Embed Size (px)
Citation preview
The Role of PsychoticDisorders in ReligiousHistory ConsideredEvan D. Murray, M.D.Miles G. Cunningham, M.D., Ph.D.Bruce H. Price, M.D.
The authors have analyzed the religious figuresAbraham, Moses, Jesus, and St. Paul froma behavioral, neurologic, and neuropsychiatricperspective to determine whether new insights canbe achieved about the nature of their revelations.Analysis reveals that these individuals hadexperiences that resemble those now defined aspsychotic symptoms, suggesting that theirexperiences may have been manifestations ofprimary or mood disorder-associated psychoticdisorders. The rationale for this proposal isdiscussed in each case with a differential diagnosis.Limitations inherent to a retrospective diagnosticexamination are assessed. Social models ofpsychopathology and group dynamics are proposedas explanations for how followers were attracted andnew belief systems emerged and were perpetuated.The authors suggest a new DSM diagnosticsubcategory as a way to distinguish this type ofpsychiatric presentation. These findings support thepossibility that persons with primary and mooddisorder-associated psychotic symptoms have hada monumental influence on the shaping of Westerncivilization. It is hoped that these findings willtranslate into increased compassion andunderstanding for persons living with mentalillness.
(The Journal of Neuropsychiatry and ClinicalNeurosciences 2012; 24:410–426)
A man in his late 20s with paranoid schizophreniaexplained during a neurological evaluation that he
could read minds and that for years he had heard voicesrevealing things about friends and strangers alike. Hebelieved he was selected by God to provide guidancefor mankind. Antipsychotic medications prescribed byhis psychiatrists diminished these abilities and reducedthe voices, and therefore he would not take them. Heasked, “How do you know the voices aren’t real?” “Howdo you know I am not The Messiah?”He affirmed, “Godand angels talked to people in the Bible.”Later, we reflected on what he had said. He raised
poignant questions that are rarely discussed in academicmedicine. Every day, physicians, nurses, psychologists,and social workers alike encounter and care for peoplewho experience psychotic symptoms. About 1% of emer-gency room visits and 0.5% of all primary care visits inthe United States are related to psychotic symptoms.1,2
As many as 60% of those with schizophrenia havereligious grandiose delusions consisting of believingthey are a saint, God, the devil, a prophet, Jesus, or someother important person.3 Diminished insight abouthaving a mental disorder is part and parcel of thecondition, occurring in 30%–50% of persons with schizo-phrenia.4 How do we explain to our patients that theirpsychotic symptoms are not supernatural intimationswhen our civilization recognizes similar phenomenain revered religious figures? On what basis do we
Received September 13, 2011; revised March 15, 2012; accepted March22, 2012. From the Dept. of Neurology, McLean Hospital, HarvardMedical School, Belmont, MA (EDM, BHP); Dept. of Psychiatry,McLean Hospital, Harvard Medical School, Belmont, MA (MGC);Dept. of Neurology, Massachusetts General Hospital, HarvardMedicalSchool, Belmont, MA (EDM, BHP). Send correspondence to Evan D.Murray, M.D., Dept. of Neurology, McLean Hospital, Belmont, MA;e-mail: [email protected]
Copyright © 2012 American Psychiatric Association
410 http://neuro.psychiatryonline.org J Neuropsychiatry Clin Neurosci 24:4, Fall 2012

distinguish between the experiences of psychiatric pa-tients and those of religious figures in history?
A review of the medical literature revealed little dis-cussion of these specific issues utilizing modern neu-ropsychiatric and behavioral neurologic principles. Anexamination of the revelation experiences of prominentreligious figures was needed to determine whether newinsights could be achieved about their nature through theapplication of neuropsychiatric and behavioral neurologicprinciples. We undertook this examination with the intentof promoting scholarly dialogue about the rational limitsof human experience and to educate persons living withmental illness, healthcare providers, and the general publicthat persons with psychotic symptoms may have hada considerable influence on the development of Westerncivilization. The selection of personalities for analysis wasbased on 1) the existence of narratives recounting the in-dividual’s mystical experiences and behaviors; 2) the po-tential similarity of these experiences to psychiatricphenomena; 3) the high degree of impact their life storieshad onWestern civilization in terms of influencing themesfound in literature and art, religious thought and practice,philosophy, concepts of social order, and jurisprudence.The following is a retrospective diagnostic examination ofAbraham, Moses, Jesus, and St Paul. It is hoped that thisinvestigation will help translate the veneration, love, anddevotion felt by many for these religious figures into in-creased compassion and understanding for persons withmental illness.
ABRAHAM
The Bible is the earliest source of information about thelife of Abraham, the patriarch of Judaism, Christianity,and Islam. The historical existence of Abraham is thesubject of some academic controversy. Our discussionwill proceed on the premise that he was a historicalfigure. The events occurring during his lifetime aregenerally thought to have taken place sometime between2000 BCE and 1630 BCE, but this is a subject of somedebate. He is described as having had interactive mys-tical experiences of an auditory and visual nature (seeFigure 1), that influenced his behaviors throughout mostof his life (see Table 1). This phenomenology closelyresembles that described in the Diagnostic and Sta-tistical Manual of Mental Disorders (DSM-IV-TR).5 Apply-ing the DSM-IV-TR paradigm, Abraham’s auditory andvisual perceptual experiences and behaviors could be
understood as auditory hallucinations (AH), visual hal-lucinations (VH), delusions with religious content, andparanoid-type (schizophrenia subtype) thought content(see Table 1 for examples). These psychiatric featuresoccur together as a constellation in psychotic disordersof both primary psychiatric origin and secondary tomedical and neurological conditions.5 According to theDSM-IV-TR, the diagnosis of schizophrenia requires atleast two out of five symptoms from Criterion Aand then fulfillment of the five remaining criteria (seeTable 2). Criterion A might theoretically be fulfilledby the presence of his auditory and visual perceptualexperiences. Abraham is not recounted as having hadsymptoms that can now be appreciated as disorganiza-tion, catatonia, negative psychiatric symptoms (affectiveflattening, alogia, or avolition), or cognitive difficultiessuch as impaired concentration, attention, or memory.The lack of detailed information about his life preventsus from understanding whether he experienced a declinein social or occupational functioning, as compared withthe period before the onset of his perceptual experiences,as required by Criterion B. Criterion C’s requirementabout persistence and duration of symptoms is fulfilledby the period of 100 years or more during which he hadthese experiences. His generally good state of health isindicated by a purported lifespan of 175 years withoutmentioned infirmity. Abraham appeared not to sufferfrom debilitating depressive- or manic-like symptoms,thereby diminishing the likelihood of mood disorderassociated psychoses, such as depression with psychoticfeatures, bipolar disorder, or schizoaffective disorder.Other potential causes of such experiences need to be
explored. The ingestion of hallucinogenic substances isknown to produce mystical experiences. There has beenspeculation that plants with psychoactive propertieswere valued by the ancient Israelites, but no direct evi-dence has been uncovered for their actual use for in-ducing mystical experiences in this population.6 Anotherpossibility would be that of epilepsy-induced mysticalexperiences. Persons with epilepsy may experience ic-tal, postictal, or interictal schizophrenia-like symptoms,which can be indistinguishable from primary psychoticdisorders7,8 and occur in roughly 2%–7% of persons withepilepsy;9 2.2% of temporal lobe-onset seizures may beassociated with religious experiences.10,11
Grandiose and messianic-type delusions are recog-nized as occurring in association with complex partialseizure disorders.12 Published cases show ictal religiousexperiences to be awe-inspiring or ecstatic, but generally
J Neuropsychiatry Clin Neurosci 24:4, Fall 2012 http://neuro.psychiatryonline.org 411
MURRAY et al.

not successful in imparting detailed or complex infor-mation.10,13–17 Postictal psychosis (PIP) is more commonand tends to occur in close proximity to seizure clustersand can also be associated with a recent exacerbationin seizure frequency.18 It is estimated to account for aquarter of psychosis in epilepsy19,20 and occurs in up to18% of medically intractable focal epilepsy patients.21,22
Of persons with PIP, up to 25% may have religiousdelusions.
Only 2% of those who go on to have interictalpsychosis have religious delusions.23,24 Interictal psy-chosis is otherwise not readily distinguishable fromschizophrenia, but may manifest preservation of affect,fewer negative symptoms, and, arguably, greater in-sight. The greater similarities may lay in positive symp-tomatology; that is, that of thought disorder, delusions,and hallucinations.7 Reliable prevalence data are lack-ing, but it has been proposed that between 30% and60% of patients with partial seizures will also havesecondary generalized seizures.25–27
Abraham is not recounted as having had any in-firmities that might resemble the phenomena we nowcommonly understand to accompany seizures. Specifi-cally, there are no signs of repetitive behaviors, such asuncontrolled generalized or partial shaking, orofacial
automatisms, stereotyped behavioral changes, recurrentand consistent auras of fear (although fear did accom-pany some episodes), staring spells, loss of conscious-ness, falling spells, tongue-biting, or incontinence. Hisability to engage in varied dialogue with his halluci-nations would not be very typical of an ictal per-ceptual change, since seizures tend toward beingstereotyped in nature and not to be so changeableand interactive.10,13–17,28,29 Most generalized seizures,and, often, complex partial seizures, are associated withamnesia for the period during and immediately after aseizure, and persons often have baseline day-to-daycognitive impairments in memory and executive do-mains.30,31 There are no indications that Abraham ex-perienced uncontrolled motor events, amnestic periods,or cognitive impairments of any kind. A postictal or in-terictal psychotic state cannot be excluded, but is notparticularly suggested on the basis of the availableinformation.The absence of apparent affective, medical, or neuro-
logical conditions increases the possibility that a psy-chotic disorder could have been present. Schizophreniais often accompanied by both disorganized behavior andthought processes that interfere with life functioning.5
In the case of Abraham and in the others that follow,
FIGURE 1. Abraham Being Stopped From Sacrificing His Son Isaac by a Vision of an Angel (Genesis 22:9–12)
Laurent de la Hyre: Abraham Sacrificing Isaac (c1650), Musée Saint-Denis, Reims, France
412 http://neuro.psychiatryonline.org J Neuropsychiatry Clin Neurosci 24:4, Fall 2012
PSYCHOTIC DISORDERS IN RELIGIOUS HISTORY

disorganization and cognitive impairments are not ap-parent. Paranoid schizophrenia (PS), however, is a subtypeof schizophrenia that tends tomanifest little or no disorga-nization, has preserved functional affect, and is associatedwith better occupational and social functioning.5
Psychotic disorder, not otherwise specified (PD NOS)is another reasonable diagnostic alternative. PD NOSincludes those persons with psychotic symptomatologyfor which there is inadequate or contradictory informa-tion or symptoms that do not meet criteria for anyspecific psychotic disorder.5 Abraham’s clinical profilewould appear to best resemble that of PS or PD NOS,and perhaps, less likely, an affective disorder-relatedpsychosis. Abraham stands as the earliest case of a pos-sible psychotic disorder in literature.
