Embed Size (px)
Citation preview
The Role of Stroke Team in
Post Acute Care of Stroke
Yin, Jiu-Haw, MD. Director, Stroke Center
Cheng Hsin General Hospital Taipei, Taiwan
May 29th, 2016
Stroke is a leading cause of
serious, long-term disability, the
effects of which may be
prolonged with physical,
emotional, social, and
financial consequences not only
for those affected but also for
their family and friends.
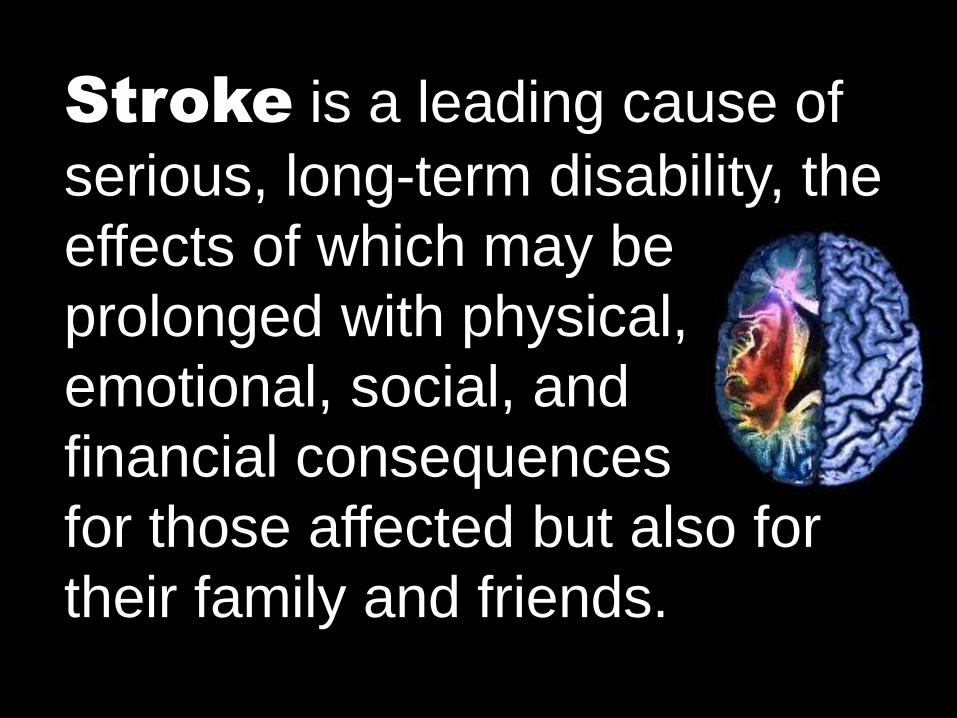
Global and regional burden of
stroke during 1990-2010
Lancet. 2014 Jan 18;383(9913):245-54
