Embed Size (px)
Citation preview

MIG_01161_Migraine Pathophysiology_DT3 3/28/2016 11:34 AM
Eric J. Eross, D.O.Director, The CORE Institute Center for Headache Medicine
Fellowship‐Trained Headache Medicine Specialist, Mayo ClinicAssociate Clinical Professor, Midwestern University
Founder & President, Glia Sciences, INC.
Financial Disclosures:
Grant / Research Support
Clinical / Research Consultant
Speakers’ Bureau Major Stock Holder/ Investor
Other Financial / Material Support
Allergan YES no YES no no
ATI YES no no no no
Avinir no no YES no no
Depomed no no YES no no
Eli Lilly YES no no no no
Glia Sciences YES YES YES YES YES
Pernix no no YES no no
Teva no no YES no no
Upsher-Smith no YES no no no

Overview of Presentation
Clinical Features
PathophysiologyEffective Treatments
Overview of Presentation
Throbbing / Pounding
Worsening with Activity
Photophobia / Phonophobia
Nausea and Vomiting
Allodynia
Misdiagnosis as Sinus Headache
Misdiagnosis as Tension-Type Headache
Medication Overuse Headache (MOH)
Migraine specific acute treatments- triptans
DHE vs. triptan site(s) of action
Early vs. late treatment
Treatment while experiencing allodynia
Rescue with NSAID’s or steroids
MOA for preventative pharmaceuticals
CLINICAL FEATURES: EFFECTIVE TREATMENT:
Common triggers
Family history
MOA of osteopathic manipulation
New targets- CGRP, Sub P, NKA, etc.
MOA of blocks, stimulators, OT-A, TCMS

Objectives:
List the (ICHD-3 beta) diagnostic criteria for migraine headache and apply them effectively in clinical practice
Briefly explain the pathophysiology behind the main clinical features seen in migraine
Describe the site and mechanism(s) of action of at least three acute and three preventative treatments for migraine
Migraine Prevalence Compared With Other Neurologic Diseases
0.09% 0.71% 0.96% 1%
6.7%
12.1%
0
5
10
15
MS Epilepsy PD+HD Stroke AD Migraine
MS = multiple sclerosis; PD+HD = Parkinson disease + Huntington disease; AD = Alzheimer’s disease.1. Hirtz D. et al. Neurology. 2007;68:326–337. 2. National Institute of Neurological Disorders and Stroke. Available at: www.ninds.nih.gov. Accessed May 17, 2007.
Dis
ease
pre
vale
nce
, % 9.46%1.3x
Migraine: A Disabling Headache Disorder Burden
– Among the world’s 20 most disabling diseases (WHO)– Indirectly costs employers up to $13 billion per year– Direct medical costs exceed $1 billion per year
– “same level of disability as dementia, quadriplegia and acute psychosis”
WHO = World Health Organization.Pietrobon D. Neuroscientist. 2005;11:373–386; Stovner LJ et al. Cephalalgia. 2007;27:193–210.Linde M. Acta Neurol Scand. 2006;114:71–83; ICHD. Cephalalgia. 2004;24 (Suppl 1):9–160.Hu XH. et al Arch Intern Med. 1999;159:813–818.
A Sophisticated Array of Effective Treatment Options
PREVENTATIVE: ABORTIVE:
• Dietary modification• Trigger identification & avoidance• Exercise• Sleep hygiene / improvement• Biofeedback• Stress management & relaxation• Acupuncture• Osteopathic manipulation• Nutraceuticals• Herbal preparations• Pharmaceuticals• Onabotulinum Toxin A injections• Peripheral nerve blockade / stimulation
• Biofeedback and progressive relaxation• Sleep induction• Acupuncture• Osteopathic manipulation• Biofeedback• Nutraceuticals• Herbal preparations• Occipital nerve blocks• Trigeminal nerve blocks• Neurostimulation• Triptans• Ergots & DHE• NSAID’s• Antiemetics• IV infusions
Migraine Without Aura:International Headache Society Criteria
A. At least 5 attacks fulfilling criteria B through D
B. Headache attacks: 4 to 72 hours
C. Headache with at least 2 of the following characteristics1. Unilateral2. Pulsating3. Moderate or severe pain intensity4. Aggravation by or causing avoidance of routine physical activity
D. During headache at least 1 of the following:1. Nausea and/or vomiting2. Photophobia and phonophobia
E. Not attributed to another disorder
Headache Classification Subcommittee of the International Headache Society. Cephalalgia. 2004;24 (suppl 1):1–160.
Migraine With Aura:International Headache Society CriteriaA. At least 2 attacks fulfilling criteria B through D
B. Aura consisting of at least 1 of the following, but no motor weakness1. Fully reversible visual symptoms*2. Fully reversible sensory symptoms*3. Fully reversible dysphasic speech disturbance
C. At least 2 of the following1. Homonymous visual symptoms and/or unilateral sensory symptoms2. ≥1 aura symptom over ≥5 minutes, and/or different aura symptoms in
succession over ≥5 minutes3. Each symptom: ≥5 and ≤60 minutes
D. Headache fulfilling criteria B through D for migraine without aura begins during the aura or follows aura within 60 minutes
E. Not attributed to another disorder
* Including positive features and/or negative features.Headache Classification Subcommittee of the International Headache Society. Cephalalgia. 2004; 24 (suppl 1):1–160.

