Embed Size (px)
DESCRIPTION
The ROLE of GLUCAGON in DIABETES : An Update Pierre Lef èbvre. Cairo, Egypt, September 2007. 1923. Murlin et al The discovery. 1942 Czyste Hospital Warsaw Ghetto. Studies on « Hunger’s disease » by Dr Emil Apfelbaum et al. 1949. Foà* et al Cross-circulation experiments - PowerPoint PPT Presentation
Citation preview

1
The ROLE of GLUCAGON in DIABETES :An Update
Pierre Lefèbvre
Cairo, Egypt, September 2007

2

3

4
1923
Murlin et al The discovery

5
1942Czyste Hospital Warsaw
GhettoStudies on « Hunger’s disease » by Dr
Emil Apfelbaum et al

6

7

8
1949
Foà* et alCross-circulation experiments
*Only Author I know to have published a paper when in utero …

9

10

11
Insulin-inducedhypoglycemia inthe « donor » dog
Paradoxical hyperglycemia in the dog receiving PDV blood

12
1959-1960
Unger et al The first polypeptide radio-immunoassay

13
Roger UNGER

14
1973

15
Topics
Importance of glucagon for the maintenance of glucose Importance of glucagon for the maintenance of glucose homeostasishomeostasis
The physiology of glucagon production and how glucagonexerts its effects
Abnormalities of glucagon secretion in patients with T2DM

16
Pancreatic Islet Hormones Are Critical for Normal Glucose Tolerance
HGO = hepatic glucose outputAdapted from Unger RH. Metabolism. 1974;23:581–593
Glucose
-Cells -Cells
Insulin Glucagon–+
Glucose
uptake
HGO
+

17
+Glucagon*
(plasma concentration)
–
–Insulin*
(plasma concentration)
+Glucose
(plasma concentration)
The Physiological Balance Between Insulin and Glucagon is Essential for Normal Metabolic Control
*Insulin and glucagon secretion are also influenced by other nutrients, hormones, and neural input Adapted from Berne RM, Levy MN, eds. Physiology. St. Louis, Mo: Mosby, Inc; 1998:822–847

18
Glucagon is Important to Maintain Adequate FPG Levels Between Meals
Adapted from Unger RH. Diabetes. 1983;32:575–583
α-Cell
Blood glucose4.5 mmol/L (81 mg/dL)
4 g/h
6 g/h
Glucagon
10 g/h
+
Glucose production = Glucose
utilization

19
Normal Reciprocal Response of Insulin and Glucagon in Persons Without Diabetes
CHO = carbohydrateAdapted from Unger RH, et al. N Engl J Med. 1971;285:443–449
Glucose
mg%
12010080
–60 0 60 120 180 240Time (min)
CHO Meal
Insulin
μU/m
L
12080400
Glucagon
90
pg/m
L 120110100
Postprandial Insulin and Glucagon Responses in Persons Without Diabetes

20
Topics
Importance of glucagon for the maintenance of glucose homeostasis
The physiology of glucagon production and how glucagonThe physiology of glucagon production and how glucagonexerts its effectsexerts its effects
Abnormalities of glucagon secretion in patients with T2DM

21
α-Cell Function is Regulated by Nutrient, Neural and Hormonal Influences
Adapted from Dunning BE, et al. Diabetologia. 2005;48:1700–1713
Stimulatory Factors (↑ Glucagon)Stimulatory Factors (↑ Glucagon) Inhibitory Factors (↓ Glucagon)Inhibitory Factors (↓ Glucagon)
Hypoglycaemia
Protein meal
Amino acids
Stress; adrenaline (epinephrine)
Sympathetic/parasympathetic nerves
GIP
Glucose
Carbohydrate meal
Ketones
Insulin
Somatostatin
GLP-1

