Embed Size (px)
Citation preview

AAiPNhrb
A
0©d
S
The Role of Anti–Tumor NecrosisFactor Receptor Agents in Cancer
Survivors: Does the Risk Justify the Benefit?
Paul Chapman, Lee Cranmer, W.G. Dixon, K.L. Hyrich, John R. Patterson, D.P.M. Symmons,
Mary Toporcer, and Michael J. Mastrangelorabtsflmptc
itocladsfmcnsicsftntoansstdo
wd
miqtooqtnvttlhsvrrtmctopv
T
C
umMwsIo1ecsm
At times we encounter clinical prob-lems for which there are no directly ap-plicable evidence-based solutions, butwe are compelled by circumstances toact. When doing so we rely on relatedevidence, general principles of bestmedical practice, and our experience.Each ”Current Clinical Practice” featurearticle in Seminars in Oncology de-scribes such a challenging presentationand offers treatment approaches fromselected specialists. We invite readers’comments and questions, which, withyour approval, will be published in sub-sequent issues of the Journal. It is hopedthat sharing our views and experienceswill better inform our management deci-sions when we next encounter similarchallenging patients. Please send yourcomments on the articles, your challeng-ing cases, and your treatment successesto me at [email protected]. Ilook forward to a lively discussion.
Gloria J. Morris, MD, PhDCurrent Clinical Practice Feature Editor
nti-tumor necrosis factor(TNF) receptor therapeutics,such as entanercept (Enbrel;
mgen, Thousand Oaks, CA), inflix-mab (Remicade; Centocor, Malvern,A), adalimumab (Humira; Abbott,orth Chicago, IL), and likely others,ave revolutionized the treatment ofheumatoid arthritis. Their use haseen successfully extended to other
ddress correspondence to Michael J. Mas-trangelo, MD, Ben Franklin House, Suite 314,834 Chestnut St, Philadelphia, PA 19107. E-mail: [email protected]
270-9295/10/$ - see front matter2010 Published by Elsevier Inc.
foi:10.1053/j.seminoncol.2010.01.001
eminars in Oncology, Vol 37, No 1, Februa
heumatologic diseases, plaque psori-sis, and most recently inflammatoryowel disease. The full spectrum ofhe utility of these immunosuppres-ive agents for the treatment of in-ammatory/autoimmune diseases re-ains to be defined. The number ofatients under chronic treatment withhese immunosuppressive agents willontinue to expand exponentially.
The association between chronicmmunosuppression, whether it bereatment (eg, organ transplantation)r disease (eg, human immunodefi-iency virus [HIV] infection, chronicymphocytic leukemia [CLL]) related,nd malignancy has been amplyocumented. Chronically immuno-uppressed patients are at greatest riskor developing lymphoma1–3 and skinalignancies, especially squamous
ell cancer4 and more recently mela-oma. Although less well de-cribed, the course of cancer in themmunosuppressed patient seems ac-elerated.5 Discontinuing immuno-uppression is not a realistic optionor organ transplant patients. Ratherhese patients are surveilled for malig-ancy and problems are dealt with ashey arise. Despite great advances inrgan transplantation, the limitedvailability of donor organs keeps theumber of patients at risk relativelymall. Although HIV infection is con-iderably more common, advances inhe treatment of the underlying con-ition should reduce the risk of sec-ndary malignancies.
Anti-TNF receptor therapy like-ise has been associated with theevelopment of malignancy and of-
ers several unique challenges. The bry 2010, pp 11-19
echanism of immunosuppressions unique in that it is the conse-uence of targeting a specific signalransduction pathway. At presentne can only speculate as to whetherr not this will alter the pattern (fre-uency, time course, histological
ypes) of second malignancies. Theumber of patients in harm’s way isast and rapidly expanding. The risko these patients goes well beyondhat of developing a new primary ma-ignancy, as many individuals willave had a prior cancer and, althougheemingly disease-free, will harbor aariably definable likelihood of recur-ence. These patients also will be atisk for developing a second cancer ofhe same histology or an associatedalignancy (eg, breast and ovarian
ancers). Since anti-TNF receptorherapy can be considered “optional,”ncologists are being asked to ap-rove such therapy in cancer survi-ors.
HE PROBLEM
ase Report
A 52-year-old woman (DOB 1955)nderwent excision of a deeply pig-ented mid-sternal skin lesion onay 26, 1998 (her age 43), whichas interpreted as a superficial
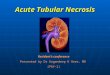
preading melanoma of Clark’s levelI invasion and a Breslow thicknessf 0.3 mm (Figure 1). On June 12,998, the area was more widely re-xcised and the surgical defect waslosed primarily. There was no re-idual disease in the biopsy speci-en. She was followed on a regular
asis since that time primarily for
11

tmttsf2n1ihtci
d(depf
ysrstmghaptam
vbtrrg
srfisrwta3
wtlotmaooumotosrfot5wntccticle
otm
Fmt verv
12 P. Chapman et al
he development of a second pri-ary cutaneous melanoma. The pa-
ient had multiple clinically dysplas-ic nevi. An excisional biopsy ofingle dysplastic nevi was per-ormed in May 1998 and in May001, and another two dysplasticevi were removed on December5, 2005. Her last routine visit was
n September 2007, at which time aemogram, liver function chemis-ries, lactate dehydrogenase, andhest x-ray failed to indicate any ev-dence of metastatic melanoma.