The Natural Course of a Typical Migraine Attack
Adapted with permission from Linde M. Acta Neurol Scand. 2006;114:71–83.
Premonitory phase
Headachephase
Resolution Postdrome
Headache
Time
Au
ra
12
Theoretical Model of a Migraine Cycle
Adapted from Expert Review Neurother. 4(3) 391–430 (2004) with permission of Future Drugs Ltd.
Initiatingmechanisms
Perpetuatingmechanisms
Resolvingmechanisms
Trigger
Low threshold

13
Migraine Triggers and Precipitants
0
25
50
75
100
Stress
Hormon
es
Not eat
ing
Wea
ther
Sleep
dis
turb
ance
Perfu
me
or o
dor
Neck
pain
Light(s
)
Alcohol
Smoke
Sleep
ing
late
Heat
Food
Exerc
ise
Sexua
l act
ivity
Fre
qu
enc
y (%
)
Adapted with permission from Kelman L. Cephalalgia. 2007; 27:394–402.
N=1,207 patients with migraine 75.9% reported triggers
– 40.4% infrequently– 26.7% frequently– 8.8% very frequently
14
Migraine Pathophysiology:Proposed Mechanisms
TVS = trigeminovascular system.Adapted with permission from Pietrobon D. Neuroscientist. 2005;11:373–386.
Aura CSD
Cortical neuronal hyperexcitability
Activation and peripheral sensitization of TGVS
Neurogenicinflammation
Centralsensitization
HEADACHE
?
+
+
Genetic predisposition
Migraine initiation
Pain generation/
perpetuation
Abnormal brainstem function

15
Low threshold to abnormal cortical activity
TGVS = trigeminovascular system.
Pietrobon D, Striessnig J. Nat Rev Neurosci. 2003;4:386–398; Pietrobon D. Neuroscientist. 2005;11:373–386.
The “vascular theory” not supported by experimental evidence: → migraine does not start in the blood vessels
Cortical Spreading Depression (?)
The Primary Cause of the Migraine Headache Lies in the Brain
Cortical neuronal hyperexcitability and/orbrainstem dysfunction
Activation & sensitization of the TGVS
Prolonged headache pain of migraine
Genetic predisposition in some patients
Trigger
16
Dura
Migraine Pathophysiology: Central Role of the Trigeminovascular System
Trigeminal nerves
TNC
CSD = cortical spreading depression; TNC = trigeminal nucleus caudalis.
Pietrobon D et al. Nat Rev Neuro. 2003;4:386–398.
PAIN
CSD
TGVS activated