22
Glucagon Stimulation of Hepatocytes Leads to Increased Hepatic Glucose Production
TCA = trichloroacetic acidAdapted from McMurry J, et al. Fundamentals of General, Organic, and Biological Chemistry. 4th ed. Upper Saddle River, NJ:Prentice Hall; 2006Jiang G, Zhang BB. Am J Physiol Endocrinol Metab. 2003;284:E671-E678
Glycolysis
Glycogenolysis
HGP
Glucose
Glucagon
-+
Glycogenesis
Gluconeogenesis
-+

23
Glucagon From α-Cells is Responsible for 75%of HGP
HGP = hepatic glucose production*Somatostatin and insulin were delivered to induce selective glucagon deficiency †Healthy, non-obese men age 18–30Adapted from Liljenquist JE, et al. J Clin Invest. 1977;39:369–374
150
100
50Net
Spl
anch
nic
Glu
cose
Pro
duct
ion
(mg/
min
)
Time (min)–30 0 30 60 90 120
START INFUSION*
<.01 <.01 <.01 <.01<.01
<.01 <.01 <.01
75% in HGP
vs baseline
N = 8†

24
Changes in Glucagon/Insulin Ratio Regulate HGO and Glycogen Synthesis in Normal Physiology
HGO = hepatic glucose output*All measurements made after a standard mixed meal in healthy volunteers ages 18–40 years†HGO completely suppressed after 30 minutes of meal intakeAdapted from Taylor R, et al. J Clin Invest. 1996;97:126–132
Liver Glycogen (mmol/L)*HGO (mg/kg.min)*†Glucagon/Insulin ratio*
| | | | | |0 120 240 360 480 600
40 –
30 –
20 –
10 –
0 –
Minutes
(n= 6) (n= 6) (n= 8)
2.5 –
2.0 –
1.5 –
1.0 –
0.5 –
0 –
Minutes
| | | | | |0 120 240 360 480 600
350 –
300 –
250 –
200 –
150 –
Minutes
| | | | | |0 120 240 360 480 600

25
Topics
Importance of glucagon for the maintenance of glucose homeostasis
The physiology of glucagon production and how glucagonexerts its effects
Abnormalities of glucagon secretion in patients with T2DMAbnormalities of glucagon secretion in patients with T2DM

26
T2DM = type 2 diabetes mellitusAdapted from Rhodes CJ. Science. 2005; 307:380–384
α-Cells (glucagon)
Normal T2DM
β-Cells(insulin)
• Disorganised and misshapen • Marked reduction in β-cell number • Amyloid plaques
Amyloid plaque
Pancreatic Islet Morphology: Structural Defects are Evident in T2DM

27
Islet Dysfunction Leads to Hyperglycaemiain T2DM
HGO = hepatic glucose outputAdapted from Unger RH. Metabolism. 1974;23:581–593
T2DM pancreatic islet
Glucose
Fewer -cells -cell hypertrophy
Insufficient insulin Excess glucagon–+
Less effective glucose uptake
HGO↑
↑

28
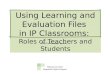
In T2DM, Insufficient Insulin and Elevated Glucagon Secretion Result in Hyperglycaemia
Adapted from Müller WA, et al. N Engl J Med. 1970;283:109–115
CHO meal
Glucagon
Time (min)
75
100
125
150
–60 0 60 120 180 240
pg/m
L
Insulin0
50
100
150
μU/m
L
0Glucose100
200
300
400
mg/
dL NGTT2DM
NGTT2DM
NGTT2DM

29
Decreased Glucose Disposal and Increased HGP Contribute to Increased FPG in T2DM
HGP = hepatic glucose production; FPG = fasting plasma glucose; T2DM = type 2 diabetes mellitusAdapted from DeFronzo RA. Diabetes. 1988;37:667–687
1.01.52.02.53.03.54.04.5
50 100 150 200 250 300FPG (mg/dL)
Glycogenolysis andGluconeogenesis
(mg/kg • min)
Excessive glucagon-mediatedglucose output
0.81.21.62.02.42.8
50 100 150 200 250 300
Glucose Clearance
(mL/kg • min)Impairedinsulin-mediated glucose disposal
Diagnosis

