Embed Size (px)
Citation preview

INTRODUCTION
Clinical assessment of the abdomen in the trauma patientcan be difficult. Evacuation of the patient from the ruralsetting may involve decisions about the most appropriatemethod of transportation. Delay in surgery for patientswith exanguinating haemorrhage has been universallyassociated with poor outcomes. The sensitivity of the clin-ical exam in the blunt trauma patient has been shown tobe as low as 69.8%.1 Clinicians face the challenge in avariety of ways.
The American College of Surgeons introduced theAdvanced Trauma Life Support (ATLS®) course in 1980.This resulted from a perceived need to improve the man-agement of the trauma patient in the rural setting. Thiscourse has now been disseminated around the world and
provides a disciplined and structured approach to earlytrauma care.
Trauma patients are often previously well and activeindividuals who become subjected to excessive kineticforces that immediately threaten their well-being or sur-vival. Time is of the essence and the basic principles ofairway management (with cervical spine stabilisation),breathing control, and circulation support are fundamen-tal to the initial resuscitation.
Trauma patients frequently have altered levels of con-sciousness and may be unable to respond meaningfully tothe clinician’s questions. Once the airway has been pro-tected and adequate ventilation established, the assess-ment moves on to the diagnosis and control of thehaemorrhage.
Haemorrhage may be apparent or concealed. Openwounds, which are bleeding profusely, will be controlledby direct pressure. Haemorrhage into the abdomen orchest is often initially covert and may be difficult to detectclinically. Young trauma patients show remarkably fewsigns of haemorrhage until up to 30% of blood volume islost. Agitation and tachycardia are early non-specificsigns of significant haemorrhage. By the time the bloodpressure has fallen, up to 40% of blood volume may be
Aust. J. Rural Health (1999) 7, 85–89
Correspondence: Dr Peter Freeman, Clinical Director, Depart-ment of Emergency Medicine, Auckland Hospital, Private Bag92024, Auckland, New Zealand. E-mail: <[email protected]>
P. Freeman, MBChB, FRCS, FFAEM, FACEM.
Accepted for publication January 1999.
THE ROLE OF ULTRASOUND IN THEASSESSMENT OF THE TRAUMA PATIENT
Department of Emergency Medicine, Auckland Hospital, Auckland, New Zealand
ABSTRACT: Ultrasound assessment of the patient with blunt abdominal trauma will enhance diagnostic accuracyand facilitate decision making about the need for urgent surgery. Numerous studies have reported the role ofultrasound in the assessment of the trauma patient. Focused ultrasound has been shown to compare in sensitivity todiagnostic peritoneal lavage and is helpful in assessing the need for a laparotomy. Ultrasound is safe, cheap andportable. The investigation is non-invasive and painless. The trauma ultrasound scan can be completed in under 3minutes and should be performed during the initial trauma assessment. The technique is not difficult to learn.Advances in technology are likely to make portable ultrasound increasingly appropriate to rural clinical practice.Detection of haemoperitoneum will be more accurate when ultrasound is available in the early care of trauma on a 24hour basis and, to achieve this, clinicians managing trauma will need to become competent in the application of thefocused ultrasound exam.
KEY WORDS: haemoperitoneum, trauma, ultrasound.
Peter Freeman
Clinical Article OA 233 EN

86 AUSTRALIAN JOURNAL OF RURAL HEALTH
lost. Early definitive surgery is required in many of thesepatients.
The objective in the assessment of the trauma patientis therefore to perform life-saving resuscitation and decidewhich patients require definitive management and/orimmediate surgery. Patients with penetrating abdominal orchest wounds clearly mandate immediate surgery and nofurther investigation is necessary.
