Embed Size (px)
Citation preview
Nutrition Vol. 13, No. 9(Suppl), 1997
The Route of Nutritional Support in the Critically II1: Physiological and
Economical Considerations
PAUL FROST, MRCP, AND DAVID BIHARI, FRACP
From the Department of Intensive Care, The St. George Hospital, Sydney, Australia
ABSTRACT
Although it generally is accepted that early enteral nutrition is of benefit to criticaily ill patients, there is little evidence to support this assertion. Nevertheless, enteral nutrition has many advantages over total parenteral nutrition (TPN), the latter being associated with several complications. Animal studies have shown that injury and infection can lead to gut atrophy and increased mucosal permeability. Translocation of bacteria and endotoxin in these animal models may initiate a systemic inflammatory response and cause multiple organ fallure (MOF). Again, there is little direct evidence to suggest that similar mechanisms operate in humans. As a cause of MOF, simple splanchnic ischemia and reperfusion may be sufficient with no absolute requirement for translocation. In this setting, enteral nutrition may preserve splanchnic blood flow and prevent mucosal breakdown. Unfortunately there is a widespread misconception that gastric stasis, the absence of bowel sounds, and recent abdominal surgery preclude enteral feeding. There are few absolute contraindications to early enteral feeding and with motivated staff, the use of prokinetics, and the availability of jejunal feeding tubes, the majority of intensive care patients can be red enterally. Enteral feeding is more cost effective than TPN, but TPN remains a common therapeutic intervention in the intensive care unit and represents a significant burden on health care budgets. Nutrition support teams have led to savings, particularly by identifying patients who have been inappropriately prescribed TPN and also by preventing excessive enteral feeding. Nutrition 1997; 13(Suppl):58S-63S. ©Elsevier Science Inc. 1997
Key words: enteral nutrition, total parenteral nutrition, critical illness, cost benefit analysis, nutritional support
INTRODUCTION
Critical illness nearly always is accompanied by a catabolic state that leads most obviously to skeletal muscle wasting but also to the malfunction of all organ systems including the im- mune, respiratory, and gastrointestinal systems. It seems intu- itively sensible to provide exogenous nutrients in an attempt to ameliorate this catabolic state, but, surprisingly, this approach is still the subject of debate. Although it is true that there are few well-designed, prospective, randomized controlled clinical trials (RCCTs) to justify early nutrifional support in critically ill patients, 1 there a rea variety of reasons for the absence of convincing evidence. First, such trials need to be very large, given the heterogeneous nature of the population of critically ill patients studied and the beneficial effect of nutritional sup- port alone on outcome may be very small. Moreover, there are now obvious ethical difficulties in proceeding with a large RCCT in which the control group receives no nutritional sup- port during their intensive care unit (ICU) stay. Finally it has been suggested that the beneficial influence of nutritional sup- port may be inversely proportional to the severity of illness.
Hence, it is probably unreasonable to anticipate great benefit in patients with acute overwhelming illness. 2 With regard to the question of the preferred route of nutritional support, the position is more clear; whenever possible, feeding using the enteral route is preferred. Nevertheless, the exact nature of such nutritional support, i.e., the most appropriate constituents to be administered by the enteral route, has become a contentious issue reflecting a greater emphasis on the importance of the function of various nutrients in the host's response to injury and sepsis. This arficle centers upon some aspects of the physio- logical and economic rationale behind preferences concerning route of feeding.