0
50
100
150
200
250
300
1990 2005 2010
Survivor
Mortality
0
50
100
150
200
250
300
1990 2005 2010 an
nu
al r
ate
(per
10
0,0
00
per
son
-ye
ars)
High-income countries Low & middle-income countries
246.32
96.45
221.19
72.33
217.26
60.54
251.93
130.49
277.48 281.12
115.06 104.98
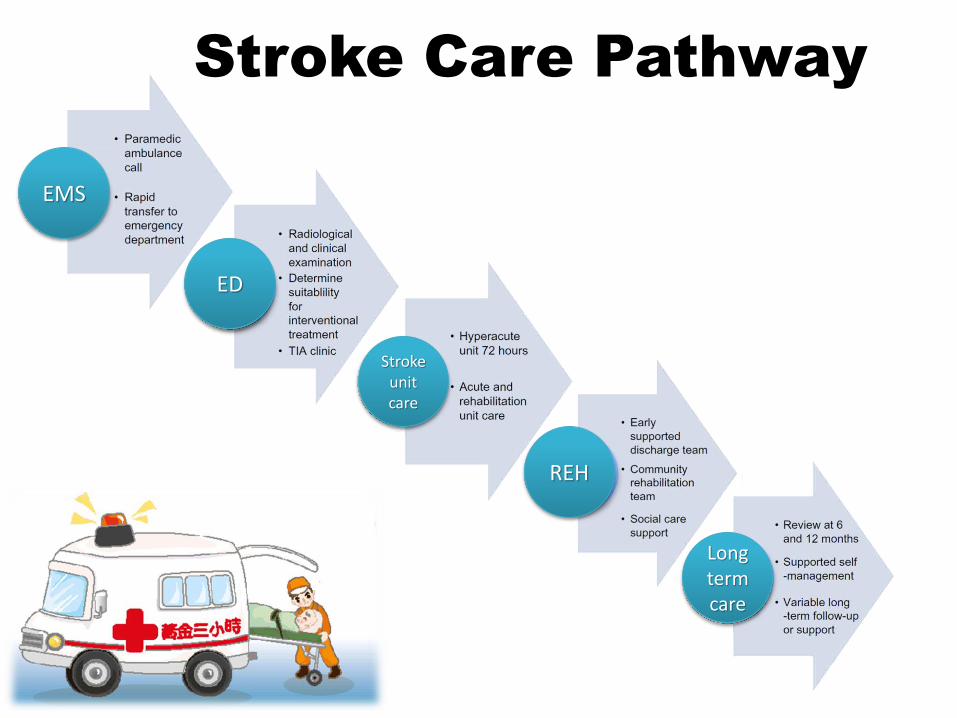
Stroke Care Pathway
EMS
ED
Stroke unit care
REH
Long term care
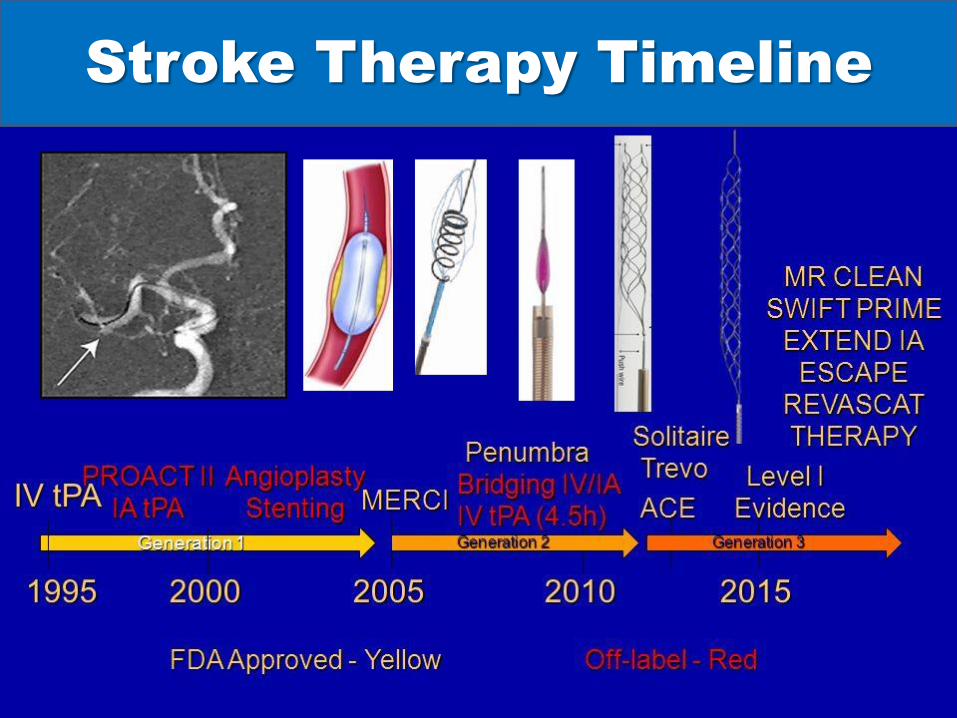
Stroke Therapy Timeline
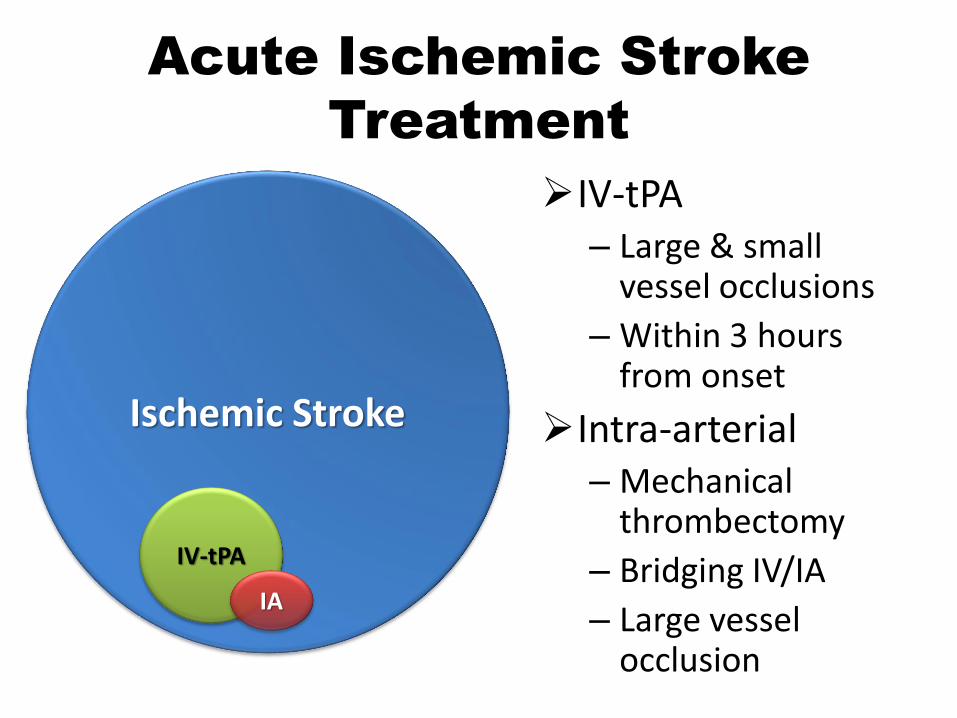
Acute Ischemic Stroke
Treatment
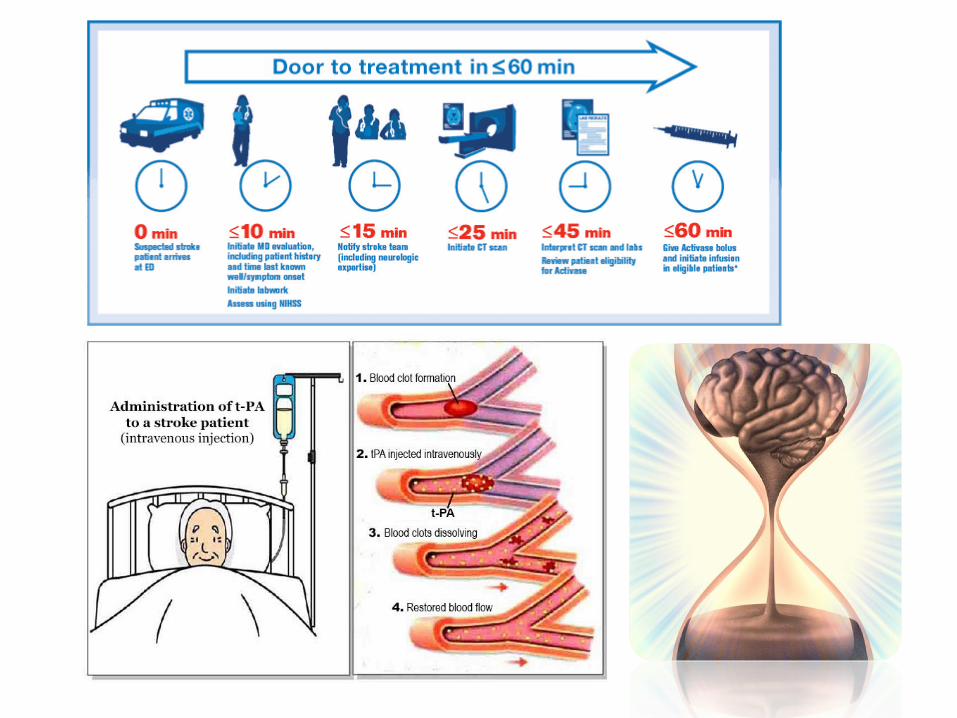