Patients with closed intraperitoneal or intrathoracichaemorrhage present a major diagnostic challenge in thetrauma room. Since its introduction in 1965, diagnosticperitoneal lavage (DPL) has become the traditional inves-tigation for blunt abdominal trauma in unstable patients.Focused abdominal ultrasound has now been shown tohave many advantages over DPL and it is replacing DPLas the diagnostic study of first choice in some majortrauma centres.2
DIAGNOSTIC PERITONEAL LAVAGEVERSUS FOCUSED ABDOMINALULTRASOUND
Unstable trauma patients in whom the clinical abdominalexamination is equivocal, have traditionally been sub-jected to a DPL if the condition of the patient leads theclinician to suspect intra-abdominal injury. Diagnosticperitoneal lavage involves introducing a blunt catheterinto a small surgical incision in the mid-line of theabdomen, following which a litre of warm, sterile isotonicfluid is infused into the peritoneal cavity and thendrained. Contamination of the effluent with blood, whitecells or bacteria would indicate intra-abdominal injury.The procedure is highly sensitive (100%) and has resultedin a significant number of unnecessary laparotomies.3 Theinvestigation is invasive and carries a 1% complicationrate. The process cannot be repeated and leaves free fluidand air in the peritoneal cavity. The surgical procedurecan take as long as 20 minutes to perform in inexperi-enced hands.
In contrast, ultrasound can be a very rapid and non-invasive investigation. Focused abdominal ultrasound inthe trauma patient has been shown to have a sensitivity inthe order of 90% for the detection of haemoperitoneum.4
False positives are rare. The skill to perform a focusedexam can be learned by attending a basic introductorycourse and after a brief learning curve, emergency physi-cians and surgeons have achieved comparable sensitiv-ities to radiologists.4,5 Identification of haemoperitoneumon ultrasound has been found to correlate well with theneed for a therapeutic laparotomy.6 Small amounts ofintraperitoneal blood may be undetectable by ultrasound,
whereas a DPL is likely to be positive. The amount offluid detectable by ultrasound is disputed in the litera-ture, but it will be clearly dependent on the experience ofthe operator. The amount of free blood, however, is lessimportant than the clinical condition of the patient. Ultra-sound is easily repeated and studies have shown thatsequential focused scanning can improve the sensitivity ofthe test.2
Modern ultrasound machines are small and mobileand do not impede the trauma team during the initialassessment. Advances in technology are making feasiblethe concept of a portable ultrasound scanner suitable foruse in trauma in the rural environment.
IS ULTRASOUND SAFE?
Diagnostic ultrasound applied transcutaneously for greyscale imaging has been in clinical use since the late1950s. To date the results of numerous follow-up studieson patients, including children who have been scannedantenatally, have failed to demonstrate any biologicaleffects that could be attributed to grey scale ultrasoundimaging.
Ultrasound produces images by bouncing sound wavesoff structures and representing the echo as an image on ascreen. Different structures have varying echogenicity andsome of the sound energy is absorbed by the tissues. Asultrasound propagates through biological tissue some ofthe energy is converted to heat. B mode grey scale imag-ing, which is applicable to the trauma environment, hasbeen investigated and found to confer no significant bio-logical effect.7 Pulsed Doppler studies used in some vas-cular, cardiac, and foetal examinations do have thepotential to cause a thermal effect that may producebiologically significant temperature rises. Bone has thegreatest capacity to be effected by the thermal reaction,and developing fetal central nervous tissue is the mostsensitive biological structure. Time constraints and mini-mum acoustic output are recommended when usingpulsed Doppler studies.
FOCUSED ABDOMINAL SONOGRAPHY INTRAUMA (FAST)
Sonography performed in the trauma room is very differentto the comprehensive examination used by radiologysonography departments. The objectives when usingfocused abdominal sonograpy in trauma (FAST) are toanswer a few specific questions. The investigation must betaken to the bedside of the patient who may be undergoingfull trauma assessment and resuscitation. The ultrasound

ULTRASOUND ASSESSMENT OF THE TRAUMA PATIENT: P. FREEMAN 87
machine can be operated by a clinician who is part of andfamiliar with the initial assessment in trauma. The examshould take no more than 5 minutes and, with experience,can be usually completed in under 3 minutes.8 Thefocused ultrasound examination is structured and usuallyinvolves imaging four areas. These are: (i) the right flank,to show the hepato-renal pouch (Morison’s pouch); (ii) theleft flank, to show the peri-splenic view; (iii) the supra-pubic window, to image the pelvis; and (iv) the subcostalpericardial view. Intraperitoneal blood shows as a blackhypo-echoic area filling the pelvis or Morison’s pouch.Bleeding from the spleen or liver in the supine patientpreferentially flows into the hepato-renal pouch and downthe para-colic gutters into the pelvis. The subcostal peri-cardial view completes the trauma exam and may demon-strate pericardial fluid which, in the trauma patient, islikely to be blood. Intercostal blood can sometimes beidentified above the diaphragm from the flank views.