PHYSIOLOGICAL CONSIDERATIONS
Normal gut structure and function depends upon an adequate delivery of oxygen and other nutfients to the mucosa. During starvaüon, criücal illness, or the administration of TPN, these basic requirements may not be met. Many different animal studies have demonstrated that in these circumstances, gut atro- phy and changes in mucosal permeability can ensue. It has
Correspondence to: David Bihari, FRACP, Department of Intensive Care, The St. George Hospital, Gray Street, Kogarah, NSW 2217, Australia
Nutrition 13(Suppl):58S-63S, 1997 ©Elsevier Science Inc. 1997 Printed in the USA. All rights reserved. ELSEVIER
0899-9007/97/$17.00 PII S0899-9007(97)00207-4

NUTRITIONAL SUPPORT IN THE CRITICALLY ILL 59S
been suggested that these changes might allow the passage of bacteria (translocation) or maerom01ecules such as endotoxin into the systemic circulation resulting in inflammatory mediator activation, an acute inflammatory response (so-caUed systemic inflammatory response syndrome), and ultimately single or multiple organ failure (MOF).3 However, the evidence for this hypothesis is largely derived from small animal (rodent) mod- eis of bums, trauma, and sepsis and should be interpreted cau- tiously. Perhaps not surprisingly, the rat and human small intes- tines behave differently when subjected to similar stresses, e.g., starvation in the rat can result in small bowel atrophy within 4 d 4 whereas the human bowel may remain normal for --<2 wk of starvation. -~ If total parenteral nutrition (TPN) is adminis- tered to a rat, gut atrophy may occur within 3 d, whereas there is very little evidence to demonstrate whether TPN-induced intestinal atrophy actually occurs in humans. Small groups of children on long-term TPN have been studied, but only mild focal villus atrophy has been demonstrated. 6 Further confusion exists over the relationship among changes in gut permeability, the presence or absence of mucosal atrophy, and the occurrence of bacterial translocation. Illig et al.7 investigated gut lactulose permeability and the phenomenon of bacterial translocation in four groups of rats; the first group received TPN, the second group received the same solution but by the enteral route, the third group received the solution divided between the two routes (intravenous and enteral), and the fourth was allowed to feed normally. These authors found that although the strict TPN group demonstrated mucosal atrophy and an increased perme- ability to lactulose, the incidence of bacterial translocation was not significantly different between the four groups. They con- cluded that septic states occurring in association with TPN or trauma and apparently originating from the gut may be initiated by macromolecules (cytokines, other inflammatory mediators) arising from the gut itself rather than from bacteria within the lumen. In this sense, bacterial translocation could be the end result rather than the prime cause of systemic sepsis. 7
Another confounding factor in the interpretation of the sig- nificance of bacterial translocation in humans is the suggestion that the presence of bacteria in mesenteric lymph nodes might represent a normal physiological phenomenon that allows the organism to produce appropriate immune responses to gut lumi- nal pathogens. At this time, there is little direct evidence in humans to implicate gut bacterial or bacterial product transloca- tion as a cause of MOF. Because simple splanchnic (including hepatic) ischemia and reperfusion is enough to initiate a pro- found inflammatory response, it may not be necessary to invoke translocation as an absolute requirement for the development of organ dysfunction. In any event, the assertion that the gut is the "motor of M O F " remains unproven.
Given the importance of splanchnic ischernia and reperfu- sion in shock states (its early development in any form of shock and its relatively late reversal during the phase of resuscitation), enteral nutrition may have a cyto-protective effect by enhancing or maintaining splanchnic blood flow. Indeed, one experimental model did in fact demonstrate that early enteral nutrition could restore gastrointestinal blood flow after an acute lung injury. 8 Although it is difficult to imagine that early enteral nutrition could improve splanchnic blood flow in the setting of uncor- rected hypovolernia or an inadequate cardiac output, the pres- ence of nutrients within the lumen of the gastrointestinal tract might act to preserve blood flow, and this could have important implications for the prevention of mucosal breakdown and stress ulceration.
Aside from the possible association of TPN with impaired gastrointestinal barrier function, there are other important con-
sequences associated with the unphysiological practice of by- passing the gut and delivering nutrients directly into the blood. In addition to the well-described mechanical complications of central venous cannulation, venous thrombosis, catheter-related sepsis, 9 and severe metabolic disturbances such as hyperglyce- mia, there is jusüfiable concern regarding the hazards of intra- venous lipids. Intravenous fat has many weU-documented im- munosuppressive effects: intravenous long-chain triglycerides reduce the functions of the reticulo-endothelial system, 10 neu- trophils,'l and tläe ratio of T helper to T suppressor cells.12 This potent immunosuppressive effect is illustrated by the fact that TPN-fed animals and patients undergoing skin grafting or solid organ transplantation have better graft s u r v i v a l . 13 In addition, Freeman et al. ~4 demonstrated that the risk of coagulase nega- tive staphylococcal bacteremia in neonates could be attributed to the administration of lipid emulsions (feeding with lipid increased the prevalence by six times).
It is important to note that the gut regulates the absorption of trace elements. When the gut is bypassed and trace elements given parenterally, there may be no effective way to increase their excretion. Excessive tissue deposition of iron has been demonstrated in children on long-term TPN.15 Other complica- tions of TPN that continue to warrant attention include TPN- induced steatosis 16 and cholecystitis.
