Embed Size (px)
Citation preview


11
The children most at risk of missing out onthe Millennium agenda, and on their rightsunder the Convention on the Rights of theChild, live in all countries, societies andcommunities. An excluded child is one wholives in an urban slum in Venezuela andtakes care of her four siblings; a Cambodiangirl living alone with her brothers becauseher mother had to go elsewhere to find ajob; a Jordanian teenager working to helphis family and unable to play with hisfriends; an orphan in Botswana who lost hismother to AIDS; a child confined to awheelchair and unable to attend school inUzbekistan; or a young boy working as adomestic in Nepal.
At first glance, these children’s lives mayappear poles apart: Each of them faces adifferent set of circumstances and strugglesto overcome distinct obstacles. Yet they allhave something in common: They arealmost certainly excluded from essentialgoods and services – vaccines, micronutri-ents, schools, health-care facilities, waterand sanitation, among others – and deniedthe protection from exploitation, violence,abuse and neglect, and the ability to partici-pate fully in society, which is their right.
Exclusion harms children on many levels
At the national level, the exclusion of chil-dren from their rights to essential services isoften the product of macro factors, such asmass poverty, weak governance, the uncon-tained spread of major diseases such asHIV/AIDS, and armed conflict. At the sub-national level, among vulnerable and mar-ginalized groups, exclusion is also the resultof disparities in access to services on thebasis of income and geographic location,and through overt discrimination on thegrounds of gender, ethnicity or disability.
Violations of protection rights – includingthe loss or lack of a formal identity, the©
UN
ICE
F/H
Q99
-080
8/ R
oger
LeM
oyne
The Root Causes of Exclusion
ISSUE: Exclusion acts against children in all countries, societies andcommunities. At the national level, the root causes of exclusion arepoverty, weak governance, armed conflict and HIV/AIDS. Statisticalanalyses of key MDG indicators related to child health and educa-tion show a widening gap between children growing up in countrieswith the lowest level of development, torn by strife, underserved byweak governments or ravaged by HIV/AIDS and their peers in therest of the developing world. These factors not only jeopardizethese children’s chances of benefiting from the Millennium agenda,they also increase the risk that they will miss out on their childhoodand face continued exclusion in adulthood.
Because the MDGs are based on national averages, inequalitiesamong children within the same country that contribute to, andresult in, their exclusion may be obscured. Disaggregated data fromnational statistics and household surveys indicate sharp disparitiesin health-care and education outcomes on the basis of householdincome and geographic location. Inequalities in children’s health,rate of survival and school attendance and completion also fallalong the lines of gender, ethnicity or disability. These inequitiesmay occur because children and their caregivers are directly excluded from services, because they live in areas that are poorerand more poorly serviced, because of the high costs of access toessential services, or because of cultural barriers such as language,ethnic discrimination or stigmatization.
ACTION: Tackling these factors requires swift and decisive action in four key areas:
• Poverty and inequality. Adjusting poverty-reduction strategies and expanding budgets or reallocating resources to social invest-ment will assist millions of children in the poorest countries and communities.
• Armed conflict and ‘fragile’ States. The international communitymust seek to prevent and resolve armed conflict and engage withcountries with weak policy/institutional framework to protect children and women and provide essential services. Emergencyresponses for children caught up in conflict should include services for education, child protection and the prevention of HIV transmission.
• HIV/AIDS and children. Greater attention should be given to theimpact of HIV/AIDS on children and adolescents and to ways of protecting them from both infection and exclusion. The GlobalCampaign on Children and HIV/AIDS will play a significant role inthis regard.
• Discrimination. Governments and societies must openly confrontdiscrimination, introduce and enforce legislation prohibiting it,and implement initiatives to address exclusion faced by womenand girls, ethnic and indigenous groups and the disabled.
2T H E S TAT E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 6
SUMMARY

12 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 6
absence of state protection for childrendeprived of family support, the exploitationof children and premature entry into adultroles – also leave individual childrenexposed to exclusion.
This chapter focuses on the factors thatcause children to be excluded from essentialservices – mostly of health care and educa-tion – at the national and subnational levels.These impediments, often long-standing anddeeply entrenched, are the product of eco-nomic, social, gender and cultural processesthat can be addressed and must be altered.Even if they persist, our binding commit-ments to children compel us to take the nec-essary actions to mitigate their impact. (Themany factors that deprive children of pro-tection against violations of their rights atthe individual level, which lessens their visi-bility in their societies and communities,will be examined in Chapter 3).
Macro-level causes of exclusion
Poverty, armed conflict and HIV/AIDS areamong the greatest threats to childhoodtoday.1 They are also among the most significant obstacles to the achievement ofthe Millennium agenda for children at theregional and country levels. Statistical analy-ses of key MDG indicators related to child
health and education – under-five mortality,malnutrition, primary school enrolment,among others – show a widening gap in thehealth and education of children growing upin countries with the lowest level of develop-ment, torn by strife or ravaged by HIV/AIDS,compared with their peers in the rest of theworld. Without a concerted effort, childrenin these countries will become even moreexcluded over the next decade.
Children in the least developed countries
are most at risk of missing out
Children are disproportionately representedamong the poor, since the least developedcountries tend to have the youngest popula-tions, and income-poor families tend to havemore children than richer ones. Poor childrenare more likely to be engaged in labour,which could mean missing out on an educa-tion and, as a result, on the opportunity togenerate a decent income that would allowthem to escape poverty in the future.2 Denieda decent standard of living and, often, educa-tion, information and vital life skills, they arevulnerable to abuse and exploitation.
Poverty reduction is a central objective of theMillennium agenda, targeted explicitly in twoof the eight goals (MDG 1 and MDG 8), anda significant factor in the other six. In MDG 1,the primary aim is to reduce income povertyby cutting in half the proportion of peopleliving on less than a dollar a day; in MDG 8,a key objective is to address the special needsof the least developed countries.
Raising incomes through economic growthis an essential component of poverty-reduction strategies and has been partic-ularly successful in Asia since 1990.3 Buteconomic growth by itself is insufficient toaddress the ways in which children experi-ence material poverty – i.e., as deprivationof essential services and goods. The extentof this deprivation is appalling: More than 1 billion children suffer from one or moreextreme forms of deprivation in adequatenutrition, safe drinking water, decent sanita-tion facilities, health-care services, shelter,education and information.4
Children living in the least developed countries are the most likely to face severe
Industrializedcountries
0 10 20 30 40 50
Developingcountries
Leastdeveloped
countries
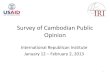
21%
6%
37%
11%
49%
16%
Under 18 population as a % of total population (2004)
Under 5 population as a % of total population (2004)
Percentage
Figure 2.1: The least developed countries are the
richest in children
Source: UNICEF calculations based on data from United Nations Population Division.

T H E R O O T C A U S E S O F E X C L U S I O N 13
Why children in the least developed countries risk missing out
Least developed Developing
countries countries World
Survival
Under-five mortality rate (per 1,000 live births, 2004) 155 87 79Infant mortality rate (per 1,000 live births, 2004) 98 59 54
Nutrition
Proportion of under-fives who are moderately or severely underweight (percentage, 1996-2004a) 36 27 26
Proportion of under-fives suffering from moderate or severe stunting (percentage, 1996-2004a) 42 31 31
Immunization
Proportion of one-year-old children immunized against DPT3 (percentage, 2004) 75 76 78
Proportion of one-year-old children immunized against HepB3 (percentage, 2004) 28 46 49
Health care
Proportion of under-fives with an acute respiratory infectiontaken to a health provider (percentage, 1998-2004a) 38 54b 54b
Proportion of under-fives with diarrhoea receiving oral rehydration and continued feeding (1996-2004a) 36 33b 33b
HIV/AIDS
Adult prevalence rate (15-49 years, end-2003) 3.2 1.2 1.1Adults and children living with HIV (0-49, thousands, 2003) 12,000 34,900 37,800
Education and gender parity
Percentage of primary school entrants reaching grade 5 (administrative data, 2000-2004a) 65 78 79
Net primary school attendance ratio, boys (1996-2004a) 60 76 76Net primary school attendance ratio, girls (1996-2004a) 55 72 72Net secondary school attendance ratio, boys (1996-2004a) 21 40b 40b
Net secondary school attendance ratio, girls (1996-2004a) 19 37b 37b
Demographics
Life expectancy at birth (years, 2004) 52 65 67Proportion of population urbanized (percentage, 2004) 27 43 49
Women
Adult literacy parity rate (females as a percentage of males, 2000-2004a) 71 84 86Antenatal care coverage (percentage, 1996-2004a) 59 71 71Skilled attendant at delivery (percentage, 1996-2004a) 35 59 63Lifetime risk of maternal death, 2000 (1 in:) 17 61 74
a Data refer to the most recent year available during the period specified. b Excludes China. Sources: For a complete list of the sources used to compile this table, see Statistical Tables 1-10, pp. 95-137.

