Embed Size (px)
Citation preview
THE ROLE OF A NEONATAL NURSING SPECIALIST IN THE PHC
RE-ENGINEERING PROCESS
vv
Vanessa Booysen Neonatal Nursing Specialist. Free State Province
UFS

MDG 4: neonatal death rates
From: 4 million neonatal deaths: When? Where? Why? Lawn J et al, The Lancet, Vol 365, March 2005

Final Neonatal Causes of Death (All 1000g+)

• The top causes of perinatal deaths are:
• a. Labour related complications (namely
intrapartum asphyxia and birth
trauma) – 17% BIG BABY
• b. Spontaneous preterm birth – 23%. Small baby (NEEDS SPECIALIZED CARE)
• c. Placental disease (namely pre-eclampsia and placental abruption) –23%.
• Unexplained stillbirths (24%)
• The majority of births (59%) occur in CHCs or district
hospitals, as do the
• majority of perinatal deaths.

Hosp79%
Home/Oth8%
Unknown13%
Place of stillbirth, 2008StatsSA, N=14 626
Hosp79%
Home/Oth10%
Unknown11%
Place of early neonatal death, 2008StatsSA, N=9 572
Hosp61%
Home/Oth25%
Unknown14%
Place of late neonatal death, 2008StatsSA, N=3 621
Hosp43%
Home/Oth41%
Unknown16%
Place of post neonatal death, 2008StatsSA, N=32 123

Proportions of Deliveries by Level of Care

PPIP Avoidable Factors: Administrator related
Immaturity Hypoxia
1. Inadequate facilities/ equipment
2. No NICU bed with ventilator
3. Lack of transport from home
4. Personnel not sufficiently trained
5. No syphilis screening
1. Inadequate facilities/ Equipment
2. Insufficient nurses3. No accessible NICU bed4. Anaesthetic delay5. Lack of transport

PPIP Avoidable Factors: Healthcare Provider Related
Immaturity Hypoxia
1. Management plan inadequate
2. Delays in referring patient3. No antenatal steroids4. Inadequate monitoring5. Resuscitation inadequate
1. Fetal distress not detected but monitored
2. Prolonged 2nd stage with no intervention
3. Fetal distress not detected and not monitored
4. Delays in referring patient
5. Poor progress, partogram not used properly

•Cross-cutting recommendations: National Perinatal
Morbidityand Mortality Committee
(NaPeMMCo)

11
Guiding principles to improve neonatal care (1)
Neonatal services should be structured in such a way that every neonate has access to the necessary level of care and the full range of services if needed.
Neonatal facilities should be specifically designed, equipped and staffed according to the needs of each level of care.
Avoidable factors responsible for the major contributors to PNMR and NMR (asphyxia, LBW, infections) should be addressed and where not preventable / avoidable, to offer best available care for these conditions.
12
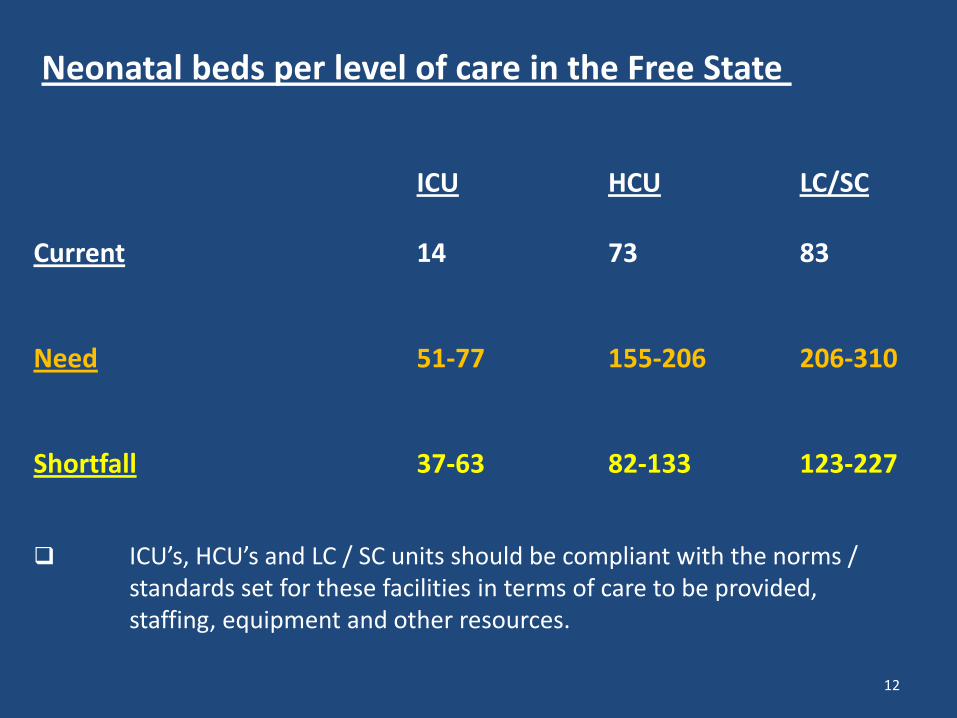
Neonatal beds per level of care in the Free State
ICU HCU LC/SC
Current 14 73 83
Need 51-77 155-206 206-310
Shortfall 37-63 82-133 123-227
ICU’s, HCU’s and LC / SC units should be compliant with the norms / standards set for these facilities in terms of care to be provided,staffing, equipment and other resources.

