Embed Size (px)
Citation preview

Journal of Surgical Oncology 2009;99:189–193
REVIEW
The Role of Lymphadenectomy in Esophageal Cancer
GAIL DARLING, MD, FACS, FRCSC*University of Toronto, Toronto, Ontario, Canada
Lymph node metastases are common in esophageal cancer and are associated with a poor prognosis. Resection and examination of 15–18 lymph
nodes is required for adequate staging of esophageal cancer. Improved survival is associated with involvement of five or fewer nodes or lymph
node ratio (LNR) of < 0.10–0.20. More extensive lymph node dissection during esophagectomy offers improved staging but may also provide
therapeutic benefit in terms of control of locoregional disease and possibly improved overall survival.
J. Surg. Oncol. 2009;99:189–193. � 2008 Wiley-Liss, Inc.
KEY WORDS: esophageal cancer; lymph nodes; staging; survival
INTRODUCTION
The incidence of esophageal cancer is increasing making
esophageal cancer the 8th leading cause of cancer deaths in North
America. Historically, the survival of patients with resected esophageal
cancer was dismal, especially if there were associated lymph node
metastases. Because of this, many surgeons believed that more radical
surgery with extensive lymph node dissection added little to survival
but increased morbidity and mortality. However, operative mortality
for esophagectomy has decreased considerably from 29% in the
1960s–1980s [1] to less than 5% in high volume centers in the current
era [2]. With reduced operative mortality, improving long-term
survival has become more important. In an effort to achieve improved
long-term survival some surgeons have applied the principles of cancer
surgery to esophagectomy including en-bloc resection and formal
lymphadenectomy. However, the role of en-bloc resection and the
extent of lymph node dissection required during esophagectomy
remain controversial.
The fact that lymph node metastases are an important factor in
staging of esophageal cancer is well accepted but there is increasing
evidence that the number of metastatic nodes, the ratio of involved
nodes to total nodes sampled (lymph node ratio (LNR)) and even the
total number of nodes resected are of prognostic significance. There is
also accumulating evidence in terms of the number of nodes required
for optimal staging and this has implications in terms of the operative
approach to esophagectomy.
Lymphadenectomy offers the opportunity for improved staging
accuracy, and likely improves locoregional control but whether it
yields improved survival is more controversial. If nodal disease is
limited, a more extensive lymphadenectomy potentially increases the
chance of an R0 resection and thereby may improve survival; however
survival advantage seems less likely if there is extensive nodal
involvement.
Reports from recent surgical series of more extensive lymph
node dissection report higher survival than older series of limited
lymphadenectomy [2–4]. However whether these reports of
improved survival are due to better control of disease, improved
perioperative care, reflects better outcomes from high volume
centers with high volume surgeons or simply stage migration, is
not clear.
PREVALENCE OF LYMPH NODEMETASTASES IN ESOPHAGEAL CANCER
Lymph node involvement is common in esophageal cancer and
occurs even with early cancers, likely related to the anatomy of the
esophagus wherein the lymphatics run in the submucosa. Lymph
node metastases have been found in up to 35% of T1b tumors and in
78–85% of T3 tumors [3,4] (see Table I).
Lymph node involvement may occur in the abdominal, thoracic, or
cervical nodes regardless of whether the primary tumor is located at the
gastroesophageal junction, distal, mid, or upper esophagus. Metastatic
nodes in the cervical lymph nodes have been found in 17% of
gastroesophageal junction tumors and 23% of distal third tumors [3].
Distant lymph node metastases (abdominal nodes for upper third
cancers and cervical nodes for lower third cancers) may occur in up to
37–40% of patients [4,5].
As tumor depth increases the extent of lymph node involvement
increases both in terms of number of nodes involved as well as the
involvement of distant nodes (see Table II). Patients who are
symptomatic with dysphagia most commonly have T2 or T3 tumors.
Lymph node metastases are found in 85% of T3 tumors and 45% had
more than four nodes involved including 40% with distant lymph node
involvement of which 27% were celiac nodes. Celiac node involve-
ment was found in 23% of T2 tumors [4].