14 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 6
deprivation and, consequently, are amongthose at greatest risk of missing out on theMillennium agenda. The statistical evidenceof their impoverishment is alarming, partic-ularly those indicators related to childrenand women’s development and well-being(see Panel: Why children in the least devel-oped countries risk missing out, page 13). In almost all cases, the least developedcountries are lagging far behind the rest of the developing world.
Two MDG indicators – under-five mortalityand completion of primary education –aptly illustrate the risks of exclusion facedby children living in the least developedcountries. In 2004, 4.3 million children –one out of every six live births – died beforethe age of five in these countries alone.5Although under-fives in the least developedcountries make up only 19 per cent of theworld’s under-fives, they account for over40 per cent of all under-five deaths. Ofthose who live to reach primary school age,40 per cent of boys and 45 per cent of girlswill not attend school. Of those who enterprimary school, over one third will notreach grade five; and around 80 per cent of all children of secondary school age willnot attend secondary school.6
Armed conflict and poor governance
escalate the risk of exclusion for children
Armed conflict causes children to miss outon their childhood in a multitude of ways.Children recruited as soldiers are deniededucation and protection, and are oftenunable to access essential health-care services. Those who are displaced,refugees or separated from their familiesface similar deprivations. Conflict height-ens the risk of children being exposed toabuse, violence and exploitation – withsexual violence often employed as aweapon of war.7 Even those children whoare able to remain with their families, intheir own homes, may face a greater riskof exclusion because of the destruction ofphysical infrastructure, strains on health-care and education systems, workers andsupplies, and increasing personal insecuritycaused by the conflict or its remnants –such as landmines and unexploded ordnance.
Chad
Rwanda
Guinea-Bissau
Equatorial Guinea
Mali
Somalia
Liberia
Afghanistan
Niger
Angola
Sierra Leone
0 50 100 150 200 250 300
Dem. Rep. of Congo
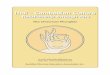
No armed conflict Major armed conflict
200
203
203
204
205
219
225
235
257
259
260
283
Under-five deaths per 1,000 live births
Figure 2.3: Most of the countries where 1 in 5
children die before five have experienced
major armed conflict since 1999
Sources: Data on child mortality: UNICEF, United Nations Population Division and UnitedNations Statistics Division; Data on major armed conflicts: Stockholm International PeaceResearch Institute, SIPRI Yearbook 2005.
Net secondary schoolenrolment ratio,
girls (2000-2004*)
0 20 40 60 80 100
9249**
26
Least developedcountries
Developingcountries
9150**
30
9683
65
9588
71
Net secondary schoolenrolment ratio,
boys (2000-2004*)
Net primary schoolenrolment ratio,
girls (2000-2004*)
Net primary schoolenrolment ratio,
boys (2000-2004*)
Industrializedcountries
Percentage
Figure 2.2: Children living in the poorest countries
are most at risk of missing out on
primary and secondary school
*Data refer to the most recent year available during the period specified.** Excludes China.Sources: Demographic and Health Surveys (DHS) and Multiple Indicator Cluster Surveys (MICS).

T H E R O O T C A U S E S O F E X C L U S I O N 15
Firm evidence of the impact of armed con-flict on children’s exclusion is limited, inpart because of gaps in research and datacollection on the numbers of childrencaught up in conflict. Nevertheless, theavailable linkages are indicative of theextent of exclusion – and alarming. Of the12 countries where 20 per cent or more ofchildren die before the age of five, nine havesuffered a major armed conflict in the pastfive years (see Figure 2.3: Most of the coun-tries where 1 in 5 children die before fivehave experienced major armed conflict since1999, page 14), and 11 of the 20 countrieswith the most elevated rates of under-fivemortality have experienced major armedconflict since 1990. Armed conflict also hasdevastating effects on primary school enrol-ment and attendance. For example, the nineconflict-affected countries where 1 in 5 chil-dren dies before the age of five have anaverage net primary school attendance ratioof 51 per cent for boys and 44 per cent forgirls, well below the corresponding averagesof 60 and 55, respectively, for the leastdeveloped countries as a whole.8
The breakdown in governance that oftenaccompanies armed conflict and the destruc-tion caused to public administration andinfrastructure are key reasons for the highrates of under-five mortality and low ratesof educational participation and attainment.But armed conflict is not the only form ofstate failure. ‘Fragile’ States are character-ized by weak institutions with high levels ofcorruption, political instability and weakrule of law.9 Such States often lack theresources to adequately support an efficientpublic administration.10 As the governmentis often incapable of providing basic servicesto its citizens, the standard of living in thesecountries can degenerate both chronicallyand acutely.
Tragically, these governance failures result inchildren becoming more excluded fromessential services. Children living in coun-tries that are unable to implement nationaldevelopment strategies to meet the MDGswill be among those most at risk of missingout on whatever benefits are derived fromthe Millennium agenda. One such country isHaiti, already the poorest country in theAmericas by most indicators and plagued by
political violence for most of its recent his-tory. The country has seen a further deterio-ration in child well-being amid the politicalturmoil of the last two years. Access to edu-cation has been affected by hikes in schoolfees, and some 60 per cent of rural house-holds still suffer from chronic food insecuri-ty, with 20 per cent extremely vulnerable.
Another example of a fragile State isSomalia, a country that has long beenamong the least developed. Its progress on human development has been furtherconstrained by the lack of a functioningnational administration since 1991. Overthis 14-year period, progress on humandevelopment has been scant, with rival warring factions claiming jurisdiction overspecific territories. The result is starklyapparent in education: The net primaryattendance ratio is lower than anywhere else in the world, at just 12 per cent forboys and 10 per cent for girls, according to the latest estimates.11 The recent re-establishment of schooling by many
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
‘Fragile’States*
5123451,524
32,232
Leastdevelopedcountries
Developingcountries
Industrializedcountries
Gro
ss n
atio
nal
inco
me
per
cap
ita
(US
$, 2
004)
Figure 2.4: ‘Fragile’ States* are among the poorest
* Countries with weak policy/institutional frameworks. A list can be found in theReferences section, p. 91.
Sources: World Bank, 2004 Country Policy and Institutional Assessment (CPIA), OverallRating, Fourth and Fifth Quintiles; and World Development Indicators 2005.

