Embed Size (px)
Citation preview

The Role of “Intent to Seek Treatment” Among Drug
Users Legally Mandated to Treatment
V.A. Stanick, A. Laudet, K. Morgen National Development and Research Institutes, Inc.,
J. Carway - VIP Community Services, Inc. NYC, NY
B. Sands NYC Health & Hospitals Corp./Woodhull Hospital Center
Funded by National Institutes on Drug Abuse Grant R03 DA13432
Correspondence [email protected]

Since inception in 1989, treatment courts has proliferated to 1,183 in2003, with many additional courts in the planning phase.1
The criminal justice field has produced the overwhelming majority of literature in the area of court-referred treatment (philosophy, target population, process, outcomes, etc.).
Demonstrated benefits that have supported the expansion of the treatment court concept are also those that have received the primary focus in literature on this topic. They include:2
1. Reduction of criminal recidivism.
2. Cost savings from drug courts (relative to cost of incarceration and crime-related costs to communities).
3. Impact on treatment retention of “mandated” clients.
Background: Treatment Courts

Limitations of current research
• Criminal justice and addiction studies have widely divergent perspectives, interests, and objectives.
• Thus there is relatively little research on addiction-related outcomes and on treatment outcomes.
• Much of the relatively small body of work in this area has been criticized for focusing primarily on “sociodemographic, rather than psychosocial characteristics” of criminal justice subgroups in addiction treatment.3
1. Recovery-promoting cognitions: Motivation Coping
2. Recovery-promoting behaviors – e.g., abstinence from D&A, 12-step meeting attendance
Outcome areas where research is needed

Prior Studies The few studies considering “psychosocial” domains among legally
mandated participants have yielded mixed results.
Of particular significance are findings regarding motivational variables (treatment motivation, readiness to change/stage of change),4 in subgroups with criminal justice involvement, ranging from “none” to “mandated.” Specifically:
Marshall & Hser (2002) reported that legally mandated clients had LOWER LEVELS of 1) treatment readiness, 2) confidence in—and 3) satisfaction with—treatment, than non-mandated peers.3
In contrast, Gregoire & Burke (2004) reported overall GREATER readiness to change in mandated clients entering treatment.4
Neither of those studies reported post-treatment outcome data to assess the impact of legal coercion and its possible interaction with readiness/motivation, treatment goal-attainment, program completion rates, etc.

Objective/Methods Objective: To extend and clarify previous work regarding the
role of recovery-related cognitions on outcomes among legally “mandated” clients in substance abuse treatment.
Specifically, we examined:
1. The association between “intent to seek treatment” and recovery-promoting cognitions at baseline (BL); and
2. The role of “intent to seek treatment” as a predictor of end of treatment (END) outcomes

KEY CONCEPTS 1. LEGAL STATUS: (entire sample) involvement with the
legal system at BL (YES?NO) IF INVOLVED
2. LEGAL MANDATE: “Was your coming to drug treatment at this time required or recommended by the criminal justice system (judge, probation/parole, etc.)?” YES/NO IF “YES” (mandated)
3. INTENT TO SEEK TREATMENT: “Do you think you would have come for drug treatment at this time if it had not been because of any legal pressure from the criminal justice authorities?” (YES/NO)
DOMAINS STUDIED 1. LEGAL INVOLVEMENT/COERCION + INTENT TO SEEK
TREATMENT
2. Baseline RECOVERY-PROMOTING COGNITION: Readiness to change, commitment to abstinence, commitment to 12-step, avoidance of high risk drug situations and 12-step attendance
3. END OF TREATMENT length of stay, treatment completion status, drug use and 12-step attendance.