The result of the FAST exam must be put into the con-text of the patient’s physiology. Trauma patients who areunstable physiologically and who have a clearly positiveultrasound scan for haemoperitoneum require immediatesurgery. Stable patients with clinical suspicion but a nega-
tive scan may benefit from repeat ultrasound or comput-erised tomography (CT) imaging. If the result of the FASTscan is equivocal in the stable patient, a CT may be indi-cated. Diagnostic peritoneal lavage is reserved for theunstable patient in whom ultrasound is unreliable, as inthe case of surgical emphysema or gross obesity.
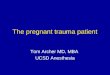
Figure 1 represents the consensus of practice at insti-tutions using ultrasound in the early management oftrauma.
TRAINING ISSUES AND CREDENTIALLING
Without doubt the most controversial area surroundingtrauma ultrasound is that of training and credentialling.Interpretation of ultrasound images requires some skilland a knowledge of sound physics. Clinicians who havebeen using ultrasound as part of their trauma work-up aretending to abandon diagnostic peritoneal lavage as the ini-tial screening test for blunt abdominal trauma.2 Studieshave clearly shown that with adequate training, traumasurgeons and emergency physicians can become compe-tent in the use of focused ultrasound. It has also beenshown that the introduction of ultrasound in the trauma
FIGURE 1: Algorithm for the use of ultrasound in the investigation of blunt abdominal trauma. BAT, blunt abdominal trauma; US,
ultrasound; DPL, diagnostic peritoneal lavage; CT, computerised tomography; OR, operating room.

88 AUSTRALIAN JOURNAL OF RURAL HEALTH
assessment actually increased the number of referralsto the radiology department for definitive ultrasoundstudies.9
Clearly the level of training required to perform a 2minute trauma scan will be different to that required for afull sonographic assessment or echocardiography. TheAmerican experience would indicate that 150 scans wouldallow adequate exposure to sufficient true positives toachieve a level of operator competence.10
A three-level program for training is proposed:(1) Level I (basic): Attendance at a 2 day (16 hour) work-shop, including introduction to sound physics, basicapplication of the imaging techniques, and practical expe-rience with live models.(2) Level II (credentialled): As for level I, but after aperiod of supervised practice including 150 mentoredscans and a further 16 hour lecture and practical course.(3) Level III: Advanced practice to include achieving theDiploma in Diagnostic Ultrasound.
Most clinicians credentialled to use ultrasound in theemergency department for trauma patients will berequired to achieve level II.
THE INTRODUCTION OF FOCUSEDULTRASOUND TO CLINICAL PRACTICE
Trauma centres which have introduced ultrasound to thetrauma team assessment have published significant bene-fits to patients.11 The most satisfactory process of intro-duction involves collaboration with the department ofradiology. However, not always is the radiology or sonogra-phy department supportive of ultrasound moving into thetrauma room and out of the hands of sonographers. Bene-fits to patients need to override issues of ownership orterritory. Training of clinicians by experienced sonogra-phers, radiologists, emergency physicians, cardiologists orobstetricians are all appropriate. Most clinicians who havecompleted a basic course in focused ultrasound find thatthe interpretations of sonographic images of Morison’spouch are easier to interpret than a chest X-ray. It isaccepted practice that the surgeon, intensivist or emer-gency physician will interpret a supine chest X-ray on atrauma patient. Based on this interpretation, the patientmay be taken to theatre or subjected to further investiga-tion, such as an angiography. It is logical that the sameclinicians involved in the early management of traumashould be capable of performing and interpreting ultra-sound images that may benefit the patient by the earlydiagnosis of haemoperitoneum, which will expedite defini-tive surgical intervention.