13
Guiding principles to improve neonatal care (2)
More focus on low technology high impact interventions / modalities of care at district (L1) and regional (L2) hospitals.-
- Baby Friendly Hospital Initiative environment. MBFHI
- Neonatal Resuscitation HBB
- Basic and essential newborn care, eg. neonatal emergencies, feeding, nasogastric feeds, oxygen administration and monitoring, IV fluid therapy, temperature regulation, glucose monitoring, jaundice, infections and identifying early markers of medical / surgical neonatal conditions.
- Adhere to disease / disorder specific referral criteria to ensure timeous STABILISATION and referral of ill neonates to the correct level of care.

14
Guiding principles to improve neonatal care (3)
The neonatal and obstetric services cannot function in isolation. Goodcommunication, interaction and co-ordination of these services are pivotal.
An efficient and safe neonatal and maternal transport service isessential at provincial, regional and district level. Issues to addressinclude: referral criteria, referral routes, modes of transport (road + air),escorts, vehicles, equipment, staff, training, procedure to arrange fortransport and response times. KMC during transport
In utero transport of a fetus at risk to ensure that the mother deliverin a facility where the newborn has access to the appropriate level of care.
Improve communication, co-operation and co-ordination between thelevels of care.
The outreach programme should address level specific neonatal care
issues. MSSN????

15
Guiding principles to improve neonatal care (3)
• Use of level of care specific newborn care treatment protocols MSSN ???
• Breastfeeding
• Breastmilk banks.
• Kangaroo mother care.
• Neurodevelopmental sensitive newborn care.
• Motherhood empowerment programmes.
• Pulse oximetry and vital signs monitoring.
• Non invasive respiratory support e.g. CPAP, “IN/OUT” surfactant, emergency ventilation, TPN and head / whole body cooling (under supervision of apaediatrician) should be considered for HCU in regional hospitals identified as
future “developing tertiary hospitals”.

16
Guiding principles to improve neonatal care (7)
ALL LEVELS of hospitals and CHC’s should have a KMC ward and a
LC / SC neonatal service,Basic laboratory and imaging services should be available at the hospital.
Regional hospitals,
Donor Breastmilk bank, Well equiped HCU and a LC ward
Some regional hospitals may qualify to have a HCU with selected down scaledICU functions (“developing tertiary hospital”)
A paediatrician with an interest in and experience of neonatal care, should be head of the neonatal service. A laboratory, imaging , and a general surgery service should be available.

17
Guiding principles to improve neonatal care (4)
Audits, statistics and quality control / assurance should be an integral partof the neonatal service.
Each of the guiding principles to improve neonatal care should be further refined and transformed into a well structured and workable programme of action and then integrated into a detailed level specificneonatal care and outreach programs
The community paediatrician, obstetrician and Neonatal Nursing Specialist and midwife have a pivotal role to play in the implementation of the neonatal care and outreach programme.