CLINICAL OBSERVATIONS
In addition to the array of detrimental effects associated with TPN, there has been a steady accumulation of clinical trials comparing total enteral nutrition (TEN) with TPN. In general, these demonstrate better outcomes in enterally fed pa- tients although the case mix of patients studied has been rather limited (Table I) . Even if, as has been suggested, apparent improvements in outcome are due to the avoidance of the harm- ful effects of TPN rather than any benefits associated with TEN, 17 these tl'ials still suggest that TPN is best avoided when- ever it is possible to feed an individual via the enteral route. The methodology of some of these studies also has been criticized because they were not blinded, is but it is difficult to imagine a practical protocol that would avoid this weakness. In an analy- sis of the effects of TPN alone, the multicenter, Veterans Affairs TPN Co-operative Study Group, was able to demonstrate that preoperative TPN (in elective surgical patients) was associated with an increase in postoperative infectious complications. Ben- eficial effects only were seen in patients who were malnour- ished severely, 19 but because none of the groups studied were critically ill, it is difficult to transpose these results to patients requiring intensive care. Nevertheless, these clinical trials taken in conjunction with the possible benefits of early enteral nutri- tion on gastric mucosal function and the known hazards of TPN make the enteral route the route of choice for the provision of nutrition in critically ill patients. Despite this considerable body of evidence, a recent survey found that only 74% of patients eligible to receive enteral nutrition in the ICU were started on enteral feeds. 2° There were a variety of reasons for this disappointing observation, not least the widespread misconcep- tion that bowel sounds taust be present before enteral feeding can be initiated, their absence indicating an adynamic bowel. In fact, it is known that the critically ill, and patients who have undergone laparotomy often have normal small intestinal motility in association with gastric and colonic paresis. In these patients, it is hardly surprising that bowel sounds are absent because any noise requires the presence of gas in the gut; if the stomach is not contracting and transferring gas into the duodenum, then the small intestine contracts silently. 2l In our experience, 80-90% of critically ill patients tolerate some en-

60S NUTRITIONAL SUPPORT IN THE CRITICALLY ILL
TABLE I.
RESULTS OF CLINICAL STUDIES COMPARING TEN WITH TPN
Studies Results
Adams et al. (1986)3»; 46 trauma patients randomized to receive either TPN or TEN (via a jejunostomy). No significant difference in age (TPN: 29 _+ 10 y; TEN: 30 +_ 9. y)
Moore Jones et al. (1989)36; 63 patients with major abdominal trauma randomized to a control or enterally fed group, via a needle catheter jejunostomy (control: 29.3 ___ 2.1 y; TEN: 30.5 _+ 2.2 y).
Moore et al37; meta-analysis of 8 trials in 1992 comparing TEN with TPN in high-risk surgical patients with trauma and nontranmatic condiüons (TEN: 41.0 _+ 1.5 y; TPN: 41.8 ___ 1.5 y).
Kudsk et al. (1992)38; 96 trauma patients randomized to TPN or enteral nutrition (TPN: 30.6 _+ 1.4 y; TEN: 30.4 ___ 1.7 y).
Wicks et al. (1994)2s; 24 patients undergoing prirna~ orthotopic liver transplantation randomized to either enteral feed or TPN (rnean age 46 y; range 16-62 y).
Early postoperative jejunostomy feeding is as safe and efficacious as TPN with comparable complication rates
Reduced septic complications in TEN group. Early enteral nutrition well-tolerated in severely injured
High-risk postoperaüve surgical paüents will tolerate early TEN. These patients have reduced morbidity rates compared with those paüents administered TPN
Significantly lower incidence of septic morbidity in patients fed enterally after blunt and penetrating abdominal trauma
Enteral feeding after liver transplantation is practical, efficacious, and less expensive than TPN
TEN, total enteral nutrition; TPN, total parenteral nutrition.