IV-tPA – Large & small
vessel occlusions
– Within 3 hours from onset
Intra-arterial – Mechanical
thrombectomy
– Bridging IV/IA
– Large vessel occlusion
Ischemic Stroke
IV-tPA
IA
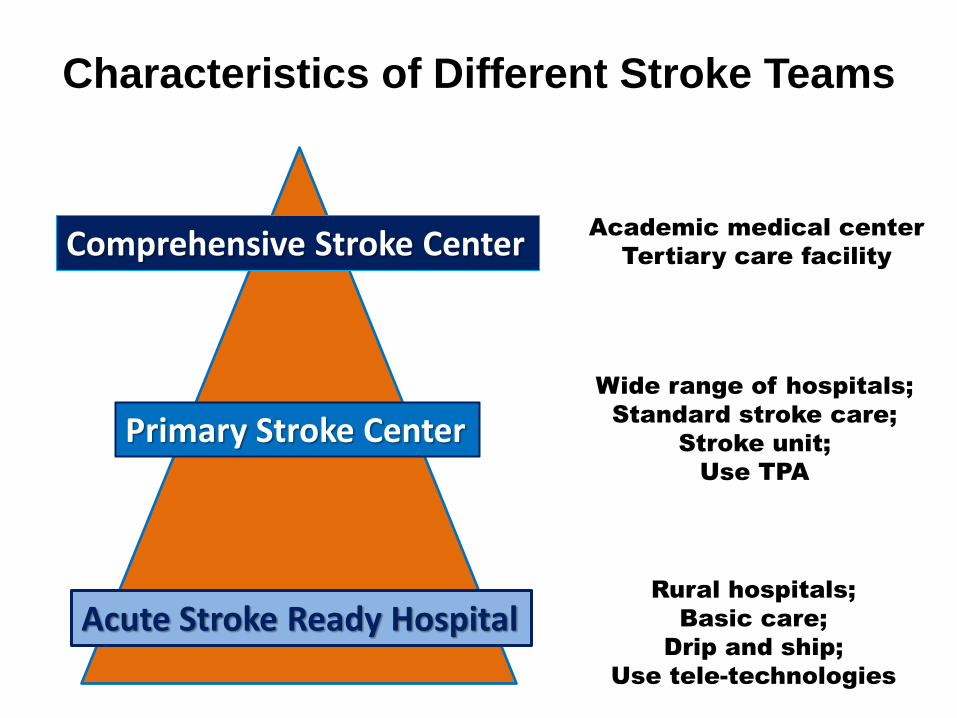
Characteristics of Different Stroke Teams
Comprehensive Stroke Center
Primary Stroke Center
Acute Stroke Ready Hospital
Academic medical center
Tertiary care facility
Wide range of hospitals;
Standard stroke care;
Stroke unit;
Use TPA
Rural hospitals;
Basic care;
Drip and ship;
Use tele-technologies