HYPOTHESES H1 Legally coerced and non-coerced groups do not differ in
(BL) levels of RECOVERY-PROMOTING COGNITIONS or (END) treatment outcome measures (LENGTH OF STAY, TREATMENT COMPLETION, DRUG USE and 12-STEP ATTENDANCE).
H2 Among legally mandated participants, those who INTENDED TO SEEK TREATMENT independently of adjudication, compared to those who did not will have significantly higher levels of (BL) RECOVERY PROMOTING COGNITIONS and better outcomes at END (i.e., LENGTH OF STAY, TREATMENT COMPLETION, DRUG USE and 12-STEP ATTENDANCE).
STUDY DESCRIPTION Data collected in the context of a NIDA-funded investigation of
predictors and effectiveness of 12-step participation as an aftercare resource.
Participants (total N = 314) recruited from two large inner-city, publicly funded outpatient substance abuse treatment facilities within New York City.
Data were gathered at admission to index treatment and treatment end (completion or drop-out).
End of treatment interviews conducted with 221 participants to date (78% of valid cohort – in treatment =<30 days))
Participation was voluntary and based on informed consent. Computer-assisted semi-structured interviews approximately 2.5
hours in duration, administered at each data collection point. Participants received $30 at each interview.

DESCRIPTION OF SAMPLE (N = 221)
Male 58%Age (mean) 39 years (range = 19-60)African American 63%Hispanic 35%Education (mean): 10.6 years (range = 3-16)Primary income:
Government assistance 75(%)Job (on or off the books) 6Other legitimate income 18Illegal sources 1
Hepatitis C+ 22%HIV+ 9%Mental Health Problem (ever) 41%Substance Use past yr. 82%Substance Use past month 32%First time in treatment 59%
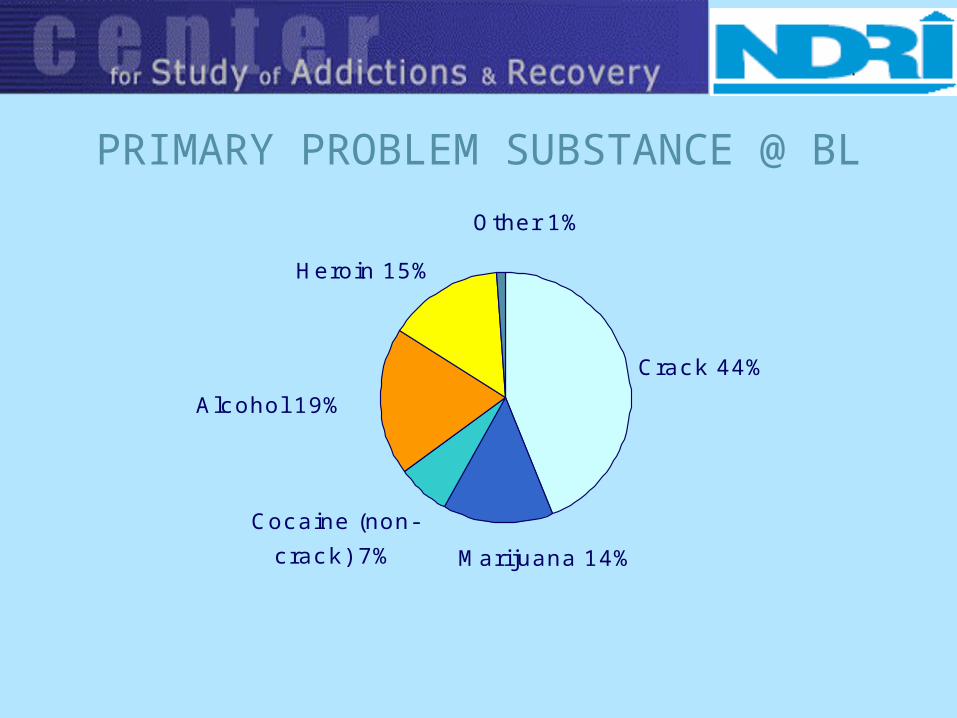
PRIMARY PROBLEM SUBSTANCE @ BL
Cocaine (non-
crack) 7%
Heroin 15%
Alcohol 19%
Marijuana 14%
Crack 44%
Other 1%
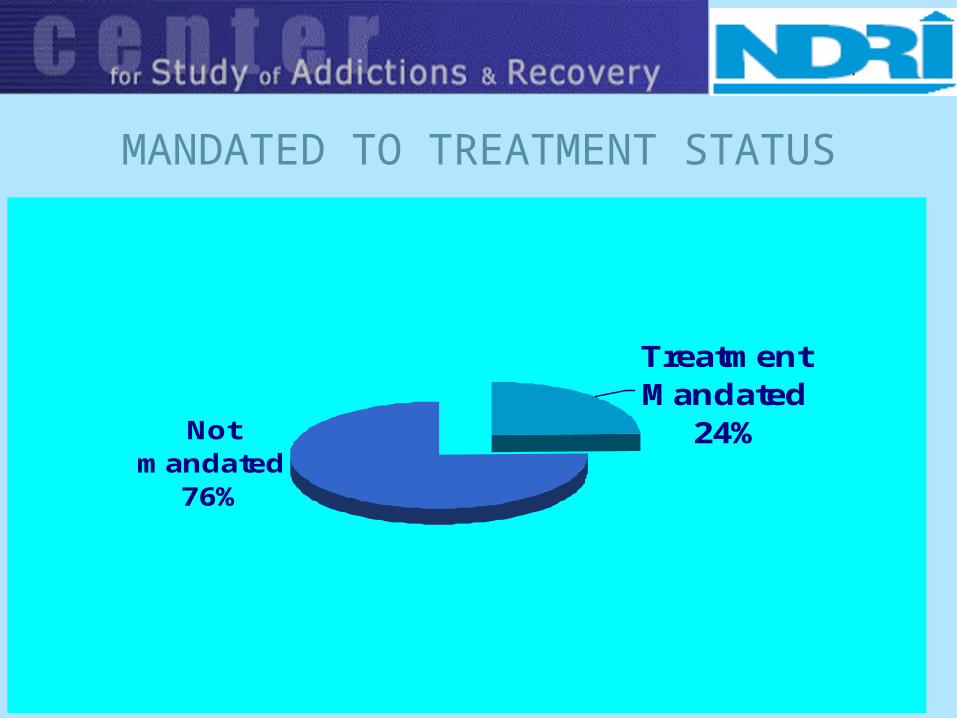
MANDATED TO TREATMENT STATUS
Not mandated
76%
Treatment Mandated
24%

