Embed Size (px)
Citation preview
The Royal College of Midwives Audit of Midwifery Practice
Full Report
The work described in this report was undertaken by
Dr Marianne Mead
Senior Visiting Research Fellow at the University of Hertfordshire
Jane Munro
Quality and Audit Development Advisor
The Royal College of Midwives
Acknowledgements
We would like to thank all the midwives who took the time participate in this audit.
The support of the following people assisted in the design of the audit and review of the findings
Mervi Jokinen, Practice and Standards Development Adviser, Learning Research and Practice Development International Office, The Royal College of Midwives
Frances Day-Stirk Director, Learning Research and Practice Development, International Office, The Royal College of Midwives Sue Macdonald, Education & Research Manager, Learning Research and Practice Development International Office, The Royal College of Midwives
Gillian Smith, Director of The Royal College of Midwives UK Board for Scotland
This report should be cited as:
Royal College Of Midwives (RCM) 2010 The Royal College Of Midwives’ Audit Of
Midwifery Practice London : RCM
Published by the Royal College of Midwives Trust, December 2010
© RCM Trust
December 2010
1
Executive Summary
The Royal College of Midwives (RCM) Campaign for Normal Birth (CNB) has a focussed
role in promoting normal birth and supporting midwifery practice by providing
information to build midwives’ confidence in physiological processes of labour and
minimal intervention. The CNB uses different strategies to reach its aim, all of them
underpinned by safe midwifery practice.
It is known that certain techniques and practices can impact positively or adversely on
women’s experience of labour (RCM 2008)1 and that interventions should not be offered
while labour is progressing normally. However, in an environment of constant change
within maternity care and service delivery, the CNB recognised there was a lack of
contemporary information on the activities that midwives undertook.
In order to develop new material or address practice issues that could have optimum
impact, RCM actioned a snapshot study of midwives activities in antenatal, intranatal and
postnatal care. The original aim had been to audit two practices: fetal surveillance in
labour and directed pushing, to obtain a baseline of contemporary midwifery practice in
these areas. Whilst developing the initial questionnaire, the design evolved and became
an exploration of current practice in relation to national guidelines and the involvement
of other healthcare workers in the maternity team.
Methodology
A UK wide survey of RCM members on the RCM email database, was undertaken during
the period 28th October 2009 to 2nd December 2009. The number of the midwives on the
RCM database with an email address at the time was 13,782. Members were invited to
contribute to a Bristol On-line survey of three questionnaires, one each on ante-, intra-
and postnatal practice.
1 RCM Evidence based guidelines for midwifery-led care in labour (2008) London: RCM http://www.rcm.org.uk/college/policy-practice/guidelines/practice-guidelines/
2
The questionnaires included sections where questions targeted actual care provided to
women and respondents were asked to recall three recent cases to record their practice
as well as the involvement of other members of the maternity team. In other sections
respondents were asked direct questions about what they would consider to be normal
care provision for women designated suitable for midwifery led care. The response rate
to the survey was 15.6% with 856, 686 and 612 responses to the three questionnaires
respectively.
Audit Findings
Though the practice environment reported on covered nearly equally community and
hospital for antenatal and postnatal care, the intrapartum care was, in the main,
provided in hospital. There was a small representation of home birth and caseload
midwifery and surprisingly, some who stated that they had no option to provide
midwifery led care. This would indicate that the models of care midwives practice in are
still traditional and policy changes have not impacted on this.
Profile of respondents
The majority of respondents worked within the NHS and were employed by an NHS
Trust/Hospital in units where rotation between midwifery led care and obstetric led care
was encouraged. Their main areas of current clinical practice were intrapartum care in a
hospital setting and postnatal care in the community.
The midwives responding to the audit reflected the geographic spread of midwives who
are members of the RCM including those in England, Scotland, Wales and Northern
Ireland.
Antenatal care
Approximately half of the antenatal booking visits took place at the GP’s surgery,
demonstrating that midwives are continuing to work within GP practices. A quarter of
bookings took place in midwifery led facilities (e.g. Birth Centre, Sure Start/Children’s
Centres). This indicates that the initial care provided access for women in the
3
community and as most of the midwives mentored student midwives, the students would
also experience working with women in the community.
Information drawn from the responses regarding booking visits demonstrates that
midwives appear to be more focussed on exploring issues around womens’ previous
medical history than on their social history e.g. home conditions, and domestic abuse.
The National Institute for Health and Clinical Excellence (NICE)2 guidelines on antenatal
and postnatal mental health have highlighted the importance of asking questions about
mental health at booking and postnatally. This audit indicates that less than 50% of
midwives use the two NICE (2007) recommended questions for screening. As these
questions are more explorative than direct questions, this may reflect the shape and
style of maternity notes which normally have a ‘tick box’ format that could direct the
interview. It may also have been affected by who was completing the booking history,
their experience and seniority, which was outside the survey objectives.
Overall midwives appeared to undertake observations as recommended by NICE (2008)3
guidelines at booking and throughout pregnancy and the number of appointments
women had antenatally correlated with the NICE recommendations.
On the quality of information provided to first time parents, it appeared that midwives
placed more importance on the antenatal and intrapartum period, and delegated
Maternity Support Workers (MSWs) to deliver postnatal information.
41% of the midwives reported discussing the birth plan once, and 47% several times
during pregnancy. It is encouraging that the birth plan discussion is being prioritised on
more than one occasion. However it is concerning that 12% of respondents reported
that they did not have enough time for this discussion at all, given the widespread
knowledge that having an opportunity to discuss plans for labour and birth and gaining
information for decision making, is very important to women. This appears frequently in
guideline recommendations.
2 NICE (2007) Antenatal and postnatal mental health. London : NICE http://guidance.nice.org.uk/CG45/NICEGuidance
3 NICE (2008) Antenatal care. Routine care for the healthy pregnant woman London : NICE http://guidance.nice.org.uk/CG62/NICEGuidance
4
Place of birth
In reporting the intended place of birth, a home birth was planned for 17% of the women
recalled in this survey, a free standing birth centre/midwifery led unit for 8%, while the
rest had planned a hospital birth (75%). In terms of the actual place of birth, the
majority of women (57%) laboured and gave birth in a consultant unit, followed by
(22%) in an alongside midwifery led unit, 7% in a free standing midwifery led unit , and
an above the national average (14%) gave birth at home. This is a positive finding as
only 3 respondents specifically worked in a homebirth team. This supports practices
including initial labour assessment taking place at home, which is another factor that can
influence the place of birth and reduce intervention. About a fifth (19%) of the women
were assessed at home.
Intrapartum care
Fetal heart monitoring
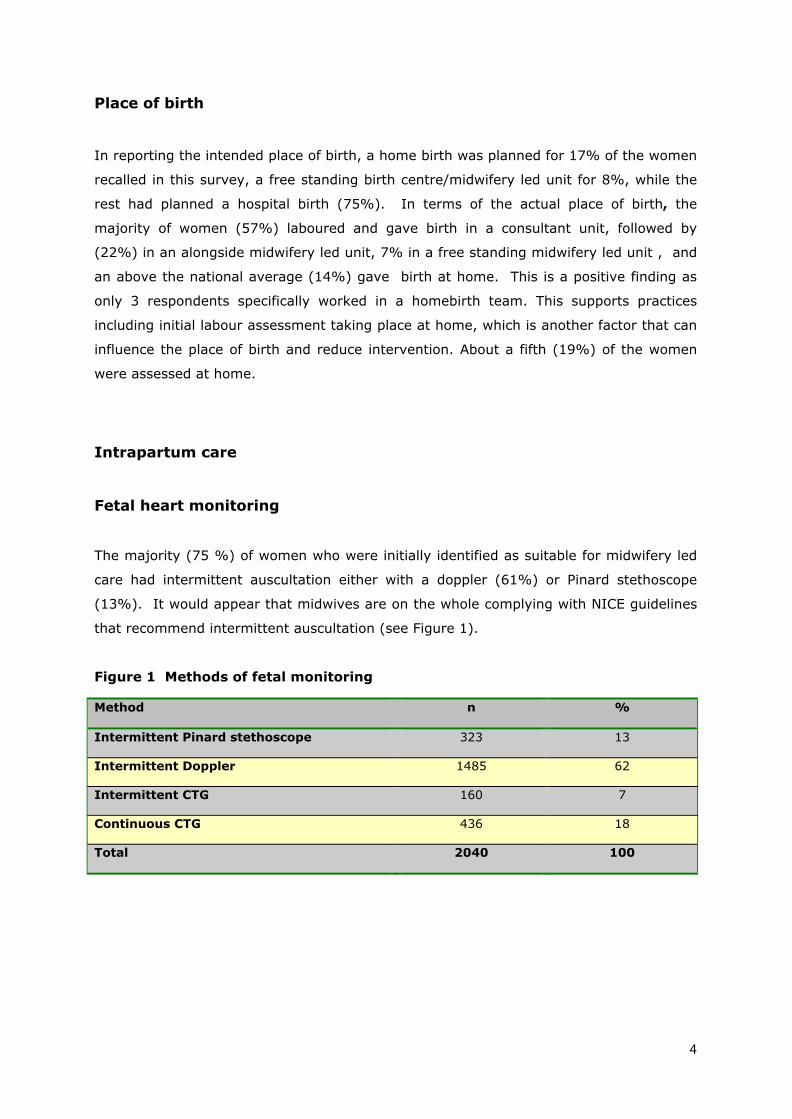
The majority (75 %) of women who were initially identified as suitable for midwifery led
care had intermittent auscultation either with a doppler (61%) or Pinard stethoscope
(13%). It would appear that midwives are on the whole complying with NICE guidelines
that recommend intermittent auscultation (see Figure 1).
Figure 1 Methods of fetal monitoring
Method n %
Intermittent Pinard stethoscope 323 13
Intermittent Doppler 1485 62
Intermittent CTG 160 7
Continuous CTG 436 18
Total 2040 100
5
One to One care
The data on provision of one to one care introduced the role of doula as a person
providing support to some women. This model may become more prominent in the
future, shaped by national projects currently underway, and may impact on the quality of
care by the midwife.
Assessment of progress in labour
When midwives were asked which methods they use to assess the progress of labour
they stated that they gave significant weight to maternal behavioural change, as well as
clinical assessments.
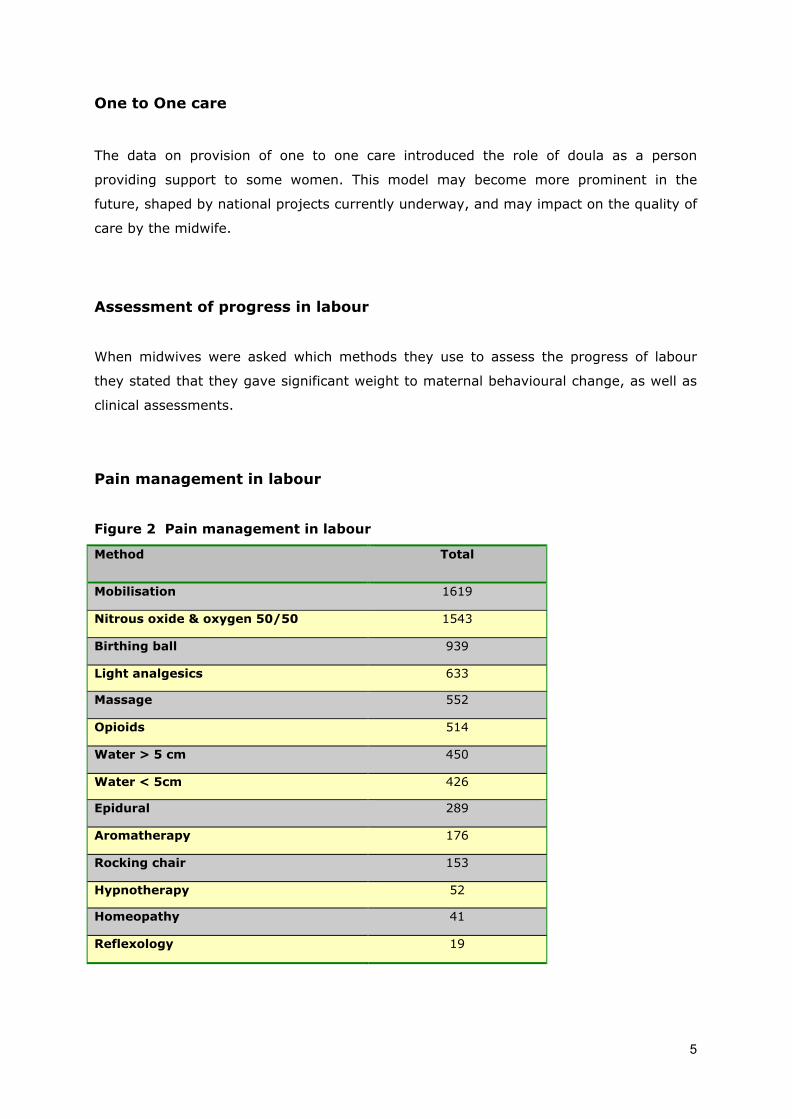
Pain management in labour
Figure 2 Pain management in labour
Method Total
Mobilisation 1619
Nitrous oxide & oxygen 50/50 1543
Birthing ball 939
Light analgesics 633
Massage 552
Opioids 514
Water > 5 cm 450
Water < 5cm 426
Epidural 289
Aromatherapy 176
Rocking chair 153
Hypnotherapy 52
Homeopathy 41
Reflexology 19
6
Of the 14 pain management approaches for labour methods listed (see Figure 2), a
significant number of alternative methods appear to be used by midwives to support
women in labour.
Positions adopted during labour can facilitate or hinder physiological birth, and it was
noted that mobilisation was highest on the list. The high numbers of women using water
and birthing balls show that many labour environments are providing diverse equipment
and midwives appear confident in using these methods.
Birth positions
The semi-recumbent position on the bed was reported as the most common birth
position (34%), followed by the “all fours” or kneeling position (23%). A sizeable
proportion (16%) of this group gave birth in water. In line with the recent survey by the
Care Quality Commission (CQC 2010)4, a surprising number (6%) of spontaneous births
took place in the lithotomy position, a position usually used for instrumental deliveries.
This is an issue that needs further exploration as this practice is not recommended by
NICE for normal labour and births 5. If it is being chosen to encourage more effective
pushing, education is needed on which other positions could provide a better effect.
Management of the third stage
The management of the third stage of labour indicates that the favoured practice is
active management. Taking into consideration that 43% of the women gave birth in
environments conducive to physiological labour, the active management numbers remain
high. This is an area of practice that requires attention as it questions whether this is
appropriate practice within physiological birth and suggests that midwives might lack
confidence in physiological management of the third stage.
4 Care Quality Commission (CQC) (2010) Maternity services Report http://www.cqc.org.uk/aboutcqc/howwedoit/involvingpeoplewhouseservices/patientsurveys/maternityservices.cfm
5 NICE (2007) Intrapartum care. Care of healthy women and their babies during childbirth. NICE: London http://guidance.nice.org.uk/CG55/NICEGuidance
7
Postnatal care
Location of provision of postnatal care
As might be expected, most postnatal care appeared to take place in the home. Only
5% of responses identified the use of any local “postnatal clinics”. The model of care
most midwives worked in did not provide continuity of carer. In the majority of cases,
midwives involved in postnatal care were only involved with these women for that period
only, as opposed to combining postnatal care with ante- and/or intranatal care. As the
frequency of visits appear to have reduced and one third of the women were transferred
out of midwifery care by day ten, this significantly reduces midwives’ opportunity to get
to know women. This could mean that midwives have to concentrate on selected clinical
assessments, as days when visits peaked were around, for example, when they were
taking blood for neonatal bloodspot screening. Also a high level of contact with the
midwife was by telephone only.
Midwives also reported that some of ‘their’ women and babies still had identified
problems on transfer of care. This emphasises the importance of communication with
other health care professionals, and suggests that a staged handover in these more
complex cases may be better practice.
Involvement of students and other members of the maternity care team
As the midwife or student midwife was identified as being responsible for most routine
antenatal observations and ordering of tests during pregnancy, students are exposed to,
and supported in, undertaking antenatal care for women identified as suitable for
midwife-led care. The observations include calculation of Body Mass Index (BMI),
abdominal palpation, measurement of fundal height and fetal heart auscultation.
The majority of clinical observations undertaken in pregnancy and labour were done by
midwives or student midwives. Some practices reported as being undertaken by MSWs
were inappropriate (eg vaginal examination and initial labour assessment). However,
this may have been due to data entry error, as the numbers were very small.
8
In the postnatal period, some care was described as being provided by MSWs. Midwives
were present at most postnatal visits, but MSWs did undertake some postnatal visits
(12%) on their own. This may reflect difficulties with staffing levels impacting on the
amount of postnatal care being provided directly by midwives. This was in contrast to
the experience of student midwives, where only 2% appeared to undertake postnatal
visits on their own. This has major implications for ensuring that students achieve
sufficient experience in all areas of midwifery care and in particular the nuances of
postnatal care. This may have an impact on the students achieving experience,
competence in the whole range of midwifery skills, achieving their required EU directives,
and in ensuring they are confident as midwives.
Limitations
This survey was from a sample targeted from the email address database held by the
RCM. It cannot be assumed that the respondents are representative of the whole
population of midwives or that the cases they “selected” are representative of the
general care provided by midwives to women. Care must also be exercised in the
interpretation of these results as this is self-reported practice rather than observed or
corroborated evidence.
Conclusion
This audit provides an interesting and useful ‘snapshot’ of midwives current practice and
how it reflects national guidelines. Clearly midwives know what is recommended in
national guidelines and the results suggest that their practice is in line with the
guidelines.
The key findings of the audit are
The issues of domestic violence and mental health appear to be still difficult for
midwives to identify.
Some midwives in this audit perceived that there was insufficient time to discuss
birth plans with women at booking or during the antenatal period.
While the majority of women were assessed in a consultant unit, about a fifth of
the women had an initial labour assessment at home.
9
The key practitioner at birth was recorded as the midwife, and a small proportion
as the student midwife.
The semi-recumbent position on the bed, is still the most common position for
birth, but closely followed by the hands knees position.
Midwives appear to give significant weight to maternal behavioural change as a
means of assessing progress in labour, as well as clinical assessments.
44% of full examinations of the newborn were reported as being undertaken by
the midwife.
At the time of this audit there appeared to be very little use of children’s centres
or clinics other than in GP practices.
The role of MSWs at this point appears to be limited, though they are providing
some postnatal support.
Student midwives appear to be undertaking less postnatal visits on their own
than MSWs. This may have a crucial impact on reducing their potential
experience, competence and confidence as future autonomous midwives
Key recommendations
○ That appropriate education and training opportunities are identified and developed
locally to enable midwives to be competent and confident in discussing issues of
domestic abuse and mental health.