The community paediatrician, obstetrician and Neonatal Nursing Specialist and
midwife have a pivotal role to play
Baby
Obst
Neon Nurse
Paed
Midw

• 1. REGIONAL CLINICIANS TO BE APPOINTED to establish, run and monitor and evaluate outreach programmes for maternal and neonatal health.
• THE MORE SENIOR THE OVERSEEING IS THE BETTER THE CARE
More Deaths in District Hospital
Cross-cutting recommendations: National Perinatal Morbidity
and Mortality Committee (NPMMC)

Ten worst performing districts – all child health indicators 2011
• O Tambo DM• J T Gaetsewe DM• Ehlanzeni DM
• T Mofutsanyane DM• A Nzo DM• Zululand DM• Waterberg DM• uMgungundlovu DM• Sisonke DM• Umkhanyakude DM


FREE STATE PROVINCE

FREE STATE: Thabo MofutsanyanePopulation 750 000
36.3
30.5
10.3
32.6
27.5
9.6
37
31.7
10.5
0
5
10
15
20
25
30
35
40
PNMR SBR ENDR
Nu
mb
er\
10
00
bir
ths
or
live
bir
ths
2007
2008
2009
Assisting Poorly performing districts
• Solutions to be developed with full participation of the provinces and districts.
• Ownership by the province and district & avoiding a top-down approach.
• Specific solutions for specific districts & health facility. Working smarter and being more efficient instead of asking for more resources.
• How?
• Process mapping in order to identify and pin-point bottlenecks and come up with solutions.
• Quality Improvement methodology can be expanded to child health programs.

Manapo implements saving of mothers and babies
• Mofumahadi Manapo Mopeli Regional Hospital in Qwa-Qwa takes pride in saving babies and mothers by starting to implement Primary Health Care Re-engineering programs
• HEALTH WISE
• Issue 21. 22 November 2011

Bought Equipment: Cozy Cots

Bubble CPAPS

Brand new Neonatal HC Unit

Brand new Neonatal HC Unit

Public Private Partnership
• “Thanks to Private Paediatric specialists,DrsWessels, Van Lill and Van der Merwe who agreed
to enter into Public Private Partnership with Manapo so as to improve, empower and
capacitate the staff in rendering quality service to the community of
Thabo Mofutsanyana district. Their practice is in BETHLEHEM, a daily 60MIN
DRIVE TO ManapoDr van Lill and Mediclinic agreement to transfer
‘tertiary’ babies to Hoogland Medi Clinic for ventilation

First baby in the unit kicking; with the dedicated Public Private Partnership Team Paediatrician, Dr Elsa van der Merwe; baby sucking expressed breast
milk, breathing room air, off CPAP! WOW!

Very first baby “saved” in Manapo

• The setting up of this Neonatal HC Unit, now prevents delay in giving IN/OUT Surfactant .
• Saves unnecessary travelling costs and referral time of up to 7 hrs and about 400 km transfers to the already overcrowded hospital, Pelonomi,inBloemfontein.
• Thus overall we are preventing neonatal complications, IVH, BPD Hypothermia and death.

• HEALTH CARE WORKERS TRAINED ON:
• Neonatal Resuscitation,
• Kangaroo Mother Care,
• Neuro Developmental Care of the Pre Term Infant,
• Transporting the Pre Term Infant
• and Breastfeeding and the Pre term Infant....

Training done in Thabo Mofutsanyane



Private Paediatrician Dr Riaan v Lill.

Brand new KMC Unit at ManapoHospital

Training of EMS Staff on Resus and KMC Transport

•The proof is in the......

Pudding........

•stats and graphs

0
2
4
6
8
10
12
14
Aug-11 Sep-11 Oct-11 Nov-11 Dec-11 Jan-12
1
3
0
1
0
3
10
11
8
9
13
1
Early neonates - 8, Late neonates - 43
Mofumahadi Manapo Mopeli Regional Hospital: Neonatal deaths:
August 2011 - January 2012
Inpatient death - early neonatal
Inpatient death - late neonatal

The first premature baby who benefitted from theproject, was born on 7 November 2011 with Hyaline
Membrane disease

Neonatal High Care “hubs of excellence”
• Xhariep – Diamant Hospital Jagersfontein
• Fezile Dabe –Fezi Ngunbentombi, Sasolburg
• Lejweluputswa – Khatleho Virginia
• Motheo – Botsabello Hospital
• MIDWIFE
• VS
• PEADIATRIC NURSE
• VS
• NEONATAL NURSING SPECIALIST

Early Neonatal Mortality Rates (All 1000g+)

MIDWIFE supporting the WELL BABY

But what about the SICK NEONATE ????