17
Parasympathetic Contribution to Migraine Pathophysiology
Adapted with permission from Goadsby PJ et al. N Engl J Med. 2002;346:257–270.Pietrobon D et al. Nat Rev Neuro. 2003;4:386–398.
18
FHM: a rare inherited form of migraine
Genetically heterogenous autosomal dominant
Genetic Predisposition:Familial Hemiplegic Migraine
FHM = familial hemiplegic migraine. 1. Sanchez del-Rio M et al. Curr Opin Neurol. 2006;19:294–298. 2. Pietrobon D. Neurotherapeutics. 2007;4:274–284.
Gene Protein Consequence
FHM-1 CACNA1A P/Q Ca2+
channels↑ presynaptic Ca2+
FHM-2 ATP1A2 Na+/K+-ATPase
↓ K+ and glutamate clearance
FHM-3 SCN1A Na+
channelPersistent Na+ influx

19
Familial Hemiplegic Migraine:Functional Implications of Gene Mutations
Adapted with permission from Sanchez del-Rio M et al. Curr Opin Neurol. 2006;19:294–298.
FHM-1CACNA1A gene
Cav2.1 Ca2+
Gain of function
FHM-2ATP1A2 gene
α2-subunitNa+/K+ ATPase pump
Loss of function
FHM-3SCN1A gene
Nav1.1Sodium channel
Gain of function
↑Glu/↑K+
CSD
Synapticmetabolism
(including glucose uptake)
20
Cortical Neuronal Hyperexcitability:Multiple Mechanisms
Enhanced release of excitatory neurotransmitters– For example, elevated plasma glutamate concentration
in patients with migraine– Identified genetic mutations in FHM
Reduced intracortical inhibition
Low brain Mg2+
Altered brain energy metabolism
NMDA = N-methyl-D-aspartate.Pietrobon D. et al. Nat Rev Neurosci. 2003;4:386–398.

21
Initiating Mechanisms of Headache Pain: Cortical Spreading Depression
Wave of intense cortical neuron activity– ↑ rCBF
Followed by neuronal suppression – ↓ rCBF– Often coincides with
headache onset
Velocity: 2–3 mm/min
Underlies visual aura
Occurs in clinically silent areas of the cortex?– Migraine without aura
rCBF = regional cerebral blood flow.
Adapted with permission from Hadjikhani N, Sanchez del-Rio M, et al. Mechanisms of migraine aura revealed by functional MRI in human visual cortex. Proc Natl Acad Sci U S A. 2001;98:4687-4692. Copyright 2001 National Academy of Sciences, U.S.A.
Pietrobon D. Neuroscientist. 2005;11:373–386; Goadsby PJ et al. N Engl J Med. 2002;346:257–270.
Time(s)
Blood oxygenation1 min
Occipital cortex
22
Initiating Mechanisms of Migraine: Brainstem Dysfunction
Dysfunction in areas involved in central control of nociception– PAG
Induces migraine?– Brainstem generator
Facilitates activation and sensitization of TNC neurons?– Decreased descending
inhibition during a migraine attack
PAG = periaqueductal gray regionAdapted with permission from Pietrobon D. Nat Rev Neurosci. 2003;4:386–398.
PAG
TGVS activation
HEADACHE
Substance P

23
Activation of the Trigeminovascular System and Pain Generation
Adapted with permission from Iadecola C. Nat Med. 2002;8:110–112.Bolay H. et al. Nat Med. 2002;8:136–142.
24
Activation of the Trigeminovascular System: Physiologic ImpactMeningealevents• Inflammation• Peripheral sensitization
Vasodilation of cerebral vessels
Adapted with permission from Durham PL. N Engl J Med. 2004;350:1073–1075.
Brainstemevents• Pain signal to CNS
• Central sensitization
• Allodynia

