Embed Size (px)
Citation preview

(2003). In R.J. Davidson, K.R.Scherer, & H.H. Goldsmith (Eds.),Handbook of affective sciences.New York: Oxford University Press
THE ROLE OF EMOTION ON PATHWAYS
TO POSITIVE HEALTH
CarolD. Ryff and Burton H. Singer
A second generic observation setting the stage for whatfollows is the relative paucity of knowledge about positiveemotion-health linkages. Our goal is to bring greater atten-tion to salubrious conn~ons between affective experi-ence and health. mental and physical. An emphasis onpositive health, we note, does not translate simplisticallyto a focus on exclusively positive affe:ctive experience. Aswe will argue. one of the intrigiling challenges of futurework is to unearth basic processes whereby negative emo-tions, ubiquitous in human experience, can be trans-formed into benign. or even beneficial. inBuences onhealth. Finally. while we seek to U;nderscore the positivehealth theme, much in our chapter deals with the role ofem()tion in illness as that is where most prior work hasbeen conducted.
Many of the core questions in affective science (e.g.. Arethete basic emotions? What are the antecedents and func-
. tions of emotion? How do inQividuals differ in emotionalreactivity?) have developed without explicit connection tothe realm of human health. Alternatively. when emotionhas entered the health realm (e.g.. Does anger increase car-diovascular risk? Is optimism protective?), it hU fre-quently been with little connection to mainstream re-search in affective science. This separation is not a stateof affairs to lament. but rather represents opportunities forthe future in - ~hich the fields of emotion and health canenrich and extend each other.
Our objective in this chapter is to bring the nexus be-tween these realms into focus via discussion of five guid-ing premises for relating emotion to health. These serve asconceptual guideposts for exami~ past, current, and fu-ture empirical studies. and do so with an emphasis ontestable hypotheses. The five premises are: (1) emotionsconseque~tial for health are about something; (2) healthrequires a focus on co-occurring cliscrete emotions; (3)health is biopsychosocial in nature and necessitates in~-gration of phenomenology and neurophysiology; (4) cu-mulative, chronic emotions are consequential for health;and (5) emotion can be protective and promote positivehealth. Each premise is illustrated via separate substantivestudies. although a unifying theme across them is the needfor integrativ~ endeavors that put together psychosocialexperience. underlying biological mechanisms. and healthoutcomes.
Premise I. Emotions Consequential forHealth Are About Something
In building connections between affective experience andhealth, we propose that it is particularly valuable to an.chor emotion in the life contexts in which they occur. Thisis a call for greater emphasis on what gives rise to emo-tion. Ekman's (1992) description of basic emotions em.phasized that they '"evolved for their adaptive value indealing with fundamental life-tasks" (p. 171). He drew onnumerous works of others to summarize the universal pre-dicaments (achievements. losses, frustrations), the com.
1083

1084 PART X. EMOTIOt-l AND HEALTH
over the course of his life by his inability to come to theassistance of his father as he called for help in the con-centration camp. He was, in fact, unable to speak at theNobel Peace Prize ceremony in his honor in 1986 becauseof the following recollection.
I see myself once again with my father on the lastday of his life, the last night. I was near him as heagonized, but not at the hour of his death. I speakof it in "Night. " He called me. My father called
me, gently, we~y. I heard him moaning. I heardhim calling. His cries tore me apart; they tear meapart still. In spite of the danger I should havegone to him, run to him. I should have said to .him:"I'm here Father. Your son will never leave you." Ishould have told him something, anything. But wewere forbidden to speak. I would have beenb~aten, beaten to death. I would have been ~led. Iwas afraid then. I am affaid now. (pp. 270-271)
mon adaptational tasks (fafing danger. progressing towarda goal), the recurrent situ,tions (fighting, falling in love,escaping predators, confropting sexual infidelity) that cat-alyze emotion. Simply pu~ emotions are designed to dealwith "inter-organismic encpunters" (po 171)-they are fun~damentally about somethfitg.
To those outside the fiJld of affective science, callingfor attention to what emo~ons are about may seem gra-tuitous-indeed, an obvio~ point. However, extant workin the affective field reve8ls that it is the exception, notthe rule, to focus on the fundamel:ltallife-tasks describedabove. In examining the oltigins and functions of positiveand negative affect, Carvet and ~Cheier (1990) m(1ke thepoint that how good and b~d feelings arise is a pervasivelyneglected question: "Ind~, it is remMkable how rarelyanyone ever asks where aff~ct comes from" (p. 22), and goon to note that many form4iations discuss only what hap-pens once affect is already present. Likewise. the literatureaddressing the basic s~cture. of emotion and affect(Green, Salovey, &; Truax, ,1999; Russell &; Barrett, 1999;Watson, Wiese. Vaidya, &; tellegen. 1999; Yik, Russell, &;Barrett, 1999) is primarily ~bout momentary. free-floatingassessments of reported f+lings. At the level of neUralsubstrates the focus is also I"more on the architecture andoperating characteristics of the affect system than on theantecedent condition for arpusing positive or negative af-fect" (Cacioppo, Gardner, ~ Berntson, 1999, p.849).
Drawing on these distinctions. Russell and Barrett(1999) distinguish betweerl core affect as the most ele-mentary c~nsciously accejlSible affective. feelings (and~eir neurophysi~logical cqunterparts) that ".need not.bedirected at anything" (p. 896), and protOtypICal emotionepisodes, Which are fee~~ concerned with a specific ob-ject-"one is afraid of, is *gry with, is in love with, orhas pity for something" (p. ~06). Most parsing of affectivespace has been about the former, not the latter (see laterdiscussion of discrete versu, dimensional models in Prem-ise II). Moreover, when f~lings about something havebeen considered, the focu~ is typically on "temporaryevents and slices of time" (~ 805). They note that love andhate, prototypical exempl$ of emotion, as in lifelonglove of an offspring, are no~ part of their purview.
Why do we advocate for greater focus on the funda-.mental life tasks that give rise to emotion in buildingbridges to health? A first reason is that emotional reactionsto core life challenges are, we propose, powerful elicitorsof affect-both phenomenol~gically and physiologically. Itis grinding fefJlings of defe~t or exhilarating triumph inpursuing sought-after goals, along with the comforting se-curity or tormen,ting despafr in primary social relation-ships, that leave a greh.t imprint on psyche and soma. Fur-ther. given our advanced cognitive capacities. thesepoignant, sometimes elevatfng, sometimes debasing hu-man feelings may well be r~activated simply by tbj!1kingabout them. Elie Wiesel (19~9) wrote about being haunted
Early on in the affective field, Da{Win asked whether wecan feel anger. fear. sadness. and enjoyment when we arealone (1872/1998). For the human species. the answerseems a resounding yes; we suggest that this capacity isconsequential for hltalth.
A further reason for focusing on what emotions areabout intersects with studies of life stressors that havebeen previously linked to intervening neuroendocrine,cardiovascular. and immunological mechanisms impli-cated in health outcomes (McEwen 8r. Schmeck, 1994; Sa-polsky, 1992; Weiner, 1992). That is, notable benefits re-garding the explication of mechanisms follow fromfocusing on the ~damental life-tasks that give rise toemotion. This interface between the psychobiology of lifestress and the emergent field of affective science repre-sents another promising nexus for cross-fertilization andinterdisciplinary inquiry. Emotiou. it can be argued, hasbeen insufficiently elaborat~d in the stress literature. Con-comitantly, anchoring the study of affect in fundamentallife-tasks provides connection to neurophysiologicalmechanisms implicated in stress.
Yet another reason for emphaSizing what emotions areabout pertains to the challenge of discerning whether par-ticular emotional responses are adaptive. maladaptive,healthy, unhealthy, warranted. or unwarrantect. Davidson,Jackson. and Kalin (2000) argue that to answer these ques-tions, it is critical to know the context in which the affectis experienced-that is, what the feelings are about. Theyfurther suggest that "context-inappropriate responding." ahypothesized product of hippocampal dysfunction, is ahallm3rk of certain forms of psychopathology.
To illustrate the consequential nature (for health) offeelings about something, we offer two examples below.The first pertains to emotions about significant others, andthe second involves emotions about racism. We select

\.
CHAPTER 57. THE ROLE OF EMOTION ON PATHWAYS TO POSITIVE HEAlTH 1085
these examples because they bring into high relief the ex-tent to which health questions may l~ad to distinct waysof organizing affective experience fro$ currently availablemodels. For example, most key social emotions (e.g., love,hate, affection, attachment, jealousy, envy) are notably ab-sent in f()rmulations of core affect (R~sell & Barrett, 1999;Watson, Wiese, Vaidya, & Tellegen, 1999; Yik et al., 1999).Similarly, the experience of racism may not be fruit:ful1ycaptured by two.,dimensional models of valence (positive,n~ative) and activation (low, high). This is not a criticismof such models, as they were not designed with healthquestions in mind, but rather an observation that pushingforward agendas on emotions and health may requirenovel conceptualizations of the affect!ve realm. A furtherreason for selecting these two illusttations is that bothhave been previously linked to heal~ outcomes.
Still other literatures map the biological processes as-sociated with social interactions. be they affiliative expe-riences. social isolation. or social conflict (e.g., "Carter,1998; Coe. 1993; Cohen &; Herbert, 1996; Kiecolt-Glaser etal., 1997; Knox &; Uvnas-Moberg. 1998: Panksepp. 1998b;Seeman &; McEwen, 1996; Uchino et al.. 1996; Uvnas-Moberg. 1998). This is where biological sequelae at mul-tiple physiological levels (cardiovascular, neuroendocrine.immunological) are examined. .
lliustrating what emotion is about and its links to phys-iology is the growing literature on marital cqnflict. Kiecolt-Glaser et al. (1997) have shown that among adults in long-term marriages. 30 minutes of conflict discussion wasassociated with changes in cortisol. adrenocorticotropichonnone (ACTH). and norepinephrine in women. but notmen, Both husbands and wives showed poorer immuno-logical response during conflict, Among newlyweds.Kiecolt-Glaser et al. (1996) also found higher cortisol andepinephrine levels among wives. but only those whosehusbands had high probabilities of withdrawal responsein their negative communication. More frequent positivebehaviors were also associated with lower epinephrineand higher prolactin levels among wives, but not hus-bands. Other studies have linked marital conflict withhigh blood pressure (Ewart. Taylor. Kraemer. &; Agras.1991). pituitary and adrenal honnones{Malarkey. Kiecolt-Glaser, Pearl. &; Glaser. 1994). and physiological arousal(Levenson. Carstensen. &; GOttman (1994).
Taylor, Repetti. and Seeman (1997) have also exploredthe nature of "unhealthy environments" at the family leveland how they get under the skin. Their review points tothree characteristics of the social environments that un-dermine the health of children and adolescents: a socialclimate that is confliCtual'and angry. or even violent andabusive; parent-child relationships that are unresponsiveand lacking in cohesiveness. warmth. and emotional sup-port; and a p~nting style that is either overly controllingand dominating, or uninvolved with little imposition ofrules and structure, Such characteristics were linked todepression and maladaptive ways of coping in children aswell as health-threatening behaviors in adolescents.
Emotion is a critical ingredient in putting together thepieces of social experience and biology. That is. the affec-tive experiences in proximal and primary social relation-ships-that is. feelings of love. nurturance, intimacy. af-fection, and attachment in the positive scenario. orexperiences of anger. bitterness. resentment. humiliation.and withdrawal in the negative case-are likely centralactivators of physiological mechanisms that subsequentlyfeed into health outcomes. This is not to overlook the in1-portant behavioral routes through which social supportin1pacts health, such as how significant others promoteand encourage positive health practices (Berkman. 1995;Spiegel &: Kimerling. 2001; Taylor et al.. 1997). Rather. itis a call to sharpen and heighten the emphasis on the emo-
Emotions About Significant Others
By significant othersl we refer to those individuals (chil-dren, parents, spouses, co-workers. friends) deemed cen-tral players in one's life. Affective experience surroundinginteraction with such individuals cQinStitutes a primarycategory of the inter-organismic enco~ters described byEkman. Moreover, a large and growins literature has doc-umented links betWeen the social rQlationaJ realm andmorbidity and mortality (Berkman Br Breslow. 1983;House, Landis, & Umberson, 1988; ~ &:: Singer, 2000;Seeman, 1996; Seeman, Berkman, Bl+zer Br Rowe, 1994;Uchino, Cacioppo. & Kiecolt-Glaser, 1996). A review ofeight major epidemiological studies (Berkman, 1995) in-dicated' that, in each case, mortality was significantlylower among persons who were more socially integrated.
This research has frequently emphaSized structural fea-tures of social rela~onships, such as the size and prox-imity of one's social network (e.g.. whether one is marriedor liVing alone. whether one has a close confidant; numberof close friends or relatives and frequency of contact withthem). Notably less concern has been given to the emo-tional texture and depth of such social relations, althoughlimited questions about emotional support are sometimesincluded (e.g.., Berkman, Leo-Summer~. & Horwitz, 1992;Glass Br Maddox. 1992). The nature 01 the emotions thatactually constitute suCh emotional support is rarely elab-orated.
There are nonetheless separate lite$tures dealing withintimacy, attachment, marital intera~on, and pa:rent-child relations. wherein the emotionaf texture of key so-cial relationships is extensively probed (e.g., Berscheid &Reis, .1998; Carstensen. Gottman, & LQvenson, 1995; Car-stensen, Graff, Levenson, &; Gottman. 1996; Cassidy &Shaver. 1999; Fitness, 1996; Fitness & Fletcher, 1993; Ha-zan &: Shaver. 1994: Reis &: Patrick, )996; Ryff, Si,nger,Wing, &: Love, 2001). These ~endas t, however, rarelyconnected to studies of health (Ryff &: Singer, 2000). ,