LYMPHADENECTOMY INESOPHAGEAL CANCER
It is controversial whether lymphadenectomy is of therapeutic value
or whether increased lymph node harvest simply allows better staging.
*Correspondence to: Dr. Gail Darling, MD, FACS, FRCSC, AssociateProfessor and Program Director Thoracic Surgery, University of Toronto,Toronto General Hospital 9N-955, 200 Elizabeth St, Toronto, ON, CanadaM5G 2C4. Fax: 416-340-3660. E-mail: [email protected]
Received 9 October 2008; Accepted 17 October 2008
DOI 10.1002/jso.21209
Published online 19 December 2008 in Wiley InterScience(www.interscience.wiley.com).
� 2008 Wiley-Liss, Inc.

Controversy also exists as to the extent of lymph node dissection
required.
EXTENT OF LYMPHADENECTOMY ANDACCURACY OF STAGING
As might be expected, more lymph nodes are harvested with more
extensive surgery. Junginger [6] reported a median of 16 (0–67) nodes
resected via a transhiatal resection versus 28 (0–84) for a transthoracic
procedure (P¼ 0.000). With increase in the number of lymph nodes
harvested the number of nodes found to have metastases also increased.
In a study of 2,597 patients from the SEER database, patients classified
as N0 had fewer lymph nodes identified than those classified as N1 [7].
Other investigators have reported a strong correlation between the
number of lymph nodes examined and number involved [8]. For
example, patients who were N0 had a mean lymph node count of
14.2� 7.1 whereas the lymph node count was 18.0� 9.3 in patients
found to have lymph node metastases [9]. Barbour [10] reported on
366 patients of whom 68% had examination of at least 15 nodes. These
patients were more likely to have positive lymph node metastases
compared to patients who had less than 15 nodes examined (P< 0.01).
Comparing transthoracic with transhiatal esophagectomy, the ratio
of N0: N1 in transthoracic resections was 39.2%: 60.8%, whereas for
transhiatal resections the ratio was 56.1%: 43.9% [11]. Similarly, Kang
[12] also found increased lymph node involvement with increased
number of nodes dissected. Nodal metastases were found in 53% of
patients having a three-field dissection with a median of 33 nodes
resected, whereas nodal metastases were found in 33% of patients
having a one-field dissection with a median of 17 nodes resected.
NUMBER OF LYMPH NODES REQUIREDFOR ACCURATE STAGING
A consensus conference of experts meeting in 1995 suggested that
accurate pathological staging of esophageal cancer required resection
of at least 15 nodes [13].
Although a minimum number of more than 12 nodes examined
provided >90% staging sensitivity, data from others suggest that
the minimum number required is at least 15 [14]. Bollschweiler [8]
reported that survival for N0 patients was significantly less if 15 or
fewer lymph nodes were examined. This suggests that, examination
of less than 15 nodes understages the patient and supports the
recommendation that a minimum of 15 nodes must be examined for
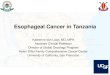
accurate staging. In Junginger’s study, the median survival for the
patients having a transthoracic versus transhiatal resection was
24 months versus 13 months (P¼ 0.004) and 5-year survival was
33% versus 12%. However this survival benefit was limited to only
those who were N0. Further, patients who had a transthoracic resection
but <16 nodes resected had a similar prognosis to those having a
transhiatal resection suggesting that these patients were understaged
[6] (see Fig. 1).
Barbour’s finding that patients with less than 15 nodes examined are
less likely to have nodal metastases identified also supports the concept
that a minimum of 15 nodes must be examined for accurate staging
[10] van Sandick [15] also recommended 15 nodes as the minimum
number required for accurate staging in that with less than 15 nodes
examined, N0 versus N1 was the deciding factor in prognosis but with
greater than 15 nodes examined, LNR became the most important
prognostic factor.
Rizk [16], however, identified 18 lymph nodes as the minimum
number of nodes required for optimal staging. When 18 or more lymph
nodes are removed, depth of invasion (T-status) was no longer
prognostic for survival.
