Embed Size (px)
Citation preview
Kidney International, Vol. 65 (2004), pp. 2003–2017
PERSPECTIVES IN BASIC SCIENCE
The role of vascular endothelial growth factor (VEGF) in renalpathophysiology
BIEKE F. SCHRIJVERS, ALLAN FLYVBJERG, and AN S. DE VRIESE
Renal Unit, Department of Internal Medicine, Gent University Hospital, Gent, Belgium; Medical Department M (Diabetes andEndocrinology), Medical Research Laboratories, Institute of Experimental Clinical Research, Aarhus University Hospital, Aarhus,Denmark; and Renal Unit, Department of Internal Medicine, AZ Sint-Jan AV, Brugge, Belgium
The role of vascular endothelial growth factor (VEGF) in renalpathophysiology. Vascular endothelial growth factor (VEGF)is an endothelial-specific growth factor that promotes endothe-lial cell proliferation, differentiation and survival, mediatesendothelium-dependent vasodilatation, induces microvascularhyperpermeability and participates in interstitial matrix re-modeling. In the kidney, VEGF expression is most promi-nent in glomerular podocytes and in tubular epithelial cells,while VEGF receptors are mainly found on preglomerular,glomerular, and peritubular endothelial cells. The role of VEGFin normal renal physiology is essentially unknown. The ab-sence of prominent effects of VEGF blockade in normalexperimental animals suggests a limited function during home-ostasis, although a role in the formation and maintenance ofglomerular capillary endothelial fenestrations has been sug-gested. VEGF and its receptors are up-regulated in experi-mental animals and humans with type 1 and type 2 diabetes.Inhibition of VEGF has beneficial effects on diabetes-inducedfunctional and structural alterations, suggesting a deleteriousrole for VEGF in the pathophysiology of diabetic nephropa-thy. VEGF is required for glomerular and tubular hypertro-phy and proliferation in response to nephron reduction, andloss of VEGF is associated with the development of glomeru-losclerosis and tubulointerstitial fibrosis in the remnant kidney.No firm conclusions on the role of VEGF in minimal changeor membranous glomerulonephritis can be drawn. VEGF maybe an essential mediator of glomerular recovery in prolif-erative glomerulonephritis. Glomerular and tubulointerstitialrepair in thrombotic microangiopathy and cyclosporin nephro-toxicity may also be VEGF-dependent. In conclusion, VEGFis required for growth and proliferation of glomerular and per-itubular endothelial cells. While deleterious in some, it may con-tribute to recovery in other forms of renal diseases.
Key words: compensatory hypertrophy, diabetic nephropathy, glomeru-lonephritis, transplant rejection, vascular endothelial growth factor(VEGF), uremia.
Received for publication April 24, 2003and in revised form August 7, 2003, and September 25, 2003Accepted for publication December 3, 2003
C© 2004 by the International Society of Nephrology
Vascular endothelial growth factor (VEGF-A orVEGF), formerly called vasculotropin or vascular per-meability factor (VPF), belongs to a family of multipo-tent cytokines, also including VEGF-B, -C, -D, -E, andplacenta growth factor [1]. Alternative exon splicing of asingle VEGF gene results in at least six different isoforms.They are homodimeric glycoproteins of 121, 145, 165,183, 189, and 206 amino acids (VEGF121−206) in humansand are one amino acid shorter in rodents [2]. VEGF121,VEGF165, and VEGF189 are the most abundantly ex-pressed isoforms, whereas VEGF145 and VEGF206 arecomparatively rare [2]. VEGF stimulates endothelialcell proliferation and differentiation, increases vascularpermeability, mediates endothelium-dependent vasodi-latation, and supports vascular survival by preventingendothelial apoptosis [1, 2]. In addition, VEGF inducesplasminogen activator, plasminogen activator inhibitor-1 and interstitial collagenase, factors important inmatrix remodeling. Furthermore, VEGF promotesmonocyte chemotaxis and expression of adhesionmolecules [1, 2]. VEGF165, VEGF189, and VEGF121 differin affinity for heparin and heparan-sulfate proteoglycans(VEGF189 > VEGF165 > VEGF121) and in mitogenic ef-fect (VEGF165 > VEGF121) [2]. VEGF165, VEGF189, andVEGF206 are in most part sequestered in the extracellu-lar matrix and at the cell surface, whereas VEGF121 andVEGF145 are freely released [2]. The receptors for VEGF,previously described as fms-like tyrosine kinase (Flt-1)and fetal liver kinase 1 (Flk-1/KDR), now designated asVEGFR-1 and VEGFR-2, respectively, are high-affinitytransmembrane tyrosine kinase receptors [2]. SolubleVEGFR-1 (sVEGFR-1), a splice variant of VEGFR-1,regulates VEGF availability by binding VEGF in the cir-culation [3, 4]. Neuropilin-1 and Neuropilin-2 act as iso-form specific co-receptors for VEGF [5]. Hypoxia is themain stimulus for VEGF expression and/or production.Several growth factors and cytokines such as epidermalgrowth factor, transforming growth factor b (TGF-b),platelet-derived growth factor (PDGF), insulin-likegrowth factor I (IGF-I), angiotensin II, interleukin-1
2003

2004 Schrijvers et al: VEGF in renal pathophysiology
(IL-1), and IL-6 also have the potential to up-regulateVEGF expression. VEGF may be induced by other fac-tors as well [i.e., prostaglandins, mechanical stress, hy-perglycemia, advanced glycation end products (AGEs),protein kinase C (PKC), and reactive oxygen species(ROS)]. VEGF up-regulates the expression of endothe-lial nitric oxide synthase (NOS3) in endothelial cells andincreases the production of nitric oxide [6]. Several linesof evidence have indicated that VEGF exerts its biologiceffects through nitric oxide [7]. Nitric oxide may down-regulate VEGF expression and thus function in a negativefeedback regulator mechanism [8]. Recently, 15 differ-ent sequence polymorphisms have been identified withinthe VEGF gene, including a C/T base change at position−460, a G/C change at +405 and a A/C change at −141[9]. The−460C/+405G and−460T/+405C haplotypes arethe most frequently observed in the normal population[9]. A correlation of the +405 genotype with productionof VEGF has been demonstrated in vitro [9] and in vivo[10], with the highest VEGF production for the GG geno-type, intermediate production for the GC genotype andlowest production for the CC genotype [9]. Further, thecombination of the +405G genotype with other polymor-phisms resulted in higher VEGF promotor activity [11].A deletion/insertion (D/I) polymorphism at the −2549position of the VEGF promotor region has been linkedto increased transcriptional activity [12].
Angiopoietins form another family of endothelial-specific growth factors consisting of angiopoietin-1(Ang-1) and angiopoietin-2 (Ang-2), which bind to tyro-sine kinase receptors Tie1 and Tie2 [13]. Angiopoietinsand VEGF play co-ordinated and complementary rolesin vascular homeostasis [13]. Ang-2 stimulates new bloodvessel formation in the presence of VEGF, but promotesendothelial apoptosis and vessel regression when VEGFlevels are low [14].
VEGF IN RENAL PHYSIOLOGY
This section elaborates on the expression and the po-tential role of VEGF, angiopoietins, and their receptorsin the normal adult kidney. A comprehensive discussionof the role of the VEGF system in renal developmentis beyond the scope and space limitations of this re-view and has been published elsewhere [15]. Culturedrat and human mesangial cells express both mRNA ofVEGF121, VEGF165, and VEGF189, and VEGF protein[16, 17]. In rodent and human kidneys, VEGF mRNAand/or protein were detected predominantly in glomeru-lar podocytes, distal tubules, and collecting ducts, and toa lesser extent in some proximal tubules [3, 16, 18–23].The expression of the different VEGF isoforms in normalhuman glomeruli was complex and variable with substan-tial inter- and intraindividual variation [3]. Ang-1, but notAng-2, was identified in adult human glomeruli, partic-
ularly in podocytes [24]. VEGFR-1 and VEGFR-2 weredetected in cultured rat and human mesangial cells [25–28] and in cultured rat renal tubular epithelial cells [29],but not in cultured primary human podocytes [30]. In con-trast, conditionally immortalized human podocytes ex-pressed VEGFR-1, VEGFR-3 and Neuropilin-1 but notVEGFR-2 [31]. Cultured mouse glomerular endothelialcells and transformed tubular epithelial cells expressedNeuropilin-1 and Neuropilin-2 [32]. Neuropilin-1 wasalso detected in cultured human mesangial cells [25, 27]and in cultured primary human glomerular podocytes[30]. The expression of VEGFR-1, VEGFR-2, sVEGFR-1, and Neuropilin-1 in isolated human glomeruli wasalso heterogenous [3, 30]. In human kidney, VEGFR-1and VEGFR-2 were predominantly expressed on pre-glomerular, glomerular, and peritubular endothelial cells[20, 23, 27, 33]. In rat kidney, VEGFR-2 expression wasdetected in glomerular and peritubular endothelial cells,in distal convoluted tubules and collecting ducts, andin cortical interstitial fibroblast and medullary intersti-tial cells, whereas VEGFR-1 was expressed more diffusein proximal and distal tubules [19, 29]. In human kid-ney, Neuropilin-1 was detected in glomerular podocytes[30]. Neuropilin-1 and Neuropilin-2 were localized in per-itubular capillary endothelial cells in adult mouse and ratkidney [32]. Tie2 was demonstrated in glomerular cap-illary endothelial cells of human and rat glomeruli andin cultured human microvascular endothelial cells [24].In summary, in vivo, capillary endothelial cells expressVEGFR-1, VEGFR-2, and Tie2, glomerular podocytesexpress Neuropilin-1 and produce VEGF and Ang-1.
Although the functions of constitutively expressedVEGF and VEGF receptors in the normal kidney arelargely unknown, some hypotheses may be derived fromthe peculiar distribution of the molecule and its recep-tors in the kidney. VEGF is strongly expressed by vis-ceral epithelial cells while its binding sites are localizedon glomerular endothelial cells. If one assumes the ex-istence of a paracrine loop in the glomerulus, VEGFmust move in the opposite direction of the glomerularfiltrate in order to bind to its receptors. The presenceof such complex mechanism suggests that the strategiclocalization of podocytes is required for the correct sens-ing and interpretation of the stimulus for VEGF release.VEGF may be involved in the induction and maintenanceof the fenestrae in glomerular capillary endothelial cells[37]. Given the role of VEGF in promoting microvascu-lar permeability, it has been speculated that VEGF mayregulate glomerular permeability, although it is generallyacknowledged that the capillary fenestrations do not rep-resent the ultimate barrier to filtration. Recently, in vitroevidence indicated that VEGF may act as an autocrinefactor on calcium homeostasis and cell survival in humanpodocytes [31]. In contrast to the prominent expression ofthe VEGF system in the adult kidney, the administration

Schrijvers et al: VEGF in renal pathophysiology 2005
or inhibition of VEGF in normal adult animals appears tohave only minimal effects. In the isolated perfused rat kid-ney, administration of VEGF increased the renal bloodflow but did not influence the glomerular filtration rate orthe permselectivity of the glomerular barrier wall [34]. Invivo infusions of VEGF into the renal artery of rats didnot influence protein excretion rate [34]. The administra-tion of neutralizing monoclonal anti-VEGF-antibodies tonormal rats had no effect on glomerular filtration rate orglomerular volume [35]. Injection of a VEGF165 aptamer,an oligonucleotide-based VEGF165 antagonist, in normalrats had no effect on kidney and glomerular morphology,did not induce proteinuria and did not affect glomerularcell proliferation and the number of endothelial fenes-trations [36]. In contrast, podocyte-specific heterozygousand homozygous deletions of VEGF in mice resulted inproteinuria and endotheliosis by 21/2 weeks of age, andin perinatal lethality, respectively, with loss of endothelialfenestrations or failure to form fenestrations [37]. Con-versely, podocyte-specific overexpression of VEGF165 ledto a collapsing glomerulopathy [37].