11086 PART X. EMOTION A~D H~lTH
tional featilres of key social ilnteractions and their atten-dant neurophysiological und~innings.
gender discrimination) with passive coping responses(e.g.. keeping quiet and accepting treatment) were 4.4times more likely to have self-reported hypertension thanAfrican-American women whose coping techniques weremore active. The links between the emotional reactions toracism. coping styles. and subsequent health sequelae inthe immune system and stress-induced neuroendocrineresponses (see Clark et al., 1999) constitute important di-rections for future inquiry. cO
Our objective in including racism as an illustration ofthe importance of assessing what emotions are about un-derscores the need to anchor affective experience in thechallenges, sometimes chronic, of individual lives. We:posit that these are what elicit powerful, and frequentlyrecurrent. human emotions. It is the purported intensityand persistence (both subject to empirical scrutiny) thatmakes these affective experiences relevant starting pointsfor building bridges to health outcomes .via diverse neu-roph ysiological mechanisms.
Although our emphasis has been on emotions aboutracism, we note that such inquiry has broader relevance.Gallo and Matthews (1999), for example, have proposedthat negative emotions (specifically, depression, hopeless-ness, anxiety. hostile attitudes, and affect) may medi~tethe association between socio&conomic status and health.Thus, it is not ethnic/racial status, but rather social in-equalities, even among minority groups, that are conse-quential for health. Carroll et al. (1997) also emphasize thelinks between socioeconomic status, hostility, and bloodpressure reactions to mental stress.
Finally. underscoring the high prevalence of perceiveddiscrimination in the general U.S. population and itsstrong associations with mental health, Kessler, Mickel-son, and Williams (1999) argue that perceived discrimi-nation needs to be taken much more seriously in futurestudies of stress and mental health~ The perception thatone has been discriminated against is, we submit, ~ ex-perience prompting significant, perhaps powerful; emo-tional response.
Premise II. Health Requires a Focus onCo-Occurrence of Discrete Emotions
Dimensional and Categorical Models of Emotion
Emotions of Oppression: The AffectiveExperience of Racism
A second illustration draws on broader social structuralinfluences on affective experi~nce, a realm largely missingin current studies of emotion. Here we c°IJ;sider the emo-tions associated with being a member of a group that issocially denigrated and deni~ fair opportunities in life.These are the feelings.tied to the experience of racism. Anemergent literature is exploring the stress associated withracism and its biopsychosociat sequelae (Clark. Anderson,Clark. & Williams, 1999). ~can Americans are dispro-portionately exposed to environmental stimuli that aresources of stress (chronic and acute). and they have ahigher prevalence of hyperten~ion and all-causemortalitythan do Caucasians of comparable levels of education(pappas, Queen, Hadden, &: Fi$her. 1993). While such dif-ferences may reflect an unequal distribution of wealth,they are also likely linked to differential exposure to stres-sors like racism and unfair treatment (Krieger. 1990; Wil-liams. Yu. Jackson, &: Anderson. 1997). Perceived racialdiscriminationt we note, has also been investigated withother ethnic minority groups. such as Southeast Asian ref-ugees (Noh, Beiser, Kaspar. H()u. &: Rummens, 1999).
Numerous responses may follow the perception thatone has been subjected to racis~, such as anger, anxiety.frustration, fear, helplessness-hopelessness, paranoia, andresentment. The ways in whi~ African Americans copewith anger-the affective state most commonly reportedto follow perceptions of racism-have been related to car-diovascular reactivity and re~ting blood pressure (Arm-stead, Lawler. Gorden. Cross. &: Gibbons. 1989; Johnson &:Browman, 1987). Investigating the efficacy of general cop-ing strategies as moderators of perceived racism. Armsteadet al. (1989) found that as outward expression of angerincreased. blood pressure levels decreased after viewingracist video scenes, Other re$ponses to racism includesuppression of anger and use of alcohol. or other sub-stances to blunt angry feelings (Armstead et al., 1989).Chronic feelings of helplessness or hopelessness mayevoke depression and other feelings of frustration, r~sent-ment, and distrust, themselves leading to maladaptive.health behaviors (overeating. passivity. avoidance).
Recent work by McNeilly et al. (1996) outlines a broadrange of emotional and coping responses to racism andmethods for measuring them. One hypothesis is that overtime, chronic perceptions of ~cism coupled with morepassive coping may lead to frequent increases in and pro-longed activation of sympathetic functioning. resulting inhigher resting systolic blood pressure levels. Krieger(1990) found that African-Amencan women (more than 45years old) who responded to ~air treatment (racism and
Those who study affect give considerable attention tostructural questions. such as whether positive and nega-tive affect are best construed as ind"ependent or bipolardimensions (e.g.. Diener, Smith. & Fujita. i995; Russell &Barrett. 1999; Watson et aI., 1999; Yik et aI., 1999). andthe extent to which measurement error obscures under-standing of these questions (Green, Goldman. & Salovey.1993; Green et aI.. 1999). Comparison of multiple models(e.g.. Barrett & Russell. 1998; Larsen & Diener. 1992; Wat.

~APTER 57, THE ROlf OF EMOT...ON ON PATHWAYS TO POSITIVE HEALTH 1087
u"
son &: Tellegen, 1985; Thayer. 1989) reveals a convergentemphasis on tWo dimensions of valence (positive and neg-ative) and two dimensions of activation (high and low).With differing positions as to where to place the axes inthis dimensional space (Russell &: Barr$tl. 1999).
Juxtaposed with such dimensionallnodels are modelsof discrete or basic emotions. which fo~ on distinguish-able (by their facial signals, temporal profiles. presence inother primates) features of anger, fear. sadness. enjoyment,disgust, surprise, and possibly contempt, shame, guilt, em-barrassment. and awe. The question thus arises as towhether those who study links between emotion andhealth "are best served by dimensional or discrete models.Wat$on and Pennebaker (1989) advocated a dimensionalmodel, arguing ili;at a substantial body of data show pos-itive correlations between measures of negative affect andreports of somatic symptoms. with the further suggestionthat this correlation is independent of various component$(anxiety, depression. anger) constituting the affective pole.Leventhal and Patrick-Miller (1993) challenged this posi-tion. arguing that'it is essential to disaggregate the negativeaffect pole. Differential models do a better job of account-ing for changes in symptomatology over time (e.g.. de-pression sh,ows a positive association with increases insymptoms, but anxiety does not).
Additionally. Leventhal and Patrick-Miller (1993)pointed out that differential negative affect$ are necessaryto understand the mediation of stress-disease relation-ships. Although measured in different ways. hostility isimplicated in the long-term development of atherosclero-sis leading to coronary occlusions and increased proba-bility of acute coronary events during environmentalcrises (see Matthews, 1988; Smith. 1992). Depression.however. is not predictive of coronary disease (Matthews,1988), although depression, hopelessness-helplessness.re-pressive cop~ style. and deficient social support havebeen associated with cancer outcomes. such as cancer di-agnosis, patient prognosis at time of diagnosis. rate of can-cer recurrence, years survived, and pati~t mortality (Con-trada. Leventhal. &; O'leary. 1990). Dl1awing on animalmodels, Leventhal and Patrick-Miller (1~93) offer possibleformulations of physiological mechanisms: Helpless ani-mals show depletion of brain norepinephrine and activa-tion of the hypothalamic-pituitary-adrenal axis. resultingin release of corticosteroids in the bloodstream. with thelatter linked to increased growth of imp{anted tumors, de-creased T -lymphocyte proliferation. and decreased naturalkiller (NK) cell activity.
As these summaries indicate, legitimate argument$ canbe made for bringing both dimensional ~d discrete mod-els of emotion to the study of health. To some extent, how-ever, the dichotomy itself is problematic. That is. dimen-sional approaches cover wide territory. but for healthpurposes. they reduce affective experience to overly ge-neric component$ (e.g., feeling good or bad, feeling
aroused or unaroused) that may be of limited value forprobing differentiated responses to fundamental life-tasks.Alternatively, discrete models offer greater focus on dif-ferentiated emotional states, but lack scope regarding alarger panoply of responses that may ensue from engage.-ment in life challenges. Thus, what may be critical forhealth outcomes is a third alternative-namely, the co-occUn'ence of discrete emotions. Further. recalling ourprior emphasis on what gives rise to emotion in the courseof living, we suggest that few significant experiencesprompt only single emotions or can be adequately cap-tw'ed by only two dimensions (valence and activation).
Racism, for example, likely prompts a constellation ofaffective experiences that include diverse emotions-an-ger, fear, resentment, perhaps along with sadness andhopelessness (see prior discussion of Clark et al., 1999).Alienation, a likely component of discrimination, itself in-volves multiple feelings; including the sense of power-lessness, social isolation, normlessness, and lack of mean-ing (Seeman, 1959. 1975). Moreover, different individualslikely have different combinations of these negative re.-sponses, and these variations can be empiriCally exploitedby assessing co-occurring discrete emotions.
Simila,rly, emotions about significant others (spouse,chIldren, parents), when they are positive. may involvelove, affection, pride; intimacy, security. Fredrickson(1998) argues that love involves a fusion of many positiveemotions, the combination of which broadens the scopeof thought and action as well $S b\illds personal, social,and physical resources. Alternatively, negative family dy-namics may involve combinations of hostility, bitterness,and anger, or despair, detachment, and .loneliness, withdiffering configurations haVing different physiological se.-quelae. Miller, Dopp. Myers, et at. (1999), in studying mar-ital conflict, found that displays of anger in husbands highin cynical hostility were associated with greater elevationsin systolic and diastolic blood pressure, cortisol, and in-creases in natural killer cell numbers and cytotoxicity,whereas for men low in cynical hostility, anger was asso-ciated with smaller increases in heart rate and naturalkiller cell cytotoxicity. None of women's affect scores wererel~ted to cardiovascular. neuroendocrine, or immuno-logic outcomes. leading the authors to suggest that otheremotions (e.g., sadness) may be more relevant for wives'physiological responses. Finally, the affective experienceof illness (e.g., cancer, heart disease) may also involveblends of discrete emotions (fear, anger, sadness combinedwith heightened levels of intimacy and connection-seeSpiegel &: Kimerling, 2001).
Thus, a key reason for attending to co-occurring affec-tive responses to life challenges is that they provide moreaccurate rendering of the subjective experiences-theemotional phenomenology-prompted by fundamentallife-tasks. A second reason relates to mapping the neuro-physiological ,mechanisms on the route to health and the

1088 PAR.T X. EMOTION AND ~EAlTH
argument that more differentiated assessment of subjectiveexperience will provide greater precision in understand-ing individual differences in th~ neural substrates anddownstream endocrinological ~d immunological se-quelae of emotion. (See Premise ~ on the phenomenologyand physiology of emotion for ~er elaboration of thispoint).
recent family dynamics. new developments in the stockmarket. or the weather. Similarly, laboratory studies of af-fective style may inflate profiles of dispositional differ-ences as a function of the standardized ~nature of thestim\ili employed. Such standardization is. of course, nec-essary to draw meaningful conclusions across respon-dents. but it may at the same time mask the variabilityevident in emotional reactivity to challenges of daily life.
From the health van~e point. stable, traitlike affectivedispositions are nonetheless likely to be of consequencein the recurrence, or chronicity. of emotional experienceand its neurophysiological subs~tes. The above obser-vations do not dispute this point; rather, they underscorethe need to attend to what emotions are about in the in-terest of better discerning those who are, and are.not, sta-ble in their affective responses.
Premise III. Health Is Biopsychosocial inNature and Requires Integration ofPhenomenoiogy and Neurophysiology
What of Emotional Dispositionsand Affective Style?
Our advocacy for the stu<!y of co-QCc~g discrete emo-tions, anchored in fundamental life tasks, may seem atodds with the emerging evidence of the links between per-sonality traits and affect, sUch as neuroticism and negativeaffect, or extraversion and positive affect (Emmons &; Di-ener, 1985; Watson &; Clark, 1992), or dispositional opti-mism (Scheier &; Carver, 1992), characterizations of affec-tive style (Davidson, 1998). Collectively, theseformulations emphasize the stable, recurrent ways inwhich individuals experience affeCt and respond to stim-uli from the environment. From this perspective, a focuson co-occurring discrete emotions may seem empiricallyun~eldy and even unnecessary. Knowledge of an indi-vidual's characteristic way of reacting to life challengesmay be all that is required, thereby obviating the need formore tedious assessment of diverse, person-specific com-binations of affective response to life tasks.
To this issue we bring insight £rom another re8lm re-garding the question of whether personality is stable orchanging (Block, 1982). Drawing on years of longitudinaldata. Block empirically documented that some individualsare stable in their personality profiles over time and othersare not. Given established connections between person-ality and affect, it is likely that in the affective realm, someindividuals will similarly show stable, dispositional affec-tive profiles. while others will reveal more affective vari-ability, depending on the life challenges confronted. Map-ping detailed emotional responses to different tasks willthus be fundamental to distinguish between the two.
Parenthetically. this observation rai~es the question asto whether prior claims that emoti()nal responses are dis-positional and traitlike have been premature. Why mightthis ~ the case? At the level ofself-teport, studies of affectvariability (Watson &; Walker, 1996) and related argumentsfor the traitlike nature of intra-indiVidual variability in af-fect (Eid &; Diener, 1999) may overstate the case for stabil-ity by virtue of the free-floating assessmen,ts of affect. Thatis, respondents are not asked to report their subjectivefeelings about anything, but rather to indicate how oftenthey felt particular emotions at particular temporal inter-vals. For some, this may be a particularly difficult task,given that on a specific day, or at aspecifi~ moment, onemight have a host of different feelings depending onwhether they were about the current situation at work,
From multiple vantage points comes the argument that hu-man health is fundamentally a matter of interacting bio-logical and psychosocial processes. In the field of psycho-somatic medicine, Engel'~ (1977) biopsychosocial modelof illness emphasized interacting systems at cellular, tis-sue, o~anismic, interpersonal, and environmental levels.SimilarJy, Liposki (1986; see also Fava, 1999a) defined thescope of psychosomatic medicine as a scientific disciplineconcerned with the study of the relationships of biologi-cal, psychological, and social determinants of health anddisease; Fava and Sonino's (2000) history of the psycho-sQmatic field clarifies its dramatic growth in recent de-cades, now spanning numerous realms at the interlace ofbehavioral science, basic biology, and clinical medicine.They underscore the leitmotif of this work-namely, thatthe mind and body are two inseparably linked aspe9t5 ofhealth that, although distinguished for methodologicaland communicative purposes, require integrated points ofobservation.
Within clinical medicine, Engel (1998) also under-stood, with remarkable depth and eloquence, that the phy-sician, as scientist, must operate concurrently in tWomodes. one observational, the other relational. The obser-vational mode is where data are collected in the classicalempirical-analytic approach with its emphasis on carefulmeasurement and accurate description. The relationalmode. however, requires attending to the human realm. inwhich language. symbols, thoughts, and feelings are themeans by which private experience is organized and com-municated. "It is through dialogue that the physicianlearns the nature and history of the patient's experiencesand clarifies on the one hand what they mean for the pa-tient, and on the other, what they might mean in terms of