○ That more tools and resources be developed by the RCM CNB for midwives to
work with women to encourage ‘off the bed’ positions during labour and birth.
○ That midwives consider critically the role and responsibilities of the student
midwife in the context of gaining appropriate experience, competence and
confidence in the full role of the midwife.
○ That the range of midwifery services within local community settings are
promoted
○ That midwives and others engaged in maternity services use local audit to identify
local practice and practice development.
○ That the potential for new research triggered by these findings, in support of
effective practices related to labour and birth positions, be explored.
10
Introduction
This study was undertaken by the Royal College of Midwives (RCM), under the auspices
of the Campaign for Normal Birth (CNB) to gain a baseline of contemporary midwifery
practice in the UK.
The original aim had been to audit two practices, fetal surveillance in labour and directed
pushing, to obtain a ‘snap shot’ baseline of contemporary midwifery practice in these
areas. It is known that certain techniques and practices can impact positively or
adversely on women’s experience of labour (RCM 2008) and that interventions should
not be offered while labour is progressing normally. However, in an environment of
constant change within maternity care and service delivery, the CNB recognised there
was a lack of contemporary information on the activities that midwives undertook.
Whilst developing the questionnaire the design was expanded to include information on
the student experience and to explore practice in relation to national guidelines and the
involvement of other healthcare workers in the maternity team.
Three areas of practice were surveyed separately: antenatal, intrapartum and postnatal.
Methodology
RCM members on the RCM email database were invited to contribute to the online survey
though a link to three questionnaires on Bristol On-line, one each on antenatal,
intrapartum and postnatal practice. The number of the midwives on the database at the
time was 13,782.
In the parts of the questionnaire dealing with actual care provided for women,
respondents were asked to use 3 recent cases to illustrate their current practice and the
involvement of other members of the maternity team.
The survey was launched on 28th October 2009 with a deadline for completion on 2nd
December 2009. Two email reminders were sent at weekly intervals after the second
week of the launch to encourage a higher response rate. After each reminder, there was
a marked increase in the responses.
The overall response rate to the survey was 15.6% of the number of midwives on the
RCM email data base.
11
The three questionnaires received the following number of responses:
Antenatal - 856 responses
Intrapartum - 686 responses
Postnatal - 612 responses
These numbers could be expected to be used as denominators for all the answers, but
there were a missing number of answers, therefore the total given for each question, is
the denominator for that question. The percentages in the tables have all been rounded
up or down to whole numbers, as appropriate.
This report presents the key findings of the audit.
Findings
Profile of respondents
The majority of respondents worked within the NHS and were employed by an NHS
Trust/Hospital in units where rotation between midwifery led care and obstetric led care
was encouraged.
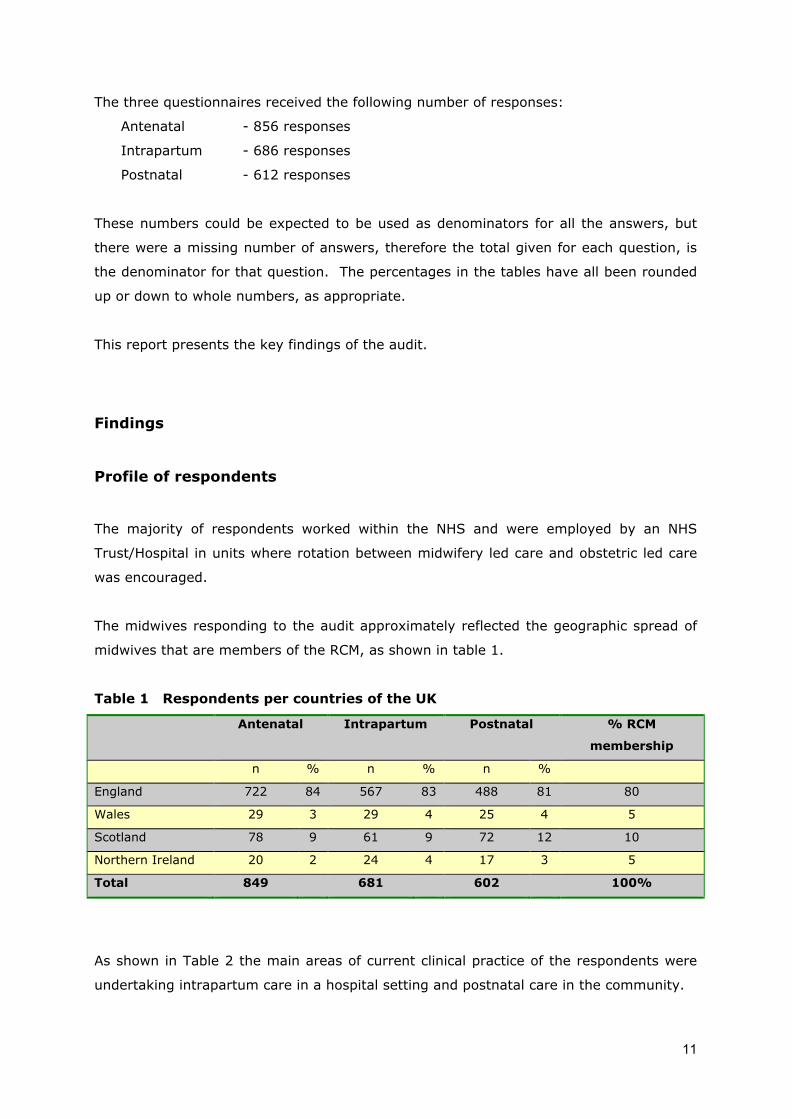
The midwives responding to the audit approximately reflected the geographic spread of
midwives that are members of the RCM, as shown in table 1.
Table 1 Respondents per countries of the UK
Antenatal
Intrapartum Postnatal % RCM
membership
n % n % n %
England 722 84 567 83 488 81 80
Wales 29 3 29 4 25 4 5
Scotland 78 9 61 9 72 12 10
Northern Ireland 20 2 24 4 17 3 5
Total 849 681 602 100%
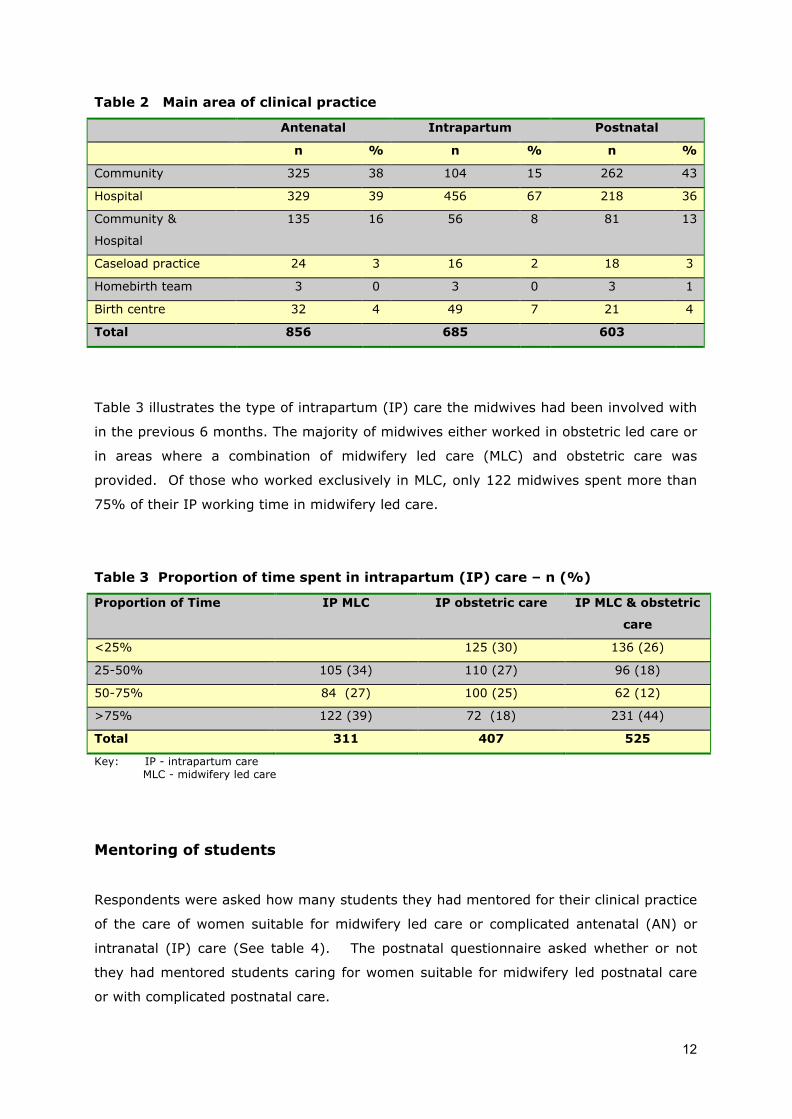
As shown in Table 2 the main areas of current clinical practice of the respondents were
undertaking intrapartum care in a hospital setting and postnatal care in the community.
12
Table 2 Main area of clinical practice
Antenatal Intrapartum Postnatal
n % n % n %
Community 325 38 104 15 262 43
Hospital 329 39 456 67 218 36
Community &
Hospital
135 16 56 8 81 13
Caseload practice 24 3 16 2 18 3
Homebirth team 3 0 3 0 3 1
Birth centre 32 4 49 7 21 4
Total 856 685 603
Table 3 illustrates the type of intrapartum (IP) care the midwives had been involved with
in the previous 6 months. The majority of midwives either worked in obstetric led care or
in areas where a combination of midwifery led care (MLC) and obstetric care was
provided. Of those who worked exclusively in MLC, only 122 midwives spent more than
75% of their IP working time in midwifery led care.
Table 3 Proportion of time spent in intrapartum (IP) care – n (%)
Proportion of Time IP MLC IP obstetric care IP MLC & obstetric
care
<25% 125 (30) 136 (26)
25-50% 105 (34) 110 (27) 96 (18)
50-75% 84 (27) 100 (25) 62 (12)
>75% 122 (39) 72 (18) 231 (44)
Total 311 407 525
Key: IP - intrapartum care MLC - midwifery led care
Mentoring of students
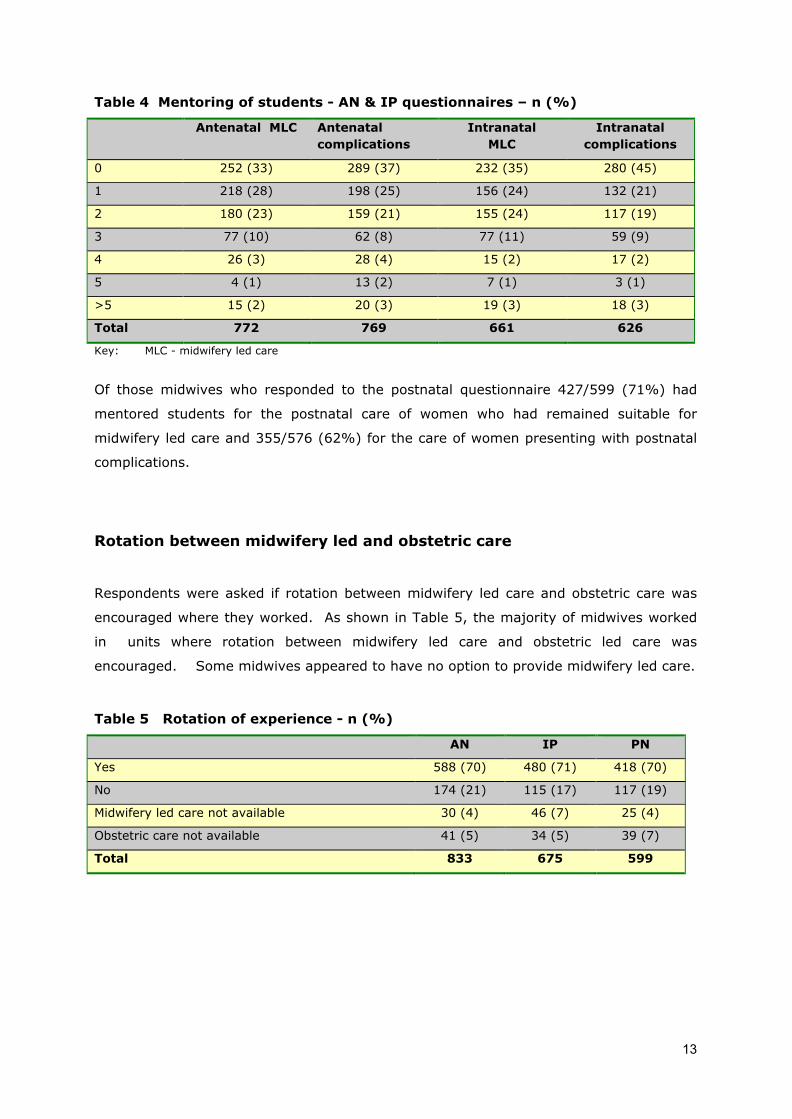
Respondents were asked how many students they had mentored for their clinical practice
of the care of women suitable for midwifery led care or complicated antenatal (AN) or
intranatal (IP) care (See table 4). The postnatal questionnaire asked whether or not
they had mentored students caring for women suitable for midwifery led postnatal care
or with complicated postnatal care.
13
Table 4 Mentoring of students - AN & IP questionnaires – n (%)
Antenatal MLC Antenatal complications
Intranatal MLC
Intranatal complications
0 252 (33) 289 (37) 232 (35) 280 (45)
1 218 (28) 198 (25) 156 (24) 132 (21)
2 180 (23) 159 (21) 155 (24) 117 (19)
3 77 (10) 62 (8) 77 (11) 59 (9)
4 26 (3) 28 (4) 15 (2) 17 (2)
5 4 (1) 13 (2) 7 (1) 3 (1)
>5 15 (2) 20 (3) 19 (3) 18 (3)
Total 772 769 661 626
Key: MLC - midwifery led care
Of those midwives who responded to the postnatal questionnaire 427/599 (71%) had
mentored students for the postnatal care of women who had remained suitable for
midwifery led care and 355/576 (62%) for the care of women presenting with postnatal
complications.
Rotation between midwifery led and obstetric care
Respondents were asked if rotation between midwifery led care and obstetric care was
encouraged where they worked. As shown in Table 5, the majority of midwives worked
in units where rotation between midwifery led care and obstetric led care was
encouraged. Some midwives appeared to have no option to provide midwifery led care.
Table 5 Rotation of experience - n (%)
AN IP PN
Yes 588 (70) 480 (71) 418 (70)
No 174 (21) 115 (17) 117 (19)
Midwifery led care not available 30 (4) 46 (7) 25 (4)
Obstetric care not available 41 (5) 34 (5) 39 (7)
Total 833 675 599
14
Antenatal Care
Place of booking
Respondents were asked to recall three women (designated as suitable for midwifery-led
care) whom they had seen for the initial booking appointment and that they had
provided care for during the antenatal period.
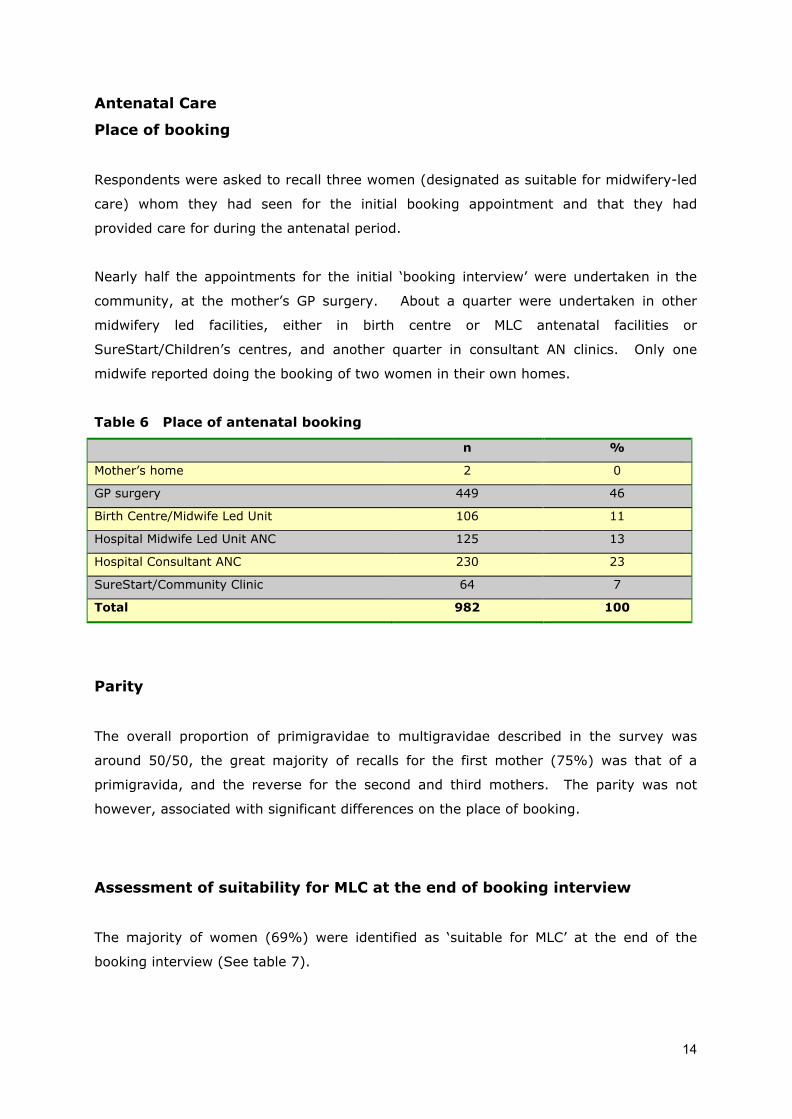
Nearly half the appointments for the initial ‘booking interview’ were undertaken in the
community, at the mother’s GP surgery. About a quarter were undertaken in other
midwifery led facilities, either in birth centre or MLC antenatal facilities or
SureStart/Children’s centres, and another quarter in consultant AN clinics. Only one
midwife reported doing the booking of two women in their own homes.
Table 6 Place of antenatal booking
n %
Mother’s home 2 0
GP surgery 449 46
Birth Centre/Midwife Led Unit 106 11
Hospital Midwife Led Unit ANC 125 13
Hospital Consultant ANC 230 23
SureStart/Community Clinic 64 7
Total 982 100
Parity
The overall proportion of primigravidae to multigravidae described in the survey was
around 50/50, the great majority of recalls for the first mother (75%) was that of a
primigravida, and the reverse for the second and third mothers. The parity was not
however, associated with significant differences on the place of booking.
