Embed Size (px)
Citation preview

Saudi Journal of Ophthalmology (2013) 27, 97–106
Review Article
The role of cerebrospinal fluid pressure in glaucoma and otherophthalmic diseases: A review
Peer review under responsibilityof Saudi Ophthalmological Society,King Saud University Production and hosting by Elsevier
Access this article onlinwww.saudiophthaljournwww.sciencedirect.com
Received 9 January 2013; accepted 11 March 2013; available online 17 March 2013.
a Department of Ophthalmology, University of North Carolina Hospitals, Chapel Hill, NC, USAb Ophthalmology, Glaucoma Service, Duke University Eye Center, Durham, NC, USA
⇑ Corresponding author. Address: Ophthalmology, Duke University Eye Center, 2351 Erwin Rd Box 3802, Durham, NC 27710, USA. Tel.: +1 90421.e-mail address: [email protected] (R.R. Allingham).
David Fleischman, MD a; R. Rand Allingham, MD b,⇑
Abstract
Glaucoma is one of the most common causes of blindness in the world. Well-known risk factors include age, race, a positive familyhistory and elevated intraocular pressures. A newly proposed risk factor is decreased cerebrospinal fluid pressure (CSFP). This con-cept is based on the notion that a pressure differential exists across the lamina cribrosa, which separates the intraocular space fromthe subarachnoid fluid space. In this construct, an increased translaminar pressure difference will occur with a relative increase inelevated intraocular pressure or a reduction in CSFP. This net change in pressure is proposed to act on the tissues within the opticnerve head, potentially contributing to glaucomatous optic neuropathy. Similarly, patients with ocular hypertension who have ele-vated CSFPs, would enjoy a relatively protective effect from glaucomatous damage. This review will focus on the current literaturepertaining to the role of CSFP in glaucoma. Additionally, the authors examine the relationship between glaucoma and other knownCSFP-related ophthalmic disorders.
Keywords: Cerebrospinal fluid pressure, Translaminar pressure, Glaucoma, Papilledema, Idiopathic intracranial hypertension,Microgravity
� 2013 Production and hosting by Elsevier B.V. on behalf of Saudi Ophthalmological Society, King Saud University.http://dx.doi.org/10.1016/j.sjopt.2013.03.002
Introduction
Glaucoma is a distinct optic neuropathy, which results in acharacteristic nerve damage and a typical pattern of visualfield loss. Intraocular pressure (IOP) is one of the most impor-tant risk factors. One approach to the classification of glau-coma is open versus closed angle forms. Closed-anglevariants of glaucoma have elevated IOP that is caused by pri-mary or secondary pathologies that share anatomic crowdingor closure of the aqueous humor drainage system or angle. Inopen-angle forms of glaucoma the drainage angle is open,but for a variety of reasons the IOP may be elevated or re-mains in the normal range. Regardless of the type of glau-coma, intraocular pressure reduction by a medical or
surgical approach has been shown to decrease incidenceand progression of glaucoma.
Why glaucoma occurs with normal tension glaucoma(NTG) or does not occur in some patients with ocular hyper-tension (OHT) has been debated for decades. Explanationsfor NTG include hypotheses of a ‘‘susceptible optic nerve,’’intrinsic retinal or ganglion cell pathology, inflammatorycauses, undocumented elevations in IOP, and others. Thereis likely an interplay of susceptibility factors that decreasesthe threshold for glaucomatous injury in these patients de-spite seemingly normal intraocular pressures, or alternativelycauses a different type of glaucoma. Vascular or perfusionabnormalities may be important, perhaps in concert withpressure fluctuations, neuronal excitotoxicity, genetic
e:al.com
19 684

98 D. Fleischman, R.R. Allingham
mutations or predisposition, or other pressure-independentfactors.1–3 However, it has been determined that reducingIOP is beneficial in patients with normal tension glaucoma.Conversely, a variety of explanations have been offered forthe observation that a relatively small percentage of patientswith documented elevation of IOP out of the normal rangeultimately develop glaucomatous damage. For these reasonsit has become clear that factors in addition to IOP play animportant role in glaucoma pathogenesis.
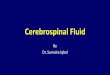
Figure 1. Histologic anatomy of the posterior globe and optic nerve with surthat acts as a sieve and allows the passage of exiting retinal ganglion cell axosubarachnoid space between the dura mater and the pia mater investing theHistology Learning System (Deborah W. Vaughan, PhD).
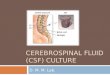
Figure 2. Spectrum of cerebrospinal fluid
Recent studies have implicated the role of pressure of theprimary fluid within the central nervous system, the cerebro-spinal fluid (CSF), as a major contributor to glaucoma. Theanatomical landmark of interest is the lamina cribrosa, a thinarea of scleral tissue that separates two differentially pressur-ized compartments – the intraocular space and the orbitalsubarachnoid space. (Fig. 1) The difference in pressure be-tween these two fluid spaces is termed the translaminar pres-sure. When described as a function of pressure across the
rounding tissue. The lamina cribrosa (red) is a thin section of scleral tissuens and the retinal vessels. The cerebrospinal fluid (blue) flows within the
optic nerve. Modified and reproduced with permission, Boston University
pressure-related ophthalmic disease.

CSFP and Glaucoma 99
tissues of the optic nerve and lamina cribrosa the term ismore accurately stated as the translaminar pressure gradient.It is hypothesized that an elevated posteriorly-directed pres-sure differential may contribute to optic nerve damage andproduces posterior bowing of the lamina cribrosa, which isoften seen in patients with glaucoma. At the other end ofthe spectrum, increased posterior pressure, a pressure vectorin the anterior direction toward the intraocular fluid compart-ment, associated with elevated intracranial hypertension, cancause papilledema. (Fig. 2).
We review here the risk factors for glaucoma in the con-text of this glaucoma–CSFP model. The relevant anatomy isreviewed, as are plausible mechanisms that could result inglaucomatous optic neuropathy as well as conditions on theother end of the CSFP spectrum that are also explained bythis model.