VEGF IN RENAL PATHOPHYSIOLOGY
Diabetic nephropathy
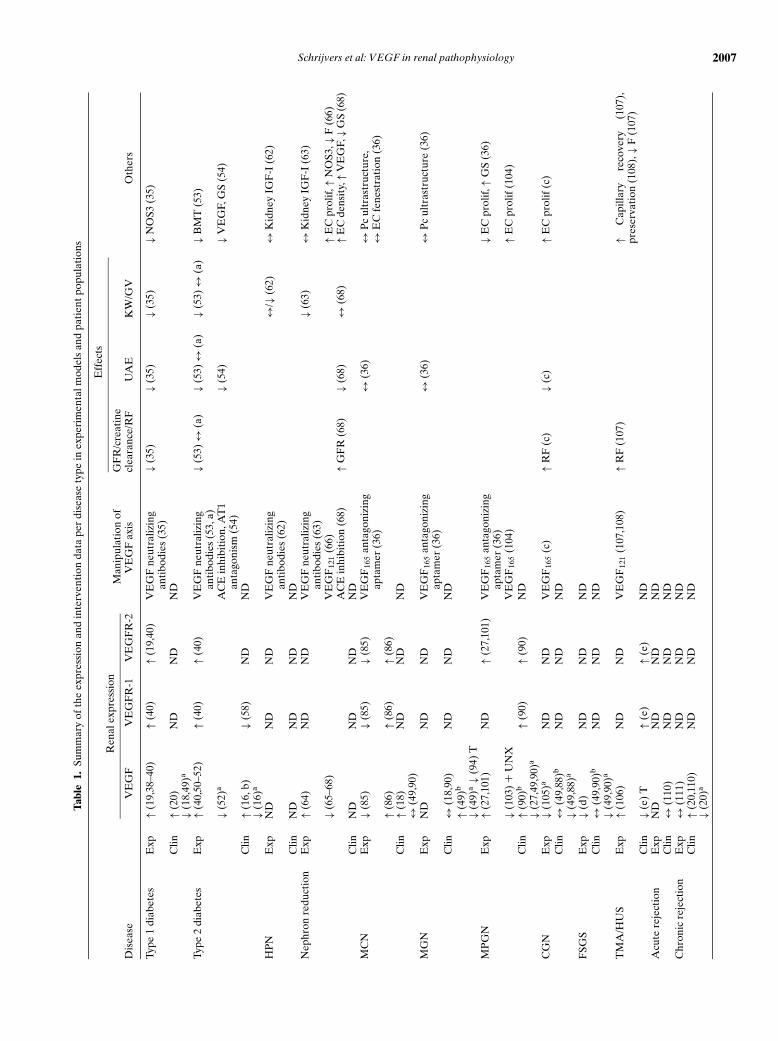
Type 1 diabetes. VEGF mRNA and protein expres-sion were increased at the onset of diabetes in geneticallydiabetic BioBreeding rats [38], in glomerular podocytes,distal tubules and collecting ducts after 3 weeks and 32weeks of streptozotocin (STZ)-diabetes in rats [19] and inrenal tubular and vascular compartments in STZ-diabeticrats with superimposed hypertension [39]. More specifi-cally, the VEGF164 and VEGF188 isoforms increased af-ter STZ-diabetes induction which was reversed by insulintreatment [40]. Glomerular VEGFR-1 and VEGFR-2mRNA expression were higher after 6 weeks of STZ-diabetes [40]. Similarly, VEGFR-2 mRNA was increasedin glomerular and peritubular endothelial cells and inter-stitial cells after 3 weeks of STZ-diabetes but not after32 weeks [19]. To assess the role of VEGF in the patho-physiology of early renal dysfunction in diabetes, type 1diabetic rats were treated with monoclonal neutralizinganti-VEGF-antibodies for 6 weeks. Inhibition of VEGFabolished the diabetes-associated glomerular hyperfiltra-tion, glomerular hypertrophy, and urinary albumin ex-cretion (UAE) without an effect on metabolic control[35]. In addition, the diabetes-associated up-regulationof NOS3 expression was prevented, further supportingthe evidence that nitric oxide acts as a downstream me-diator of VEGF [35].
Both increased [abstract; Abdel Aziz MY, NephrolDial Transplant 12:1538a, 1997] [41, 42] and unaltered[43, 44] serum or plasma VEGF levels were observedin type 1 diabetic patients versus control subjects. Var-ious studies examined a correlation between circulat-
ing VEGF levels and parameters reflecting the sever-ity of diabetic nephropathy. VEGF levels were higherin macroalbuminuric type 1 diabetics than in patientswithout complications [41, 45] and microalbuminuric pa-tients [abstract; Abdel Aziz MY, Nephrol Dial Transplant12:1538a, 1997]. Other studies reported no differences inVEGF levels between type 1 diabetic patients with andwithout (micro)albuminuria [43, 44, 46]. Correlations be-tween VEGF levels and glycemic control, severity of dia-betic nephropathy, and degree of UAE were observed insome [abstract; Abdel Aziz MY, Nephrol Dial Transplant12:1538a, 1997] [41] but not in all studies [43, 44, 46, 47].A positive correlation was found between serum VEGFlevels and nailfold capillary permeability in type 1 diabet-ics [47]. Urinary VEGF excretion was unchanged in pa-tients with diabetic nephropathy compared with controlsubjects [48]. Renal biopsies from patients with diabeticnephropathy showed fewer glomerular VEGF mRNApositive cells than biopsies from controls [18]. Glomeru-lar VEGF expression was highest in the patients withmildest sclerotic changes and was particularly strong inviable glomerular podocytes [20], but reduced or absentin sclerotic glomeruli [20, 49]. Atrophic tubules were neg-ative for VEGF mRNA, except for a weak signal in distaltubules, whereas interstitial cells often had pronouncedVEGF mRNA and protein positivity [20]. In patientswith type 1 diabetes and a minimum diabetes durationof 10 years, the frequency of the +405 CC genotype,which is associated with lower VEGF protein produc-tion in peripheral blood mononuclear cells (PBMC) [9],was increased compared with control subjects [abstract;Summers AM, J Am Soc Nephrol 13:248A, 2002]. An in-crease in the −460 T allele was found in patients with mi-croalbuminuria or proteinuria compared to patients withnormoalbuminuria [abstract; Summers AM, J Am SocNephrol 13:248A, 2002]. The D allele and DD genotypeof the VEGF D/I polymorphism at −2549 of the promo-tor region were associated with susceptibility to diabeticnephropathy in type 1 diabetics and the presence of theD allele was linked to increased transcriptional activity[12].
Type 2 diabetes. Renal and/or glomerular VEGFmRNA were increased in diverse experimental mod-els of type 2 diabetes [i.e., modestly in insulin-resistantZucker fatty/fatty rats and more pronounced in Zuckerdiabetic fatty (ZDF) rats [40], in db/db mice [50], and inOtsuka Long-Evans Tokushima fatty (OLETF) rats] [51].In OLETF rats, VEGF mRNA expression was increasedonly in the early period of diabetic nephropathy [51]. InZDF rats, VEGF mRNA levels rose early in the course ofdiabetes and remained elevated up to 7 months [52]. At9 months, when glomerulosclerosis was most pro-nounced, renal VEGF mRNA levels were reduced [52].VEGFR-1 and VEGFR-2 mRNA were also elevated inZDF rats [40]. Treatment with anti-VEGF-antibodies in

2006 Schrijvers et al: VEGF in renal pathophysiology
db/db mice attenuated the diabetes-associated increasesin kidney weight, glomerular volume and UAE, andabolished the increase in basement membrane thicknessand creatinine clearance [53]. In addition, the antibodiestended to reduce the mesangial matrix expansion [53]. Incontrast, in Goto-Kakizaki rats, an experimental model oflean type 2 diabetes, anti-VEGF-antibodies only tendedto reduce glomerular hypertrophy and had no effect onUAE or creatinine clearance [abstract; Schrijvers BF,J Am Soc Nephrol 13:764A, 2002]. Treatment of OLETFrats with temocapril or CS-866, an angiotensin II type 1receptor (AT1) antagonist, improved glomerulosclerosis,reduced urinary protein excretion and VEGF staining,suggesting that AT1 may be involved in the overproduc-tion of VEGF in diabetic nephropathy [54].
Plasma VEGF levels were higher in type 2 diabeticsthan in controls [55]. In another study, plasma VEGFlevels were elevated only in type 2 diabetic patientswith characteristics of atherosclerosis [56]. Plasma VEGFtended to rise with increasing UAE [55], however, otherstudies reported no such correlation [47, 57]. In type 2 di-abetic patients, VEGF did not correlate with serum cre-atinine [57] or capillary permeability [47]. There wereno differences in sVEGFR-1 plasma levels between dia-betic patients with or without atherosclerosis and con-trol subjects [56]. Urinary VEGF excretion increasedwith the progression of diabetic nephropathy and cor-related weakly with the levels of serum creatinine, crea-tinine clearance, microalbuminuria, and proteinuria [16].In biopsies with mild changes of diabetic nephropathy,VEGF was up-regulated in glomerular podocytes anddistal tubular cells. In biopsies with advanced changes,VEGF staining was decreased or negative in scleroticglomeruli but remained intense in tubules [16]. Morerecently, in patients with type 2 diabetic nephropathy,glomerular VEGF mRNA expression, observed predom-inantly in podocytes, was higher than in normal kidneys,but in contrast to the previous study, VEGF expressionwas higher in patients with advanced renal morphologicchanges than in patients with mild-moderate mesangialexpansion and tubulointerstitial changes [abstract;Kanesaki Y, J Am Soc Nephrol 13:8A, 2002]. In glomeruliof type 2 diabetic patients, VEGF mRNA level wasinversely related to albumin excretion rate [abstract;Bortoloso E, Diabetologia 42:273A, 1999]. Tubuloint-erstitial VEGF and VEGFR-1 mRNA were lower inpatients with severe diabetic nephropathy [58]. Whilethe ratio between VEGF121 and VEGF165 correlatedwith mesangial matrix expansion in one study [abstract;Bortoloso E, Diabetologia 42:273A, 1999], no relationwith the severity of the histologic changes was foundin another [58]. As VEGF121 is freely diffusable andVEGF165 is mostly bound to extracellular matrix, thepathophysiologic relevance of the ratio between both iso-forms remains to be determined.
Conclusion. Data regarding circulating VEGF levelsin patients with diabetes are highly discrepant. As VEGFis a paracrine mediator, systemic levels may not ade-quately reflect changes in the local VEGF system [43]. Inaddition, the assay methods vary substantially betweenthe studies (i.e., VEGF isoform specificity, detection oftotal or free VEGF and interference with VEGF-bindingmolecules such as a2-macroglobulin) [59]. Finally, deter-minations of serum and plasma VEGF levels may dif-fer, owing to release from platelets and leukocytes aftersampling [60, 61]. Renal expression of VEGF and its re-ceptors is more consistently up-regulated in experimentalanimals and patients with type 1 and type 2 diabetes, espe-cially early in the course of diabetes (Table 1). Inhibitionof VEGF resulted in beneficial effects on the diabetes-associated renal changes, underlining a deleterious rolefor VEGF in the pathophysiology of diabetic nephropa-thy. Although the cause of the up-regulation of the VEGFsystem in diabetes remains unknown, several factors rel-evant to the pathogenesis of diabetic nephropathy havebeen shown to promote VEGF expression in different celltypes, including hyperglycemia, AGEs, PKC, angiotensinII, various cytokines, and aldose reductase.
High protein–induced nephropathy
One study examined the potential role of VEGF inhigh protein–induced renal and glomerular enlargement(Table 1) [62]. Mice fed a diet containing 45% proteinexhibited early glomerular hypertrophy and kidneyenlargement compared with mice on a 20% protein con-taining diet. Treatment with a monoclonal neutraliz-ing VEGF-antibody abolished the high protein–inducedglomerular hypertrophy without affecting kidney or bodyweight. Kidney IGF-I was up-regulated in high protein–fed mice and not affected by treatment with the VEGF-antibody. Consequently, as IGF-I has been implicatedin high protein–induced renal growth, VEGF could bea downstream mediator of IGF-I. This study illustratesthat VEGF plays a major role in high protein-inducedglomerular growth [62].