25
CGRP and substance P activate mast cells
Mast cell degranulation– Histamine– NGF– Serotonin– Proinflammatory
cytokines TNF, IL-1, IL-6
Neurogenic InflammationMeninges
Longoni M, Ferrarese C. 2006;27 (Suppl 2):S107–110; Pietrobon D. Neuroscientist. 2005;11:373–386.Durham PL N Engl J Med. 2004;350:1073–1075. Edvinsson L, Uddman R. Brain Res Rev. 2005;48:438–456.Theoharides TC. et al. Brain Res Rev. 2005;49:65–76; Goadsby PJ. Trends Mol Med. 2007;13:39–44.Levy D. et al. Headache. 2006;46 (suppl 1):S13–S18; Levy D. et al. Pain. 2007; April 23; [Epub ahead of print].
26
Vasodilation of Cerebral Vessels
NO
Adapted with permission from Durham PL. N Engl J Med. 2004;350:1073–1075.
27
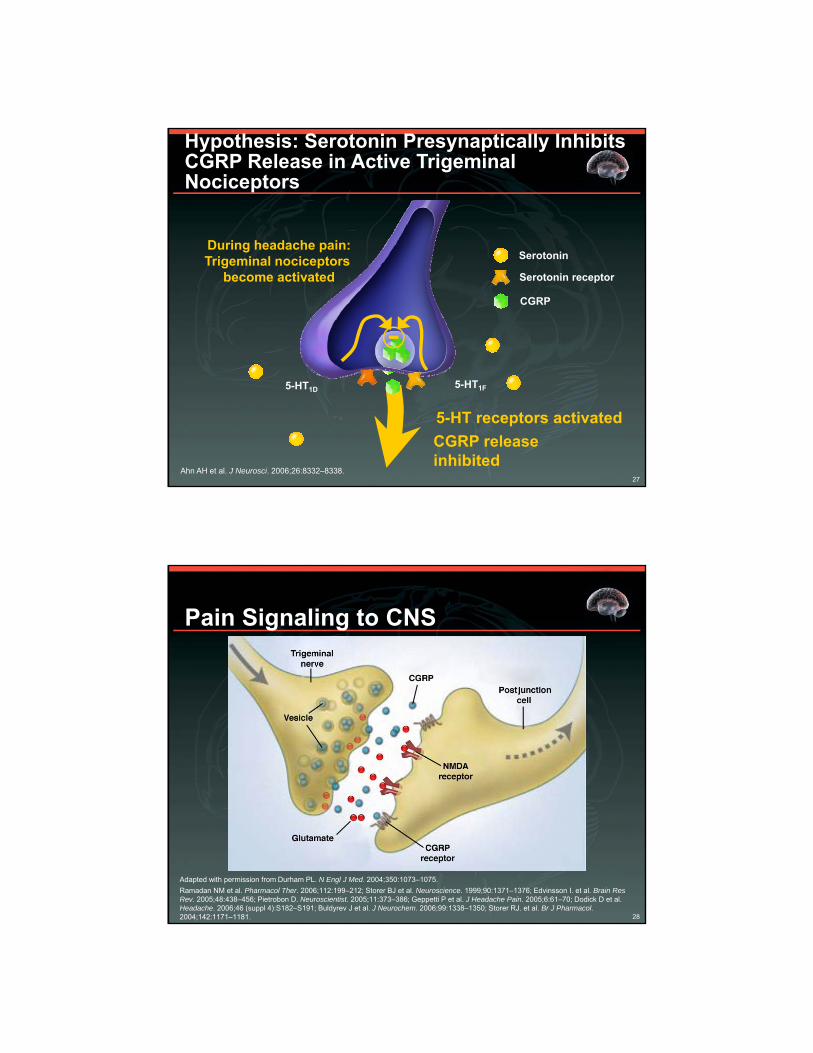
5-HT receptors activated
CGRP releaseinhibited
During headache pain:Trigeminal nociceptors
become activated
Hypothesis: Serotonin Presynaptically Inhibits CGRP Release in Active Trigeminal Nociceptors
Serotonin
5-HT1D 5-HT1F
CGRP
Ahn AH et al. J Neurosci. 2006;26:8332–8338.
Serotonin receptor
28
Pain Signaling to CNS
Adapted with permission from Durham PL. N Engl J Med. 2004;350:1073–1075.
