the Office of Research on Minority Health
2000 2010

Expansion of Cultural Competence
Early models (cross-cultural)
Newer models(Cultural Competence)
Populations Immigrants, refugees
All people of color, other disadvantaged groups
(those affected by health disparities)
Concepts Culture, Language
Culture, Language, Prejudice, Stereotyping, Social Determinants of Health
Scope Interpersonal interactions
Health Care Systems, Communities

Definitions of Cultural Competence
• Interpersonal Cultural Competence– The ability of individual health care professionals to
establish effective interpersonal and working relationships with patients (and each other) that supersede cultural differences1
• Health System Cultural Competence– The ability of health care providers and organizations to
understand and respond effectively to the cultural and linguistic needs brought by patients to the health care encounter2
1Cooper & Roter, 2OMH 2001
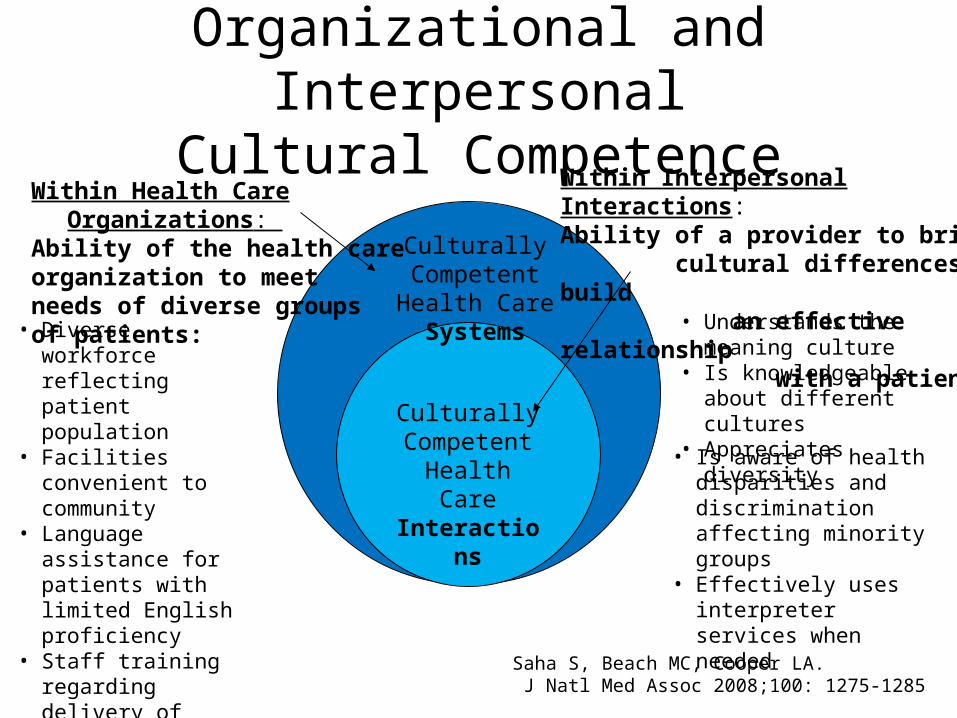
Organizational and InterpersonalCultural Competence
Within Health Care Organizations: Ability of the health care organization to meet needs of diverse groups of patients:
Culturally Competent Health
Care Systems
Culturally Competent Health Care Interactions
Within Interpersonal Interactions: Ability of a provider to bridge cultural differences to build an effective relationship with a patient:
• Understands the meaning culture
• Is knowledgeable about different cultures
• Appreciates diversity• Is aware of health
disparities and discrimination affecting minority groups
• Effectively uses interpreter services when needed
• Diverse workforce reflecting patient population
• Facilities convenient to community
• Language assistance for patients with limited English proficiency
• Staff training regarding delivery of culturally and linguistically appropriate services
• Culturally appropriate health education materials
Saha S, Beach MC, Cooper LA. J Natl Med Assoc 2008;100: 1275-1285