Nephron reduction
Uninephrectomized mice are characterized by an in-creased glomerular volume and kidney weight in the rem-nant kidney and an early transient increase in kidneyIGF-I concentration [63]. To explore a role for VEGFin compensatory renal changes after uninephrectomy,these animals were treated with anti-VEGF-antibodies,which abolished the glomerular enlargement and par-tially blocked the renal growth without affecting re-nal IGF-I levels [63]. After a 75% surgical nephronreduction, the remnant kidneys of C57Bl6xDBA2/F1mice displayed compensatory glomerular and tubular
Schrijvers et al: VEGF in renal pathophysiology 2007
Tabl
e1.
Sum
mar
yof
the
expr
essi
onan
din
terv
enti
onda
tape
rdi
seas
ety
pein
expe
rim
enta
lmod
els
and
pati
entp
opul
atio
ns
Eff
ects
Ren
alex
pres
sion
Man
ipul
atio
nof
GF
R/c
reat
ine
Dis
ease
VE
GF
VE
GF
R-1
VE
GF
R-2
VE
GF
axis
clea
ranc
e/R
FU
AE
KW
/GV
Oth
ers
Type
1di
abet
esE
xp↑(
19,3
8–40
)↑(
40)
↑(19
,40)
VE
GF
neut
raliz
ing
anti
bodi
es(3
5)↓(
35)
↓(35
)↓(
35)
↓NO
S3(3
5)
Clin
↑(20
)N
DN
DN
D↓(
18,4
9)a
Type
2di
abet
esE
xp↑(
40,5
0–52
)↑(
40)
↑(40
)V
EG
Fne
utra
lizin
gan
tibo
dies
(53,
a)↓(
53)↔
(a)
↓(53
)↔
(a)
↓(53
)↔
(a)
↓BM
T(5
3)
↓(52
)aA
CE
inhi
biti
on,A
T1
anta
goni
sm(5
4)↓(
54)
↓VE
GF,
GS
(54)
Clin
↑(16
,b)
↓(58
)N
DN
D↓(
16)a
HP
NE
xpN
DN
DN
DV
EG
Fne
utra
lizin
gan
tibo
dies
(62)
↔/↓
(62)
↔K
idne
yIG
F-I
(62)
Clin
ND
ND
ND
ND
Nep
hron
redu
ctio
nE
xp↑(
64)
ND
ND
VE
GF
neut
raliz
ing
anti
bodi
es(6
3)↓(
63)
↔K
idne
yIG
F-I
(63)
↓(65
–68)
VE
GF
121
(66)
↑EC
prol
if,↑N
OS3
,↓F
(66)
AC
Ein
hibi
tion
(68)
↑GF
R(6
8)↓(
68)
↔(6
8)↑E
Cde
nsit
y,↑V
EG
F,↓G
S(6
8)C
linN
DN
DN
DN
DM
CN
Exp
↓(85
)↓(
85)
↓(85
)V
EG
F16
5an
tago
nizi
ngap
tam
er(3
6)↔
(36)
↔P
cul
tras
truc
ture
,↔
EC
fene
stra
tion
(36)
↑(86
)↑(
86)
↑(86
)C
lin↑(
18)
ND
ND
ND
↔(4
9,90
)M
GN
Exp
ND
ND
ND
VE
GF
165
anta
goni
zing
apta
mer
(36)
↔(3
6)↔
Pc
ultr
astr
uctu
re(3
6)
Clin
↔(1
8,90
)N
DN
DN
D↑(
49)b
↓(49
)a↓(
94)
TM
PG
NE
xp↑(
27,1
01)
ND
↑(27
,101
)V
EG
F16
5an
tago
nizi
ngap
tam
er(3
6)↓E
Cpr
olif,
↑GS
(36)
↓(10
3)+
UN
XV
EG
F16
5(1
04)
↑EC
prol
if(1
04)
Clin
↑(90
)b↑(
90)
↑(90
)N
D↓(
27,4
9,90
)a
CG
NE
xp↓(
105)
aN
DN
DV
EG
F16
5(c
)↑R
F(c
)↓(
c)↑E
Cpr
olif
(c)
Clin
↔(4
9,88
)bN
DN
DN
D↓(
49,8
8)a
FSG
SE
xp↓(
d)N
DN
DN
DC
lin↔
(49,
90)b
ND
ND
ND
↓(49
,90)
a
TM
A/H
US
Exp
↑(10
6)N
DN
DV
EG
F12
1(1
07,1
08)
↑RF
(107
)↑
Cap
illar
yre
cove
ry(1
07),
pres
erva
tion
(108
),↓F
(107
)C
lin↓(
e)T
↑(e)
↑(e)
ND
Acu
tere
ject
ion
Exp
ND
ND
ND
ND
Clin
↔(1
10)
ND
ND
ND
Chr
onic
reje
ctio
nE
xp↔
(111
)N
DN
DN
DC
lin↑(
20,1
10)
ND
ND
ND
↓(20
)a
2008 Schrijvers et al: VEGF in renal pathophysiology
Tabl
e1.
(Con
tinu
ed)
Eff
ects
Ren
alex
pres
sion
Man
ipul
atio
nof
GF
R/c
reat
ine
Dis
ease
VE
GF
VE
GF
R-1
VE
GF
R-2
VE
GF
axis
clea
ranc
e/R
FU
AE
KW
/GV
Oth
ers
Cyc
losp
orin
eE
xp↑(
112–
114)
↑(11
2–11
4)↑(
112–
114)
VE
GF
neut
raliz
ing
anti
bodi
es(1
15)
↓(11
5)↑
Dam
age,
BU
N,
hem
atur
ia(1
15)
neph
roto
xici
tyV
EG
F12
1(1
16)
↓Str
uctu
rald
amag
e(1
16)
AC
Ein
hibi
tion
,AT
1an
tago
nism
(113
)↓V
EG
F,↓V
EG
FR
-2,↓
F(1
13)
Clin
ND
ND
ND
ND
Cys
tic
kidn
eyE
xp↑(
117)
ND
ND
ND
dise
ases
Clin
↑(11
8)↑(
118)
↑(11
8)N
DIs
chem
ia/r
eper
fusi
onE
xp↔
(119
)↔
(120
)↑(
120)
ND
inju
ryC
linN
DN
DN
DN
DC
onge
nita
lNS
Exp
ND
ND
ND
ND
Clin
↔(1
21)
ND
↔(1
21)
ND
Lup
usne
phri
tis
Exp
ND
ND
ND
ND
Clin
↑(12
3)N
DN
DN
D↓(
49)
Abb
revi
atio
nsus
ed:
BM
T,ba
sem
ent
mem
bran
eth
ickn
ess;
CG
N,
cres
cent
icgl
omer
ulon
ephr
itis
;C
lin,
clin
ical
;D
M,
diab
etes
mel
litus
;E
C,
endo
thel
ial
cell;
Exp
,ex
peri
men
tal;
F,fib
rosi
s;F
SGS,
foca
lse
gmen
tal
glom
erul
oscl
eros
is;
GF
R,
glom
erul
arfil
trat
ion
rate
;G
S,gl
omer
ulos
cler
osis
;G
V,
glom
erul
arvo
lum
e;H
PN
,hi
ghpr
otei
n–in
duce
dne
phro
path
y;H
US,
hem
olyt
icur
emic
synd
rom
e;IG
F-I
,in
sulin
-lik
egr
owth
fact
orI;
KW
,kid
ney
wei
ght;
MC
N,m
inim
alch
ange
neph
ropa
thy;
MG
N,m
embr
anou
sgl
omer
ulon
ephr
itis
;MP
GN
,mes
angi
opro
lifer
ativ
egl
omer
ulon
ephr
itis
;NO
S3,e
ndot
helia
lni
tric
oxid
esy
ntha
se;P
c,po
docy
te;p
rolif
,pr
olif
erat
ion;
RF,
rena
lfun
ctio
n;T,
tubu
li;T
MA
,thr
ombo
tic
mic
roan
giop
athy
;UA
E,u
rina
ryal
bum
inex
cret
ion;
UN
X,u
nine
phre
ctom
y;↓r
educ
ed;↑
enha
nced
;↔no
chan
ge;N
D,n
oda
ta;(
a)ab
stra
ct;S
chri
jver
sB
F,J
Am
Soc
Nep
hrol
13:7
64A
,200
2;(b
)ab
stra
ct;K
anes
akiY
,JA
mSo
cN
ephr
ol13
:8A
,200
2;(c
)ab
stra
ct;S
him
izu
A,J
Am
Soc
Nep
hrol
13:3
6A,2
002;
(d)
abst
ract
;Kai
rait
isL
K,J
Am
Soc
Nep
hrol
13:3
36A
,200
2;(e
)ab
stra
ct;t
eL
ooD
M,J
Am
Soc
Nep
hrol
13:2
51A
,200
2.aSc
lero
tic
glom
erul
ior
cres
cent
sin
cres
cent
icgl
omer
ulon
ephr
itis
;bP
rese
rved
glom
erul
i.
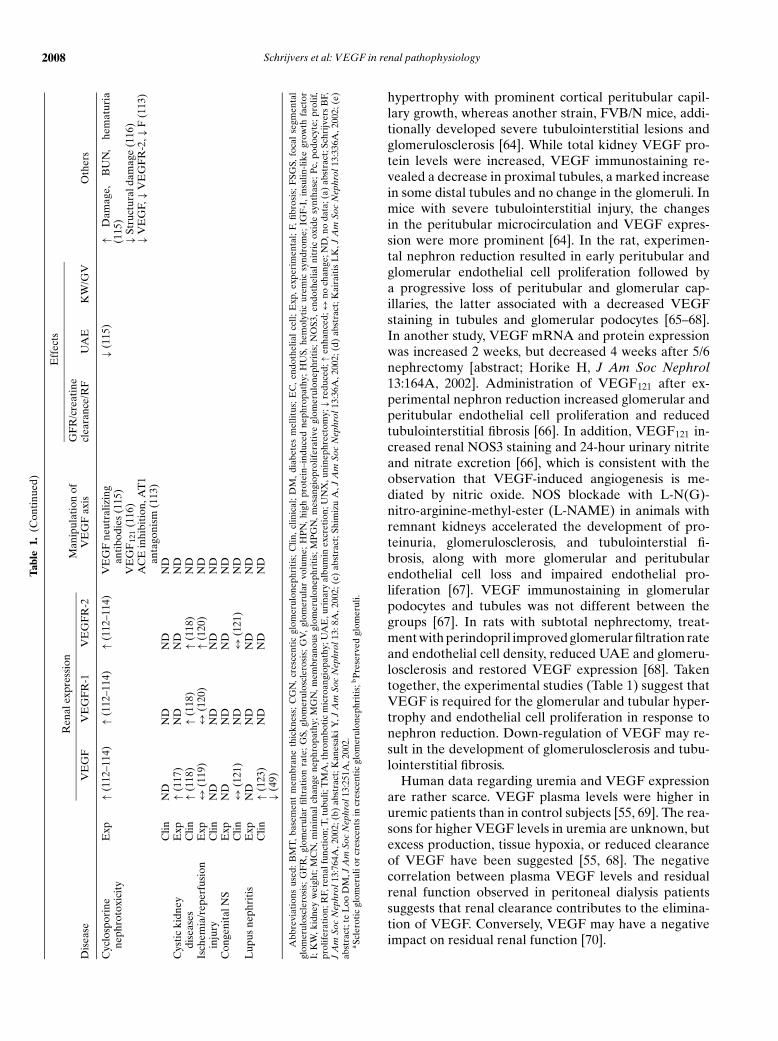
hypertrophy with prominent cortical peritubular capil-lary growth, whereas another strain, FVB/N mice, addi-tionally developed severe tubulointerstitial lesions andglomerulosclerosis [64]. While total kidney VEGF pro-tein levels were increased, VEGF immunostaining re-vealed a decrease in proximal tubules, a marked increasein some distal tubules and no change in the glomeruli. Inmice with severe tubulointerstitial injury, the changesin the peritubular microcirculation and VEGF expres-sion were more prominent [64]. In the rat, experimen-tal nephron reduction resulted in early peritubular andglomerular endothelial cell proliferation followed bya progressive loss of peritubular and glomerular cap-illaries, the latter associated with a decreased VEGFstaining in tubules and glomerular podocytes [65–68].In another study, VEGF mRNA and protein expressionwas increased 2 weeks, but decreased 4 weeks after 5/6nephrectomy [abstract; Horike H, J Am Soc Nephrol13:164A, 2002]. Administration of VEGF121 after ex-perimental nephron reduction increased glomerular andperitubular endothelial cell proliferation and reducedtubulointerstitial fibrosis [66]. In addition, VEGF121 in-creased renal NOS3 staining and 24-hour urinary nitriteand nitrate excretion [66], which is consistent with theobservation that VEGF-induced angiogenesis is me-diated by nitric oxide. NOS blockade with L-N(G)-nitro-arginine-methyl-ester (L-NAME) in animals withremnant kidneys accelerated the development of pro-teinuria, glomerulosclerosis, and tubulointerstial fi-brosis, along with more glomerular and peritubularendothelial cell loss and impaired endothelial pro-liferation [67]. VEGF immunostaining in glomerularpodocytes and tubules was not different between thegroups [67]. In rats with subtotal nephrectomy, treat-ment with perindopril improved glomerular filtration rateand endothelial cell density, reduced UAE and glomeru-losclerosis and restored VEGF expression [68]. Takentogether, the experimental studies (Table 1) suggest thatVEGF is required for the glomerular and tubular hyper-trophy and endothelial cell proliferation in response tonephron reduction. Down-regulation of VEGF may re-sult in the development of glomerulosclerosis and tubu-lointerstitial fibrosis.