1089QiAPTER 57. THE ROlE OF EMOTION ON PATHWAYS TO POSITIVE HEALTH
cluded subjective experience from the core Characteristicsthat distinguish basic emotions on the grounds that "toolittle is known about how subjectivity maps on to otheraspects of an emotional experience" (p. 175). This line ofreasoning and related Criticisms, or dismissal, or self-reported emotion, are problematic for the study of humanhealth. which requires attending simultaneously to phe-nomenology an,d neurophysiology. Accordingly, we ex-amine below the issues revolving around self-reportedemotion. underscoring its essential role in the processlinking the psychosocial realm to health. in addition. wecall for explicit examination of points of convergence anddiscrepancy between the felt experience of emotion andund~rlying neurophysiological substrates. The fit. or lackthereof, between these two constitutes a critical nexus forunderstanding individual differences in how emotion in-fluences health. Further. the juxtaposition of the phenom-enology and neurophysiology offers important opportu-nities to understand how one side might afford protectivefeatures to offset the vulnerabilities of the other.
The Perils of Self-Reported Affect
Despite the fact that much of the work on the structure ofthe affective domain has been conducted with self-reportmeasures (Watson et al., 1999; Yik et al., 1999), recurrent.criticisms plague these data. The call to "move beyondself-report data in exploring the structure of affect" (Di-ener, 1999, p. 804) reflects concerns with self-report bi-ases, motivational influences, and the fact that languagedoes not always capture affective experience (Cacioppo etal.. 1999; Green et al., 1999). Thus. individuals are viewedas unreliable reporters pf their own affect because theyengage in distortion (conscioUs or unconscious). some-times responding carelessly or randomly. or even not ac-tually knowing (or remembering) how ~ey feel, or felt.
Those who study emotion via language only furthercomplicate matters. English emotion words have been de-scribed as falling into 25 categories of synonymS (Shaver.Schwartz, Kirson. &: O'Connor, 1987). This taxonomy hasbeen used to probe emotion nomenclature universals inmajor geographical.and linguistic groupings (Hupka. Len-ton. &: Hutchison. 1999). Four basic linguistic emotion cat-
Iegories were identified-the first. pertaining to categoriesof anger and guilt (which exist in all languages); the sec-ond to categories of adoration, alarm, amusement, and de-pression (which also exist in all languages); the third tocategories of alienation. arousal. and agony; and the fourthto the category eagerness. Many of these linguistic basics(e.g.. guilt. adoration, alienation. agony) are. we note.missing in current self-report instruments of affect.
In addition to the linguistic parsing of affective space. in-dividualdifferences in language use, r~ferred to as linguisticstyles, have also been put forth as an independent and mean-ingful way to study personality (Pennebaker &: King, 1999).
other systems in the natUral hierarchy, be they biochemi-cal and physiological, or psychological and social" (p. 8).Engel's wisdom was in understanding that the two modesconstitute, not separate alternatives, but a single, inte-grate'd means for data disclosure, clarification, and inter-
pretation.Among those studying health from more mechanistic,
biological cornel'S there is also recognjjtion that phenom-enology and physiology must ultimately be linked. WalterCannon (194Z), using observations from other cultures andcenturies, clarified that the experience of fear can, in itself,induce death. Selye (1956) emphasized enVironmentalstressors that produce a disease-prod~cing adaptationalsyndrome, with subsequent researchers elaborating widevariability in the extent to which environmental changesare appraised as threatening or stressful (FolkInan et al.,1986; Pearlin, Lieberman, Menaghail, 8r. Mullan, 1981;Thoits, 1995). Recently, the concept of allostatic load(McEwen, 1998; McEwen 8r. Stellar, 1993; McEwen & See-man, 1999) has been described as the price paid by thebody for chronic overactivityor underactivity of multiplephysiological systems (autonomic, HPA axis, cardiovas-cular, metabolic, and immune). Central to the formulationof allostatic load is the interpretation of and reaction tolife challenge as benign or threatening. That is, while pri-mary emphasis is given to the intera<rting physiologicalsystems that constitute the response to I::hallenge, the pro-cess begins with the perception of the cliallenge-a pivotaljuncture that determines, depending on the construal,whether physiological systems Will be activated.
In the field of affective science, Davidson (1998) alsodraws attention to "one of the most striking features ofhuman emotion" (p. 307), which is the variability acrossindividuals in the quality and intensity of dispositionalmood and emotional reactions to similar incentives andchallenges. He then elaborates features of "affective style"to organize these individual differences. Parameters of af-fective chronometry include: threshold for reactivity, peakamplitude of response, rise time to peak, and recoverytime. These neural substrates are core components of emo.,tion regulation and are consequential for understandingwhat underlies, at the level of brain function, psychopa-thology. Activation of these responses begins with subjec-tive experience-sometimes conscious, other times not,sometimes expressed in words, other times in behavior(e.g., the face) and physiology (e.g., heart rate). Probing thephenomenology of how individuals e~erience their lifechallenges is thus essential to understand what sets thischronometry in motion.
Parenili.etically, it is useful to recall that the emotionfield has not always been receptive to the phenomenolog-ical realm as a fundamental part of its purview. E~mAD(1992) acknowledged that "the subjective experience ofemotion, how each emotion feels, is for some at the centreof what an emotion is'~ (P. 175), but he nonetheless ex-

1090 PART X. EMOTION AND ~EAlTH
1983). Moreover, when asked, retrospective questionshave typically been comparative (e.g., how would you rateyour happiness/life satisfaction now compared to fiveyears ago?).
For present purposes, the central question is the extentto whiCh such data (whether based on current, global, orretrospective reports) are plagued by distortion. Remark;.ably little research has actually documented the scope ofthis problem. Note that studies showing the variability ofwell-being depending on external factors, suCh as whetherit is a rainy or sunny day, or whether the. individual is ina pleasant or unpleasant room (Schwarz &: Strack, 1999),are not in themselv~s evidence for the fallibility of self-reported subjective states, but rather may be testimony tofinely tuned human capacities for discerning subjectivestates. Nonetheless, some have advocated for the use ofinforDlant reports or aggregated daily emotion reportS(Diener, Smith, &: Fujita, 1995) to address potential bias,while others have focused on behavioral assessments (e.g.,facial expressions of emotion). Kahneman, as noted above,'calls for measures based in neurophysiology. There aredifficulties, however, with each alternative. Regarding theuse of informants, the major challenge is deciding what todo when there are discrepancies, whiCh frequently occurs,between the targeted respondent and his or her inforDlant.Who to believe in such cases-whose report is to be takenas true? Obs~rvational tools are extremely valuable, butsome emotional experiences (e.g., love, despair, aliena-tion) may not have clear facial or behavioral displays.Moreover, many core life challenges involve co-occurringemotions. Other biologically based measures su1fer fromthe same conundrum as inforDlant reports-namely, whatto do when the measures inside the skin. or brain, do notsquare with self-reported states? What, in such contexts,constitutes the true measure of the affective state-whatpeople say they feel, or what the EEG readings show?
We raise these diverse questions to underscore thepoint that there is no single.. final arbiter of affective ex-perience. Human emotion is both internal and external,phenomenolo~cal and physioiogical-.-both are ultimatelyrequired to capture the phenomena. Moreover, the two arejointly needed to clarify the significance of the other.Whatever their failings, self-report measures have been,and will continue to be, essential to validate newly emer-gent assessments of affect on the biolo~cal side. Kahne-man, in fact, noted that for the brain-based measures {)fmomentary affect to work they would need to be highlycorrelated with subjective reports. Less hypothetically, Da-vidson and colleagues (Davidson, 1998; Sutton &: David-son, 1997; Tomarken, Davidson, Wheeler, &: Doss, 1992)have dramatically advanced the interpretive significanceof asymmetric prefrontal activation by showing that left-frontally activated people report more positive and lessnegative affect than their right-frontally activated counter-parts, and similarly that those with greater left-sided pre-
That is, people verbally express themselves in stable andunique ways. This observation raises the fuither wrinklethat structured, self-report inventoties of affect may not in-clude the tenns spontaneously selected by individuals todescribe their feelings, thus forcingtatings on a host oftennsthat may exist outside an individual's linguistic style. Evenif individuals choose similar terms to describe their feelingsas those on self-report instruments, there is the additionalquandary of not knowing whether particular words meanthe same thing tQ different individu~.
Given these difficulties, it is not surprising that at-tempts to build knowledge of emotion on a foundation ofwords {the affective tower of Babel?) are greeted with sus-picion. Some argue for alternative approach9s to the as-sessment of subjective states, such as measures of "objec-tive happiness" (Kahneman, 1999, 2000), which seek tominimize the biases of self-report. Using the example of"How happy was Helen in March?" Kahneman argues thatHelen's retrospective judgment is a "fallible estimate ofher objective well-being" (1999, p. 4), which is contrastedwith objective happiness defined as the cumulative record'of "instant utility" (i.e., being pleased or distressed at aparticular moment) over the relevant perjod of time.
This bottom-up construction -of happiness requires that.~omentary experiences be characterized on a good/bad di-mension. Kahneman further suggests that a promising ap-proach to the measurement of this dimension may reside inneuropsychology and the psychophysiology of affect:
It is conceivable. if not likely. that a compositephysiological measurement of the good/bad re-sponse could eventually be constructed. and thatthis measurement would be quite highly correlatedwith subjective experience of pleasure and distress.Continuous records of affective State could possi-bly be derived from non-invasive measures of lo-calized brain activity eventually leading to accu-rate assessments of well-being over time. Themovement from science fiction to practical applica-tion is likely to be rapid in this domain. (1999.p.10)
Regarding the fallibility of Helen's retrospective ac-count of her happiness in March. we note that the priorfield of subjective well-being has r$rely, if ever. been in-terested in recalled accounts of pdcular prior momentsor periods (see Diener. 1984; Diener, Suli,Lucas, &; Smith.1999; Veroff. Douvan. &; Kulka. 1981). The self-reportquestions that constitute this realm pertain to how indi-viduals feel now. or how they feel generally. The formercannot suffer from retrospective bias because they are notretrospective. Global or general assessments are also notretrospective, although some individuals may draw onpast feelings to make such judgments. or others may beinfluenced by current mood states (Schwarz &; Clore,