Primary open-angle glaucoma, normal tensionglaucoma, ocular hypertension – and thetranslaminar pressure difference
The earliest evidence that CSFP may play a role in glau-coma was reported by Yablonski and colleagues. In the catmodel, CSFP4 was lowered to –4 mm Hg. One eye was thencannulated to produce a pressure of 0 mm Hg, while theother eye was unchanged and maintained at a normal pres-sure. After 3 weeks, the uncannulated eye developed opticnerve damage consistent with glaucomatous optic neuropa-thy. The eye that was cannulated and maintained at a lowpressure similar to the CSF pressure did not develop opticneuropathy. Morgan and colleagues later performed elegantstudies that examined the effect of altering pressure of theintraocular and subarachnoid spaces on the lamina cribrosain a dog model. They reported that varying CSFP was similarto altering IOP on the lamina cribrosa, and therefore may berelevant in the pathogenesis of glaucoma.5 A follow-up studydetermined that this effect was possibly similar in human do-nor eyes.6
Berdahl and colleagues reported a large-scale retrospec-tive study based on electronic records available from theMayo Clinic. Medical records were obtained on over 30,000patients who underwent diagnostic lumbar punctures. Thosewith a diagnosis of primary open-angle glaucoma were com-pared to age-matched patients without glaucoma as con-trols. Intracranial pressure in POAG patients was lower thanthose without glaucoma (9.2 ± 2.9 mmHg versus13.0 ± 4.2 mmHg respectively, p < 0.0001).7 A second studyexamined ocular hypertensive patients, as well as normal ten-sion glaucoma patients. Compared to age-matched controls,patients with POAG were again found to have a statisticallylower CSFP compared to controls (9.1 ± 0.77 mmHg versus11.8 ± 0.71 mmHg, respectively). Patients with NTG hadeven lower pressures compared to standard POAG patients(8.7 ± 1.16 mmHg). Ocular hypertension patients were foundto have higher CSFP compared to the control patients(12.6 ± 0.85 mmHg versus 10.6 ± 0.81 mmHg, respectively;p < 0.05).8
Ren et al. examined this in a prospective study conductedin Chinese subjects. Patients with POAG (N = 43, 29 POAG;14 NTG) were compared to 71 non-glaucomatous controls.This study confirmed the finding that patients with high-pres-sure POAG had lower CSF (11.7 ± 2.7 mmHg) compared to
normal patients (12.9 ± 1.9 mmHg). They also noted that pa-tients with NTG had lower CSFP compared to either POAGor non-glaucomatous controls (9.5 ± 2.2 mmHg). Given theprospective nature of this study, the examiners were ableto calculate the translaminar pressure difference(CSFP � IOP) and were able to correlate this measurementto the mean deviation of patient’s visual fields. In this studylarger translaminar pressure differences were positively cor-related with visual field loss.9 A second study by the samegroup examined ocular hypertension patients compared tonormal patients. Similar to the study by Berdahl et al., a sta-tistically significant difference between CSFP in OHTN andnon-glaucomatous control subjects was found with OHT pa-tients having significantly higher pressures (16.0 ± 2.5 mmHgversus 12.9 ± 1.9 mmHg, respectively; p < 0.001).10
Risk factors for glaucoma: a different perspective
The studies cited above provide evidence of a relationshipbetween CSFP and glaucoma, which raises additional ques-tions about other factors that may be related to CSFP and,by association, with glaucoma pathogenesis. Therefore, theeffect of factors such as age, sex, and body mass index(BMI) has been studied to better understand how thesemay affect CSFP as a potential risk factor for glaucoma andother ocular diseases.
Age
Among the multiple risk factors for primary open-angleglaucoma, age is one of the most noteworthy. Numerousstudies in the United States and around the world have iden-tified age as an independent risk factor.11–19 A recent studyby Fleischman et al. found a relationship between CSF andage, which may offer an explanation for age as a risk factorfor POAG.20 Electronic medical records of all patients whohad a lumbar puncture performed at the Mayo Clinic inRochester, Minnesota during a 13-year period (1996–2009)were screened. Patients using medications or having medicaldiagnoses known to affect CSFP were excluded from analy-sis. After all entry criteria were met, 12,118 patients werequalified for investigation. It was found that mean CSFPwas stable from ages 20–49 years. However, mean CSFP pro-gressively declined after age 49, from 11.5 ± 2.8 mmHg inthe 20–49 age group to 8.4 ± 2.4 mmHg in the over 90 yearage group (p < 0.001), a 27% reduction.
Assuming a stable IOP, this decline in CSFP with agewould result in a significant increase in the translaminar pres-sure gradient. Morgan’s studies suggest that the mechanicaleffect of changes in CSFP plays a significant role on the mor-phology of the lamina cribrosa.21,22 Assuming that a decreasein CSFP is equivalent to a similar increase in IOP, we can eval-uate this effect in reported population studies that haveexamined the prevalence and IOP measurements of personsdiagnosed with glaucoma and controls (Fig. 3). For example,the Baltimore Eye Survey revealed a 4-fold increase in risk inthe development of glaucoma by a change in IOP of+3 mmHg.11,23 The Beaver Dam Eye Study found that, onaverage, there was a 5 mmHg difference in IOP between pa-tients with glaucoma and those without.13 In Tajimi, Japan,researchers found that a 4 mmHg rise in IOP increased riskfor POAG in twofold, even within a normal range of

Figure 3. Averaged data of Friedman’s meta-analysis prevalence studies of primary open-angle glaucoma in the United States, with the age-relateddecrease in cerebrospinal fluid pressure superimposed. Data shown are from Caucasian patients, which constitute the principal group contained withinthe Mayo Clinic population.
100 D. Fleischman, R.R. Allingham
IOP.24,25 These data suggest that the observed 3 mmHgmean reduction of CSFP with advancing age may be animportant risk factor for glaucoma that has not been ac-counted among populations.