INTENT TO SEEK TREATMENT STATUS(Mandated Subgroup Only—n=54)
NO
61%
YES
39%
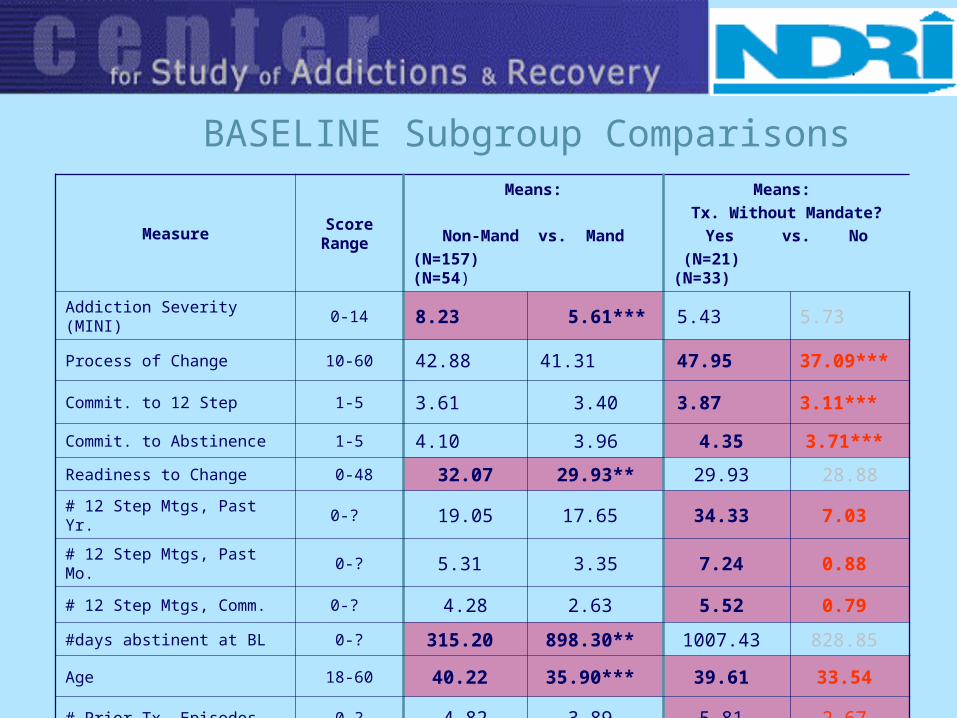
BASELINE Subgroup Comparisons
MeasureScore Range
Means:
Non-Mand vs. Mand(N=157) (N=54)
Means: Tx. Without Mandate?
Yes vs. No (N=21) (N=33)
Addiction Severity (MINI) 0-14 8.23 5.61*** 5.43 5.73
Process of Change 10-60 42.88 41.31 47.95 37.09***
Commit. to 12 Step 1-5 3.61 3.40 3.87 3.11***
Commit. to Abstinence 1-5 4.10 3.96 4.35 3.71***
Readiness to Change 0-48 32.07 29.93** 29.93 28.88
# 12 Step Mtgs, Past Yr. 0-? 19.05 17.65 34.33 7.03
# 12 Step Mtgs, Past Mo. 0-? 5.31 3.35 7.24 0.88
# 12 Step Mtgs, Comm. 0-? 4.28 2.63 5.52 0.79
#days abstinent at BL 0-? 315.20 898.30** 1007.43 828.85