MOSES
The story of Moses in the Bible is thought to have itssetting sometime between 1550 BCE and 1200 BCE.32
The stories about Moses include a great deal of infor-mation about his background, life functioning, beliefs,actions, and perceptual experiences (see Figure 2).Moses had perceptual experiences and behaviors thatfind closest parallel today with the DSM-IV-TR–definedphenomena of command AHs, VHs, hyperreligiosity,grandiosity, delusions, paranoia, referential thinking,and phobia (about people viewing his face). (See Table 3for examples.) Many of these features may occur to-gether in schizophrenia, affective disorders, and schiz-oaffective disorder.5 Moses also did not appear to haveany disorganization, catatonia, or negative psychiatricsymptoms, or difficulties with concentration, attention,and memory (see Table 2). Criterion A for schizophreniacould theoretically be fulfilled by his experiences thatresemble delusions and hallucinations. In fulfillment ofCriterion B, Moses’ social and occupational functioningcould be said to have declined from that of a presumablyeducated member of the Egyptian royal family to havingfled Egyptian society to become a shepherd working onthe periphery of the desert in a foreign land (Exodus 2:15–22). His flight from Egypt occurred before the onsetof AH and VH, thereby suggesting a prodromal decline
TABLE 1. Selected Examples of Passages With FeaturesResembling Psychiatric Phenomena
AbrahamAuditory and visual hallucinationsa: Genesis 12:1–3; 12:7; 13:14; 15:1–
11; 17:1–21;22:1–2; 22:11–12 (Figure 1)Paranoid Type (PS subtype) thought processesb: Genesis 12:3 (implies
a very Abraham-centered worldview of dispensing universalblessings and curses based on one’s interactions with Abraham);12:11–13; 14:22; 17:14; 20:11; 21:11–14 (potential mistrust, as seen bythe sending-away of his first-born son to eliminate competition forhis second son); 23:4 (He referred to himself as a stranger in a land heunderstood to be his inheritance from God); 24:3 (potential mistrustseen in the rejection of intermarriage for his son Isaac with anywomen in his region); 25:6 (potential mistrust as seen by the sending-away of of all his sons so as to remove Isaac’s competitors).
MosesAuditory and visual hallucinations of a grandiose nature with
delusional thought contenta: Exodus 3:2 (Figure 2); Exodus33: 21–23 related to 34:5–6
Paranoid Type (PS subtype) thought contentb: Exodus 32:25–29Phobia: Exodus 34:33Referential Thought Processes: Exodus 8:12–13, 8:31, 9:23, 9:33,
10:13–15, 10:22 (possible sandstorm)JesusParanoid-type (PS subtype) thought contentb: Matthew 10:34–39, 16:
21–23, 24:4–27; Mark 13:5–6; Luke 10:19; John 3:18; John 14:6–11Auditory and visual hallucinationsa: Matthew 3:16–17, 4:3–11; Luke 10:
18; John 6:46, 8:26, 8:38–40, 12:28–29Referential thought processes: Mark 4:38–40 (Figure 3); Luke 18:31PaulAuditory and visual hallucinationsa: Acts 9:4–6,16:9,18:9, 22:7–11
(Figure 4), 26:13–18; 2 Corinthians 12:2–9Paranoid-type (PS subtype) thought contentb: 1 Corinthians 10:
20–22; 11:29–32; 1:20–21; 2 Corinthians 6:14; 7:1; 11:12–15; 11:21–23
aHallucinations in PS are typically related to the themes ofdelusions.5
bParanoid-type (PS subtype) thought content: Delusions are typicallypersecutory or grandiose or both. Delusions with other themes, such asjealousy, religiosity, or somatization may also occur. They are usuallyorganized around a theme.5
All biblical references are from The New Oxford Annotated Biblewith the Apocrypha, Revised Standard Version. Edited by May HG,Metzger BM, New York, Oxford University Press, 1977.
TABLE 2. Diagnostic Criteria for Schizophrenia
A. Characteristic symptoms: Two or more of the following, eachpresent for much of the time during a 1-month period (or less, ifsymptoms remitted with treatment).
DelusionsHallucinationsDisorganized speechGrossly disorganized behavior or catatonic behaviorNegative symptoms: affective flattening, alogia, or avolitionNote: Only one Criterion A symptom is required if the delusions are
bizarre or hallucinations consist of a voice keeping up a runningcommentary on the person’s behavior or thoughts, or two or morevoices conversing with each other.
B. Social/occupational dysfunction: For a significant portion of thetime since the onset of the disturbance, one or more major areas offunctioning, such as work, interpersonal relations, or self-care, aremarkedly below the level achieved prior to the onset.
C. Duration: Continuous signs of the disturbance persist for at least 6months. This 6-month period must include at least 1 month ofsymptoms (or less, if symptoms remitted with treatment)
D. Schizoaffective and mood-disorder exclusionE. Substance/general medical condition exclusionF. Relationship to a pervasive developmental disorder
Adapted from the Diagnostic and Statistical Manual of MentalDisorders, 4th Edition, Text Revision. Washington, DC, AmericanPsychiatric Association, 2000, pp 297–343.
J Neuropsychiatry Clin Neurosci 24:4, Fall 2012 http://neuro.psychiatryonline.org 413
MURRAY et al.

in functioning before the onset of psychosis. A prodromerefers to the early symptoms and signs of an illness thatprecede the characteristic manifestations of the acute,fully developed illness. A prodromal period may pre-cede the onset of schizophrenia by months to up to 10years in 70% of patients33 and up to 20 years in somecases.34 The period over which Moses had these ex-periences was in excess of 40 years, fulfilling CriterionC. His social functioning and leadership skills weresufficiently intact to have made it less likely that he hadperiods of debilitating major depression or florid maniathat might have undermined his effectiveness as a leader.This could fulfill Criterion D by reducing the likelihoodof mood disorder-associated psychosis. It should benoted that the religious writings attributed to Moses’
authorship, the Pentateuch, could suggest the presenceof an exaggerated urge to write. Such hypergraphia is anonspecific finding more commonly associated withmania, hypomania, or mixed states; however, it is also afeature of schizophrenia and temporal lobe epilepsy.35–37
Trimble writes that the hypergraphic output of schizo-phrenic and epileptic patients is rarely creative. They areoften loosely mystical, and both perseverative and vaguein content.37 In contrast to the relative paucity of poetswith schizophrenia or epilepsy, he observes that thenumber of poets suggested to have mood disorders arerepresented in far greater numbers.37 Therefore, mooddisorder-associated psychoses remain quite viable in thecase of Moses.There is no indication in the Bible that Moses ex-
perienced metabolic dysregulations or that he usedhallucinogenic intoxicants as an explanation for his be-havioral or perceptual changes. There are also no keyfeatures, as previously mentioned, to implicate epilepsyas a cause of mystical experiences. He lived a long life, inexcess of 100 years, arguing against the presence ofprogressive medical or neurological illnesses. The cri-teria for diagnosis of PS would be fulfilled by the pre-dominance of delusions and hallucinations in the absenceof disorganization, negative psychiatric symptoms, orcognitive impairment.An increased propensity for violence has been ob-
served in some individuals with PS.38 Moses’ increasedpropensity for violence could be viewed as corroborativefor a diagnosis of PS. Reasonable diagnostic alternativesmight include PD NOS, bipolar disorder, and schizo-affective disorder. If the first five books of the bible arecredited to Moses’ authorship, then a bipolar disorder orperhaps schizoaffective disorder would be more compat-ible with his writing abilities.