Human data regarding uremia and VEGF expressionare rather scarce. VEGF plasma levels were higher inuremic patients than in control subjects [55, 69]. The rea-sons for higher VEGF levels in uremia are unknown, butexcess production, tissue hypoxia, or reduced clearanceof VEGF have been suggested [55, 68]. The negativecorrelation between plasma VEGF levels and residualrenal function observed in peritoneal dialysis patientssuggests that renal clearance contributes to the elimina-tion of VEGF. Conversely, VEGF may have a negativeimpact on residual renal function [70].
Schrijvers et al: VEGF in renal pathophysiology 2009
Glomerulonephritis
Minimal change nephropathy. Minimal changenephropathy (MCN) has been speculated to result fromthe release of soluble circulating factors by mononuclearcells that alter glomerular permeability. As VEGF maybe a regulator of glomerular permeability, the release ofVEGF by PBMC has been scrutinized. In cultured PBMCfrom patients with MCN, the effects of various cytokineson the secretion of VPF in the culture supernatant wereinvestigated [71–80]. VPF is an older term for VEGFand is determined by quantifying the intradermal per-meability in guinea pigs. Cultured PBMC, activated byconcanavalin-A or lipopolysaccharide, secreted VPF [71–82] and the VPF levels in the culture supernatant werehigher in PBMC from nephrotic MCN patients than frompatients in remission or control subjects [71–80]. IL-2,IL-12, IL-15, and IL-18 stimulated and TGF-b1, IL-4, IL-10, and IL-13 inhibited VPF release by activated PBMCfrom patients with MCN [71–79]. Patients treated withsteroids had lower VPF levels in PBMC supernatant thanuntreated patients [71–78]. In contrast, VEGF mRNAexpression in unstimulated PBMC was not different be-tween children with steroid-sensitive nephrotic syndrome(SSNS) in relapse and children with SSNS in remis-sion [83] or controls [84]. The potential role of VEGFin the development of proteinuria was also investigatedin experimental MCN [85, 86]. In puromycin aminonu-cleoside nephrosis (PAN) rats, an experimental modelof human MCN, the renal mRNA expression of VEGFand its receptors VEGFR-2 and VEGFR-1 was down-regulated [85]. In contrast, in hyperalbuminemia-inducedrat nephrosis, another model of human MCN, VEGF andits receptors were up-regulated and correlated with theseverity of proteinuria [86]. In PAN rats, treatment witha VEGF165 aptamer for 6 days did not affect proteinuria,podocyte swelling, foot-process fusion, or glomerular en-dothelial fenestrations [36], suggesting that VEGF165 isnot involved in the disease process, although a pathogenicrole for other isoforms is not excluded. Plasma VEGFconcentrations (free VEGF121 and VEGF165) andurine VEGF/creatinine ratios were not elevated duringrelapses of childhood SSNS when compared with remis-sion and normal controls [84]. Likewise, plasma or uri-nary VEGF levels were not different between patientswith MCN in the nephrotic state and those in remis-sion [83] or healthy controls [87, 88]. In contrast, urinaryVEGF levels were increased in patients with MCN withnephrotic syndrome when compared with patients with-out nephrotic syndrome and healthy controls, and corre-lated with the degree of proteinuria [89]. Urinary VEGFlevels decreased rapidly after steroid therapy [89]. Pa-tients with MCN in the nephrotic state and in remissiondisplayed a similar VEGF protein and mRNA expres-sion mainly localized in glomerular podocytes [90]. Incontrast, in situ hybridization revealed that VEGF
mRNA expression was up-regulated in podocytes inMCN and correlated with the urinary protein excretion[18]. In two patients with systemic lupus erythematosus(SLE) and minimal light microscopic changes VEGF ex-pression was normal [49]. The allele frequencies of thedinucleotide repeat polymorphisms within the VEGFR-1 gene were not different between patients with MCNand normal controls [91]. Similarly, polymorphisms in theVEGF gene promotor were not associated with the de-velopment of proteinuria in MCN [abstract; Watson CJ,J Am Soc Nephrol 9:A2497, 1998]. Further, the genotypefrequencies of the VEGF gene polymorphisms −460 C/T,−141 A/C, and +405 G/C were not different in childrenwith SSNS versus controls [92].
The lack of consistent alterations in the VEGF systemin experimental animals or patients with MCN (Table 1),does not allow firm conclusions to be drawn about therole of VEGF in the pathophysiology of MCN. Method-ologic difficulties may interfere with the correct interpre-tation of the results. PBMC in culture may be in anaerobicmetabolism, which may affect the expression of VEGF.Pitfalls in the determination of circulating VEGF lev-els have been described above. Further, high urinaryVEGF levels may merely reflect podocyte loss and uri-nary podocyte excretion [93] rather than an active in-volvement of VEGF in the disease process. It has evenbeen suggested that urinary VEGF may be derived fromthe circulation and as such may be nothing more than anassay for proteinuria [89].
Membranous glomerulonephritis. Cultured lympho-cytes from nephrotic membranous glomerulonephritis(MGN) subjects did not release VPF in their super-natants [82]. In rats with passive Heymann nephritis, anexperimental model of MGN, proteinuria, podocyte foot-process fusion and subepithelial immune deposits werenot affected by treatment with a VEGF165 aptamer for7 days [36]. Urinary VEGF excretion was decreased inpatients with idiopathic MGN compared with controlsubjects, but did not correlate with serum VEGF, renalfunction or proteinuria [48]. In the follow-up of some pa-tients, however, a reduction of proteinuria was associatedwith increasing urinary VEGF excretion and the changein proteinuria over one year correlated inversely with thechange in urinary VEGF [48]. As mentioned above, de-creased VEGF excretion in MGN may be explained bypodocyte injury and increased VEGF excretion duringclinical improvement by partial recovery of podocytes.In 10 nephrotic MGN patients with already a significantdegree of glomerulosclerosis, there was no difference inrenal VEGF mRNA expression compared with normalkidneys and no correlation between VEGF expressionand the degree of proteinuria [18]. Another study, in-cluding two patients with membranous nephropathy, oneidiopathic and one lupus nephritis class IV, reported kid-ney VEGF protein and mRNA expression to be similar

2010 Schrijvers et al: VEGF in renal pathophysiology
as in controls and localized mainly in podocytes [90]. Inthree other cases of MGN, VEGF mRNA and protein ex-pression was strong in relatively preserved glomeruli butdecreased or absent in sclerotic areas [49]. A recent studydemonstrated reduction of VEGF immunostaining in thetubular epithelium of MGN patients versus controls [94].The C allele of the VEGF −460 C/T polymorphism wasassociated with progression toward end-stage renal fail-ure in patients with idiopathic membranous nephropa-thy [abstract; Summers AM, J Am Soc Nephrol 13:260A,2002].
No consistent pattern of changes in the VEGF systememerges from these studies (Table 1). Difficulties withthe interpretation of urinary VEGF levels have been de-scribed above. The discrepant results of VEGF expres-sion in renal biopsies of patients with MGN are likelydue to differences in the degree of glomerulosclerosis, asloss of podocytes implicates loss of VEGF. It thus remainsunclear whether VEGF plays a role in the pathophysiol-ogy of MGN.
Membranoproliferative glomerulonephritis. ThePOEMS syndrome is a multisystemic syndrome charac-terized by polyneuropathy, organomegaly, endocrinopa-thy, M protein, and skin changes. Renal involvement canoccur and has been described as membranoproliferativeglomerulonephritis-like lesions [95]. Circulating VEGFlevels were elevated in POEMS syndrome comparedwith normal controls [96, 97] or with patients with pri-mary membranoproliferative glomerulonephritis [98].There was no difference in serum VEGF levels betweenPOEMS patients with and without renal involvement[98]. Further, serum VEGF levels in POEMS patientsdid not correlate with glomerular alterations [95].
Mesangioproliferative glomerulonephritis (MPGN).PBMC of patients with IgA nephropathy (IgAN) re-sponded similarly to cytokines as those of MCN pa-tients, with stimulation of VPF release by IL-2, IL-12,IL-15, and IL-18 and inhibition by TGF-b1, IL-4, IL-10, and IL-13 [71–78]. In contrast, VEGF mRNA lev-els in unstimulated PBMC were not different betweenIgAN patients and healthy volunteers and did notcorrelate with clinical or pathologic parameters [99].Incubation of human mesangial cells with aberrantly gly-cosylated IgA resulted in a down-regulation of VEGFmRNA expression and decreased VEGF release inthe culture medium [100]. During recovery of anti-Thy 1.1 nephritis, an experimental model of MPGN,up-regulation of VEGF mRNA in podocytes and themesangial region, and of VEGFR-2 mRNA in theglomerular capillary walls was associated with endothe-lial cell proliferation (Table 1) [27, 101]. In accordance,administration of a VEGF165 antagonizing aptamer re-duced glomerular endothelial cell proliferation and inhib-ited glomerular capillary repair resulting in glomerularsclerosis [36]. Glucocortocoids decreased VEGF releaseand aggravated proteinuria in anti-Thy 1.1 nephritic rats
possibly due to impairment of glomerular endothelialrepair [102, 103]. Rats with anti-Thy 1.1 nephritis com-bined with uninephrectomy [103] or Habu-snake venominjection [104] developed progressive glomerulosclerosisand renal insufficiency. In the former model, regenera-tion of glomerular endothelial cells and VEGF mRNAexpression were decreased [103]. In the latter model,the administration of recombinant human VEGF165 en-hanced endothelial cell proliferation and glomerularcapillary repair [104]. Serum VEGF levels were not dif-ferent in patients with IgAN compared with normal con-trols [87, 88]. In contrast, urinary VEGF levels wereincreased in patients with IgAN with nephrotic syndromewhen compared with patients without nephrotic syn-drome and healthy controls, and correlated with the de-gree of proteinuria [89]. In patients with MPGN due toIgAN, Henoch-Schonlein nephritis, non-IgA prolifera-tive glomerulonephritis and lupus nephritis, VEGF pro-tein and mRNA were expressed by glomerular podocytesand mesangial cells but were faint or absent in areas ofglomerulosclerosis (Table 1) [49, 90]. In patients withearly primary MPGN [90] or IgAN, expression of VEGFand its receptors was up-regulated, but in IgAN patientswith more severe interstitial damage, VEGF stainingwas decreased [abstract; Horike H, J Am Soc Nephrol13:164A, 2002] [27]. In patients with MPGN, includingIgAN, the presence of the VEGF −460 CC genotype orC allele was associated with progression toward end-stagerenal disease [abstract; Summers AM, J Am Soc Nephrol13:260A, 2002].
In conclusion, VEGF may be essential for glomerularrepair in MPGN. Depressed VEGF synthesis resultingfrom podocyte injury may contribute to endothelial cellloss and favor the development of glomerulosclerosis.