In 1978 (age 23) the patient wasiagnosed with antinuclear antibodyANA)-positive rheumatoid arthritisuring her first pregnancy. The dis-ase was controlled initially withrednisone, hydroxychloroquine sul-
igure 1. Superficial spreading melanm with melanophages and a patchy
oxylin & eosin stain) (A) Low-power o
ate, and minocycline. In 1999, one u
ear after the diagnosis of melanoma,he experienced a flare-up of herheumatoid arthritis. A discussion en-ued regarding the safety of initiatingherapy with an anti-TNF receptoredication. Because of concern re-
arding the possible exacerbation ofer melanoma, parenteral gold ther-py was initiated instead. Because ofersistent symptoms, anti-TNF recep-or therapy was started in 2001. Shechieved an excellent and durable re-ission.The patient did well until she de-
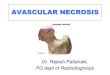
eloped what clinically appeared toe a sinusitis that failed to respondo conservative therapy. A chest x-ay performed on January 8, 2008evealed a right hilar mass and sug-ested multiple lung nodules (Fig-
. Clark’s level II, Breslow thickness 0.3hocyte infiltrate in the dermis (hema-
iew; (B) higher power.
re 2). A computed tomography
can confirmed the presence of theight hilar mass and more clearly de-ned multiple pulmonary nodulesuggestive of lung cancer. On Feb-uary 8, 2008, the patient under-ent a left upper lobe wedge resec-
ion that revealed three foci ofdenocarcinoma of the lung (Figure). Systemic therapy was initiated.
This patient with dysplastic nevias diagnosed with rheumatoid ar-
hritis well before the diagnosis of aow-risk melanoma. She was underncologic surveillance primarily forhe development of a second pri-ary cutaneous melanoma, as well
s for the unlikely recurrence of theriginal melanoma. With the devel-pment of disabling and otherwisenmanageable symptoms of rheu-atoid arthritis, the patient’s oncol-
gist was asked if anti-TNF receptorherapy was permissible. The oncol-gist agreed to treatment and inten-ified surveillance for possible recur-ence of the melanoma, as well asor lymphoma and a second cutane-us malignancy. The rheumatoid ar-hritis promptly remitted. More than
years elapsed without problemsith lymphoma or with her mela-oma. Several months after a rou-ine check up (to include a normalhest x-ray), the patient developed aough unresponsive to conservativeherapy. A chest x-ray revealed find-ngs consistent with a primary lungancer widely metastatic within theungs. Biopsy confirmed the pres-nce of adenocarcinoma of the lung.
Various experts were asked topine on the management of this pa-ient, and where appropriate com-ent on the following issues:
(1) Was the “explosive” develop-ment of adenocarcinoma ofthe lung in this nonsmokingfemale from a nonsmokinghousehold consequent to theanti-TNF receptor therapy orsimply a known pattern ofpresentation of the disease?
(2) Would you have approvedthe use of anti-TNF receptortherapy in this patient with oth-
omalymp
erwise unresponsive and dis-

R
tdsberteps
ohsaget
mblntn
wmwto
ttaotgttbgqcafwWado
mha
fnt
aeil
MO
wadwtirucailrtvltscTttcatsntaiwstg
Fa lung
Anti-TNF receptor agents in cancer survivors 13
abling rheumatoid arthritiswith a very-low-risk melanoma(albeit it with dysplastic nevi)and no special risk for anyother solid tumor?
(3) Had you approved the use ofanti-TNF receptor therapy,how would you have moni-tored the patient for malig-nancy, if at all?
(4) Would you now discontinuethe anti-TNF receptor therapy?
HEUMATOLOGIST’S OPINION
With regard to the case report,he onset of rheumatoid arthritisuring pregnancy is unusual. It wastated that she was ANA-positive,ut no mention is made of the pres-nce of rheumatoid factor or, moreecently anti-cyclic citrullinated pep-ide (anti-CCP) antibodies. The dis-ase was initially controlled withrednisone, hydroxychloroquineulfate, and minocycline.
In May 1998 she had an excisionf a melanoma and subsequently hasad very careful follow-up. In 1999,he had a flare-up of her rheumatoidrthritis. A discussion ensued re-arding the safety of the TNF block-rs and she was given a trial of gold
igure 2. Chest x-ray. Posteroanteriorble pulmonary nodules suggestive of
herapy. With failure of gold treat- r
ent, she was then given a TNFlocker and she achieved an excel-
ent and durable remission. Unfortu-ately, 8 years later she developedhe explosive onset of adenocarci-oma of the lung.