teral feed in the first few days of admission regardless of whether bowel sounds are present or not. 22 It also is thought erroneously that certain types of abdominal surgery, e.g., bowel resections, are relative contraindications to enteral feeding but there is no evidence to suggest that this is the case. 23 There are, however, real problems related to gastrointestinal dysfunction, especially gastric paresis, that present an obstacle to successful enteral feeding. However, gastric stasis often can be overcome by perseverance and the judicious use of prokineüc agents, z4 Beale et al.22 observed that most ICU patients could be red enterally. During a 12-mo period, the enteral route was used in all patients who required nutrition. Enteral nutrition only was stopped and TPN prescribed if the volume of aspirate exceeded the feed despite a 12-h rest period and prokinetic agents. With this approach, the proportion of patients receiving enteral nutrition alone increased significantly from 48% in the first 4 mo to 91% in the last 4 mo (P < 0.01). 22 Occasionally for reasons of comfort or anatomy, certain patients are unable to tolerate eren a fine nasogastric tube. Fortunately there are a variety of other routes by which enteral nutrition can be pro- vided (Table II) . It is important to note that there are various biological reasons that favor the intragastric route for enteral feeding, e.g., gastric acid secretion, which is the principal bacte- ricidal mechanism of the stomach, is diminished when nutrition is delivered to the duodenum. 25
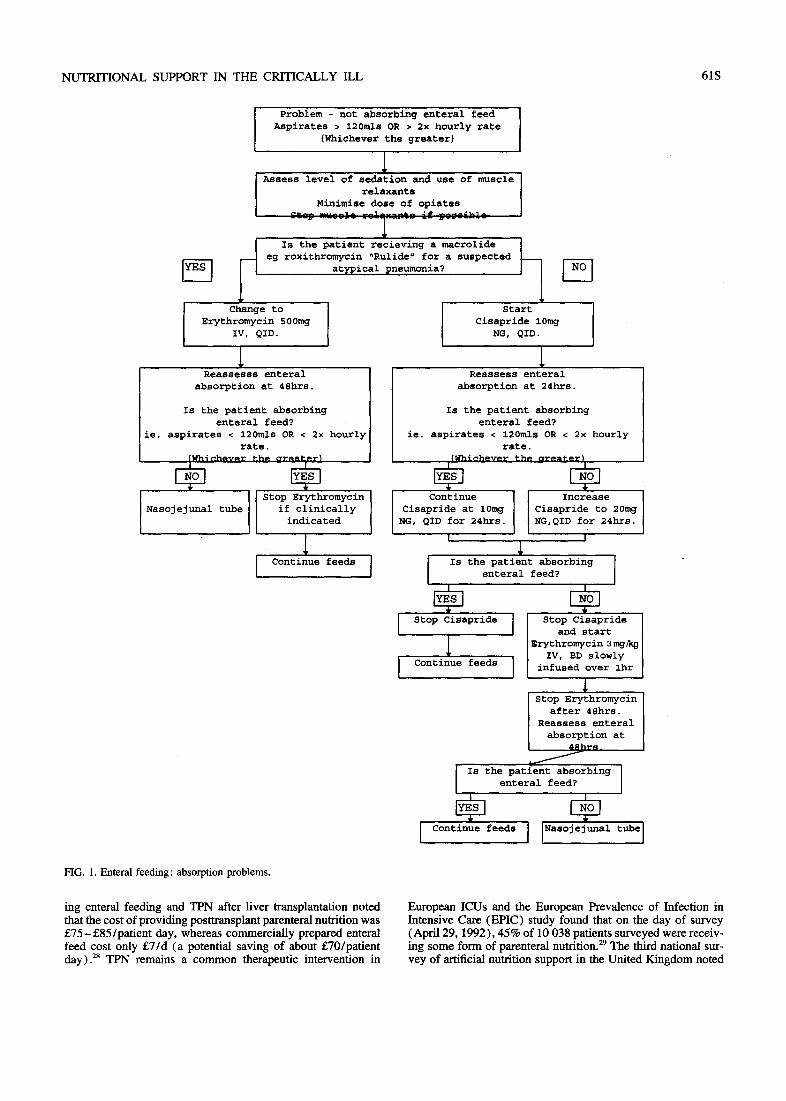
It has been suggested that TPN and enteral nutrition could be used together to provide nutritional support, the TPN being withdrawn once successful enteral nutrition is established. A1- though this approach might be used on a general ward, it has inherent dangers in the ICU. First, it exposes the critically ill patient unnecessarily to the adverse effects of TPN. Second, it introduces the potential for a less rigorous pursuit of successful enteral feeding, attending staff being lulled into a false sense of security. In our view, there are few indications for the combi- nation of TPN and enteral nutrition in the ICU. We have pro- duced a management algorithm that incorporates the use of prokinetic agents and where necessary a nasojejunal tube to overcome absorpüon problems in enterally fed patients (Fig. 1 ) .26 This has allowed us to feed the majority of our patients
enteraUy. There is no doubt that perceived problems regarding access to the gastrointestinal tract and the establishment of enteral feeding are surmountable.