Crescentic glomerulonephritis. In mice with anti-glomerular basement membrane glomerulonephritis, anexperimental model of crescentic glomerulonephritis,loss of glomerular capillaries was temporally associatedwith decreased VEGF, VEGFR-2, Ang-1, and Tie2 im-munostaining and up-regulation of Ang-2, especially inglomeruli with crescents or sclerosis (Table 1) [105]. Inantiglomerular basement membrane glomerulonephritisrats, treatment with VEGF165 resulted in recovery of thenecrotizing and crescentic lesions, proliferation of en-dothelial cells and capillary repair, and improved renalfunction and proteinuria [abstract; Shimizu A, J Am SocNephrol 13:36A, 2002]. Serum VEGF levels were higherin patients with crescentic glomerulonephritis, includ-ing pauci-immune rapidly progressive glomerulonephri-tis, Henoch-Schonlein purpura nephritis and IgAN, thanin normal control subjects or in patients with MCN, IgAN,and focal segmental glomerular sclerosis (FSGS) [49, 87,88]. Serum VEGF levels correlated with crescent fre-quency, tubulointerstitial injury, and glomerular mono-cyte infiltration, but not with urinary protein excretion orserum creatinine levels [49, 87, 88]. Serum VEGF levels

Schrijvers et al: VEGF in renal pathophysiology 2011
decreased after corticosteroid therapy [49, 88]. VEGF ex-pression was normal in glomeruli with preserved architec-ture but decreased or absent in glomeruli compressed bycrescents and in sclerotic areas (Table 1) [49, 88]. Takentogether, the experimental data suggest that VEGFaccelerates glomerular recovery in crescentic glomeru-lonephritis. Further, for the first time, a role for angiopoi-etins in glomerular disease is suggested. Up-regulation ofAng-2 may be an appropriate adaptive response to pro-mote new vessel formation, but in the presence of lowVEGF levels it may contribute to endothelial apoptosisand vessel regression [14].
FSGS. VEGF mRNA expression in unstimulatedPBMC was higher in children with FSGS than in thosewith MCN but the difference was not significant [83].Rats developed proteinuria after the injection of the su-pernatant of cultured PBMC from FSGS patients sug-gesting that a “glomerular permeability factor” releasedfrom PBMC may change glomerular permeability andresult in proteinuria in FSGS [81]. In a murine FSGSmodel, adriamycin nephrosis, areas of interstitial expan-sion and tubular atrophy were associated with increasedstaining of hypoxia inducable factor-1 (HIF-1) in tubularand interstitial cells, reduced VEGF staining and loss ofcortical microvasculature [abstract; Kairaitis LK, J AmSoc Nephrol 13:336A, 2002). Plasma VEGF levels werehigher in proteinuric patients with FSGS than in thosewith MCNS but the difference was not significant [83].Serum VEGF levels in FSGS patients were not differentfrom those in control subjects [48, 87, 88]. Urinary VEGFexcretion, on the other hand, was higher than normalin patients with FSGS, but did not correlate with serumVEGF, renal function, or proteinuria [48]. In patientswith FSGS, VEGF protein and mRNA expression werenormal in preserved glomeruli but absent or very lowin glomeruli with segmental or global sclerosis (Table 1)[49, 90]. Rare polymorphisms in the VEGF gene promo-tor were not associated with the development of protein-uria in FSGS [abstract; Watson CJ, J Am Soc Nephrol9:A2497, 1998]. In contrast, the CC genotype and C al-lele of the more common −460 C/T polymorphism wereassociated with progression to end-stage renal disease inpatients with FSGS [abstract; Summers AM, J Am SocNephrol 13:260A, 2002].
The low renal VEGF expression and increased urinaryVEGF excretion in FSGS may be secondary to podocyteinjury and loss in the urine. No solid conclusions on therole of VEGF in the pathophysiology of FSGS can thusbe drawn.
Thrombotic microangiopathy (TMA)/hemolyticuremic syndrome (HUS)
A rat model of renal TMA with histologic featuressimilar to human HUS was induced by antiglomerularendothelial cell antibodies which produced loss of
glomerular and peritubular capillary endothelium [106].An early transient increase in VEGF immunostain-ing was observed in glomerular podocytes and corti-cal tubules, but despite proliferation of glomerular andperitubular endothelial cells, progressive glomerular andtubulointerstitial damage, and renal failure developed[106]. The hypothesis that angiogenic growth factors mayaccelerate recovery of renal microvascular injury wasstudied in experimental TMA (Table 1) [107, 108]. Sub-cutanous administration of VEGF121 resulted in greaterrecovery of the renal microvasculature together with abetter renal function and less tubulointerstitial fibrosis[107]. VEGF121-treated rats had higher urinary nitritesand nitrates excretion, suggesting that the angiogenic ef-fects of VEGF were mediated by nitric oxide [107]. Ina more severe form of renal TMA in rats with acutemassive renal infarction, VEGF administration resultedin reduced glomerular endothelial cell apoptosis, pre-served microvascular endothelium and less cortical andmedullary necrosis [108]. Elevated serum and plasmaVEGF levels were found in HUS patients compared withcontrols and correlated with the severity of the disease[abstract; te Loo DM, J Am Soc Nephrol 13:251A, 2002].In three patients with HUS, immunohistochemistry ofrenal biopsy material showed increased VEGFR-1 andVEGFR-2 in the glomeruli, and absent VEGF stainingin tubuli compared to controls [abstract; te Loo DM, J AmSoc Nephrol 13:251A, 2002). In conclusion, VEGF maybe required for glomerular and tubulointerstitial repairin TMA.
Renal transplantation
Acute rejection. To study the possible relationshipsbetween VEGF gene polymorphisms and the risk ofacute renal allograft rejection, single nucleotide substi-tutions in the VEGF gene were identified in 173 whiterenal allograft recipients [109]. The correlation betweenVEGF gene polymorphisms and VEGF production wasinvestigated in vitro in PBMC from healthy individuals.Homozygotes with −1154G/G genotype and −2578C/Cgenotype showed the greatest risk of rejection and hadthe highest production of VEGF by stimulated PBMCfrom healthy volunteers, as compared with −1154A/Aand −2578A/A genotypes, respectively. Heterozygoteswith −1154G/A and −2578C/A genotypes demonstratedan intermediate risk. In biopsies of patients with acuterejection or temporary allograft dysfunction, VEGF im-munostaining appeared to be quite similar to that of nor-mal human kidney, but biopsies from normal kidneyswere not included in this study (Table 1) [110].
Chronic rejection. In the Fischer (F344) donor toLewis recipient rat renal allograft, a well-established ex-perimental model of chronic allograft rejection, no dif-ferences in VEGF mRNA expression were observedbetween allografts and isografts at any time. VEGF

2012 Schrijvers et al: VEGF in renal pathophysiology
expression did not correlate with the extent ofmacrophage or myofibroblast infiltration [111]. In kid-neys from four patients with chronic vascular rejection,VEGF mRNA and protein expression was increasedcompared with normal kidneys, most notably in prox-imal and distal tubular cells and interstitial cells andto a lesser extent in vascular smooth muscle cells andthe mononuclear inflammatory infiltrate [20]. Viableglomerular podocytes displayed marked VEGF mRNAexpression, but VEGF mRNA labeling was reducedor absent in sclerosed glomeruli [20]. Similarly, in-creased renal VEGF protein expression was observedin glomerular podocytes and mesangial cells, vascu-lar smooth muscle cells, and some endothelial cellsand tubulointerstitium of kidneys in 17 patients withchronic renal allograft rejection, particularly in intersti-tial cells likely to be macrophages [110]. Renal VEGFimmunostaining was increased in patients with chronicrejection when compared with patients with acute re-jection or temporary allograft dysfunction [110]. The in-creased VEGF expression in glomeruli and particularlyinterstitium of human kidneys with chronic allograft re-jection may be induced by hypoxia, as a consequenceof reduced blood flow [20]. Other hypotheses for theup-regulation of VEGF include production of VEGF bymacrophages or proliferating glomerular mesangial cells[110]. Alternatively, VEGF may contribute to the recruit-ment of macrophages into the interstitium.
Cyclosporine nephrotoxicity. In a rat model of chroniccyclosporine nephrotoxicity, VEGF mRNA and proteinexpression as well as VEGFR-1 and VEGFR-2 mRNAexpression were up-regulated as early as 7 days after ex-posure (Table 1) [112–114]. The increased VEGF andVEGFR-1 expression continued until day 28, whereasVEGFR-2 expression declined but remained higher thanin control rats [112, 113]. Immunostaining for VEGF wasparticularly strong in proximal and distal tubular cells andoccasionally in glomerular podocytes [113]. Treatmentwith enalapril or losartan improved the tubulointerstitialfibrosis and afferent arteriolopathy, and decreased VEGFmRNA and protein expression and VEGFR-2 mRNA ex-pression [113]. L-NAME worsened both glomerular fil-tration rate and cyclosporine-induced interstitial fibrosisand arteriolopathy, and further increased VEGF mRNAand protein expression while L-arginine had the oppo-site effect, suggesting that nitric oxide down-regulatesVEGF expression in cyclosporine nephrotoxicity [114].In a mouse model of acute cyclosporine toxicity, spe-cific blockade of VEGF by a monoclonal antibody in-creased the deleterious effects of cyclosporine on the kid-ney [115]. Mice treated with the VEGF-antibody showedenhanced tubular toxicity, more apoptotic nuclei, in-creased blood urea nitrogen and hematuria comparedwith mice treated with cyclosporine alone or with cy-closporine and an irrelevant IgG [115]. However, urinary
protein excretion was higher in cyclosporine-treated micethan in cyclosporine and VEGF-antibody–treated mice[115]. In vitro, the cyclosporine-induced toxicity in cul-tured murine proximal tubular epithelial cells also in-creased in the presence of a VEGF antibody [115]. Ina rat model of chronic cyclosporine nephrotoxicity, ad-ministration of exogenous VEGF121 resulted in renopro-tective effects (i.e., osteopontin expression, macrophageinfiltration, collagen III deposition were decreased versuscontrol rats and afferent arteriolopathy was dramaticallyimproved) [116]. Treatment with VEGF121 also loweredblood pressure, which was suggested to be mediated bythe accelerated recovery from tubulointerstitial and mi-crovascular injury in VEGF-treated rats [116]. The roleof VEGF in human cyclosporine nephrotoxocity has notbeen evaluated.
In summary, the expression of the VEGF system isincreased in experimental cyclosporine nephrotoxicity.VEGF-blockade aggravated and VEGF-administrationameliorated the cyclosporine-induced injury, suggestinga role for VEGF in the repair process induced by cy-closporine nephrotoxicity.
Other kidney diseases
Cystic kidney diseases. One experimental study inves-tigated the expressions of VEGF, HIF-1a and HIF-3ain polycystic kidney lesions that occurred spontaneouslyin two rats [117]. Compared with the kidneys of controlrats, VEGF protein expression was increased in the innerstripe of the outer medulla where cystic alterations wereprominent. HIF-1a and HIF-3a protein expressions wereincreased in proximal tubuli and in the thin loop of Henle,respectively. In kidneys from 14 patients with autosomal-dominant polycystic kidney disease (ADPKD), increasedangiogenesis was identified, especially in the cyst wallsand around the cysts [118]. In addition, VEGF proteinwas expressed in the epithelial cysts cells, VEGFR-2 pro-tein in some capillaries surrounding the cysts and someglomeruli, whereas VEGFR-1 was expressed irregularlyin some cyst cells and remnant tubular cells. Furthermore,VEGF165 was demonstrated in cultured ADPKD cellsand in their supernatant, and VEGF secretion was in-creased during hypoxia [118]. In patients with acquiredcystic kidney disease, IL-6, IL-8, and VEGF concentra-tions were higher in the cyst fluid than in the blood, andhigher than in patients with other cystic nephropathies(i.e., ADPKD or renal cell carcinoma). Taken together,these findings suggest an angiogenic role for VEGF in thepathogenesis of cystic kidney diseases, likely triggered bylocal hypoxia [117] and involving the development of apericystic circulation which may be necessary for cyst cellsto grow [118].