I cannot proffer an opinion as tohether the “explosive” develop-ent of adenocarcinoma of the lungas consequent to the anti-TNF
herapy or simply a known patternf presentation of the disease.
Approval of the use of anti-TNFherapy in this patient involves ob-aining more information than isvailable in the case report. Obvi-usly her physicians were reluctanto use this therapy since a course ofold therapy was administered ini-ially. Had she been off all medica-ion when she developed an exacer-ation of her disease, I would haveiven her prednisone, hydroxychloro-uine sulfate, and possibly minocy-line (along with osteoporosis ther-py) for 4 to 6 months with carefulollow-up. With no improvement, Iould have added methotrexate.ith no improvement on methotrex-
te, I would have added an anti-TNFrug therapy. I would try to stretchut the therapy and attempt to inter-
showing a right hilar mass and prob-cancer.
upt treatment after several months. If a
y concerns were met, I would notesitate to use the anti-TNFs in thebove situation.
As regards monitoring the patientor malignancy, I would have doneothing beyond what was done inhe report.
Finally, uncontrolled rheumatoidrthritis is a terrible problem. I wouldxplore treatments that were compat-ble with optimal treatment for herife-limiting lung cancer.
John R. Patterson, MDDepartment of Medicine
Jefferson Medical CollegePhiladelphia, PA
EDICALNCOLOGIST’S OPINION
Anti-TNF antibodies have becomeidely used for rheumatoid arthritis
nd other serious autoimmune con-itions. Data from cohort studies asell as meta-analyses of randomized
rials suggest that anti-TNF antibod-es are associated with an increasedisk of malignancies. There is somencertainty as to which malignan-ies may be more commonly associ-ted with these agents; reports havendicated increased rates of hemato-ogical and solid tumors. In the cur-ent case report, a woman beingreated for rheumatoid arthritis de-eloped metastatic non-small cellung cancer despite no previous his-ory of smoking. If I had been con-ulted on this case, I would haveoncurred with the use of the anti-NF therapy given the severity of
he rheumatoid arthritis. Given thathe absolute increase in malignan-ies associated with treatment withnti-TNF drugs appears to be rela-ively low, and the fact that non-mall cell lung cancer can arise inonsmokers, there is no way to de-ermine whether the anti-TNF ther-py contributed to the lung cancern this particular case. I think it
ould be hard to justify aggressivecreening for malignancies in pa-ients receiving anti-TNF therapyiven how low the absolute risk is
view
nd given that there is no consensus

as
twimaperbmtcitctdm
tsnrt
MO
aele
yf2mca
igaasc(annrihoc
tlWrrhmtm
guttPagtctstotasrpteaa
Fmt
14 P. Chapman et al
s to which type of malignancieshould be targeted for screening.
In this particular case, in the set-ing of metastatic lung cancer, Iould seriously consider discontinu-
ng the anti-TNF treatment. Mouseodels have suggested that tumors
rising in severely immunosup-ressed hosts failed to be “immuno-dited” by the immune system.6 As aesult, these tumors can potentiallye recognized and rejected by a nor-al immune system. This is in con-
rast to tumors that arise in immuno-ompetent mice that have beenmmuno-edited and are ignored byhe immune system. In the currentase report, the lung cancer arose inhe setting of immunosuppressionue to the anti-TNF antibody treat-
igure 3. Histopathology of a lung noducin production (hematoxylin & eosin
hyroid transcription factor 1 (TTF1).
ent. It is possible that this lung a
umor is unedited by the immuneystem and that removing the immu-osuppression could result in tumoregression. I believe it would cer-ainly be worth a try.
Paul Chapman, MDDepartment of Medicine
Memorial Sloan-Kettering CancerCenter
New York, NY
EDICALNCOLOGIST’S OPINION
The index patient had a history ofstage I melanoma on the sternum
xcised in 1998. She also had aong history of rheumatoid arthritis,ventually requiring therapy with an
(A) High power—gland formation andin). (B) Immunohistology—positive for
nti- TNF antibody. TNF blockade r
ielded a substantial improvementor the patient after initiation in001. Unfortunately, she developedultifocal non-small cell lung can-
er in 2008, requiring systemic ther-py.
This case highlights a number ofssues faced by practicing oncolo-ists relating to anti-TNF therapy,nd more generally by the class ofgents referred to as biological re-ponse modifiers. Three very clini-al questions are raised by this case:1) What is the risk of using thesegents in a patient with a prior diag-osis of cancer, in this case, mela-oma; (2) What is the overall cancerisk associated with anti-TNF agentsn patients without a prior canceristory; and (3) What is the impactf these agents on the course of can-er once it subsequently develops?