30
Suppression of Endogenous Glucose Production is Impaired in T2DM
HGO = hepatic glucose outputAdapted from Kelley D, et al. Metabolism. 1994;43:1549–1557
Time (minutes)-30 -15 0 30 60 90 120 150 180 210 240 270 300
Meal
2
6
10
14
18
Endo
geno
us G
luco
se(µ
mol
/min
/kg)
NGT (n= 12)
T2DM (n= 18)

31
α-Cell Sensitivity to Glucose is Reduced in T2DM
AGRarg= mean acute glucagon response to arginine from 2 to 5 min; PG50 = plasma glucose level required for half-maximal suppression of AGRargT2DM = type 2 diabetes mellitus; *Healthy men ages 18–29Adapted from Ward WK, et al. J Clin Invest. 1984;74:1318–1328. Dunning B, et al. Diabetologia. 2005;48:1700–1713
NGT* (n = 8)T2DM (n = 8)
180 -
150 -
120 -
90 -
60 -
30 -0 100 200 300 400 500 600 700
AGR a
rg (p
g/m
L)
Plasma Glucose Level (mg/dL)
PG50

32
In Patients with T2DM, Suppression of Glucagon Reduces Glycogenolysis and Plasma Glucose Levels
†P <0.0001 between groups; ‡P <0.001between groups§As assessed by [14C] glucose appearanceProtocol: somatostatin and insulin delivered to mimic glucagon deficiency, then glucagon infused to simulate a non-suppressed day,or delayed by 2 hours to create transient glucagon deficiency (suppressed day)Adapted from Shah P, et al. J Clin Endocrinol Metab. 2000;85:4053–4059
Glucagon GlucoseGlycogenolysis§
Glu
cose
(m
mol
/L)
-60 0 60 120 180 240 300 3604
6
8
10
12
Time (min)
↓50-g glucose‡
Glu
cago
n (n
g/L)
-60 0 60 120 180 240 3003600
100
200
Time (min)
50
150
↓
†† † †
50-g glucose
dpm
/kg/
min
0 60 120 180 240 300 3600
4,500
3,000
1,500
Time (min)
‡
‡‡
‡
↓50-g glucose
(n= 9)
Non-suppressed glucagon Suppressed glucagon

33
Effect of a glucagon monoclonal antibody on glucose excursion during an OGTTIn ob/ob mice. Data from Sorensen et al , Diabetes 2006, 55: 2843-2848 m

34

35
Hyperglucagonemia is a feature of all forms of diabetes
« Dual A- and B-cell abnormality » ?A-cell insulin resistance ?Hyperglycemia-induced desensitization of the A-cell (Glucotoxicity ? )

36
An alternative hypothesis*
-Insulin and glucagon are secreted in a pulsatile manner-Normal intra-islet insulin pulsatility helps avoiding excessive glucagon release-Normal insulin pulsatility is lost in diabetesThus, loss of normal intra-islet insulin pulsatility may be involved in the hyperglucagonemia of diabetes *Lefèbvre, Paolisso and Scheen 1991

37
Lelio ORCI

38

39

40
Pulsatile insulin and glucagon-induced glucagon release*
Nine Type 1 diabetic patients Very small insulin infusion given either continuously (circulating insulin levels ~15 µU/ml) or same total amount of insulin given in 13 min pulses and both compared to saline infusion No significant effect on blood glucose After 52 minutes, 5gm iv arginine pulse and evaluation of integrated glucagon response
*Paolisso et al , JCEM1988,66: 1220-26

41

42

43
New support for the intra-islet insulin hypothesis
MEIER JJ, KJEMS LL, VELDHUIS JD , LEFEBVRE PJ and BUTLER PC : Postprandial Suppression of Glucagon Secretion Depends on Intact Pulsatile Insulin Secretion : Further Evidence for the Intraislet Insulin Hypothesis*
*Diabetes , 55:1051-1056,2006