Using Behavioral Models to Understand Ethnic Differences in Care-Seeking for Depression
Behavioral beliefs
Effectiveness
Medications
Counseling
Prayer
Perceived need
Value of outcome
External Variables
Demographics
Race, Ethnicity Gender, Age, Education
Illness variables
Treatment Experience
Social Support
Life Events
Internal Variables
Normative beliefs
Family would be disappointed
Attitudes toward behavior
Treatment acceptability
Subjective norms
Employer stigma Friend stigma
Behavioral Intention
Plans to seek help
Behavior
Seeks treatment
Modified from The Theory of Reasoned Action (Azjen, 1996)

Sample Comments Made by Patients in Depression Focus Groups
“I did pray a lot. I’m a Christian, and I would pray and pray and find verses of scripture.”
African-American male, age 30
Spirituality
Cooper-Patrick L et al, JGIM 1997;12:431-438

Sample Comments Made by Patients in Depression Focus Groups
“And I didn’t want anyone to know that I was taking this prescription. I just didn’t
want to feel like I was crazy.”
African-American female, age 53
Stigma
Cooper-Patrick L et al, JGIM 1997;12:431-438

Sample Comments Made by Patients in Depression Focus Groups
“This guy [my doctor] was just a plain old nice guy, you know…he was very, very
sharp…I thought, whatever this guy tells me for the most part, if it sounds sensible, I’ll
give it a try.”
African American male, age 28
Patient-provider relationships
Cooper-Patrick L et al, JGIM 1997;12:431-438

Sample Comments Made by Patients in Depression Focus Groups
“If it’s gonna make me feel good, make me feel good right away so I can get up
and start doing what I want to do. I don’t want it to take a long time to kick in.”
female, age 41
Attributes of treatment: Medicines
Cooper-Patrick L et al, JGIM 1997;12:431-438

Sample Comments Made by Patients in Depression Focus Groups
“When you explain to me what the medicine’s going to do and what I can expect
from it, I feel much more comfortable.”
female, age 41
Attributes of treatment: Patient education
Cooper-Patrick L et al, JGIM 1997;12:431-438

Most Important Aspects of Depression Care to Patients
1. Health provider interpersonal skills
2. Treatment effectiveness
3. Treatment problems
4. Patient education, information, and understanding
5. Intrinsic spirituality * (African Americans)
6. Financial access
7. Primary care provider recognition of depression
Cooper LA et al, Gen Hosp Psychiatry 2000;22:163-173

African Americans rate spirituality as more important in depression care
Cooper LA et al, Journal of General Internal Medicine 2001;16:634-638
All p-values <0.05
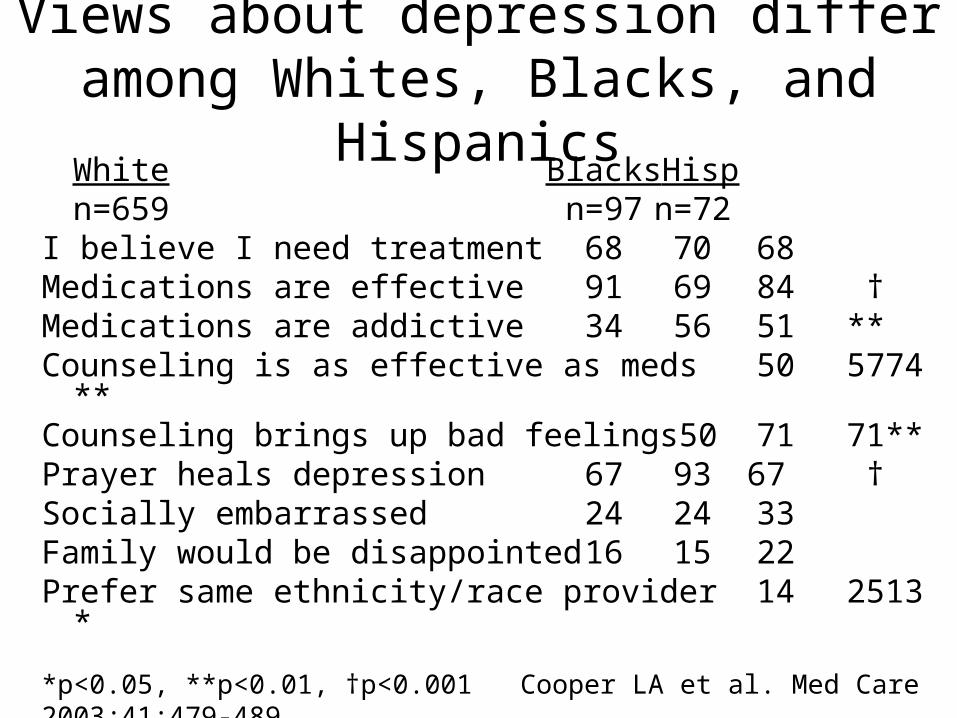
Views about depression differ among Whites, Blacks, and Hispanics
White Blacks Hispn=659 n=97 n=72
I believe I need treatment 68 70 68Medications are effective 91 69 84 †Medications are addictive 34 56 51 **Counseling is as effective as meds 50 57 74 **Counseling brings up bad feelings 50 71 71 **Prayer heals depression 67 93 67 †Socially embarrassed 24 24 33Family would be disappointed 16 15 22Prefer same ethnicity/race provider 14 25 13 *
*p<0.05, **p<0.01, †p<0.001 Cooper LA et al. Med Care 2003;41:479-489