CHAPTER 57. THE ROLE OF EMOTION ON PATHWAYS 10 POSITIVE HEALTH 1091
frontal activation report more behavioral activation (rela-tive tQ behavioral inhibition) compared to those exhibitingmore right-sided prefrontal activation. Measures of pre-frontal asymmetry also predict reactivity to elicitors ofemotion-those with more left-sided prefrontal activationat baseline report more positive affect to positive filmclips. while those with more right-sided activation re-ported more negative affect to the negative film clips(Wheeler. Davidson, &: Tomarken, 1993).
Thus. across these studies, it is the correspondence be-tween the reported states (via self-report instruments) andthe electrical signals in the brain that ate key to advancingunderstanding of the neural subsqates of affective vulner-ability or affective strengths. In fact. it. is not possible tomake senSe of the affective system at the biolQgicallevelwithout showing meaningful connections at the level ofsubjectively experienced and reported emotion. The co-nundrum is that the two levels rarely perfectly match.Thus, it is the discrepancies between the self-reportedstates and the biological indicators that are cause for con-cern. It is to these that we now turn.
Probing the Discrepancies BetweenSelf-Reported Affect and Biology
physiologically costly, and further show thai those with il-lusory mental health have greater Goronary reactivity tolaboratory tasks than those with genuine mental health.The point we draw attention to is that the biological (heartrate) measures are essential to distinguish betWeen the twotypes of self-reported mental health. That is, distortion oftrue subjective states becomes evident via the nexus withphysiology. Similarly, Weinberger, Schwartz, and David-son (1979) ~robed the phenomenon of repression (experi-encing little anxiety on a conscious level but adopting ahighly defensive approach to life) by juxtaposing self-reported levels of anxiety and social desirability withphys-iological measures of arousal.
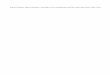
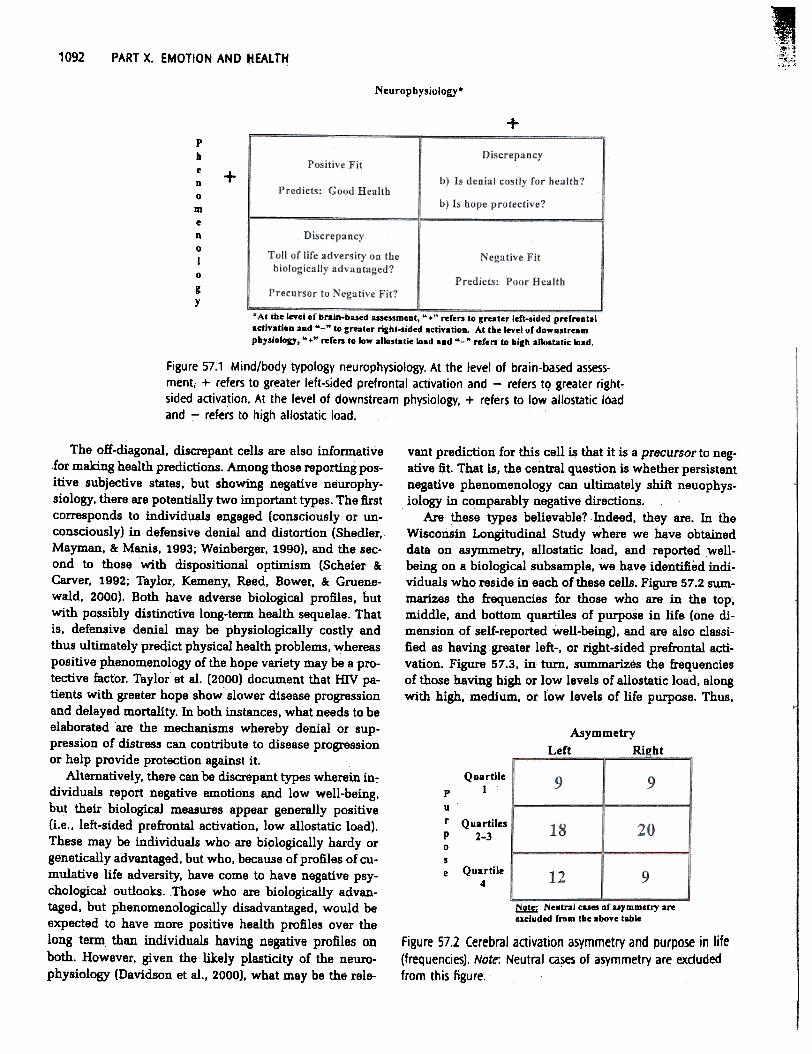
Alternatively, it is useful to consider the possible jux-taposition of those who have biological (perhaps genetic)predispositions to show greater right-$ided prefrontal ac-tivation (Davi!ison, 1998) in response to environmentalstimuli, but who have psychosocial strengths and gener-ally positive phenomenology. A useful question in this in-stance is whether these compensating influences on thepsychosocial side afford protective benefits offsetting oth-erwise adverse downstream consequences (endocrinolog-ical, immunological). To push forward scientific agendasthat follow from the convergence or divergence of phe-nomenology and neurophysiology, we present the cross-classification summarized in Figure 57.1. This two-by-twoscheme illustrates various mind/body types for whichuseful predictions regarding health outcomes can bemade. The rows of the table make a distinction betweenthose showing generally positive versus negative profilesat the phenomenological (sell-report) level; the columnspertain to distinctions between positive versus negativeprofiles at the neurophysiological level. We consider ce-rebral activation asymmetry from the work of Davidson,with its distinctio.ns between greater left (+) versus right(-) activation (Davidson, 1998; Sutton.\; Davidson, 1997)as an example of brain-based assessment, while distinc-tions between low (+) versus high (-) levels of allostaticload (McEwen &; Stellar, 1993; Seeman, Singer, Rowe, Hor-witz, &: McEwen, 1997) serve as instances of downstream
physiological processes.The convergent cells, positive and negative fit, corre-
spond to those whose phenomenology and physiologymatch at equivalently valenced levels. These constitutethe most straightforward cases from which to make pre-dictions about health, with the positive subjective states,greater left-sided activation. and low allostatic load con-stituting amind/body integration, described as positive fit,which predicts positive health outcomes (resistance to dis-ease, delayed onset of disease, quicker recovery fromacute health challenges). Alternatively, negative fit refersto those with the configuration of negative phenomenol-ogy, greater right-sided activation, and high allostatic load,which is predictive of poor health (vulnerability to mental
and physical pathology).
When phenomenological and neurophysiological data donot line up, what does it mean? We sugsest that it is usefulto make distinctions between discrepancies that are theresult of measurement problems, on either, or both sides,and discrepancies that are meaningful and substantive.Larsen and Fredlickson (1999) provide a compre~nsiveoverview of the reliability and validity of numerous tech-niques (self-report, observer ratings, facial measures, au-tonomic measures, brain-based measures, vocal mea-sures). These issues are consequential; Green, Goldman,and Sillovey (1993) showed that claims that positive andnegative affect are independent were obscured by me~-surement error that, once taken into account, revealed abipolar structure. We concur with Larsen and Fredricksonthat the emotion field is advanced by increased emphasison simultaneous use of multiple measures. As notedabove, much of the validation of assessments in one realm(self-report, behavioral, autonomic, brain-based) requiresshowing convergence with the others.
Nonetheless, there are instances in which the self-reportdata do not square with the neurophysiological measures,and the discrepancy is meaningful. In fact, we submit thatthe degree of "fit" between these two levels may be a usefuldimension of individual differences in affective experi-ence. For example, one instance of poor correspondencepertains to the situation in which the individual, via $elf-report. puts forth a strongly positive evaluation, but clinicaljudgments suggest otherwi$e. Shedler, Mayman, and Manis(1993) refer to this as the "illusion of mental health." Theyargue that the defensive denial of diSb:ess is, however,
-~".\1092 PART X. EMOTION AND ~EALTH
Neurophysiology.
+PbeD0meD0I0
gy
+
. At the level or brain-based assessmeat, "." reren to greater left-sided prerroataladiyatiea aad "-" te greater right-sided actiyatieD. At the level of do..astreamphysiology, "." ref en to 10.. allostatie load and "-" refen to high anGst-tic load.
Figure 57.1 Mind/body typology neurophysiology. At the level of brain-based assess-ment, + refers to greater left-sided prefrontal activation and - refers tQ greater right-
sided activation. At the level of downstream physiology, + refers to low allostatic loadand - refers to high allostatic load.
vantprediction for this cell is that it is a precursor to neg-ative fit. That is, the central question is whether persistentnegative phenomenology can Ultimately shift neuophys-iology in comparably negative directions.
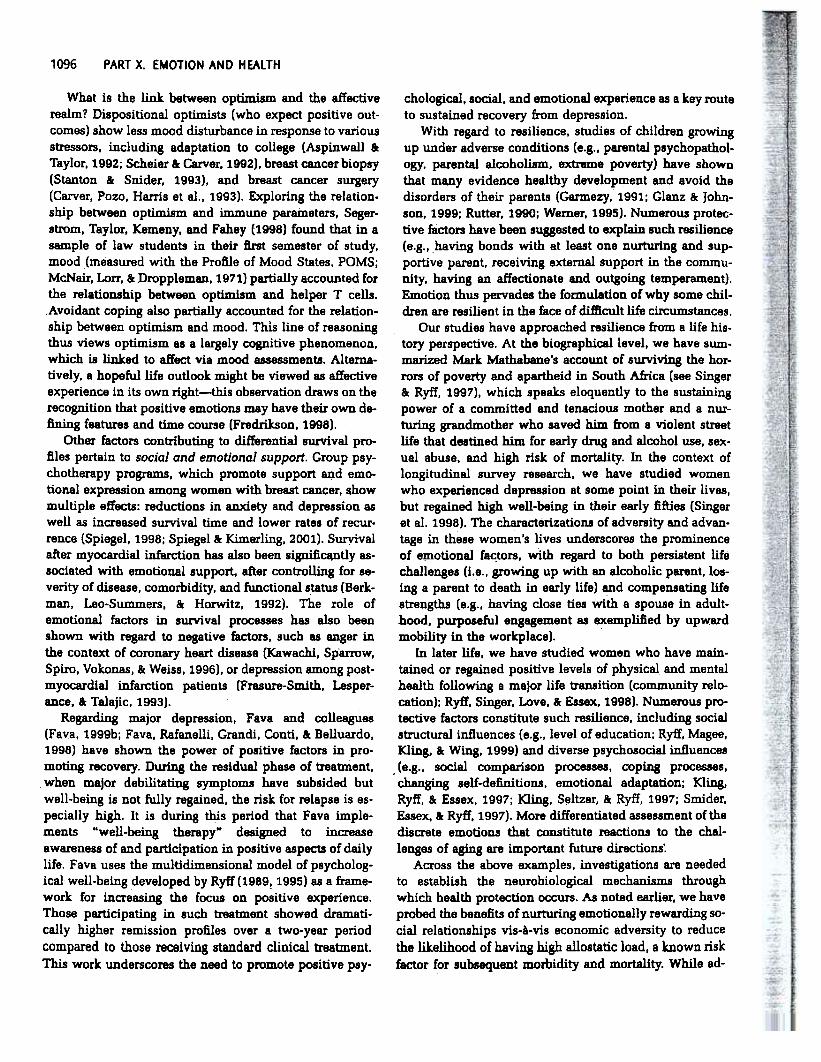
Are these types believable? Indeed, they are. In theWisconsin Longitudinal Study where we have obtaineddata on asymmetry, allostatic load, and reported well-being on a biological subsample, we have identified indi-viduals who reside in each of these cells. Figure 57.2 sum-marizes the frequencies for those who are in the top,middle, and bottom quartiles of purpose in life (one di-mension of self-reported well-beingJ, and are also classi-fied as having greater left-, or right-sided prefrontal acti-vation. Figure 57.3. in turn, summarizes the frequenciesof those having high or low levels of allostatic load, alongWith high, medium, or low levels of life purpose. Thus,
AsymmetryRiebtLeft
The off-diagonal, discrepant cells are also infomlative.for making health predictions. Among those reporting pos-itive subjective states, but showing negative neurophy-siology. there are potentially two important types. The firstcorresponds to individuals engaged (consciously or un-consciously) in defensive denial and distortion (Shedler,Mayman, &: Manis, 1993; Weinberger, 1990), and the sec-ond to those with dispositional optimism (Scheier &:Carver, 1992; Taylor, Kemeny, Reed, Bower, &: Gruene-wald, 2000). Both have adverse biological profiles, butwith possibly distinctive long-tenn health sequelae. Thatis, defensive denial may be physiologically costly andthus ultimately predict physical health problems. whereaspositive phenomenology of the hope variety may be a pro-tective factor. Taylor et al. (2000) document that mv pa-tients with greater hope show slower disease progressionand delayed mortality. In both instances, what needs to beelaborated are the mechanisms whereby denial or sup-pression of distress can contribute to disease progressionor help provide protection against it.
Alternatively, there can be discrepant types wherein in7dividuals report negative emotions and low well-being,but their biological measures appear generally positive(i.e., left-sided prefrontal activation, low allostatic load).These may be individuals who are bi910gically hardy orgenetically advantaged, but who, because of profiles of cu-mulative life adversity. have come to have negative psy-chological outlooks. Those who are biologically advan-taged, but phenomenologically disadvantaged, would beexpected to have more positive health profiles over thelong term than individuals having negative profiles onboth. However, given the likely plasticity of the neuro-physiology (Davidson et al., 2000). what may be the rele-
Quartilep 1
ur Quartilesp 2-30se Quartile
4
~ Neutral cases of alymmetry areexcluded from tile above table
Figure 57.2 Cerebra! actiyation asymmetry and purpose in life(frequendes). Note: Neutral ca.se5 of a~mmetry are exdudedfrom this figure.

~HAPTER 57. THE ROLE-OF EMOTION ON PATHWAYS TO POSITIVE HEALTH 1093
purp0se
Figure ~7.3 Allostatic load and purpose in 1ife (frequencies).
the convergent types are evident, but discrepancies arealso part of the empirical reality. Longitudinally, our ob-jective is to track the health predictions following fromthe preceding typology. The work underscores the impor-tance of constructing life pathways that simultanepuslymonitor what is occurring phenomenologically. and neu-rophysiologically, as the different combinations may, pro-vide routes to understan~ variation m health trajecto-ries ~ugh time.
Premise IV. Cumulative, Chronic EmotionsAre Consequential for Health
perception of emotion-eliciting qualities of events, andeven emotional episodes that are not prototypical"(p. 805). Despite this pervasive and long-standing empha-sis on emotions of brief duration, we suggest that the link-age to health requires a shift to a different time scale. Thatis, what is consequential for health are those features ofaffective experience of long duration: prolonged moodstates and emotional dispositions, and more important,chronic, recurrent emotions and their cumulation overtime. Why does a focus on health call for this temporalshift? Prim8rlly, it is. because" the neurophysiologicalmechanisms that are the nexus between the emotional eX-perience and health outcomes will be chronically, or re-peatedly, activated. It is this physiological wear "and tearthat is hypothesized to be costly for the organism. To il-lustrate these ideas, we slImma:rlze an emerging p~o~of research on the topic of allostatic load and its connec-tion to emotion via assessment of cumulative relationship
profiles.Allostatic load is derived from the concept of allostasis,
which captures at the biological level the capacity of theorganism to adapt to oncoming challenges and therebyprevent the unfolding of pathophysiological processes(Sterling &: Eyer, 1988). Emphasis is on the dynamism ofinternal physiology and the fact that healthy functioningrequires ongoing adjustments and adaptations to the in-ternal physiological milieu. Throu~ allostasis, the auto-nomic nervous s~m, the hypothalamic-pituitary-adrenal (HPA) axis, the cardiovascular, and metabolicsystems protect the body by responding to internal andexternal stress. The long-term price of overactivity or un-deractivity of these systems is referred to as allostatic load(McEwen &: Stellar, 1993), representing th~ cumulativewear and tear from chronic stress. Allostatic load has beenoperationalized with multiple indicators from the abovesystems. including blood pressure. waist-hip ratio, totaland HDL cholesterol, glycosylated hemoglobin, cortisol,epinephrine: norepinephrine, and DHEA-S (Seeman;Singer, Rowe, Horwitz, &: McEwen, 1997}.
Allostatic load has been shown in longitudinal researchto predict incident cardiovascular disease and later lifedeclirie in physical functioning and memory loss (Seemanet al., 1997). Recent findings over a 7.S-year period furthershow that high allostatic load was predictive of subse-quent mortality (Seeman, McEwen, Rowe, .\; Singer, 2001).Such fuidings document the linkage from this multiple-system construct to morbidity and mortality. The questionon the other side of the equation is, What contributes to,or protects one from, high allostatic load? We hypothe-sized that social relational experiences-in particular theemotional features of key significant relationships (i.e.,parents, spouse)-and their cumulation over ~e wouldcontribute to differences in allostatic load: with those onmore negative relationship pathways more likely to havehigh load than those on more positive re!ationship path-
To date, much of the field of affective science has focusedon momentary, short-term emotions. Ekman (1992), infact, defined basic emotions in part by their temporal pro-files-namely, that they have quick onset and brief dura-tion. He algued that it is adaptive for .the organism to beable to mobilize quickly and for such mobilization to notlast very long. "If one emqtion-arousing event typicallyproduced a set of response changes which endure forhours regardless of what was occurring in the externalworld, emotion would be less responsive than I think theyare to rapidly changing circwnstances" (p. 185). EkmA~further distinguished emotions from moods, which last forhows or days, noting that moods are "highly saturatedwith one or another emotion-irritability with anger, dys-phoria with sadness, apprehensiveness with fear, euphoriawith a type of enjoyment" (p. 186). S~tes that endure forweeks or months were not moods, however, but moreproperly identified as affective disorders (E-iI:!!:!-an, 1994).Significantly, enduring positi.ve feelings (e.g., love) wereomitted from this classification scheme.
The persistent emphasis on emotion as brief experienceis illustrated by Russell and Barrett's (1999) formulationof prototypical emotional episodes, which are "limited totemporary events and slices in time. We omit tempera-ment, attitudes, sentiments, emotional dispositions of anykind, prolonged mood states, psychiatric symptoms, sim-ple evaluative responses, perception of emotion in others,

PART X: EMOTION ANO HEALTH1094
'CC0
(J';:c-...2";.cCI:c-c-CGJ(J...GJ
D..
Figure 57.4 Social relationship pathways and allostatic load
hold income in childhood and/or adulthood. Those withpersistently low economic profiles had greater likelihoodof high allostatic load compared to those with persistentlyhigh economic profiles. although the differences were notstatistically significant. When cumulative relationshipprofiles were combined with economic data, clear patternsemerged. Specifically. those with economic disadvantagein childhood and on the negative relationship pathwaywere significantly more likely to have high allostatic loadthan those with economic advantage in childhood and onthe positive relationship pathway. illustrating the protec-tive role of good social relationships. we aiao found thatthose with economic disadvantage in childhood but per-sistently positive social relationships were also signifi-cantly less likely to have high allostatic load than thosewith similar economic beginningA but negative relationalexperiences. These findings underscore the possible so-cioemotional routes through which health resilience vis-A-vis life challenge is achieved.
The above findings represent but one attempt to linkcumulative emotional experience to a composite of phys-iological mechanisms implicated in later life morbidityand mortality. They also illustrate the use of more person-centered analytic methods (Singer. Ryff. Carr. &: Magee.1998). which may be critiCal in establishing biopsychc>-social models of health. Typological. person-centeredanalyses are. we note. of groWing interest in the behavioralsciences (Be~. 1998; Magnus8on.1998; Robins. John.&: Caspi. 1998). There are. in addition. numerous impor-tant avenues for extending these preliminary results. Atthe level of the emotional experience. there is need forimproved measures that probe the relevant depths of sig-nificant social ties. We drew on the lives of famous cou-ples (i.e.. Leo and Sonya Tolstoy. Elizabeth Barrett Brown-ing and Robert Browning. Freida Kahlo and Diego Rivera)to illustrate the texture and detail required to capture thelived experience of emotion (both positive and negative)with significant others (see Ryff. Singer. Wing. &: Love.
2001).
ways. This formulation illustrates the need to focus onemotions that are about something as well u the impor-tance of tracking recurrent, cwnulative profiles of emo-tion.
These questions were ~~~ed in the context of a lon-gitudinal study of midlife adults (Ryff, Singer, Wing, &.Love, 2001). For a biological subsample of members of theWisConsin Longitudinal Study on whom meuures of al-lostatic load were obtained, we created relationship path-ways based on self-reported usessments of quality of re-lationships with mother and father (in childhood) andwith spouse in adulthood. The Parental Bonding Scale(Parker, Tupling, I: Brown, -1979) probes multiple aspectsof caring and warmth in the mother/child and father/childbond (e.g., "S/he was affectionate to me. S/he spoke to mewith a warm and friendly voice. S/he seemed emotionallycold to me. S/he frequently smUe.d at me. S/he made mefeel I wasn't wanted."). For adult. spousal relationships,four different aspects of intimacy were assessed with thePersonal Assessment of Intimacy Relationships' (PAIR,Schaefer &. Olson, 19811. The emotional and sexual sub-scales included the most intimate fonus of connection be-tween spouses, while the intellectual and recreationalsubscales emphasized mutually enjoyed experiences,companionship, and the scope of shared communication.
We defined the individual to be on a negative relation-ship pathway if she or he had large negative evaluationsof both mother and father in childhood and/or had largelynegative evaluations of emotional/sexual and intellectual/recreational ties to spouse. The majority of those who ex-perienced negative childhood ties (both men and women)also reported negative spousal ties. We defined an indi-vidual to be on a positive pathway if she or he rated atleast one parent as caring and reported at least one com-bined category of intimacy (emotional/sexual; intellecb18l/recreational) with spouse.
Using a sample of 101 midlife adults (4~ women, 55men), we found that, indeed, those on the negative rela-tionship pathway were significantly more likely to havehigh allostatic load than those on the positive relationshippathway (see Figure 57.4). The effects were stronger formen than women, but nonetheless supported the guidinghypothesis in both cases. In a subsequent analysis (Singer&. Ryfi, 1999), the potentially protective features of persis-tently good social relationships vis-A-vis life adversity wuexamined. The targeted life challenge wu economic dis-advantage. Drawing on the growing interest in the healthconsequences of socioeconomic inequalities (see Adler etal., 1994), we hypothesized that persistent economic dis-advantage would increue the likelihood of high allostaticload, thereby illuminating possible mechanisms in theSE5-health link..
Again, with the WLS biological subsample, diverse eco-nomic pathways were constructed depending on whetherrespondents were above or below the median on house-