Ramadan NM et al. Pharmacol Ther. 2006;112:199–212; Storer BJ et al. Neuroscience. 1999;90:1371–1376; Edvinsson I. et al. Brain Res Rev. 2005;48:438–456; Pietrobon D. Neuroscientist. 2005;11:373–386; Geppetti P et al. J Headache Pain. 2005;6:61–70; Dodick D et al. Headache. 2006;46 (suppl 4):S182–S191; Buldyrev J et al. J Neurochem. 2006;99:1338–1350; Storer RJ. et al. Br J Pharmacol. 2004;142:1171–1181.
29
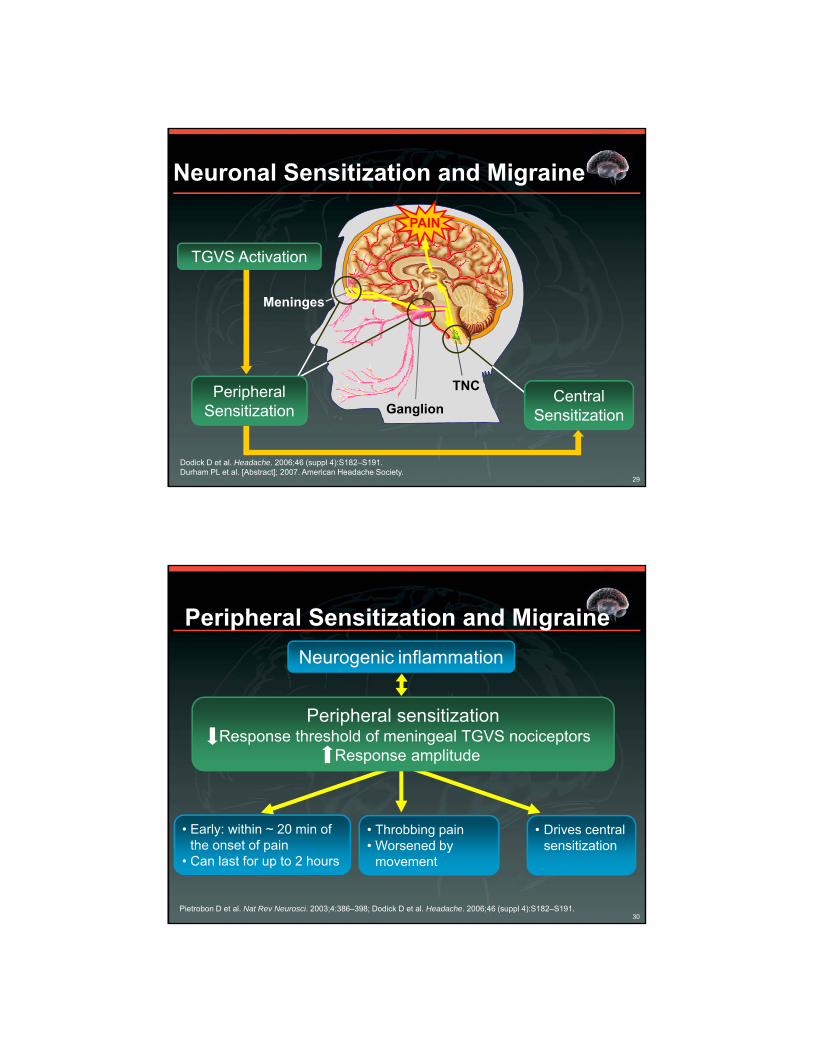
TNC
PAIN
Neuronal Sensitization and Migraine
TGVS Activation
Dodick D et al. Headache. 2006;46 (suppl 4):S182–S191.Durham PL et al. [Abstract]; 2007. American Headache Society.
Central Sensitization
Peripheral Sensitization
Meninges
Ganglion
30
Peripheral sensitizationResponse threshold of meningeal TGVS nociceptors
Response amplitude
Peripheral Sensitization and Migraine
Neurogenic inflammation
• Early: within ~ 20 min of the onset of pain
• Can last for up to 2 hours
• Throbbing pain • Worsened by
movement
• Drives central sensitization
Pietrobon D et al. Nat Rev Neurosci. 2003;4:386–398; Dodick D et al. Headache. 2006;46 (suppl 4):S182–S191.