16 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 6
communities – with the support of interna-tional agencies – is a welcome development,but years of underinvestment have leftSomalia lagging behind the rest of the developing world in education.
Strengthening governance in fragile States isconsidered by many, and with good justifi-cation, to be a prerequisite for meeting thegoals of the Millennium agenda. Donorsand international agencies may be wary ofincreasing non-humanitarian assistance tothe government of a fragile State, but theircommitments to children must compel themto engage with these States to ensure thatchildren’s rights are protected and theirneeds met. The simple truth is that childrencannot wait until governance improves –long delays may result in them missing outon their childhood altogether.
HIV/AIDS is wreaking havoc with
children’s lives in the worst-affected
countries
Combating HIV/AIDS is a central objectiveof the Millennium Development Goals,specifically addressed in MDG 6. Children
living with or affected by HIV/AIDS, or incountries with high prevalence rates, face anextremely high risk of exclusion from accessto essential services, care and protection, asparents, teachers, health workers and otherbasic service providers fall sick and eventu-ally die. The epidemic is tearing away at thesocial, cultural and economic fabric of fami-lies, the first line of protection and provisionfor children that safeguards against theirexclusion from essential services and expo-sure to harm. Some 15 million children havealready lost one or more parents to the dis-ease, and millions more have been madevulnerable as the virus exacerbates otherchallenges to the health and development of families, communities, provinces and, in the worst-affected countries, wholenations.12 Of those orphaned by AIDS, 12.1 million, or more than 80 per cent, arein sub-Saharan Africa, reflecting not onlythe region’s disproportionate burden of HIV infection, but also the epidemic’s relative maturity.13
The protracted illness and eventual death of parents and other caregivers exert enor-mous pressures on children, who often haveto assume adult roles in treatment, care andsupport. Surviving siblings can suffer stigmaand discrimination in their communities andsocieties, experience greater exposure to violence, abuse and exploitation and dropout of school for a variety of reasons.
In addition to orphaning and the loss ofcaregivers, lack of access to essential ser-vices and increased risk of missing out onan education, HIV/AIDS also threatens thevery survival of children and young people.Every day, nearly 1,800 children under 15are infected.14 Children under 15 accountfor 13 per cent of new global HIV infectionsand 17 per cent of HIV/AIDS deaths annu-ally.15 The pandemic has reversed the gainsin child survival made in many of the worst-affected countries and has dramaticallyreduced average life expectancy in thosecountries, particularly in southern Africa.16
With the pandemic spreading to more andmore countries and population groups, theworst impact on children is still to come. Itis estimated that in 2004, almost 5 millionpeople became infected with HIV – the most
Industrializedcountries
0 10 20 30 40 50 60 70 80 90 100
CEE/CIS
Eastern andSouthern Africa
Latin Americaand Caribbean
East Asia andPacific
South Asia
Middle East andNorth Africa
West andCentral Africa
Women (15-49) Men (15-49) Children (0-14)
26 73 1
34 66 1
38 60 2
27 72 2
30 67 3
45 51 4
53 39 8
53 40 7
Percentage of total population living with HIV, 2003*
Figure 2.5: Children account for an increasing
proportion of people living with HIV
*Figures may not add up to 100% due to rounding.
Source: UNICEF calculations based on data from Joint United Nations Programme onHIV/AIDS, Report on the Global HIV/AIDS Epidemic, 2004.

T H E R O O T C A U S E S O F E X C L U S I O N 17
in a single year since the pandemic began inthe early 1980s. Young people aged between15 and 24 years now account for nearly onethird of people living with HIV/AIDS glob-ally.17 Given that it can take up to a decadefor any decrease in HIV prevalence to betranslated into lower death rates from AIDS– owing in large part to the slow roll-out of antiretroviral treatments – deaths fromAIDS will continue and the number oforphans will rise. In those countries whereHIV/AIDS is already at epidemic levels,tackling the disease is imperative not only to meet MDG 6, but also to reverse recentincreases in under-five mortality rates – particularly in Eastern and Southern Africa– and to reduce the risk of exclusion fromeducation and the protection of a familyenvironment for orphans and other vulnerable children.
Subnational factors that can result
in exclusion
National aggregates fail to capture the full
picture of exclusion for children
Assessment of indicators related to children’swell-being is most frequently undertaken atthe national level. There are a number ofreasons for this: The national level is thefundamental unit of statistical analysis forcountries; estimates for national aggregatesare generally more widely available than forany sub-country group; standardization ofstatistics often requires national-level andnationally funded survey programmes; andinternational agencies also compile nationalaggregates on key indicators related to theMillennium agenda. The national govern-ment is also the signatory to internationalcommitments to children and the principaltrustee for their implementation.
However, assessing child well-being on thebasis of national aggregates alone has itslimitations. National averages are, bynature, summary measures that most clearlydepict the situation of the majority; as such,they do not provide a full picture. To gain amore complete understanding of the exclu-sion that some children face within a coun-try, disaggregated indicators derived fromnational statistics or household surveys arerequired. Data that are disaggregated geo-
graphically – as well as by gender, ethnicgroup or other salient dimensions – are keyto identifying the risk of exclusion and areimmensely useful as a tool for programmedesign. Disaggregated data are particularlyimportant for advocacy and policy purposesin countries where the national averagesmay indicate that, based on current trends,some or all of the MDGs will be met.
Disaggregated national statistics or house-hold surveys on children’s well-being are not available in all countries. But the exist-ing evidence, based on the Demographicand Health Surveys (DHS) and MultipleIndicator Cluster Surveys (MICS), is fairlycomprehensive and indicates a clear result:Within countries, there are usually signifi-cant disparities in child well-being anddevelopment across geographical and other axes.
These disparities reflect exclusion in relativeterms, quantifying a child’s well-being com-pared to that of his or her peers. A countrywith a high national average of primaryschool attendance or enrolment, for exam-ple, may still face wide internal variationsowing to the marginalization of particularsegments of the population. One such coun-
© U
NIC
EF/
HQ
02-0
255/
Thie
rry
Gee
nen

18 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 6
try is Venezuela, where survey data fromDHS and MICS indicate that although netprimary school attendance approaches 94per cent, almost 15 per cent of children ofprimary school age living in the poorest 20per cent of households miss out on primaryeducation, compared with less than 2 percent in the richest quintile.
One of the biggest risks for children is that,with the MDGs being based on nationalaverages, such inequalities within countriesmay be obscured. The magnitude of thesedisparities can be great, and they risk beingignored when MDG-based strategies arebeing developed and implemented. This isparticularly true in countries where themajority of children are afforded the mini-mum health-care and education thresholdsset out in the Millennium agenda. In suchsettings, the sharp divide between the mostprivileged children and those denied accessto essential services contributes to their further marginalization and may in itself be a root cause of discrimination.
Income inequalities threaten children’s
survival and development
In every developing country where disaggre-gated data by household income are avail-
able,18 children living in the poorest 20 percent of households are significantly morelikely to die before the age of five than thoseliving in the richest 20 per cent.
Latin America and the Caribbean is theregion with the highest inequalities inhousehold income in the developing world;countries in this region also have among thehighest inequalities in child mortality. Thecountry with the greatest inequality inunder-five mortality is Peru, where childrenliving in the poorest quintile are five timesmore likely to die before their fifth birthdaythan children from the wealthiest 20 percent of the population.
Though disparities in under-five mortalityrates are not as sharply pronounced in other regions, they can still be marked. On average, a child born into the poorest20 per cent of households is three timesmore likely to die than a child born into therichest quintile in East Asia and the Pacificregion, two and a half times more likely todie in the Middle East and North Africa andaround twice as likely in the South Asia andCEE/CIS regions. Although several of thecountries in these regions are either on trackor making good progress towards MDG 4,the poorest children are still twice as likely
© U
NIC
EF/
HQ
00-0
140/
She
hzad
Noo
rani