Body mass index
Body Mass Index (BMI) is another variable that has beenreported as a risk factor for glaucoma. A positive correlationbetween increased BMI and glaucoma, especially in women,was identified in Newman-Casey and colleagues’ large longi-tudinal cohort study in a mostly Caucasian population(86.7%).26 In their study of the relationship between POAGand components of the metabolic syndrome, an elevatedBMI in women had a 6% increased hazard of developingOAG. The study revealed no increased risk for glaucoma inmen. The Tajimi Eye Study (Japan) compared 119 patientswith POAG and 2755 controls, and found no statistically sig-nificant difference between BMI in either group (22.5 vs. 22.9respectively, p = 0.28).24 On the other hand, Leske’s Barba-dos Eye Study identified that a decreased BMI was associ-ated with greater risk for glaucoma in the Barbados
Figure 4. Graph of mean cerebrospinal fluid pressure with body mass
population of African ancestry.27 Other studies have had sim-ilar findings to Leske’s, except in NTG patients or based onsex.28–30
In their prospective study of CSFP and POAG, Ren andcolleagues found a positive correlation between BMI andCSFP. In this study, the mean age was 45.7 ± 11.3 years,and the mean BMI was 23.7 ± 2.7. Univariate analysis re-vealed CSFP was significantly correlated with higher BMI(r = 0.50; p < 0.001).31 In a retrospective study, Berdahlet al., reported results from an analysis of electronic medicalrecords obtained from 4235 patients with measured BMI.(Fig. 4) Women had a slightly lower BMI (mean 26.0 ± 5.8)while men had a slightly higher BMI (27.4 ± 4.6). Univariateregression models identified a positive linear relationship be-tween BMI and CSFP (r2 = 0.20, p < 0.001). There was a37.7% increase in BMI from BMI 18 (8.6 ± 2.1 mmHg) to 39(14.1 ± 2.5 mmHg).20,32,33
Since BMI is positively associated with CSFP the questionarises as to whether higher BMI may be protective for POAGand the converse, if lower BMI may increase risk for glau-coma. The studies cited above found that increased BMI ap-peared to be protective for POAG in female subjects,
index between 18 and 39. Bars represent one standard deviation.

CSFP and Glaucoma 101
although this protection was not conferred upon male sub-jects. The reason for this discrepancy is unclear. It is possibleother factors, such as some hormonal element, may beinvolved.34
Race
Race is a well-documented risk factor for glaucoma. It is ofgreat interest to determine whether CSFP varies among dif-ferent populations and whether this may be part of the expla-nation for differences in prevalence of glaucoma betweenvarious ethnic groups. Unfortunately, there is no study pow-ered to determine if there is any differential effect of raceon CSFP. Future large-scale studies of various populationswill be necessary to determine the effect, if any, of race onCSFP.
Physiology of CSFP
The translaminar pressure difference is a relatively simplis-tic term that does not account for what is clearly a complexrelationship between pressure within and surrounding variedtissue compartments, body position, and other known andunknown factors. The pressures within the orbital subarach-noid space, which comprise the retrolaminar pressures, arelikely different than the pressures in the cranial vault andthe remainder of the neuraxis. CSF pressures are directlyresponsive to changes in body position as well as diurnal var-iation. For example, when humans are upright, intracranialfluid pressure, due to hydrostatic fluid shifts, may drop to�5 mmHg. Why would the pressure measured by a lumbarpuncture have any relevance?
Embryology of the optic nerve, flow of the CSF
The development of the optic vesicle begins at day 22with an evagination from the wall of the diencephalon, whichcreates the optic vesicle. The optic vesicle invaginates andforms the optic cup and the optic stalk. The cavity of the op-tic stalk is eventually filled with the axons of the retinal gan-glion cells as well as the retinal vessels. The optic nerve, ofcourse, is an extension of the central nervous system, andas such is invested by the meninges. The optic nerve, as it ex-its the eye, is enclosed in dural, arachnoid and pial sheaths, aswell as the circulating fluid of the central nervous system, thecerebrospinal fluid (CSF). The CSF originates in the choroidplexus within the third, fourth, and inferior horn of the lateralventricles, and drains into the arachnoid villi of the cerebralvenous system, as well as through lymphatic channels.35–39
The fluid flows freely throughout the neuraxis within the sub-arachnoid space, which includes the optic nerve.
Anatomy and physiology
For the glaucoma-CSF model to make sense, it is essentialto understand the anatomy of the optic nerve head. This mustbe done in the broader context of the central nervous systemas well as the intraocular space. The anatomical landmark ofinterest is the lamina cribrosa, a thin sieve-like perforation ofthe posterior sclera through which the axons of the retinal gan-glion cells exit the eye. It is generally believed that the laminacribrosa is the major site of injury for vision loss related to glau-
coma.40–43 This is also the site that experiences the pressuregradient between the intraocular and extraocular spaces.6,44
The difference between these two spaces is termed the trans-laminar pressure difference. The resulting force imparted bythe difference of the two pressures is dependent on the thick-ness of the lamina cribrosa. Jonas et al., in a histomorphometricstudy of the lamina cribrosa in glaucomatous and non-glauco-matous eyes noted that the central lamina cribrosa thickness ina control group was nearly 250 micrometers thicker than theglaucoma group. These investigators concluded that this in-crease in the translaminar pressure gradient in these casesmight be important contributors to the glaucomatous patho-physiological process.
Effect of posture on CSFP
The CSFP measured in the supine position is a static mea-sure of a dynamic process. Lenfeldt found that CSFP mea-sured by lumbar puncture accurately represents intracranialpressure in the lateral decubitus position.45 However, theCSFP in the intracranial vault decreases and even falls to sub-zero values in a standing position, and then approachesequivalence in a prone position. Additionally, the dynamicsof the orbital CSF flow may be different than that of the restof the neuraxis. While a different pressure may exist withinthe orbital CSF compartment, it is nevertheless continuouswith the rest of the spinal column, and there is evidence thatpressure is transmitted to the optic nerve sheath from fluidchanges elsewhere in the contiguous subarachnoid space.46
Although a formulaic relationship between the orbital CSFPand intracranial pressure has not been elucidated to thispoint, the fact that there is pressure transduction betweenthe neuraxis and the orbital CSFP suggests that these twocompartments should not be considered separately. There-fore, for the purpose of considering the translaminar pressuredifference, it is more useful to relatively interpret lumbarpuncture data, as opposed to considering the retrolaminarpressure strictly as the lumbar puncture opening pressure.
Idiopathic intracranial hypertension (IIH) and papilledemaserve as useful examples. In describing IIH, Corbett and Meh-ta considered an abnormally elevated CSFP to be greaterthan 250 mm H2O (or 18.4 mmHg) as measured in the lateraldecubitus position.47 A pressure under 200 mm H2O(14.7 mmHg) is considered normal however. Therefore, lessthan 4 mmHg is clinically significant, even before taking intoaccount gross overestimates of the retrolaminar pressure inthe upright position, which is the case approximately two-thirds of a typical day. The measurement of the opening pres-sure from a lumbar puncture is important, however it is notpossible currently to assess the impact of postural changeson the biomechanics and physiology of the lamina cribrosa.
What contributes to the pressure of the cerebrospinalfluid?
