Embed Size (px)
Citation preview

The Role of OT in
Hospice and Palliative Care
Janice Kishi Chow, MA, OTR/LPalo Alto VA Hospice and Palliative Care Center
April 23, 2013

Objectives
•What is hospice and palliative care?
•What role does OT play?
Hospice
•Non-curative comfort care
•Psychosocial support
•Life expectancy is less than 6 months
•Affirms life
•Accepts death as a normal process
•Neither hastens or postpones death

Palliative care•“Palliare” : to cloak
• Non-curative, comfort care
• Arose from modern hospice care
• Symptom management for those not terminally ill
• Provided at an stage of an illness or disease
• In conjunction with curative treatments
• Segues into hospice care

Impact of Hospice and Palliative
Care• Misconception that hospice and palliative care hastens death
• Journal of Pain and Symptom Management, March 2007
• Hospice patients lived mean average of 29 days longer
• CHF: +181 days
• New England Journal of Medicine, August 2010
• Early palliative care of Lung CA: 2.7 months longer
Possible Factors thatContribute to Survival
• Weakened patients avoid risks of over-treatment
• Hospice care can improve monitoring and treatment
• Psychosocial support may lessen burden of care, increase desire to live, and prolong life
• Early management of symptoms may stabilize disease
• Stability may prolong life

Role of OT in Hospice and Palliative
Care
•Maximize occupational engagement
•Decline is dynamic
•Modification and adaptation
•Support the grieving process
Tom*
•47 year old male veteran
•Metastatic rectal cancer (dx’d 4 mo. prior)
•Chemo, XRT
•Stage 4 coccyx ulcer
•Severe hip, back and ulcer pain
•BLE strength grossly 2-/5
*Name changed

Tom’s goals
•Pain relief
•Full recovery
•Improve strength
•Transfer into a wheelchair
•Go outside with his family
•Walk
Themes
•Decreased insight vs. Faith
•Poor endurance vs. Denial
•Poor rehab potential vs. “Rehab moments”

Treatment•Edge of bed activities
•Pre-functional AAROM
•Retrograde massage
•Theraputty exercises
•Psychosocial support

Wheelchair Fitting
•Tilt-in-Space Recliner w/c
•Cushion with gel insert
•22” hand rims
•Front brakes
•Family education

Maximizing Function
•Dynamic sitting balance activities
•Cooking activity
•ADL retraining
Ham and Cheese Crescent roll

Cancer Dying Trajectory
12 11 10 9 8 7 6 5 4 3 2 1 0
Months Before Death
Health Status
Hallenbeck, J. L. Palliative Care Perspectives. 2003, Oxford University Press.

Cancer Dying Trajectory
12 11 10 9 8 7 6 5 4 3 2 1 0
Months Before Death
Health Status
Hallenbeck, J. L. Palliative Care Perspectives. 2003, Oxford University Press.
Functional Plateau
Sudden decline(probable pulmonary embolism or sepsis)
Chuck*
•75 year old male veteran
•Palliative care admission
•H/o CHF and COPD
•Retired truck driver
•Married with children and grandchildren
•Recurrent short stays over 2 years
* Name changed

•Symptom management (SOB, fatigue)
•Maximize function
•Maximize time with family
Chuck’s goals