31
Central sensitizationNeuronal hyperexcitability in the TNC
Possibly due to: CGRP Ca2+ glutamate (NMDA)
Central Sensitization and Migraine
Peripheral sensitizationincoming stimulation from the
trigeminal nerve
•Later: within ~60 min of the onset of pain
•Can last up to 10 hours
•Allodynia•Prolongation of the attack
•Drives sensitization of higher-order neurons
Dodick D, Silberstein S. Headache. 2006;46(suppl 4):S182–S191.
32
Measurable Neuropeptide Levels in the External Jugular Vein During Migraine Attacks
± 0 = no change from before headache.↑ = significant increase in neuropeptide level.Adapted with permission from Edvinsson L, Uddman R. Brain Res Rev. 2005;48:438–456.
VIP Substance P CGRP
Migraine without aura ± 0 ± 0 ↑
Migraine with aura ± 0 ± 0 ↑
Trigeminal neuralgia ± 0 ± 0 ↑
Cluster headache ↑ ± 0 ↑
Chronic paroxysmal headache
↑ ± 0 ↑

33
Activation of the Trigeminovascular System:Primary Neuromediators in Migraine
Origin of ReleaseSuggested
Meningeal ActionsBrain-stem
TGVSNerves
ParasympNerves Vasodilation
Mast Cell Degranulation
Plasma Extravasation
Neuro-peptides
CGRP Substance P
VIP Small Molecules
NO Glutamate
CGRP = calcitonin gene–related peptide; VIP = vasoactive intestinal peptide.Pietrobon D. Neuroscientist. 2005;11:373–386; Edvinsson L. et al. Brain Res Rev. 2005;48:438–456;Ramadan NM et al. Pharmacol Ther. 2006;112:199–212; Storer RJ et al. Neuroscience. 1999;90:1371–1376.Theoharides TC et al. Brain Res Rev. 2005;49:65–76; Goadsby PJ. Trends Mol Med. 2007;13:39–44.Storer RJ et al. Br J Pharmacol. 2004;142:1171–1181.
34
CGRP: Central Role in Migraine
Main neuropeptide released by activated TGVS neurons in migraine– Major neuropeptide of the TGVS
Infusion in susceptible individual induces migraine
During migraine: increased in jugular venous blood, cerebrospinal fluid, saliva– Also elevated in blood between attacks
Physiologic actions:– Vasodilation– Meningeal mast cell degranulation– Activation of second-order neurons in the TNC
Goadsby PJ, Edvinsson L. Ann Neurol. 1993;33:48–56.66; Gulbenkian S. et al. Peptides. 2001;22:995–1007.Edvinsson L, Uddman R. Brain Res Rev. 2005;48:438–456; Lassen LH et al. Cephalalgia. 2002;22:54–61.Edvinsson L. Headache. 2006;46:1088–1094; Sarchielli P. et al. Neurology. 2001;57:132–134.Bellamy JL. et al. Headache. 2006;46:24–33; Ashina M. et al. Pain. 2000;86:133–138.Pietrobon D. Neuroscientist. 2005;11:373–386; Theoharides TC. et al. Brain Res Rev. 2005;49:65–76. Storer RJ. et al. Br J Pharmacol. 2004;142:1171–1181.
35
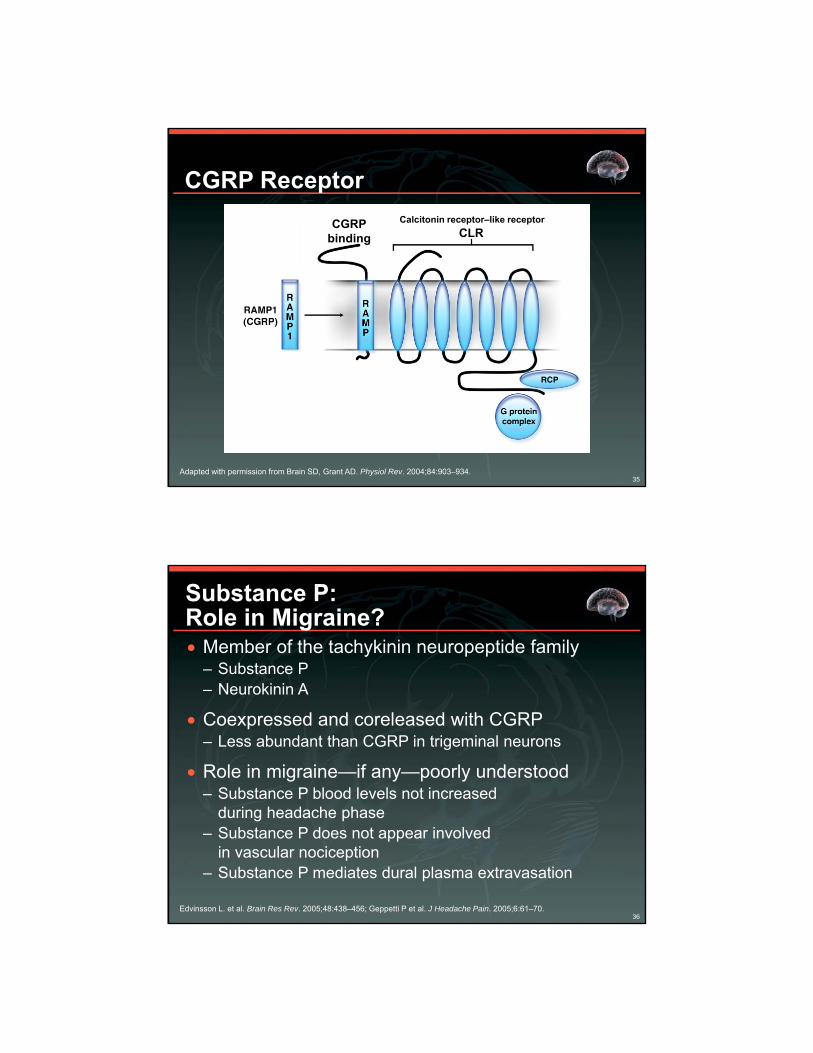
Calcitonin receptor–like receptor
CGRP Receptor
Adapted with permission from Brain SD, Grant AD. Physiol Rev. 2004;84:903–934.
CLRCGRP
binding
36
Substance P:Role in Migraine? Member of the tachykinin neuropeptide family
– Substance P– Neurokinin A
Coexpressed and coreleased with CGRP– Less abundant than CGRP in trigeminal neurons
Role in migraine—if any—poorly understood – Substance P blood levels not increased
during headache phase– Substance P does not appear involved
in vascular nociception– Substance P mediates dural plasma extravasation
Edvinsson L. et al. Brain Res Rev. 2005;48:438–456; Geppetti P et al. J Headache Pain. 2005;6:61–70.