Assessment of suitability for MLC at the end of booking interview
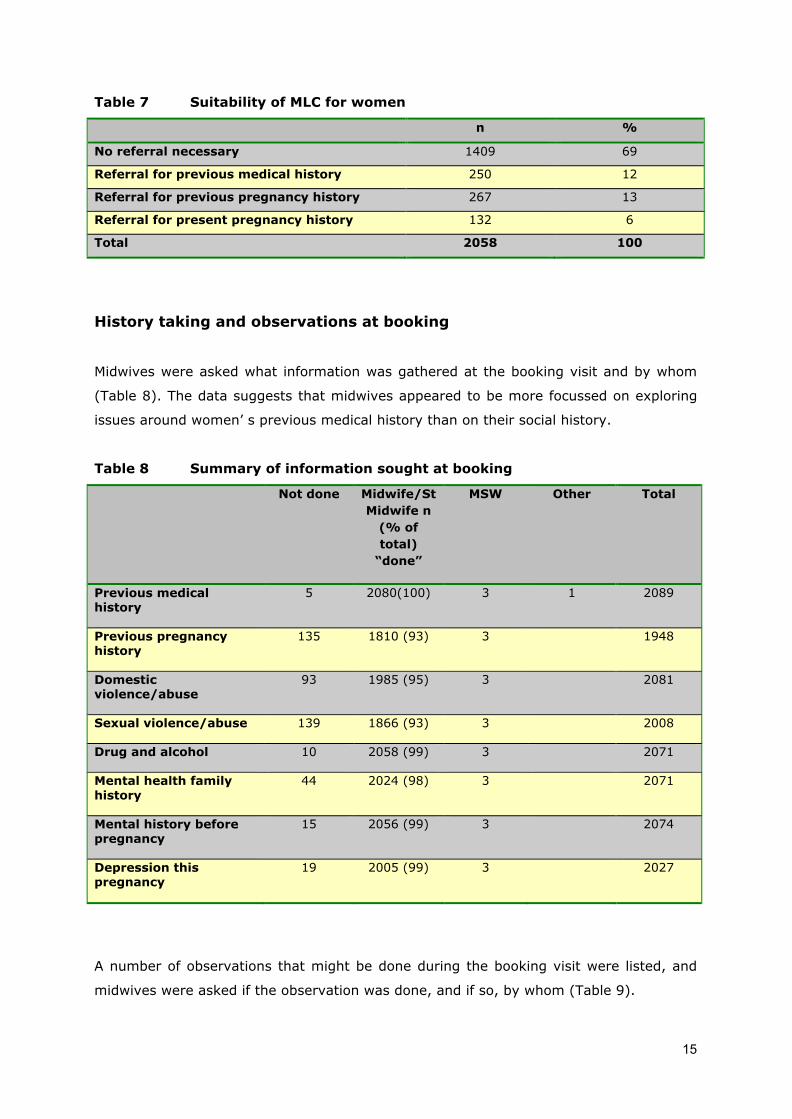
The majority of women (69%) were identified as ‘suitable for MLC’ at the end of the
booking interview (See table 7).
15
Table 7 Suitability of MLC for women
n %
No referral necessary 1409 69
Referral for previous medical history 250 12
Referral for previous pregnancy history 267 13
Referral for present pregnancy history 132 6
Total 2058 100
History taking and observations at booking
Midwives were asked what information was gathered at the booking visit and by whom
(Table 8). The data suggests that midwives appeared to be more focussed on exploring
issues around women’ s previous medical history than on their social history.
Table 8 Summary of information sought at booking
Not done Midwife/St Midwife n
(% of total)
“done”
MSW Other Total
Previous medical history
5 2080(100) 3 1 2089
Previous pregnancy history
135 1810 (93) 3 1948
Domestic violence/abuse
93 1985 (95) 3 2081
Sexual violence/abuse 139 1866 (93) 3 2008
Drug and alcohol 10 2058 (99) 3 2071
Mental health family history
44 2024 (98) 3 2071
Mental history before pregnancy
15 2056 (99) 3 2074
Depression this pregnancy
19 2005 (99) 3 2027
A number of observations that might be done during the booking visit were listed, and
midwives were asked if the observation was done, and if so, by whom (Table 9).
16
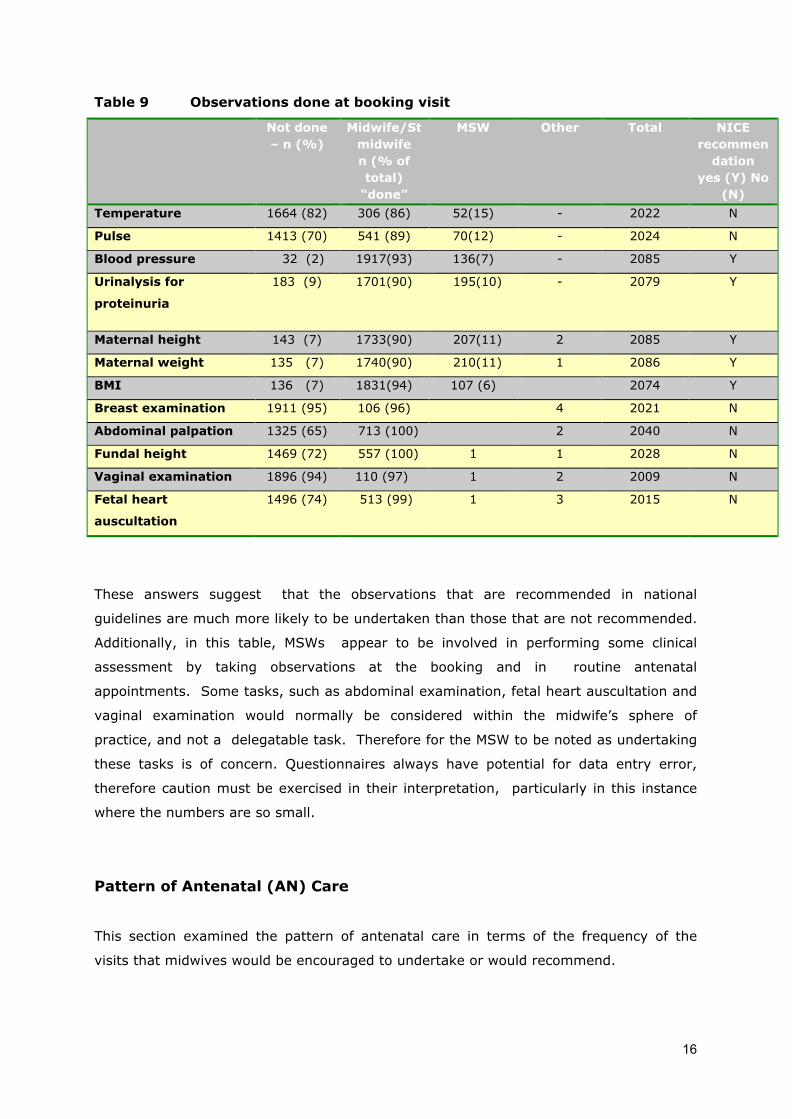
Table 9 Observations done at booking visit
Not done – n (%)
Midwife/St midwife n (% of total)
“done”
MSW Other Total NICE recommen
dation yes (Y) No
(N) Temperature 1664 (82) 306 (86) 52(15) - 2022 N
Pulse 1413 (70) 541 (89) 70(12) - 2024 N
Blood pressure 32 (2) 1917(93) 136(7) - 2085 Y
Urinalysis for
proteinuria
183 (9) 1701(90) 195(10) - 2079 Y
Maternal height 143 (7) 1733(90) 207(11) 2 2085 Y
Maternal weight 135 (7) 1740(90) 210(11) 1 2086 Y
BMI 136 (7) 1831(94) 107 (6) 2074 Y
Breast examination 1911 (95) 106 (96) 4 2021 N
Abdominal palpation 1325 (65) 713 (100) 2 2040 N
Fundal height 1469 (72) 557 (100) 1 1 2028 N
Vaginal examination 1896 (94) 110 (97) 1 2 2009 N
Fetal heart
auscultation
1496 (74) 513 (99) 1 3 2015 N
These answers suggest that the observations that are recommended in national
guidelines are much more likely to be undertaken than those that are not recommended.
Additionally, in this table, MSWs appear to be involved in performing some clinical
assessment by taking observations at the booking and in routine antenatal
appointments. Some tasks, such as abdominal examination, fetal heart auscultation and
vaginal examination would normally be considered within the midwife’s sphere of
practice, and not a delegatable task. Therefore for the MSW to be noted as undertaking
these tasks is of concern. Questionnaires always have potential for data entry error,
therefore caution must be exercised in their interpretation, particularly in this instance
where the numbers are so small.
Pattern of Antenatal (AN) Care
This section examined the pattern of antenatal care in terms of the frequency of the
visits that midwives would be encouraged to undertake or would recommend.
17
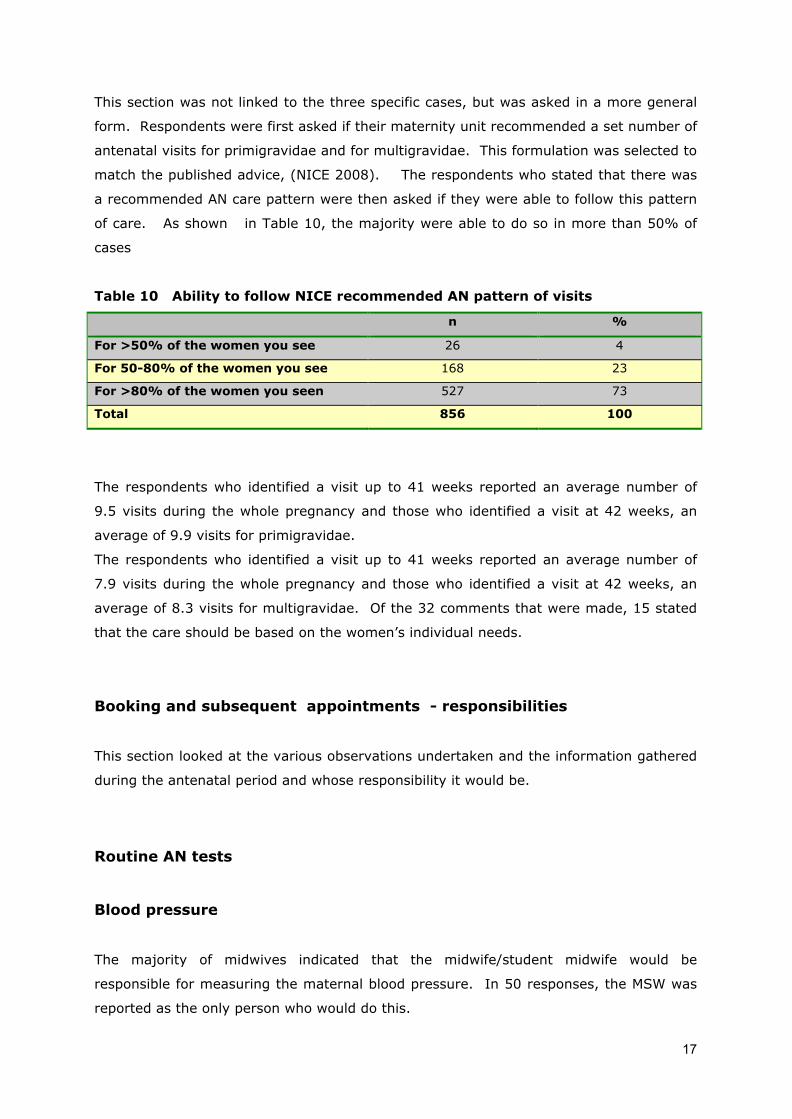
This section was not linked to the three specific cases, but was asked in a more general
form. Respondents were first asked if their maternity unit recommended a set number of
antenatal visits for primigravidae and for multigravidae. This formulation was selected to
match the published advice, (NICE 2008). The respondents who stated that there was
a recommended AN care pattern were then asked if they were able to follow this pattern
of care. As shown in Table 10, the majority were able to do so in more than 50% of
cases
Table 10 Ability to follow NICE recommended AN pattern of visits
n %
For >50% of the women you see 26 4
For 50-80% of the women you see 168 23
For >80% of the women you seen 527 73
Total 856 100
The respondents who identified a visit up to 41 weeks reported an average number of
9.5 visits during the whole pregnancy and those who identified a visit at 42 weeks, an
average of 9.9 visits for primigravidae.
The respondents who identified a visit up to 41 weeks reported an average number of
7.9 visits during the whole pregnancy and those who identified a visit at 42 weeks, an
average of 8.3 visits for multigravidae. Of the 32 comments that were made, 15 stated
that the care should be based on the women’s individual needs.
Booking and subsequent appointments - responsibilities
This section looked at the various observations undertaken and the information gathered
during the antenatal period and whose responsibility it would be.
Routine AN tests
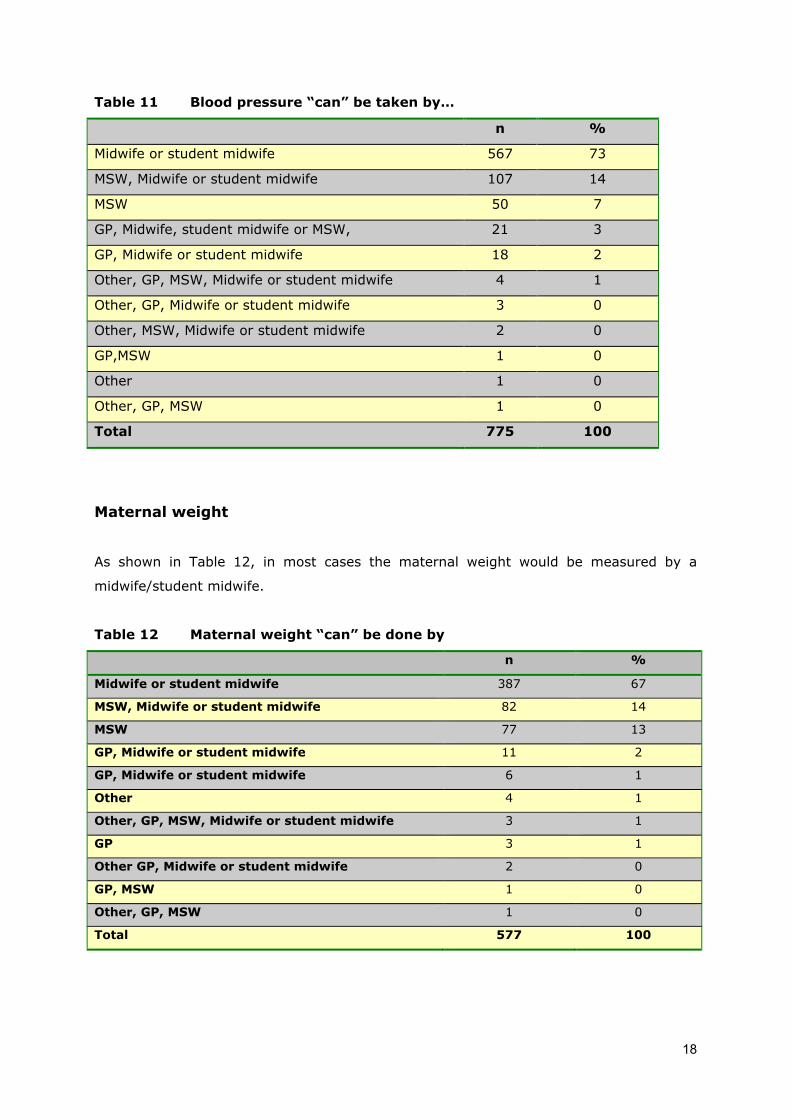
Blood pressure
The majority of midwives indicated that the midwife/student midwife would be
responsible for measuring the maternal blood pressure. In 50 responses, the MSW was
reported as the only person who would do this.
18
Table 11 Blood pressure “can” be taken by…
n %
Midwife or student midwife 567 73
MSW, Midwife or student midwife 107 14
MSW 50 7
GP, Midwife, student midwife or MSW, 21 3
GP, Midwife or student midwife 18 2
Other, GP, MSW, Midwife or student midwife 4 1
Other, GP, Midwife or student midwife 3 0
Other, MSW, Midwife or student midwife 2 0
GP,MSW 1 0
Other 1 0
Other, GP, MSW 1 0
Total 775 100
Maternal weight
As shown in Table 12, in most cases the maternal weight would be measured by a
midwife/student midwife.
Table 12 Maternal weight “can” be done by
n %
Midwife or student midwife 387 67
MSW, Midwife or student midwife 82 14
MSW 77 13
GP, Midwife or student midwife 11 2
GP, Midwife or student midwife 6 1
Other 4 1
Other, GP, MSW, Midwife or student midwife 3 1
GP 3 1
Other GP, Midwife or student midwife 2 0
GP, MSW 1 0
Other, GP, MSW 1 0
Total 577 100
19
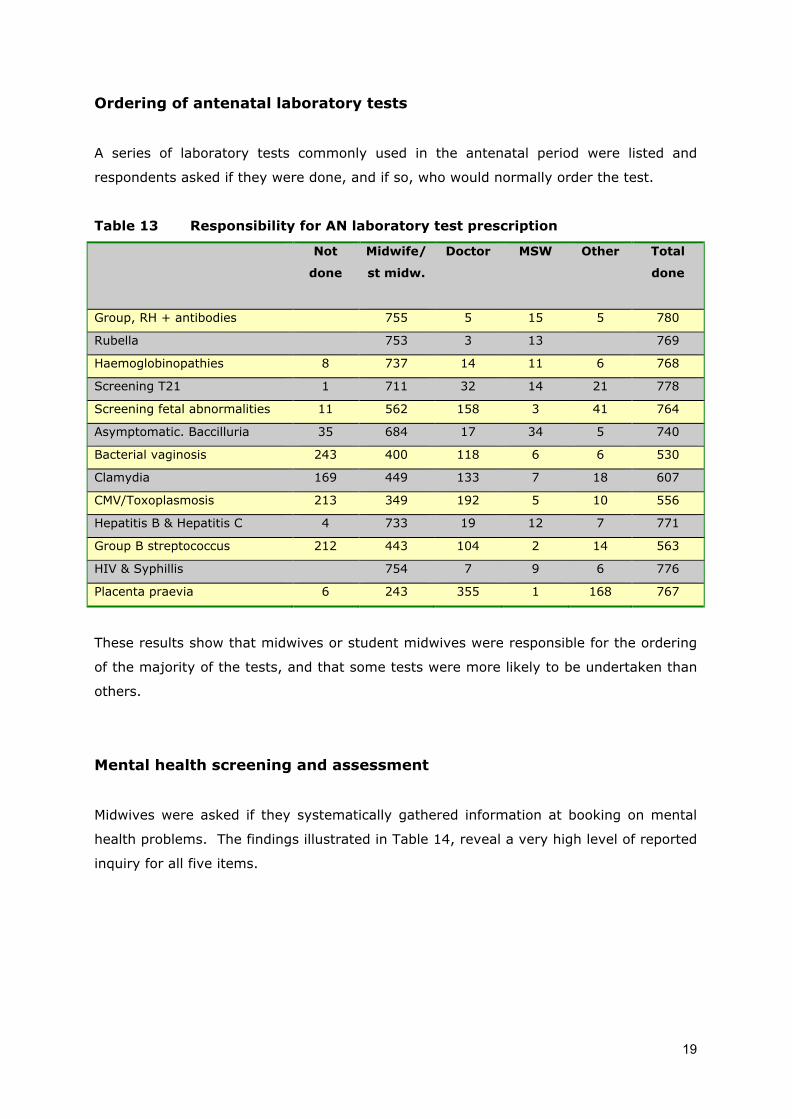
Ordering of antenatal laboratory tests
A series of laboratory tests commonly used in the antenatal period were listed and
respondents asked if they were done, and if so, who would normally order the test.