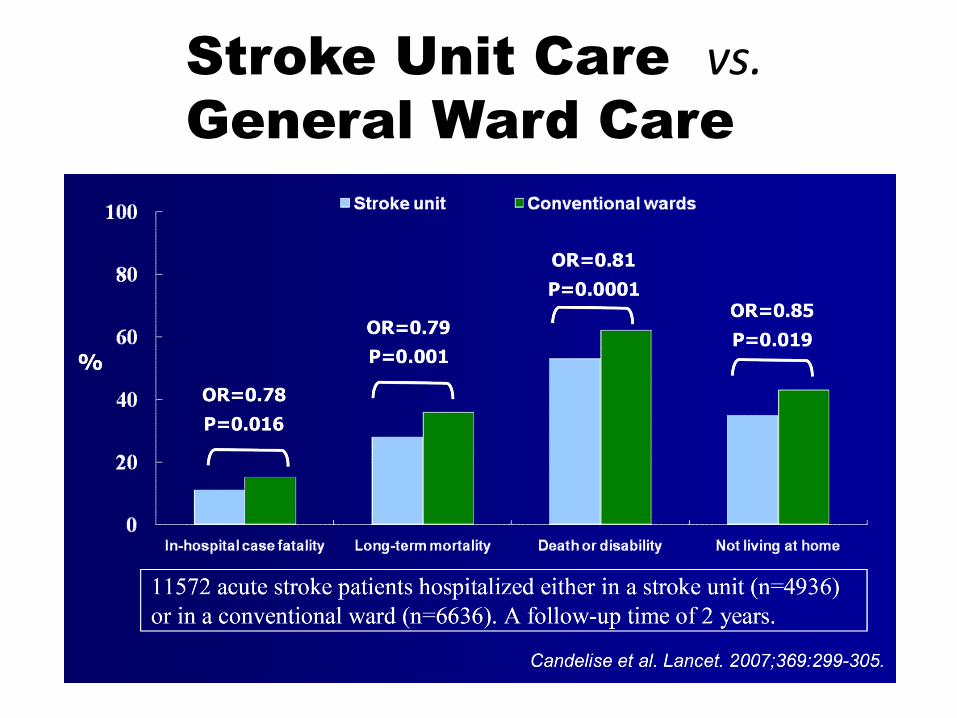
Stroke Unit Care vs. General Ward Care
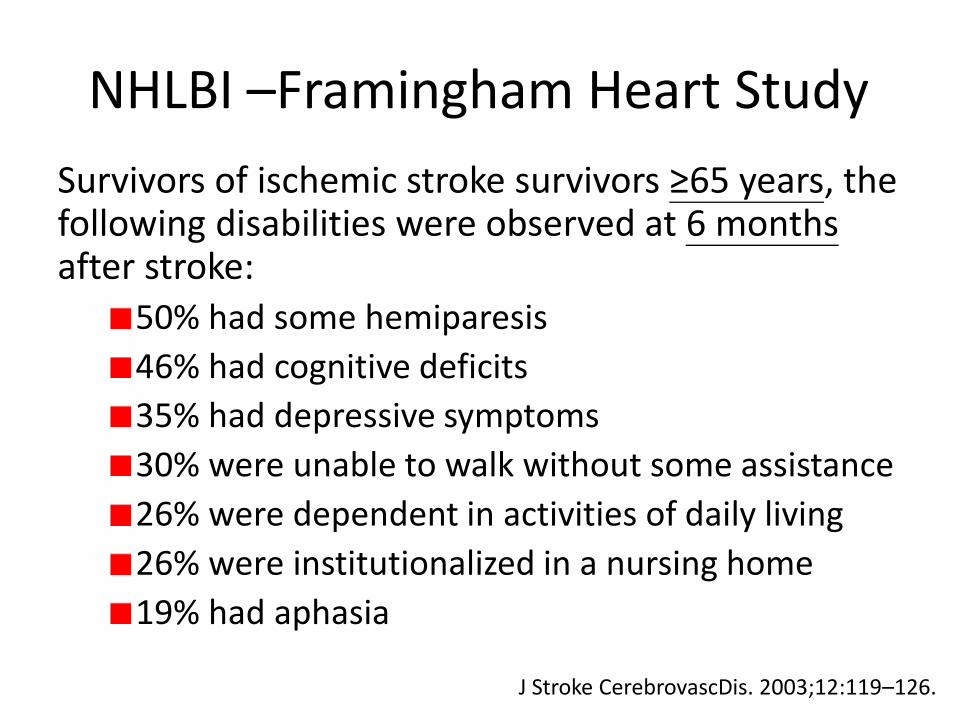
NHLBI –Framingham Heart Study
Survivors of ischemic stroke survivors ≥65 years, the following disabilities were observed at 6 months after stroke:
50% had some hemiparesis
46% had cognitive deficits
35% had depressive symptoms
30% were unable to walk without some assistance
26% were dependent in activities of daily living
26% were institutionalized in a nursing home
19% had aphasia
J Stroke CerebrovascDis. 2003;12:119–126.