JESUS
Jesus is the foundation figure of Christianity, who isthought to have lived between 7–2 BCE and 26–36 CE.The New Testament (NT) recalls Jesus as having ex-perienced and shown behavior closely resembling theDSM-IV-TR–defined phenomena of AHs, VHs, delu-sions, referential thinking (see Figure 3), paranoid-type(PS subtype) thought content, and hyperreligiosity (seeTable 1). He also did not appear to have signs orsymptoms of disorganization, negative psychiatricsymptoms, cognitive impairment, or debilitating mood
FIGURE 2. Moses’ Vision of the Burning Bush (Exodus 3:2)
Moses Before The Burning Bush (1613–14) By Domenico Feti, atKunsthistorisches Museum, Vienna, Austria
414 http://neuro.psychiatryonline.org J Neuropsychiatry Clin Neurosci 24:4, Fall 2012
PSYCHOTIC DISORDERS IN RELIGIOUS HISTORY
disorder symptoms. NT accounts about Jesus mentionno infirmity. In terms of potential causes of perceptualand behavioral changes, it might be asked whetherstarvation and metabolic derangements were present.The hallucinatory-like experiences that Jesus had in thedesert while he fasted for 40 days (Luke 4:1–13) mayhave been induced by starvation andmetabolic derange-ments. Arguing against these as explanations for all ofhis experiences would be that he had mystical orrevelation experiences preceding his fasting in the desertand then during the period afterward. During theseperiods, there is no suggestion of starvation or metabolicderangement. If anything, the stories about Jesus and hisfollowers suggest that they ate relatively well, ascompared with the followers of his contemporary, Johnthe Baptist (Luke 7:33–34). Epilepsy-associated psy-chotic symptoms are possible, but Jesus is not recountedas having any of the previously-mentioned commonhallmarks of epilepsy. A decline in his occupational andsocial functioning cannot be established because of a lackof sufficient information. His experiences appear to haveoccurred over the course of at least the year before hisdeath. The absence of physical maladies or apparentepilepsy leaves primary psychiatric etiologies as moreplausible. As seen with the previous cases, Jesus’experiences can be potentially conceptualized withinthe framework of PS or psychosis NOS. Other reason-able possibilities might include bipolar and schizoaffec-tive disorders.
There is a 5%–10% lifetime risk of suicide in personswith schizophrenia.39 Suicide is defined as a self-inflicteddeath with evidence of an intention to end one’s life. TheNT recounts Jesus’ awareness that people intended tokill him and his taking steps to avoid peril until the timeat which he permitted his apprehension. In advance, he
explained to his followers the necessity of his death asprelude for his return (Matthew 16:21–28; Mark 8:31;John 16:16–28). If this occurred in the manner de-scribed, then Jesus appears to have deliberately placedhimself in circumstances wherein he anticipated hisexecution. Although schizophrenia is associated withan increased risk of suicide, this would not be a typicalcase. The more common mood-disorder accompani-ments of suicide, such as depression, hopelessness,and social isolation, were not present,40 but other riskfactors, such as age and male gender, were present.Suicide-by-proxy is described as “any incident in whicha suicidal individual causes his or her death to be carriedout by another person.”41,42 There is a potential parallelof Jesus’ beliefs and behavior leading up to his death tothat of one who premeditates a form of suicide-by-proxy.
ST. PAUL (SAUL OF TARSUS)
St. Paul lived during the first century CE. It has beenspeculated that his religious experiences resulted fromtemporal lobe epilepsy.43 We would argue that it is notnecessary to invoke epilepsy as an explanation for theseexperiences. St Paul’s mood in his letters ranged fromecstatic to tears of sorrow, suggesting marked moodswings.44,45 He endorsed an abundance of sublimeauditory and visual perceptual experiences (2 Corinthi-ans 12:2–9) that resemble grandiose hallucinations withdelusional thought content. He manifested increasedreligiosity and fears of evil spirits, which resemblesparanoia. These features may occur together, in asso-ciation with primary and mood disorder-associated psy-chotic conditions.
TABLE 3. Clinical Signs and Symptoms of Schizophrenia
Religious Figures
Behaviors Resembling Abraham Moses Jesus St Paul
Auditory hallucinations + + + +Visual hallucinations + + + +Hyper-religiosity + + + +Grandiosity + + + +Delusions + + + +Paranoia + + + +Disorganization — — — —Negative symptoms — — — —Duration of symptoms years .40 years .1 year yearsDecline in occupational functioning I + I I
+: present; —: not present; I: inconclusive evidence or unknown.
J Neuropsychiatry Clin Neurosci 24:4, Fall 2012 http://neuro.psychiatryonline.org 415
MURRAY et al.
In 2 Corinthians 12:7, St Paul relates “a thorn wasgiven me in the flesh, a messenger from Satan, to harassme, to keep me from being too elated.” This thorn hasbeen speculated to be a reference to epilepsy.43 Othertheories have proposed that the thorn was a physicalinfirmity, the opposition of his fellow Jews,46 or a ha-rassing demon.47
We propose that he perceived an apparition or voicethat he understood to be a harassing, demonic messenger
from Satan. This perceptionmight have afflicted himwithsome amount of negative commentary of the type char-acteristic for psychotic conditions, resulting in psycho-logical distress.The complexity of Paul’s interactions in his perceptual
experiences weighs against a seizure ictus as a cause, asdoes the lack of evidence for more common epilepticaccompaniments, such as repetitive stereotyped behav-ioral changes and cognitive symptoms, as previously
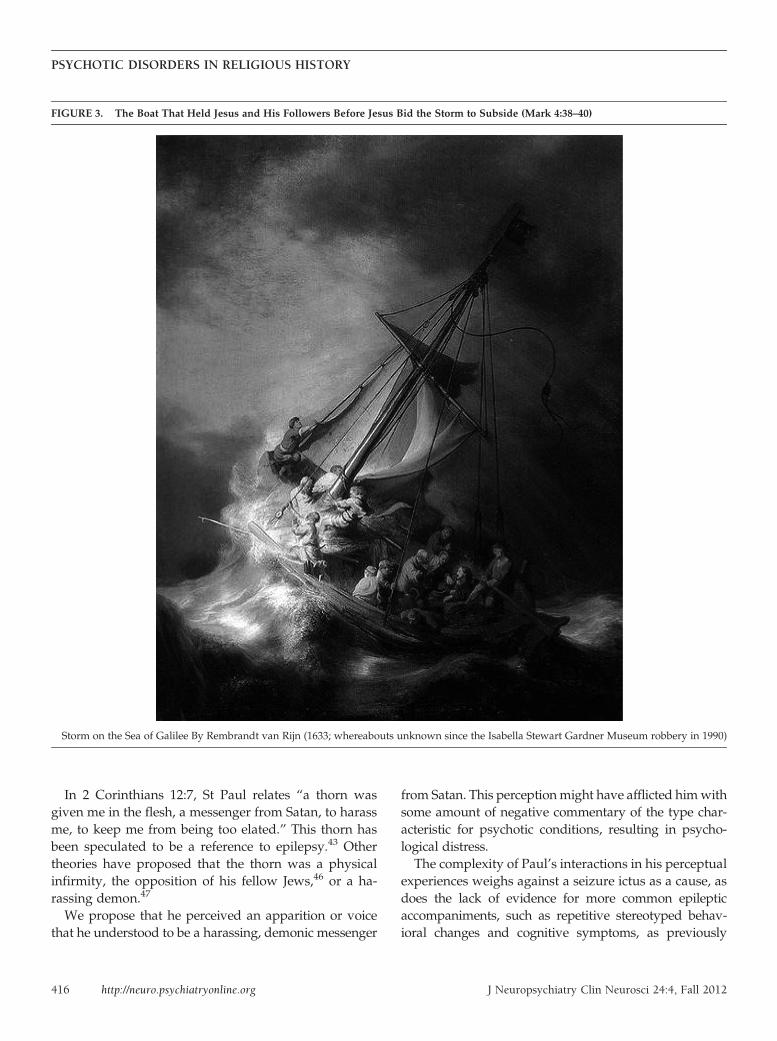
FIGURE 3. The Boat That Held Jesus and His Followers Before Jesus Bid the Storm to Subside (Mark 4:38–40)
Storm on the Sea of Galilee By Rembrandt van Rijn (1633; whereabouts unknown since the Isabella Stewart Gardner Museum robbery in 1990)
416 http://neuro.psychiatryonline.org J Neuropsychiatry Clin Neurosci 24:4, Fall 2012
PSYCHOTIC DISORDERS IN RELIGIOUS HISTORY

discussed. Paul does, however, manifest a number of per-sonality characteristics similar to the interictal personal-ity traits described by Geshwind,48–50 such as deepenedemotions; possibly circumstantial thought; increased con-cern with philosophical, moral and religious issues; in-creased writing, often on religious or philosophicalthemes; and, possibly, hyposexuality (1 Corinthians 7:8–9). These characteristics are controversial as to their spe-cificity for epilepsy,51,52 with a preponderance of largerstudies not confirming a specific personality type asso-ciated with seizure disorders.51–57 Similar features mayalso be present in bipolar disorder5,35,36 and schizophre-nia.35,36 As previously mentioned, productive writing tendsto be more strongly associated with mood disorders thanpsychosis or epilepsy. This is persuasive toward Paul hav-ing amood disorder, rather than schizophrenia or epilepsy.