To reliably assess and balancehese risks, both the severity and like-ihood of the risk must be known.
hile some estimate of the severity ofisks can be undertaken, almost noeliable data exist regarding the likeli-ood of the risks. Therefore, recom-endations regarding anti-TNF use at
he present must rely on clinical judg-ent.We have faced the first issue, re-
arding the advisability of anti-TNFse for rheumatoid arthritis in pa-ients with a prior melanoma his-ory, in our Cutaneous Oncologyrogram Clinic. Typically, patientsre referred to us by rheumatolo-ists for oncologic “clearance” prioro receiving anti-TNF therapy. Theompeting risks to be weighed arehe risk of recurrent melanoma ver-us the risk of inadequately con-rolled rheumatoid arthritis. Whilencologists may tend to focus onhe consequences of recurrent mel-noma, one must not discount theevere consequences of progressiveheumatoid arthritis: severe chronicain, debility due to joint destruc-ion, and even mortality due to sideffects of alternative medicationsnd secondary effects of rheumatoidrthritis itself.
At present, data regarding the
ule.sta
isk of reactivation of melanoma in

asaatpniwiucttTe
gmibtptpnsmawwrvdahrapkuptmt
taoeimevipn
wnt1apdymaasca
rmncmtcssoasmAfanrtrmpvrcsibrntamptmytnni
sckm
motadediseoad
srTttetdgmWpcOwrrhcctc
oexbtldrtldpad
Anti-TNF receptor agents in cancer survivors 15
nti-TNF–treated patients consists ofeveral case reports.7 Assuming mel-noma in reported cases reflects re-ctivation of known previouslyreated melanoma and not an occultrimary lesion, the reference mela-oma lesion had not been cured by
nitial surgical treatment. Whether itould have recurred when it did,
rrespective of anti-TNF therapy, isnknown. While there are biologi-ally plausible reasons that reactiva-ion of melanoma could occur underhe immunological influence of anti-NF therapy, this remains a hypoth-sis.
Clinically, the likelihood of aiven patient’s melanoma recurringust be balanced against the sever-
ty of disease warranting anti-TNFlockade. Perhaps the most impor-ant component is educational: theatients must be aware of the limi-ations of our available data and theotential risks associated with mela-oma recurrence, including the pos-ibility of death due to metastaticelanoma. Patients with stage III mel-
noma and a high recurrence risk mayeigh the risks differently than thoseith a low, but not zero, recurrence
isk. Similarly, those with severe ad-anced rheumatoid arthritis or otheriseases responsive to anti-TNF ther-py may be more inclined to accept aigher theoretical risk of melanomaecurrence versus patients with lessggressive disease and perhaps unex-lored therapeutic alternatives. Theey point is that adequate patient ed-cation (and, for medico-legal pur-oses, documentation of that educa-ion) is critical to allow the patient toake an informed decision regarding
he use of these remarkable therapies.The US Food and Drug Administra-
ion has recognized that TNF block-de is associated with increased riskf malignancy (see package inserts forntanercept, dated April 2009; inflix-mab, dated April 2009; and adali-
umab, dated March 2009). How-ver, the absolute risks are actuallyery small. For example, in random-zed controlled trials of infliximab, 14atients were diagnosed with malig-
ancies, the most common of which tere breast, colorectal, and mela-oma, among 4,019 infliximab-
reated patients versus one among,597 controls (0.52/100 patient-yearsmong infliximab-treated v 0.11/100atient-years among controls). Me-ian follow-up period was about 0.5ears and thus the malignancy riskay increase over time. Similar data
re presented for entanercept anddalimumab. These data suggest thatome cancer cases are probably asso-iated with anti-TNF therapy, but thebsolute risk is low.
Complicating this discussion inegards to melanoma is the potentialelanoma risk associated with alter-
ative therapies for rheumatologiconditions. Methotrexate is com-only prescribed for rheumatoid ar-
hritis. As it has been in use for de-ades, methotrexate is unlikely to beubjected to large-scale controlled as-essment, preventing the acquisitionf safety data comparable to that fornti-TNF antibodies. Several retro-pective studies of the cancer risk ofethotrexate have been undertaken.study from Australia indicated a 1.5-
old increased risk of malignancy, andthreefold increase in risk of mela-
oma among methotrexate-treatedheumatoid arthritis patients versushe general population.8 Another ret-ospective study compared risk ofalignancy in rheumatoid arthritisatients treated with methotrexateersus those treated with biologicalesponse modifiers, including etaner-ept, infliximab, or adalimumab.9 Thetudy examined 7,306 patients receiv-ng methotrexate and 1,152 receivingiological response modifiers. Theisk of hematologic and solid malig-ancies, including melanoma, was sta-istically indistinguishable. Again, thebsolute risk was small: for solid tu-ors, the risk was 1.6 malignancieser 100 person-years of use amonghose treated with biological responseodifiers versus 1.8 per 100 person-
ears for methotrexate-treated pa-ients. In general, the risk of mela-oma or other solid tumors shouldot prevent use of anti-TNF therapy, if
t is likely to be beneficial. An excep-
ion might be patients with a knownyndrome increasing melanoma orancer risk, such as a family withnown p16 mutations associated withelanoma.Finally, what is the course of a
alignancy, such as melanoma,nce it develops in patients activelyreated with anti-TNF blockade? Were again faced with lack of reliableata. Given the association with dis-ase development, it would be pru-ent to discontinue anti-TNF therapyn such patients. Further therapyhould be undertaken according tostablished oncologic principles, basedn the type of malignancy, its stage,nd the patient’s general medical con-ition.