INFLUENCE OF NUMBER OF LYMPH NODESEXAMINED AND SURVIVAL
Utilizing the Surveillance, Epidemiology and End-Results (SEER)
database, Schwartz and Smith [7] examined a cohort of 2,597 patients
who had resection for whom complete data was available and found
that total lymph node count or negative lymph node count are
independent predictors of survival in multivariate analysis. Lymph
node counts >30 were associated with the best overall survival, but this
finding was most significant for N0 patients although still a factor
for N1 patients. In multivariate analysis, negative lymph node count
>15 and total lymph node count >30, were interchangeable.
Patients with 30þ lymph nodes examined had a 5-year overall
survival of 41% versus 25% for 2–4 nodes examined (P< 0.05). Even
in patients with N1 disease this benefit persisted with 5 year
overall survival of 19% for those with 30þ resected nodes versus
9% for 2–4 nodes. The effect of lymph node count on survival applied
equally to both squamous and adenocarcinoma. The authors projected
an increase in overall survival at 5 years of 4–5% for every 10 lymph
nodes identified [7].
Bollschweiler also reported a correlation between number of nodes
examined and prognosis. For patients without lymph node metastases,
prognosis was better if they had more than 15 nodes examined
compared to those with <15 nodes examined, (HR¼ 0.3 95% CI: 0.1–
0.6, P< 0.01). Once lymph node metastases were identified this
finding was no longer applicable [8].
Various investigators have reported the optimum number of
resected nodes and have attempted to identify a ‘‘cut point’’ above
which there is no further improvement in survival. However in the
population-based study reported by Schwarz and Smith, no cut point
could be identified. They reported continually improving survival in all
categories from 2–4 nodes up to 30þ nodes. This finding applied
equally to patients with negative nodes as well as those with positive
nodes [7].
Journal of Surgical Oncology
TABLE I. Prevalence of Nodal Disease in Relation to T Stage[3]
T-status Positive nodes (%)
pT1s 0/1 (0.0)
pT1a 0/1 (0.0)
pT1b 8/23 (34.8)
pT2 17/24 (70.8)
pT3 96/123 (78.0)
pT4 1/2 (50.0)
All 122/174 (70.1)
TABLE II. Relationship Between Tumor Depth and Lymph Node Status[4]
T-stage
Prevalence of
positive nodes (%)
Median number of
positive nodes 1–4 nodes positive (%) >4 nodes positive (%)
Prevalence of positive
distant nodes (%)
T1a 1/16 (6) 2 1/16 (6) 0/16 (0) 0/16 (0)
T1b 5/16 (31) 1 4/16 (25) 1/16 (6) 1/16 (6)
T2 10/13 (77) 2 9/13 (69) 1/13 (8) 4/13 (31)
T3 47/55 (85) 5 22/55 (40) 25/55 (45) 22/55 (40)
190 Darling

NUMBER OF METASTATIC LYMPH NODES
The number of lymph nodes involved by metastatic disease also
influences survival and reflects burden of disease. With fewer
metastatic nodes, survival is better than if many nodes are involved.
Various investigators have identified <3 nodes [17,18], <4 nodes
[19,20], <5 nodes [8,21,22], or <7 involved nodes as predictive of
survival [23]. However in a series where 40þ lymph nodes were
resected in all patients, there was no adverse effect on prognosis with
increased lymph nodes involvement suggesting a therapeutic benefit to
lymphadenectomy [5].
Rizk [16] used recursive repartitioning and identified that the
presence of involved nodes as the most important predictor of survival
using the current AJCC staging system but adding the number of
involved nodes as a separate variable demonstrated that >4 metastatic
lymph nodes was single most important predictor of survival
irrespective of T-stage.
LYMPH NODE RATIO (LNR)
The ratio of metastatic to total lymph nodes (the LNR) has been
shown to be a prognostic factor in esophageal cancer but the value of
LNR that is most predictive of survival is debated (see Table III).