ECONOMIC CONSIDERATIONS
Cost benefit analysis, parücularly the allocation of costs in dollars to intangible effects associated with nutritional sup- p o r t - f o r example, the suffering associated with a day of nau- sea or abdominal bloating in the ICU, applied at the bedside of an individual patient, remains an anathema to most physi- cians and rightly so! However, in these days of scarce resources, a knowledge of the cost effectiveness of various interventions is a reasonable expectation of pracücing clinicians so as to allow appropriate forward planning in the implementation of the necessary budgetary restrictions. When considering nutri- tional support, it has become clear that feeding by the enteral route is more cost effective than TPN. 27 A recent study compar-
TABLE II.
ROUTES OF ACCESS FOR DELIVERY OF ENTERAL NUTR1TION
Route Methods of placement
Nasoenteric Via nasopharynx or at laparotomy Nasogastric Nasoduodenal/jejunal
Enterocutaneous Percutaneous endoscopic
gastroscopy Percutaneous endoscopic
jejunoscopy Feeding gastroscopy
jejunostomy
Endoscopy, image intensification blind techniques at the time of laparotomy
Endoscopic placement through anterior abdominal wall
Placement of feeding tube as above beyond the pylorus
Open surgical procedure or via the laparoscope
NUTRITIONAL SUPPORT IN THE CRITICALLY ILL 61S
I Problem - not absorbing enteral feed Aspirates > 120mls OR > 2x hourly rate
(Whichever the greater)
Assess level of sedation and use of muscle relaxants
Minimise dose of opiates . . . . . . ' k l
¢
eg roxithromycin "Rulide" for a suspected atypical pneumonia ?
I Change to Start Erythromycin 500mg Cisapride 10mg
IV, QID. NG, QID.
absorption at 48hrs. absorption at 24hrs.
Is the patient absorbing Is the patient absorbing enteral feed? enteral feed?
le. aspirates < 120mls OR < 2x hourly ie. aspirates < i20mls OR < 2x hourly rate. rate.
(Wh~c.heve.r the_ crre.ate.r~ tWhlch~ve.r the. clre.ate.r~
Nasojejunal tube if clinically Cisapride at 10mg Cisapride to 20mg indicated NG, QID for 24hrs. NG,QID for 24hrs.
l ' ~ '
I StOp Cisapride [ Stop Cisapride and start
I Erythromycin 3rag~g IV, BD slowly
I Continue feeds I infused over ihr
Stop Erythromycin after 48hrs.
Reassess enteral absorption at
48hr~_ /
I Is the patient absorbing enteral feed?
tube I
FIG. 1. Enteral feeding: absorption problems.
ing enteral feeding and TPN after liver transplantaüon noted that the cost of providing posttransplant parenteral nutriüon was £75-£85/pat ient day, whereas commercially prepared enteral feed cost only £7/d (a potenüal saving of about £70/patient day). 28 TPN remains a common therapeufic intervention in
European ICUs and the European Prevalence of Infecäon in Intensive Care (EPIC) study found that on the day of survey (April 29, 1992), 45% of 10 038 paüents surveyed were receiv- ing some form of parcnteral nutrition. 29 The third national sur- vey of arüficial nutrition support in the United Kingdom noted

62S NUTRITIONAL SUPPORT IN THE CRITICALLY ILL
that in 1993, some 62 997 days of TPN were administered in hospitals, 3° (this figure probably being considerably higher because it was derived from incomplete data). It is not difficult to see how TPN can have an enormous impact on health care budgets. Using data from the Department of Veterans Affairs Cooperative Trial of perioperative TPN, Eisenberg et al. 31 ad- dressed the quesUon of whether TPN used in this way saved money in any subgroup of patients, particularly those who were malnourished. They concluded that perioperative TPN did not result in decreased costs for any subgroup of patients re-empha- sizing the present view that the indicafions for TPN are specific and limited to a small group of malnourished patients who are unable to absorb nutrients from their gastrointestinal traets. Given the cost implications of TPN, it is disappointing that it continues to be prescribed so frequently when enteral nutrition would be more appropriate. In a retrospective study of 31 pa- tieres receiving artificial nutritional support, a nutfition support team (NST) identified 12 patients for whom TPN had been prescribed and in whom enteral feeding would have been more appropriate. 32
Apart from ensuring the appropriate use of TPN or indeed any sott of nutritional support that often may be used inappro- priately in the hospital setüng, e.g., in the treatment of any patient with severe irreversible disease, it has been suggested that NSTs provide cost containment in a variety of other ways. 33 The early recognition of oveffeeding can have significant cost
implications. Foster et a l . 34 measured energy expenditure in 100 parenteraUy fed patients whose calorific intake was based on predictive equations. They found that an "average 1076 ___ 660 kcal /d in excess of the measured energy expenditure was being administered to these patients. It was suggested that the cost of TPN could be cut by 22% by using metabolic cart studies routinely. 34 Given the apparent benefits of a dedicated NST, it is disappointing to note that in the United Kingdom, the per- centage of ICUs with access to such teams had only increased from 32% in 1991 to 37.3% in 1994. 30 Unfortunately budget holders in the United Kingdom still perceive NSTs as cost generating despite evidence to the contrary and clinicians con- tinue to dislike the idea of a distinct specialist team "interfer- ing" in patient management.