In most simplistic terms, much like the eye, the CSFP is aproduct of production and drainage of fluid. If we look atthe relationship of age and CSFP described above, thechange in pressure may be a product of decreased resistanceto CSF outflow or decreased CSF production with advancingage. There is no evidence that outflow resistance decreaseswith age – on the contrary, studies report CSF flow resistance

102 D. Fleischman, R.R. Allingham
increases with age.39,48 However, the choroid plexus under-goes aging changes that lead to decreased CSF produc-tion.49–51 Current evidence suggests that vasopressin, ahormone that regulates the choroid plexus is responsiblefor a reduction in CSF production. Further, vasopressin-secreting neurons show increased activity with aging.52,53
This is speculative, of course, but these data do supportthe role of reduced CSF production rather than increaseddrainage as a possible cause of decrease in CSFP with age.
BMI and CSFP
The effect of body mass index on the cerebrospinal fluidpressure likely involves a biomechanical explanation. BMI ispositively and independently associated with CSFP.31,32 It isuseful to look at the conceptual opposite of glaucoma – idio-pathic intracranial hypertension. Studies of IIH suggest thatobesity, in particular central obesity, increases intra-abdominalpressure.54,55 This results in an increase in venous pressurefrom compression of the large central veins, and this ultimatelyincreases intracranial venous pressure with a corresponding in-crease in intracranial pressure. A similar mechanism may beresponsible for the effect of BMI in general. However, it is likelythat other factors may play a role in this relationship.
Diurnal variation
Diurnal variation of intraocular pressure has been identi-fied as a normal physiological process,56,57 but also an inde-pendent risk factor for the progression of glaucoma.58 This isjust one factor in the translaminar pressure gradient, so it isuseful and necessary to understand if changes exist in CSFPas a product of the circadian rhythm. To date, it is still un-known to what extent, if any, diurnal variability has an influ-ence on the spinal fluid pressure. Severs’ group identified asignificant diurnal fluctuation in CSFP in rats, with pressuresnearly 4 mmHg higher during the nighttime compared tothe daytime (p < 0.05).59,60 Conversely, Lin and Liu foundno significant circadian intracranial pressure variation in Spra-gue–Dawley rats.61 The latter authors conclude that thetranslaminar pressure difference is projected to be higherduring the dark period only due to the change in IOP.
A recent study by Samuels and colleagues investigatedcentral control of the individual elements of the translaminarpressure difference – CSFP and IOP – in the context of thecircadian rhythm.62 The dorsomedial and perifornical hypo-thalamic neurons receive input from the suprachiasmic nu-cleus, the main regulator of the circadian rhythm. Thesedorsomedial and perifornical nuclei, in turn, contain manyefferent sympathetic neurons that likely have an importantrole in carrying out the characteristic physiological changes.Microinjections of GABAA receptor antagonists were admin-istered into the dorsomedial and perifornical hypothalamusin a rat model demonstrated an asynchronous elevation ofboth CSFP and IOP. These data suggest that IOP and CSFP,and in turn, fluctuation in the translaminar pressure gradientmay be influenced by diurnal variation.
Genetics
Evidence is rapidly mounting on the importance of a ge-netic basis for glaucoma. In the context of the CSFP–glau-
coma model, there is early evidence that genetic lociassociated with risk for POAG may also be involved in CSFregulation.63,64 In a study by Wiggs et al., researchers foundthat a single nucleotide polymorphism (SNP) located on chro-mosome 8q22 falls in a region that is known to be activelytranscribed by choroid plexus epithelial cells, nonpigmentedciliary epithelial cells, and iris pigment epithelial cells. It isintriguing that cells responsible for the production of thetwo circulating fluids of the central nervous system, therespective contributors to the translaminar pressure differ-ence, have been strongly associated to NTG.
Imaging studies
MRI
Mostly stemming from the desire to approximate intracra-nial pressures in idiopathic intracranial hypertension, neuro-imaging has been utilized in an attempt to detect elevatedintracranial pressures. The only ways to accurately assessthe spinal fluid pressures to date are through invasive tech-niques, including lumbar puncture. Since there is some riskassociated with lumbar punctures or other intraventricularpressure measurements, non-invasive techniques for estimat-ing cerebrospinal fluid pressures are highly coveted. Mag-netic resonance imaging (MRI) may be one possibility.Many studies have advocated the use of MR imaging in theestimation of either increased or decreased intracranial pres-sure.65–70
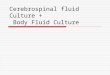
If retrolaminar pressures are indeed important, then thepressure in the orbital subarachnoid space must be investi-gated more closely. Therefore, the diameter or changes inthe optic nerve subarachnoid space width could be usefulin assessing relative pressures for the retrolaminar compo-nent of the translaminar pressure gradient. (Fig. 5) Wanget al. found that patients with NTG patients have a signifi-cantly smaller optic nerve subarachnoid space width (ON-SASW) compared to non-glaucomatous patients.71 Thesefindings are consistent with the hypothesis that lower CSFPmay play a role in POAG.
Ultrasound
Ultrasound, while not able to provide for posterior opticnerve sheath measurements, can reliably reveal nerve sheathdiameters in the most anterior aspect of the intraorbitalnerve. Again, interest in this field stems from finding a surro-gate for lumbar puncture in patients with papilledema andpresumed idiopathic intracranial hypertension46,72–74; to dateno studies on glaucoma patients have been performed. Thismay be an important imaging modality for studying CSF andpressure dynamics in the orbital nerve. Based on Wang’s MRimaging study, even at 3 mm posterior to the globe, therewere significant differences in nerve sheath diameters be-tween glaucomatous and non-glaucomatous patients.71 Thisis within the range that ultrasound could accurately image.While unable to provide a quantitative estimation of pressure(no more than MR imaging could provide), a qualitative esti-mation has significant utility.
Fluid, compartment and pressure dynamics would likelybest be measured with ultrasonography due to its flexibility,easy use – especially in comparison to MRI. As humans spend

Figure 5. Magnetic resonance imaging studies are being used to determine the width of the subarachnoid space of the orbital portion of the opticnerve. As an example, (A) a T2-weighted axial turbo spin echo (TSE) image of a 27 year old white female with an opening pressure of 32 cm H2O withidiopathic intracranial hypertension, and (B) a T2-weighted axial TSE image of an 86 year old Hispanic female with end-stage primary open angleglaucoma. Although not measured, there is a gross difference in subarachnoid space thickness of the optic nerve between the two patients.