It appears from the data that the more lymph nodes examined, the
lower the value of LNR, which is prognostic. However if insufficient
nodes are examined the LNR ceases to be useful as a prognostic tool.
LNR was identified as the strongest predictor of survival (P< 0.0001)
if 15 or more nodes were resected, with LNR >0.3 having the
poorest survival (HR 5.6 95% CI: 3.0–11.4) whereas for patients with
<15 nodes resected the presence or absence of lymph node metastases
was predictive of survival but not the LNR [16].
RELATIONSHIP BETWEEN LYMPH NODECOUNT AND PROGNOSIS
In patients with N1 disease who have a transthoracic R0 resection,
dissection of 16 or more lymph nodes offers a survival advantage over
those who have <16 nodes (Fig. 1). Also, in a multivariate analysis
total number of lymph nodes resected was a significant independent
predictor of survival (P¼ 0.019) [6]. Rizk identified that survival was
improved in patients with T2–3 tumors with 0–4 involved
lymph nodes if more than 18 lymph nodes were removed and
suggested that the improved survival was related to improved staging
and stage migration with more extensive lymph node dissection. The
likelihood of finding positive nodes was higher and the number of
positive nodes was higher with an adequate (>18 nodes) lymph node
resection [16].
RELATIONSHIP BETWEEN EXTENT OFSURGICAL RESECTION AND PROGNOSIS
A number of studies report improved survival with more extensive
surgery [2–4].
In Japan, three-field lymphadenectomy has been standard practice
since the 1980s. Nishimaki [24] reported 5 year survival of 68% after
three-field lymphadenectomy and Akiyama reported 5 year survival of
54% compared to 34% for three versus two-field lymphadenectomy in
node negative patients [25]. Similarly a randomized trial of cervical
and upper mediastinal lymph node dissection for squamous cell
carcinoma of the thoracic esophagus reported overall survival of 66%
at 5 years for the extended dissection with harvest of a mean of
82 nodes versus 48% for standard dissection with a harvest of 43 nodes
[26].
In a study examining the effect of one-, two-, or three-field
lymphadenectomy increased survival was reported with increasing
extent of lymph nodes resection. Overall survival at 5 years was 21.2%
versus 36.3% versus 53.7% for patients resected with a one-, two-, or
three-field lymphadenectomy (P¼ 0.019). However the benefit of
more extensive lymphadenectomy was predominantly in the N0 group
[12]. This suggests that the benefit is predominantly related to stage
migration.
These series all document high lymph node counts with more
extensive surgery.
In the only randomized trial of transthoracic esophagectomy versus
transhiatal esophagectomy in which the lymph node count for the
former was 31 and 16 for the latter, improved survival was reported
with 5 year overall survival of 39% versus 29% but this did not reach
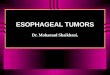
statistical significance [27]. However, in a larger population based
study of 402 patients from Finland, there was a survival benefit with
two-field lymphadenectomy with a 5 year survival of 50.0% for
patients who had a two-field lymphadenectomy versus 23.2% for those
who had less extensive operations (P¼ 0.005) [28] (see Fig. 2).
Although Junginger [6] reported improved survival after transthor-
acic resection compared to transhiatal esophagectomy, the survival
benefit was statistically significant only for patients who had an
R0 resection, or were N0 or if N1 with 16 or more nodes resected
Journal of Surgical Oncology
Fig. 1. Kaplan–Meier curves for patients with pN1 squamous cellcarcinoma of the esophagus undergoing R0 resection by transhiatal(TH) versus transthoracic (TT) (�16 vs. <16 dissected thoracic lymphnodes) [6]. Reproduced with permission.