Physicians engage in less depression talk and rapport-building with depressed African Americans
Ghods BK, Roter D, Ford DE, Larson S, Arbelaez J, Cooper LA. J Gen Intern Med 2008; 23:600-6
P=0.04 P=0.01
P=0.07
P=0.30

Questions to guide selection of tailored vs. targeted message strategy• Is there variability on the key determinants of depression
care-seeking?– Tailoring: high
– Targeted: high or low
• Are there mechanisms for gathering individual-level data from the target population?– Tailored: needed
– Targeted: not needed
• What is the level of awareness or understanding of the problem in the target population?– Tailored: high
– Targeted: high or low

Black and Blue: A culturally targeted videotape about depression

Sample comments made by patients in videotape focus group
Theme Sample Comments
Most effective parts of the videotape
“I think having real people with real problems was effective.”
Ways to improve the videotape
“It would have been more effective if maybe we had more specifics on what caused their depression, and how they got through it, and what treatment worked for them.”
Identification with people in the videotape
“Depression, in the younger fellow who talked, yes, everything he said hit home to me.”
Primm AB, Cabot D, Pettis J, Vu HT, Cooper LA. J Natl Med Assoc 2000;94:1007-1016

Sample comments made by patients in videotape focus group
Theme Sample Comments
Race, ethnicity and cultural issues
“I’ve never really paid much attention to videos in the past because they mainly had Caucasians that I couldn’t really relate to, and to sit here and watch something with people who look like me, talk like me, and went through what I went through, seeing is believing that black people have gone through this.”
“A lot of reasons we [blacks] don’t seek out this help that we so desperately need, is because as African-American children, we’re taught to be strong-don’t let them see you cry. Then when you show up you don’t know what to say, “ I need help, can somebody help me?”

Sample comments made by patients in videotape focus group
Theme Sample Comments
Stigma and stereotypes
“I was surprised to see so many men [in the video] because a lot of times [depression] is called the woman’s disease because men don’t really get upset ‘cause they have a strong backbone, so it was cool to see men going though it.”
Spirituality “The other thing [that was effective about the video] as the faith piece, other people who are of your faith that tell you, you don’t pray, you need to pray harder, that’s all you need to do. That’s not true.”

Agreement with statements about medical aspects of depression
Primm AB, Cabot D, Pettis J, Vu HT, Cooper LA. J Natl Med Assoc 2000;94:1007-1016