Paul’s religious conversion on the road to Damascus(Acts 9:1–19, 22:6–13, 26:9–16) is an event understood asmarked by the acute onset of blindness. This blindnesshas been hypothesized to have been postictal in nature43
or psychogenic.58 There appears to be a lack of clarity asto whether this was literal visual blindness or meta-phorical, since Paul refers to persons outside his im-mediate belief system as spiritually blind or having theireyes closed to spiritual truth (Acts 28:26; Romans 11:8,11:10; 2 Corinthians 4: 3–5; Ephesians 1:18). Differencesin the three most detailed conversion-experience ac-counts contribute to this ambiguity. Acts 26:12–18 relateshis conversion, during which a vision of Jesus tasks himto spiritually open the eyes of the people to whom hewill be sent (see Figure 4). In this account, there is nomention of acute-onset visual loss followed by its re-storation. The application of the blindness metaphor inActs 26:12–18 may suggest that Paul’s own loss of visionwas equally metaphorical and served as a descriptor ofhis profound realization of feeling suddenly bereft ofspiritual understanding; that is, realizing his eyes to bespiritually closed, before the completion of his conver-sion to the new religious sect. In such an emotional state,it is speculated that he might have required encourage-ment and emotional assistance to reach Damascus.Another possibility would be that of blindness due toconversion disorder. The absence of other episodes ofvisual loss (i.e., lack of event stereotypy), the absence offeatures often seen with postictal blindness (a general-ized seizure, anosognosia for deficit, or a gradual returnof vision),59 the presence of complex, mood-congruentauditory–visual experiences resembling hallucinations,and the possible sudden return of his eyesight with a
compassionate touch does not fit well into a readilydiscernable neurological pattern of vision loss. His per-ceptual experiences, mood variability, grandiose-likesymptoms, increased concerns about religious purity,and paranoia-like symptoms could be viewed as re-sembling psychotic spectrum illness (see Table 1). Psy-chiatric diagnoses that might encompass his constellationof experiences and manifestations could include para-noid schizophrenia, psychosis NOS, mood disorder-associated psychosis, or schizoaffective disorder. Paul’spreserved ability to write and organize his thoughtswould favor a mood disorder-associated explanation forhis religious experiences.
COMMENTARY ABOUT DIFFERENTIALDIAGNOSIS
Although Abraham had a revelatory experience duringsleep (i.e., the prophecy foretelling his descendants’being enslaved in Egypt [Genesis 15:12–16]), and Paulhad visions during the night (Acts 16:9, 18:9); most of therevelations experienced by these figures are not wellexplained by sleep phenomena such as dreams. A host ofother conditions might precipitate revelation-like per-ceptual experiences (Table 4). Perhaps the foremost ofthese possibilities would be postictal and interictal psy-chotic states, which cannot be entirely excluded, sinceconvulsions can be absent in some cases, and an absenceof description in the sources does not exclude the pos-sibility of seizures. Fear did occur with a number ofAbraham and Moses’ experiences, raising the prospectof a seizure aura of fear. Not all of their mystical ex-periences are recounted as associated with fear, indi-cating a lack of seizure-like stereotypy. In the event thatseizure-related psychotic states were etiologic, the path-way to psychosis would be different, but the premise ofpsychosis having a formative role in their revelatoryexperiences would still be viable.Nevertheless, based on the available descriptions that
mention features bearing a striking resemblance to psy-chotic symptoms and the absence of mention of eventsresembling overt seizures, it is more parsimonious toexplain these experiences as potentially due to a primarypsychiatric condition. The remaining conditions in Table4 are not particularly suggested by a medical review ofthe source material.A shared psychotic disorder (folie à deux) is a possi-
bility for each of the subjects discussed. The essential
J Neuropsychiatry Clin Neurosci 24:4, Fall 2012 http://neuro.psychiatryonline.org 417
MURRAY et al.
feature of this condition is that of a delusion that de-velops in an individual who is involved in a closerelationship with another person, sometimes termed the“inducer” or “primary case,” who already has a psy-chotic disorder with prominent delusions. The individ-ual completely or partly comes to share the delusionalbeliefs of the primary case.5,60 In our subjects, there areno known close associates having an equivalent spec-trum and magnitude of symptoms who might serve therole of a primary case. Conversely, each of our subjectsmight also have theoretically served as a primary case ina shared psychotic-disorder relationship. Among otherpsychiatric explanations, which should be mentioned for
completeness, are those of mystical experiences occur-ring as a result of unconscious forces.61 These maymanifest by way of conversion disorder or a dissociativecondition such as a trance-like state or dissociativeidentity disorder (DID). Another possibility would bethat of a deliberate misrepresentation of supernaturalrevelation. This hypothesis would require significant in-terpolation to support. An argument against this wouldbe that the sources used appear entirely sincere abouttheir belief in the divine origin of these experiences.A very complex state of affairs would be that of a psy-chotic disorder comorbid with deliberate misrepresen-tations, conversion symptoms, dissociative trance-like
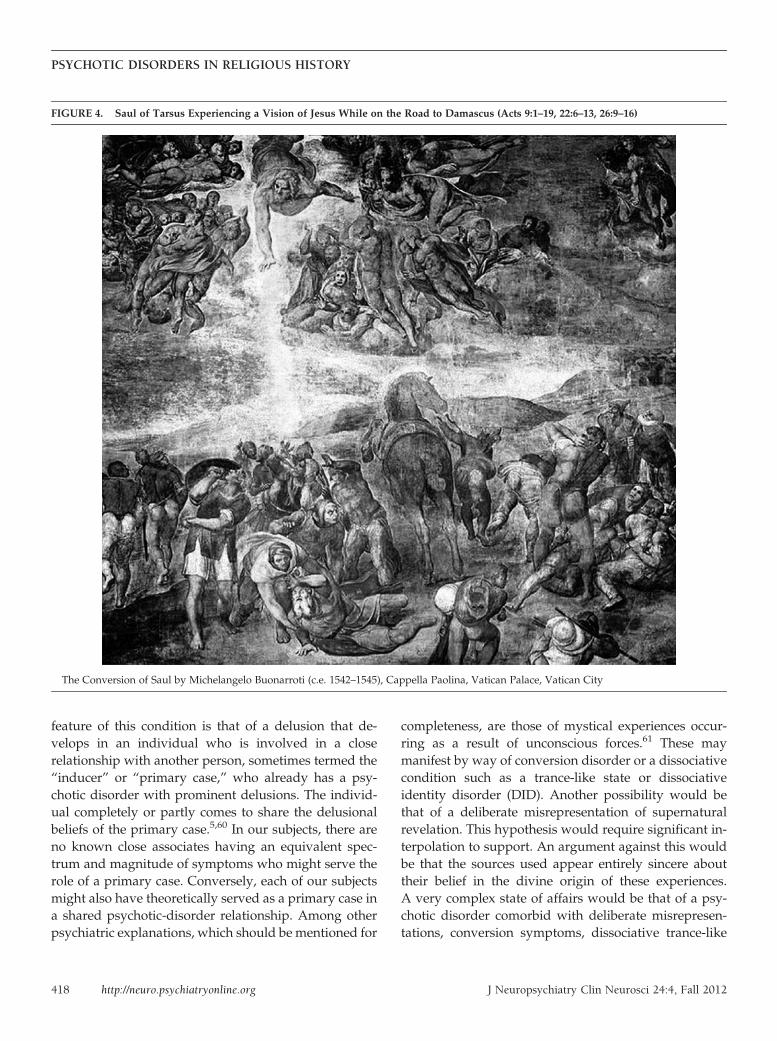
FIGURE 4. Saul of Tarsus Experiencing a Vision of Jesus While on the Road to Damascus (Acts 9:1–19, 22:6–13, 26:9–16)
The Conversion of Saul by Michelangelo Buonarroti (c.e. 1542–1545), Cappella Paolina, Vatican Palace, Vatican City
418 http://neuro.psychiatryonline.org J Neuropsychiatry Clin Neurosci 24:4, Fall 2012
PSYCHOTIC DISORDERS IN RELIGIOUS HISTORY

states, and DID. These hypotheses are mentioned toensure an adequate appraisal of the possibilities despitean acknowledged inability to substantiate any of theseprocesses being at work.
LIMITATIONS OF THE ANALYSIS
The sources relied upon to derive information about oursubjects are not medical records. The modern readerfaces challenges interpreting events far removed fromour own time and culture and which are recounted ina different language by authors who had their ownbiases. It might be supposed that our subjects can only beunderstood in the context of these factors and accordingto the norms of religious experience of their day. Othersmight advise that these religious writings should only beinterpreted nonliterally, that is, metaphorically andabstractly, thereby eliminating the possibility of medicalscrutiny.
Still others might propose that medical knowledge isalways in a state of flux, which renders impermanentthis type of analysis because of its dependence on theprevailing medical vogue of the day.62 Retrospectivediagnosis may also be asserted to be a transgression ofmedical principles, since a medical opinion is renderedon a patient who was never seen or examined.62
Starting with the last point, since it would offer anobstacle to any prerequisite ability to derive informationabout persons not present for examination, it is our viewthat it is an oversimplification to state that all diagnosismust ethically and methodologically rest upon havingthe patient present in person. The behavioral and
neurological fields of medicine frequently rely upon theobservations of family, friends, and associates of ourpatients because of patients’ sometime reticence to talkabout their symptoms, insufficiency of information, orinaccuracies of self-reporting. Samples of a patient’swriting are frequently used to assess movement,63
thought content, language function, organization, andability to abstract. Moreover, advances in understandinghuman physiology have afforded us some confidence forinterpreting certain types of findings, such as those at-tributed to the 6th century BCE Indian physicianShushruta, who described sweet urine.64 We need nothave been present to recognize a probable case of di-abetes mellitus. Similarly, other conditions may bearsufficient signs through their descriptions in literature toallow discussion about their causes. The figures we havediscussed have information to draw upon, some ofwhich is held by religious tradition to be authored by theindividuals (Moses and Paul), and some authored byclose associates (of Jesus and Paul), who have potentiallyprovided more information about them than availablefor most persons born before the present age. We re-cognize an important limitation inasmuch as we ap-proach these source documents as most likely beingcomposites of the perspectives and beliefs of authors,most of whom would not have personally known oursubjects.65,66 This would be similar to other ancientwriters who related stories about people and events thatthey were not present to witness. This analysis dependsupon our sources’ reflecting, in some measure, actualpeople and events as they were.The reader is then reminded that the medical in-
terview and examination are not fixed in any generalway. It is understood that a physician must adjust bothinterview and examination according to purpose andcircumstance.67,68 A psychiatrist may restrict examina-tion to discussion about relevant feelings and percep-tions, never physically touching the patient, but stillreliably deducing level of alertness, orientation, atten-tion, ability to self-regulate and perceive social cues,thought organization, language abilities, memory, in-sight, judgment, and general intelligence, among otherthings. A surgeon may emphasize the need to palpatea mass to determine its characteristics. These approachesare very different and are adjusted according to specificgoals. The paradigm for understanding behavior in termsof a brain–behavior relationship is largely a product ofthe last century of brain research, and it was not avail-able to our predecessors.69 It is a useful exercise to apply
TABLE 4. Causes of Psychosis Secondary to Medical orNeurological Conditions
Brain neoplasmsComplex migraineDeliriumDementing illnessEncephalitis (infectious, autoimmune, or paraneoplastic)Endocrine dysfunctionEpilepsy (ictal, postictal, and interictal)Hypnagogic imageryInfection (such as neurosyphilis)Malnutrition/starvationMetabolic derangementsMetabolic storage diseasesParasomniaPoisonings and intoxicationsStrokeTraumatic brain injury sequelaeVitamin deficiencies (B1 or B12)
J Neuropsychiatry Clin Neurosci 24:4, Fall 2012 http://neuro.psychiatryonline.org 419
MURRAY et al.