Table 13 Responsibility for AN laboratory test prescription
Not
done
Midwife/
st midw.
Doctor
MSW Other Total
done
Group, RH + antibodies 755 5 15 5 780
Rubella 753 3 13 769
Haemoglobinopathies 8 737 14 11 6 768
Screening T21 1 711 32 14 21 778
Screening fetal abnormalities 11 562 158 3 41 764
Asymptomatic. Baccilluria 35 684 17 34 5 740
Bacterial vaginosis 243 400 118 6 6 530
Clamydia 169 449 133 7 18 607
CMV/Toxoplasmosis 213 349 192 5 10 556
Hepatitis B & Hepatitis C 4 733 19 12 7 771
Group B streptococcus 212 443 104 2 14 563
HIV & Syphillis 754 7 9 6 776
Placenta praevia 6 243 355 1 168 767
These results show that midwives or student midwives were responsible for the ordering
of the majority of the tests, and that some tests were more likely to be undertaken than
others.
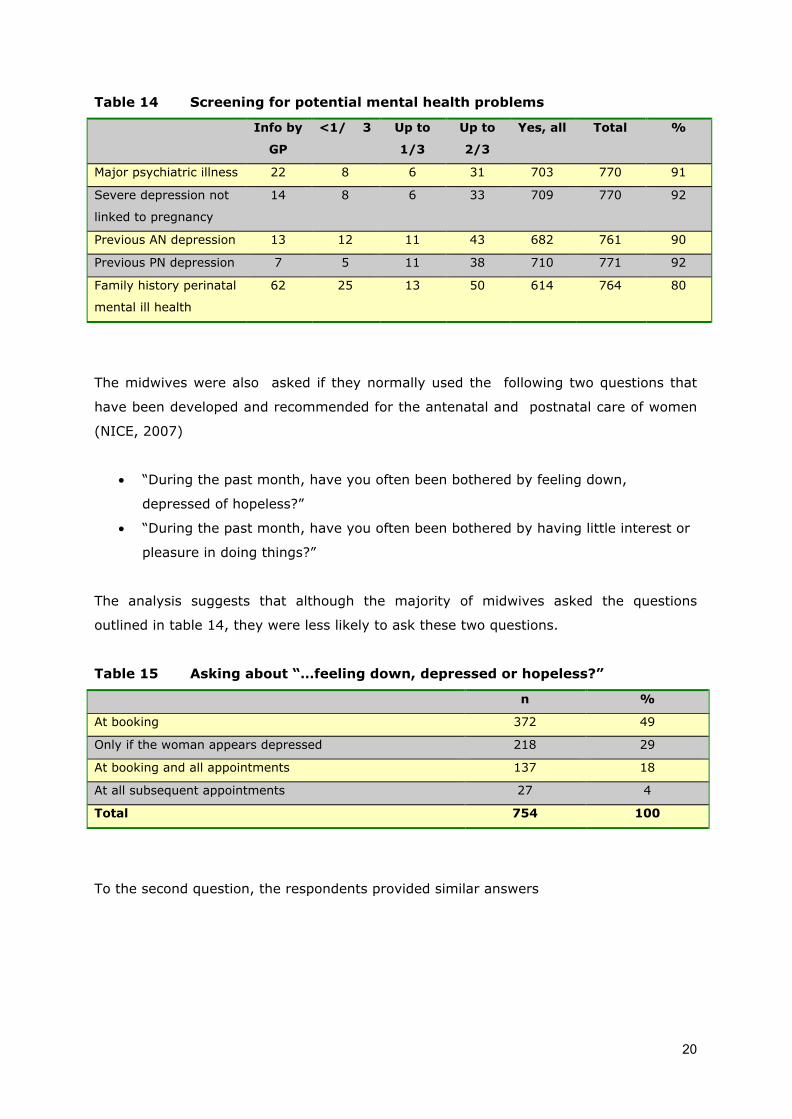
Mental health screening and assessment
Midwives were asked if they systematically gathered information at booking on mental
health problems. The findings illustrated in Table 14, reveal a very high level of reported
inquiry for all five items.
20
Table 14 Screening for potential mental health problems
Info by
GP
<1/ 3 Up to
1/3
Up to
2/3
Yes, all Total %
Major psychiatric illness 22 8 6 31 703 770 91
Severe depression not
linked to pregnancy
14 8 6 33 709 770 92
Previous AN depression 13 12 11 43 682 761 90
Previous PN depression 7 5 11 38 710 771 92
Family history perinatal
mental ill health
62 25 13 50 614 764 80
The midwives were also asked if they normally used the following two questions that
have been developed and recommended for the antenatal and postnatal care of women
(NICE, 2007)
• “During the past month, have you often been bothered by feeling down,
depressed of hopeless?”
• “During the past month, have you often been bothered by having little interest or
pleasure in doing things?”
The analysis suggests that although the majority of midwives asked the questions
outlined in table 14, they were less likely to ask these two questions.
Table 15 Asking about “…feeling down, depressed or hopeless?”
n %
At booking 372 49
Only if the woman appears depressed 218 29
At booking and all appointments 137 18
At all subsequent appointments 27 4
Total 754 100
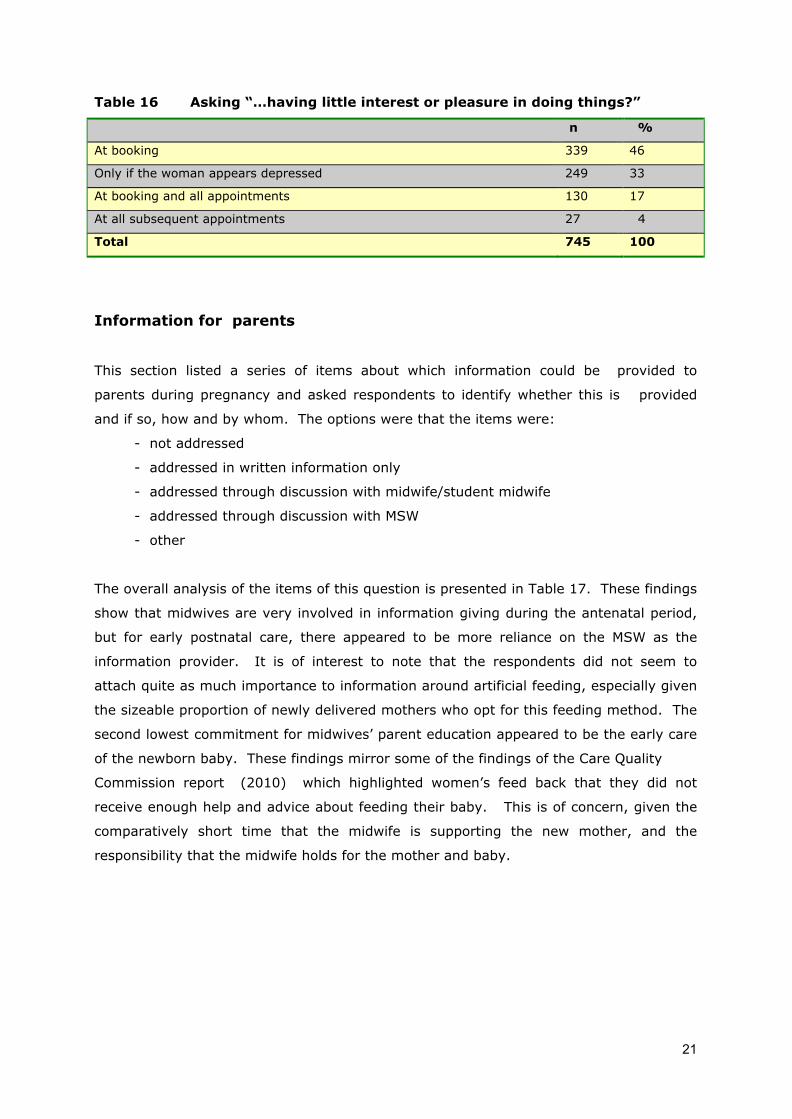
To the second question, the respondents provided similar answers
21
Table 16 Asking “…having little interest or pleasure in doing things?”
n %
At booking 339 46
Only if the woman appears depressed 249 33
At booking and all appointments 130 17
At all subsequent appointments 27 4
Total 745 100
Information for parents
This section listed a series of items about which information could be provided to
parents during pregnancy and asked respondents to identify whether this is provided
and if so, how and by whom. The options were that the items were:
- not addressed
- addressed in written information only
- addressed through discussion with midwife/student midwife
- addressed through discussion with MSW
- other
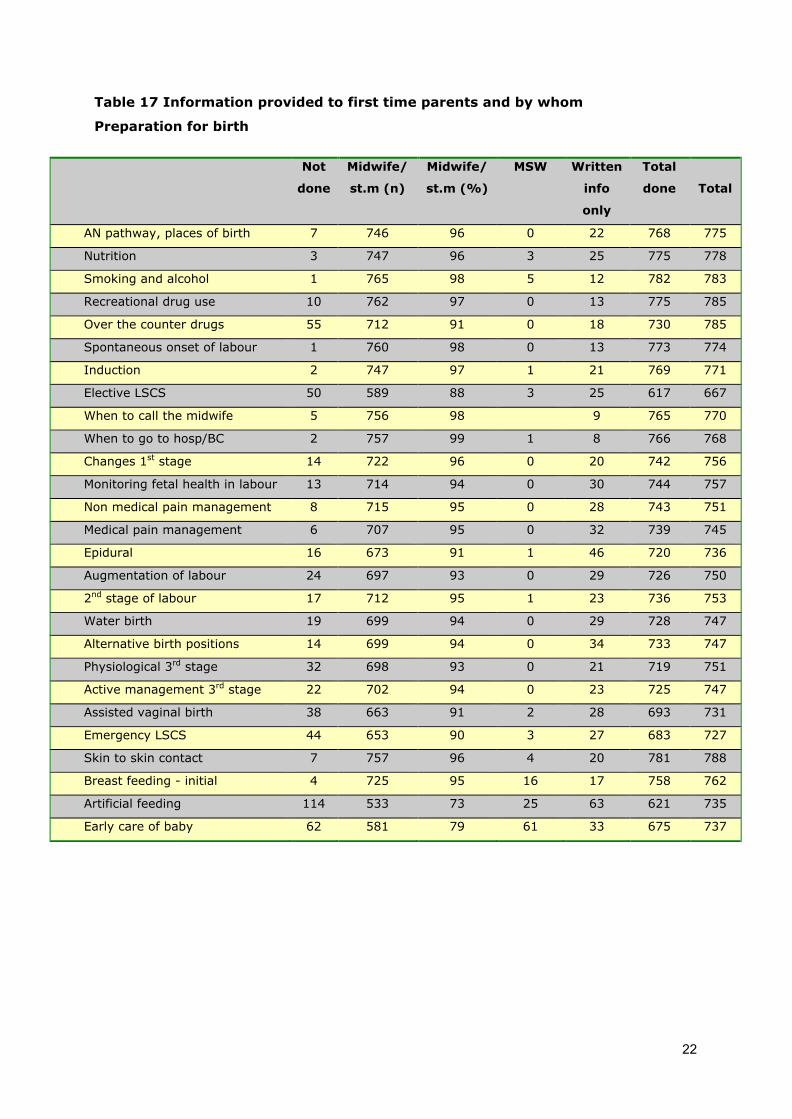
The overall analysis of the items of this question is presented in Table 17. These findings
show that midwives are very involved in information giving during the antenatal period,
but for early postnatal care, there appeared to be more reliance on the MSW as the
information provider. It is of interest to note that the respondents did not seem to
attach quite as much importance to information around artificial feeding, especially given
the sizeable proportion of newly delivered mothers who opt for this feeding method. The
second lowest commitment for midwives’ parent education appeared to be the early care
of the newborn baby. These findings mirror some of the findings of the Care Quality
Commission report (2010) which highlighted women’s feed back that they did not
receive enough help and advice about feeding their baby. This is of concern, given the
comparatively short time that the midwife is supporting the new mother, and the
responsibility that the midwife holds for the mother and baby.
22
Table 17 Information provided to first time parents and by whom
Preparation for birth
Not
done
Midwife/
st.m (n)
Midwife/
st.m (%)
MSW Written
info
only
Total
done
Total
AN pathway, places of birth 7 746 96 0 22 768 775
Nutrition 3 747 96 3 25 775 778
Smoking and alcohol 1 765 98 5 12 782 783
Recreational drug use 10 762 97 0 13 775 785
Over the counter drugs 55 712 91 0 18 730 785
Spontaneous onset of labour 1 760 98 0 13 773 774
Induction 2 747 97 1 21 769 771
Elective LSCS 50 589 88 3 25 617 667
When to call the midwife 5 756 98 9 765 770
When to go to hosp/BC 2 757 99 1 8 766 768
Changes 1st stage 14 722 96 0 20 742 756
Monitoring fetal health in labour 13 714 94 0 30 744 757
Non medical pain management 8 715 95 0 28 743 751
Medical pain management 6 707 95 0 32 739 745
Epidural 16 673 91 1 46 720 736
Augmentation of labour 24 697 93 0 29 726 750
2nd stage of labour 17 712 95 1 23 736 753
Water birth 19 699 94 0 29 728 747
Alternative birth positions 14 699 94 0 34 733 747
Physiological 3rd stage 32 698 93 0 21 719 751
Active management 3rd stage 22 702 94 0 23 725 747
Assisted vaginal birth 38 663 91 2 28 693 731
Emergency LSCS 44 653 90 3 27 683 727
Skin to skin contact 7 757 96 4 20 781 788
Breast feeding - initial 4 725 95 16 17 758 762
Artificial feeding 114 533 73 25 63 621 735
Early care of baby 62 581 79 61 33 675 737
23
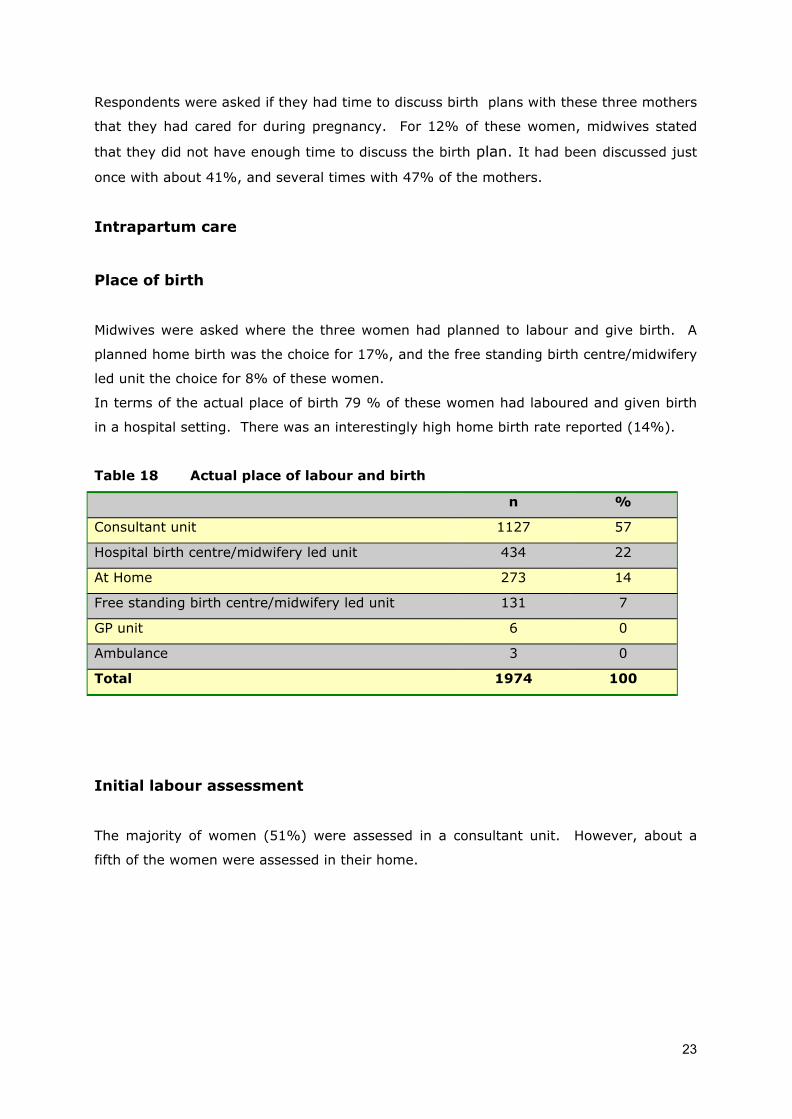
Respondents were asked if they had time to discuss birth plans with these three mothers
that they had cared for during pregnancy. For 12% of these women, midwives stated
that they did not have enough time to discuss the birth plan. It had been discussed just
once with about 41%, and several times with 47% of the mothers.
Intrapartum care
Place of birth
Midwives were asked where the three women had planned to labour and give birth. A
planned home birth was the choice for 17%, and the free standing birth centre/midwifery
led unit the choice for 8% of these women.
In terms of the actual place of birth 79 % of these women had laboured and given birth
in a hospital setting. There was an interestingly high home birth rate reported (14%).