CSFP and Glaucoma 103
most of their day in an upright position, intracranial and orbi-tal nerve pressures fall to subatmospheric pressures.75,76
Even differences in the prone and supine position, due tohydrostatic effects and gravity, may result in changes in theorbital CSFP. While it is possible to perform MRI in a varietyof positions, it is far more challenging. Therefore, ultrasoundoffers a potentially more available and practical method tostudy orbital fluid dynamics in multiple positions.
The CSF model in idiopathic intracranialhypertension and microgravity-induced visualimpairment/intracranial pressure
Idiopathic intracranial hypertension
If glaucoma is a disease that is due in part to decreasedintracranial pressure, it then serves as the conceptual oppo-site to idiopathic intracranial hypertension (IIH). Idiopathicintracranial hypertension is a potentially blinding conditionthat results in papilledema from increased intracranial pres-sure. Interestingly, both IIH and glaucoma produce similar vi-sual field defects. As described above, there are someanatomical explanations for a transient increase in CSFP.Clinical studies also implicate medications such as antibiotics,vitamin A, retinoid analogues, and hormonal contracep-tives.77–80 In addition, there are multiple case reports of pa-tients with ocular hypertension who were treated withpressure-lowering surgery and subsequently developedpapilledema; they were later found to suffer from IIH.81–83
This suggests that intraocular pressure may actually be an-other element in this disease. This raises an intriguing ideaof increasing the intraocular pressure for the purpose oftreating papilledema.84,85 Much like the findings of Berdahland Ren, an elevated cerebrospinal fluid pressure, as foundin ocular hypertension, could potentially be protective forglaucoma.
An interesting observation of CSFP trends from the MayoClinic database places IIH and glaucoma at opposite ends ofa spectrum. A study performed using the Mayo Clinic medi-cal record system from 1976 to 1990 identified nine patientswith IIH.86 Although the sample size is small, the highest rate
of the disease occurred between ages 15 and 44, and pa-tients with a BMI over 26 had a 7–8-fold increased risk ofIIH compared to the general population. Generally, patientswith IIH tend to be younger females with an increased bodymass index.87 Glaucoma patients tend to be older and thin-ner. These pressures are essentially reference ranges perage and BMI group. It could be imagined that those patientsat the higher end of the reference range, perhaps over twostandard deviations in the age and BMI charts, would havesignificantly higher CSF pressures. This, coupled with de-creased intraocular pressure, could contribute to IIH. Anopposite scenario may exist in glaucoma.
Microgravity-induced visual impairment/intracranialpressure
A newly described clinical condition resulting from pro-longed space travel may also highlight the importance ofthe translaminar pressure difference. Mader et al. reportedthat seven astronauts who were in prolonged space missionsreturned with visual disturbances and found to have elevatedintracranial pressures and papilledema.88 We have suggestedthat papilledema may be due in part to a cephalad fluid shiftof the CSF which would provide a persistent higher-than-normal retrolaminar pressure.89 This does not explain the ele-vated CSFP recorded, however. There are likely biomechan-ical and physiological metrics for baroregulation that arealtered by prolonged microgravitational exposure. For exam-ple, just as the carotid sinus contains baroreceptors that reg-ulate blood pressure, perhaps a similar system exists whichregulates cerebrospinal fluid pressures. After months in amicrogravitational environment, the baroreceptors could re-quire a significant period of time to return to normal. It hasalso been suggested that the valveless venous system withinthe intracranial space may cause stagnant venous flow inmicrogravity causing a decrease in CSF outflow.90 Again, asafe increase in intraocular pressure may be an option to de-crease the translaminar pressure gradient and simulatingocular hypertension.84,85 Finding or developing medicationsor devices that could safely and transiently increase intraocu-lar pressure may be of interest.

104 D. Fleischman, R.R. Allingham
Conclusion
A decreased cerebrospinal fluid pressure may act in a sim-ilar manner as an increased intraocular pressure by increasingthe translaminar pressure difference. Reduced CSFP may of-fer a partial explanation for POAG that occurs in the pres-ence of normal IOP and may be a contributing factor formost other forms of glaucoma. Our current inability to quan-tify the retrolaminar pressure gradient limits efforts to ex-plore this hypothesis. However, if it was possible to accountfor IOP, lamina cribrosa thickness, and CSFP a formulaic cal-culation could be developed that might help predict glau-coma risk, risk of glaucoma progression, as well ascontribute to our understanding of other CSFP-related oculardiseases and provide novel therapeutic opportunities.
Acknowledgements
Duke University Eye Center and Department of Ophthal-mology, University of North Carolina Hospitals are recipientsof unrestricted grants from the Research to Prevent Blind-ness, New York, NY.
References
1. Chang EE, Goldberg JL. Glaucoma 2.0: neuroprotection,neuroregeneration, neuroenhancement. Ophthalmology 2012;119(5):979–86.
2. Shields MB. Normal-tension glaucoma: is it different from primaryopen-angle glaucoma? Curr Opin Ophthalmol 2008;19(2):85–8.
3. Caprioli J. Neuroprotection of the optic nerve in glaucoma. ActaOphthalmol Scand 1997;75(4):364–7.
4. Yablonski M, Ritch R, Pakorny K. Effect of decreased intracranialpressure on optic disc. Invest Ophthalmol Vis Sci 1979;18(Suppl.):165.
5. Morgan WH, Yu DY, Alder VA, Cringle SJ, Cooper RL, House PH, et al.The correlation between cerebrospinal fluid pressure and retrolaminartissue pressure. Invest Ophthalmol Vis Sci 1998;39(8):1419–28,PubMed PMID: 9660490. Epub 1998/07/11. eng.
6. Balaratnasingam C, Morgan WH, Johnstone V, Pandav SS, Cringle SJ,Yu DY. Histomorphometric measurements in human and dog opticnerve and an estimation of optic nerve pressure gradients in human.Exp Eye Res 2009;89(5):618–28, PubMed PMID: 19523943. Epub2009/06/16. eng.
7. Berdahl JP, Allingham RR, Johnson DH. Cerebrospinal fluid pressureis decreased in primary open-angle glaucoma. Ophthalmology2008;115(5):763–8.
8. Berdahl JP, Fautsch MP, Stinnett SS, Allingham RR. Intracranialpressure in primary open angle glaucoma, normal tension glaucoma,and ocular hypertension: a case-control study. Invest Ophthalmol VisSci 2008;49(12):5412–8, PubMed PMID: 18719086. Pubmed CentralPMCID: 2745832.
9. Ren R, Jonas JB, Tian G, Zhen Y, Ma K, Li S, et al. Cerebrospinal fluidpressure in glaucoma: a prospective study. Ophthalmology2010;117(2):259–66.