CONCLUSION
With the advances in ultrasound technology, the focusedexam is becoming a readily available and cost-effectiveinvestigation to perform at the bedside. Modern ultra-sound machines are user-friendly and mobile. Video orstill recording is available for reporting images. The sensi-tivity of focused ultrasound has been shown in large stud-ies on trauma patients to support its application as ascreening test for haemoperitoneum. The technology issuitable for the rural enviroment.
Focused ultrasound will not replace CT for organimaging in the stable trauma patient, but may well replaceDPL except in a minority of trauma patients who, due tosurgical emphysema or obesity, are unsuitable for ultra-sound. Ultrasound is also considered to be unreliable incases of bowel injury or retroperitoneal haemorrhage.
The question, therefore, that needs to be answered inthe trauma room is not, ‘Is there blood in the peritonealcavity?’ but rather, ‘Is the blood loss into the peritonealcavity causing instability that will mandate surgery?’.With the increasing use of conservative management andminimal intervention surgery for splenic and liverinjuries, small amounts of blood in the peritoneal cavitydetectable by DPL have become less significant. Ultra-sound is slowly finding its place in the trauma room as atool to be used by clinicians to establish which unstabletrauma patients are likely to benefit from early surgery.
REFERENCES
1 Rothlin MA, Naf R, Amgwerd M, Candinas D, Frick T,Trentz O. Ultrasound in blunt abdominal and thoracictrauma. Journal of Trauma 1993; 34: 488–495.
2 Hoffmann R, Nerlich M, Muggia-Sullam M et al. Bluntabdominal trauma in cases of multiple trauma evaluated byultrasonography: A prospective analysis of 291 patients.Journal of Trauma 1992; 32: 452–458.
3 Liu M, Lee CH, P’eng FK. Prospective comparison of diag-nostic peritoneal lavage, computed tomographic scanning,and ultrasonography for the diagnosis of blunt abdominaltrauma. Journal of Trauma 1993; 35: 267–270.
4 Ma OJ, Mateer JR, Ogata M, Kefer MP, Wittmann D, Apra-hamian C. Prospective analysis of a rapid trauma ultra-sound examination performed by emergency physicians.Journal of Trauma 1995; 38: 879–885.
5 Buzzas GR, Kern SJ, Smith RS, Harrison PB, Helmer SD,Reed JA. A comparison of sonographic examinations fortrauma performed by surgeons and radiologists. Journal ofTrauma 1998; 44: 604–606.
6 Porter RS, Nester BA, Dalsey WC et al. Use of ultrasoundto determine need for laparotomy in trauma patients.Annals of Emergency Medicine 1997; 29: 323–330.

ULTRASOUND ASSESSMENT OF THE TRAUMA PATIENT: P. FREEMAN 89
7 Barnett SB, Kossoff G, Edwards MJ. Is diagnostic ultra-sound safe? Medical Journal of Australia 1994; 160:33–37.
8 Thomas B, Falcon RE, Vasquez D et al. Ultrasound evalua-tion of blunt abdominal trauma: Program implementation,initial experience, and learning curve. Journal of Trauma1997; 42: 384–388.
9 Heller MB, Melanson SW, Patterson J. Does the institution
of an emergency department training program in emergencyultrasonography change the number of sonograms orderedfrom radiology? (abstract). Society of Academic EmergencyMedicine 1997; 157: 393.
10 Heller M. Emergency ultrasound: Out of the acoustic shad-ows. Annals of Emergency Medicine 1997; 29: 380–382.
11 Rozycki GS, Shackford SR. Ultrasound: What every traumasurgeon should know. Journal of Trauma 1996; 40: 1–4.