TABLE III. Lymph Node Ratio as a Predictor of Survival
LNR Author
Nodes
examined
>0.10 Hagen [4] 48 P< 0.001
>0.10 Eloubeidi [20] HR 1.63 (95%CI: 1.25–2.11
P¼ 0.0013)
>0.105 Tachibana [5] 40þ HR¼ 3.366 (95% CI: 1.092–10.37)
P¼ 0.0345
0.01–01.9 Schwarz [7] 8 P< 0.0001
>0.20 Roder [22] 34 P< 0.001
>0.20 Bollschweiler [8] 28 P< 0.01
>0.20 Wijnhoven [17] 11 HR 2.39 (95% CI: 1.51–3.76)
P< 0.001
>0.20 Greenstein [23] 11 P< 0.001
>0.30 van Sandick [15] 12 HR 5.6 (95% CI: 3.0–11.4)
(P< 0.0001)
Role of Lymphadenectomy in Esophageal Cancer 191

(see Table IV). Others have reported a survival benefit with more
extensive lymph node dissection for N0 patients (P¼ 0.0379) but not
for the overall group of patients (median disease specific survival for
transthoracic vs. transhiatal resections; 31.4months vs. 16.7 months)
[11].
In a case control study of patients with locally advanced esophageal
cancer (T3 N1), overall survival was 32% with en-bloc esophagectomy
(52 nodes) versus 9% with transhiatal esophagectomy. Inclusion
criteria for this study mandated that 20 or more lymph nodes must be
resected. Although the number of nodes resected with the en-bloc
procedure (median 52 nodes, range 21–85) was significantly higher
than for the transhiatal procedure (median 29 nodes, range 20–60)
(P¼ 0.03), the number of involved nodes was similar (median 5 vs. 7),
suggesting that more extensive surgery confers a survival advantage
not just related to stage migration. However, this benefit disappeared if
>9 nodes were involved. This suggests that with increasing numbers of
lymph node metastases the likelihood of distant metastatic disease is
increased and hence more radical surgery is unlikely to provide any
survival advantage [29].
SITE OF LYMPH NODE METASTASES
Although the current staging system classifies certain lymph node
groups as M1 disease, several investigators have found that involve-
ment of these nodal groups does not have a different prognosis from
other sites of lymph node involvement and furthermore does not have
the same prognostic implications as distant organ involvement. In the
report by Rizk et al., [16] there is no survival difference between M1a
or b lymph node groups and survival for these patients was similar to
patients with >4 positive lymph nodes irrespective of their AJCC
stage. This suggests that the M1a/b designation adds little to the
staging system and specifically should not be used to exclude patients
from therapeutic options. Others also report no difference between
M1a and b lymph node metastases in terms of survival and these
patients have similar survival to stage III patients and specifically have
better survival than patients with M1 disease in non-lymph node sites
[5,17,19,20,21,27]. Hagen [4] reported no difference in 5-year survival
between M1a or b nodes (33%) and regional node metastases (37%)
(P¼ 0.214). Survival at 5 years was 37% for celiac node negative
patients versus 29% for celiac node positive patients (P¼ 0.63).
CORRELATION OF LYMPH NODEINVOLVEMENT WITH RISK OF DISTANT
METASTATIC DISEASE
Increasing lymph node involvement is predictive of distant
metastatic disease. Distant metastatic disease was found 92% of
patients with more than 10 involved lymph nodes, as compared to 45%
of patients with only 1–4 nodes involved and 0% with no nodal
involvement [20]. LNR also predicts distant metastatic disease. In
patients with a LNR of >0.10 metastatic disease was found in 84%
versus 43% with a LNR 0.01–0.10 and 0% if LNR was zero
(P< 0.001) [4].
From several studies it is clear that with increasing number of
metastatic lymph nodes, there is an increasing risk of systemic disease
such that more extensive lymph node dissection offers no further
survival advantage over more limited dissection.
EXTENT OF LYMPHADENECTOMY ANDLOCOREGIONAL RECURRENCE
Locoregional recurrence is high after transhiatal esophagectomy
occurring most often in the mediastinum (40–52%) whereas
locoregional recurrence is reduced to 5–8% after en-bloc resection.
This is clearly related to the ability to perform a complete
lymphadenectomy. Control of locoregional disease is important from
a quality of life perspective but may also impact on overall survival
[3,30].