10. Ren R, Zhang X, Wang N, Li B, Tian G, Jonas JB. Cerebrospinal fluidpressure in ocular hypertension. Acta Ophthalmol 2011;89(2), e142-8, PubMed PMID: 21348961. Epub 2011/02/26. eng.
11. Tielsch JM, Sommer A, Katz J, Royall RM, Quigley HA, Javitt J. Racialvariations in the prevalence of primary open-angle glaucoma: theBaltimore eye survey. JAMA 1991;266(3):369–74.
12. Friedman DS, Wolfs RC, O’Colmain BJ, Klein BE, Taylor HR, West S,et al. Prevalence of open-angle glaucoma among adults in the UnitedStates. Arch Ophthalmol 2004;122(4):532–8.
13. Klein BE, Klein R, Sponsel WE, Franke T, Cantor LB, Martone J, et al.Prevalence of glaucoma. The beaver dam eye study. Ophthalmol1992;99(10):1499–504.
14. Quigley HA, West SK, Rodriguez J, Munoz B, Klein R, Snyder R. Theprevalence of glaucoma in a population-based study of Hispanicsubjects: proyecto VER. Arch Ophthalmol 2001;119(12):1819–26.
15. Kini MM, Leibowitz HM, Colton T, Nickerson RJ, Ganley J, DawberTR. Prevalence of senile cataract, diabetic retinopathy, senile maculardegeneration, and open-angle glaucoma in the Framingham eyestudy. Am J Ophthalmol 1978;85(1):28–34.
16. Dielemans I, Vingerling JR, Wolfs RC, Hofman A, Grobbee DE, JongPT. The prevalence of primary open-angle glaucoma in apopulation-based study in The Netherlands. Ophthalmology1994;101(11):1851–5.
17. Mitchell P, Smith W, Attebo K, Healey PR. Prevalence of open-angleglaucoma in Australia. The blue mountains eye study. Ophthalmology1996;103(10):1661–9.
18. Varma R, Ying-Lai M, Francis BA, Nguyen BB, Deneen J, Wilson MR,et al. Prevalence of open-angle glaucoma and ocular hypertension inLatinos: the Los Angeles latino eye study. Ophthalmology2004;111(8):1439–48.
19. Wensor MD, McCarty CA, Stanislavsky YL, Livingston PM, Taylor HR.The prevalence of glaucoma in the Melbourne visual impairmentproject. Ophthalmology 1998;105(4):733–9.
20. Fleischman D, Berdahl JP, Zaydlarova J, Stinnett SS, Fautsch MP,Allingham RR. Cerebrospinal fluid pressure decreases with older age.PLoS ONE 2012;7(12):e52664.
21. Morgan WH, Chauhan BC, Yu DY, Cringle SJ, Alder VA, House PH.Optic disc movement with variations in intraocular and cerebrospinalfluid pressure. Invest Ophthalmol Vis Sci 2002;43(10):3236–42,PubMed PMID: 12356830. Epub 2002/10/03. eng.
22. Morgan WH, Yu DY, Cooper RL, Alder VA, Cringle SJ, Constable IJ.The influence of cerebrospinal fluid pressure on the laminacribrosa tissue pressure gradient. Invest Ophthalmol Vis Sci1995;36(6):1163–72, PubMed PMID: 7730025. Epub 1995/05/01. eng.
23. Sommer A, Tielsch JM, Katz J, Quigley HA, Gottsch JD, Javitt J, et al.Relationship between intraocular pressure and primary open angleglaucoma among white and black Americans. The Baltimore eyesurvey. Arch Ophthalmol 1991;109(8):1090–5.
24. Suzuki Y, Iwase A, Araie M, Yamamoto T, Abe H, Shirato S, et al. Riskfactors for open-angle glaucoma in a Japanese population: the Tajimistudy. Ophthalmology 2006;113(9):1613–7.
25. Iwase A, Suzuki Y, Araie M, Yamamoto T, Abe H, Shirato S, et al. Theprevalence of primary open-angle glaucoma in Japanese: the Tajimistudy. Ophthalmology 2004;111(9):1641–8.
26. Newman-Casey PA, Talwar N, Nan B, Musch DC, Stein JD. Therelationship between components of metabolic syndrome and open-angle glaucoma. Ophthalmology 2011;118(7):1318–26.
27. Leske MC, Connell AM, Wu SY, Hyman LG, Schachat AP. Riskfactors for open-angle glaucoma. Arc Ophthalmol 1995;113(7):918–24.
28. Asrani S, Samuels B, Thakur M, Santiago C, Kuchibhatla M. Clinicalprofiles of primary open angle glaucoma versus normal tensionglaucoma patients: a pilot study. Curr Eye Res. 2011;36(5):429–35.
29. Pasquale LR, Willett WC, Rosner BA, Kang JH. Anthropometricmeasures and their relation to incident primary open-angleglaucoma. Ophthalmology 2010;117(8):1521–9.
30. Ramdas WD, Wolfs RC, Hofman A, Jong PT, Vingeling JR, JansoniusNM. Lifestyle and risk of developing open-angle glaucoma: theRotterdam study. Arch Ophthalmol 2011;129(6):767–72.
31. Ren R, Wang N, Zhang X, Tian G, Jonas JB. Cerebrospinal fluidpressure correlated with body mass index. Graefe’s Arch Clin ExpOphthalmol 2012;250(3):445–6.
32. Berdahl JP, Fleischman D, Zaydlarova J, Stinnett SS, Allingham RR,Fautsch MP. Body mass index has a linear relationship withcerebrospinal fluid pressure. Invest Ophthalmol Vis Sci2012;53(3):1422–7, PubMed PMID: 22323469. Pubmed CentralPMCID: 3339912.
33. Fleischman D, Allingham RR, Berdahl JP, Fautsch MP. Body mass,spinal fluid, and glaucoma. Ophthalmology 2011;118(6):1225–6,author reply 6.
34. Agapova OA, Kaufman PL, Hernandez MR. Androgen receptor andNFkB expression in human normal and glaucomatous optic nervehead astrocytes in vitro and in experimental glaucoma. Exp Eye Res2006;82(6):1053–9.
35. McComb GJ, Hyman S. Lymphatic drainage of cerebrospinal fluid inthe cat. In: Shapiro KMA, Portnoy H, editors. Hydrocephalus. NewYork, NY: Raven Press; 1984. p. 83–97.