The index patient under discus-ion had a low risk of melanomaecurrence after primary treatment.he patient had progressive rheuma-
oid arthritis and even underwent aherapeutic trial of an alternative, par-nteral gold, prior to using anti-TNFherapy. Other than the presence ofysplastic nevi, she has no history sug-esting an underlying syndrome ofarkedly increased melanoma risk.e would thus advise her that her
rior melanoma history was not aontraindication to anti-TNF therapy.ngoing monitoring in this patientould have involved screening
elated to her melanoma history (pe-iodic skin examinations, directedistory and physical examinations,hest-x-ray) and age/sex-appropriateancer screening (breast examina-ion, possibly mammography, cervi-al cancer screening).
This nonsmoking patient devel-ped non-small cell lung cancer. Inter-stingly, this was detected on a chest-ray in January 2008, and had noteen present on a prior study of Sep-ember 2007. By the time of histo-ogic diagnosis in February 2008, theisease was apparently unresectable,equiring systemic therapy. Whetherhis aggressive disease course was re-ated to anti-TNF therapy or coinci-ental is unknown, but it would berudent to discontinue anti-TNF ther-py after the diagnosis of metastaticisease.
In conclusion, this case illustrates

ivldtitfaiititti
E
imwwtpflcdrcimawnaeavmlwms
tuthT
rpcctoadeefrolsapbctcbmealtcttwtw
membeitperinatmtwtsmTd
laSlathtsfattagn
wawitpftpaRpTdaTnmD2obmmowmsen
aTtncoTr
16 P. Chapman et al
mportant issues for oncologists in ad-ising patients about the use of bio-ogical response modifiers. Definitiveata regarding the oncologic risks ofhese therapies are lacking, especiallyn those with a prior history of cura-ively treated cancer and in those suf-ering a disease recurrence. More reli-ble data may be acquired by thenstitution of prospective patient reg-stries composed of those beingreated with anti-TNF therapy. As newmmune-modifying agents are addedo the pharmacopoeia, these ques-ions will continue to face oncologistsn their clinical practices.
Lee D. Cranmer, MD/PhDSkin Cancer Institute
Arizona Cancer CenterUniversity of Arizona
Tucson, AZ
PIDEMIOLOGISTS’ OPINION
This case report provokes manynteresting questions. Is the risk of
elanoma increased in patientsith rheumatoid arthritis? If so,hat is the relative contribution of
he disease itself and its immunosup-ressive treatments? What is the in-uence of anti-TNF therapy uponancer incidence? More specifically,oes anti-TNF therapy increase theisk of new incident malignancy (in-luding recurrence and metastasis)n patients who have a prior treated
alignancy? And can anti-TNF ther-py be continued safety in patientsho develop an incident malig-ancy? The first two questions haven existing evidence base, reviewedlsewhere.10 The third question ismassing more literature.11 Con-ersely, the evidence base for the re-aining questions is scarce. Nonethe-
ess, clinicians repeatedly wrestleith similar clinical scenarios andust make treatment decisions de-
pite the paucity of evidence.Is it even possible to determine
he influence of anti-TNF therapypon the risk of malignancy in pa-ients with rheumatoid arthritis whoave a prior malignancy? When anti-
NF therapy was tested in phase III randomized controlled trials (RCTs),rior malignancy was often an ex-lusion criterion.12–14 Such RCT dataannot therefore address this ques-ion. British Society for Rheumatol-gy (BSR) guidelines for the use ofnti-TNF therapy in the United King-om were necessarily based uponxpert opinion rather than clinicalvidence. The theoretical potentialor anti-TNF therapy to increase theisk of malignancy15 and the absencef any relevant data from the RCTs
ed to the advice that: “cautionhould be exercised in the use ofnti-TNF therapies in patients withrevious malignancy. The potentialenefits of treatment need to beonsidered against the risks relatedo potential recurrence of the spe-ific malignancy. If patients haveeen free of any recurrence of theiralignancy for 10 years there is no
vidence for a contraindication tonti-TNF therapy.”16 Similar guide-ines were adopted in other coun-ries. Thus any observational studyonducted after the introduction ofhese guidelines can only addresshe question by analyzing patientsith prior malignancy who, despite
he guidelines, have been treatedith anti-TNF therapy.Several European academic rheu-
atology biologics registers werestablished since 2001 with the pri-ary aim of addressing the safety of
iologic therapy in rheumatic dis-ases.17 The findings of these stud-es, with respect to the above scien-ific question, have so far only beenublished in abstract form.18,19 Thearly findings appear reassuring: theate of new or recurrent malignancyn patients with prior malignancy isot higher in patients treated withnti-TNF therapy compared to tradi-ional disease-modifying anti-rheu-atic drugs (DMARDs). It is impera-
ive that these results are interpretedith great caution, evaluating the po-
ential biases and confounders of ob-ervational studies. Patients with prioralignancy selected to receive anti-NF treatment may be systematicallyifferent in their risk of new or recur-
ent malignancy than patients se- tected not to receive anti-TNF ther-py, introducing a selection bias.econd, results cannot be extrapo-ated to inform treatment decisionsbout patients with prior malignancyhat clinicians would not previouslyave considered treating. Such pa-ients are not represented in thetudy, and may behave differentlyrom those included. Third, the aver-ge follow-up time is still short inhese studies. Reassuring findings af-er only a few years may not hold truefter longer follow-up, particularlyiven the long latency of some malig-ancies.