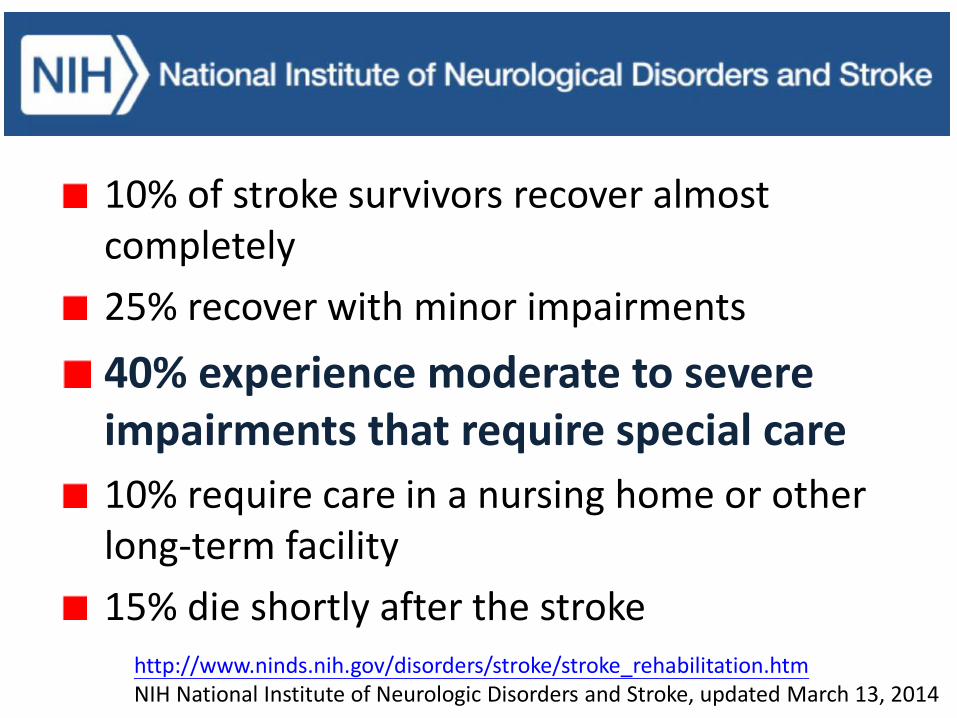
10% of stroke survivors recover almost completely
25% recover with minor impairments
40% experience moderate to severe impairments that require special care
10% require care in a nursing home or other long-term facility
15% die shortly after the stroke http://www.ninds.nih.gov/disorders/stroke/stroke_rehabilitation.htm NIH National Institute of Neurologic Disorders and Stroke, updated March 13, 2014

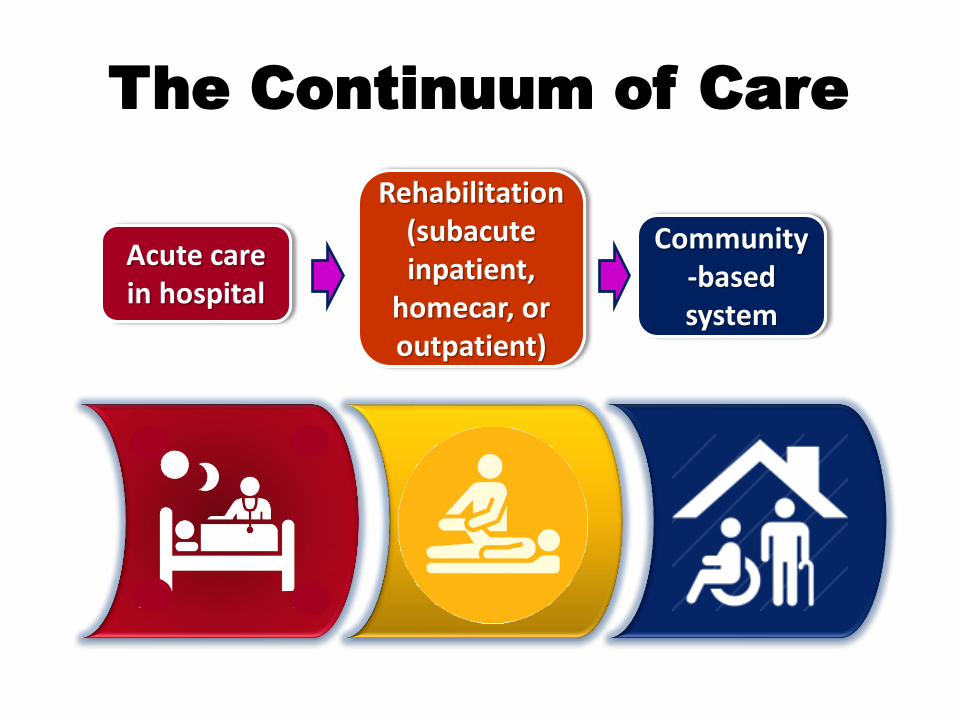
The Continuum of Care
Acute care in hospital
Rehabilitation (subacute inpatient,
homecar, or outpatient)
Community-based system
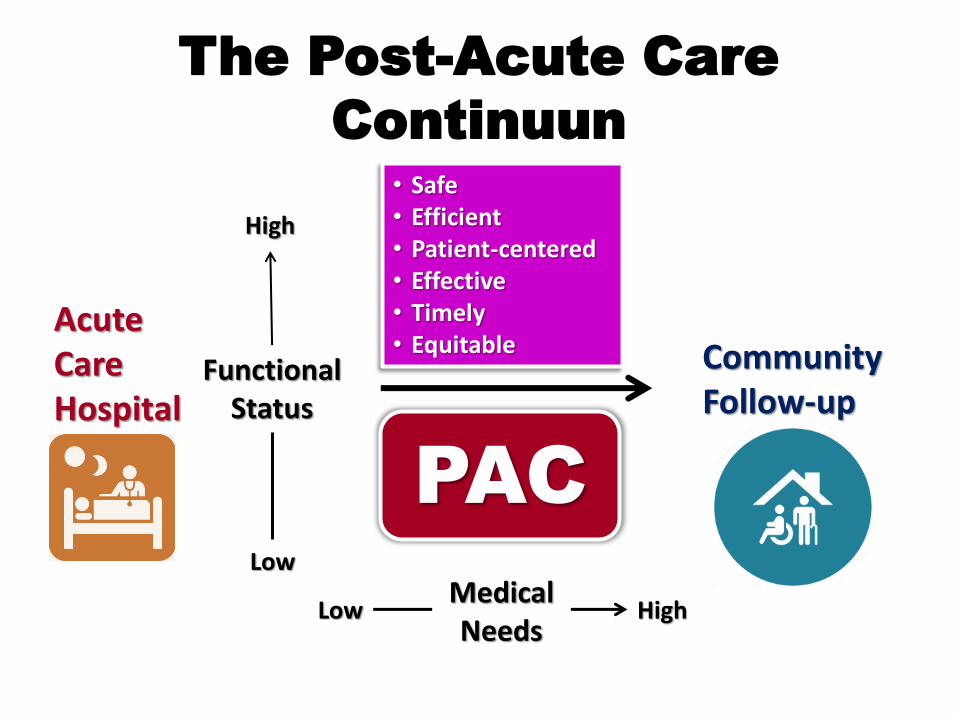
The Post-Acute Care
Continuun
Acute Care Hospital
Community Follow-up
High
Low
Functional Status