Age 18-60 40.22 35.90*** 39.61 33.54
# Prior Tx. Episodes 0-? 4.82 3.89 5.81 2.67
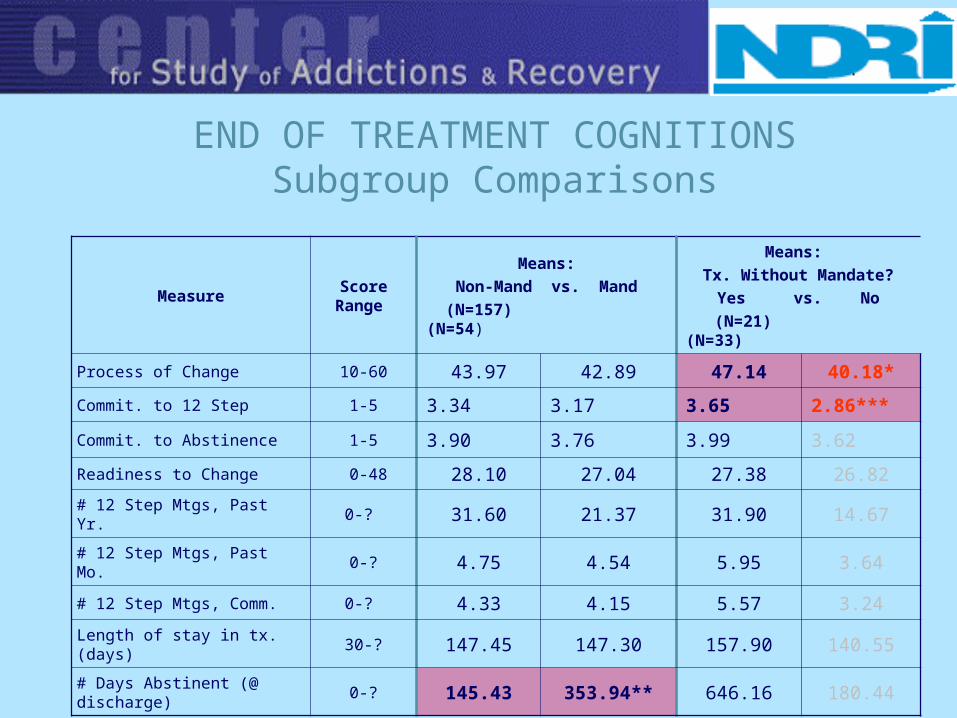
END OF TREATMENT COGNITIONSSubgroup Comparisons
MeasureScore Range
Means:Non-Mand vs. Mand
(N=157) (N=54)
Means: Tx. Without Mandate?
Yes vs. No (N=21) (N=33)
Process of Change 10-60 43.97 42.89 47.14 40.18*
Commit. to 12 Step 1-5 3.34 3.17 3.65 2.86***
Commit. to Abstinence 1-5 3.90 3.76 3.99 3.62
Readiness to Change 0-48 28.10 27.04 27.38 26.82
# 12 Step Mtgs, Past Yr. 0-? 31.60 21.37 31.90 14.67
# 12 Step Mtgs, Past Mo. 0-? 4.75 4.54 5.95 3.64
# 12 Step Mtgs, Comm. 0-? 4.33 4.15 5.57 3.24
Length of stay in tx. (days) 30-? 147.45 147.30 157.90 140.55
# Days Abstinent (@ discharge)
0-? 145.43 353.94** 646.16 180.44