Ischemia/reperfusion injury. Cultured rat kidneytubular epithelial cells subjected to hypoxia showed

Schrijvers et al: VEGF in renal pathophysiology 2013
increased VEGF staining in the periphery of the cells[119]. In a rat model of renal ischemia/reperfusion injury,whole kidney VEGF mRNA and protein expression wasnot increased following ischemia or ischemia and reper-fusion, although preexisting VEGF in tubular epithelialcells redistributed from the cytoplasm to the basolateralsurface [119]. Further, VEGFR-1 mRNA expression wasnot changed, whereas VEGFR-2 mRNA expression wasup-regulated most prominent in glomerular endothelialcells and peritubular capillaries, but also in some tubu-lar epithelial cells [120]. It was speculated that the in-creased VEGFR-2 expression in peritubular capillariesduring ischemia/reperfusion injury may direct the effectsof VEGF released by ischemic tubular epithelial cells toadjacent endothelial cells in order to preserve the cap-illary blood supply and to promote tubular cell survivaland recovery [120].
Congenital nephrotic syndrome of the Finnish type. Inkidney samples of infants with congenital nephrotic syn-drome of the Finnish type, expression and localization ofVEGF and VEGFR-2 mRNA was similar to normal adulthuman kidney [121]. VEGF protein expression was alsonot different from normal kidneys except for an intensejuxtaglomerular staining [121].
Lupus nephritis. VEGF mRNA in PBMC of patientswith SLE did not differ from those of controls [122].VEGF plasma levels were higher in SLE patients than incontrols, and SLE patients with renal failure had higherlevels than those with normal renal function [123]. VEGFprotein expression was increased in distal tubules, col-lecting ducts and some podocytes in SLE patients withmoderate renal failure [123]. In two cases of SLE withdiffuse endocapillary proliferative glomerulonephritis,renal VEGF expression was reduced [49].
Wegener’s granulomatosis. Serum VEGF levels werehigher in patients with Wegener’s granulomatosis thanin normal controls [124]. Serum VEGF levels weremarkedly elevated in patients with major disease versusminor disease activity, suggesting that VEGF may be amarker of disease activity [124].
Renal cell carcinoma. VEGF promotes the growthof renal cell carcinoma, by virtue of its angiogenesis-inducing potential [125]. A detailed description of therole of VEGF in renal cell carcinoma is, however, beyondthe scope and space limitations of this review.
INTERFERENCE WITH THE VEGF AXIS
Several strategies exist to target VEGF and its re-ceptors, including VEGF neutralizing antibodies, VEGFantagonizing aptamers, VEGF receptor-blocking anti-bodies, VEGF receptor antagonists, and angiopoietins[126]. So far, the experience with these treatments inrenal disease is limited to animal models. A human-ized anti-VEGF monoclonal antibody (bevacizumab)
and an anti-VEGF pegylated aptamer (EYE001) are cur-rently evaluated in clinical trials to treat various typesof cancer, as well as macular degeneration and dia-betic retinopathy [127, 128]. VEGF receptor antagonistsare also available. SU5416 and ZM323881 are specificfor VEGFR-2, whereas PTK787/ZK222584 inhibits bothVEGFR-1 and VEGFR-2 [126]. Other strategies to re-duce VEGF-mediated effects, including placenta growthfactor inhibition and drugs that interfere with signalingmolecules in the VEGF signal transduction pathway suchas Src/Fyn kinase inhibitors, are in development or inearly stages of testing [126]. Targeting specific VEGF sig-naling molecules might be a way to distinctively inhibitspecific actions of VEGF.
Interference with the renin-angiotensin system may bean indirect means to affect the VEGF axis, but the in-teraction between both systems is complex. In culturedmesangial cells angiotensin II induced VEGF expression[129], whereas in tubular epithelial cells angiotensin IIdiminished VEGF expression [65]. In agreement, diver-gent effects have been reported with in vivo blockadeof the renin-angiotensin system. Angiotensin-convertingenzyme (ACE) inhibition or AT1 antagonism reducedVEGF expression in diabetic nephropathy [54] and incyclosporine nephrotoxicity [113], suggesting that AT1may be involved in the VEGF overexpression observedin these pathologies. In contrast, ACE inhibition was as-sociated with an increased VEGF expression in the rem-nant kidney [68].
CONCLUSION
The strategic localization of VEGF in the vicinity of thefiltration barrier and its known effects on microvascularpermeability have engendered the hypothesis that VEGFcontrols glomerular permeability in the normal adult kid-ney and induces proteinuria in pathologic conditions. Al-though a large number of studies have been designed toexamine this hypothesis, none has been able to firmlysupport it. Correlations of plasma or urinary VEGF lev-els with proteinuria in diverse glomerular pathologieshave been inconsistent. Positive correlations between uri-nary VEGF levels and proteinuria may relate to urinarypodocyte loss rather than to a causative link betweenrenal up-regulation of VEGF and development ofproteinuria. The inhibition of VEGF in experimentalglomerulonephritis did not affect proteinuria. The laud-able effect of VEGF-blockade on proteinuria in experi-mental diabetes may be indirect through inhibition of thedisease process. Finally, podocyte-specific overexpressionof VEGF caused a collapsing glomerulopathy rather thanproteinuria.
The paramount task of VEGF in the adult glomerulusappears to be the stimulation of capillary endothelial cellgrowth and proliferation. This may be inappropriate in

2014 Schrijvers et al: VEGF in renal pathophysiology
diabetic nephropathy where it contributes to glomerularhypertrophy and hyperfiltration, but may be an essentialrepair mechanism in glomerulonephritis and TMA. Sim-ilarly, tubular cells may respond to hypoxia or injury withthe production of VEGF that stimulates proliferation ofperitubular capillaries in order to overcome the tubulardamage.
As the VEGF system is affected in a wide variety of kid-ney diseases, interventions to manipulate VEGF may bepromising therapeutic tools. Several strategies to eitherinhibit or enhance the VEGF axis have shown promisingresults in animal models of renal disease, but no data inhumans are presently available.
The VEGF gene is highly polymorphic and certainpolymorphisms may be associated with alterations inthe expression of VEGF. Although the diagnostic im-portance of genotyping renal patients remains to beestablished, some VEGF polymorphisms may developinto useful markers of disease susceptibility and/orprogression.
ACKNOWLEDGMENTS
B. Schrijvers is supported by the Institute for the Promotion ofInnovation by Science and Technology in Flanders (IWT), A. Flyvb-jerg is supported by the Danish Diabetes Association, the Eva andHenry Frænkels Memorial Foundation, and the Danish Medical Re-search Council.
Reprint requests to An De Vriese, Renal Unit, AZ Sint-Jan AV Rud-dershove 10, B-8000 Brugge, Belgium.E-mail: [email protected]
REFERENCES
1. FERRARA N, GERBER HP: The role of vascular endothelial growthfactor in angiogenesis. Acta Haematol 106:148–156, 2001
2. NEUFELD G, COHEN T, GENGRINOVITCH S, POLTORAK Z: Vascularendothelial growth factor (VEGF) and its receptors. FASEB J13:9–22, 1999
3. WHITTLE C, GILLESPIE K, HARRISON R, et al: Heterogeneous vascu-lar endothelial growth factor (VEGF) isoform mRNA and recep-tor mRNA expression in human glomeruli, and the identificationof VEGF148 mRNA, a novel truncated splice variant. Clin Sci97:303–312, 1999
4. HORNIG C, BARLEON B, AHMAD S, et al: Release and complex for-mation of soluble VEGFR-1 from endothelial cells and biologialfluids. Lab Invest 80:443–54, 2000
5. NAKAMURA F, GOSHIMA Y: Structural and functional relation ofneuropilins. Adv Exp Med Biol 515:55–69, 2002
6. HOOD JD, MEININGER CJ, ZICHE M, GRANGER HJ: VEGF upregu-lates ecNOS message, protein, and NO production in human en-dothelial cells. Am J Physiol 274:H1054–H1058, 1998
7. TILTON RG, CHANG KC, LEJEUNE WS, et al: Role for nitric oxidein the hyperpermeability and hemodynamic changes induced byintravenous VEGF. Invest Ophthalmol Vis Sci 40:689–696, 1999
8. TSURUMI Y, MUROHARA T, KRASINSKI K, et al: Reciprocal relationbetween VEGF and NO in the regulation of endothelial integrity.Nat Med 3:879–886, 1997
9. WATSON CJ, WEBB NJ, BOTTOMLEY MJ, BRENCHLEY PE: Identifi-cation of polymorphisms within the vascular endothelial growthfactor (VEGF) gene: Correlation with variation in VEGF proteinproduction. Cytokine 12:1232–1235, 2000
10. AWATA T, INOUE K, KURIHARA S, et al: A common polymorphism inthe 5′-untranslated region of the VEGF gene is associated with di-abetic retinopathy in type 2 diabetes. Diabetes 51:1635–1639, 2002
11. STEVENS A, SODEN J, BRENCHLEY PE, et al: Haplotype analysis ofthe polymorphic human vascular endothelial growth factor genepromoter. Cancer Res 63:812–816, 2003
12. YANG B, CROSS DF, OLLERENSHAW M, et al: Polymorphisms of thevascular endothelial growth factor and susceptibility to diabeticmicrovascular complications in patients with type 1 diabetes mel-litus. J Diabetes Complications 17:1–6, 2003
13. SATCHELL SC, MATHIESON PW: Angiopoietins: Microvascular mod-ulators with potential roles in glomerular pathophysiology. JNephrol 16:168–178, 2003
14. LOBOV IB, BROOKS PC, LANG RA: Angiopoietin-2 displays VEGF-dependent modulation of capillary structure and endothelial cellsurvival in vivo. Proc Natl Acad Sci USA 99:11205–11210, 2002
15. ROBERT B, ABRAHAMSON DR: Control of glomerular capillarydevelopment by growth factor/receptor kinases. Pediatr Nephrol16:294–301, 2001
16. CHA DR, KIM NH, YOON JW, et al: Role of vascular endothe-lial growth factor in diabetic nephropathy. Kidney Int 58 (Suppl77):S104–S112, 2000
17. IIJIMA K, YOSHIKAWA N, CONNOLLY DT, NAKAMURA H: Humanmesangial cells and peripheral blood mononuclear cells producevascular permeability factor. Kidney Int 44:959–966, 1993
18. BAILEY E, BOTTOMLEY MJ, WESTWELL S, et al: Vascular endothelialgrowth factor mRNA expression in minimal change, membranous,and diabetic nephropathy demonstrated by non-isotopic in situhybridisation. J Clin Pathol 52:735–738, 1999
19. COOPER ME, VRANES D, YOUSSEF S, et al: Increased renal expres-sion of vascular endothelial growth factor (VEGF) and its receptorVEGFR-2 in experimental diabetes. Diabetes 48:2229–2239, 1999
20. GRONE HJ, SIMON M, GRONE EF: Expression of vascular endothe-lial growth factor in renal vascular disease and renal allografts. JPathol 177:259–267, 1995
21. KANG DH, ANDERSON S, KIM YG, et al: Impaired angiogene-sis in the aging kidney: Vascular endothelial growth factor andthrombospondin-1 in renal disease. Am J Kidney Dis 37:601–611,2001