Table 18 Actual place of labour and birth
n %
Consultant unit 1127 57
Hospital birth centre/midwifery led unit 434 22
At Home 273 14
Free standing birth centre/midwifery led unit 131 7
GP unit 6 0
Ambulance 3 0
Total 1974 100
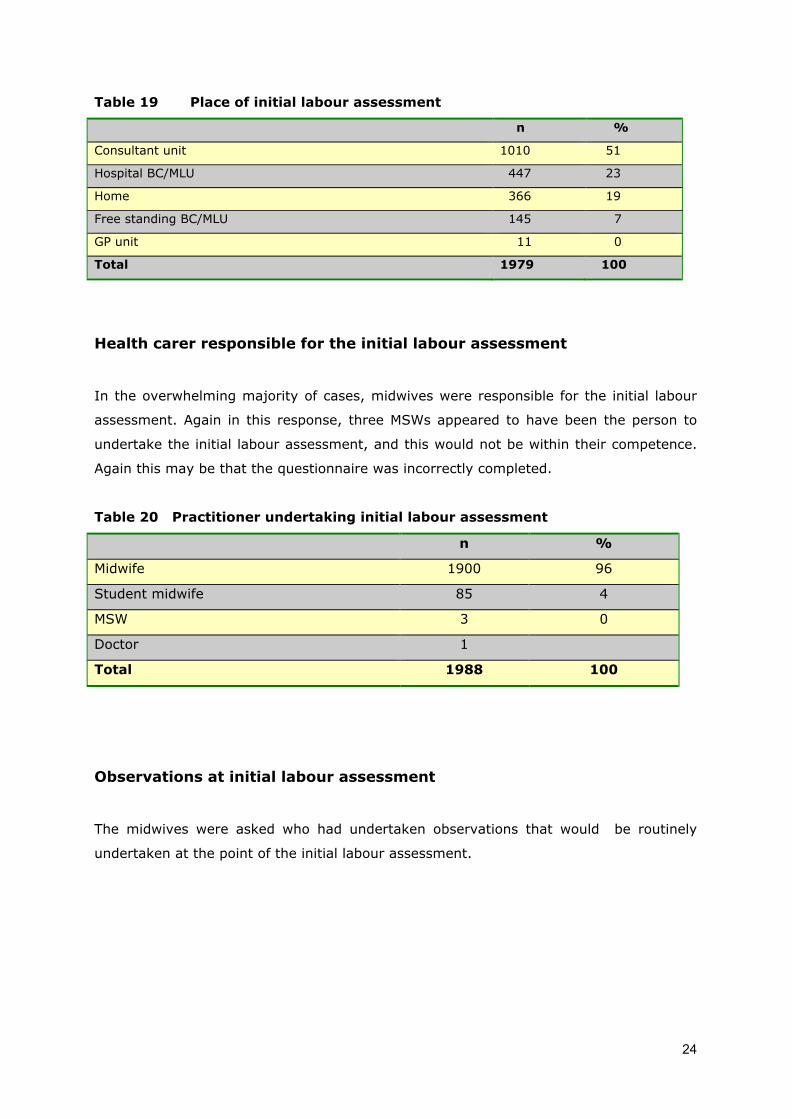
Initial labour assessment
The majority of women (51%) were assessed in a consultant unit. However, about a
fifth of the women were assessed in their home.
24
Table 19 Place of initial labour assessment
n %
Consultant unit 1010 51
Hospital BC/MLU 447 23
Home 366 19
Free standing BC/MLU 145 7
GP unit 11 0
Total 1979 100
Health carer responsible for the initial labour assessment
In the overwhelming majority of cases, midwives were responsible for the initial labour
assessment. Again in this response, three MSWs appeared to have been the person to
undertake the initial labour assessment, and this would not be within their competence.
Again this may be that the questionnaire was incorrectly completed.
Table 20 Practitioner undertaking initial labour assessment
n %
Midwife 1900 96
Student midwife 85 4
MSW 3 0
Doctor 1
Total 1988 100
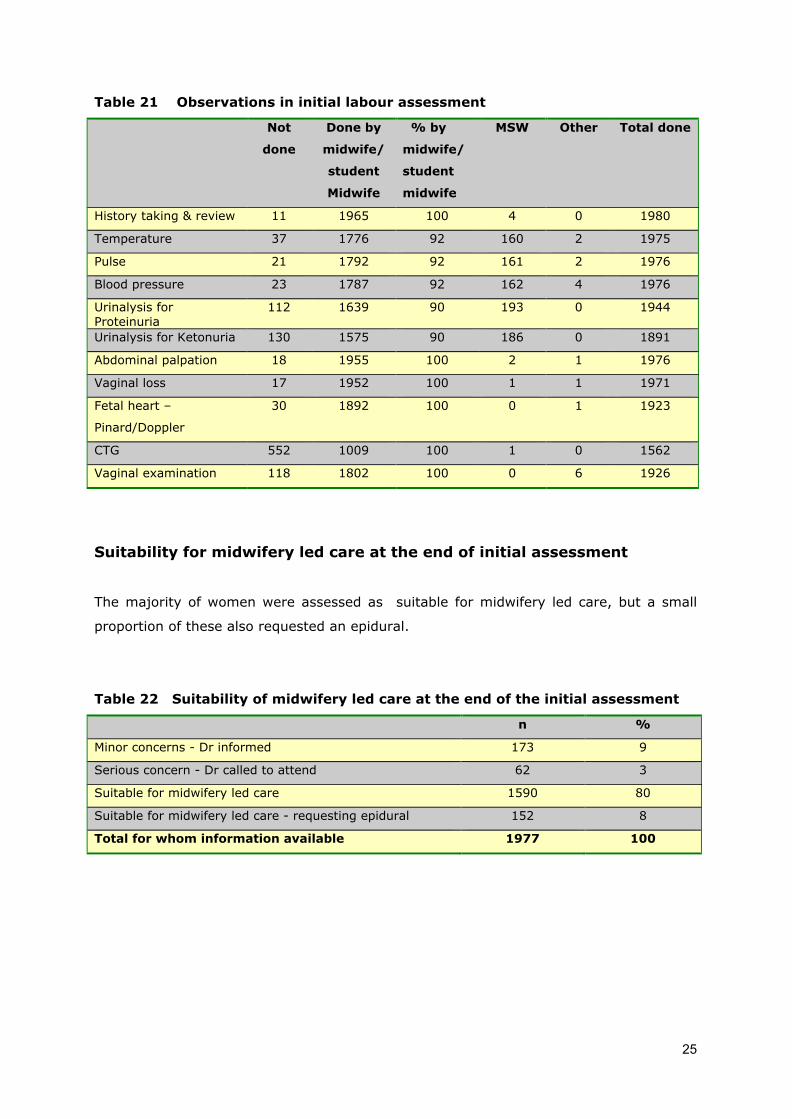
Observations at initial labour assessment
The midwives were asked who had undertaken observations that would be routinely
undertaken at the point of the initial labour assessment.
25
Table 21 Observations in initial labour assessment
Not
done
Done by
midwife/
student
Midwife
% by
midwife/
student
midwife
MSW
Other Total done
History taking & review 11 1965 100 4 0 1980
Temperature 37 1776 92 160 2 1975
Pulse 21 1792 92 161 2 1976
Blood pressure 23 1787 92 162 4 1976
Urinalysis for Proteinuria
112 1639 90 193 0 1944
Urinalysis for Ketonuria 130 1575 90 186 0 1891
Abdominal palpation 18 1955 100 2 1 1976
Vaginal loss 17 1952 100 1 1 1971
Fetal heart –
Pinard/Doppler
30 1892 100 0 1 1923
CTG 552 1009 100 1 0 1562
Vaginal examination 118 1802 100 0 6 1926
Suitability for midwifery led care at the end of initial assessment
The majority of women were assessed as suitable for midwifery led care, but a small
proportion of these also requested an epidural.
Table 22 Suitability of midwifery led care at the end of the initial assessment
n %
Minor concerns - Dr informed 173 9
Serious concern - Dr called to attend 62 3
Suitable for midwifery led care 1590 80
Suitable for midwifery led care - requesting epidural 152 8
Total for whom information available 1977 100
26
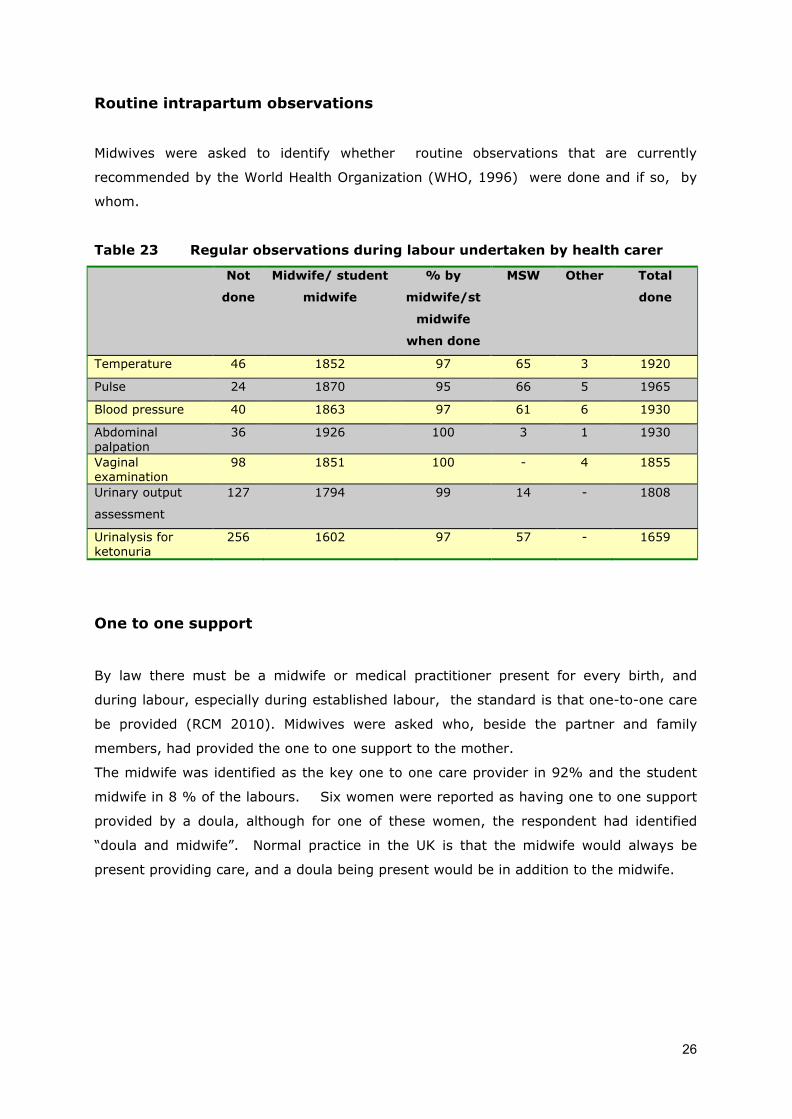
Routine intrapartum observations
Midwives were asked to identify whether routine observations that are currently
recommended by the World Health Organization (WHO, 1996) were done and if so, by
whom.
Table 23 Regular observations during labour undertaken by health carer
Not
done
Midwife/ student
midwife
% by
midwife/st
midwife
when done
MSW Other Total
done
Temperature 46 1852 97 65 3 1920
Pulse 24 1870 95 66 5 1965
Blood pressure 40 1863 97 61 6 1930
Abdominal palpation
36 1926 100 3 1 1930
Vaginal examination
98 1851 100 - 4 1855
Urinary output
assessment
127 1794 99 14 - 1808
Urinalysis for ketonuria
256 1602 97 57 - 1659
One to one support
By law there must be a midwife or medical practitioner present for every birth, and
during labour, especially during established labour, the standard is that one-to-one care
be provided (RCM 2010). Midwives were asked who, beside the partner and family
members, had provided the one to one support to the mother.
The midwife was identified as the key one to one care provider in 92% and the student
midwife in 8 % of the labours. Six women were reported as having one to one support
provided by a doula, although for one of these women, the respondent had identified
“doula and midwife”. Normal practice in the UK is that the midwife would always be
present providing care, and a doula being present would be in addition to the midwife.
27
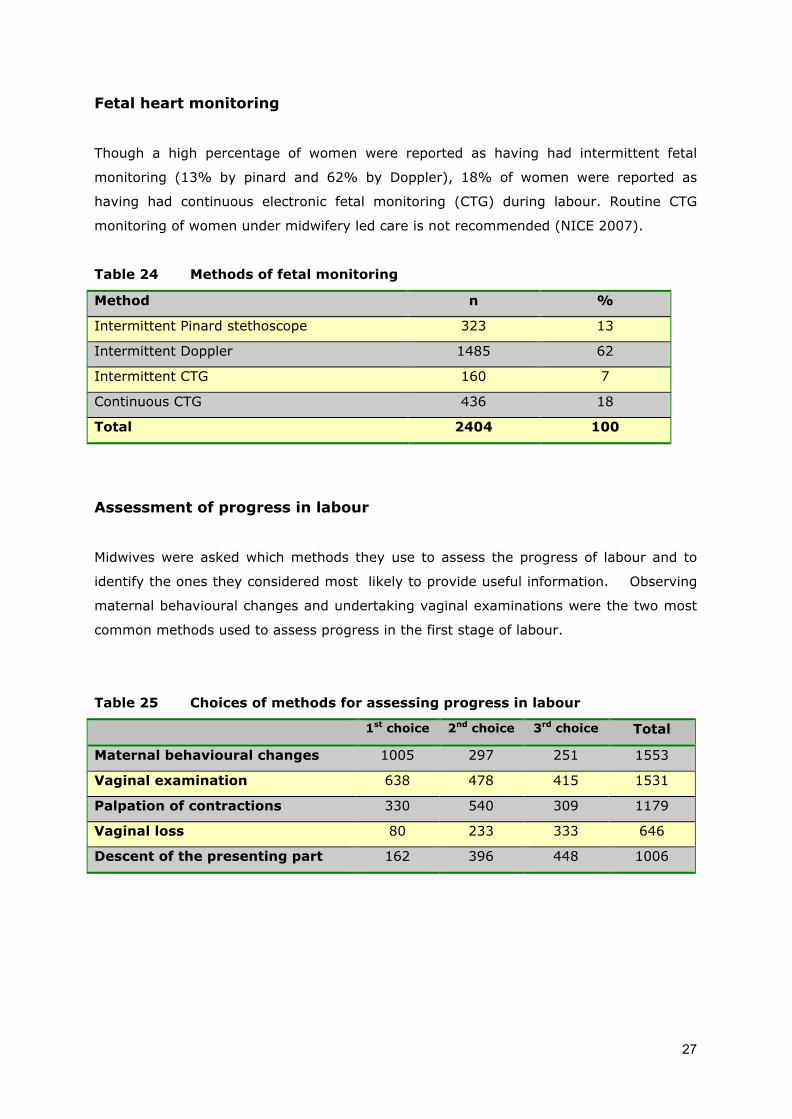
Fetal heart monitoring
Though a high percentage of women were reported as having had intermittent fetal
monitoring (13% by pinard and 62% by Doppler), 18% of women were reported as
having had continuous electronic fetal monitoring (CTG) during labour. Routine CTG
monitoring of women under midwifery led care is not recommended (NICE 2007).
Table 24 Methods of fetal monitoring
Method n %
Intermittent Pinard stethoscope 323 13
Intermittent Doppler 1485 62
Intermittent CTG 160 7
Continuous CTG 436 18
Total 2404 100
Assessment of progress in labour
Midwives were asked which methods they use to assess the progress of labour and to
identify the ones they considered most likely to provide useful information. Observing
maternal behavioural changes and undertaking vaginal examinations were the two most
common methods used to assess progress in the first stage of labour.
Table 25 Choices of methods for assessing progress in labour
1st choice 2nd choice 3rd choice Total
Maternal behavioural changes 1005 297 251 1553
Vaginal examination 638 478 415 1531
Palpation of contractions 330 540 309 1179
Vaginal loss 80 233 333 646
Descent of the presenting part 162 396 448 1006
28
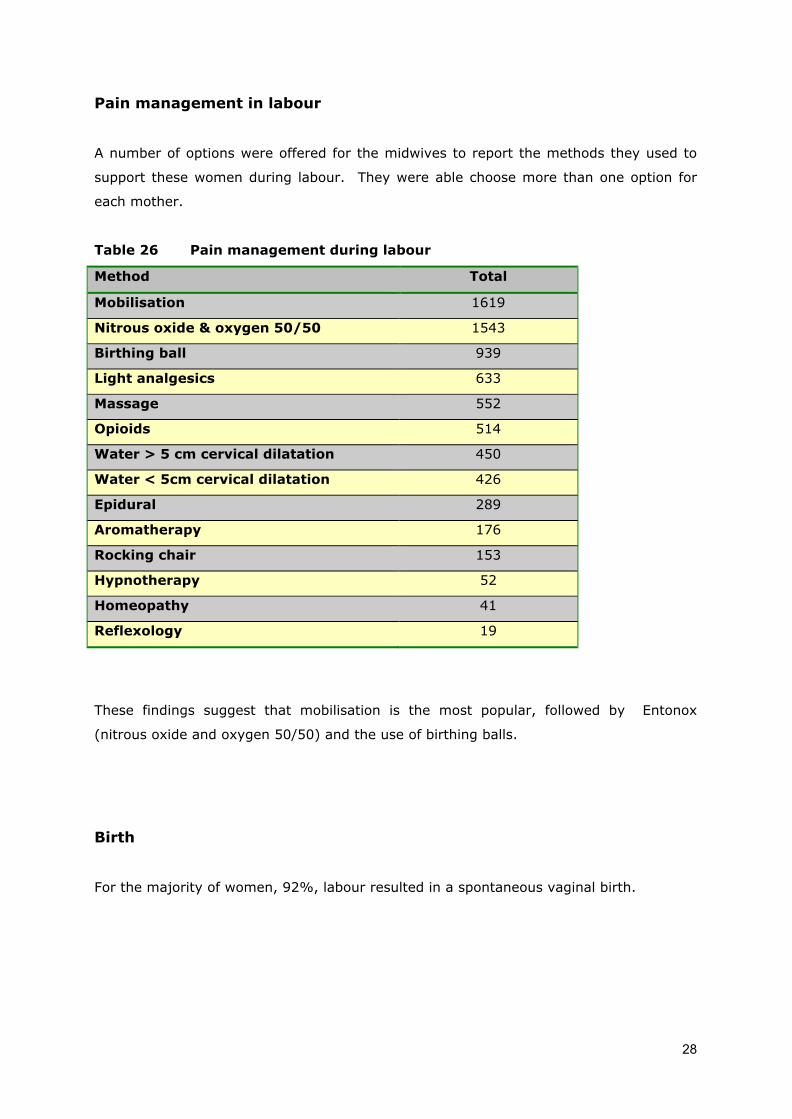
Pain management in labour
A number of options were offered for the midwives to report the methods they used to
support these women during labour. They were able choose more than one option for
each mother.