36. McComb GJ, Hyman S. Lymphatic drainage of cerebrospinal fluid inthe primate. In: Johansson BB, Winder H, editors. Pathophysiology ofthe blood-brain barrier. New York City, NY: Elsevier SciencePublishers; 1990. p. 421–37.

CSFP and Glaucoma 105
37. Papaiconomou C, Zakharov A, Azizi N, Djenic J, Johnston M.Reassessment of the pathways responsible for cerebrospinal fluidabsorption in the neonate. Childs Nerv Syst 2004;20(1):29–36.
38. Zakharov A, Papaiconomou C, Koh L, Djenic J, Bozanovic-Sosic R,Johnston M. Integrating the roles of extracranial lymphatics andintracranial veins in cerebrospinal fluid absorption in sheep.Microvasc Res 2004;67(1):96–104.
39. Nagra G, Johnston MG. Impact of ageing on lymphatic cerebrospinalfluid absorption in the rat. Neuropathol Appl Neurobiol2007;33(6):684–91.
40. Edwards ME, Good TA. Use of a mathematical model to estimatestress and strain during elevated pressure induced lamina cribrosadeformation. Curr Eye Res 2001;23(3):215–25, PubMed PMID:11803484. Epub 2002/01/23. eng.
41. Hollander H, Makarov F, Stefani FH, Stone J. Evidence of constrictionof optic nerve axons at the lamina cribrosa in the normotensive eye inhumans and other mammals. Ophthalmic Res 1995;27(5):296–309,PubMed PMID: 8552370. Epub 1995/01/01. eng.
42. Jonas JB, Berenshtein E, Holbach L. Anatomic relationship betweenlamina cribrosa, intraocular space, and cerebrospinal fluid space.Invest Ophthalmol Vis Sci 2003;44(12):5189–95, PubMed PMID:14638716. Epub 2003/11/26. eng.
43. Jonas JB, Berenshtein E, Holbach L. Lamina cribrosa thickness andspatial relationships between intraocular space and cerebrospinal fluidspace in highly myopic eyes. Invest Ophthalmol Vis Sci2004;45(8):2660–5, PubMed PMID: 15277489. Epub 2004/07/28. eng.
44. Jonas JB, Mardin CY, Schlötzer-Schrehardt U, Naumann GO.Morphometry of the human lamina cribrosa surface. InvestOphthalmol Vis Sci 1991;32(2):401–5.
45. Lenfeldt N, Koskinen LO, Bergenheim A, Malm J, Eklund A.Cerebrospinal fluid pressure assessed by lumbar puncture agreeswith intracranial pressure. Neurology 2007;68:155–8.
46. Dubost C, Gouez AL, Zetlaoui PJ, Benhamou D, Mercier FJ,Geeraerts T. Increase in optic nerve sheath diameter induced byepidural blood patch: a preliminary report. Br J Anaesth2011;107(4):627–30.
47. Corbett JJ, Mehta MP. Cerebrospinal fluid pressure in normal obesesubjects and patients with pseudotumor cerebri. Neurology1983;33(10):1386–8.
48. Albeck MJ, Skak C, Nielsen PR, Olsen KS, Børgesen SE, Gjerris F. Agedependency of resistance to cerebrospinal fluid outflow. J Neurosurg1998;89(2):275–8.
49. May C, Kaye JA, Atack JR, Schapiro MB, Friedland RP, Rapoport SI.Cerebrospinal fluid production is reduced in healthy aging.Neurology 1990;40(3 Pt 1):500–3.
50. Redzic ZB, Preston JE, Duncan JA, Chodobski A, Szmydynger-Chodobska J. The choroid plexus cerebrospinal fluid system: fromdevelopment to aging. Curr Top Dev Biol 2005;71:1–52.
51. Serot JM, Béné MC, Faure GC. Choroid plexus, agingof the brain, and Alzheimer’s disease. Front Biosci 2003;8(May):515–21.
52. Faraci FM, Mayhan WG, Heistad DD. Effect of vasopressin onproduction of cerebrospinal fluid: possible role of vasopressin (V1)-receptors. Am J Physiol 1990;258(1 Pt 2), R94-8.
53. Frolkis VV, Kvitnitskaya-Ryzhova TY, Dubiley TA. Vasopressin,hypothalmo-neurohypophyseal system and ageing. Arch GerontolGeriatr 1999;29(3):193–214.
54. Karahalios DG, Rekate HL, Khayata MH, Apostolides PJ. Elevatedintracranial venous pressure as a universal mechanism inpseudotumor cerebri of varying etiologies. Neurology1996;46(1):198–202.
55. Sugerman HJ, DeMaria 3rd EJ, Nakatsuka M, Sismanis A. Increasedintra-abdominal pressure and cardiac filling pressures in obesity-associated pseudotumor cerebri. Neurology 1997;49(2):507–11.
56. Liu JH, Kripke DF, Hoffman RE, Twa MD, Loving RT, Rex KM, et al.Nocturnal elevation of intraocular pressure in young adults. InvestOphthalmol Vis Sci 1998;39(13):2707–12.
57. Mansouri K, Weinreb RN, Liu JH. Effects of aging on 24-hourintraocular pressure measurements in sitting and supine bodypositions. Invest Ophthalmol Vis Sci 2012;53(1):112–6.
58. Asrani S, Zeimer R, Wilensky J, Gieser D, Vitale S, Lindenmuth K.Large diurnal fluctuations in IOP are an independent risk factor inpatients with glaucoma. J Glaucoma 2000;9(2):134–42.
59. Starcevic VP, Morrow BA, Farner LA, Keil LC, Severs WB. Long-termrecording of cerebrospinal fluid pressure in freely behaving rats.Brain Res 1988;462(1):112–7.
60. Morrow BA, Starcevic VP, Keil LC, Severs WB. Intracranialhypertension after cerebroventricular infusions in conscious rats.Am J Physiol 1990;258(5 Pt 2), R1170-6.
61. Lin JS, Liu JH. Circadian variations in intracranial pressure andtranslaminar pressure difference in Sprague-Dawley rats. InvestOphthalmol Vis Sci 2010;51(11):5739–43.
62. Samuels BC, Hammes NM, Johnson PL, Shekhar A, McKinnon SJ,Allingham RR. Dorsomedial/Perifornical hypothalamic stimulationincreases intraocular pressure, intracranial pressure, and thetranslaminar pressure gradient. Invest Ophthalmol Vis Sci2012;53(11):7328–35, PubMed PMID: 23033392. Pubmed CentralPMCID: PMC3487489. Epub 2012/10/04. eng.