T H E R O O T C A U S E S O F E X C L U S I O N 19
to die before five as the richest children (see Panel: Income disparities and child survival, page 20).
Within countries, low income is a majordeterrent to primary school participation.Children of primary school age from thepoorest 20 per cent of households in devel-oping countries are 3.2 times more likely tobe out of primary school than those fromthe wealthiest 20 per cent. Moreover, 77 percent of children out of primary school comefrom the poorest 60 per cent of householdsin developing countries; this disparity iseven greater in Latin America and theCaribbean (84 per cent) and Eastern andSouthern Africa (80 per cent).19
Children living in rural areas and among
the urban poor often face a high risk of
exclusion
Rural areas tend to be poorer and more dif-ficult to reach with health-care services andeducation than urban areas. Accordingly, innearly all countries where household dataon child mortality rates are available, ruralchildren are more likely to die before theage of five than their urban peers. Some 30per cent of rural children in developing
countries are out of school, compared with18 per cent of those living in urban areas,and over 80 per cent of all children out ofprimary school live in rural areas. Possiblebarriers to their attendance include distance,the likelihood that their parents are less edu-cated or do not value formal education andthe failure of governments to attract goodteachers to the countryside.20
Geographic divides often overlap withincome inequality within urban communi-ties. In many of the world’s cities, the mostimpoverished citizens live in slums, tene-ments and shanty towns, areas which aregeographically separate from the most afflu-ent. More than 900 million people live inslums; most lack access to safe drinkingwater, improved sanitation facilities, sufficient living space and decent qualityhousing with secure tenure.21 The exclusionof children living in these communities –which are often severely lacking in essentialservices and state protection – can sometimes approach levels experienced in rural areas.22
Inequalities in children’s health, rate of sur-vival and school attendance and completionalso fall along the lines of gender, ethnicity
West andCentralAfrica
Eastern andSouthern
Africa
0
20
40
60
80
100Male
Female
South Asia World Middle East andNorth Africa
CEE/CIS East Asiaand thePacific
Latin Americaand the
Caribbean
Industrializedcountries
65 65
8075
8784
9084
90 8995 97 96 98 98 100
6155
Net
pri
mar
y sc
ho
ol a
tten
dan
cera
tio
, 199
6-20
04*
Figure 2.6: In several regions, girls are more likely to miss out on primary school than boys
*Data refer to the most recent year available during the period specified.
Source: United Nations Children’s Fund, Levels, Trends and Determinants of Primary School Participation and Gender Parity, Working Paper, 2005.

20 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 6
In 2004, an estimated 10.5 million chil-dren died before they reached agefive,a most from preventable diseases.Combating these unnecessary deathsand meeting Millennium DevelopmentGoal 4 – reduce child mortality by twothirds between 1990 and 2015 – will bea central focus for all those workingtowards the fulfilment of the promisesof the Millennium agenda for children.
Addressing the inequalities and disparities within countries must be an essential component of all pro-grammes and policies that aim toreduce child mortality.
In countries where household dataare available from surveys such as theDemographic and Health Surveys andthe Multiple Indicator Cluster Surveys,
it is clear that children living in thepoorest 20 per cent of households aresignificantly more likely to die duringchildhood than those living in therichest 20 per cent of the population.b
The least developed countries tend to have lower inequalities in child survival between rich and poor, withmortality rates remaining high even in the richest families. Countries in sub-Saharan Africa, for example, havelower levels of disparity in child mortality rates than less impoverisheddeveloping regions.
Income disparities often translate intodisparities in the nutritional status ofchildren. Over 5.5 million childrenunder five die every year from causes related to malnutrition.c
Encompassing more than just hunger,malnutrition can lead to weakenedimmune systems when vitamin A islacking and a child is neither hungrynor underweight. Even when it doesnot cause death, malnutrition caninflict lifelong damage on a child’shealth and development.
Vaccine-preventable diseases causemore than 2 million deaths everyyear, of which approximately 1.4 million occur in children under agefive.d While huge strides have beenmade worldwide to increase vaccina-tion coverage, there is still room forimprovement. Tragically, the poorestchildren are also at a disadvantagewhen it comes to immunization. The richest children are more thantwice as likely to have received themeasles vaccination as the poorest 20 per cent of children in Azerbaijan,the Central African Republic, Chad,the Democratic Republic of theCongo, Niger and northern Sudan.
Income disparities and child survival
Equally likely
2 timesas likely
3 timesas likely
4 timesas likely
5 timesas likely
SwazilandKenya
RwandaLesotho
MongoliaDominican Republic
GuyanaSenegal
Trinidad and TobagoViet NamSuriname
GambiaZambia
Guinea-BissauDem. Rep. of Congo
MyanmarSao Tome and Principe
Sudan (North)Azerbaijan
Central African Rep.BurundiAngola
ComorosSierra Leone
ChadNiger
Equatorial GuineaIraq
Lao People’s Dem. Rep.
In 13 countries where data are available, children from the poorest 20 per cent of the pop-ulation are more than twice as likely to be underweight for their age, and in Swazilandthey are five times as likely to be underweight.Source: UNICEF calculations based on data from Demographic and Health Surveys (DHS)and Multiple Indicator Cluster Surveys (MICS).
How likely is a poor child to be underweight
compared to a rich child?

T H E R O O T C A U S E S O F E X C L U S I O N 21
If income disparities are notaddressed, it is likely that the poorestchildren will continue to make up adisproportionate share of the childmortality figures, even if nationalgoals are met. Overall, in 23 of the 56 countries with household surveysallowing for disaggregation byincome, poorer children are morethan twice as likely to die before theirfifth birthday, with some of thesecountries making progress towardsthe goals at the national level andothers failing.
See References, pages 90-91.
Peru
Haiti
Latin Americaand Caribbean
East Asiaand Pacific
Middle Eastand North Africa
South Asia
CEE/CIS Sub-SaharanAfrica
No inequality
2 times as likely
3 times as likely
4 times as likely
5 times as likely
6 times as likely
Indonesia
Cambodia
Egypt
Jordan
India
Pakistan
Turkey
Uzbekistan
South
Africa
Chad
How likely is a poor child
to die before age 5,
compared to a rich child?*
*Individual lines within the regional blockeach represent a country surveyed.
Source: UNICEF calculations based ondata from Demographic and HealthSurveys (DHS) and Multiple IndicatorCluster Surveys (MICS).
Rwanda Uzbekistan
MongoliaGuyana
MyanmarBolivia
Sao Tome and PrincipeDominican Republic
TajikistanLesothoBurundiZambia
MadagascarSwazilandVenezuela
KenyaComoros
Iraq Guinea
Côte d’IvoireSierra Leone
Lao People’s Dem. Rep.Equatorial Guinea
AngolaViet Nam
TogoCameroon
Chad Azerbaijan
Dem. Rep. of CongoSudan (North)
NigerCentral African Rep.
Equally likely
Twice aslikely
3 timesas likely
How likely is a rich child to be vaccinated against
measles compared to a poor child?
Source: UNICEF calculations based on data from Demographic and Health Surveys (DHS)and Multiple Indicator Cluster Surveys (MICS).

22 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 6
or disability. These inequities occur whenchildren and their caregivers are directlyexcluded from services because they live inareas that are poorer and more poorly serviced, or because cultural barriers such as language, ethnic discrimination orstigmatization prevent them from receivingneeded services.
Discrimination against girls excludes them
from education
Gender discrimination is specificallyaddressed by MDG 3, which promotes gender equality and the empowerment ofwomen, with the attached target of elim-inating gender disparity in education.
Education provides the opportunity for girls(and boys) to become more empowered andself-confident as they acquire the range ofknowledge, skills, attitudes and values criti-cal to negotiating an equal place in society.Gender inequality in education means thatfor every 100 boys out of primary school,there are 117 girls who also miss out on primary education.23 While the gender gapin primary education has been closing
steadily since 1980, many countries havefailed to meet the MDG 3 target of genderparity in primary education by 2005, andthe regions with the highest gaps will haveto make even greater gains if gender parityis to be achieved as part of universal pri-mary school completion by 2015.
Gender gaps in secondary education areeven more pronounced: of 75 developingcountries surveyed by UNICEF, only 22were on course to meet the MDG 3 targetof gender parity at the secondary schoollevel, while 25 were far from the goal.24
Girls’ exclusion from education in compari-son to boys – especially in South Asia, sub-Saharan Africa and the Middle East andNorth Africa – is one of the clearest statisti-cal indicators of gender discrimination.
But gender discrimination is both more sub-tle and all-pervasive than can be measuredin the statistics about gender parity inschooling. Gender plays a major part indetermining which children end up beingexcluded from essential services and are,therefore, most at risk of missing out on theMillennium agenda. Many of the groups of
© U
NIC
EF/
HQ
99-1
146/
Tom
isla
v P
eter
nek