,CHAPTER 57. JHE ROLE OF EMOTION ON PATHWAYS TOPOSIT/VE HEALTH 1095
work is the likely bidirectionality between affective re-sponses and illness behavior or disease.
Emphasis on the adverse consequences of negativeemotion neglects the potentially consequential influencesof emotion on positive health promotion (Ryff &. Singer,1998a, 1998b, 2000, 2O01). Salubrious psychosocial fac-tors, such as having good-quality relations with others ora sense of engagement and purpose in one's life, may becentral contributors to the "physiological substrates offlourishing" that. in turn. help maintain the optimal hu-man functioning of the organism. New interest surroundsquestions of what it means to thrive (Ickovics &. Park,1998} and what the possible benefits are of positive emo-tions (Fredrickson, 1998). Our final pr.emise thus is thatemotion can, in fact. be protective and promote positivehealth.
We divide this section into three parts. The first ex-amines extant research on recovery and resilience, prob-ing the extent to which emotion (phenomenologically andneuropnysiologically) may be a part of the story. The sec-ond addresses positive health promotion and the extent towhich emotional experience can be protective, aiding inthe prevention or delay of mental and physical healthproblems. The third section considers the "intermingling"of positive and negative emotion in understanding optimalmental and physical health. The argument is that goodhealth does not ensue from simplistic models whereinpositive emotions are maximized and negative emotionsminimized. Rather, optimal functioning' requires refinedformulations of how the two wQrk beneficially together.
At the level of interveniDgbiological mechanisms, wealso underscored the need to examine brain oxytocin.opioids. and prolactin systems as key participants in ex-periences of social solidarity, warmth. and nurturance.Oxytocin. in particular; has been shown to increase in re-sponse to the onset of pair-bonding in adults, maternalattachment, infant attachment. maternal responsivity. pos-itive social behaviors or contact. onset of sexual beha\lior.and exploration or approach to novelty (Carter. 1998;Panksepp. 1998a; Uvnas-Moberg. 1998). As an underscoreto the theme of cumulative effects, social bondS lead torepeated exposures to positive social stimuli and. thereby.to repeated release of oxytocin (Uvnas-Moberg. 1998). Inhumans. such positive experiences can be stored in mem-ories. which in themselves may reactivate physiologicalprocesses. Pertinent to health outcomes. evidence fromanimal models further suggests that chronic oxytocin re-lease is capable of producing long-term reductions inblood pressure and heart rate (Petersson. Alster. Lunde-berg. 8c Uvnas-Moberg. 1996). Such findings point to a hostof new research directions at the human level.
Finally. while our focus on the health significance ofcumulative emotional experience has been elaboratedwith a focus on social ties. we emphasize the need to ex-tend this formulation to a wider realm. Chronic emotionalexperience in the workplace. where most hours of the dayare spent. constitutes one important domain. Occupa-tional stress has, of course. been linked to physical andmental health Oackson 8c Warr. 1984; Link. Lennon. 8cDohrenwend. 1993; Lundberg. 1999; Karasek.. Baker.Maixer. Ahlbom. 8c Theorell. 1981), but the emotional fea-tures of work. life (e.g.. feeling harassed. demeaned. orchronically criticized on the job; feeling energized and en-gaged by work. demands; worrying about hazardous workconditions) are not well understood. Our prior emphasison emotions associated with racism and discriminationare another direction for probing prominent and likelypersistent feelings of daily life that may be consequentialfor health.
The Rote of Emotion in Recovery and Resilience
Mounting evidence points to the importance of optimismand hope in the face of health challenge. Positive expec-tations have been shown to predict better health after hearttransplantation (Leedham. MeyerQwitz. Muirhead. &:Frist.1995). and optimists show more rapid recovery from cor-onary bypass surgery and have less severe anginal painthan pessimists (Fitzgerald. Tenn. Aftleck. &: Pransky.1993). In the HIV model.1>ptimism predicts disease courseand mortality. HIV men who were asymptomatic and didnot have negative expectations showed less likelihood ofsymptom development in the follow-up period (Reed. Ke-meny. Taylor. &: Visscher. 1999). Importantly. HIV menwith unrealistically optimistic beliefs about their own sur-vival actually lived longer (Reed. Kemeny, Taylor. Wang.&: Visscher. 1994). Moreover, those who were able to findmeaning in their loss of a close partner maintained CD4 Thelp cells over the follow-up period and were less likelyto die (Bower, Kemeny. Taylor, &: Fahey. 199B). Thus. op-timism, hope, and meaning emerge as resources that maypreserve not only mental but also physical health (Scheier&: Carver. 1992; Taylor. Kemeny. Reed. Bower. &: Gruene-
wald. 2000).
Premise V. Emotion Can Be Protective andPromote Positive Health
Extensive prior emphasis has been given to the linksbetween emotion and illness (see Leventhal &; Patrick-Miller, 1993). The topic of how anger, anxiety. dysphoricaffect and depression. and hopelessness-helplessness con-tribute to dysfunction of various biological systems and.thereby, to disease has constituted a large segment of thescience to date. Moreover, the pathways through whichaffective disturbances influence physical disorders havebeen inqreasingly specified (Cohen &. Rodriguez. 1995).These pathways include biological. behavioral. cognitive.and social processes. An important message in current
1096 PART X. EMOTION AND HEALTH
What is the link between optimism and the affectiverealm? Dispositional optimists (who expect positive out-comes) show less mood disturbance in response to variousstressors. including adaptation to college (Aspinwall &:Taylor. 1992; Scheier &: Carver. 1992). breast cancer biopsy(Stanton &: Snider, 1993), and breast cancer surgery(Carver. Pozo. Harris et al.. 1993). Exploring the relation-ship between optimism and immune parameters. Seger-strom. Taylor. Kemeny. and Fahey (1998) found that in asample of law students in their first semester of study,mood (measured with the Profile of Mood States, POMS;McNair. Lorr. &:Droppleman.197'1) partially accounted forthe relationship between optimism and helper T cells._Avoidant coping also partially accounted for the relation-ship between optimism and mood. This line of reasoningthus views optimism as a largely c~tive phenomenon.which is linked to affect via mood assessments. Alterna-tively, a hopeful life outlook might be viewed as affectiveexperience in its own right-this observation draws on therecognition that positive emotions may have their own de-fining features and time course (Fredrikson. 1998).
Other factors contributing to differential survival pr0-files pertain to social and emotional support. Group psy-chotherapy programs. which promote support ~d emo-tional expression among women with breast cancer. $howmultiple effects: reductions in anxiety and depression aswell as increased survival time and lower rates of recur-rence (Spiegel. 1998; Spiegel &: Kimerling. 2001). Suryivalafter myocardial infarction has also been signifi~tly as-sociated with emotional support. after controlling for se-verity of disease. comorbidity. and functional status (Berk-man, Leo-Summers. & Horwitz. 1992). The role ofemotional factors in survival processes has also beenshown with regard to negative factors. such as anger inthe context of coronary heart disease (Kawachi. Sp"arrow,Spiro, Vokonas. & Weiss. 1996). or depression among post-myocardial infarction patients (Frasure-Smith. lesper-ance. &: Talajic. 1993).
Regarding major depression, Fava and colleagues(Fava, 1999b; Fava. Rafanelli. Grandi, Conti. & Belluardo,1998) have shown the power of positive factors in pro-moting recovery. During the residual phase of treatIIient,when major debilitating symptoms have subsided butwell-being is not fully regained. the risk for relapse is es-pecially high. It is during this period that Fava imple-ments "well-being therapy" designed to increaseawareness of and participation in positive aspects of dailylife. Fav&. uses the multidimensional model of psycholog-ical well-being developed by Ryff (1989, 1995) as a frame-work for increasing the focus on positive experience.Those participating in such treatment showed dramati-cally higher remission profiles over a two-year periodcompared to those receiving standard clinical treatment.This work underscores the need to promote positive psy-
chological, social, and emotional experience as a key routeto sustained recovery from depression.
With regard to resilience, studies of children growingup under adverse conditions (e.g., parental psychopathol-ogy. parental alcoholism, extreme poverty) have shownthat many evidence healthy development and avoid thedisorders of their parents (Garmezy, 1991: Glanz & John-son, 1999: Rutter, 1990; Werner, 1995). Numerous protec-tive factors have been suggested to explain such resilience(e.g., having bonds with at least one nurturing and sup-portive parent, receiving external support in the commu-nity, having an affectionate and outgoing temperament).Emotion thus pervades the formulation of why some chil-dren are resilient in the face of difficult life circumstances.
Our studies have approached resilience fram a life his-tory perspective. At the biographical level, we have sum-marized Mark Mathabane's account of surviving the hor-rors of poverty and apartheid in South Africa (see Singer& Ryfi. 1997). which speaks eloquently to the sustainingpower of a committed and tenacious mother and a nur-turing grandmother who saved him from a violent streetlife that destined him for early drug and alcohol use, sex-ual abuse, and high risk of mortality. In the context oflongitudinal survey research, we have studied womenwho experienced depression at some point in their lives,but regained higl-1 well-being in their early fifties (Singeret al. 1998). The characterizations of adversity and advan-tage in these women's lives underscores the prominenceof ePlotional factors, with regard to both persistent lifechallenges (i.e., growing up with an alcoholic parent. los-ing a parent to death in early life) and compensating lifestrengths (e.g.. having close ties with a spouse in adult-hood. purposeful engagement as exemplified by upwardmobility in the workplace).
In later life, we have studied women who have main-tained or regained positive levels of physical and mentalhealth following a major life transition (community relo-cation); Ryff. Singer. Love. a: Essex. 1998). Numerous pro-tective factors constitute such resilience. including socialstructural influences (e.g.. level of education; Ryff, Magee.Kling. a: Wing. 1999) and diverse psychosocial influences
. (e.g.. social comparison processes, coping processes,changing self-definitions. emotional adaptation; Kling.Ryff. & Essex. 1997; Kling. S~ltzer. &. Ryff. 1997; Smider,Essex. &: Ryff, 1997). More differentiated assessment of thediscrete emotions that constitute reactions to the chal-lenges of aging are important future directions:
Across the above examples. investigations are neededto establish the neurobiological mechanisms throughwhich health protection occurs. As noted earlier. we haveprobed the benefits of nurturing emotionally rewarding so-cial relationships vis-A.-vis economic adversity to reducethe likelihood of having high allostatic load, a known riskfactor for subsequent morbidity and mortality. While ad-

~APTER57. T~e ROlf OF EMOTION OH PATHWAYS TO posITIve HEALTH 1097
verse outcomes, particularly under conditions of high risk..have been avoided, what is unknown is whether suchavoidance represents a reversal of neurophysiological sys-tems, or compensatory responses, or both. In Animal mod-els, ,those reared in emotionally impoverished environ-ments have been shown to react to stress more radicallythroughout their lives than those reared in enriched en-vironments (Caldji et al., 1998). However, these effectshave been shown to be reversible-those exposed to In-adequate nurturing in early life can, if subsequently rearedby a high licking and grooming foster mother, show nor-mal functioning and healthy adult lives. What these mod-els offer is critically needed understanding of how suchbehavioral interventions regulate the development of neu-ral systems.
Emotion in Health Promotion and Prevention
have been heavily weighted on the side of relational con-flict and dysfunction as risk factors for behavioral, mental.and physical health problems. In the prior section on whatemotions are about (see Premise I). we reviewed findingsthat are mapping the physiological sequelae of maritalconflict, a richly expanding area of inquiry. The counter-part agenda (i.e.. mapping the physiological substrates ofrelational flourishing) has received dramatically less atten-tion. The emotional upside of significant social ties andhow they impact health is thus a major priority for future
inquiry.It is animal models, particularly studies of positive af-
filiation (Carter, 1998; Panksepp, 1998a) that may lead theway with regard to the neurobiology of relational flourish-ing. Animal attachment can be operationalized as selec-tive socioemotional bonds. and thus facilitate observationand experimentation connecting these bonds to physio-logical substrates. A review of caregiver-infant and adult-heterosexual pair bonds revealed recurrent associationsbetween activity in the HPA aXis and expression of socialbehaviors. Central ~europeptides, especially oxytocin andvasopressin, are implicated in social bonding and socialinteraction. Uvnas-Moberg (1997. 1998; Petersson et al.,1996) suggests that oxytoctn may mediate the benefits ofpositive social interaction on health. Oxytocin levels ~raised by somatosensory stimulation (e.g., breast-feeding,suckling) as well as touch and warm temperatures. In bothmale and female rats, oxytocin exerts potent antistress ef-fects, such as decreases in blood pressure, heart rate, andcortisol levels, with effects lasting from one to severalweeks. Viewed over the long term, and underscoring ourtheme of cumulation, social bonds lead to repeated ex-posure to positive social stimuli and~ thereby, repeated re-lease of oxytocin. And, as we noted earlier, such positiveexperiences in humans may be stored in memories, whichin themselves may reactivate these physiological pro-cesses.
Further innovative avenues for lin,king positive expe-rience, particularly of the relational variety, to health per-tain to interest in nerve growth factors (Panksepp, 1998b)and the anabolic growth-promoting hormones that em-body thriving (Epel, McEwen, &: Ickovics, 1998) and helpmaintain or repair the body. At the behavioral level, thereis also much room for expanding the positive focus.Laughter and humor-significant social and emotional ex-periences-may have important health-promoting sub-strates, as Norman Cousins (1979/1995) advocated sometime ago. We would also underscore the need for ex-panded emphasis on what Solomon (1993) referred to asthe "passions"-those central, defuling goals and pursuitsof our lives. "Our passions are not the animal intrusionsand physiologically based disruptions that they have al-ways been thought to be" (p. xiv). Rather, our passions arethe very sources of our interests, meaning, and purposes-"
With regard to positive health promotion, we reiterate theimportance of optimism and hope as well as social andemotiqnal support. Optimjsts and minimally anxiousadults have been shown to have lower ambulatory bloodpressure and more positive moods than pessimistic andanxious adults (Raikkonen, Matthews, Flory, Owens, 8r:Gump, 1999). Individuals growing up with feelings ofwarmth and closeness. with parents had, 35 years later.decreased incidence of diagnosed diseases in midlife (cor-onary artery disease, hypertension, duodenal ulcers. al-coholism (Russek 8r: Schwartz, 1991). Earlier we summa-rized epidemiological studies that have mappedcontributions of the social ties and integration to host re-sistance. reduced morbidity, and delayed mortality (Berk-man. 1995; Cassel, 1976; Cohen, Doyle. Skoner. Rabin, 8r:Gwaltney, 1997; House et al., 1988).
Elsewhere we have juxtaposed the extensive literatureson the health benefits of good social supports with theextensive literatures on attachment. close and personal re-lationships, and marital quality (Ryff 8r: Singer. 2000,2001). What is notable is the missing interchange betweenthese realms. Those in the social support arena have beenexplicitly concerned with health outcomes and, as such.have contributed advances regarding social influences onmorbidity and mortality. Extant assessments of socialre-lationships, however, have not probed the depths of rela-tional flourishing, particularly emotional features-what it.means to have loving, intimate. ful:filling. and enjoyableties to others (Ryff 8r: Singer. 2000). Alternatively. socialrelationship researchers who probe early and later life at-tachments and close personal relationships. includingmarital and family ties. elaborate some features of deep,meaningful. loving human connection. but these agendasare rarely connected to health.
Moreover, when social relationship researchers haveprobed the health significance of key social ties, inquiries