our modern models of how behavior correlates to neuralanatomy to test limits for localization and diagnosis whilerecognizing and offering scrutiny to their limitations.
We can briefly outline an example of how an un-derstanding of modern functional neuroanatomy canallow a previously unattainable degree of discernmentabout an individual not present for examination. Settingaside questions about authenticity of authorship andactuality of events, we will look at what might be de-termined about St. Paul, ostensibly from his own hand.His writings indicate that he traveled extensively, evensurviving many physical hardships (2 Corinthians 11:23–27). These activities would minimally necessitate ge-nerally intact motor function, sensation, and coordina-tion. These abilities are now known to be accomplishedthrough the action of specific brain cortical–subcorticalcircuits (in frontal and parietal lobes) that are linkedin a type of parallel processing and modulated by thecerebellum. The cortical–subcortical circuits are com-posed of their cortical target regions, and have as theirconstituents the striatum (caudate, putamen, ventralstriatum), globus pallidus, and substantial nigra, andthalamus, which then projects back to the cortex.70 Thesesystems would appear to be grossly intact, to enduresuch extended travel and hardship. Paul’s detailed re-collections of events and his references to the contents ofprevious epistles advocate for intact memory systems,both semantic and episodic, at the time of his writing.These memory systems are now understood to be relianton a deep-brain circuitry consisting of the hippocampus,fornix, mamillary body, mamillothalamic tract, anteriornucleus of the thalamus and cingulated gyrus (circuit ofPapez). Paul spoke to many people on his journeys,indicating adequate function of language, which is de-pendent on perisylvian cerebral structures. His ability toform social relationships and speak persuasively usingsome metaphorical language suggests relatively pre-served basic functions of frontal lobe and limbic systems,which oversee self-regulation, emotions, abstraction,ability to organize thoughts, and focus attention. Hisability to maintain wakefulness, speak, eat, and breathesupports an adequately functioning brainstem. For cir-cumscribed purposes, this examination can be moreenlightening than that of a 1st-century-trained physiciansitting in the room with St Paul or that of a 21st-centuryphysician without the appropriate training. Morenuanced assessment of cognition and behavior mightbe achieved via application of neuropsychiatric and be-havioral neurological approaches that utilize modern
understanding about patterns of neurological and psy-chiatric illnesses. The preceding inventory of St. Paul’sgenerally intact neural systems can be largely extendedto each of our subjects. This would be the first suchinventory supporting a general preservation of such neu-ral systems for Abraham, Moses, Jesus, and St Paul. Itis acknowledged that medical analyses are, in the end,susceptible to being incorrect or incomplete and shouldalways be open to revision when new information be-comes available. Without academic scrutiny of methodsand conclusions, improvements in understanding can-not be achieved.We now turn to several lines of reasoning that favor
the credibility of our proposals.First, schizophrenia research has yielded compelling
evidence to support the model for genetic vulnerability,coupled with environmental and psychosocial stressors,the so-called diathesis–stress model, as a mechanism bywhich schizophrenia occurs.71–73
Cross-cultural clinical characteristics,74 an increasedrisk of having the disorder according to degree of kinshipto those affected, a host of identified genes affecting riskfor developing schizophrenia, and an increased preva-lence of subtle brain developmental abnormalities in per-sons with schizophrenia70,75 suggest interactions betweengenetic and environmental influences75,76 that, so far as isknown, would not be expected to have been different inpersons living in the ancient world.A second point hinges upon recognizing psychosis in
the pages of ancient writings. Psychosis has been knownby many names throughout history. Only recently hasmore precise nomenclature been developed. It should beno surprise that we would have difficulties recognizingcases in ancient writings when gazing through the eyes ofancient authors. Modern understanding about psychosisholds that a central feature is thought processes reflectinga highly distorted view of reality or a complete loss ofcontact with reality. DSM-IV-TR indicates that the term“psychotic” refers to a constellation of symptoms thatmay vary to some extent across diagnostic categories, butit generally refers to delusions, any prominent hallucina-tions, disorganized speech, or disorganized or catatonicbehavior.5 A delusion is a false belief based on incorrectinference about external reality that is firmly sustaineddespite what almost everyone else believes and despitewhat constitutes incontrovertible and obvious proof orevidence to the contrary.The belief is not one ordinarily accepted by other mem-
bers of the person’s culture or subculture.5 Delusional
420 http://neuro.psychiatryonline.org J Neuropsychiatry Clin Neurosci 24:4, Fall 2012
PSYCHOTIC DISORDERS IN RELIGIOUS HISTORY

conviction occurs on a continuum.5 The depictions of oursubjects indicate that they may have either found theirown experiences not entirely believable to themselves,understood that their experiences would be hard forothers to believe, or that they were perceived by theircontemporaries as being mad. Genesis: 12–20 recountsthat God made promises of blessings, progeny, and landto Abraham. Despite these assurances, Abraham’s fear ofdeath prompted him to surrender his wife to the affectionof kings on two occasions in order to forestall his ownexecution. Moses, for his part, points out to God inExodus 4:1 that the message he was given to bring to theIsraelites stood a good chance of not being believedby a people whom we would now characterize aspolytheistic,77 superstitious, and therefore more likely tohave accepted such happenings. Their rapid reversion toprevious religious practices despite a series of miracles(Exodus 32) appears to support Moses’ concern. Mark 3:21 confirms an occasion where Jesus’ friends and familyviewed him as mad or “beside himself.” It is intrinsic tohis narrative that the people of his hometown (Mark 6:1–6) and the religious authorities of the day also did notaccept his message. St Paul’s contemporary Festus, thelocal Roman governor of Judea, in Acts 26:24 exclaimedthat Paul appeared “mad” or not sane. These events areclosest in time to our subjects andmight suggest psychotictype thought processes.
A third point speaks to the concern that religious andcultural factors of the day need to be taken into account.DSM-IV-TR recognizes that visual and auditory halluci-nations with a religious content may be a part of normalreligious experience in some cultures.5 Rediger observesthat there is a tendency of the Western mind-set topathologize spiritual experiences and that there maybe an overdependence of psychological interpretationon material existence.78 He suggests that there is ananosognosia for experiential phenomena that exist out-side the narrow band of consciousness that psychologyapprehends and that there is a great deal to learn fromEastern traditions in this regard.78 He recommends anapproach that correlates phenomena falling outside thepsychological paradigm with medical science ratherthan pathology. In harmony with this perspective is therecognition that some spiritual experiences can havevery beneficial effects for transforming the lives of someindividuals, allowing them to surmount obstacles andchange destructive behaviors. In response to thesethoughts, we emphasize that our intent is not to provethat the experiences of our subjects could not have
resulted from normal religious experiences in the con-text of cultural factors; it is to apply a modern neuro-behavioral paradigm to the experiences of our subjectsand thereby advance a dialogue about the rational limitsof perceptual experience. Toward this, we point out thattheir experiences, if they occurred as narrated, mightalso be conceptualized as psychotic spectrum becauseof their resemblances, by way of their recurrent nature,intensity, subject matter, grandiose-like qualities, andsimilarity to psychotic auditory-visual phenomena.It is recognized that the content of schizophrenic de-
lusions and hallucinations is significantly influenced bysociocultural background. Different cultural experiencescan result in different delusional form and content.79,80
The DSM-IV-TR criteria presume our ability to distin-guish psychotic phenomena from other normal experi-ences in the context of a given culture. Unfortunately,evidence-based algorithms for accomplishing this arenot available. Further complicating our task is the gulfof time over which we must work. Overcoming theseobstacles in some measure might again be accomplishedthrough drawing on the perspectives of persons closer intime and culture to our subjects.The earliest believers found the experiences of the
subjects sufficiently removed from the sphere of normallife so as to be understood as a product of a highly un-usual relationship with a divine force.66 Those who didnot believe may have had various reasons, some ofwhich would have been that the message was too farfrom their reality to be accepted.From today’s vantage-point, if our subjects’ experi-
ences had resulted only from a convergence of normal in-dividual and community religious experiences, we shouldhave expected numerous such stories and therefore noreason to take notice of these now because of their mun-dane nature. Surviving literature, whether of ClassicalGreek, Roman period, or biblical origin, does not providesupport that it was commonplace in the ancient world forthe general population to have recurrent auditory-visualexperiences as grand in scope as those of our subjects. Thepopulations of the earliest followers of such new belief-systems, as those of our subjects, would constitute smallgroups able to accept the beliefs before the emergence ofsocial pressures related to larger group dynamics. How dowe explain the existence of the earliest followers? Theirpresence would not be expected from an association withindividuals having a highly distorted view of reality.Social models of psychopathology may be useful
for understanding how this might have happened.