37
Substance P Receptors
Khedkar SA et al. Internet Elec J Molec Design. 2004;3:1–11.
Substance Pbinding
38
Glutamate: Central Role in Migraine Increased brain levels of glutamate may underlie cortical
hyperexcitability in patients with migraine
CSD– Is propagated by glutamate– Can be induced by NMDA and Mg2+ depletion (which releases NMDA
receptors)
Trigeminovascular activation– Glutamate-positive neurons found in all migraine pain-relay centers– All glutamate receptor subtypes expressed on the trigeminal system
Pain signaling to CNS and central sensitization– Involves glutamate
Ramadan NM. CNS Spectr. 2003;8:446–449. Longoni M et al. Neurol Sci. 2006;27 (suppl 2):S107–S110.

39
Nitric Oxide and Migraine Potent vasodilator
NO donors induce migraine in susceptible humans
NOS-containing fibers found around cranial blood vessels– Parasympathetic fibers– Trigeminal sensory fibers
May contribute to vasodilation and activation of the TGVS nociceptive nerve terminals
Role as a neurotransmitter– NOS expressed in trigeminal nerve cell bodies– May be involved in the activation and/or sensitization of TNC neurons
NOS = nitric oxide synthase.Edvinsson L et al. Brain Res Rev. 2005;48:438–456;Ramadan NM et all. Pharmacol Ther. 2006;112:199–212;Pietrobon D. et al. Nat Rev Neurosci. 2003;4:386–398.
40
Neurogenicinflammation
Migraine Pathophysiology:Summary
Cortical neuronal hyperexcitability
Abnormal brainstem function
Activation of TGVSNeuromediator release
(CGRP, glutamate)HEADACHE
+
+
Genetic predisposition
Initiation
Pain generation/perpetuation
TGVS = trigeminovascular system.
Adapted with permission from Pietrobon D. Neuroscientist. 2005;11:373–386.
Centralsensitization
Peripheralsensitization
+
(?)
(?)





