Finatly, although it is clear that enteral feeding involves lower staff and material costs than TPN, it is true to say that on occasion, the need to consult gastroenterologists and radiolo- gists to obtain access to the gastrointestinal tract beyond the pylorus can increase patient management costs. However, it has been suggested that the cost savings achieved by abändon- ing TPN in whomever possible may allow intensive care staff to purchase endoscopes and develop the necessary skills to access the gastrointestinal tract thereby negating the need for recourse to other specialties. 13 In any event, there are many good physiological and economic reasons why the enteral route is the preferred method of delivering nutritional support.
REFERENCES
1. Kortez RL. Nutritional supplementation in the ICU. How critical is nutrition for the criticaUy ill? Am J Respir Crit Care Med 1995; 151:570
2. Soeters PB, Steven WM, Damink O. Nutritional considerations in the critically ill. Curr Opin Crit Care 1996;2:153
3. Baue AE. The role of the gut in the development of multiple organ dysfunction in cardiothoracic patents. Ann Thorac Surg 1993; 55:822
4. Goodlad RA, Plumb JA, Wright NA. Epithelial cell proliferation and intestinal absorptive function during starvation and refeeding in the rat. Clin Sci 1988;74:301
5. Guedon C, Schmitz J, Lerebours E, et al. Decreased brush border hydrolase activities without gross morphologic changes in human intestinal mucosa after prolonged total'parenteral nutrition of adults. Gastroenterology 1986;90:373
6. Rossi TM, Lee PC, Young C, Ijota A. Small intesfinal mucosa changes, including epithelial cell proliferafive activity, of children receiving total parenteral nutrition (TPN). Dig Dis Sci 1993; 38:1608
7. Illig KA, Ryan CK, Hardy DJ, Rhode J, Locke W, Sax HC. Total parenteral nutrition-induced changes in gut mucosal function: atro- phy alone is not the issue. Surgery 1992; 112:631
8. Purcell PN, Davis K, Branson RD, Johnson DJ. Continuous duode- nal feeding restores got blood flow and increases gut oxygen utilisa- tion during PEEP ventilation for lung injury. Am J Surg 1993; 165:188
9. Mughal MM. Complications of intravenous feeding catheters. Br J Surg 1989;76:145
10. Seidner DL, Masioli EA, Istfan NW, et al. Effects of long chain triglyceride emulsions on reticuloendothelial system function in humans. JPEN 1989; 13:614
11. Robin AP, Arain I, Phuangsab A, Holian O, Roccaforte P, Barret JA. Inla-avenous fat emulsion acutely suppresses neutrophil cherni- luminescence. JPEN 1989; 13:608
12. Gogos CA, Kalfarentzos FE, Zoumbos NC. Effect of different types of TPN on T lymphocyte subpopulations and NK cells. Am J Clin Nutr I990;51:119
13. Atkinson S, Bihari D. Enteral nutrition in intensive care: no more "gastrointestinal neglect." Curr Med Lit Anaesthesiol 1994; 8:3
14. Freeman J, Goldmann DA, Smith NE, Sidebottom DG, Epstein MF,
Platt R. Association of intravenous lipid emulsion and coagulase- negative staphylococcal bacteremia in neonatal intensive care units. N Engl J Med 1990;23:301
15. Hariz MB, Goulet D, De Potter S, Girot R, Ramboud C, Colomb V. Iron overload in children receiving prolonged parenteral nutrition. J Paediatr 1993; 123:238
16. Braxton C, Lowry SF. Parenteral nutrition and liver dysfunction, new insight? JPEN 1995; 19:3
17. Alpers DH, Stenson WF. Does total parenteral nutrition-induced intestinal mucosal atrophy occur in humans and can it be affected by enteral supplements? Curr Opin Gastroenterol t996; 12:169