J Neuropsychiatry Clin Neurosci 24:4, Fall 2012 http://neuro.psychiatryonline.org 421
MURRAY et al.

Social-distance theory and communications-disorder the-ory suggest that differentiating sanity from psychosis canbe achieved, based on the degree to which beliefs hamperor facilitate communication and acceptance by society.Those who deviate excessively from the societal norms donot relate to the populace, are not understood, becomesocially isolated and stigmatized, and may be identifiedas not sane.81 This point of view might define as sane anyperson who is able to maintain acceptance and commu-nication with a social group. Not accounted for by thistheory are individuals who appear to demonstrate sus-tained paranoid, grandiose, messianic-type delusions,who, in more modern times, have drawn numbers ofadherents. Two such individuals are David Koresh, of theBranch Dravidians,82 and Marshall Applewhite, of theHeaven’s Gate cult.83 There are others in recent times whohave claimed to be prophet, messiah,84 Jesus,85 Buddha,86
avatar,87 or madhi,88 who have acquired followings. IfDavid Koresh and Marshall Applewhite are appreciatedas having psychotic-spectrum beliefs, then the premisebecomes untenable that the diagnosis of psychosis mustrigidly rely upon an inability tomaintain a social group. Asubset of individuals with psychotic symptoms appearsable to form intense social bonds and communitiesdespite having an extremely distorted view of reality.The existence of a better socially functioning subsetof individuals with psychotic-type symptoms is cor-roborated by research indicating that psychotic-likeexperiences, including both bizarre and non-bizarredelusion-like beliefs, are frequently found in the generalpopulation. This supports the idea that psychotic symp-toms likely lie on a continuum.89–92
Political-psychologymodels of leader–follower relation-ships may provide useful insights as to how early fol-lowers could have coalesced around our subjects.Wilner93
surveyed the literature on the topic of charismatic leader-ship and defined it as a relationship between a leader anda group of followers, having the following properties:
1. The leader is perceived by the followers as somehowsuperhuman.
2. The followers blindly believe the leader’s statements.3. The followers unconditionally complywith the leader’s
directives for action.4. The followers give the leader unqualified emotional
support.
Also, Wilner identifies four “catalytic factors” that areshared by charismatic leaders. The first factor is theassimilation of a leader to one or more of the dominant
myths of his society or culture. The second is the per-formance of what appears to be an extraordinary orheroic feat. The third is the projection of the possessionof qualities with an uncanny or a powerful aura. Finally,there is outstanding rhetorical ability”93.It is reasonable to speculate that a charismatic leadership–
follower group dynamic was present between our sub-jects and their followers. Little further comment can bemade about Abraham in this regard since so little in-formation is available about him. Moses felt himself notto be a good speaker, and his brother Aaron was ap-pointed to speak on his behalf to the community (Exodus4:10–16). This raises interesting questions about whatroles community members might contribute to thefunctioning of a leadership–follower dynamic in orderto supplement the leader’s deficiencies. The narrativesof Jesus and Paul have details which could fit intoa charismatic leader–follower paradigm of groupbehavior.Creating and sustaining groups would be dependent
on additional mechanisms:Wilfred Bion94 observed three patterns of group
behavior that occur in healthy, mature adults, whereingroup members act as if they are dominated: the de-pendency group, the pairing group, and the fight–flightgroup. The dependency group turns to an omnipotentleader for security, behaving as if they do not have in-dependent minds of their own. Members blindly seekdirections and follow orders unquestioningly. They tendto idealize and place the leader on a pedestal. When theleader fails to meet the standards of omnipotence andomniscience, a period of denial, then anger, and dis-appointment result. In the pairing group, the membersact as if the goal of the group is to bring forth a messiah,someone who will save them. There is an air of optimismand hope that a new world is around the corner. Thefight–flight group organizes itself in relationship to aperceived outside threat. The group itself is idealizedas part of a polarizing mechanism, while the outsidepopulation is regularly seen as malevolent in motivation.The threatening outside world is at once a threat tothe existence of the group and the justification for itsexistence. Each of these group types regularly character-izes the followers in charismatic leader–follower rela-tionships.95 It is reasonable to propose that one or moreof these types of group dynamics were present tovarying degrees, whether simultaneously or in varioussequences, in our subjects’ groups as they developedtheir beliefs over time.
422 http://neuro.psychiatryonline.org J Neuropsychiatry Clin Neurosci 24:4, Fall 2012
PSYCHOTIC DISORDERS IN RELIGIOUS HISTORY

How do individuals with mental illness rise topositions of leadership? Ghaemi96 sets forth a hypothesisthat there are key elements associated with mentalillness that may be beneficial for leadership abilities:realism, resilience, empathy, and creativity.96 His anal-ysis of several notable political, military and businessleaders and review of psychological research leads to hisproposal that depression can be associated with anincrease in each of these qualities, and mania can beassociated with an enhancement of creativity and re-silience. Depression promotes leaders’ being more re-alistic and empathic, whereas mania promotes theirbeing more creative and resilient.96 He adds that whendepression andmania occur together in bipolar disorder,it may result in a further increase in leadership skills.Such individuals, he proposes, benefit indirectly fromentering and leaving these mood states in addition tobeing in their well state between episodes.96 If this wereto hold true, then our subjects might be more likely tohave affective disorder-associated psychotic conditionsand thereby could have benefitted from spending periodsin various mood states, including their well states. Thequality of realismwould be expected to bemost adverselyaffected in a psychotic state, especially when judged fromthe standpoint of modern sensibilities. With respect toreligious beliefs arising during historical periods pre-ceding the advent of increased understanding about thenatural world, there might have been less by which tojudge this quality and, therefore, more cultural toleranceor acceptance of a wider range of ideas.
A shared psychotic disorder5,60 is another means bywhich the earliest followers may have received theirbeliefs, with each of our subjects being a primary case.Although occurring primarily in the form of a dyadicrelationship, paranoid delusions have been reported tooccasionally occur in larger sect-like groups whosemembers become infused with the paranoid ideation ofa dominant member. Norman Cameron termed this a“paranoid pseudocommunity.”97–99 This term is used todenote an imagined persecutorial conspiracy directed atthe group member. Once separated from the group’ssocial fabric, many members have been observed to re-gain the ability to view others without undue levels ofsuspicion.100 This pattern of group behavior may lie alonga continuum with that of the fight–flight group describedby Wilfred Bion. Much more speculatively, each of oursubjects and their followers could have been either aninitiator or recipient in a chain of persons who transmitdelusional-like beliefs. Each recipient would then act as
the primary case to another individual. No reported casesof such a chain of transmission of delusion-like beliefs areknown to the authors, and, therefore, this possibility ishighly speculative. Generally speaking, it is an individu-al’s insight and amenability to reason that are importantmeans by which sane and psychotic thought processes aredistinguished. A significant limitation of this analysis isthat we cannot now know towhat degree the beliefs of oursubjects were fostered and maintained within a cultural“microbubble,” and to what degree their beliefs wereamenable to being changed through reasonable processes.Last, in response to the proposal that a non-literal
interpretation of religious writings is most advisable, it isobserved that, since the earliest of times, believers haveunderstood our subjects’ experiences as having occurredliterally as described. As such, a great many of these ex-periences bear a striking resemblance towell-characterizedpsychiatric phenomena. This raises the prospect of anunusual degree of accuracy in the sources with regard tothese details.Discussion about a potential role for the supernatural
is outside the scope of our article and is reserved forthe communities of faithful, religious scholars, andtheologians, with one exception. It is our opinionthat a neuropsychiatric accounting of behavior need notbe viewed as excluding a role for the supernatural.Herein, neuropsychiatric mechanisms have been pro-posed through which behaviors and actions might beunderstood. For those who believe in omnipotent andomniscient supernatural forces, this should pose no ob-stacle, but might rather serve as a mechanistic explana-tion of how events may have happened. No disrespect isintended toward anyone’s beliefs or these venerablefigures.If such is perceived after reading this analysis it might
be asked whether there is a stigma in the reader’s mindabout mental illness. Any stigma toward persons withmental illness is rejected by the authors.
FUTURE DIRECTIONS
Research into this postulated form of psychiatric pre-sentation might be facilitated by development of a newDSM diagnostic subcategory of schizophrenia or psy-chosis and an improved recognition that a continuum ofpsychotic symptomatology likely exists.This subcategory might be referred to as a grandiose or
supraphrenic (supra [above or beyond] phrenic [mind])
J Neuropsychiatry Clin Neurosci 24:4, Fall 2012 http://neuro.psychiatryonline.org 423
MURRAY et al.

variant. It would encompass those who are symptomaticfor 6 months or more, with an organized and relativelynonbizarre delusional system, grandiosity, often delu-sional narcissism, possible hallucinations, and an ex-tremely intense feeling of being supernaturally selectedfor a mission. It would recognize that when this occurs inindividuals with generally average-or-higher intelligence,strong communication skills, a high degree of magneticcharisma, and the ability to effectively engender empathy,these individuals may be capable of convincing orpsychologically enthralling groups or populations ofindividuals to follow their directives for undefinedperiods of time. Their goals are partly or wholly basedon or inspired by psychotic thought processes. Thesethought processes may yield beliefs that are closelyrelated to other common societal beliefs, but they are notvery amenable to reason. Affected individuals may de-monstrate a preserved ability to maintain a social group,be very persuasive, and become socially elevated in agroup and exercise inordinate influence over others inthe group. Their beliefs may result in the sponsorship ofactivities that are lethal to self and others and are outsidethe norms for their society. Disorganization, negativepsychiatric symptoms, and cognitive dysfunction are notsignificantly present. Affective features may be present,but are not usually debilitating. Hyperreligiosity wouldbe a frequent accompaniment, but is not necessarilyrequired, since extreme devotion to other socio-politicalbelief systems or perceived extraterrestrial or supernat-ural forces might serve as surrogates. These individuals
are capable of having extraordinary influence onindividuals and society.