Bearing in mind these limitations,e can be relatively reassuring that,
ssuming the clinician has carefullyeighed up the risk and the benefit
n the individual patient, anti-TNFherapy may be given to someatients with prior malignancy. Un-
ortunately, there is a signal that pa-ients with prior melanoma have aoorer outcome when treated withnti-TNF therapy. The BSR Biologicsegister reported 17 patients withrior melanoma who received anti-NF therapy. Three of 17 patientseveloped incident cancers after anverage follow-up time of 3 years.his compared to no incident malig-ancies in 10 patients with priorelanomas treated with traditionalMARD therapy after an average ofyears’ follow-up.19 The possibility
f a causal relationship is supportedy the finding that anti-TNF therapyight increase the risk of de novoelanoma,20 and that supraphysi-
logical doses of TNF have been usedith melphalan for the treatment ofelanoma.21 This emerging signal
uggests that particular caution is nec-ssary for patients with prior mela-oma considering anti-TNF therapy.
There is no existing literaturebout the safety of continuing anti-NF therapy in patients with rheuma-
oid arthritis who develop a malig-ancy while on treatment. However,hemotherapy for malignancy oftenbviates the need for ongoing anti-NF therapy, where control of activeheumatoid arthritis is a byproduct of
he cancer immunosuppression. Be-
ysTastdw
D
ritocc
pcwtsiwdtlsalmFmfnnrsoccrpcnh
aatakcttrtbntrcaoiT
ttctb5ndtwdwdtaiaroOtscotqwac“nftwy
btnsosmdn2pnwlbsitnpyytaaat
crmsbai
S
ammssgbarcto
Anti-TNF receptor agents in cancer survivors 17
ond the rheumatology literature,tudies examining the benefit of anti-NF therapy in patients with cancer-ssociated anorexia may also provideome reassurance for continuingreatment in patients with rheumaticisease who develop malignancieshile on therapy.
William G. Dixon, MRCP, PhDKimme L. Hyrich, MD, PhD,
FRCPCDeborah P.M. Symmons, MD,
FFPH, FRCPEpidemiology Unit
The University of ManchesterManchester, UK
ERMATOLOGIST’S OPINION
I believe all dermatologists andheumatologists would agree thatnhibition of the immune responseo improve the signs and symptomsf an autoimmune disease also de-reases the body’s ability to combatertain types of malignancies.
In my 20 years of dermatologyractice, now focusing primarily onutaneous oncology, the frequencyith which I encounter the devas-
ating effects of immunosuppres-ion has increased dramatically. Its clear that immunosuppression,
hether it is disease- (HIV, CLL),rug- (anti-rejection agents, chemo-herapeutic agents) or radiation-re-ated, may cause profound progres-ion of cutaneous malignancies. Inddition, treatment of a primary ma-ignancy may result in the develop-
ent of a secondary malignancy.or example, secondary leukemiasay occur as a result of the therapy
or breast carcinoma, ovarian carci-oma, and lymphomas. Therefore, aotable increase in clinical responseates with newer immunosuppres-ive treatment regimens is not with-ut its risks. This dilemma is suc-inctly demonstrated in the presentase report. At this time, there is noeasonable explanation for the “ex-losive” development of adenocar-inoma of the lung in this patient, aonsmoker not exposed to second-
and smoke. cAlthough difficult to assign an ex-ct cause–effect relationship to thenti-TNF receptor therapy, one cer-ainly must maintain a heightenedwareness to this probability. Wenow that TNF is essential in theausation of vascular necrosis, inurn causing an ischemic insult toumor cells. Likewise, TNF-� has di-ect cytotoxic effects mediated byhe apoptosis pathway on suscepti-le tumor cells. It may stimulate in-ate immunity, induce inflamma-ion, inhibit tumorogenesis and viraleplication, and also increase tumoroncentrations of coadministeredntineoplastic drugs. A recent studyn aging and decreased cutaneous
mmunity22 suggests insufficientNF-� as one possible mechanism.