Table 26 Pain management during labour
Method Total
Mobilisation 1619
Nitrous oxide & oxygen 50/50 1543
Birthing ball 939
Light analgesics 633
Massage 552
Opioids 514
Water > 5 cm cervical dilatation 450
Water < 5cm cervical dilatation 426
Epidural 289
Aromatherapy 176
Rocking chair 153
Hypnotherapy 52
Homeopathy 41
Reflexology 19
These findings suggest that mobilisation is the most popular, followed by Entonox
(nitrous oxide and oxygen 50/50) and the use of birthing balls.
Birth
For the majority of women, 92%, labour resulted in a spontaneous vaginal birth.
29
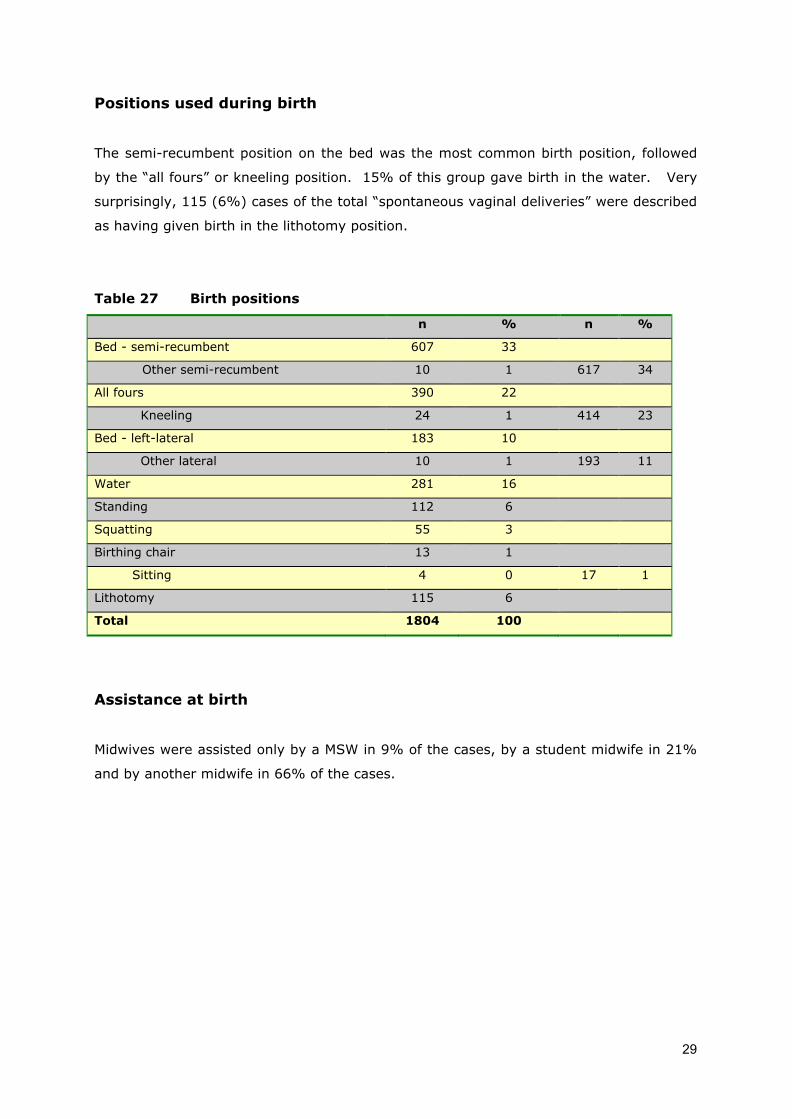
Positions used during birth
The semi-recumbent position on the bed was the most common birth position, followed
by the “all fours” or kneeling position. 15% of this group gave birth in the water. Very
surprisingly, 115 (6%) cases of the total “spontaneous vaginal deliveries” were described
as having given birth in the lithotomy position.
Table 27 Birth positions
n % n %
Bed - semi-recumbent 607 33
Other semi-recumbent 10 1 617 34
All fours 390 22
Kneeling 24 1 414 23
Bed - left-lateral 183 10
Other lateral 10 1 193 11
Water 281 16
Standing 112 6
Squatting 55 3
Birthing chair 13 1
Sitting 4 0 17 1
Lithotomy 115 6
Total 1804 100
Assistance at birth
Midwives were assisted only by a MSW in 9% of the cases, by a student midwife in 21%
and by another midwife in 66% of the cases.
30
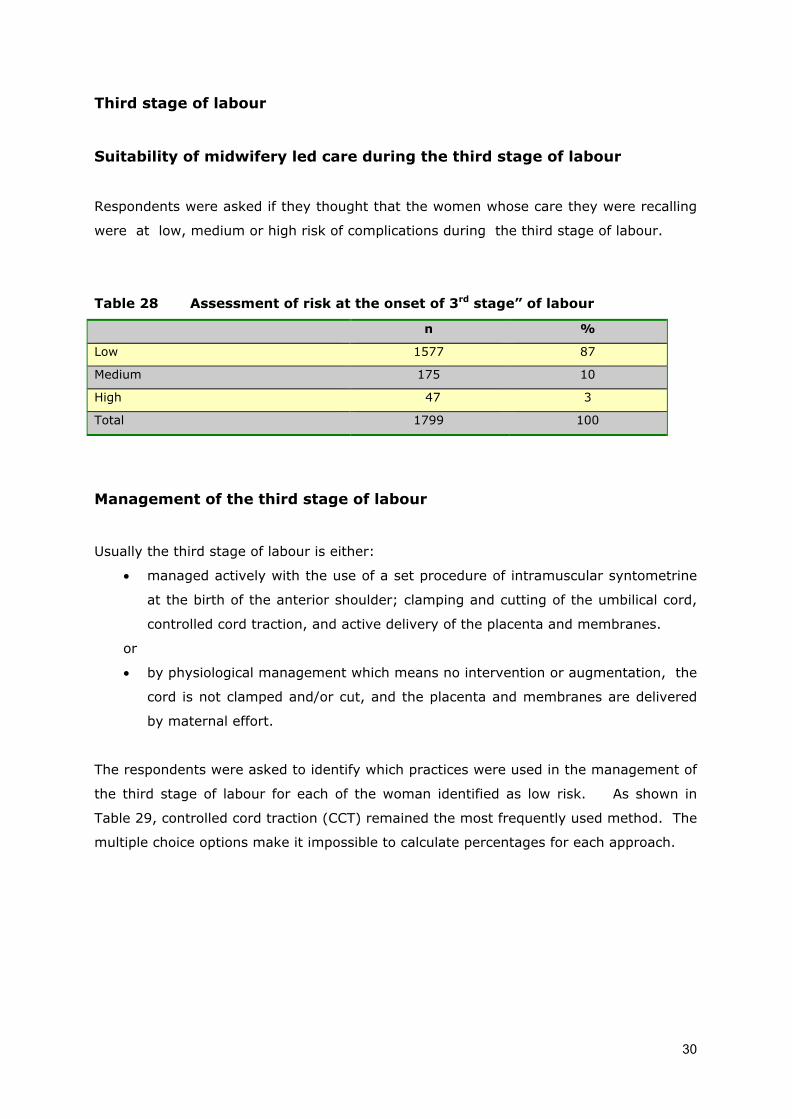
Third stage of labour
Suitability of midwifery led care during the third stage of labour
Respondents were asked if they thought that the women whose care they were recalling
were at low, medium or high risk of complications during the third stage of labour.
Table 28 Assessment of risk at the onset of 3rd stage” of labour
n %
Low 1577 87
Medium 175 10
High 47 3
Total 1799 100
Management of the third stage of labour
Usually the third stage of labour is either:
• managed actively with the use of a set procedure of intramuscular syntometrine
at the birth of the anterior shoulder; clamping and cutting of the umbilical cord,
controlled cord traction, and active delivery of the placenta and membranes.
or
• by physiological management which means no intervention or augmentation, the
cord is not clamped and/or cut, and the placenta and membranes are delivered
by maternal effort.
The respondents were asked to identify which practices were used in the management of
the third stage of labour for each of the woman identified as low risk. As shown in
Table 29, controlled cord traction (CCT) remained the most frequently used method. The
multiple choice options make it impossible to calculate percentages for each approach.
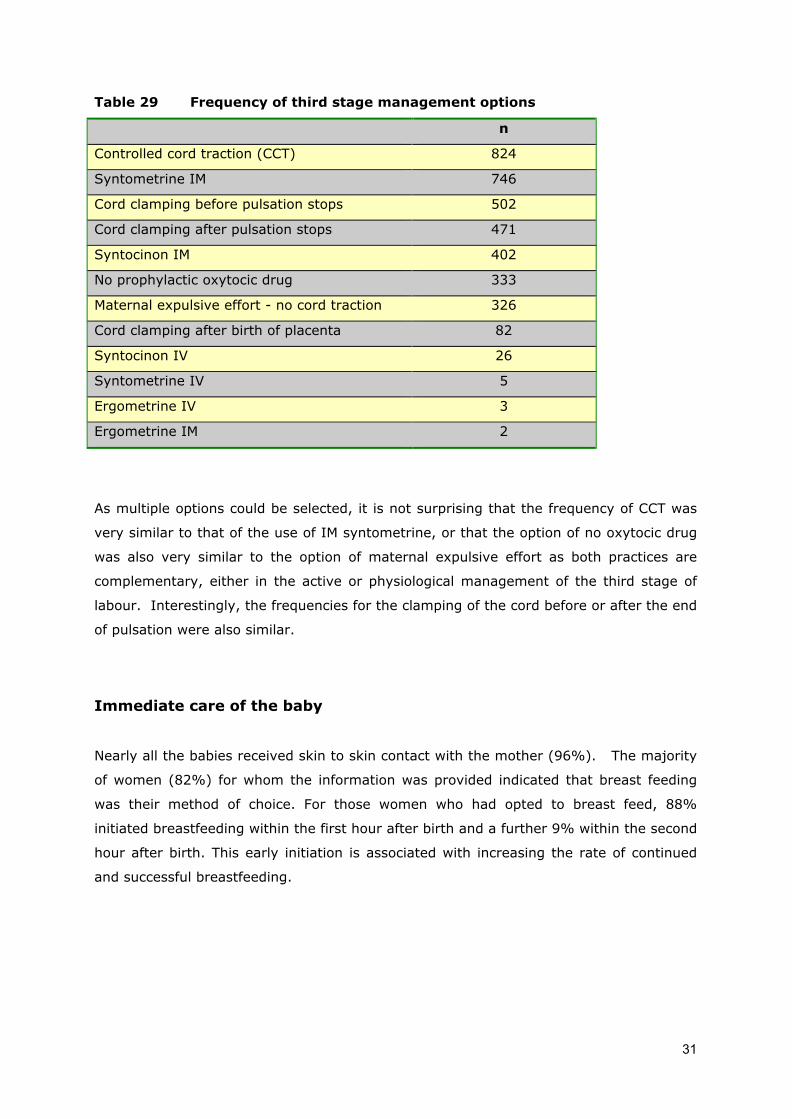
31
Table 29 Frequency of third stage management options
n
Controlled cord traction (CCT) 824
Syntometrine IM 746
Cord clamping before pulsation stops 502
Cord clamping after pulsation stops 471
Syntocinon IM 402
No prophylactic oxytocic drug 333
Maternal expulsive effort - no cord traction 326
Cord clamping after birth of placenta 82
Syntocinon IV 26
Syntometrine IV 5
Ergometrine IV 3
Ergometrine IM 2
As multiple options could be selected, it is not surprising that the frequency of CCT was
very similar to that of the use of IM syntometrine, or that the option of no oxytocic drug
was also very similar to the option of maternal expulsive effort as both practices are
complementary, either in the active or physiological management of the third stage of
labour. Interestingly, the frequencies for the clamping of the cord before or after the end
of pulsation were also similar.
Immediate care of the baby
Nearly all the babies received skin to skin contact with the mother (96%). The majority
of women (82%) for whom the information was provided indicated that breast feeding
was their method of choice. For those women who had opted to breast feed, 88%
initiated breastfeeding within the first hour after birth and a further 9% within the second
hour after birth. This early initiation is associated with increasing the rate of continued
and successful breastfeeding.
32
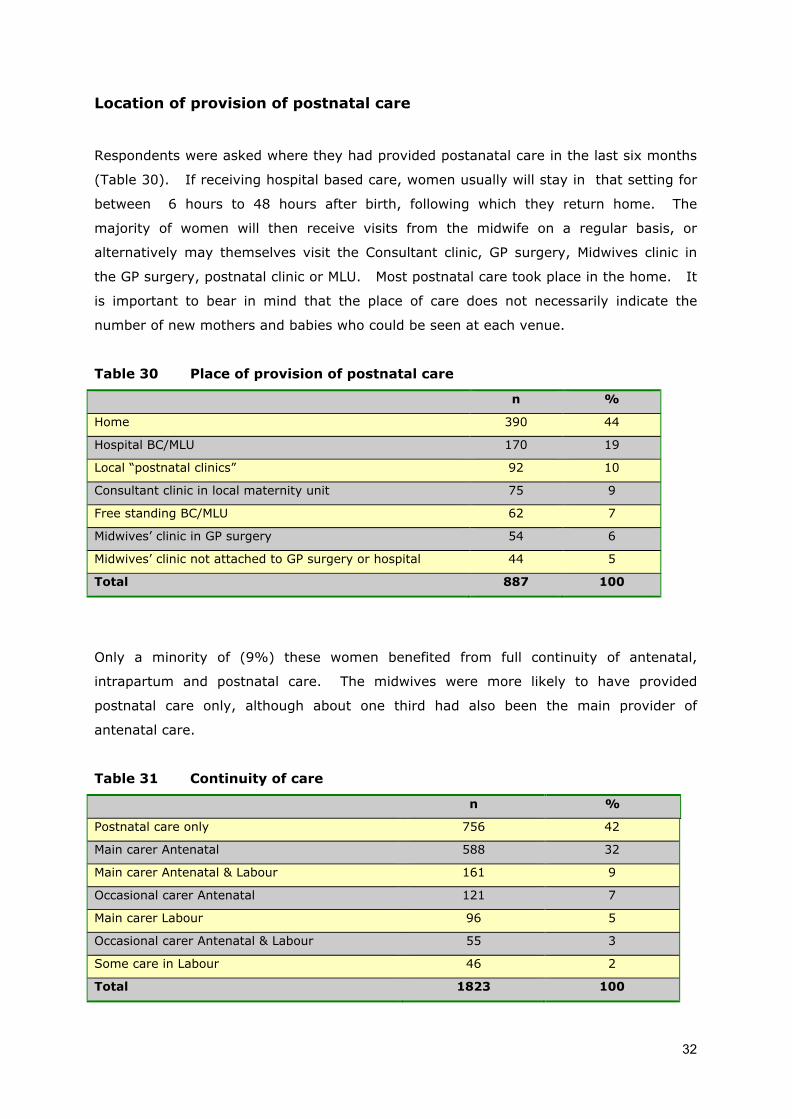
Location of provision of postnatal care
Respondents were asked where they had provided postanatal care in the last six months
(Table 30). If receiving hospital based care, women usually will stay in that setting for
between 6 hours to 48 hours after birth, following which they return home. The
majority of women will then receive visits from the midwife on a regular basis, or
alternatively may themselves visit the Consultant clinic, GP surgery, Midwives clinic in
the GP surgery, postnatal clinic or MLU. Most postnatal care took place in the home. It
is important to bear in mind that the place of care does not necessarily indicate the
number of new mothers and babies who could be seen at each venue.
Table 30 Place of provision of postnatal care
n %
Home 390 44
Hospital BC/MLU 170 19
Local “postnatal clinics” 92 10
Consultant clinic in local maternity unit 75 9
Free standing BC/MLU 62 7
Midwives’ clinic in GP surgery 54 6
Midwives’ clinic not attached to GP surgery or hospital 44 5
Total 887 100
Only a minority of (9%) these women benefited from full continuity of antenatal,
intrapartum and postnatal care. The midwives were more likely to have provided
postnatal care only, although about one third had also been the main provider of
antenatal care.
Table 31 Continuity of care
n %
Postnatal care only 756 42
Main carer Antenatal 588 32
Main carer Antenatal & Labour 161 9
Occasional carer Antenatal 121 7
Main carer Labour 96 5
Occasional carer Antenatal & Labour 55 3
Some care in Labour 46 2
Total 1823 100
33
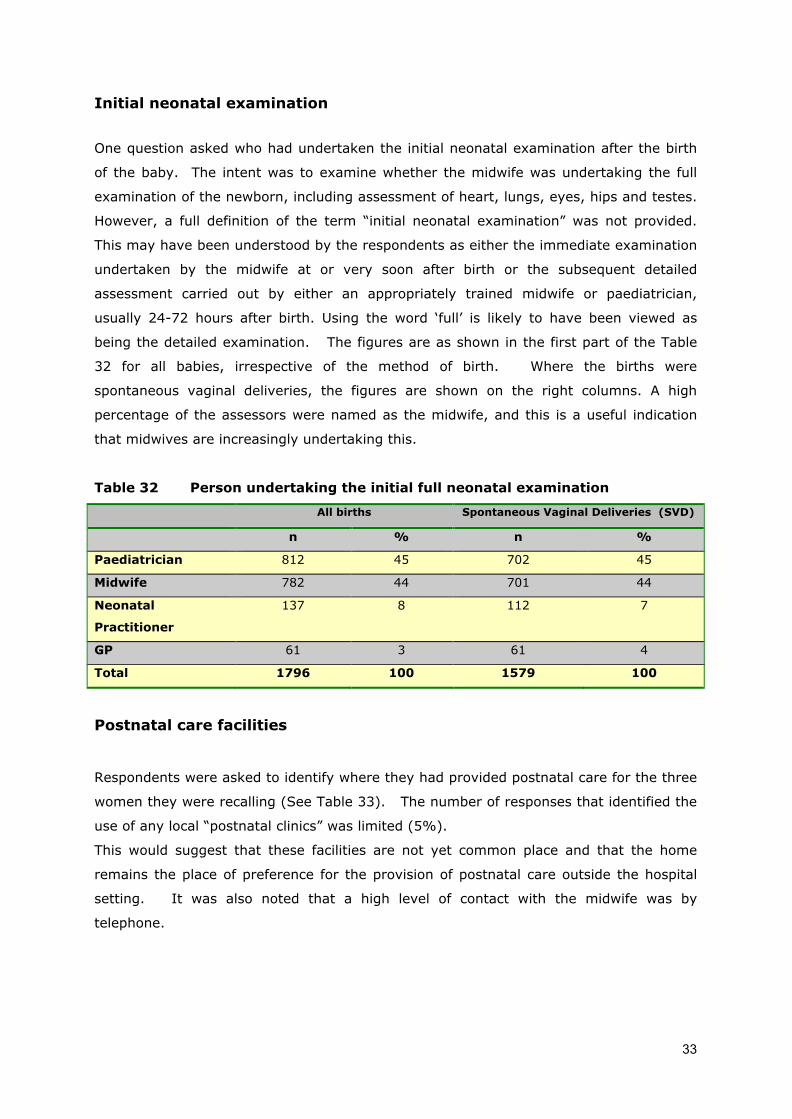
Initial neonatal examination
One question asked who had undertaken the initial neonatal examination after the birth
of the baby. The intent was to examine whether the midwife was undertaking the full
examination of the newborn, including assessment of heart, lungs, eyes, hips and testes.