CONCLUSION
We suggest that some of civilization’s most significantreligious figures may have had psychotic symptoms thatcontributed inspiration for their revelations. It is hopedthat this analysis will engender scholarly dialogue aboutthe rational limits of human experience and serve toeducate the general public, persons living with mentalillness, and healthcare providers about the possibilitythat persons with primary and mood disorder-associatedpsychotic-spectrum disorders have had a monumentalinfluence on civilization.
Figure Credits: Figure 1: Wikipedia: http://en.wikipedia.org/wiki/File:Abraham.jpg; Figure 2: Wikipedia: http://yo.wikipedia.org/wiki/F%C3%A1%C3%ACl%C3%AC:Domenico_Fetti_004.jpg; Figure 3: Wikipedia: http://en.wikipedia.org/wiki/File:Rembrandt_Christ_in_the_Storm_on_the_Lake_of_Galilee.jpg; Figure 4: Wikipedia Commons: http://commons.wikimedia.org/wiki/File:4paul1.jpg.Written with financial support from the Sidney R. Baer, Jr.
Foundation, St Louis, MO.We thank Steven Schachter, M.D., Professor of Neurology,
Harvard Medical School; and Jeffrey Rediger, M.D., M.Div.,Assistant Professor of Psychiatry, Harvard Medical School;and The Center for Brain, Law, and Behavior at theMassachusetts General Hospital, Boston, MA.
References
1. Hazlett SB, McCarthy ML, Londner MS, et al: Epidemiologyof adult psychiatric visits to U.S. emergency departments.Acad Emerg Med 2004; 11:193–195
2. Baillargeon J, Thomas CR,Williams B, et al: Medical emergencydepartment utilization patterns among uninsured patientswith psychiatric disorders. Psychiatr Serv 2008; 59:808–811
3. Rudaleviciene P, Stompe T, Narbekovas A, et al: Are religiousdelusions related to religiosity in schizophrenia? Medicina(Kaunas) 2008; 44:529–535
4. Baier M: Insight in schizophrenia: a review. Curr PsychiatryRep 2010; 12:356–361
5. American Psychiatric Association: Diagnostic and StatisticalManual of Mental Disorders, 4th Edition, Text Revision. Wash-ington, DC, American Psychiatric Association, 2000, pp 297–343
6. Shannon B: Biblical entheogens: a speculative hypothesis.Time and Mind 2008; 1:51–74
7. Elliott B, Joyce E, Shorvon S: Delusions, illusions, and hal-lucinations in epilepsy, 2: complex phenomena and psychosis.Epilepsy Res 2009; 85:172–186
8. Nadkarni S, Arnedo V, Devinsky O: Psychosis in epilepsypatients. Epilepsia 2007; 48(Suppl 9):17–19
9. de Araújo Filho GM, da Silva JM, Mazetto L, et al: Psychoses ofepilepsy: a study comparing the clinical features of patients withfocal versus generalized epilepsies. Epilepsy Behav 2011; 20:655–658
10. Ogata A, Miyakawa T: Religious experiences in epilepticpatients with a focus on ictus-related episodes. PsychiatryClin Neurosci 1998; 52:321–325
11. Kanemoto K, Kawasaki J, Kawai I: Postictal psychoses: incomparison with acute interictal psychoses. Jpn J PsychiatryNeurol 1994; 48:209–211
12. Brewerton TD: Hyperreligiosity in psychotic disorders. J NervMent Dis 1994; 182:302–304
13. Landtblom AM, Lindehammar H, Karlsson H, et al: Insularcortex activation in a patient with “sensed presence”/ecstaticseizures. Epilepsy Behav 2011; 20:714–718
14. Picard F, Craig AD: Ecstatic epileptic seizures: a potentialwindow on the neural basis for human self-awareness. EpilepsyBehav 2009; 16:539–546
424 http://neuro.psychiatryonline.org J Neuropsychiatry Clin Neurosci 24:4, Fall 2012
PSYCHOTIC DISORDERS IN RELIGIOUS HISTORY
15. Asheim Hansen B, Brodtkorb E: Partial epilepsy with“ecstatic” seizures. Epilepsy Behav 2003; 4:667–673
16. Naito H, Matsui N: Temporal lobe epilepsy with ictal ecstaticstate and interictal behavior of hypergraphia. J Nerv Ment Dis1988; 176:123–124
17. Cirignotta F, Todesco CV, Lugaresi E: Temporal lobe epilepsywith ecstatic seizures (so-called Dostoevsky epilepsy). Epi-lepsia 1980; 21:705–710
18. Prendergast J, Spira P, Schnieden V: Post-ictal psychosis: anunusual clinical entity. Aust N Z J Psychiatry 1999; 33:433–435
19. Dongier S: Statistical study of clinical and electroencephalo-graphic manifestations of 536 psychotic episodes occurring in516 epileptics between clinical seizures. Epilepsia 1959/1960;1:117–142
20. Kanemoto K: Postictal psychoses, in Progress in EpilepticDisorders: Neuropsychiatric Issues in Epilepsy. Montrouge,France. Edited by Inoue Y, Matsuura M. John Libbey Eurotext,2010, pp 27–34
21. Umbricht D, Degreef G, Barr WB, et al: Postictal and chronicpsychoses in patients with temporal lobe epilepsy. Am JPsychiatry 1995; 152:224–231
22. Kanner AM, Stagno S, Kotagal P, et al: Postictal psychiatricevents during prolonged video-electroencephalographic mon-itoring studies. Arch Neurol 1996; 53:258–263
23. TrimbleM, Kanner A, Schmitz B: Postictal psychosis. EpilepsyBehav 2010; 19:159–161
24. Kanemoto K: Postictal psychoses, revisited, in The Neuro-psychiatry of Epilepsy. Edited by Trimble MR, Schmitz B.Cambridge, U.K., New York, Cambridge Univ. Press, 2002,pp 117–131
25. Devinsky O: Epilepsy: Patient and Family Guide, 3rd Edition.Demos Health, 2007, pp 20
26. Holmes GL: Epilepsy.com. Temporal Lobe Epilepsy. http://www.epilepsy.com/epilepsy/epilepsy_temporallobe; last accessed 05/28/2011)
27. Professional Advisory Board: EpilepsyFoundation.org. TemporalLobe Epilepsy. http://www.epilepsyfoundation.org/about/types/syn-dromes/temporallobe.cfm; last accessed June 4, 2011)
28. Dolgoff-Kaspar R, Ettinger AB, Golub SA, et al: Numinous-like auras and spirituality in persons with partial sei-zures. Epilepsia 2011; 52:640–644 10.1111/j.1528- PubMed1167.2010.02957.x. Epub 2011 Feb 5.
29. Cavanna AE, Cavanna S, Cavanna A: Epileptic seizures andspirit possession in Haitian culture: report of four cases andreview of the literature. Epilepsy Behav 2010; 19:89–91
30. Bortz JJ: Neuropsychiatric and memory issues in epilepsy.Mayo Clin Proc 2003; 78:781–787
31. Patrikelis P, Angelakis E, Gatzonis S: Neurocognitive andbehavioral functioning in frontal lobe epilepsy: a review.Epilepsy Behav 2009; 14:19–26
32. Hoffmeier, James K: Israel in Egypt: The Evidence for theAuthenticity of the Exodus Tradition. Oxford UniversityPress, 1999
33. Schultze-Lutter F, Ruhrmann S, Hoyer C, et al: The initialprodrome of schizophrenia: different duration, differentunderlying deficits? Compr Psychiatry 2007; 48:479–488
34. Yung AR, McGorry PD: The prodromal phase of first-episodepsychosis: past and current conceptualizations. SchizophrBull 1996; 22:353–370
35. Flaherty AW: Frontotemporal and dopaminergic control ofidea-generation and creative drive. J Comp Neurol 2005;493:147–153
36. Flaherty A: The Midnight Disease: The Drive to Write,Writer’s Block, and the Creative Brain. New York, MarinerBooks, 2005, p 41
37. Trimble MR. The Soul in the Brain: The Cerebral Basis ofLanguage, Art, and Belief. Baltimore, MD, Johns Hopkins,2007, p 101–114
38. Nestor PG: Mental disorder and violence: personalitydimensions and clinical features. Am J Psychiatry 2002;159:1973–1978
39. Hor K, Taylor M: Suicide and schizophrenia: a systematicreview of rates and risk factors. J Psychopharmacol 2010;24(Suppl):81–90
40. Meltzer HY: Suicidality in schizophrenia: a review of theevidence for risk factors and treatment options. CurrPsychiatry Rep 2002; 4:279–283
41. Lord V: Suicide by Cop: Inducing Officers to Shoot. NewYork, Loose Leaf Law Publications, 2004
42. Keram E, Farrell B: Suicide by Cop: Issues in Outcome andAnalysis. Suicide and Law Enforcement, 2001, pp 587–599
43. Landsborough D: St Paul and temporal lobe epilepsy. JNeurol Neurosurg Psychiatry 1987; 50:659–664
44. Rieu CH: Introduction, notes, in The Acts of the Apostles.Translated by Rieu CH. New York, Penguin Classics, 1957,pp 9–39, 133–136, 170–171
45. Pfleiderer O: Lectures on the influence of the Apostle Paul onthe development of Christianity, delivered in London andOxford, April and May, 1885. Williams and Norgate, 1897,p 43
46. The New Oxford Annotated Bible with the Apocrypha:Revised Standard Version. Edited by May HG, Metzger BM.New York, Oxford University Press, 1977, pp 1408
47. The Reformation Study Bible New King James Version SproulRC. Nashville, TN, Thomas Nelson Publishers, 1995, p 1408
48. GeschwindN: Behavioural changes in temporal lobe epilepsy.Psychol Med 1979; 9:217–219
49. Geschwind N: Interictal behavioral changes in epilepsy.Epilepsia 1983; 24(Suppl 1):S23–S30
50. Waxman SG, GeschwindN: The interictal behavior syndrome oftemporal lobe epilepsy. Arch Gen Psychiatry 1975; 32:1580–1586
51. Benson DF: The Geschwind syndrome. Adv Neurol 1991;55:411–421
52. Schachter S: Religion and the Brain: Evidence from TemporalLobe Epilepsy, in Where God and Science Meet: How Brainand Evolutionary Studies Alter Our Understanding of Re-ligion, Vol 2. Edited by McNamara P. Westport, CT, Praeger,2006, pp 171–188
53. Devinsky O, Najjar S: Evidence against the existence ofa temporal lobe epilepsy personality syndrome. Neurology1999; 53(Suppl 2):S13–S25
54. Mungas D: Interictal behavior abnormality in temporal lobeepilepsy: a specific syndrome or nonspecific psychopathol-ogy? Arch Gen Psychiatry 1982; 39:108–111
55. Rodin E, Schmaltz S: The Bear-Fedio personality inventoryand temporal lobe epilepsy. Neurology 1984; 34:591–596
56. Stark-Adamec C, Adamec RE, Graham JM, et al: Complexitiesin the complex partial seizures personality controversy.Psychiatr J (Univ Ott) 1985; 10:231–236
J Neuropsychiatry Clin Neurosci 24:4, Fall 2012 http://neuro.psychiatryonline.org 425
MURRAY et al.