children considered in this report are nottaken beyond the reach of internationaldevelopment efforts by their gender alone,but their gender clearly plays a major partin determining their vulnerability. Genderdiscrimination also results in limited accessof women to basic health-care services,which increases the risk of maternal andchild mortality.
Women’s disempowerment results in exclu-sion for their children. Mothers are generallythe first caregivers for children. In situationsand settings where they are denied access tobasic services, essential resources, or infor-mation, it is the children who suffer thegreatest exclusion. Impediments to progressin the fight against gender discriminationinclude the continued lack of good qualitydata disaggregated by sex, the paucity offinancial and technical resources forwomen’s programmes at both internationaland national levels and the lack of repre-sentation in the political sphere.25
Discrimination on the basis of ethnicity is
widespread
Ethnicity is a set of characteristics – cultural,social, religious and linguistic – that forms a distinctive identity shared by a communityof people. It is a natural expression of humandiversity and a source of strength, resilienceand richness in the human family. But whena child faces discrimination because of eth-nicity, the risk of exclusion from essentialservices and protection rises sharply.
There are some 5,000 ethnic groups in theworld, and more than 200 countries havesignificant minority ethnic or religiousgroups. Most countries – around two thirds– have more than one religious or ethnicgroup that accounts for at least 10 per centof the population.26 Some ethnic groups arespread across national borders – for example, the Roma in Central and EasternEurope or residents of Chinese descent inmany countries in South-East Asia. Someare minorities, accounting for a small pro-portion of the national population, whileothers make up a significant share of thepopulation but have little power in societyas a result of their isolation and, very often,deep historical disadvantage.27
T H E R O O T C A U S E S O F E X C L U S I O N 23
A common thread among ethnic groups isthat they often face considerable marginal-ization and discrimination. Almost 900 mil-lion people belong to groups that experiencedisadvantage as a result of their identity,with 359 million facing restrictions on theirreligion. Around the world, some 334 mil-lion people face restrictions or discrimina-tion related to their language. In over 30sub-Saharan African countries (containing80 per cent of the region’s population), forinstance, the official language is differentfrom the one most commonly used, andonly 13 per cent of children in these coun-tries are taught in their mother tongue inprimary school.28
Discrimination on the basis of ethnicity can erode self-worth and confidence in
© U
NIC
EF/
HQ
01-0
675/
Ale
jand
ro B
elag
uer

24 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 6
children and deprive them of opportunitiesfor growth and development, blunting thepromise that is every child’s birthright.Prejudice at community and institutionallevels can restrict opportunities for membersof an ethnic group. In terms of career choic-es and advancement, access to politicaloffice or community leadership, members of ethnic minorities may find their participa-tion in society limited – even where thereare laws prohibiting bias and exclusion.Exclusion based on ethnicity can lead toarmed conflict and even ethnic violence –witness the atrocities along ethnic lines
being committed in Darfur, Sudan, since 2003.
Indigenous children can face multiple
barriers to full participation in society
Indigenous peoples have many characteris-tics and experiences in common with ethnicminorities, but they are distinct from them.Indigenous communities are more likelythan ethnic minorities to insist on their rightto a separate culture linked to a particularterritory and their history. They have gener-ally maintained their own language, culture
The Roma population constitutesEurope’s largest and most vulnerableminority, estimated at between 7 and 9 million people. With no historicalhomeland, roughly 70 per cent ofRoma live in Central and EasternEurope (CEE), and in former SovietUnion countries. Nearly 80 per centlive in countries that joined theEuropean Union (EU) in 2004 or are in the process of negotiating EU membership.a
Exclusion in all its dimensions –social, political, economic or geo-graphic – has affected Roma for cen-turies and has taken the form of overtethnic discrimination. Faced with prej-udices and fears that they are an infe-rior and dangerous people, Romatend to live in ghettos, segregatedfrom the rest of society, and are evenbarred from restaurants and otherpublic places.b
Roma are also among the most impov-erished cultural groups in Central andEastern Europe. Research shows thatnearly 84 per cent of Roma in Bulgariaand 88 per cent of Roma in Romanialive below the national poverty lines.Poverty among Roma is even higher inHungary, with 91 per cent of the groupliving below the national poverty line.c
Because of limited education, a low
level of skills and discrimination in thelabour market, in some Roma settle-ments not a single person is regularlyengaged in formal employment.d
Many Roma children attend separateschools or are segregated whenattending mainstream schools. Romachildren attending Roma-only schoolsfind themselves in overcrowded class-es as a result of geographic and socio-economic segregation.e
As many as 75 per cent of Roma chil-dren in Central and Eastern Europe areplaced in special schools for the men-tally disabled,f but not for genuinehealth reasons. This practice, which iscommon, is related to the economicbenefits that come with special educa-tion. In some CEE countries, childrenwho are sent to schools for the mental-ly challenged receive food subsidies,educational materials and transporta-tion, as well as room and board. Romaparents often agree to place their chil-dren in special schools without fullyunderstanding the long-term conse-quences of their action, and even ifthey do, some families think they haveno other alternatives.g
A study conducted in 2001 by theOpen Society Institute (Budapest), aprivate grant-making foundation,found that 64 per cent of Roma chil-
dren in the second grade placed inspecial schools in Bulgaria, the CzechRepublic, Hungary and Slovakia wereconsidered ‘mentally challenged’.Over a two-year period, the majorityof these students, when placed in special-education pilot classes, wereable to meet the requirements of themainstream curriculum.h
As disturbing as it is, this picture of exclusion is by no means complete. For instance, in Serbia andMontenegro, national statistics on education do not always include the most-excluded children. Issues affect-ing Roma girls are still not addressedin Romania, where the greatest num-ber of Roma people, between 1 and 2million, live. Moreover, in Bosnia andHerzegovina, attendance of Romachildren in schools is sporadic, andthey are almost completely absentfrom the upper grades of primary and secondary schools.
The education system is not the onlyone that is failing Roma children.More than half of the children aban-doned in medical institutions inRomania – 57 per cent – are of Romaethnic origin. Often lacking the appro-priate identity documents and birthcertificates necessary for health insur-ance enrolment, Roma communities
The marginalization of Roma communities and their children