Treatment
•Energy conservation
•Adaptive equipment
•Power mobility
•Psychosocial support
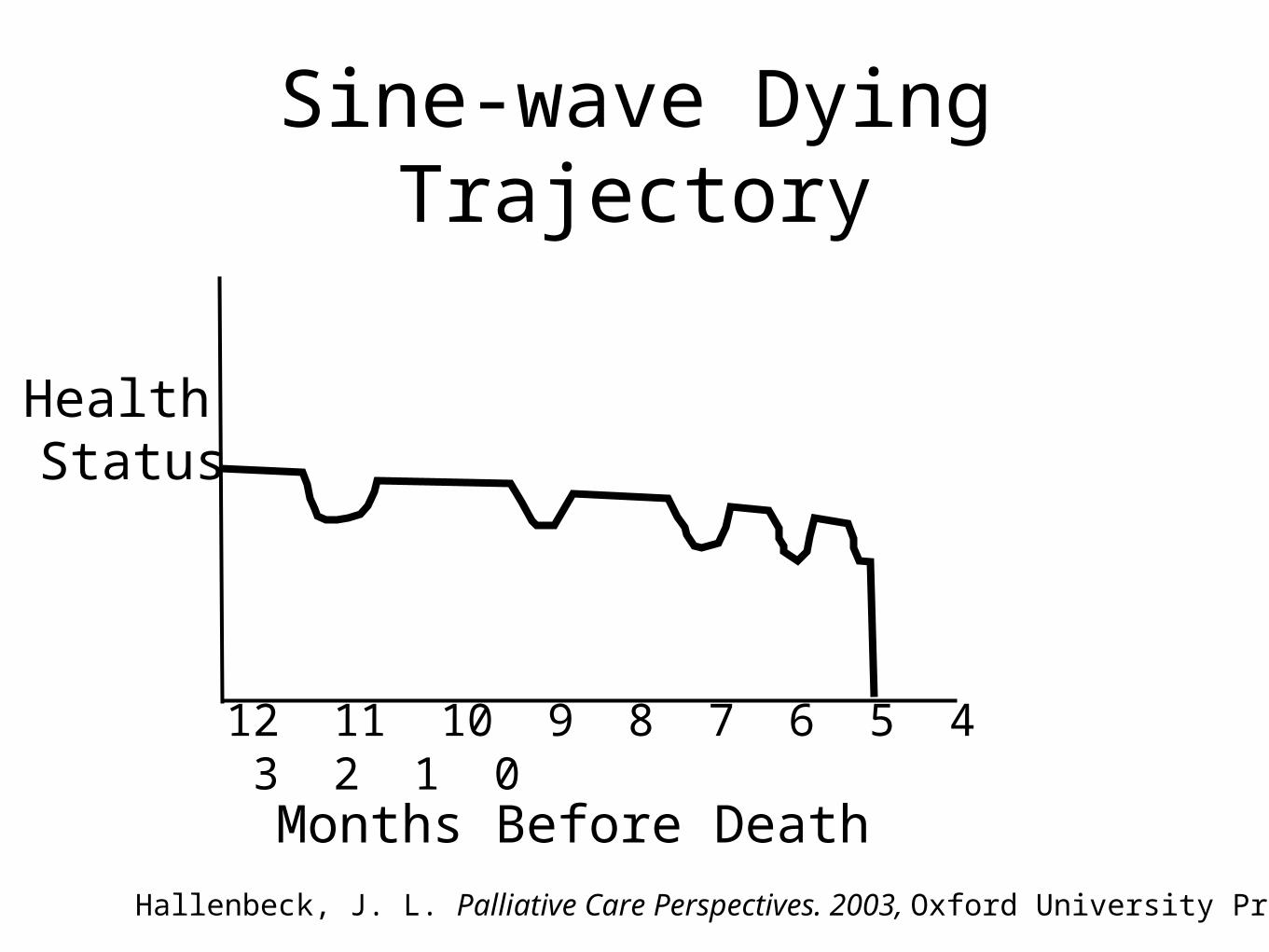
Sine-wave Dying Trajectory
12 11 10 9 8 7 6 5 4 3 2 1 0
Months Before Death
Health Status
Hallenbeck, J. L. Palliative Care Perspectives. 2003, Oxford University Press.
Conclusion
•Hospice and Palliative Care
•Non-curative comfort care and psychosocial support
•Alleviates pain and suffering
•Improves quality of life

Conclusion
•Role of OT
•Maximizes occupational engagement
•Support grieving clients

Practical Application
•Palliative Care Consult
•Symptom management
•Facilitate discharge planning
•Medical and psychosocial support
•End of life discussions

References
• Addington-Hall, J. M. & Higginson, I. J. (2001). Introduction. In Addington-Hall, J. M. & Higginson, I. J. (Eds.), Palliative Care for Non-cancer Patients. New York: Oxford University Press.
• Connor SR, Pyenson B, Fitch K, Spence C, Iwasaki K. (2007). Comparing hospice and nonhospice patient survival among patients who die within a three- year window . Journal of Pain Symptom Management. 33(3):238-46.
• Hallenbeck, J. L. Palliative Care Perspectives. 2003, Oxford University Press.
• Ternel, J.S., Greer, J.A., Muzinkansky A., Gallagher, R.N., Admane, S., Jackson, V. A., Dahlin,, C. M., Blinderman, C. D., Jacobsen, J., Pirl, W. F., Billings, J. A., & Lynch, T. J. (2010). Early palliative care for patients with metastatic non-small-cell lung cancer. New England Journal of Medicine. 363(8):733-42.
• World Health Organization (WHO). Cancer: palliative care. Retrieved April 16, 2013 from http://www.who.int/cancer/palliative/en/