END OF TREATMENT OUTCOMES Subgroup Comparisons [2]
MeasureFrequencies (%):
Non-Mand vs. MandSig.
Frequencies (%):Tx. Without Mandate?
Yes vs. No
Sig.
Used D/A since
Baseline @ Discharge?
NO 38.9 38.0
.910
57.9 25.8
.023
YES 61.1 62.0 42.1 74.2
Did you leave the program
because you graduated?
NO 59.9 63.0
.687
42.9 75.8
.015
YES 40.1 37.0 57.1 24.2

BASELINE FINDINGS SUMMARYComparisons of NON-MANDATED and MANDATED groups found:1. Age NON-MANDATED OLDER THAN MANDATED2. Dependence severity - MANDATED LESS SEVERELY DEPENDENT
than NON-MANDATED3. Readiness to Change (NON-MANDATED >MANDATED)4. # days abstinent from drugs/alcohol at baseline (MANDATED
reporting longer abstinence than NON-MANDATED)
Comparisons of mandated subgroups defined by INTENT (vs. NO INTENT) to seek treatment regardless of court mandate found:
1. Age: INTENT group OLDER than NO INTENT.2. Commitment to 12 Step: INTENT group > NO INTENT3. Commitment to Abstinence: INTENT > NO INTENT 4. Frequency of 12 Step Meeting Attendance: INTENT > NO INTENT
(all measures: past year, past month 5. Process of Change: INTENT > NO INTENT6. 12-Step attendance: community-based meeting locations INTENT
> NO INTENT.

END OF TREATMENT FINDINGS SUMMARY
Comparisons of NON-MANDATED and MANDATED groups indicated:1. NO DIFFERENCES in reported drug use since baseline, length of
treatment stay, rate of program graduation (vs. early drop-out), nor in commitment to abstinence/12 Step, Readiness to Change at discharge, or Process of Change.
2. The single comparison yielding significant results was that of total number of days abstinent (mandated>non-mandated).
Comparisons of mandated subgroups defined by INTENT (vs. NO INTENT)
to seek treatment regardless of court mandate found:1. Process of Change and Commitment to 12 Step: INTENT > NO INTENT2. Reported drug/alcohol use since baseline: NO INTENT > INTENT3. Rate of program graduation (vs. early drop-out): INTENT group left tx.
due to graduation at a higher rate than NO INTENT.

HYPOTHESES/CONCLUSIONS: H1
(H1)Legally coerced and non-coerced clients do not differ in (BL) levels of RECOVERY-COGNITIONS or END OF TREATMENT outcome measures
1. BASELINE Readiness to Change results (NON-MANDATED > MANDATED) did not support this hypothesis.
2. DISCHARGE results generally supported the hypothesis.
• BASELINE results strongly supported the hypothesis, EXCEPT in the case of readiness to change
• DISCHARGE results supported to the hypothesis—most strongly evident in the strikingly greater rates of graduation, abstinence during treatment, and Commitment to 12 Step in the INTENT group.
HYPOTHESES/CONCLUSIONS: H2
H2: Among legally coerced participants, the subgroup WITH INTENT TO SEEK TREATMENT independently of adjudication, will demonstrate significantly higher levels of recovery promoting cognitions @ BL and and better outcomes@ DIS.