How do clinicians manage pa-ients today, with the uncertainty ofhe role of TNF-� in each individualancer? I would also have approvedhe use of an anti-TNF receptorlocker as therapy for a young (age4), otherwise healthy (thin mela-oma 9 years prior, nonsmoker, ar-ent follower of good health main-enance and prevention) femaleith an almost 30-year history of aebilitating autoimmune disorderho had tried and failed many stan-ard first-, second-, and third-linereatments. The use of an approvednd available TNF-� blocking agentmproves quality of life. Shechieved an excellent and durableemission but 7 years later devel-ped a life-threatening malignancy.f course there is cause for concern
hat her drug therapy promoted aecondary malignancy. These con-erns are outlined in the discussionn the biology of TNF-� above. Therue dilemma is not whether she re-uired this course of therapy, butas there a “safer” alternative? If the
nswer is “no” then we, as physi-ians, must assist our patients withthe hands they are dealt.” I wouldot have seen this particular patientor skin screening more frequentlyhan every 6 months, unless thereas an urgent concern. After 10
ears disease-free, she would re-
eive yearly total body skin checks tased on her melanoma history. Athis time, I do not monitor nonmela-oma or melanoma patients athorter intervals based on their usef biological agents. Standardcreening for thin melanoma (� 1m in thickness) survivors does not
ictate yearly chest x-ray studies. Aormal chest x-ray in September007 and the development of an ex-losive cancer in January 2008 sig-al both physicians and patientsith the reality that secondary ma-
ignancies may occur and they cane very aggressive. I do not sub-cribe to the use of an unnecessarymmunosuppressive agent in a pa-ient with a life-threatening malig-ancy, until I am certain that theatient will survive for at least 2ears and more conservatively, 5ears. If they do survive, reintroduc-ion of a TNF-� blocker needs to bemutual agreement between doctornd patient if no alternative accept-ble therapies are available at thatime.
The truth remains that cancer is aomplex disease. We must weight theisks of cancer recurrence, develop-ent of secondary malignancy, and
everity of the underlying illnessefore utilizing immunosuppressivegents in our treatment armamentar-um.
Mary Toporcer, MDDermatology and Dermatologic
SurgeryDoylestown, PA
UMMARY AND ASSESSMENT
The introduction of anti-TNFgents into the therapeutic arma-entarium for a variety of “autoim-une” diseases seemingly has re-
ulted in a dramatic improvement inymptoms and arrest of disease pro-ression. This impressive clinicalenefit has fueled the use of thesegents placing a vast population atisk for toxicity. Concurrent in-reases in the incidences of manyypes of cancer and in the numberf cancer survivors make it inevitable
hat questions will be asked of oncolo-
gitstcra
waavhOetrcpbocttfiamrsbaatctDE(lswaR
ttbtttdmtsmc
afbtcdt
R
1
1
1
1
1
1
1
1
1
1
2
18 P. Chapman et al
ists regarding the advisability of us-ng of anti-TNF agents in these pa-ients who also have clinicallyignificant autoimmune disease. Inhe absence of adequate data, clini-ians will have to rely on their expe-ience and their judgment to informnd advise patients.
This case typifies the patient abouthom oncologists will be consulted:cancer survivor with a debilitating
utoimmune disease resistant to con-entional therapy but predictablyighly responsive to anti-TNF therapy.f the multiple factors to be consid-red, the one of greatest concern andhe simplest to define is the risk ofecurrence of the previously treatedancer in the absence of immunosup-ressive therapy. Also assessable, al-eit much less precisely so, is the riskf developing a second but unrelatedancer. However, in almost all caseshis risk will be substantially less thanhat of recurrence. Even less well de-ned is the impact of anti-TNF ther-py on these risks. As cited by Cran-er and by Dixon et al above, this
isk, although imprecisely definedeems none the less minimal. Also toe considered are the severity of theutoimmune disease, alternative ther-pies if any, and the anticipated dura-ion of treatment, which is usuallyhronic. These factors are similar tohose employed by the US Food andrug Administration in their Riskvaluation and Mitigation StrategyREMS) for postmarketing surveil-ance of drugs and biologicals to as-ure that the agent’s benefits out-eigh the risks.23 Anti-TNF agents are
mong the drugs with approvedEMS programs.
Typically, anti-TNF therapy con-rols the symptoms but does not curehe disease. Thus treatment tends toe chronic. In the cancer survivor,he goal is to achieve reasonable con-rol of the autoimmune disease withhe least immunosuppression (lowestose and shortest duration of treat-ent). When treatment is protracted,
he interspersion of drug-free intervalshould be considered. The patient isonitored for the anticipated can-
er-related risks. In patients under
ctive treatment for cancer, the needor anti-TNF therapy may be obviatedy the immunosuppressive effects ofhat therapy. When that does not oc-ur, perhaps the decision to re-intro-uce anti-TNF therapy is best left tohe informed patient.
Michael Mastrangelo, MDDepartment of Medical Oncology
Jefferson Medical CollegePhiladelphia, PA
EFERENCES1. Wolfe F, Michaud K. Lymphoma in
rheumatoid arthritis. The effect ofmethotrexate and anti-tumor necro-sis factor therapy in 18,572 patients.Arthritis Rheum. 2004;50:1740–51.