SUMMARY
More extensive lymph node dissection clearly provides more
accurate staging of nodal disease. All studies reported increased
proportion of N1 patients with more extensive nodal dissection. It is
also clear that more extensive node dissection reduces locoregional
recurrence. Whether more extensive dissection improves survival is
unclear, however from the available data, it appears that if lymph
node involvement is limited to <3–5 perhaps even up to 7 nodes,
long term survival may be improved by more radical lymph
node dissection. However, with greater number of nodes involved,
there is a higher probability of systemic disease and more extensive
lymph node dissection appears to add little in terms of survival benefit
although it still confers advantage in terms of local control and
prognostication.
REFERENCES
1. Earlam R, Cunha-Melo JR: Oesophageal squamous cell carci-noma: A critical review of surgery. Br J Surg 1980;67:381–390.
Journal of Surgical Oncology
TABLE IV. Prognosis in Patients With Squamous Cell Carcinoma After
Transthoracic (TTE) Versus Transhiatal Esophagectomy (THE)[6]
Surgical
procedure
Median survival
(months)
5-year
survival (%) P-value
R0N0
TTE 38 41 0.023
THE 14 17
R0N1
TTE 12 26
TTE< 16
nodes
10 18
TTE� 16 25 32 0.034 (vs. THE)
THE 12 0
Fig. 2. Five-year survival of patients with resection of adenocarci-noma of the esophagus with either two-field lymphadenectomy (-) orless extensive lymphadenectomy (- - -). Reproduced with permission.
192 Darling

2. Altorki NK, Girardi L, Skinner DB: En Bloc esophagectomyimproves survival for stage III esophageal cancer. J ThoracCardiovasc Surgy 1997;114:948–956.
3. Lerut T, Nafteux P, Moons J, et al.: Three-field lymphadenectomyfor carcinoma of the esophagus and gasroesophageal junction in174 R0 resections: Impact on staging, disease-free survival andoutcome. Ann Surg 2004;240:962–974.
4. Hagen JA, DeMeester SR, Peters JH, et al.: Curative resection foresophageal adenocarcinoma: Analysis of 100 enbloc esoph-agectomies. Ann Surg 2001;234:520–531.
5. Tachibana M, Dhar DK, Kinugasa S, et al.: Esophageal cancerwith distant lymph node metastasis. J Clin Gastroenterol 2000;31:318–322.
6. Junginger T, Gockel I, Heckhoff S: A comparison of transhiataland transthoracic resections on the prognosis in patients withsquamous cell carcinoma of the esophagus. Eur J Surg Oncol2006;32:749–755.
7. Schwarz RE, Smith DD: Clinical Impact of lymphadenectomyextent in resectable esophageal cancer. J Gastrointest Surg 2007;11:1384–1394.
8. Bollschweiler E, Baldus SE, Schroder W, et al.: Staging ofesophageal carcinoma: Length of tumor and number of involvedregional lymph nodes. Are these independent prognostic factors?J Surg Oncol 2006;94:355–363.
9. Gu Y, Swisher SG, Ajani JA, et al.: The number of lymphnodes with metastasis predicts survival in patients withesophageal or esophagogastric junction adenocarcinoma whoreceive preoperative chemoradiation. Cancer 2006;106:1017–1025.
10. Barbour AP, Rizk NP, Gonen M, et al.: Lymphadenectomy foradenocarcinoma of the gastroesophageal junction (GEJ): Impactof adequate staging on outcome. Ann Surg Oncol 2007;14:306–316.
11. Yekebas EF, Schurr PG, Kaifi JT, et al.: Effectiveness of radicalen-bloc esophagectomy compared to transhiatal esophagectomyin squamous cell cancer of the esophagus is influenced by nodalmicrometastases. J Surg Oncol 2006;93:541–549.
12. Kang CH, Kim YT, Jeon SH, et al.: Lymphadenectomy extent isclosely related to long-term survival in esophageal cancer. EurJ Cardiothorac 2007;31:154–160.