63. Pasquale LR, Loomis SJ, Kang JH, Yaspan BL, Abdrabou W, Budenz DL,et al. CDKN2B-AS1 genotype-Glaucoma feature correlations inprimary open-angle glaucoma patients from the United States. Am JOphthalmol 2012;S0002–9394(12):00552, Epub Oct 27 Epub aheadof print.
64. Wiggs JL, Yaspan BL, Hauser MA, Kang JH, Allingham RR, Olson LM,et al. Common variants at 9p21 and 8q22 are associated withincreased susceptibility to optic nerve degeneration in glaucoma.PLoS Genet 2012;8(4):e1002654, Epub 2012 Apr 26.
65. Rohr A, Jensen U, Riedel C, Baalen AV, Barsch MC, et al. MR imagingof the optic nerve sheath in patients with craniospinal hypotension.AJNR Am J Neuroradiol 2010;31(9):1752–7.
66. Rohr AC, Riedel C, Fruehauf MC, Baalen Av, Bartsch T, Hedderich J,et al. MR imaging findings in patients with secondary intracranialhypertension. AJNR Am J Neuroradiol 2011;32(6):1021–9.
67. Alperin N, Lee SH, Sivaramakrishnan A, Hushek SG. Quantifying theeffect of posture on intracranial physiology in humans by MRI flowstudies. J Magn Reson Imaging 2005;22(5):591–6.
68. Watanabe A, Horikoshi T, Uchida M, Ishigame K, Kinouchi H.Decreased diameter of the optic nerve sheath associated with CSFhypovolemia. AJNR Am J Neuroradiol 2008;29(5):863–4, Epub 2008Feb 29.
69. Watanabe A, Kinouchi H, Horikoshi T, Uchida M, Ishigame K. Effect ofintracranial pressure on the diameter of the optic nerve sheath. JNeurosurg 2008;109(2):255–8.
70. Degnan AJ, Levy LM. Pseudotumor cerebri: brief review of clinicalsyndrome and imaging findings. AJNR Am J Neuroradiol2011;32(11):1986–93.
71. Wang N, Xie X, Yang D, Xian J, Li Y, Ren R, et al. Orbital cerebrospinalfluid space in glaucoma: the Beijing intracranial and intraocularpressure (iCOP) study. Ophthalmology 2012;119(10):2065–73,PubMed PMID: 22749084. Epub 2012/07/04. eng.
72. Bäuerle J, Nedelmann M. Sonographic assessment of the optic nervesheath in idiopathic intracranial hypertension. J Neurol 2011;258(11):2014–9.
73. Rajajee V, Vanaman M, Fletcher JJ, Jacobs TL. Optic nerveultrasound for the detection of raised intracranial pressure.Neurocrit Care 2011;15(3):506–15.
74. Soldatos T, Chatzimichail K, Papathanasiou M, Gouliamos A.Optic nerve sonography: a new window for the non-invasiveevaluation of intracranial pressure in brain injury. Emerg Med J2009;26(9):630–4.
75. Magnaes B. Body position and cerebrospinal fluid pressure. Part 1:clinical studies on the effect of rapid postural changes. J Neurosurg1976;44(6):687–97.
76. Magnaes B. Body position and cerebrospinal fluid pressure. Part 2:clinical studies on orthostatic pressure and the hydrostatic indifferentpoint. J Neurosurg 1976;44(6):698–705.
77. Wall M. Idiopathic intracranial hypertension (pseudotumor cerebri).Curr Neurol Neurosci Rep 2008;8(2):87–93, PubMed PMID:18460275. Epub 2008/05/08. eng.
78. Wall M. Idiopathic intracranial hypertension. Neurol Clin2010;28(3):593–617.
79. Wall M, George D. Idiopathic intracranial hypertension: a prospectivestudy of 50 patients. Brain 1991;114(Pt 1A):155–80.
80. Givre SJ, Fleischman D. Intracranial hypertension in a patient usingtopical adapalene. J Neuroophthalmol 2008;28(2):156–8.
81. Abegg M, Fleischhauer J, Landau K. Unilateral papilledema aftertrabeculectomy in a patient with intracranial hypertension. KlinMonatsbl Augenheilkd 2008;225(5):441–2, PubMed PMID:18454392. Epub 2008/05/06. eng.
82. Kawasaki A, Purvin V. Unilateral optic disc edema followingtrabeculectomy. J Neuroophthalmol 1998;18(2):121–3, PubMedPMID: 9621269. Epub 1998/06/11. eng.

106 D. Fleischman, R.R. Allingham
83. Greenfield DS, Wanichwecharungruang B, Liebmann JM, Ritch R.Pseudotumor cerebri appearing with unilateral papilledema aftertrabeculectomy. Archives of ophthalmology 1997;115(3):423–6.
84. Fleischman D, Berdahl JP, Fautsch MP, Chesnutt DA, Allingham RR.Increasing intraocular pressure as treatment for papilledema. Exp EyeRes 2012. Accepted 27 Sep 2012. http://dx.doi.org/10.1016/j.exer.2012.09.008.
85. Berdahl JP, Yu DY, Morgan WH. The translaminar pressure gradientin sustained zero gravity, idiopathic intracranial hypertension, andglaucoma. Med Hypotheses 2012;79(6):719–24.
86. Radhakrishnan K, Ahlskog JE, Cross SA, Kurland LT, O’Fallon WM.Idiopathic intracranial hypertension (pseudotumor cerebri).Descriptive epidemiology in Rochester, Minn, 1976 to 1990. ArchNeurol 1993;50(1):78–80.
87. Durcan FJ, Corbett JJ, Wall M. The incidence of pseudotumorcerebri. Population studies in Iowa and Louisiana. Arch Neurol1988;45(8):875–7.
88. Mader TH, Gibson CR, Pass AF, Kramer LA, Lee AG, Fogarty J, et al.Optic disc edema, globe flattening, choroidal folds, and hyperopicshifts observed in astronauts after long-duration space flight.Ophthalmology 2011;118(10):2058–69, PubMed PMID: 21849212.Epub 2011/08/19. eng.
89. Berdahl JP, Fleischman D, Allingham RR, Fautsch M. Disc swellingand space flight. Ophthalmology 2012;119(6):1290.
90. Kim DH, Parsa CF. Space flight and disc edema. Ophthalmology2012;119(11):2420–1.