T H E R O O T C A U S E S O F E X C L U S I O N 25
and social organization distinct from thedominant trends of the societies in whichthey live. They are also likely to identifythemselves as indigenous and be identifiedas such by other groups.29 In certain coun-tries, such as Bolivia, Denmark (Greenland)and Guatemala, they represent the majorityof the population. There are some 300 mil-lion indigenous peoples in more than 70 countries, around half of whom live in Asia.30
Indigenous children can suffer cultural dis-crimination and economic and political mar-
ginalization. They are often less likely to beregistered at birth and more prone to poorhealth, to low participation in educationand to abuse, violence and exploitation.31
The Committee on the Rights of the Childhas expressed concern about the particularposition of indigenous children in Australia,Bangladesh, Burundi, Chile, Ecuador, India,Japan and Venezuela.32 Many of them are still denied their rights under theConvention on the Rights of the Child,especially with regard to birth registration,access to education and health-care services.
Information on the extent to which indige-nous children are denied their rights to sur-vival, health-care services and educationrelative to the national average is limited.Case studies in individual countries suggestthat infant and child mortality rates arehigher among indigenous groups than in the national population. In the hill provinceof Ratanakiri, Cambodia, for example,infant mortality rates are more than twicethe national average, while in Australia themortality rate for indigenous infants is threetimes the overall rate.33 Many factors con-tribute to these disparities, including envi-ronmental conditions, discrimination andpoverty. Health-care services – includingvaccination against preventable diseases –are often lacking in areas inhabited byindigenous peoples. In Mexico, for instance,there are an estimated 96.3 doctors per100,000 people nationally but only 13.8 per 100,000 in areas where indigenous people make up 40 per cent or more of the population.34
Indigenous children are less likely to be registered at birth, in part owing to theabsence of information on the issue in theirmother tongue. This can result in chronical-ly low levels of registered children at birth:For example, in the Amazonian region ofEcuador only 21 per cent of under-fiveshave a birth certificate, compared with thenational average of 89 per cent.35 The dis-tance to the nearest registration office andthe cost of the certificate can also be severedeterrents. National legislation that prohibitsindigenous peoples from registering theirchildren with indigenous names can alsoprove a strong disincentive to obtaining abirth certificate; in Morocco, for example,
and their children have very limited access tohealth-care services and are heavily depend-ent on state welfare and other transfer pay-ments. In Romania, Roma men and womenare less likely to have health insurance and tobe enrolled in a family physician’s practicethan their Romanian counterparts.
Efforts are being made to address the situa-tion. The Roma Education Initiative (REI), aproject of the Open Society Institute, in coop-eration with Children and Youth Programs inNew York, is attempting to eliminate discrimi-nation in the school systems in CEE countries– including reintegration of Roma childrenfrom special schools into formal educationand enabling them to succeed in school onequal terms with their peers – through athree-year project launched in 2002.i TheSlovak Government has recently designed aset of strategies that specifically recognizeand address the issues of the Roma minority.Moreover, in 2004, UNICEF Romania, in part-nership with the Romanian Federation ofNGOs Active in Child Protection Issues,launched the “Leave No Child Out” cam-paign dedicated to combating discriminationagainst Roma children and enhancing theiraccess to education. So far, the campaign hasreached about 65 per cent of the country’sRoma population.
See References, page 91.

26 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 6
I spent the first two weeks of my life in a neonatal intensive care unit inBremerhaven, Germany, on a UnitedStates military base. Shortly after Itook my first breath, a young captaintold my father that I had a conditionthat would cause most people aroundthe world to take me to the top of a mountain and leave me there.
The condition is a rare congenitalbone disease called osteogenesisimperfecta, which affects only about0.008 per cent of the world’s popula-tion.a It causes brittle bones resultingin fractures and, in its most extremeform, death. I have a moderate typeof osteogenesis imperfecta and haveonly had 55 fractures. I have under-gone 12 surgeries to strengthen mylegs through the insertion of metalrods into my bone marrow, as well asone attempt to prevent further curva-ture of my spine by fusing bone intothe curves.
In addition to the physical pain ofoperations and fractures, I have beenplagued with feelings of shame andself-contempt as a result of the socialstigma of disability. This is an issue I continue to grapple with today as a24-year-old law student. As a child, Idid not realize how significant thesocial reality of being disabled was,as I felt that I was a normal childwho simply had physical limitations.Still, the reality of fracturing on arandom basis was frightening andstressful to both my mother andmyself. When I was younger, mymother believed that I might fracturewhile playing so she isolated mefrom my peers. I calculated howmuch time I have spent alone, heal-ing from various injuries, and cameup with seven years of my life – afigure that does not include the yearsprior to my schooling.
My first educational experience wasat the age of three when I began toattend a preschool in Colorado, USA,composed exclusively of disabledchildren. I thought it would be won-derful to get to interact with mypeers, but our ability to socialize waslimited by their significantly moreextreme disabilities. A few years laterwe moved to California, where Ibegan attending an elementary schoolas the only disabled child integratedwith able-bodied students. I lovedschool because it gave me the much-needed opportunity to engage inhuman interaction. But there were stilltimes when I felt socially isolatedbecause of my disability, particularlywhen it came to socializing beyondthe confines of my school.
When I was eight years old, I was sentto a school for disabled children toreceive top-quality physical therapyfollowing a re-rodding procedure onmy legs. While I received excellentphysical therapy, the education wasremedial at best. What I learned in myfirst year of school was taught to mea second time. It was a nice mentalhiatus, but I am glad and lucky thatmy time there lasted only one year.
I returned to my small elementaryschool in the mountains of Californiaand was content to interact with peo-ple of similar intellectual calibre. Ibegan to develop friendships, but hadto leave school for about a year toreceive a spinal fusion. While healing,I was taught by a home-schoolteacherfor an hour a day. Again, I experi-enced a void in mental stimulation.
During the early 1990s, I enjoyed sev-eral years without experiencing anysubstantial medical issues andremained in school. But when Ientered adolescence and – like all chil-
children my age – began to becomeaware of my changing body and toexperience physical attraction to otherpeople, things took a turn for theworse. I developed feelings of sexualattraction at the same rate as mypeers, yet experienced a significanttemporal gap between having thesefeelings and being able to expressthem. I felt lost, alone and angry atmyself and the world.
I internalized feelings of hatredtowards my body, which I nowbelieve were garnered throughimages of normalized beauty stan-dards perpetuated by the media andby social stigma. Nowhere did I findpositive images expressing thehumanity of disabled people – onlythose in which we were depicted asobjects intended to provoke pity orsympathy. My self-esteem plummet-ed, and I felt like I would never escapefrom feelings of despair. Theseintense emotions were exacerbatedby the fact that I had to leave all ofmy good friends behind and go to aschool on the other side of town, asthe school my friends were going toattend was inaccessible to disabledstudents.
These feelings did not magically dis-appear when I moved across thecountry to a small town in SouthCarolina. If anything, they grew. Fromthe ages of 11 to 16 I hated myself;when I looked in the mirror I wouldcringe. This period of my life res-onates with me today, as I can stillfeel the scars of those experiences.
My life’s purpose became clear when I began attending the University ofFlorida. As a student, I developed apassion for disability activism.Through arguing points of equality,beauty and pride in disability, I
Living with disability by Bethany Stevens

T H E R O O T C A U S E S O F E X C L U S I O N 27
internalized these ideas and devel-oped the desire to catalyse positivechange for disabled people. I havehad the opportunity to represent theUnited States at two internationalconferences on disability rights inNorway, published reports throughthe United Nations and RehabilitationInternational, and organized largecampus events featuring variousnotable disabled individuals.
Through these experiences, I cameto understand how the stigma relat-ed to disability leads to social andeconomic oppression all over theworld. The reality is that the majorityof people, around 80 per cent in theUnited States alone, will become dis-abled at some point in their lifetime.b
It is my professional aspiration toinitiate a national lobbying agencythat would work not only within theestablished legal system, but alsothrough direct action to encourageindividuals, legislators and corpora-tions to reconstruct the social identity of disability.
Positive social evolution for disabledpersons can occur with education.Information about issues affectingthe disabled could be added to pub-lic school curriculums, and trainingsessions to raise awareness aboutthese issues could be mandated forlarge companies, similar to race and sexual harassment training.Governments need to include dis-ability issues in educational require-ments. People often harbournegative ideas about other groups ofpeople because of lack of awarenessand knowledge.
There is a duality in the need for acognitive revolution, existing withinable-bodied and disabled popula-tions. All too often we internalize
negative stigmas concerning our disability because we cannot see ourbeauty. For most of my life I was theonly disabled person I knew, and Ifound it truly difficult to look into themirror and see an aesthetically dif-ferent person, and yet still see beau-ty. We need a sense of internal pride,as much as society needs to acceptour abilities and assets. This realiza-tion has catalysed my desire to compile a book about the beauty in disability, featuring interviews and photographs of both notableand unknown disabled persons. The book will be dedicated to all disabled people who struggle to see their beauty, much as I did for so many years.
After years of struggling to over-come the feeling of inadequacy andshame that plagued my childhoodand early adulthood, I now believethat being disabled is the best thingthat has ever happened to me. Neverwould I have been afforded the won-derful opportunities I have experi-enced had it not been for mydisability. These opportunities andthe development of pride in my existence came with a pivotal moveinto my father’s home when I was 16years old. He recognized my human-ity and encouraged it to flourish,teaching me how to drive and sup-porting my securing of a job. Heallowed me freedom that my motherwould have never condoned, andwith it I forged an identity that I love.It is wonderful to finally love myself.It is crucial that other parents of children with disabilities allow theirchildren to obtain a sense of inde-pendence because it is necessary forself-sufficiency. It is my hope that Ican assist those living with disabilityin my community, as my father didme, so that young people like me
no longer internalize feelings ofshame about being disabled.
Bethany Stevens is a law student atthe University of Florida (UF) andhas been a disability activist for fiveyears. Ms. Stevens directed a cam-paign and petition process thatresulted in the opening of an accom-modated testing centre for studentswith disabilities at UF. She is thepresident of the Union of Studentswith Disabilities, founder of DeltaSigma Omicron and recently directed the Building a DisAbilityMovement conference hosted at UF.
See References, page 91.