Agreement with statements about treatment effectiveness

Disagreement with statementsabout treatment problems

Disagreement with statements about spirituality

Disagreement withstatements about stigma

Strategies for effective targeting• Optimize positive images
– Feature African Americans (regular and successful people) who have experienced depression and gotten better
• Dispel misconceptions– Discuss common myths and counteract with information
• Avoid negative stereotypes– Depression is a medical illness, not a character weakness or
something to be ashamed of
• Reduce stigma– Use public figures as role models
– Encourage relatives and friends of depressed individuals to try to understand the illness and be supportive
• Design: Cluster randomized trial• Population: 27 primary care providers and 132 African
American patients with depression • Setting: 10 urban, community-based clinics in
Baltimore, MD and Wilmington, DE• Interventions:
– Standard quality improvement program– Patient-centered, culturally targeted program
• Outcomes: depression resolution, guideline-concordant care, and patient ratings of care at 6 & 12 mo follow up
Blacks Receiving Interventions for Depression and Gaining Empowerment
Supported by the Agency for Healthcare Research and QualityCooper LA, Ford DE, Ghods BK, et al. Implementation Science. 2010; 5(1):18

Provider Recruitment
Patient-Centered Intervention
ProvidersN=15
*DCM contacts for active follow-up up to 12 months
Standard Intervention
ProvidersN=15
Standard Intervention
Patients*N=125
Patient-CenteredIntervention
Patients*N=125
Patient Recruitment

Bridge Study Primary Care Clinician Intervention Features
Intervention Standard Intervention
Patient-Centered
Intervention
Two academic detailing visits (CME credit)
X X
Psychiatric consultation liaison support
X X
Communication skills on interactive CD-ROM
X
Culture-specific information
X

Examples of Clinician Goals
• Improve recognition• Evaluate associated conditions• Assess suicidal ideation• Change usual antidepressant• Identify patients’ cultural
beliefs• Elicit patients’ preferences

Functions of the Medical Interview
• Data-gathering
• Patient education and counseling
• Rapport-building
• Facilitation and patient activation
Lipkin, Putnam, & Lazare, 1995
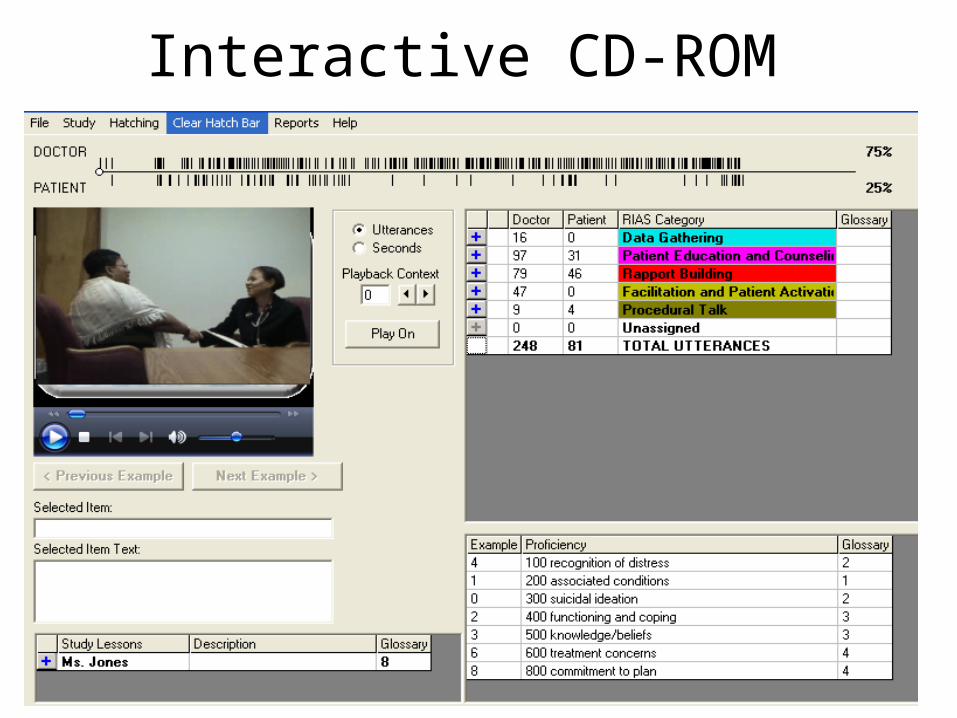
Interactive CD-ROM

Bridge Study Patient InterventionsIntervention Standard
InterventionPatient-Centered
Intervention
Needs Assessment X
Patient Centered Needs Assessment X
Education and Activation X X
Social support/informal counseling X X
Standard education materials X
Culturally targeted education materials X
Black Mental Health Alliance List X
Cultural information packet for MH Providers
X