CONCLUSIONSLegally-mandated clients may:
1. Be younger on average, and have less severe substance dependence but otherwise appear OVERALL on initial assessment to be essentially similar to their non-mandated peers in treatment, AND
2. in general have potential equal to those who are self-referred, for favorable treatment outcomes (program completion, integration into 12 Step support systems, maintenance of abstinence from drugs/alcohol, etc.) In fact with few exceptions the two groups did not differ substantially from one another.
3. HOWEVER, when only the subgroup of legally-mandated clients was examined, accounting for whether or not treatment would have been considered an option independent of the coercive force of legal authority a different picture emerges . . .
4. A distinct difference appeared in the legally mandated group at baseline, between those who had INTENT to seek treatment regardless of mandate, and those who had NO INTENT independent of the mandate.
Those with INTENT had more favorable prognostic signs than those with NO INTENT.
The NO INTENT group was younger than the INTENT group, with fewer prior treatment episodes.
5. FURTHER: That division extended to crucial treatment outcomes, with significantly greater attainment of important achievement markers by the group with INTENT (e.g., program graduation, drug/alcohol abstinence, sustained commitment to 12 Step) that might well impact on longer-term behavior.
CONCLUSIONS (contnd)

IMPLICATIONS/RECOMMENDATIONS
1. “Intent to seek treatment” may be an important factor to consider in assessment of potential candidates for legally-mandated treatment.
2. Treatment providers serving legally mandated clients might benefit from attending to this factor when designing intervention strategies, and should explore the possibility of providing specialized services for the group whose lack of intrinsic intent to enter treatment, relatively young age and lack of treatment experience may prove to be challenges to the standard array of techniques.
3. Behavioral scientists studying addiction might consider intent to seek treatment in “coerced” participants as a variable that may mediate or interact with other effects (e.g., motivation, measures of treatment outcome, etc.).
4. Future, larger scale, systematic studies are recommended to assess the utility of the concept of intent to seek treatment as a prognostic and/or modulating variable in the population of legally-mandated clients in treatment.

REFERENCES1. American University Drug Court Clearinghouse and Technical Assistance Project, 2003.2. National Drug Court Institute. “Drug Court Facts.” Drug courts: A national phenomenon.3. Marshall, G.N. and Hser, Y-I. (2002) Characteristics of criminal justice and noncriminal justice clients
receiving treatment for substance abuse. Addictive Behaviors (27), 179-192.4. Gregoire, T.K. and Burke, A.C. (2004) The relationship of legal coercion to readiness to change
among adults with alcohol and other drug problems. Journal of Substance Abuse Treatment (26), 337-343.
INSTRUMENTS Sheehan, D.V. & Lecrubier, Y. Mini International Neuropsychiatric Interview. University of South
Florida–Tampa, 2002. Prochaska JO, Velicer WF, DiClemente CC, & Fava J. (1988) Measuring processes of change:
Applications to the cessation of smoking. Journal of Consulting and Clinical Psychology, 56: 520-528.
Morgenstern, J. & McCrady, B.S. Cognitive processes and changes in disease-model treatment. In: McCrady, B.S. and Miller, W.R. (Eds.) Research on Alcoholics Anonymous: Opportunities and Alternatives, New Brunswick, NJ: Rutgers Center of Alcohol Studies, 1993, pp. 154-164.
Budd, R.J. & Rollnick, S. (1996) The structure of the Readiness to Change Questionnaire: A test of Prochaska & DiClemente’s transtheoretical model. British Journal of Health Psychology 1: 365-376.
Rollnick, S., Heather, N., Gold, R., & Hall, W. et al, (1992) Development of a short 'readiness to change' questionnaire for use in brief, opportunistic interventions among excessive drinkers. British Journal of Addiction 87(5): 743-54, 1992.