44
-40 -35 -30 -25 -20 -15 -10 -5 00.0
2.5
5.0
7.5
10.0
12.5
15.0
Post alloxanPre alloxan
p = 0.067
Glu
cose
[mm
ol/l]
0 10 20 30 40 50 60 70 80 900.0
2.5
5.0
7.5
10.0
12.5
15.0
Post alloxanPre alloxan
Testmeal
p = 0.021
Glu
cose
[mm
ol/l]
-40 -35 -30 -25 -20 -15 -10 -5 00
200
400
600
800
1000
1200
1400
p = 0.032
Insu
lin [p
mol
/l]
0 10 20 30 40 50 60 70 80 900
200
400
600
800
1000
1200
1400p = 0.079
Insu
lin [p
mol
/l]
-40 -35 -30 -25 -20 -15 -10 -5 00
20406080
100120140160
Time [min]
Glu
cago
n [p
g/m
l]
p = 0.0045
0 10 20 30 40 50 60 70 80 900
20406080
100120140160
Time [min]
Glu
cago
n [p
g/m
l]
p = 0.0037
A B
C D
E F

45
-40 -30 -20 -10 080
90
100
110
120
130
Glu
cago
n [p
g/m
l]
-40 -30 -20 -10 00
10
20
30
40
50
60
70
Time [min]
Glu
cago
n se
cret
ion
[pg/
ml/m
in]
A
B
Glucagon pulsesin the basal stateprior to alloxan in a representative pig

46
GLUCAGONPulse mass, heightand interval in the fasting state and after a meal studiedboth before and after alloxan in 7 pigs*
*Meier et al , 2005submitted

47
-20 -10 0 10 20-0.8-0.6-0.4-0.2-0.00.20.40.60.8
Lag time [min]
Cor
rela
tion
coef
ficie
nt
-20 -10 0 10 20-0.8-0.6-0.4-0.2-0.00.20.40.60.8
Lag time [min]
Cor
rela
tion
coef
ficie
nt
A
B
Pre alloxan
Post alloxan
Mean cross-correlogrammsbetween insulin and glucagon concentrationstime series in 7 pigsstudied over 90 min aftera test meal, each prior andafter alloxan treatment.
The relationship between insulin and glucagon levelsis significant before but disappears after alloxan

48
1.0
1.5
2.0
2.5p = 0.0035
Forward Reverse
Cros
s-Ap
En
1.0
1.5
2.0
2.5p = 0.80
Forward Reverse
Cros
s-Ap
En
Pre alloxan Post alloxan
« Forward » and « reverse » cross-AsPen analyses imply that, in the post-prandial state,pulsatile insulin secretion directly suppresses glucagon secretion, but that this associationis lost after a ~60% reduction in beta cell mass

49
In conclusion
It is confirmed that glucagon is secreted in distinct pulses both in the fasting state and after a meal In healthy minipigs, suppression of glucagon secretion after a meal is likely accomplished, at least in part, by increased insulin secretion This action of insulin is lost in the minipig alloxan model of Type 2 diabetes mellitus in which post-prandial insulin secretion is impaired as a consequence of an ~60% decrease in beta-cell mass
We conclude that post-prandial hyperglucagonemia in diabetes is likely due ,at least in part, to impaired insulin secretion leading to a loss of intra-islet driven suppression of glucagon secretion

50
Potential Clinical Consequence:The best way to normalize the hyperglucagonemia of diabetesmay be to restore normal insulinsecretion , including pulsatility …Increase in amplitude of insulin pulses, without changes infrequency,reported by a 6wk GLP1 infusion in 5 old patients with T2DM by Meneilly et alJCEM, 2005, 90: 6251-56

51
Glucagon: Summary
Glucagon plays an essential role in glycaemic control α-Cell sensitivity to glucose is impaired in T2DM, resulting in
excessive glucagon secretion Excessive glucagon secretion contributes to hyperglycaemia
in both IGT and T2DM Lowering glucagon levels will be a valuable therapeutic target
in the treatment of T2DM
IGT = impaired glucose tolerance; T2DM = type 2 diabetes mellitus