Low High Medical Needs
PAC
• Safe • Efficient • Patient-centered • Effective • Timely • Equitable
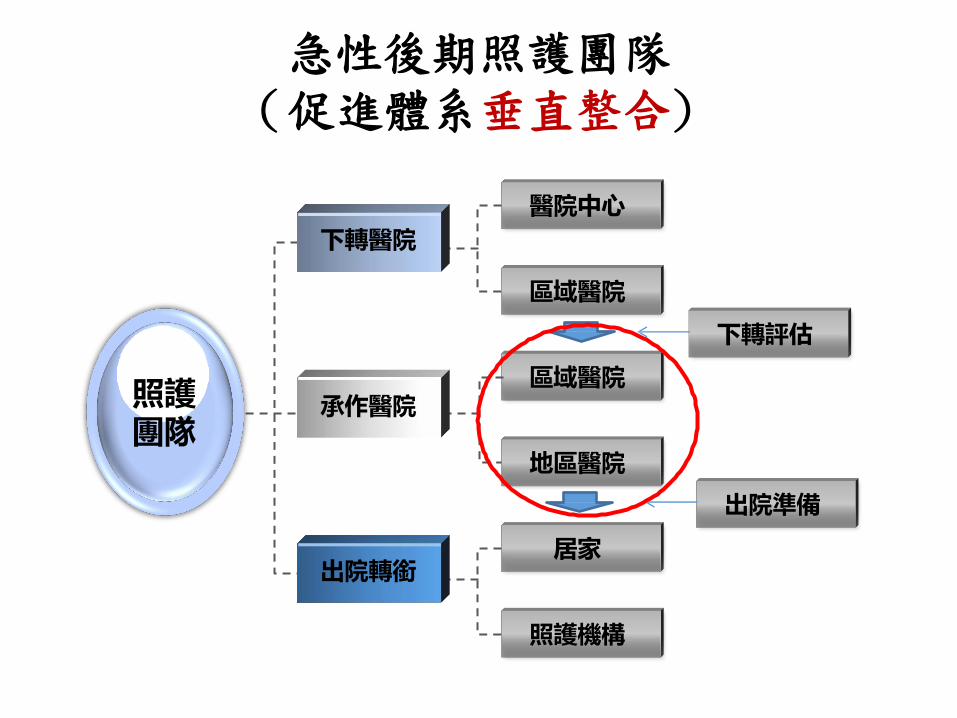
急性後期照護團隊 (促進體系垂直整合)
醫院中心
區域醫院
區域醫院
地區醫院
居家
照護機構
照護 團隊
下轉醫院
承作醫院
出院轉銜
下轉評估
出院準備
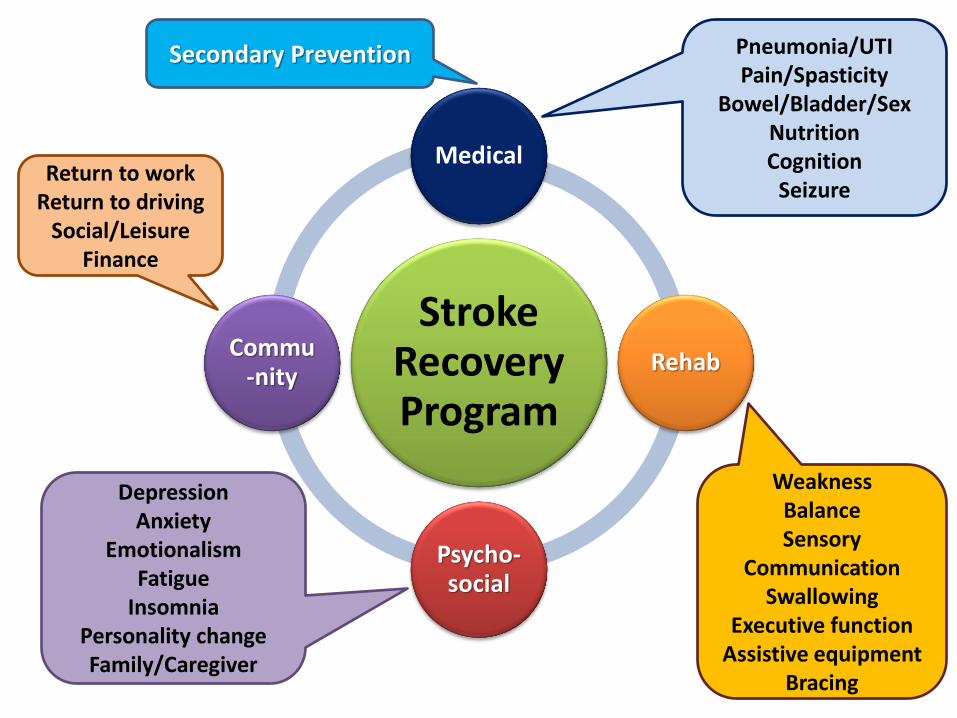
Stroke Recovery Program
Medical
Rehab
Psycho-social
Commu-nity
Pneumonia/UTI Pain/Spasticity
Bowel/Bladder/Sex Nutrition Cognition
Seizure
Secondary Prevention
Weakness Balance Sensory
Communication Swallowing
Executive function Assistive equipment
Bracing
Depression Anxiety
Emotionalism Fatigue
Insomnia Personality change Family/Caregiver
Return to work Return to driving
Social/Leisure Finance
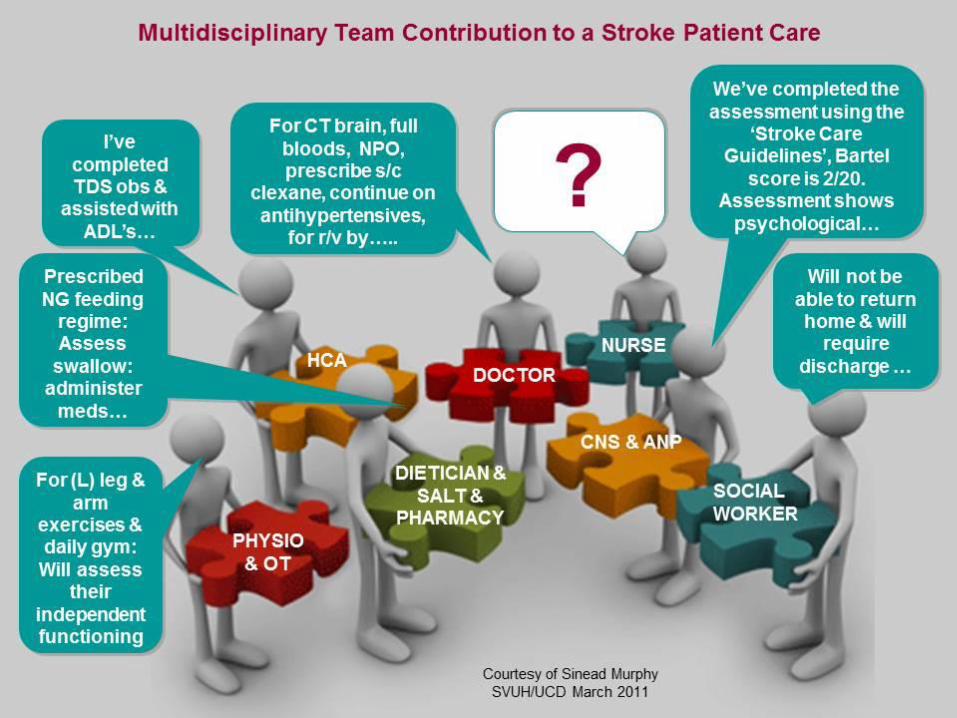
Inpatient Stroke Team
Stroke physician
Nurses
Physiotherapists (PTs)
Occupational therapists (OTs)
Speech and language therapists (SALTs)
Health care and therapy assistants (trained to support PTs or OTs)
Stroke Physicians
Focus on medical management and oversee patient care from admission through to discharge.
Most advocate for and contribute fully to multidisciplinary team (MDT) or interdisciplinary team (IDT) working.
Stroke Coordinators
Nurses or therapists
Core team members and work with stroke survivors, their families, and the wider stroke team from admission to discharge
Along with physicians and other stroke team members, stroke coordinators provide secondary prevention and behavior change advice aimed at helping stroke survivors reduce the risk of recurrent events.