13. Fumagalli U: Resective surgery for cancer of the thoracicesophagus. Results of a Consensus Coference held at the VIthWorld Congress of the International Society for Diseases of theEsophagus. Dis Esophgus 1996;9:S30–S38.
14. Dutkowski P, Hommel G, Bottger T, et al.: How many lymphnodes are needed for an accurate pN classification in esophagealcancer? Evidence for new threshold value. Hepatogastroentero-logy 2002;49:176–180.
15. van Sandick JW, van Lanschot JJ, ten Kate FJ, et al.: Indicatorsof prognosis after transhiatal esophageal resection withoutthoracotomy for cancer. J Am Coll Surg 2002;194:28–36.
16. Rizk N, Venkatraman D, Park B, et al.: The prognostic importanceof the number of involved lymph nodes in esophageal cancer;Implications for revisions for the American Joint Committee onCancer staging system. J Thorac Cardiovasc Surg 2006;132:1374–1381.
17. Wijnhoven BPL, Tran KTC, Esterman A, et al.: An evaluation ofprognostic factors and tumor staging of resected carcinoma of theesophagus. Ann Surg 2007;245:717–725.
18. Nigro JJ, DeMeester SR, Hagen JA, et al.: Nodes status intransmural esophageal adenocarcinoma and outcome after en blocesophagectomy. J Thorac Cardiovasc Surg 1999;117:960–968.
19. Rice TW, Blackstone EH, Rybicki LA, et al.: Refining esophagealcancer staging. J Thorac Cardiovasc Surg 2003;125:1103–1113.
20. Eloubeidi MA, Desmond R, Arguedas MR, et al.: Prognosticfactors for the survival of patients with esophageal carcinoma inthe U.S.: The importance of tumor length and lymph nodes status.Cancer 2002;95:1434–1443.
21. Korst RJ, Rusch VW, Venkatraman E, et al.: Proposed revisionof the staging classification for esophageal cancer. J ThoracCardiovasc Sug 1998;115:660–669.
22. Roder JD, Busch R, Stein HJ, et al.: Ratio of invaded to removedlymph nodes as a predictor of survival in squamous cellcarcinoma of the oesophagus. Br J Surg 1994;81:410–413.
23. Greenstein AJ, Litle VR, Swanson SJ, et al.: Prognosticsignificance of the number of lymph node metastases inesophageal cancer. J Am Coll Surg 2008;206:239–246.
24. Nishimaki T, Suzuki T, Suzuki S, et al.: Outcomes of extendedradical esophagectomy for thoracic esophageal cancer. J Am CollSurg 1998;186:306–312.
25. Akiyama H, Tsurumaru M, Udagawa H, et al.: Radical lymphnode dissection for cancer of the thoracic esophagus. Ann Surg1994;220:364–374.
26. Nishihira T, Hirayama K, Mori S: A prospective randomized trialof extended cervical and superior mediastinal lymphadenectomyfor carcinoma of the thoracic esophagus. Am J Surg 1998;175:47–51.
27. Hulscher JB, van Sandick JW, de Boer AG, et al.: Extendedtransthoracic resection compared with limited transhiatal resec-tion for adenocarcinoma of the esophagus. N Eng J Med 2002;347:1662–1669.
28. Sihvo EIT, Luostarinen ME, Salo JA: Fate of patients withadenocarcinoma of the esophagus and the esophagogastricjunction: A population-based analysis. Am J Gastroenterology2004;99:419–424.
29. Johansson J, DeMeester TR, Hagen JA, et al.: En bloc vstranshiatal esophagectomy for stage T3 N1 adenocarcinoma ofthe distal esophagus. Arch Surg 2004;139:627–631.
30. Barbier PA, Luder PJ, Schupfer G, et al.: Quality of life andpatterns of recurrence following transhiatal esophagectomy forcancer: Results of prospective followup in 50 patients. WorldJ Surg 1988;12:270–276.
Journal of Surgical Oncology
Role of Lymphadenectomy in Esophageal Cancer 193