However, a full definition of the term “initial neonatal examination” was not provided.
This may have been understood by the respondents as either the immediate examination
undertaken by the midwife at or very soon after birth or the subsequent detailed
assessment carried out by either an appropriately trained midwife or paediatrician,
usually 24-72 hours after birth. Using the word ‘full’ is likely to have been viewed as
being the detailed examination. The figures are as shown in the first part of the Table
32 for all babies, irrespective of the method of birth. Where the births were
spontaneous vaginal deliveries, the figures are shown on the right columns. A high
percentage of the assessors were named as the midwife, and this is a useful indication
that midwives are increasingly undertaking this.
Table 32 Person undertaking the initial full neonatal examination
All births Spontaneous Vaginal Deliveries (SVD)
n % n %
Paediatrician 812 45 702 45
Midwife 782 44 701 44
Neonatal
Practitioner
137 8 112 7
GP 61 3 61 4
Total 1796 100 1579 100
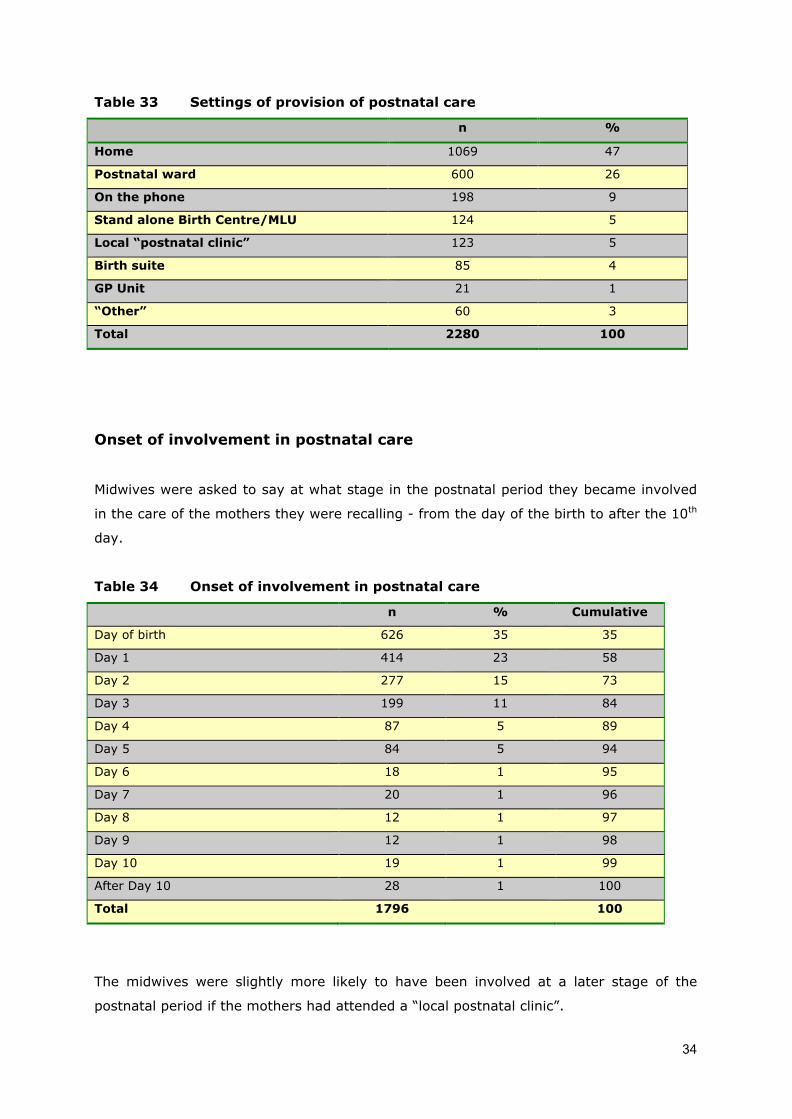
Postnatal care facilities
Respondents were asked to identify where they had provided postnatal care for the three
women they were recalling (See Table 33). The number of responses that identified the
use of any local “postnatal clinics” was limited (5%).
This would suggest that these facilities are not yet common place and that the home
remains the place of preference for the provision of postnatal care outside the hospital
setting. It was also noted that a high level of contact with the midwife was by
telephone.
34
Table 33 Settings of provision of postnatal care
n %
Home 1069 47
Postnatal ward 600 26
On the phone 198 9
Stand alone Birth Centre/MLU 124 5
Local “postnatal clinic” 123 5
Birth suite 85 4
GP Unit 21 1
“Other” 60 3
Total 2280 100
Onset of involvement in postnatal care
Midwives were asked to say at what stage in the postnatal period they became involved
in the care of the mothers they were recalling - from the day of the birth to after the 10th
day.
Table 34 Onset of involvement in postnatal care
n % Cumulative
Day of birth 626 35 35
Day 1 414 23 58
Day 2 277 15 73
Day 3 199 11 84
Day 4 87 5 89
Day 5 84 5 94
Day 6 18 1 95
Day 7 20 1 96
Day 8 12 1 97
Day 9 12 1 98
Day 10 19 1 99
After Day 10 28 1 100
Total 1796 100
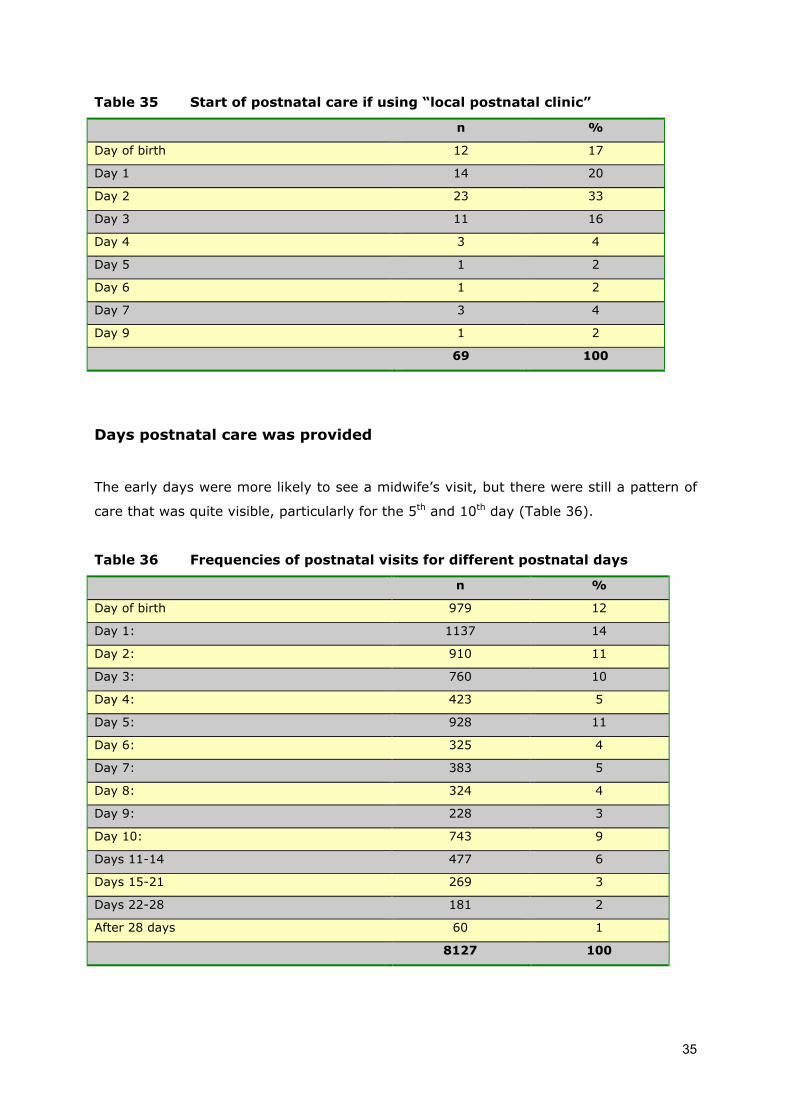
The midwives were slightly more likely to have been involved at a later stage of the
postnatal period if the mothers had attended a “local postnatal clinic”.
35
Table 35 Start of postnatal care if using “local postnatal clinic”
n %
Day of birth 12 17
Day 1 14 20
Day 2 23 33
Day 3 11 16
Day 4 3 4
Day 5 1 2
Day 6 1 2
Day 7 3 4
Day 9 1 2
69 100
Days postnatal care was provided
The early days were more likely to see a midwife’s visit, but there were still a pattern of
care that was quite visible, particularly for the 5th and 10th day (Table 36).
Table 36 Frequencies of postnatal visits for different postnatal days
n %
Day of birth 979 12
Day 1: 1137 14
Day 2: 910 11
Day 3: 760 10
Day 4: 423 5
Day 5: 928 11
Day 6: 325 4
Day 7: 383 5
Day 8: 324 4
Day 9: 228 3
Day 10: 743 9
Days 11-14 477 6
Days 15-21 269 3
Days 22-28 181 2
After 28 days 60 1
8127 100
36
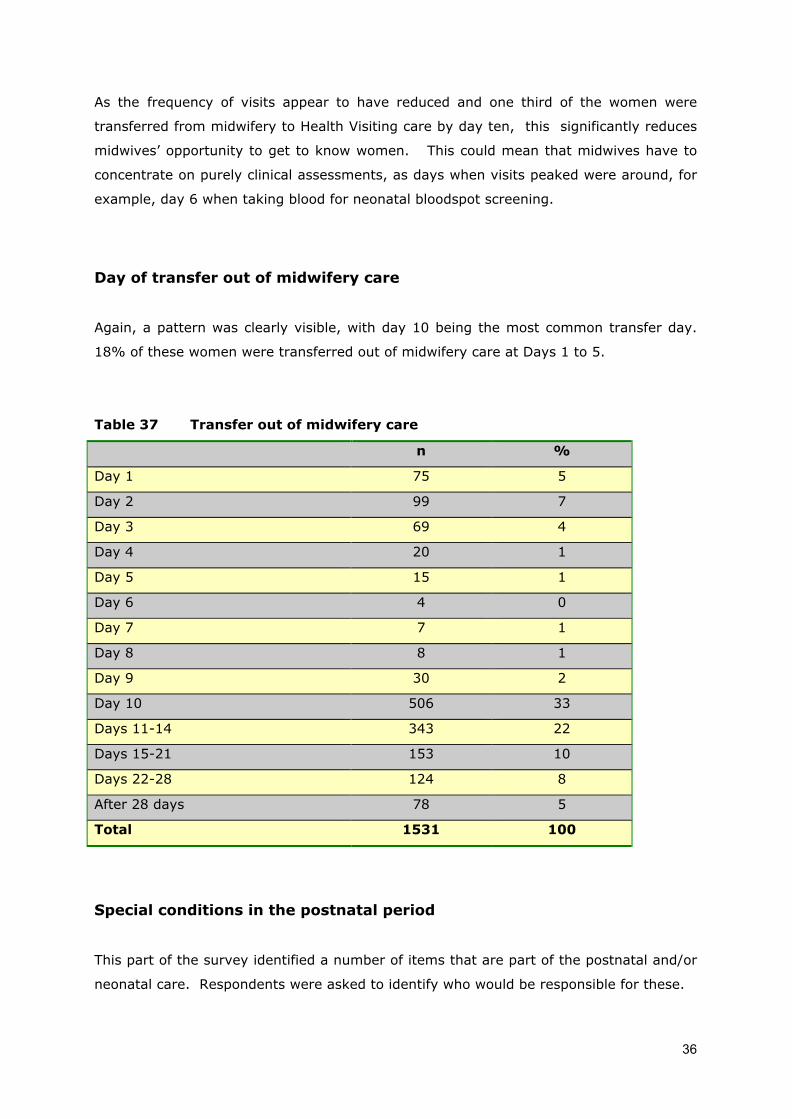
As the frequency of visits appear to have reduced and one third of the women were
transferred from midwifery to Health Visiting care by day ten, this significantly reduces
midwives’ opportunity to get to know women. This could mean that midwives have to
concentrate on purely clinical assessments, as days when visits peaked were around, for
example, day 6 when taking blood for neonatal bloodspot screening.
Day of transfer out of midwifery care
Again, a pattern was clearly visible, with day 10 being the most common transfer day.
18% of these women were transferred out of midwifery care at Days 1 to 5.
Table 37 Transfer out of midwifery care
n %
Day 1 75 5
Day 2 99 7
Day 3 69 4
Day 4 20 1
Day 5 15 1
Day 6 4 0
Day 7 7 1
Day 8 8 1
Day 9 30 2
Day 10 506 33
Days 11-14 343 22
Days 15-21 153 10
Days 22-28 124 8
After 28 days 78 5
Total 1531 100
Special conditions in the postnatal period
This part of the survey identified a number of items that are part of the postnatal and/or
neonatal care. Respondents were asked to identify who would be responsible for these.
37
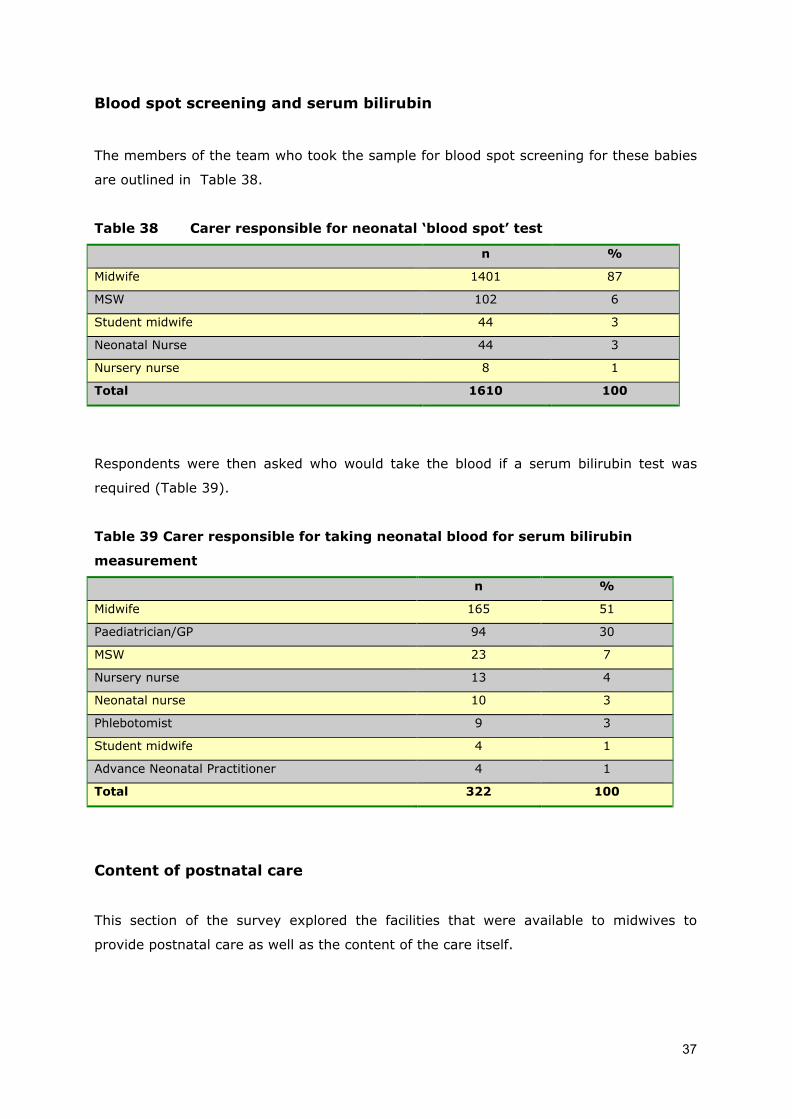
Blood spot screening and serum bilirubin
The members of the team who took the sample for blood spot screening for these babies
are outlined in Table 38.
Table 38 Carer responsible for neonatal ‘blood spot’ test
n %
Midwife 1401 87
MSW 102 6
Student midwife 44 3
Neonatal Nurse 44 3
Nursery nurse 8 1
Total 1610 100
Respondents were then asked who would take the blood if a serum bilirubin test was
required (Table 39).
Table 39 Carer responsible for taking neonatal blood for serum bilirubin
measurement
n %
Midwife 165 51
Paediatrician/GP 94 30
MSW 23 7
Nursery nurse 13 4
Neonatal nurse 10 3
Phlebotomist 9 3
Student midwife 4 1
Advance Neonatal Practitioner 4 1
Total 322 100
Content of postnatal care
This section of the survey explored the facilities that were available to midwives to
provide postnatal care as well as the content of the care itself.