l 8. Heyland DK, Cook D J, Guyatt GY. Enteral nutrition in the critically ill patient. A critical review of the evidence. Intensive Care Med. 1993; 19:435
19. The Veterans Affairs Total Parenteral Nutrition Cooperative Study Group. Perioperative total parenteral nutrition in surgical patients. N Engl J Med 1991;325:525
20. Heyland D, Cook DJ, Winder B, Brylowski L, Van de Monk H, Guyatt G. Enteral nutrition in the cfitically ill patient: a prospective survey. Crit Care Med 1993;23:1055
21. Catchpole BN. Smooth muscle and the surgeon. Aust NZ J Surg 1988;59:199
22. Beale RJ, Maynard N, Smithies MN. Changing nutritional therapy in a general ICU. Intensive Care Med 1992; 18(suppl 2):S104
23. Comelia S, Carr KD, Ling E, Boulos P, Singer M. Randomised trial of safety and efficacy of immediate postoperative enteral feeding in patients undergoing gastrointestinal resection. Br Med J 1996; 312:869
24. Dive A, Miesse C, Galanti L, et al. Effect of erythromycin on gastric motility in mechanically ventilated critically ill patients. A double blind, randomised, placebo controlled study. Crit Care Med 1995;23:1356
25. Layan A J, Orlando FG, Day AL, Kilroy RA, James PB, McGui- gan JE. The effect of duodenojejunal alimentation on gastric pH and hormones in intensive care unit patients. Chest t991; 99:695
26. Frost P, Edwards N, Bihari D. Gastric emptying in the critically il l--the way forward? Intensive Care Med 1997;23:243.
27. Twomey PL, Patching SC. Cost effectiveness of nutritional support. JPEN 1984;9:3

N U T R I T I O N A L SUPPORT IN THE CRITICALLY 1LL 63S
28. Wicks C, Somasundaram S, Bjavnason I, et al. Comparison of enteral feeding and total parenteral nutrition after liver transplanta- tion. Lancet 1994;344:837
29. Vincent JL, Bihari D J, Suter PM, et al. The prevalence of nosoco- mial infection in intensive care units in Europe. Results of the European Prevalence of Infection in Intensive Care (EPIC) study. JAMA 1995;274:639
30. Payne-James JJ, DeGava CJ, Grimble GK, Silk DBA. Artificial nutrition support in hospitals in the United Kingdom 1994. Third Naüonal Survey. Clin Nutr 1995; 14:329
31. Eisenberg JM, Slick HA, Buzby GP, Bruce K, Williford WD. Does perioperative total parenteral nutrition reduce medical care costs? JPEN 1993; 17:201
32. O'Brien DD, Hodges RE, Day AT, Waxman KS, Rebello T. Rec- ommendations of nutrition support team promote cost containment. JPEN 1985; 10:300
33. Roberts M F Levine GM. Nutrition support team recommendations can reduce hospital costs. Nutr Clin Pract 1992;7:227
34. Foster GD, Know LS, Dempsey DT, Mullen JL. Caloric require- ments in total parenteral nutrition. J Am Coll Nutr 1987;6:231
35. Adams S, Dellinger EP, Wertz J, Oreskovich MR, Simonowitz D, Johansen, K. Enteral versus parenteral nutritional support following laparotomy for t rauma--a prospective randomised study. J Trauma 1986;26:874
36. Moore EE, Jones TN. Benefits of immediate jejunostomy feeding after major abdominal t rauma--a prospective randomised study. J Trauma 1989;26:874
37. Moore FA, Feliciano DV, Andrassy RJ, et al. Early enteral feeding, compared with parenteral reduces postoperative septic complica- tions. The results of a meta-analysis. Ann Surg 1992;216:177
38. Kudsk, KAS, Croce MA, Fabian TA, et al. Enteral versus parenteral feeding effects on septic morbidity after blunt and penetrating ab- dominal trauma. Ann Surg 1992;215:503