22. KRETZLER M, SCHROPPEL B, MERKLE M, et al: Detection of mul-tiple vascular endothelial growth factor splice isoforms in singleglomerular podocytes. Kidney Int 41 (Suppl 67):S159–S161, 1998
23. SIMON M, GRONE HJ, JOHREN O, et al: Expression of vascular en-dothelial growth factor and its receptors in human renal ontogen-esis and in adult kidney. Am J Physiol 268:F240–F250, 1995
24. SATCHELL SC, HARPER SJ, TOOKE JE, et al: Human podocytes ex-press angiopoietin 1, a potential regulator of vascular endothelialgrowth factor. J Am Soc Nephrol 13:544–550, 2002
25. AMEMIYA T, SASAMURA H, MIFUNE M, et al: Vascular endothelialgrowth factor activates MAP kinase and enhances collagen syn-thesis in human mesangial cells. Kidney Int 56:2055–2063, 1999
26. TAKAHASHI T, SHIRASAWA T, MIYAKE K, et al: Protein tyrosine ki-nases expressed in glomeruli and cultured glomerular cells: Flt-1and VEGF expression in renal mesangial cells. Biochem BiophysRes Commun 209:218–226, 1995
27. THOMAS S, VANUYSTEL J, GRUDEN G, et al: Vascular endothelialgrowth factor receptors in human mesangium in vitro and inglomerular disease. J Am Soc Nephrol 11:1236–1243, 2000
28. TRACHTMAN H, FUTTERWEIT S, FRANKI N, SINGHAL PC: Effect of vas-cular endothelial growth factor on nitric oxide production by cul-tured rat mesangial cells. Biochem Biophys Res Commun 245:443–446, 1998
29. KANELLIS J, FRASER S, KATERELOS M, POWER DA: Vascular en-dothelial growth factor is a survival factor for renal tubular epithe-lial cells. Am J Physiol Renal Physiol 278:F905–F915, 2000
30. HARPER SJ, XING CY, WHITTLE C, et al: Expression of neuropilin-1by human glomerular epithelial cells in vitro and in vivo. Clin Sci101:439–446, 2001
31. FOSTER RR, HOLE R, ANDERSON K, et al: Functional evidence thatvascular endothelial growth factor may act as an autocrine factoron human podocytes. Am J Physiol Renal Phsysiol 284:F1263–F1273, 2003
32. VILLEGAS G, TUFRO A: Ontogeny of semaphorins 3A and 3F andtheir receptors neuropilins 1 and 2 in the kidney. Gene Expr Pat-terns 2:151–155, 2002
33. SIMON M, ROCKL W, HORNIG C, et al: Receptors of vascular
Schrijvers et al: VEGF in renal pathophysiology 2015
endothelial growth factor/vascular permeability factor(VEGF/VPF) in fetal and adult human kidney: Localizationand [125I] VEGF binding sites. J Am Soc Nephrol 9:1032–1044,1998
34. KLANKE B, SIMON M, ROCKL W, et al: Effects of vascular endothe-lial growth factor (VEGF)/vascular permeability factor (VPF) onhaemodynamics and permselectivity of the isolated perfused ratkidney. Nephrol Dial Transplant 13:875–885, 1998
35. DE VRIESE AS, TILTON RG, ELGER M, et al: Antibodies againstvascular endothelial growth factor improve early renal dysfunctionin experimental diabetes. J Am Soc Nephrol 12:993–1000, 2001
36. OSTENDORF T, KUNTER U, EITNER F, et al: VEGF(165) mediatesglomerular endothelial repair. J Clin Invest 104:913–923, 1999
37. EREMINA V, SOOD M, HAIGH J, et al: Glomerular-specific alterationsof VEGF-A expression lead to distinct congenital and acquiredrenal diseases. J Clin Invest 111:707, 2003
38. BRAUN L, KARDON T, REISZ-PORSZASZ ZS, et al: The regulation ofthe induction of vascular endothelial growth factor at the onsetof diabetes in spontaneously diabetic rats. Life Sci 69:2533–2542,2001
39. CHENG HF, WANG CJ, MOECKEL GW, et al: Cyclooxygenase-2 in-hibitor blocks expression of mediators of renal injury in a modelof diabetes and hypertension. Kidney Int 62:929–939, 2002
40. CHOU E, SUZUMA I, WAY KJ, et al: Decreased cardiac expres-sion of vascular endothelial growth factor and its receptors ininsulin-resistant and diabetic states: A possible explanation for im-paired collateral formation in cardiac tissue. Circulation 105:373–379, 2002
41. CHIARELLI F, SPAGNOLI A, BASCIANI F, et al: Vascular endothelialgrowth factor (VEGF) in children, adolescents and young adultswith type 1 diabetes mellitus: Relation to glycaemic control andmicrovascular complications. Diabet Med 17:650–656, 2000
42. MCLAREN M, ELHADD TA, GREENE SA, BELCH JJ: Elevated plasmavascular endothelial cell growth factor and thrombomodulin injuvenile diabetic patients. Clin Appl Thromb Hemost 5:21–24,1999
43. DIAMANT M, HANEMAAIJER R, VERHEIJEN JH, et al: Elevated matrixmetalloproteinase-2 and -9 in urine, but not in serum, are markersof type 1 diabetic nephropathy. Diabet Med 18:423–424, 2001
44. MALAMITSI-PUCHNER A, SARANDAKOU A, TZIOTIS J, et al: Serumlevels of basic fibroblast growth factor and vascular endothelialgrowth factor in children and adolescents with type 1 diabetesmellitus. Pediatr Res 44:873–875, 1998
45. HOVIND P, TARNOW L, OESTERGAARD PB, PARVING HH: Elevatedvascular endothelial growth factor in type 1 diabetic patients withdiabetic nephropathy. Kidney Int 57 (Suppl 75):S56–S61, 2000
46. CHATURVEDI N, FULLER JH, POKRAS F, et al: Circulating plasmavascular endothelial growth factor and microvascular complica-tions of type 1 diabetes mellitus: The influence of ACE inhibition.Diabet Med 18:288–294, 2001
47. BRAUSEWETTER F, JEHLE PM, JUNG MF, et al: Microvascular per-meability is increased in both types of diabetes and correlates dif-ferentially with serum levels of insulin-like growth factor I (IGF-I)and vascular endothelial growth factor (VEGF). Horm Metab Res33:713–720, 2001
48. HONKANEN EO, TEPPO AM, GRONHAGEN-RISKA C: Decreased uri-nary excretion of vascular endothelial growth factor in idiopathicmembranous glomerulonephritis. Kidney Int 57:2343–2349, 2000
49. SHULMAN K, ROSEN S, TOGNAZZI K, et al: Expression of vascularpermeability factor (VPF/VEGF) is altered in many glomerulardiseases. J Am Soc Nephrol 7:661–666, 1996
50. ZIYADEH FN, HOFFMAN BB, HAN DC, et al: Long-term preventionof renal insufficiency, excess matrix gene expression, and glomeru-lar mesangial matrix expansion by treatment with monoclonal an-titransforming growth factor-b antibody in db/db diabetic mice.Proc Natl Acad Sci USA 97:8015–8020, 2000
51. TSUCHIDA K, MAKITA Z, YAMAGISHI S, et al: Suppression of trans-forming growth factor beta and vascular endothelial growth factorin diabetic nephropathy in rats by a novel advanced glycation endproduct inhibitor, OPB-9195. Diabetologia 42:579–588, 1999
52. HOSHI S, SHU Y, YOSHIDA F, et al: Podocyte injury promotes pro-gressive nephropathy in zucker diabetic fatty rats. Lab Invest82:25–35, 2002
53. FLYVBJERG A, DAGNÆS-HANSEN F, DE VRIESE AS, et al: Ameliora-tion of long-term renal changes in obese type 2 diabetic mice by aneutralizing vascular endothelial growth factor antibody. Diabetes51:3090–3094, 2002
54. KOGA K, YAMAGISHI S, TAKEUCHI M, et al: CS-886, a new angiotensinII type 1 receptor antagonist, ameliorates glomerular anionic siteloss and prevents progression of diabetic nephropathy in OtsukaLong-Evans Tokushima fatty rats. Mol Med 8:591–599, 2002
55. WASADA T, KAWAHARA R, KATSUMORI K, et al: Plasma concentra-tion of immunoreactive vascular endothelial growth factor and itsrelation to smoking. Metabolism 47:27–30, 1998
56. BLANN AD, BELGORE FM, MCCOLLUM CN, et al: Vascular endothe-lial growth factor and its receptor, Flt-1, in the plasma of patientswith coronary or peripheral atherosclerosis, or type II diabetes.Clin Sci 102:187–194, 2002
57. SHIMADA K, BABA T, NEUGEBAUER S, et al: Plasma vascular en-dothelial growth factor in Japanese type 2 diabetic patients withand without nephropathy. J Diabetes Complications 16:386–390,2002
58. BORTOLOSO E, DEL PRETE D, GAMBARO G, et al: Vascular en-dothelial growth factor (VEGF) and VEGF receptors in diabeticnephropathy: Expression studies in biopsies of type 2 diabetic pa-tients. Ren Fail 23:483–493, 2001
59. JELKMANN W: Pitfalls in the measurement of circulating vascularendothelial growth factor. Clin Chem 47:617–623, 2001
60. BANKS RE, FORBES MA, KINSEY SE, et al: Release of the angio-genic cytokine vascular endothelial growth factor (VEGF) fromplatelets: Significance for VEGF measurements and cancer biol-ogy. Br J Cancer 77:956–964, 1998
61. NIELSEN HJ, WERTHER K, MYNSTER T, BRUNNER N: Soluble vascu-lar endothelial growth factor in various blood transfusion compo-nents. Transfusion 39:1078–1083, 1999
62. SCHRIJVERS BF, RASCH R, TILTON RG, FLYVBJERG A: High protein-induced glomerular hypertrophy is vascular endothelial growthfactor-dependent. Kidney Int 61:1600–1604, 2002
63. FLYVBJERG A, SCHRIJVERS BF, DE VRIESE AS, et al: Compensatoryglomerular growth after unilateral nephrectomy is VEGF depen-dent. Am J Physiol Endocrinol Metab 283:E362–E366, 2002
64. PILLEBOUT E, BURTIN M, YUAN HT, et al: Proliferation and remod-eling of the peritubular microcirculation after nephron reduction:Association with the progression of renal lesions. Am J Pathol159:547–560, 2001
65. KANG DH, JOLY AH, OH SW, et al: Impaired angiogenesis in theremnant kidney model: I. Potential role of vascular endothelialgrowth factor and thrombospondin-1. J Am Soc Nephrol 12:1434–1447, 2001
66. KANG DH, HUGHES J, MAZZALI M, et al: Impaired angiogenesis inthe remnant kidney model: II. Vascular endothelial growth factoradministration reduces renal fibrosis and stabilizes renal function.J Am Soc Nephrol 12:1448–1457, 2001
67. KANG DH, NAKAGAWA T, FENG L, JOHNSON RJ: Nitric oxide mod-ulates vascular disease in the remnant kidney model. Am J Pathol161:239–248, 2002
68. KELLY DJ, HEPPER C, WU LL, et al: Vascular endothelial growthfactor expression and glomerular endothelial cell loss in theremnant kidney model. Nephrol Dial Transplant 18:1286–1292,2003
69. HARPER SJ, DOWNS L, TOMSON CR, et al: Elevated plasma vas-cular endothelial growth factor levels in non-diabetic predialysisuraemia. Nephron 90:341–343, 2002
70. STOMPOR T, ZDZIENICKA A, MOTYKA M, et al: Selected growth fac-tors in peritoneal dialysis: Their relationship to markers of inflam-mation, dialysis adequacy, residual renal function, and peritonealmembrane transport. Perit Dial Int 22:670–676, 2002
71. MATSUMOTO K, OHI H, KANMATSUSE K: Interleukin 10 and inter-leukin 13 synergize to inhibit vascular permeability factor releaseby peripheral blood mononuclear cells from patients with lipoidnephrosis. Nephron 77:212–218, 1997
72. MATSUMOTO K: Interleukin 10 inhibits vascular permeability fac-tor release by peripheral blood mononuclear cells in patients withlipoid nephrosis. Nephron 75:154–159, 1997
73. MATSUMOTO K, OHI H, KANMATSUSE K: Interleukin-4 cooperateswith interleukin-10 to inhibit vascular permeability factor release
2016 Schrijvers et al: VEGF in renal pathophysiology
by peripheral blood mononuclear cells from patients with minimal-change nephrotic syndrome. Am J Nephrol 19:21–27, 1999
74. MATSUMOTO K, OHI H, KANMATSUSE K: Interleukin 12 upregulatesthe release of vascular permeability factor by peripheral bloodmononuclear cells from patients with lipoid nephrosis. Nephron78:403–409, 1998