The standard needs assessment is generic and disease-oriented
• Depressive symptoms
• Associated conditions
• Functional Status/Activities affected
• Stressors
• Social Support
• Treatment preferences

Standard InterventionPatient Education Materials
• Brochure
• Book
• DVD

The patient-centered needs assessment combines targeted and
tailored approaches• Meaning of illness from patient perspective• Perceptions of racial discrimination • Literacy and language concerns• Importance of spirituality in coping and care• Specific treatment concerns regarding
antidepressants or counseling• Financial concerns• Role of stigma• Relationships with health professionals

Patient-Centered Intervention Patient Education Materials
• Brochure
• Book
• Videotape
• Prayer card*
• Bridge Study calendar
*only if patient is spiritually oriented and/or receptive

Patients rated the patient-centered depression care manager as more helpful
*p<0.05

More patients read books and brochures -- half watched videos
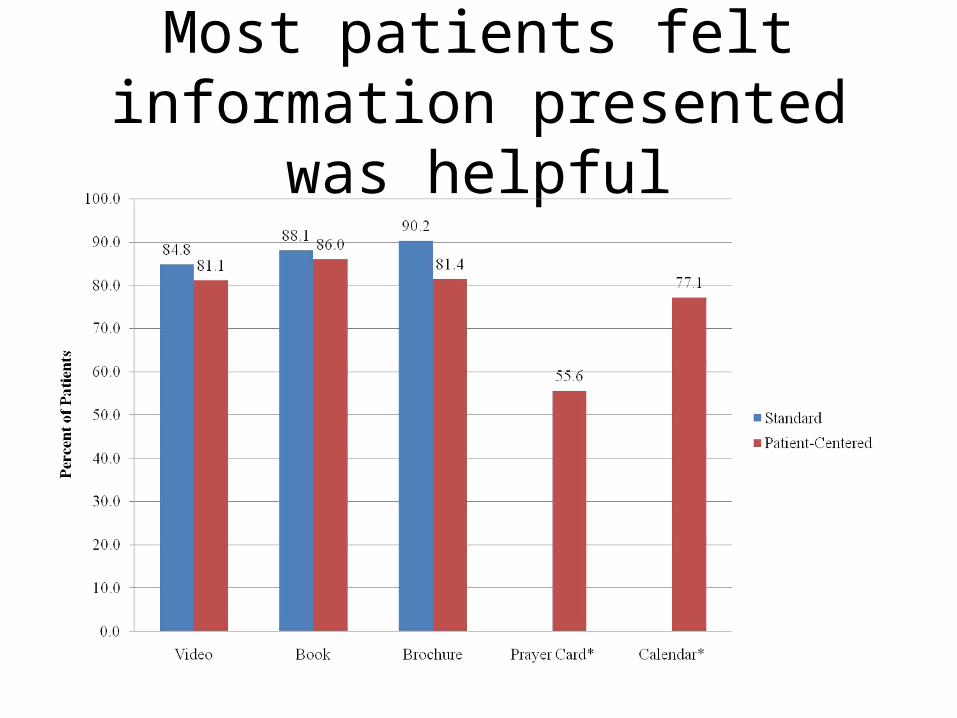
Most patients felt information presented was helpful

Most patients could identify with messages in the materials

More family members and close friends used targeted materials

Conclusions• Cultural targeting has been identified as a
potential strategy for overcoming disparities in health care
• Behavioral models can be used to identify appropriate content and strategies for targeting in healthcare interventions and materials
• Gathering data/input from targeted groups can enhance acceptability and uptake of interventions
• Combining targeting and tailoring improves perceived relevance and minimizes stereotyping

Discussion Points
• What is the added benefit of targeting over generic approaches for particular behaviors?
• For which groups is targeting most effective?
• How much customization of messaging is needed to achieve relevance?
• When is customization perceived as negative?
• Should customization be implicit or explicit?
• What are the pros and cons of being more inclusive versus more targeted in one’s approach?





