1098 PART X. EMOT10N ANq HEAltH~.~"they are the high court of consciousness to which all else,
even reason, must pay tribute" (p. xvii). Advances in af-fective neuroscience, especially interest in " approach-
related affect" (Davidson et al., 1990), add further impor.tance to bringing human passions, purposes, and pursuitsinto the phenomenology and neurophysiology of positivehuman health. These constitute an especially promising,and possibly health-promoting, realm of what emotionsare abqut (see Premise I). .
~~
~=0
ISalutogenesis and the Intermingling ofPositive and Negative Emotion
]~
At first glance, it appears that optimal health, the processof which Antonovsky..(1987) referred to as salutogenesis,would be nurtured by an abundance of positive emotionalexperiences and a dearth of negative. Numerous lines ofinquiry challenge the simplistic notion that positive emo-tions heal and negative emotions are pathogenic (Dafter,1996). We briefly highlight multiple realms of study thatfocused instead on how positive and negative emotionswork fruitfully together.
Gottman (2001) argues that negative emotions are a fun-damental part of "healthy" social relationships. He distin-guishes between "emotion-coaching" versus "emotion-dismissing" parents, which characterizes the emotionalstyles they bring to the task of rearing children (Gottman,Katz, &: Hooven, 1996). A major difference between thetwo parenting types is their distinctive modes of respond-ing to children's negative emotions, such as. anger, sad-.ness, or fear. Emotion-coaching parents.help children un-derstand and label their own negative affect, whichcontributes, in Gottman's view, to the child's developing.sense of control and optimism, and more generally, to ef-.fective emotion regulation. Emotion-dismissing parents, incontrast, equate such emotions with selfishness, loss ofcontrol, passivity, cowardice, and failure. From ~e healthangle, Gottman suggests that children with emotion-coaching parents have higher vagal tone that conveysgreater capacity for self-clilming after emotional upset.Such children were reported to have fewer infectious ill-nesses compared to children with emotion-dismissing par-ents. Thus, the emotion-coaching parent sees negative af-fect as sometimes legitimate and even valuable, because itprovides an opportunity for intimacy and/or teaching,which in turn can strengthen the bond between parent andchild.
Further emphasis on the interface of positive and neg-ative emotion comes from studies of naturally occurring,day-to-day social interactions within frameworks of at-tachment and intimacy (Berscheid &; Reis, 1998; Reis &;Patrick, 1996; Sheldon, Ryan, &: Reis, 1996). The guidingassumption is that emotional well.being follows from thenourishment one obtains from daily social contact withothers. Reis (2001) argues that intimacy interactions are
those in which self-disclosure occurs and there is a part-ner responsiveness to such disclosure. This can be, andfrequently is.'in the context of difficult. negative, painfultopics, including relational conflict. Whi1e conflict may beaffectively unpleasant. Reis underscores that it does notnecessarily undermine satisfaction ofrelatedJ;1ess needs. Itis meaningful, not unifonnly positive, social ties that pro-mote emotional well-being. These are nurtured by how in-dividualS cope constructively with negative emotion andrelationship conflict. Indeed. as Gottm~ emphasizedabove, difficult or conflictual interactions may, paradoxi-cally, be instrumental in generating enhanced closeness.Reis's work is valuable for illUminating, at the microana-lytic level, the nature of social interactions that accom-plish these ends.
Another example pertains to group psychotherapy withcancer patients (Spiegel. 1998). These interventions pro-mote social support and emotional expression. Patientsare encouraged to access, express. and work through theiremotional reactions to the stresses of cancer. Suppressionof emotion reduces intimacy in families and social net-works, limiting opportunities for direct expression of af-fection and concern' (Spiegel & Kimerling, 2001). Impor-tantly, emotional expression decreases psychiatric and. physical sYmptoms, reduces medical visits. and is linked
with enhanced immune response and decreased viral rep-lication. Much of this expression is about negative or trau-matic events, and the prospect of dying. It is the intermin-gling of tears and laughter in dealing with trauma of thedisease, in families that have adopted an atmosphere ofopen and shared problem solVing, that helps reduce anx-iety and depression, and thereby possibly influencing be-havii:lral and biological pathways of survival.
Fredrickson (1998) also emphasizes how positive emo-tions may undo the aftereffects of negative emotions. Thatis, positive emotions are efficient antidotes that may re-store autonomic quiescence following negative emotionalarousal. Eliciting positive emotions by films or markedsmiles, Fredrickson and Levenson (1998) show that posi-tive emotions speed recovery from the cardiovascular af-tereffects of fear, anxiety. and sadness. Further. Folkman(1997) underscores the importance of positive mean:ingsand emotion in coping with severe stress (e.g.. caregiving,bereavement). Coping theory, she underscores, has beenoverly focused management of distress and thus over-looked the consequential roles of positive psychologicalstates in dealing with life challenges. Finally, an extensiveliterature is emer~g on possible health benefits of emo-tional disclosure-that is. expressing (typically via writ-,ingJ feelings about past traumatic experiences (Cameron &;
Nicholls, 1998; Kelley. Leisen. &; Lumley, 1997; Penne-baker &; Beall, 1986; Pennebaker. 1995).
Taken as a whole, the above findings converge on the
important message that negative emotion is not singularlybad for health, but rather it is how negative emotion is

CHAPTER 57. THE ROLE OF EMOTION ON PATHWAYS TO POSmVE HEALTH
expressed and responded to that arbitrates its deleteriousor beneficial effects. Positive emotion is deeply entangledin such processes. both as an antidote to negative feelingsand as a consequence of working through (frequently withsignificant others) difficult emotions. Thus. it is the natureof how positive and negative emotion are entwined that iscritic~ for future h~alth research.
Conclusion
How emotion makes its way to health outcomes is, webelieve, well conceptualized via the metaphor of a path-way. The reason is that numerous kinds of infonnationmust be put together to understand how human feelingscome to be consequential for mental and physical illness,or well-being. We have emphasized that a critical ~e-dient of what goes on this pathway is what emotions areabout-:-that is, the fundamental life challenges that giverise to affective experience. With regard to the feelingsthemselves, we call for greater emphasis on co-occurringdiscrete emotions as a route to sh~ening understandingof what life tasks prompt within us. Capturing the emo-tional experience itself is, we argue, unavoidably aboutthe need to blend phenomenology and neurophysiology.Alllioughemotion has largely been construed as a short-term phenomenon, we proposed that building linkages tohealth requires focus on recurring, cumulative emotionalexperience. Finally, because far more is known about. howemotion undermines health and well-being, we advocatefor a counterpoin.t agenda that clarifies the protective andhealth-promoting features of salubrious affective experi-ence.
REFERENCESAdler, N. E., Boyce, T., Chesney, M. A., Cohen,S., Folk-
man,S., Kahn, R L., &: Syme, S. L. (1994). Socioeco-nomic status and health: The challenge of the gradient.American Psychologist, 49, 15-24.
Antonovsky, A. (1987). Unraveling the mysteries of health:How people manage stress and stay well. San Fran-cisco, CA: Jossey-Bass Publishers.
Armstead, c. A., Lawler, K A., Gorden, G., Cross, J., &:. Gib-bons, J. (1989). Relationship of racial stressors to bloodpressure responses and anger expression in Black col-lege students. Health Psychology, 8, 541-556.
Aspinwall, L. G., &: Taylor, S. E. (1992). Individual differ-ences, coping, and psychological adjustment: A longi-
, tudinal study Qf college adjustment and performance.Journal of Personality and Social Psychology, 63, 989-1003.
Barrett, L. F., &:. Russell, J. A. (1998). Independence and bi-polarity in the structure of affect. Journal of Personalityand Social Psychology, 74, 967-984.
Bergman, L. R (1998). A pattern-oriented approach tostudying individual development. In R. B. Cairns, L. RBergman, &:. J. Kagan (Eds.), Methods and models for
studying the individual (pp.83-122). London: SagePublications.
Berkman, L. F. (1995). The role of social relations in healthpromotion. Psychosomatic Medicine, 57, 245-254.
Berkman, L. F., .a.. Breslow. L. (1983). Health and ways ofliving. New York: Oxford University.
Berkman, L. F., Leo-Summers, .L., &: Horwitz, R. I. (1992).Emotional support and survival after myocardial in-farction. Annals of Internal Medicine, 117. 1003-iO09.
Berscheid, E., &: Reis, H. T. (1998). Attraction and closerelationships. In D. T. Gilbert. S. T. Fiske,- &: GI Lindzey(Eds.), Handbook of social psychology (Vol. 2, 4th ed.,pp. 193-281). Boston. MA: McGraw-Hill.
Block, J. (1982). Some enduring and consequential struc-tures of personality. In A. I. Rabin, J. Aronoff, A. M.
. Barclay, &: R. A. Zucker (Eds.), Fwther explomtions inpersonality (pp. 27-43). New York: Wiley.
Bower. J. E.; Kemeny. M. E., Taylor. S. E., &: Fahey, J. L.(1998). Cognitive processing, discovery of meaning,CD4 decline, and AIDS-related mortality among be-reaved HIV seropositive men. Journal of Consultingand Clinical Psychology, 66, 979-986.
Cacioppo, J. T., Gardner. W. L., Berntson, G. G. (1999). Theaffect system has parallel and integrative processingcomponents: Form follows function. Journal of Person-ality and Social Psychology, 76, 839-855.
Caldji, C., Tannenbaum, B., Sharma, S., Francis. D., Plot-sky, P., &: Meaney, M. (1998). Maternal care during in-fancy regulates the development of neural systemsmediating the expression of fearfulness in the rat. Pro-ceedings of the National Academy of Sciences, 95,5335-5340.
Cameron, L. D. &: Nicholls, G. (1998). Expression of stress-ful experiences through writing: Effects of a self-regulation manipUlation for pessimi~ts 'and optimists.Health Psychology, 17, 84-92.
Cannon, W. (1942). Voodoo death. American Anthropolo-gist, 44, 169-181.
Carroll, D., Smith, G. D., Sheffield, D., Shipley, M. J.. &:Mannot, M. G. (1997). The relationship between socio-economic status, hostility, and blood pressure reactionsto mental stress in men: Data from the Whitehall nStudy. Health Psychology, 16, 131-136. .
Carstensen, L. L., Gottman, J. M., &: Levenson, R. W.(1995). Emotional behavior in long-term marraige.Psy-chology and Aging, 10, 140-149.
Carstensen, L. L., Graff, J., Levenson, R W., &: Gottman,J. M. (1996). Affect in intimate relationships: the de~velopmental course of Inarriage. In C. Magai &: S. H.Mcfadden (Eds.), Handbook of emotion, adult .devel-opment, and aging (pp. 227-247). San Diego, CA: Ac-ademic Press. .
Carter, C. S. (1998). Neuroendocrine perspectives on so-cial attachnient and love. Psychoneuroendocrinology,23, 779-818.
Carver, C.S., &: Scheier, M. F. (1990). Origins and func-tions of positive and negative affect: A control-processview. Psychological Review, 97, 19-35.
Carver, C. S., Pozo, C., Harris, S. D., Noriega, V., Scheier,M. F.. Robinson, D. S.. Ketcham. A. S., Moffat, F. L., Jr.,&: Clark. K. C. (1993). How coping mediates the effectof optimism on distress: A study of women with earlystage breast cancer. Journal of Personality and SocialPsychology, 65, 375-390. .
Cassel, J. (1916). The contribution of the social environ-