2. Weyad CM, Goronzy JJ, Kurtin PJ.Editorial—lymphoma in rheuma-toid arthritis. An immune sysem setup for failure. Arthritis Rheum.2006;54:685–9.
3. Van Vollenhoven RF. Benefits andrisks of biological agents. Lymphoma.Clin Exp Rheumatol. 2004;22 suppl35:S122–5.
4. Setoguchi S, Solomon DH, Weinb-latt ME, et al. Tumor necrosis factoralpha antagonist use and cancer inpatients with rheumatoid arthritis.Arthritis Rheum. 2006;54:2757–64.
5. Fulchiero GJ, Salvaggio H, DrabickJJ, et al. Eruptive latent metastaticmelanomas after initiation of antitu-mor necrosis factor therapies. J AmAcad Dermatol. 2007;56:S65–7.
6. Dunn GP, Old LJ, Schreiber RD. Theimmunobiology of cancer immuno-surveillance and immunoediting.Immunity. 2004;21:137–48.
7. Fulchiero GJ Jr, Salvaggio H, Drab-ick JJ, et al. Eruptive latent meta-static melanomas after initiation ofantitumor necrosis factor therapies.J Am Acad Dermatol 2007;56 Suppl:S65–7.
8. Buchbinder R, Barber M, Huezenroe-der L, et al. Incidence of melanomaand other malignancies among rheu-matoid arthritis patients treated withmethotrexate. Arthritis Rheum. 2008;59:794–9.
9. Setoguchi S, Solomon DH, WeinblattME, et al. Tumor necrosis factor al-pha antagonist use and cancer in pa-tients with rheumatoid arthritis. Ar-thritis Rheum. 2006;54:2757–64.
0. Chakravarty EF, Farmer ER. Risk of
skin cancer in the drug treatment ofrheumatoid arthritis. Expert OpinDrug Safety. 2008;7:539–46.
1. Askling J, Bongartz T. Malignancyand biologic therapy in rheumatoidarthritis. Curr Opin Rheumatol.2008;20:334 –9.
2. Maini R, St Clair EW, Breedveld F, etal. Infliximab (chimeric anti-tumournecrosis factor alpha monoclonal an-tibody) versus placebo in rheumatoidarthritis patients receiving concomi-tant methotrexate: a randomisedphase III trial. ATTRACT StudyGroup. Lancet. 1999;354:1932–9.
3. Bathon JM, Martin RW, Fleisch-mann RM, et al. A comparison ofetanercept and methotrexate inpatients with early rheumatoid ar-thritis. N Engl J Med. 2000;343:1586 –93.
4. Keystone EC, Kavanaugh AF, SharpJT, et al. Radiographic, clinical, andfunctional outcomes of treatmentwith adalimumab (a human anti-tu-mor necrosis factor monoclonal an-tibody) in patients with active rheu-matoid arthritis receivingconcomitant methotrexate therapy:a randomized, placebo-controlled,52-week trial. Arthritis Rheum.2004;50:1400–11.
5. Balkwill F. Tumor necrosis factor ortumor promoting factor? CytokineGrowth Factor Rev. 2002;13:135–41.
6. Ledingham J, Deighton C. Updateon the British Society for Rheuma-tology guidelines for prescribingTNFalpha blockers in adults withrheumatoid arthritis (update of previ-ous guidelines of April 2001). Rheuma-tology (Oxford). 2005;44:157–63.
7. Zink A, Askling J, Dixon WG,Klareskog L, Silman AJ, SymmonsDP. European Biologics Registers—methodology, selected results, andperspectives. Ann Rheum Dis. 2009;68:1240–6.
8. Strangfeld A, Listing J, Herzer P, etal. RA patients with prior malig-nancy under treatment with bio-logics [abstract]. Ann Rheum Dis.2008;67 Suppl II.
9. Dixon WG, Watson KD, Lunt M, etal. The influence of anti-TNF ther-apy upon cancer incidence in pa-tients with rheumatoid arthritis(RA) who have had prior malig-nancy: results from the BSRBR [ab-stract]. Arthritis Rheum. 2008;58Suppl:S638 –9
0. Wolfe F, Michaud K. Biologic treat-
ment of rheumatoid arthritis and the
2 2 2
Anti-TNF receptor agents in cancer survivors 19
risk of malignancy: analyses from alarge US observational study. ArthritisRheum. 2007;56:2886–95.
1. Eggermont AM, ten Hagen TL.Tumor necrosis factor-based iso-lated limb perfusion for soft tis-
sue sarcoma and melanoma: tenyears of successful antivasculartherapy. Curr Oncol Rep. 2003;5:79 – 80.
2. Agius E, Lacy KE, Vukmanovic-Stejic M, et al. Decreased TNF-�synthesis by macrophages restricts
cutaneous immunosurveillance bymemory CD4� T cells during ag-ing. J Exp Med. 2009;206:1929–40.
3. Food and Drug Administration. Foodand Drug Administration Amend-ments Act of 2007. Public Law 110–
85. September 27, 2007.