28 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 6
Amazigh people must register their childrenwith a recognized Arabic name36 (seeChapter 3: Invisible Children, for a fullerdiscussion on the risk of exclusion frombirth registration).
In most countries, indigenous children havelow school enrolment rates. Scarce educa-tional facilities, governments’ failure toattract qualified teachers prepared to workin the remote areas where many indigenouspeople live and the perceived irrelevance ofmuch of the school curriculum for the local
community – all act as disincentives toschool participation. When they attendschool, indigenous children often begin their formal education at a disadvantage toother children because they are unfamiliarwith the language of instruction. Researchindicates that it takes until the third gradebefore their comprehension begins to match that of children who speak the dominant language.37
Neglect and stigmatization can result in
exclusion for children with disability
There are an estimated 150 million childrenwith disabilities in the world, most of whom live with the reality of exclusion. The vast majority of children with disabili-ties in the developing world have no accessto rehabilitative health-care or support services, and many are unable to acquire aformal education.38 In many cases, disabledchildren are simply withdrawn from com-munity life; even if they are not activelyshunned or maltreated, they are often leftwithout adequate care. Where special provi-sion is made for children with disabilities, itoften still involves segregating them in insti-tutions – the proportion of disabled childrenliving in public institutions has increased,for instance, in the countries of Central and Eastern Europe since the onset of political transition.39
Many disabilities in developing countries are directly attributable to deprivations ofessential goods and services, especially inearly childhood. Lack of prenatal care addsto the risk of disability, while malnutritioncan result in stunting or poor resistance todisease. Disabilities resulting from poornutrition or lack of vaccines can beaddressed by concerted action and donorsupport. The worldwide assault on polio – amajor cause of physical disability in the past– has resulted in a dramatic reduction in the disease, from 350,000 cases in 1988, whenthe Global Polio Eradication Initiative waslaunched, to 1,255 at the end of 2004.40
The disease is now endemic in only sixcountries – Afghanistan, Egypt, India, Niger,Nigeria and Pakistan – although transmis-sion has been re-established in several coun-tries. But despite this remarkable progress,not every child has been reached, and the
© U
NIC
EF/
HQ
04-0
971/
Gia
com
o P
irozz
i

T H E R O O T C A U S E S O F E X C L U S I O N 29
gains remain at risk of reversal until everychild is immunized.
Between 250,000 and 500,000 children arestill blinded each year by vitamin A deficien-cy, a syndrome easily prevented by oral sup-plementation costing just a few cents (givenevery 4-6 months).41 Children involved inhazardous labour or who have been con-scripted as soldiers face greatly heightenedrisks of disabling physical injury. Landminesand explosive remnants of war continue tomaim or disable children even in countriesthat are no longer in conflict. Of the 65countries that suffered mine casualtiesbetween 2002 and 2003, nearly two thirdshad not experienced active conflict duringthe period.42
Regardless of the cause, or where they live,children with disabilities require specialattention. Given the higher risk they face ofbeing excluded from school and within theirsocieties, communities and even households,children living with disabilities are liable toend up forgotten in campaigns for develop-ment that focus on statistical targets basedon national aggregates.
Tackling the root causes of
exclusion
The strategies to achieve the Millenniumagenda advanced in the reports of theUnited Nations Millennium Project and ofthe Secretary General address many of thebroad factors mentioned in this chapter andcall on governments, donors and interna-tional agencies to tackle them. Less empha-sis is given, however, to specific measuresthat would prevent exclusion for childrenfacing extreme poverty, armed conflict,weak governance, HIV/AIDS, and discrimi-nation in all its forms – particularly if,despite the increased efforts of the interna-tional community, these factors persist overthe coming decade.
Children in the least developed countries
require special attention
Addressing the special – and urgent – needsof the least developed countries has becomea priority objective for the internationalcommunity in recent years. In May 2001,
the Brussels Declaration and Programme ofAction for the Least Developed Countriesfor the Decade 2001-2010 were endorsed bythe United Nations General Assembly. Butprogress on the plan has not matched itsambition. Despite significant advances bysome least developed countries towards the plan’s individual goals, as a group theyhave made only limited inroads towardseradicating poverty and fostering sustain-able development.
Reducing poverty in the least developedcountries will require greater efforts in fivemajor areas: national development strate-gies, official development assistance, fulldebt cancellation, fair trade and enhancedtechnical assistance from donors.43
Measures agreed in 2005 at both the Group of Eight (G-8) Summit in July andthe World Summit in September will gosome way towards increasing official development assistance and reducing exter-nal debt burdens for the least developedcountries. But for development strategies tobe truly effective and sustainable, theyrequire a stronger focus on children, whoaccount for around half of the population inthese countries. As Chapter 4 will attest,poverty-reduction processes, and budgets inparticular, will need to be adjusted toexpand or reallocate resources for the socialdevelopment required to diminish the deprivations faced by millions of childrenliving in the least developed countries. Inaddition, even bolder initiatives may well berequired on official development assistance,debt reduction and fair trade to ensure thatthe Millennium agenda is met for theworld’s most impoverished nations.
Conflict resolution and prevention are
required to safeguard children and women
Preventing and resolving armed conflict arecentral objectives of the peace and securityaims of the Millennium agenda, outlined indetail in the Millennium Declaration. Withchildren and women most at risk fromarmed conflict – accounting for around 80per cent of all deaths among civilians due toarmed conflict since 199044 – conflict pre-vention and resolution are vital to ensuretheir protection and access to essential serv-ices. Where conflict does occur, emergency