57. Stevens JR: Interictal clinical manifestations of complex partialseizures, in Advances in Neurology. Edited by Penry JK, DalyDD. New York, Raven, 1975, pp 85–107
58. Stern A: [The problem of St. Paul’s epilepsy]. Psychiatr Neurol(Basel) 1957; 133:276–284
59. Brorson JR, Brewer K: St Paul and temporal lobe epilepsy. JNeurol Neurosurg Psychiatry 1988; 51:886–887
60. Shimizu M, Kubota Y, Toichi M, et al: Folie à deux and sharedpsychotic disorder. Curr Psychiatry Rep 2007; 9:200–205
61. James W: The Varieties of Religious Experience. New York,Barnes & Noble Classics, 1902, 2004, pp 416–417
62. Karenberg A: Retrospective diagnosis: use and abuse inmedical historiography. Prague Med Rep 2009; 110:140–145
63. Price BH, Richardson EP Jr: The neurologic illness of EugeneO’Neill: a clinicopathological report. N Engl J Med 2000;342:1126–1133
64. Kahn CR, King GL, Moses AC, (eds): Joslin’s DiabetesMellitus, 14th Ed. Philadelphia, PA, Lippincott, Williams &Wilkins, 2005, p 2
65. Friedman RE. Who Wrote the Bible? HarperOne, January 1,1987, pp 15–33
66. Erhman BD. The New Testament: A Historical Introduction tothe Early Christian Writings, 5th Ed. New York, Oxford Univ.Press, 2011
67. Murray ED, Price BH: The neurological examination, inComprehensive Clinical Psychiatry, 1st Ed. Edited by SternTA, Rosenbaum JF, Fava M, et al. Philadelphia, PA, Mosby/Elsevier, 2008
68. Ovsiew F, Murray ED, Price BH: Neuropsychiatric approachto the psychiatric inpatient, in Principles of Inpatient Psy-chiatry, 1st Edition. Edited by Ovsiew F, Munich R. Baltimore,MD, Lippincott Williams & Wilkins, 2008
69. Legesse B, Price BH, Murray ED: Brain–behavior relations, inEncyclopedia of Human Behavior, 2nd Edition. Edited byRamachandran VS. New York, Academic Press, 2012
70. Murray ED, Buttner N, Price BH: Depression and psychosis inneurological practice, in Neurology in Clinical Practice, 6thEd. Edited by Bradley WG, Daroff RB, Fenichel GM, et al.London, UK, Butterworth Heinemann, 2012
71. Zubin J, Spring B: Vulnerability: a new view of schizophrenia.J Abnorm Psychol 1977; 86:103–126
72. Russo J, Vitaliano PP, Brewer DD, et al: Psychiatric dis-orders in spouse caregivers of care recipients with Alz-heimer’s disease and matched controls: a diathesis-stressmodel of psychopathology. J Abnorm Psychol 1995; 104:197–204
73. Portin P, Alanen YO: A critical review of genetic studies ofschizophrenia, II: molecular genetic studies. Acta PsychiatrScand 1997; 95:73–80
74. U.S. Department of Health and Human Services (USDHHS):Mental Health: Culture, Race, and Ethnicity, A Supplementto Mental Health: A Report of the Surgeon General. Rock-ville, MD, U.S. Department of Health and Human Services,Public Health Service, Office of the Surgeon General, 2001,p 26
75. U.S. Department of Health and Human Services (USDHHS):Mental Health: A Report of the Surgeon General. Rockville,MD, U.S. Department of Health and Human Services, PublicHealth Service, Office of the Surgeon General, 1999, pp269–284
76. van Os J, Kapur S: Schizophrenia. Lancet 2009; 374:635–64577. Smith MS: The Origins of Biblical Monotheism: Israel’s
Polytheistic Background and the Ugaritic Texts. New York,Oxford Univ. Press, 2001, pp 135–157
78. Rediger J: Bipolar disorder and western anosognosia, in ThePsychospiritual Clinician’s Handbook: Alternative Methodsfor Understanding and Treating Mental Disorders. Edited byMijares S, Khalsa G. Binghamton, NY, Haworth ReferencePress, 2005, pp 205–231
79. Mohr S, Huguelet P: The relationship between schizophreniaand religion and its implications for care. Swiss Med Wkly2004; 134:369–376
80. Kim K, Hwu H, Zhang LD, et al: Schizophrenic delusions inSeoul, Shanghai, and Taipei: a transcultural study. J KoreanMed Sci 2001; 16:88–94
81. Vardy MM, Kaplan BM: Christ/messiah delusions revisited:toward an anthropological definition of religious delusions.Psychoanal Rev 2008; 95:473–487
82. Reavis DJ: The Ashes of Waco: An Investigation. SyracuseUniv Press, 1998
83. Snow RL: Deadly Cults: The Crimes of True Believers.Westport, CT, Praeger, 2003
84. TheMI5Messiah:Why David Shayler Believes He’s the Son ofGod; Mail Online. London, UK, Dailymail.co.uk; 2007
85. The Argus, Visit from the “Siberian Jesus” November 9, 200286. Akimoto H: The Aum Cult leader Asahara’s mental
deviation and its social relations. Psychiatry Clin Neurosci2006; 60:3–8
87. Kalchuri B: Meher Prabhu: Lord Meher, The Biography of theAvatar of the Age, Meher Baba Manifestation, Inc., 1986
88. Hardy R: Confusion surrounds Najaf battle. BBC News,January 31, 2007
89. Pechey R, Halligan P: The prevalence of delusion-like beliefsrelative to sociocultural beliefs in the general population.Psychopathology 2011; 44:106–115
90. Strauss JS: Hallucinations and delusions as points on continuafunction: rating scale evidence. Arch Gen Psychiatry 1969;21:581–586
91. Ellett L, Lopes B, Chadwick P: Paranoia in a nonclinicalpopulation of college students. J NervMentDis 2003; 191:425–430
92. Kelleher I, Cannon M: Psychotic-like experiences in thegeneral population: characterizing a high-risk group forpsychosis. Psychol Med 2011; 41:1–6
93. Wilner AR: The Spellbinders: Charismatic Political Leader-ship. New Haven, CT, Yale University Press, 1984
94. Bion WR: Experiences in Groups and Other Papers. London,UK, Tavistock, 1961
95. Post JM: Leaders and Their Followers in a Dangerous World:The Psychology of Political Behavior. Ithaca, NY, CornellUniversity Press, 2004, pp 187–199
96. GhaemiN: A First-RateMadness: Uncovering the Links BetweenLeadership and Mental Illness. New York, Penguin, 2011
97. Cameron N: The paranoid pseudocommunity. Am J Sociol1943; 49:37–38
98. Cameron N: Paranoid conditions and paranoia: AmericanHandbook of Psychiatry, Vol I. New York, Basic Books, 1959a
99. Cameron N: The paranoid pseudocommunity revisited. Am JSociol 1959b; 65:57–61
100. Myers PL: Paranoid pseudocommunity beliefs in a sectmilieu. Soc Psychiatry Psychiatr Epidemiol 1988; 23:252–255
426 http://neuro.psychiatryonline.org J Neuropsychiatry Clin Neurosci 24:4, Fall 2012
PSYCHOTIC DISORDERS IN RELIGIOUS HISTORY




![Introduction - Freebenjamin.lisan.free.fr/EcritsPolitiquesetPhilosophiques/... · 2018. 5. 26. · Shaitan [Satan] a déclaré : "Je me demande comment les humains prétendent aimer](https://img.pdfslide.us/doc/110x75/611e2e930df5987da71ab549/introduction-2018-5-26-shaitan-satan-a-dclar-je-me-demande.jpg)