75. MATSUMOTO K, OHI H, KANMATSUSE K: Effects of interleukin-15 onvascular permeability factor release by peripheral blood mononu-clear cells in normal subjects and in patients with minimal-changenephrotic syndrome. Nephron 82:32–38, 1999
76. MATSUMOTO K, KANMATSUSE K: Interleukin-15 and interleukin-12have an additive effect on the release of vascular permeabilityfactor by peripheral blood mononuclear cells in normals and inpatients with nephrotic syndrome. Clin Nephrol 52:10–18, 1999
77. MATSUMOTO K, KANMATSUSE K: Increased IL-12 release by mono-cytes in nephrotic patients. Clin Exp Immunol 117:361–367, 1999
78. MATSUMOTO K, KANMATSUSE K: Transforming growth factor-b1 in-hibits vascular permeability factor release by T cells in normalsubjects and in patients with minimal-change nephrotic syndrome.Nephron 87:111–117, 2001
79. MATSUMOTO K, KANMATSUSE K: Augmented interleukin-18 pro-duction by peripheral blood monocytes in patients with minimal-change nephrotic syndrome. Am J Nephrol 21:20–27, 2001
80. MATSUMOTO K, KANMATSUSE K: Interleukin-18 and interleukin-12 synergize to stimulate the production of vascular permeabil-ity factor by T lymphocytes in normal subjects and in patientswith minimal-change nephrotic syndrome. Nephron 85:127–133,2000
81. KONDO S, YOSHIZAWA N, KUSUMI Y, et al: Studies of glomerularpermeability factor (GPF) in focal segmental glomerular sclerosisand the relationship between GPF and vascular permeability factor(VPF). Clin Nephrol 52:278–284, 1999
82. BAKKER WW, BEUKHOF JR, VAN LUIJK WH, VAN DER HEM GK:Vascular permeability increasing factor (VPF) in IgA nephropa-thy. Clin Nephrol 18:165–167, 1982
83. CHEONG HI, LEE JH, HAHN H, et al: Circulating VEGF and TGF-beta1 in children with idiopathic nephrotic syndrome. J Nephrol14:263–269, 2001
84. WEBB NJ, WATSON CJ, ROBERTS IS, et al: Circulating vascular en-dothelial growth factor is not increased during relapses of steroid-sensitive nephrotic syndrome. Kidney Int 55:1063–1071, 1999
85. FAN L, WAKAYAMA T, YOKOYAMA S, et al: Downregulation of vascu-lar endothelial growth factor and its receptors in the kidney in ratswith puromycin aminonucleoside nephrosis. Nephron 90:95–102,2002
86. HORITA Y, MIYAZAKI M, KOJI T, et al: Expression of vascularendothelial growth factor and its receptors in rats with protein-overload nephrosis. Nephrol Dial Transplant 13:2519–2528,1998
87. NITTA K, UCHIDA K, HONDA K, et al: Serum vascular endothe-lial growth factor concentration in rapidly progressive glomeru-lonephritis. Nephron 80:357–358, 1998
88. NITTA K, UCHIDA K, KIMATA N, et al: Increased serum levels ofvascular endothelial growth factor in human crescentic glomeru-lonephritis. Clin Nephrol 52:76–82, 1999
89. MATSUMOTO K, KANMATSUSE K: Elevated vascular endothelialgrowth factor levels in the urine of patients with minimal-changenephrotic syndrome. Clin Nephrol 55:269–274, 2001
90. NOGUCHI K, YOSHIKAWA N, ITO-KARIYA S, et al: Activated mesan-gial cells produce vascular permeability factor in early-stagemesangial proliferative glomerulonephritis. J Am Soc Nephrol9:1815–1825, 1998
91. PARRY RG, GILLESPIE KM, CLARK AG, MATHIESON PW: Dinu-cleotide repeat polymorphisms within the Flt-1 gene in minimalchange nephropathy. Eur J Immunogenet 26:321–323, 1999
92. HOLT RC, RALPH SA, WEBB NJ, et al: Steroid-sensitive nephroticsyndrome and vascular endothelial growth factor gene polymor-phisms. Eur J Immunogenet 30:1–3, 2003
93. VOGELMANN SU, NELSON WJ, MYERS BD, LEMLEY KV: Urinaryexcretion of viable podocytes in health and renal disease. Am JPhsyiol Renal Physiol 285:F40–F48, 2003
94. SIVRIDIS E, GIATROMANOLAKI A, TOULOUPIDIS S, et al: Platelet en-dothelial cell adhesion molecule-1 and angiogenic factor expres-
sion in idiopathic membranous nephropathy. Am J Kidney Dis41:360–365, 2003
95. NAKAMOTO Y, IMAI H, YASUDA T, et al: A spectrum of clinicopatho-logical features of nephropathy associated with POEMS syndrome.Nephrol Dial Transplant 14:2370–2378, 1999
96. YAMAMOTO T, KURODA M, NISHIOKA K: Increased serum level ofvascular endothelial growth factor in Crow-Fukase syndrome. ActaDerm Venereol 81:317–318, 2001
97. WATANABE O, MARUYAMA I, ARIMURA K, et al: Overproductionof vascular endothelial growth factor/vascular permeability factoris causative in Crow-Fukase (POEMS) syndrome. Muscle Nerve21:1390–1397, 1998
98. SOUBRIER M, SAURON C, SOUWEINE B, et al: Growth factors andproinflammatory cytokines in the renal involvement of POEMSsyndrome. Am J Kidney Dis 34:633–638, 1999
99. KUBO A, NISHITANI Y, MINAMINO N, et al: Adrenomedullin genetranscription is decreased in peripheral blood mononuclear cellsof patients with IgA nephropathy. Nephron 85:201–206, 2000
100. AMORE A, CONTI G, CIRINA P, et al: Aberrantly glycosylated IgAmolecules downregulate the synthesis and secretion of vascularendothelial growth factor in human mesangial cells. Am J KidneyDis 36:1242–1252, 2000
101. IRUELA-ARISPE L, GORDON K, HUGO C, et al: Participation ofglomerular endothelial cells in the capillary repair of glomeru-lonephritis. Am J Pathol 147:1715–1727, 1995
102. HA IS, UM EY, JUNG HR, et al: Glucocorticoid diminishes vascu-lar endothelial growth factor and exacerbates proteinuria in ratswith mesangial proliferative glomerulonephritis. Am J Kidney Dis39:1001–1010, 2002
103. WADA Y, MORIOKA T, OYANAGI-TANAKA Y, et al: Impairmentof vascular regeneration precedes progressive glomeruloscle-rosis in anti-Thy 1 glomerulonephritis. Kidney Int 61:432–443,2002
104. MASUDA Y, SHIMIZU A, MORI T, et al: Vascular endothelial growthfactor enhances glomerular capillary repair and accelerates reso-lution of experimentally induced glomerulonephritis. Am J Pathol159:599–608, 2001
105. YUAN HT, TIPPING PG, LI XZ, et al: Angiopoietin correlates withglomerular capillary loss in anti-glomerular basement membraneglomerulonephritis. Kidney Int 61:2078–2089, 2002
106. NANGAKU M, ALPERS CE, PIPPIN J, et al: A new model of renalmicrovascular endothelial injury. Kidney Int 52:182–194, 1997
107. KIM YG, SUGA SI, KANG DH, et al: Vascular endothelial growthfactor accelerates renal recovery in experimental thrombotic mi-croangiopathy. Kidney Int 58:2390–2399, 2000
108. SUGA S, KIM YG, JOLY A, et al: Vascular endothelial growth fac-tor (VEGF121) protects rats from renal infarction in thromboticmicroangiopathy. Kidney Int 60:1297–1308, 2001
109. SHAHBAZI M, FRYER AA, PRAVICA V, et al: Vascular endothelialgrowth factor gene polymorphisms are associated with acute renalallograft rejection. J Am Soc Nephrol 13:260–264, 2002
110. PILMORE HL, ERIS JM, PAINTER DM, et al: Vascular endothelialgrowth factor expression in human chronic renal allograft rejec-tion. Transplantation 67:929–933, 1999
111. PILMORE HL, YAN Y, ERIS JM, et al: Time course of upregulation offibrogenic growth factors and cellular infiltration in a rodent modelof chronic renal allograft rejection. Transpl Immunol 10:245–254,2002
112. SHIHAB FS, BENNETT WM, YI H, ANDOH TF: Expression of vascularendothelial growth factor and its receptors Flt-1 and KDR/Flk-1 inchronic cyclosporine nephrotoxicity. Transplantation 72:164–168,2001
113. SHIHAB FS, BENNETT WM, ISAAC J, et al: Angiotensin II regula-tion of vascular endothelial growth factor and receptors Flt-1 andKDR/Flk-1 in cyclosporine nephrotoxicity. Kidney Int 62:422–433,2002
114. SHIHAB FS, BENNETT WM, ISAAC J, et al: Nitric oxide modulatesvascular endothelial growth factor and receptors in chronic cy-closporine nephrotoxicity. Kidney Int 63:522–533, 2003
115. ALVAREZ ARROYO MV, SUZUKI Y, YAGUE S, et al: Role of endoge-nous vascular endothelial growth factor in tubular cell protectionagainst acute cyclosporine toxicity. Transplantation 74:1618–1624,2002

Schrijvers et al: VEGF in renal pathophysiology 2017
116. KANG DH, KIM YG, ANDOH TF, et al: Post-cyclosporine-mediatedhypertension and nephropathy: Amelioration by vascularendothelial growth factor. Am J Physiol Renal Physiol 280:F727–F736, 2001
117. YOSHIDA T, KUWAHARA M, MAITA K, HARADA T: Immunohisto-chemical study on hypoxia in spontaneous polycystic liver andkidney disease in rats. Exp Toxicol Pathol 53:123–128, 2001
118. BELLO-REUSS E, HOLUBEC K, RAJARAMAN S: Angiogenesis inautosomal-dominant polycystic kidney disease. Kidney Int 60:37–45, 2001
119. KANELLIS J, MUDGE SJ, FRASER S, et al: Redistribution of cyto-plasmic VEGF to the basolateral aspect of renal tubular cells inischemia-reperfusion injury. Kidney Int 57:2445–2456, 2000
120. KANELLIS J, PAIZIS K, COX AJ, et al: Renal ischemia-reperfusionincreases endothelial VEGFR-2 without increasing VEGF orVEGFR-1 expression. Kidney Int 61:1696–1706, 2002
121. HALTIA A, SOLIN ML, JALANKO H, et al: Mechanisms of proteinuria:Vascular permeability factor in congenital nephrotic syndrome ofthe Finnish type. Pediatr Res 40:652–657, 1996
122. NISHITANI Y, KUBO A, IWANO M, et al: Imbalance betweeninterleukin-6 and adrenomedullin mRNA levels in peripheralblood mononuclear cells of patients with lupus nephritis. Clin ExpImmunol 124:330–336, 2001
123. NAVARRO C, CANDIA-ZUNIGA L, SILVEIRA LH, et al: Vascular en-dothelial growth factor plasma levels in patients with systemic
lupus erythematosus and primary antiphospholipid syndrome.Lupus 11:21–24, 2002
124. LI CG, REYNOLDS I, PONTING JM, et al: Serum levels of vascularendothelial growth factor (VEGF) are markedly elevated in pa-tients with Wegener’s granulomatosis. Br J Rheumatol 37:1303–1306, 1998
125. DVORAK HF: Vascular permeability factor/vascular endothelialgrowth factor: A critical cytokine in tumor angiogenesis and a po-tential target for diagnosis and therapy. J Clin Oncol 20:4368–4380,2001
126. VAN NIEUW AMERONGEN GP, VAN HINSBERGH VWM: Targetsfor pharmacological intervention of endothelial hyperperme-ability and barrier function. Vascul Pharmacol 39:257–272,2002
127. FERRARA N: Role of vascular endothelial growth factor in physio-logic and pathologic angiogenesis: Therapeutic implications. SeminOncol 29:10–14, 2002
128. THE EYETECH STUDY GROUP: Preclinical and phase 1A clinical eval-uation of an anti-VEGF pegylated aptamer (EYE001) for thetreatment of exudative age-related macular degeneration. Retina22:143–152, 2002
129. PUPILLI C, LASAGNI L, ROMAGNANI P, et al: Angiotensin II stim-ulates the synthesis and secretion of vascular permeability fac-tor/vascular endothelial growth factor in human mesangial cells. JAm Soc Nephrol 10:245–255, 1999






















![Critical Reviews in OncologyHematology Volume 62 Issue 3 2007 [Doi 10.1016_j.critrevonc.2007.01.006] Robert Roskoski Jr. -- Vascular Endothelial Growth Factor (VEGF) Signaling in Tumor](https://img.pdfslide.us/doc/110x75/577cd0b41a28ab9e7892e964/critical-reviews-in-oncologyhematology-volume-62-issue-3-2007-doi-101016jcritrevonc200701006.jpg)