38
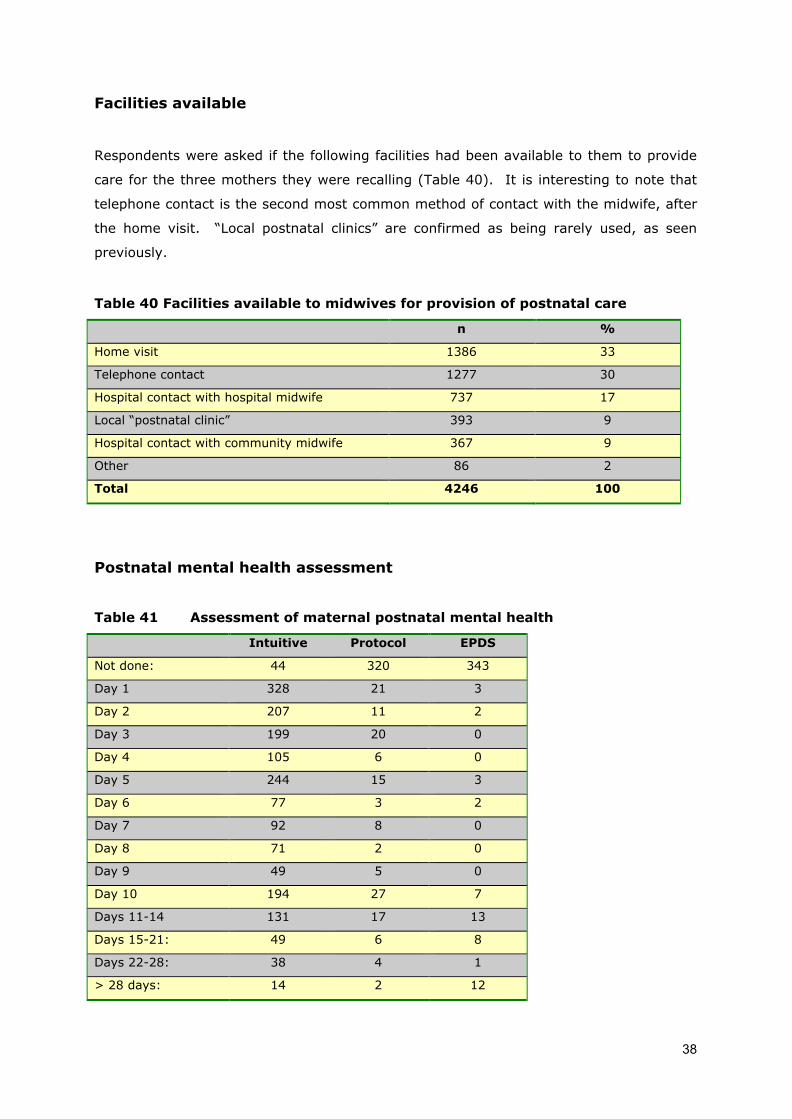
Facilities available
Respondents were asked if the following facilities had been available to them to provide
care for the three mothers they were recalling (Table 40). It is interesting to note that
telephone contact is the second most common method of contact with the midwife, after
the home visit. “Local postnatal clinics” are confirmed as being rarely used, as seen
previously.
Table 40 Facilities available to midwives for provision of postnatal care
n %
Home visit 1386 33
Telephone contact 1277 30
Hospital contact with hospital midwife 737 17
Local “postnatal clinic” 393 9
Hospital contact with community midwife 367 9
Other 86 2
Total 4246 100
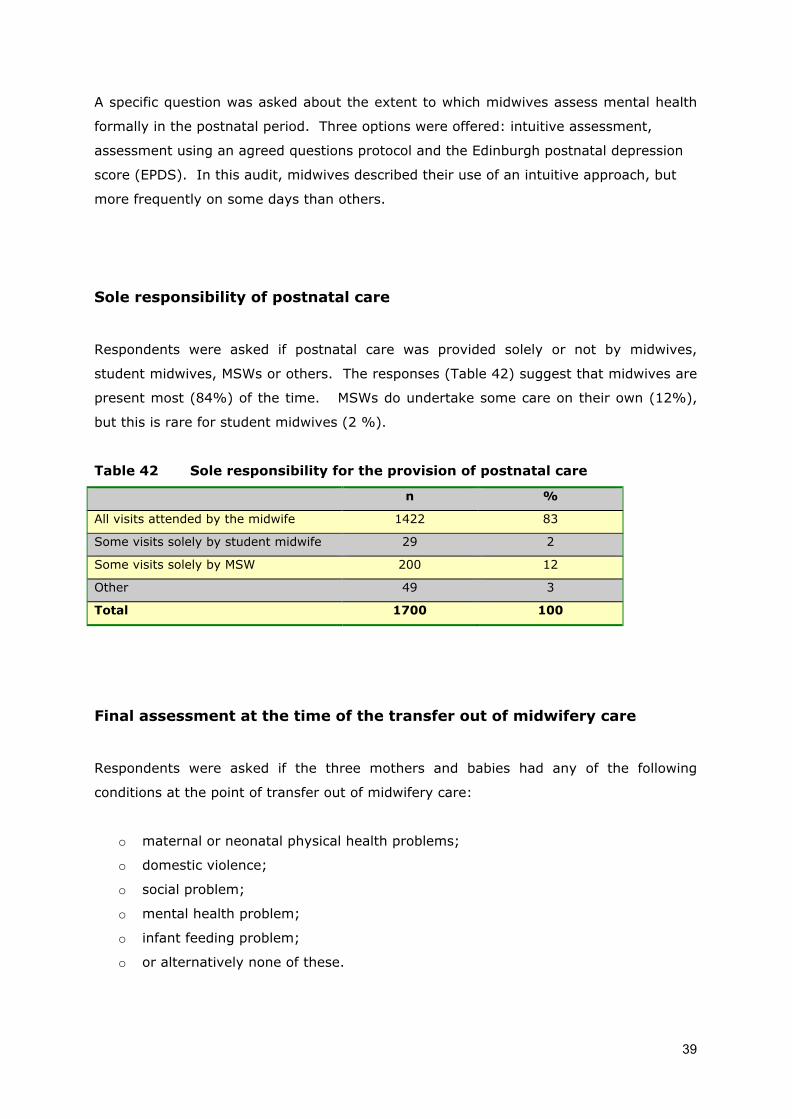
Postnatal mental health assessment
Table 41 Assessment of maternal postnatal mental health
Intuitive Protocol EPDS
Not done: 44 320 343
Day 1 328 21 3
Day 2 207 11 2
Day 3 199 20 0
Day 4 105 6 0
Day 5 244 15 3
Day 6 77 3 2
Day 7 92 8 0
Day 8 71 2 0
Day 9 49 5 0
Day 10 194 27 7
Days 11-14 131 17 13
Days 15-21: 49 6 8
Days 22-28: 38 4 1
> 28 days: 14 2 12
39
A specific question was asked about the extent to which midwives assess mental health
formally in the postnatal period. Three options were offered: intuitive assessment,
assessment using an agreed questions protocol and the Edinburgh postnatal depression
score (EPDS). In this audit, midwives described their use of an intuitive approach, but
more frequently on some days than others.
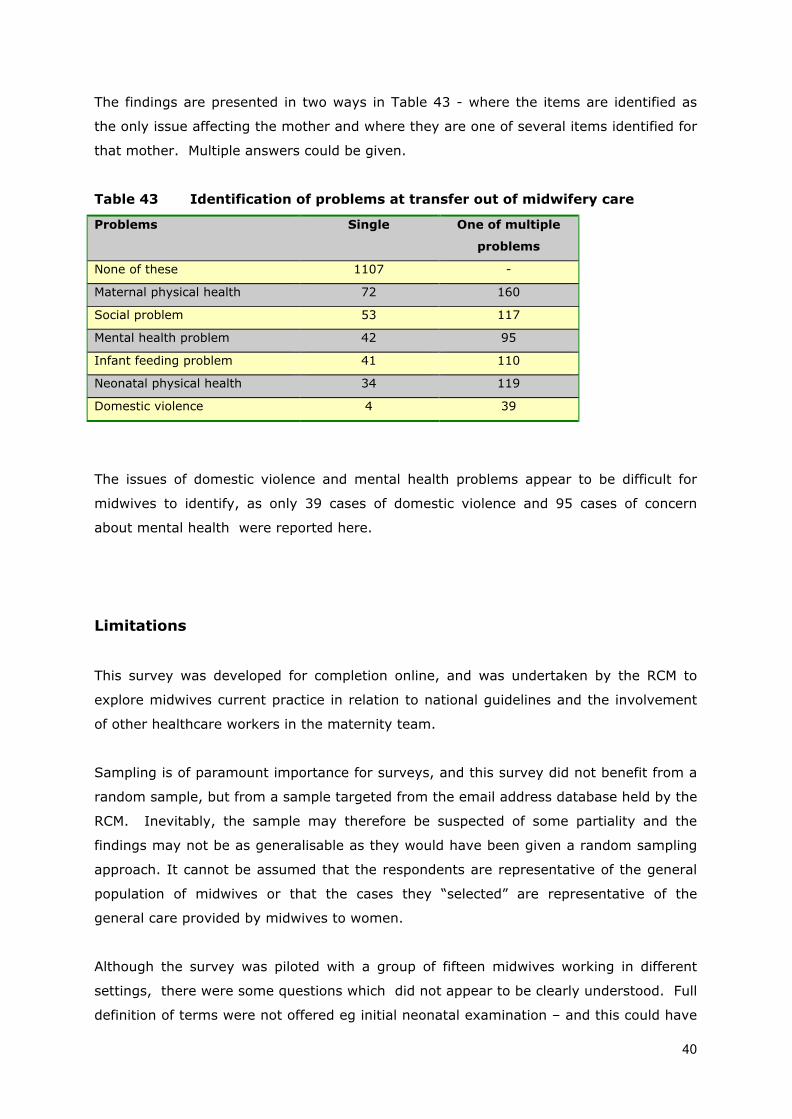
Sole responsibility of postnatal care
Respondents were asked if postnatal care was provided solely or not by midwives,
student midwives, MSWs or others. The responses (Table 42) suggest that midwives are
present most (84%) of the time. MSWs do undertake some care on their own (12%),
but this is rare for student midwives (2 %).
Table 42 Sole responsibility for the provision of postnatal care
n %
All visits attended by the midwife 1422 83
Some visits solely by student midwife 29 2
Some visits solely by MSW 200 12
Other 49 3
Total 1700 100
Final assessment at the time of the transfer out of midwifery care
Respondents were asked if the three mothers and babies had any of the following
conditions at the point of transfer out of midwifery care:
o maternal or neonatal physical health problems;
o domestic violence;
o social problem;
o mental health problem;
o infant feeding problem;
o or alternatively none of these.
40
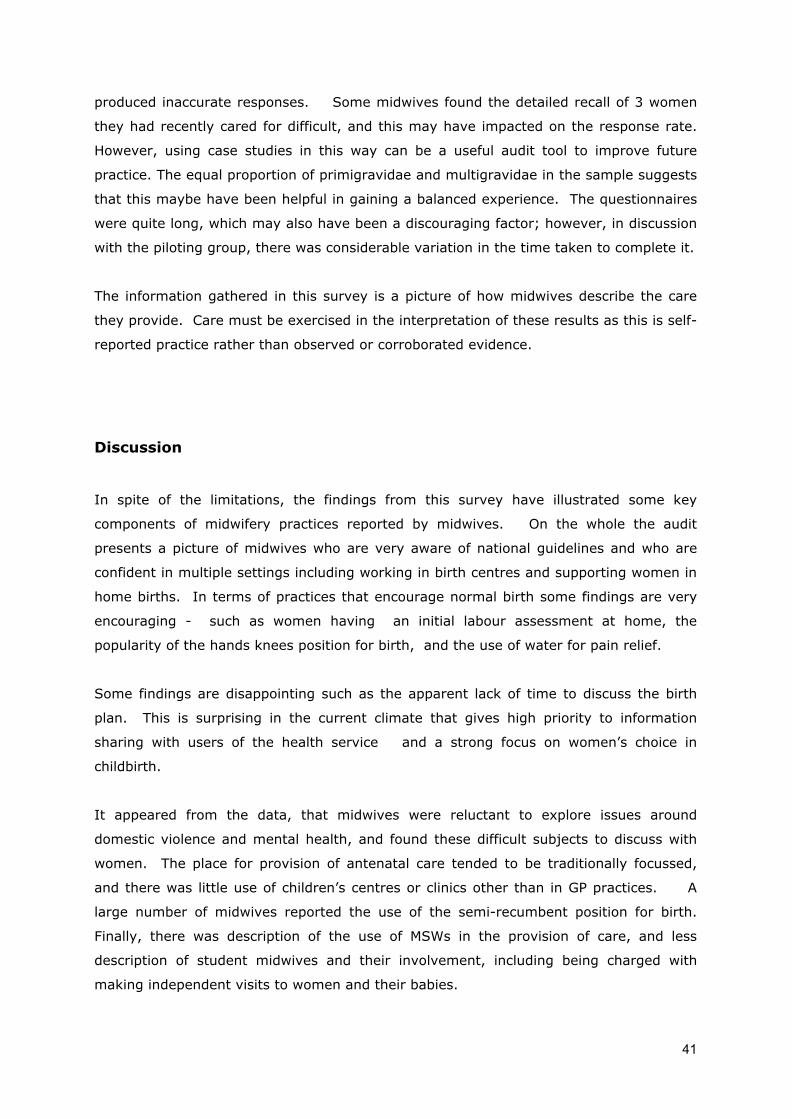
The findings are presented in two ways in Table 43 - where the items are identified as
the only issue affecting the mother and where they are one of several items identified for
that mother. Multiple answers could be given.
Table 43 Identification of problems at transfer out of midwifery care
Problems Single One of multiple
problems
None of these 1107 -
Maternal physical health 72 160
Social problem 53 117
Mental health problem 42 95
Infant feeding problem 41 110
Neonatal physical health 34 119
Domestic violence 4 39
The issues of domestic violence and mental health problems appear to be difficult for
midwives to identify, as only 39 cases of domestic violence and 95 cases of concern
about mental health were reported here.
Limitations
This survey was developed for completion online, and was undertaken by the RCM to
explore midwives current practice in relation to national guidelines and the involvement
of other healthcare workers in the maternity team.
Sampling is of paramount importance for surveys, and this survey did not benefit from a
random sample, but from a sample targeted from the email address database held by the
RCM. Inevitably, the sample may therefore be suspected of some partiality and the
findings may not be as generalisable as they would have been given a random sampling
approach. It cannot be assumed that the respondents are representative of the general
population of midwives or that the cases they “selected” are representative of the
general care provided by midwives to women.
Although the survey was piloted with a group of fifteen midwives working in different
settings, there were some questions which did not appear to be clearly understood. Full
definition of terms were not offered eg initial neonatal examination – and this could have
41
produced inaccurate responses. Some midwives found the detailed recall of 3 women
they had recently cared for difficult, and this may have impacted on the response rate.
However, using case studies in this way can be a useful audit tool to improve future
practice. The equal proportion of primigravidae and multigravidae in the sample suggests
that this maybe have been helpful in gaining a balanced experience. The questionnaires
were quite long, which may also have been a discouraging factor; however, in discussion
with the piloting group, there was considerable variation in the time taken to complete it.
The information gathered in this survey is a picture of how midwives describe the care
they provide. Care must be exercised in the interpretation of these results as this is self-
reported practice rather than observed or corroborated evidence.
Discussion
In spite of the limitations, the findings from this survey have illustrated some key
components of midwifery practices reported by midwives. On the whole the audit
presents a picture of midwives who are very aware of national guidelines and who are
confident in multiple settings including working in birth centres and supporting women in
home births. In terms of practices that encourage normal birth some findings are very
encouraging - such as women having an initial labour assessment at home, the
popularity of the hands knees position for birth, and the use of water for pain relief.
Some findings are disappointing such as the apparent lack of time to discuss the birth
plan. This is surprising in the current climate that gives high priority to information
sharing with users of the health service and a strong focus on women’s choice in
childbirth.
It appeared from the data, that midwives were reluctant to explore issues around
domestic violence and mental health, and found these difficult subjects to discuss with
women. The place for provision of antenatal care tended to be traditionally focussed,
and there was little use of children’s centres or clinics other than in GP practices. A
large number of midwives reported the use of the semi-recumbent position for birth.
Finally, there was description of the use of MSWs in the provision of care, and less
description of student midwives and their involvement, including being charged with
making independent visits to women and their babies.
42
Conclusions
The key findings of the audit are
The issues of domestic violence and mental health appear to be still difficult for
midwives to identify.
Some midwives perceived that there was insufficient time to discuss labour plans
with women at booking or during the antenatal period.
While the majority of women were assessed in a consultant unit, about a fifth of
the women had an initial labour assessment at home.
The key practitioner at birth was noted as the midwife, and a small proportion as
the student midwife.
The semi-recumbent position on the bed, is still the most common position for
birth, but closely followed by the hands knees position.
Midwives appear to give significant weight to maternal behavioural change as a
means of assessing progress in labour, as well as clinical assessments.
44% of full examinations of the newborn were reported as being undertaken by
the midwife.
At the time of this audit there appeared to be very little use of children’s centres
or clinics other than in GP practices.
The role of Maternity Support Workers at this point appears to be limited, though
they are providing some postnatal support.
The role of student midwives in undertaking postnatal visits on their own was less
than Maternity Support Workers. This may have a crucial impact on reducing
their potential experience, competence and confidence as future autonomous
midwives.
Key recommendations
That appropriate education and training opportunities are identified and developed
locally to enable midwives to be competent and confident in discussing issues of
domestic abuse and mental health.
That more tools and resources be developed by the RCM CNB for midwives to work
with women to encourage ‘off the bed’ positions during labour and birth.
That midwives consider critically the role and responsibilities of the student midwife
in the context of gaining appropriate experience, competence and confidence in the
full role of the midwife.

43
That the range of midwifery services within local community settings are promoted
That midwives and others engaged in maternity services use local audit to identify
local practice and practice development.
That the potential for new research triggered by these findings, in support of
effective practices related to labour and birth positions, be explored.
This audit provides an interesting and useful ‘snapshot’ of midwives current practice and
how it reflects national guidelines. Clearly midwives know what is recommended in
national guidelines and report that their practice is in line with the guidelines. Midwives,
managers and educationalists, and those supporting maternity services need to take the
results from this audit and further develop the service and also use this information to
inform midwives’ pre-registration education and continuing professional development.
44
References
Care Quality Commission (CQC) (2010) Maternity services Report
http://www.cqc.org.uk/aboutcqc/howwedoit/involvingpeoplewhouseservices/patientsurve
ys/maternityservices.cfm
European Parliament and European Council (2005) Directive 2005/36/EC of the
European Parliament and of the Council on the recognition of professional
qualifications http://register.consilium.eu.int/pdf/en/05/st03/st03627.en05.pdf,
NICE (2007) Antenatal and postnatal mental health. London : NICE
http://guidance.nice.org.uk/CG45/NICEGuidance
NICE (2007) Intrapartum care. Care of healthy women and their babies during
childbirth. London: NICE http://guidance.nice.org.uk/CG55/NICEGuidance
NICE (2008) Antenatal care. Routine care for the healthy pregnant woman London:
NICE http://guidance.nice.org.uk/CG62/NICEGuidance
Royal College of Midwives (RCM) (2008) Evidence based Guidelines for midwifery led
care in labour London : RCM http://www.rcm.org.uk/college/policy-
practice/guidelines/practice-guidelines/
Royal College of Midwives (RCM) (2010) One-to-one midwifery care in labour: A briefing
paper London : RCM
WHO (1996) Care in normal birth: a practical guide. Geneva: WHO
http://www.who.int/making_pregnancy_safer/documents/who_frh_msm_9624
The Royal College of Midwives Trust15 Mansfield Street, London, W1G 9NHT: 020 7312 3535 E: [email protected]