PART x. EMOTtONANDH~Lni1100
ment to host resistance. American Journal of Epidemi-ology, 104. 107-123.
Cassidy. J., &: Shaver, P. R. (1999). Handbook of attach-ment: Theory, research, and clinical applications. NewYork: Guilford.
Clark, R., Anderson. N. B., Clark. V. R.. Williams, D. R.(1999). Racism as a stressor for African Americans.American Psychologist, 54, 805-816.
Cae. C. L. (1993). Psychosocial factors and immunity innonhuman primates: A review. Psychosomatic Medi.cine, 55. 298-308.
Coe. C. L.. &: Lubach. G. R. (2001). Social context and otherpsychological influences on the development of im-munity. In C. D. Ryff &: B. Singer (Eds.J. Emotion, socialrelationships, and health (pp. 243-261). New York: Ox-ford University Press.
Cohen. S., Doyle. W..J., Skoner. D. P., Rabin, B. S., &: Gwalt-ney, J. M~ Jr. (1997). Social ties and susceptibility to the(::ommon cold. Journal of the American Medical Asso-ciation, 227, 1940-1944.
Cohen. S., &: Herbert, T. B. (1996). Health psychology: Psy-chological factors and physical disease from the per-spective of human psychoneuroimmunology. AnnualReview of Psychology, 47, 113-142.
Cohen, S.. &: Rodriguez, M. S. (1995), Pathways linking af-fective disturbances and physical disorders. HealthPsychology, 14. 374-380.
Contrada. R. J.. Leventhal, H.. &: O'Leary, A. (1990). Per-sonality and health. In L. A. Pervin (Ed.), Handbook ofpersona)ity: Theory and research' (pp. 638-669). NewYork: Guilford Press.
Cousins, N. (1979/1995). AnatoIily of an illness as per-ceived by the patient: Re.f1ections on healing and regen-eration. New York: W. W. Norton.
Dafter. R. E. (1996). Why "n~ative" emotions can some-times be positive: The spectrum model of emotions andtheir role in mind-body healing. Advances: The Journalof Mind-Body Health, 12, 6-51,
Darwin, C. (1998). The expression of the emotions in manand animals. New York: Oxford University Press. (Orig-
. inal published in 1872)Davidson, R. J. (1998). Affective style and affective disor-
ders: Perspectives from affective neuroscience. Cogni-tion and Emotion, 12. 307-330.
Davidson. R. J.. Ekman. P., Saron. C. D., Senulis, J., &: Frie-sen, W. (1990). Approach-withdrawal and cerebralasymmetry: Emotional expression and brain physiol-ogy. Journal of Personality and Social Psychology, 58,330-341. .
DaVidson, R. J., Jackson. D. C., &: Kalin. N. H. (2000). Emo-tion, plasticity. context, and regulation. PsychologicalBulletin, Special Millennium Issue, 126, 891-909.
Diener. E. (1984). Subjective well-being. PsychologicalBulletin, 95. 542-575. .
Diener, E. (1999). Introduction to the special section onthe structure of emotion. Journal of Personality and So-cial Psychology, 76. 803-804.
Diener, E., Sandvik, E.. Pavot. W., &: Gallaher. D. (1991).Response artifacts in the measurement of subjectivewell-being. Social Indicators Research, 20, 355-381.
Diener. E.. Smith. H., &: Fujita, F. (1995). The personalitystructure of affect. Journal of Personality and SocialPsychology. 69. 130-141.
Diener. E.. Suh, E.M., Lucas. R. E., &: Smith, H. L. (1999).Subjective well-being: Three decades of progress. Psy-chological Bulletin, 125. 276-302.
Bid, M., & Diener, E. (1999). Intr8individual variability inaffect: Reliability, validity, and personality correlates.Journal of Personality and Social Psychology, 76, 662-676.
Ekman, P. (1992). An argument for basic emotions. Cog-nition and Emotion, 6, 169-200.
Ekman, P. (1994). Moods, emotions, and traits. In P. Ekman& R. J. Davidson (Eds.), The nature of emotion: Fun-damental questions (pp. 56-59). New York: OxfordUniversity Press.
Emmons, R. A., & Diener, E. (1985). Personality correlatesof subjective well-being. Personality and Social Psy-chology Bulletin, 11, 89-97.
Engel, G. L. (1997). The need for a new medical model: AChallenge for biomedicine. Science, 196, 129-136
Engel, G. L. (1998). Introduction: How much longer mustmedicine's science be bound by a seventeenth centuryworld view? In G. A. Fava & H. Freyberger (Eds.) ,Handbook of psychosomatic medicine (pp. 1-21). Mad.ison, cf: Intefnactional Universities Press.
Epel, E. S., McEwen, B. S., & Ickovics, J. R. (1998). Em-bodying psychological thriving: Physical thriving iri re-sponse to stress. Journal of Social Issues, 54, 301-322.
Ewart, .C. K., Taylor, C. B., Kraemer, H. C., & Agras, W. S.(1991). High blood pressure and marital discord: Notbeing nasty matters more th~ being nice. Health Psy-chology, " 10, 155-163.
Fava, G. A. (1999a). Lipowski's legacy: The psychosomaticspirit. Psychotherapy Psychosomatics, 68, 1-2.
Fava, G. A. (1999b). Well.being therapy: Conceptual andtechnical issues. Psychotherapy and Psychosomatics,68, 171-179.
Fava, G. A., Rafanelli, C., Grandi, S., Conti, S., &; Bel-luardo, P. (1998). Prevention of recurrent depressionwith cognitive behavioral therapy. Archives of GeneralPsychiatry, 55, 816-821.
Fava, G. A., & Sonino, N. (2000). Psychosomatic medicine:Emerging trends and perspectives.. Psychotherapy Psy-chosomatics, 69. .
Fitness, J. (1996). Emotion knowledge structures in closerelationships. In G. J. O. Fletcher (Eds.), Knowledgestructures in close relationships: A social psychologicalapproach (pp. 195-217). Hillsdale, NJ: Erlbaum.
Fitness, J., &; Fletcher, G. J. O. (1993). Love, hate, anger,and jealousy in close relationships: A prototype and.co~tive appraisal analysis. Journal of Personality andSocial Psychology, 65, 942-958.
Fitzgerald, T. E., Tenn, H., Affleck, G., &; Pransky, G. S.(1993). The relative importance of dispositional opti-mism and control appraisals in quality of life after cor-onary artery bypass surgery. Journal of Behavioral Med-icine, 16,25-43.
Folkman, s. (1997). Positive psychological states and cop-ing with severe stress. Social Science and Medicine, 45,1207-1221.
Folkman, S., Lazarus, R. S., Dunkel-Schetter, C., DeLongis,A., & Gruen, R. J. (1986). The dynamics of a stressfulencounter: Cognitive appraisal, coping, and encounteroutcomes. Journal of Personality and Social Psychol-ogy, 50, 922-1003.
Frasure-Smith, N., Lesperance, M. D., & Talajic,M. (1993).Depression following myocardial infarction: Impact on6-month survival. Journal of the American Medical As-sociation, 270, 1819-1825.
Fredrickson, B. L. (1998). What good are positive emo-tions? Review of General Psychology, 2,300-319.

CHAPTER 57. THE ROLE OF EMOTION ON PATHWAYS TO POSITIVE HEALTH 1101
FredriCkson, B. 1., Levenson, R. W. (1998). Positive emo-tions speed recovery from the cardiovascular s~q\ielaeof negative emotions. Cognition and Emotion, 12,191-220.
Gallo, L. C. &. Matthews K. A. (1999), Do negative emo-tions mediate the association between socioeconomicstatus and health? Annals of the New York Acadeuzy ofSciences, 896, 226-245.
Garmezy, N. (1991). Resiliency and vulnerability of ad-verse de\telopmental outcomes associated with poverty.Behavioral Scientist, 34, 416-430.
Glanz, M. D., &. Johnson, J. L. (1999). Resilience and de-velopment: Positive life adaptations. New York: Ple-num.
Glass, T. A., &. Maddox, G. L. (1992). The quality andquantity of social support: Stroke recovery as psycho-social transition. Social Science and Medicine, 34,124g.;.1261.
Gottman, J. M. (2001). Meta-emotion; children's emotionalintelligence, and buffering children from marital con.flict. In C. D. Ryff &. B. Singer (Eds.), Emotion, socialrelationships, and health (pp. 23-40). New York: Ox-ford University Press.
Gottman, J.M., Katz, LF., &. Hooven, C. (1996). Parentalmeta-emotion philosophy and the emotional life offamilies: Theoretical models and preliminary data.Journal of Family PsychQlogy, 10, 243-268.
Green, D. P., Goldman, S.L., &. Salovey, P. (1993). Mea-surement error masks bipolarity in affect ratings. jour-nal of Personality and Social Psyr:;hology, 64, 102g.;.1041.
Green, D. P., Salovey. P., Truax, K. M. (1999). Static.. dy-namic, and causative bipolarity of affect. Journal of Per-sonality and Social Psychology, 76, 856-867.
Hazan, C., &. Shaver, P. R (1994). Attachment as an orga-nization framework for research on close relationships.Psychological Inquiry, 5, 1-22.
House, J. S.. Landis, K. R., &:. Umbers on, D. (1988). SocialrelatioQShips and health. Science, 241, 540-545.
Hupka, R B., Lenton, A. P., &. Hutchison, K. A. (1999).Universal development of emotion categories in naturallanguage. Journal of Personality and Social Psychology,77, 247-278'. .
lckoVics. J. R., &:. Park, C. L. (1998). Paradigm shift: Why afocus on health is important. Journal of Social Issues,54, 237-244. ,
Jackson, P. R., &:. Warr,' P. B. (1984). Unemployment andpsychological ill-health: The moderating rol$ of dura-tion and age. Psychological Medicine, 14, 605-614.
Johnson, E. H., &:. Browman, C. L. (1987). The relationshipof anger expression to health problems among Black'Americans in a national survey. Journal of BehavioralMedicine, 10. 103-116. ,
Kahneman, D. (1999). Objective happiness. In D. Kahne-man, E. Diener. &:. N. Schwarz (Eds.). Well-being: Thefoundations of hedonic psychology (pp 3-25). NewYork.: Russell Sage Foundation.
Kahneman, D. (2000). Experienced utility and objectivehappiness: A moment-based approach. In D. Kahneman&. A. Tversky (Eds.). Choices, values 6' frames (pp. 673-692). New York: Cambridge University Press and theRussell Sage Foundation.
Karasek, R., Baker, R., Marxer, F., Ahlbom, A., &:. Theorell,T. (1981). Job latitude, job demands and cardiovasculardisease: A prospective study of Swedish men. Ameri-can Journal of Public Health, 71,694-705.
Kawachi, I., Sparrow, D., Spiro, A., Vokonas, P., a: Weiss,S. T. (1996). A prospective study of anger and coronaryheart disease: The Normative Aging Study. Circulation,94, 2090-2095.
Kelley, ]. E., Leisen, J. C. C., a: Lumley, M. A. (1997).Health effects of emotional disclosure in rheumatoidarthritis patients. Health Psychology, 16,331-340.
Kessler, R. C., Mickelson,' K. D., Williams, D. R. (1999).The prevalence, distribution, and mental health corre-lates of perceived discriinination in the UmtedStates.Journal of Health and Social Behavior, 40, 208-230.
Kiecolt-Glaser, ]. K., Glaser, R., Cacioppo,]. T., Mac-Callum, R C., SnydersDiith, M., Cheongtag, K., 8c: Ma-larkey, W. B. (1997). Marital conflict in older adults:Endocrinological and immunological correlates. Psy-chosomatic Medicine, 59, 339-349.
Kiecolt-Glaser, ]. K., Newton, T., Cacioppo, ]. T., Mac-Callum, R. C., Glaser, R., 8c: Malarkey, W. B. (1996}. Mar-ital conflict and endocrine function: Are men reallymore physiologicallly affected than women? Journal ofConsulting and Clinical Psychology, 64, 324-332.
Kling, K. C., Ryff. C. D., a: Essex, M.]. (1997). Adaptivechanges in the self-concept during a life transition. Per-sonality and Social Psychology Bulletin, 23, 989-998.
Kling, K. C., Seltzer, M.M., 8c: RyffiC, D. (1997). Distinc-tive late life challenges: Implications for coping andwell-being. Psychology and Aging, 12, 288-295.
Knox, S. S., a: Uvnas-Moberg, K. (1998}. Social isolationand cardiovascular disease: An atherosclerotic path-way? Psychoneuroendocrinology, 23,877-890.
Krieger, N. (1990). Racial and gender discrimination: Riskfactors for high blood pressure? Social Science Medi-cine, 12,1273-1281.
Larsen, R. ]., a: Diener, E. (1992). Promises and problemswith the circumplex model of emotion.1n M. S. Clark(Ed:), Review of personality and social psychology:Emotion (Vol. 13, pp. 25-59). Newbury Park, CA: Sage.
Larsen, R. ]., 8c: Fredrickson, B. L. (1999). Measurement is-sues in emotion res.earch. In D. Kahneman, E. Diener,8i. N. Schwarz (Eds.). Well-being: The foundations afhe-donic psychology (pp. 40-60). New York: Russell SageFoundation.
Leedham, B., Meyerowitz, B. E., Muirhead, ]., 8c: Frist,M. H. (1995}. Positive expectations predict health afterheart transplantation. Health Psychology, 14, 74-79.
Levenson, R. W., Carstensen, L. L., a: Gottman. ]. M(1994}. The influence of age and gender on aff~t, phys-iology, and their interrelations: A study of long-termmarriage. Journal of Personality and Social Psychology,67,56-68.
Leventhal, H., Patrick-Miller, L. (1993}. Emotion and ill-ness: The mind is in the body. In M. LewiS, ]. M. Hav-iland (Eds.}. Handbook of emotions (pp. 365-379}. NewYork: The Guilford Press. .
Link, B. G., Lennon, M. C~, 8c: Dohrenwend. B. P. (1993}.Socioeconomic status and qepression: The role of oc-cupations Involving direction, control, and planning.American Journal of Sociology, 98, 1351-1387.
Lipowski, Z.]. (1986}. Psychosomatic medicine: Past andpresent. Canadian Journal of Psychiatry, 31, 2-21.
Lundberg, U. L. F. (1999}. Stress responses in low-statusjobs and their relationship to health risks: Musculo-skeletal disorders. Annals of the New York Academy ofSciences, 896, 162-172.
Magnusson, D. (1998). The logic and implications of aperson-oriented approach. In R.B. Cairns, L. R. Berg-