30 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 6
Every minute, a child under 15 diesof an AIDS-related illness.a Everyminute, another child becomes HIV-positive. Every minute, four youngpeople between the ages of 15 and24 contract HIV.b
These stark facts underline the dev-astating impact that HIV/AIDS is having on children and young peo-ple. The children of sub-SaharanAfrica are hardest hit, but unless theHIV pandemic is halted and sent intoretreat, Asia is on course to havehigher absolute numbers of HIVinfections by 2010.c Millions of chil-dren, adolescents and young peopleorphaned, made vulnerable or livingwith HIV are in urgent need of careand protection. If rates of HIV infec-tion and AIDS-related deaths contin-ue to rise, the crisis will persist fordecades, even as prevention andtreatment programmes expand.
HIV/AIDS is denying millions of children their childhood. The diseaseexacerbates the factors that causeexclusion, including poverty, malnu-trition, inadequate access to basicsocial services, discrimination and stigmatization, gender inequities and sexual exploitation of womenand girls.
National governments committedthemselves to addressing the impactof HIV/AIDS on children in theDeclaration of Commitmentendorsed at the United NationsGeneral Assembly Special Sessionon HIV/AIDS in 2001. But progresshas been slow. Children are oftenoverlooked when strategies onHIV/AIDS are drafted, policies formu-lated and budgets allocated. At the2005 World Summit, world leaderspledged to scale up responses to
HIV/AIDS through prevention, care,treatment, support and mobilizationof additional resources.
The Global Campaign on Childrenand AIDS – Unite for Children. Uniteagainst AIDS – launched in October2005, is a concerted push to ensurethat children and adolescents are notonly included in HIV/AIDS strategies,but become their central focus. Anoverarching aim of the campaign isto meet Millennium DevelopmentGoal 6, which aims to halt andreverse the spread of HIV/AIDS by2015. Achievement of the campaigngoals will also have positive implica-tions for the other MDGs.
Although global in reach, the cam-paign will have a strong focus on themost-affected countries in sub-Saharan Africa, home to 24 of 25countries with the world’s highestlevels of HIV prevalence.d The cam-paign seeks to provide a child-focused framework around countryprogrammes in four main areas,dubbed the ‘Four Ps’:
Prevent infection among
adolescents and young people
Reduce HIV/AIDS risks and vulnera-bility by increasing access to anduse of youth-friendly and gender-sensitive prevention information, life skills and services.
Prevent mother-to-child HIV
transmission
Increase provision of affordable and effective services that help HIV-positive pregnant girls andwomen avoid transmitting the virus to their children. Prioritize care, support and treatment pro-grammes for HIV-infected childrenand pregnant women.
Provide paediatric treatment
Provide affordable paediatric HIVdrugs, such as cotrimoxazole, to prevent opportunistic infections.
Protect and support children
affected by HIV/AIDS
Make sure a higher proportion of the neediest children receive qualityfamily, community and governmentsupport, including education, healthcare, birth registration, nutrition andpsychosocial support.
The Global Campaign on Childrenand AIDS involves partners fromevery sector of the global communi-ty. It aims to unite as many people,organizations and agencies as possi-ble under its call to action. From theoutset, the campaign was positionedwithin harmonized approaches,especially the ‘Three Ones’ princi-ples that were endorsed by a con-sensus of governments, internationalorganizations, donors and civil socie-ty; the WHO and UNAIDS ‘3 by 5’Initiative, which aims to provide sus-tained treatment for 3 million peopleliving with HIV/AIDS; and nationalpoverty reduction strategies.
In partnership, governments andagencies, activists and scientists,corporations and community work-ers, and as many others as possiblewill work through the campaign toensure that this is the last generationof children that bears the bitter bur-den of HIV/AIDS.
See References, page 91.
The Global Campaign on Children and AIDS

T H E R O O T C A U S E S O F E X C L U S I O N 31
responses should consist not only of provid-ing essential services and goods, but alsopreventing the separation of families andhelping to reunite them, initiating theresumption of schooling, organizing childprotection and preventing HIV/AIDS.45
Children living in ‘fragile’ States must not
be forgotten
‘Fragile’ States require particular attention,since a dysfunctional government willcomplicate efforts to implement any policyor obtain any non-humanitarian develop-ment assistance. Nonetheless, continuedengagement with governments of suchStates – and also non-state actors whomay wield substantial power within thesecountries – is often vital to safeguard chil-dren living in these countries from exclu-sion. Children must not be forgotten bythe international community because oftheir countries’ failings.
A global campaign to mitigate the impact
of HIV/AIDS on children is under way
The international community is stepping upits efforts to tackle HIV/AIDS through aseries of initiatives. These efforts are crucialto check the spread of the disease and tomake treatment widely available. Fargreater attention must be given, however, tothe impact of the pandemic on children andadolescents, especially girls, and to ways ofprotecting them from both infection andexclusion. To this end, UNICEF and itspartners have launched a global campaignon children and AIDS (see Panel page 30).
Governments and societies must openly
address discrimination
Tackling discrimination requires a multi-pronged approach. Many elements of discrimination are rooted in long-held socie-tal attitudes, which often governments, civilsociety and the media are reluctant to con-front. Yet confront them they must, if theyare to fulfil their commitments to children.Targeted initiatives to address the exclusionfaced by women and girls, ethnic andindigenous groups and the disabled areneeded, along with legislation to prohibitdiscrimination, and greater research onthese groups’ needs and well-being. Takenby themselves, however, such measures mayonly serve to reduce discrimination, nottackle its root causes. For these initiatives tobring about lasting change, they must beaccompanied by a courageous, open discus-sion – involving the media and civil society– on societal attitudes that foster or toleratediscrimination. The future of children atrisk of exclusion as a result of discrimina-tion depends on such courageous action.
Swift and decisive action is required
A childhood cannot wait for extreme pover-ty to be eradicated, armed conflict to abate,the HIV/AIDS pandemic to subside, or forgovernments and societies to openly chal-lenge attitudes that entrench discriminationand inequalities. Once past, a childhoodcan never be regained. For millions of chil-dren, their childhood and their futuredepend on swift and decisive action beingtaken now to address these threats.

3 %
16 %
8 %
14 %
14 %
18 %
18 %
8 %
4 %
21 %
31 %
16 %
10 %
45 % 7 %
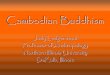
Extreme and Relative Poverty:Precursors to Exclusion
MDG 1 focuses on halving extreme poverty by 2015. While the most widely used measure of poverty is the proportion of people whose income is less than $1 a day, poverty has multiple definitions and numerous ways of affecting children.Children experience extreme poverty differently than adults: Child poverty cannot be understood only in terms of family income, and responses must takechildren’s experiences into account. Forthem, poverty is experienced as both material and developmental deprivation.*The exclusion resulting from poverty canhave lifelong impacts.
Children do not have to live in extremepoverty to feel excluded. Research suggeststhat when children do not consider them-selves to be part of families whose materialconditions are close to what is considered‘normal’ for their community, the impact is greatly felt.** This relative deprivation isbased on the idea that people decide howwell off or deprived they are – what theyshould deserve or expect – by comparingthemselves to others. Measuring the distribution of wealth within a country orterritory by comparing the differences inresources available to the wealthiest andpoorest sections of society is one simpleway to gauge inequality.
Even if the goal to end the extreme povertyfaced by millions is achieved, relative deprivation – the inequality and exclusionfaced by children and their families – willcontinue unless specific measures toencourage equality and social mobility arepursued, including the allocation ofresources for education, health care andother interventions to ensure that the rightsof every child are fulfilled.
World
Least developed countries
Developing countries
Middle East and North Africa
Central and Eastern Europe
Latin America and Caribbean
East Asia and Pacific
South Asia
Eastern and Southern Africa
West and Central Africa 55%
38%
33%
14%
10%
4%
3%
22%
41%
21%
Source: Derived from World Bank, 2005 World Developement Indicators,as reported in Statistical Table 7, pp. 122-125.
Proportion of the population living on less than $1 a day by region
* UNICEF, State of the World’s Children 2005, New York, 2004, p. 16.
** See, for example, Christian Children’s Fund, Children in Poverty: The Voices of Children, 2003.
32 T H E S T A T E O F T H E W O R L D ’ S C H I L D R E N 2 0 0 6

This map does not reflect a position by UNICEF on the legal status of any country or territory or the delimitation of any frontiers. Dotted line represents approximately the Line of Control in Jammu and Kashmir agreed upon by India and Pakistan. The final status of Jammu and Kashmir has not yet been agreed upon by the parties.
72 %
45 %
3 %
23 %
23 %
49 %
64 % 56 %
42 %
8 %
36 %
11 %
35 %
17 %
67 %
26 %
61 %
70 %
45 %
11 %
36 %
57 %
54 %
22 %
17 % 12 %
13 %
35 %
39 %
36 %
7 % 17 %
16 %
27 %
8 %
8 %
13 %
3 %
4 %
5 %
22 %
31 %
38 %
85 %
16 %
61 %
52 % 55 %
26%
34 %
3 %
A Decent Standard of Living
Distribution of income: ratio between richest 10% and poorest 10%
No data
0 - 9 times greater
10 -19 times greater
20 - 39 times greater
40 - 59 times greater
Over 60 times greater
Source: UNDP Human Development Report 2004.
% Proportion of the population living on less than one dollar a day (where greater than 2%)
Source: World Bank, 2005 World Development Indicators.
T H E R O O T C A U S E S O F E X C L U S I O N 33