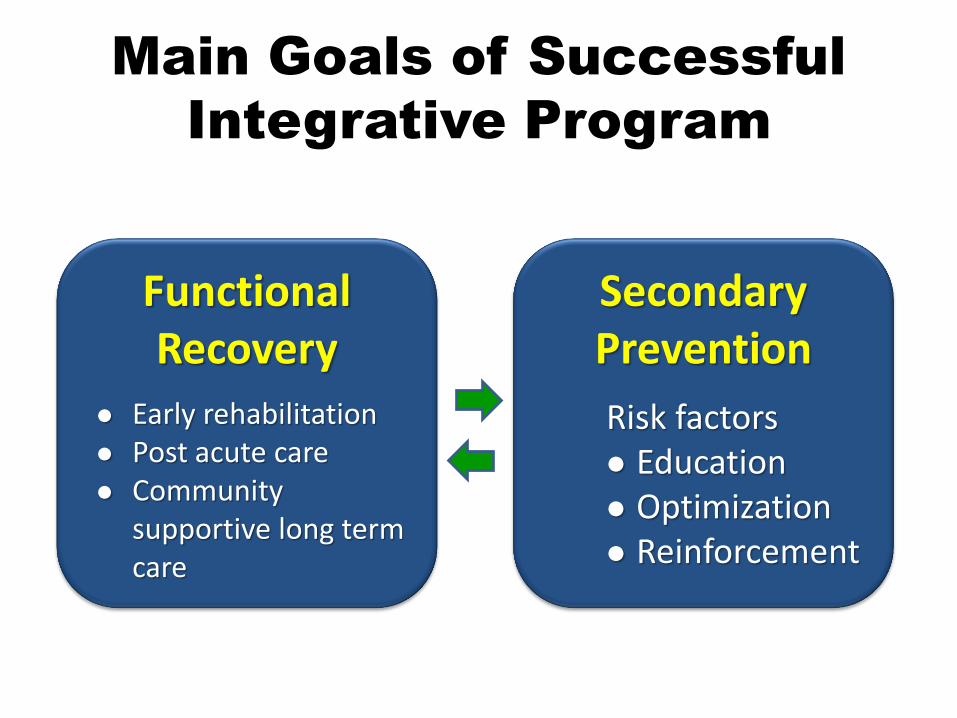
Main Goals of Successful
Integrative Program
Functional Recovery
Secondary Prevention
Early rehabilitation Post acute care Community
supportive long term care
Risk factors Education Optimization Reinforcement
• All stroke team members can support stroke survivors in practices related to improving independence in ADLs, in increased function and mobility, and in communication.
• Should use an agreed consistent approach for each problem faced by a patient, ensuring that the patient is given the same advice and taught the same technique to ameliorate or overcome it.
Intercollegiate Stroke Working Party, National Clinical Guidelines for Stroke. 4th ed. London: Royal College of Physicians; 2012.
Change in thinking
What am I trained to do (separately) as an OT or nurse?
What does the patient need and how can this be provided collaboratively by the stroke team?
MDT or IDT?
MDT: multidisciplinary team IDT: interdisciplinary team
Teams with an IDT approach were more likely to see delivery of caregiver training as a shared responsibility, more likely to share information on caregiver training in team meetings, and more likely to check with other team members that training had been provided.
Journal of Multidisciplinary Healthcare 2015:8
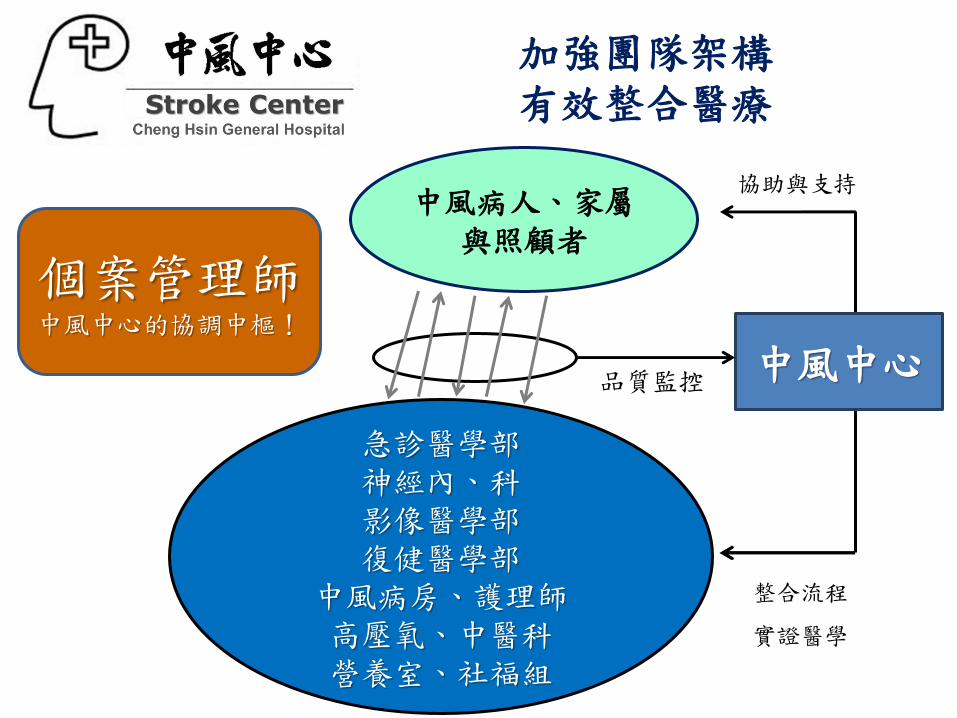
加強團隊架構 有效整合醫療
個案管理師 中風中心的協調中樞!
中風病人、家屬與照顧者
急診醫學部 神經內、科 影像醫學部 復健醫學部
中風病房、護理師 高壓氧、中醫科 營養室、社福組
中風中心 品質監控
協助與支持
整合流程
實證醫學
Conclusion
Although emerging trends in stroke management have allowed more patients to survive, many are left with varying degrees of disability.
Stroke recovery is complex and dependent on many factors, and is a unique experience for each patient.
It is essential to organize a multidisciplinary team with experience in utilizing techniques to enhance recovery and avoid preventable complications.

Thank You
For Your Attention