11G2 PART X. EMOTION ANDiHEAlT~
~~~~
~
'i!t
1~
matic event: Toward an understanding of inhibitionand disease. Journal. of Abnormal Psychology. 95,274-281. .
Pennebaker, J. W., &: King, L. A. (1999). Linguistic styles:Language use as an individual difference. Journal ofPersonality and Sociql Psychology. 77, 1296-131Z.
Petersson, M., Alster, P., Lundeberg, T., &: Uvnas-Moberg,K. (1996). Oxytocin causes long-term decrease of bloodpressure in female and male rats. Ph~iology and Be-havior, 60, 1311-1315.
RaikkOnen, K., Matthews, K. A., Flory, J.D., Owens, J. F.,&: Gump, B. B. (1999). Effects of optimism, pessimism,and trait anxiety on. ambulatory blood pressure andmood during everyday life. Journal of Personality andSocial Psychology. 76, 104-113.
Reed, G. M., Kemeny, M. E., Taylor, So E., &:Visscher, B. R.(1999). Negative HIV-specific expectancies and AIDS-related bereavement as predictors of symptom onset inasymptomatic HIV -positive gay men. Health Psychol-ogy. 18, 354-363;
Reed, G. M., Kemeny, M. E., Taylor, S. E., Wang, H.-Y. J.,&: Visscher, B. R. (1994). "Realistic acceptance" as apredictor of decreased survival time in gay men withAIDS. Health Psychology. 13, 299-307.
Reis, H. T. (2001). Relationship experiences and emotionalwell-being. In C. D. Ryff &: B. Singer (Eds.), Emotion.social relationships, and health (pp. 57-86). New York:Oxford University Press.
Reis, H. T., &: Patrick, B. C. (1996). Attachment and inti-macy: Component processes. In E. T. Higgins and A.Kruglanski (Eds.), Social psychology: Handbook of ba-sic principles (pp. 367-389). Chichester, England: Wi-ley.
Robins, R. W., John, O. P., &: Caspi, A. (1998). The typo"logical approach to studying personality. In R. B.Cairns, L. R. Bergman, &: J. Kagan (Eds.), Methods andmodels for studying the individual (pp. 135-160). Lon-don: Sage Publications.
Russek, L. G., &: Schwartz, G. E. (1997). Feelings of paren-tal caring predict health status in midlife: A 35-yearfollow-up of the Harvard Mastery of Stress Study. Jour-nal of Behavioral Medicine. 20, 1-13.
Russell, J. A., &: Barrett, L. (1999). Core affect, prototypical. emotional episodes, and other things ~ed emotion:
Dissecting the elephant. JOUlT!al of Personality and So-cial Psychology, 76, 805;...s19.
Rutter, M. (1990). Psychosocial resilience and protectivemechanisms. In J. Roll. A. S. Masten, D. Cicchetti. K. H.
'Neuchterlein, &: S. Weintraub (Eds.), Risk and prptec-tive factors in the development of psychopathology(pp. 181-214). New York: Cambridge University Press.
Ryff, C. D. (1989). Happiness is everything, or is it? Explo-rations on the meaning of psychological well-beirig.Journal of Personality and Social Psychology. 57,1069-1081.
Ryff, C. D. (1995). Psychological well-being in adult life.Current Directions in Psychological Science. 4, 99-104.
Ryff, C. D., &: Keyes, C.L.M.. (1995). The structure of psy-chological well-being revisited. .Journal of Personalityand Social Psychology. 69, 719-727.
Ryff, C. D., Magee, W. J., Kling, K. C., &: Wing, E. H. (1999).Forging macro-micro linkages in the study of psycho-logical well-being. In C. D. Ryff & V. w. Marshall (Eds.),The self and society in aging processes (pp. 247-278).New York: Springer
Ryff, C. D... & Singer, B. (2000). Interpersonal flourishing:
man, &; J. Kagan (Eds.), MethOds and models for study-ing the individual (pp. 33-64). London: Sage Publi-cations.
Malarkey, W., Kiecolt-Glaser, J. K., Pearl, D. "&: Glaser, R.. (1.994). Hostile behavior during marital conflict alters
pituitary and adrenal hormones. Psychosomatic Medi-cine, 56, 41-51.
Matthews, K. A. (1988). Coronary heart disease and typeA behavior: Update on an alternative to the Booth Kew-ley and Friedman quantitative review. PsychologicalBulletin, 104, 373-380.
McEwen, B. S. (1998). Protective and damaging effects ofstress mediators. New England Journal of Medicine,338, 171-179. -
McEwen, B. S., &; Schmeck, H. (1994). The hostage brain.New York: Rockefeller University Press.
McEwen, B. S. a: Seeman, T. (1999). ProteCtive and dam-aging effects of mediators of stress: Elaborating and test-ing the concepts of allostasis and allostatic load. An-nals of the New York Academy of Sciences, 896, 30-47.
McEwen, B. S., a: Stellar, E. (1993). Stress and the individ-ual: Mechanisms lea~ to disease. Archives of Inter-nal Medicine, 153, 2093-2101.
McKenna, M. C., Zevon, M. A., Com, B., a: Rounds, J.(1999). Psychosocial factors and the development ofbreast cancer: A meta-analysiS. Health Psychology, 18,520-531.
McNair, D. M., Lorr, M., & Droppleman, L. F. (1971). Pr0-file of mood states. San Diego: Educational and Indus-trial Testing Service.
McNeilly, M. D., Anderson, N. B., Armstead,C. A., Clark,R., Corbett, M. 0., Robinson, E. L., Pieper, C. F., a: Lip-isto, M. (1996). The perceived racism scale: A multi-dimensional a.ssessment of the perception of White ra-cism among African Americans. Rqcism and Health,Ethnicity, and Disease, 6, 154-166.
Miller, G. E., Dopp, J. M., Myers, H. F., Stevens, S. Y., &Fahey, J. L. (1999). Psychosocial predictors of naturalkiller cell mobilization during marital conflict. HealthPsychology, 18, 262-271.
Noh, S., Beiser, M., Kaspar, V., Hou, F., Rummens, J.(1999). Perceived racial discriJnination, depression,and coping: A study of Southeast Asian refugees inCanada. Journal of Health and Social Behavior, 40,193-207.
Panksepp, J. (1998a). Affective neuroscience: The foun-dations of human and animal emotions. New York: Ox-ford University Press.
Panksepp, J. (1998b). The quest for Jong-term health andhappiness: To play or not to play, that is the question.Psychological Inquiry, 9, 56-65.
Pappas G., Queen,S., Hadden, W., a: Fisher, G. (1993). Theincreasins disparity and mortality between socioeco-nomic groups in the United States, 1960 and 1986. NewEnglandjournal of Medicine, 329, 103-109.
Parker, G., Tupling, H., & Brown, L. B. (1979). A parentalbonding instrument. British Journal of Medical Psy-chology, 52, 1-10.
Pearlin, L. I., Lieberman, M. A., Menaghan, E. G., a: Mul-lan, J. T. (1981); The stress process. Journal of Healthand Social Behavior, 22, 337-356.
Pennebaker, J. W. (Ed.). (1995). Emotion, disclosure, andhealth. Washington, DC: American Psychological As-sociation.
Pennebaker, J. W., & Beall, S. K. (1986). Confronting a trau-

103CHAPTER 57. THE ROLE OF EMOTION ON PATHWAYS TO POSITIVE HEALTH
McEwen, B. S. (1997). The price of adaptation: Ano-static load and its health consequences, MacArthurstudies of successful aging. Archives of Internal Medi-cine. 157. 2259-2268.
Segerstrom, S. C., Taylor. S. E., Kemeny, M. E., &: Fahey.J. L. (1998). Optimism is associated with mood, coping.and immune change in response to stress. Journal ofPersonality and Social Psychology 74, 1646,..1655.
Selye. H. (1958). The stress of life. New York: McGraw-Hill.
Shaver, P., Schwartz, J., Kirson. D., ~ O'Connor, C. (1987).Emotion knowledge: Further exploration of a prototypeapproach. Journal of Personality and Social Psychol-08)', 52, 1061-1086.
Shedler, J., Mayman, M., ~ Mania, M. (1993). The illusionof mental health. American Psychologist, 48, 1117-1131.
SheldonrK. M., Ryan, R.. ~ Reis, H. T. (1996). What makesfor a good day? Competence and autonomy in the dayand in the person. Personality and Social Psycholo8)'Bulletin, 22. 1270-1279.
Singer, B.,I: Ryff, G. D. (1997). Racial and ethnic inequal-ities in health: Environmental, psychosocial, and phys-iological pathways. In B. Devlin, S. E. Feinberg, D. Res-niGk, ~ K. Roeder (Eds.) , Intellisence, senes, andsuccess: Scientists' response to the Bell Cwve (pp. 89-122). New York: Springer-Verlag Publications.
Singer. B., ~ Ryff, C. D. (1999). Hierarchies of life historiesand health risk.. Annals of the New York Academy ofSciences, 896, 96,..115.
Singer, B., Ryff, C. D.. Carr, D.. ~ Magee. W. J. (1998). Lifehistories and mental health: A person-centered strategy.In A. Raftery (Ed.), Sociological Methodolo8)', 1998(pp. 1-51). Washington, D.G.: American SociologicalAssociation.
Singer, B., Ryfi, C. D.. Davidson, R. J., Muller. D., Love,G. D., ~ Seeman, T. E. (2000). Pathways to positivehealth: Connectins psychosocial factors with cerebralactivation asymmetry and allostatic load. Unpublishedmanuscript.
Smider, N. A., Essex, M. J., ~ Ryff, C. D. (1996). Adapta-tion to community relocation: The interactive influenceof psychological resources and contextual factors. Psy-chology and Agins, 11,362-371.
Smith, T. W. (1992). Hostility and health: Current status ofa psychosomatic hypothesis. Health PsycholoS)', 11.139-150.
Solomon, R. C. (1993). The passions: Emotions and themeaning of life. Indianapolis: Hackett Publishing.
Spiegel, D. (1998). Effects of psychosocial treatment inprolonging cancer survival may be mediated by neu-roimmune pathways. Annals of the New York Academyof Sciences, 840, 674-683.
Spiegel, D., &: Kimerling. R. (2001). Group psychotherapyfor women with breast cancer: Relationships among so-cial support, emotional expression, and survival. InC. D. Ryff &: B. Singer (Eds.). Emotion, social relation-ships, and health (pp. 97-123). New York: Oxford Uni-versity Press.
Stanton. A. L., &: Snider, P.R. (1993). Coping with a breastcancer diagnosis: A prospective study. Health Psychol-ogy. 12. 16,..23.
Sterling. P. &: Eyer, J. (1988). Allostasis: A new paradigmto explain arousal pathology. In ]. Fisher &: J. Reason(Eds.), Handbook of life stress, cognition. and health(pp. 629-649). New York: Wiley.
A positive health agenda for the new millennium. Per-sonality and Social Psychology Review, 4, 30-44.
Ryff. C. D., &:. Singer. B. (2001). IntegratiIlg emotion iritothe study of social relationships and health. In c. D.Ryff &:. B. Singer (Eds.). Emotion. social relationships.and health (pp. 3-22). New York: Oxford UniversityPress.
Riff. c. D.. &:. Singer. B. (19984). The contours of positiv~human health. Psychological Inquiry, 9. 1-28.
Ryff, C. D.. &:. Singer. B. (1998b). Human health: New di-rections for the next millennium. Psychological In-quiry, 9, 89-65.
Ryff, C. D., Singer. B., Love, G. D.. &:. Essex. M.]. (1998).Resilience iri adulthood and later life: DefiniDg featuresand dynamic processes. In ].Lomranz (Ed.).Hazid~kof Aging and Mental Health: An Integrative Approach(pp. 69-96). New York: Plenum.
Ryff. C. D.. Siriger. B.. Wing. E. H.. &:. Love, G. D. (2001).Elective affinities and uninvited agonies: Mappingemotion with significant others onto health. In C. D.Ryff &:. B. Singer (Eds.) , Emotion, social relationships.and health (pp. 133-175). New York.: Oxford UniversityPress.
Sapolsky. R. M. (1992). Stress, the aging brain, and. themechanisms of neuron death. C.amb.ridge. MA: MITPress.
Schaefer. M. T.. &:. Olson. D. (1981). Assessing intim,cy:The PAIR Inventory. Journal of Mam'ag8 and FamilyTherapy, 7.47-60.
Scheier. M. F.. &:. Carver. c. S. (1992). Effects of optimismon psychological and physical well-being: Theoreticaloverview and empirical update. Cognitive Therapy andResearch, 16, 201-228.
Schwarz. N.. I: Clore. G. L. (1983). Mood. misattribution.and judgments of judgments of well-being: Informativeand directive functions of affect stress. Journal of Per-sonality and Social Psychology. 45. 513-523.
Schwarz. N.. &:. Strack. F. (1999). Reports of subjectivewell-beirig: Judgmental processes and their methodo-logical implications. In D. Kahneman. E. Diener. &:. NSchwarz (Eds.). Well-being: The foundations of hedonicpsychology (pp. 40-60). New York: Russell Sage Foun-dation.
Seeman. M. (1959). On the meaning of alienation. Amer-ican Sociological Review, 24. 783-791.
Seeman. M. (1975). Alienation studies. Annual Review ofSociology, 1,91-123.
Seeman. T.B..Singer. C.. Wilkinson. I: McEwen. B. (1999).Exploring a new concept of cumulative biological risk-allostatic load and its health consequences: MacArthurstudies of successful aging. Unpublished manuscript.
Seeman. T. E. (1996). Social ties and health: The benefitsof social iritegration. Annals of Epidemiology, 6. 442-451.
Seeman. T. E.. Berkman. L. F.. Blazer. D.. & Rowe.]. (1994).Social ties and support and neuroendocrine function:The MacArthur studies of successful aging. Annals ofBehavioral Medicine. 16. 95-106.
Seeman. T. E.. &:. McEwen. B. S. (1996). Impact of socialenvironment characteristics on neuroendoCrine regu-lation. Psychosomatic Medicine, 58. 459-471.
Seeman. T. E.. McEwen. B. S., Rowe,]. W.. &:. Singer. B. H.(2001). Allostatic load as a marker of cumulative bio-logical risk. Proceedings of the National Academy ofSciences, 98, 4770-4775.
Seeman. T. E.. Singer. B.. Rowe. ]. W.. Horwitz. R. &:.

1104 PART X. EMOTION ANO H~rH
fect. Journal of Personality and Social Psychology,70, 567-577.
Watson, D., & Pennebaker, J. W. (1989). Health com-plaints, stress, and distress: Exploring the central roleof negative affectivity. Psychological Review, 96, 234-254. .
Watson, D., &:. Tellegen, A. (1985). Toward a consensualstructure of mood. Psychological Bulletin, 98, 219-235.
Watson, D., Wiese, D., Vaidya, J., & Tellegen, A. (1999).The two general activation systems of affect: Structuralfindings, evolutionary considerations, and psychobio-logical evidence. Journal of Personality and Social Psy-chology, 76, 830-838.
Weinberger, D. A. (1990). The construct validity of the re-pressive coping style. In J. L Singer (Ed.), Repressionand dissociation: Implications for personality theory,psychopathology, and health (pp.337-385). Chicago:Universjty of Chicago Press.
Weinberger, D. A., Schwartz, G. E., & Davidson, R J.(1979). Low-anxious, high-anxious, and repressive cop-ing styles: Psychometric patterns and behavioral andphysiological responses to stress. Journal of AbnonnalPsychology, 88, 369-380.
Weiner, H. (1992). Perturbing the organism: The biologyof stressful experience. Chicago: University of ChicagoPress.
Werner, E. (1995). Resilience in development. CUlTent Di-rections in Psychological Science, 4. 81-85.
Wheeler. R. E.. Davison, R. J., & Tomarken, A. J. (1993)Frontal brain asymmetry and emotional reactivity: Abiological substrate of affect style. PsychophY$iology,30, 82-89.
Wiesel, E. (1999). And the sea is never full. New York:Knopf. .
Williams, D. R.. Yu, Y.. Jackson. J.. & Anderson, N. (1997).Racial differences in physical 'and mental health: So-cioeconomic status, stress, and discrimination. Journalof Health Psychology, 2, 335-351.
Yik. M.S.M. & Russell, J. A., Feldman Barrett, L (1999).Structure of self.reported current affect: Integration andbeyond. Journal of Personality and Social Psychology77, 600-619.
Sutton, S. K., &; Davidson, R J. (1997). Prefrontal brainasymmetry: A biological substrate of the behavioral ap-proach and inhibition systems. Psychological Science,8, 204-210.
Taylor, S. E., Kemeny, M. E., Reed, G. M., Bower, J. E., &Gruenewald, T. L (2000) Psychological resources,'pos-itive illusions, and health. American Psychologist, 55,99-109.
Taylor, S. E., Repetti, R L., &; Seeman, T. (1997). Healthpsychology: What is an unhealthy environment andhow does it get under the skin? Annual Review of Psy-chology, 48,411-47. '
Thayer, R. E. (1989). The.biopsychology of mood and at;-tivation. New York: Oxford University Press.
Thoits, P.A. (1995). Stress, coping, and social, support pro-cesses:! Where are we? What next? Journal of Healthand Social Behavior, Extra Issue, 53-79.
Tomarken, A. J., Davidson, R. J., Wheeler, R. E., & Doss,R C. (1992). Individual differences in anterior brainasymmetry and fundamental dimensions of emotion.journal of Personality and Social Psychology, 62, 676-687.
Uchino, B. N., Cacioppo, J. T., & Kiecolt-Glaser, J. K.(1996). The relationship between social support andphysiological processes: A review with emphasis onunderlying mechanisms and implications for health.Psychological Bulletin, 119, 488-531.
Uvnas-Moberg, K. (1997). Physiological and endocrine ef-fects of social contact. Annals of the New York Acad-emy of Science, 807,146-163.
Uvnas-Moberg, K. (1998). Oxytocin may mediate the ben-efits of positive social interaction and emotions. Psy-choneuroendocrinology, 23, 819-835.
Veroff, J., Douvan, E., & Kulka, R A. (1981). The innerAmerican: A self-portrait from 1957 to 1976. New York:Basic Books.
Watson, D., & Clark, L. A.(1992). On traits and tempera-ment: General and specific factors of emotional expe-rience and their relation to the five-factor model. Jour-nal of Personqlity, 60, 441-476.
Watson, D., &; Walker, L. M. (1996). The long-term sta-bility and predictive validity of trait measures of af-