Midwife PaedsNurse
SICK Newborn
?
Older baby/Child
Healthy newborn

District Clinical Specialist Teams
Adv Midwife
PaedNurse
PHC Nurse

HOD
Provincial Obstetrician Provincial Family PhysicianProvincial Paediatrician
Provincial Adv Midwife Provincial PHC NurseProvincial Paediatric
Nurse
Maternal service
Women’s health
Reproductive health
Child health
IMCI
Neonatal care
PHC outreach
School health
Chronic/communicable disease
Research/policy oversight
Maternal death notification/ Monitor & Evaluate /PPIP/ChPIP
Adolescent/Youth health
HIV/TB (PMTCT, NIMART, HAART, TB)
EMERGENCY CARE
DISTRICT SPECIALIST TEAMS
Dept Anesthesia
Specialised support
Nutrition

MANAGEMENT OF SICK AND
SMALL NEWBORNS
Assess & Classify
Emergency & Priority SignsVersion: Dec 2010

• TOTAL OF PEP BOOKS ORDERD THROUGHOUT THE PROVINCE
• Newborn Care 76 Modules• Primary Newborn Care 30 Modules• Maternal Care 36 Modules• Primary Maternal Care 8 Modules• Intra partum Care 12 Modules• Perinatal HIV 1 Module• Adult HIV 1 Module• Childhood TB 5 Modules• Child Health Care 4 Modules
• Total 173 modules

Training of Neonatal Nursing Specialists????
SANC DOES NOT ACKNOWLEDGE THE MOST
EVOLVING SPECIALITY AREA IN THE WORLD....AS A SPECIALITY AREA
OSD ?????...........................No.
We are losing trained and experienced “neonatal nurses” that are chasing money...OSD.
Does this mean because we are not going to be $$$$$$$$$ we must stop training????
God forbid

Training of Neonatal Nursing Specialists???? In Adv Midw Curric
Neonatal Nursing
Adv Midwifery

Training of Neonatal Nursing Specialists????
In Paeds/ Child Heath Curric HOSPICENTRIC !!
Neonatal Nursing PAEDS

• Late neonatal mortality rate:
4 per 1000 births
• Almost 1/3 of neonatal deaths occur in late neonatal period
• ¾ of these deaths (1284) were avoidable.
• Why? Inadequate monitoring and poor nursing care
Recommendations
1. Strengthen data collection and quality
2. Newborns must receive the specialised care they require– in hospitals (nurseries), NOT IN
PAEDS WARDS– postnatal care for mothers and babies
3. Ongoing strengthening of PMTCT and other HIV prevention strategies

Training of Neonatal Nursing Specialists???? In ADULT ICU HOSPICENTRIC !!
Nonatal Nursing Adult ICU

But meanwhile….Who will OVERSEE Neonatal Care
Dis die oog van die boer wat die bees vetmaak

In Conclusion
• We need to remember that ALL newborns
are vulnerable.
• Early AND late newborn deaths contribute significantly to both newborn and under-five mortality.
• Neonatal Nurses are the voice of the most vulnerable.


• Our voice needs to be heard
• We believe we can make a difference in
reducing the NNMR.
• Must we wait for 2165 to reach MDG 4???

WITS UNIVERSITY
• In the meantime WITS (in collaboration with the Nelson Mandela Childrens Hospital) is offering a Short Course in Neonatal Intensive Nursing Skills through to
• [email protected] .• This course is not accredited with SANC and will
probably not qualify you for the specialty stream in the public sector but will provide you with valuable skills and knowledge.
• In addition, there is an opportunity to cover the cost of this course through the generous bursary option available from Nelson Mandela Children’s Hospital Trust Fund.

• Meetings with:
• Min of Health together USSANA
• SANC
• Ministerial Nursing Education Task Team
• National NNASA Conference (4,5, August 2016, KZN, Pietermaritzburg)


NNASA is currently tasked to submit documents again to SANC to motivate for recognition of the qualification for clinical neonatal nursing specialists, as well as advanced neonatal nursing specialists.

The neonatal clinical nurse specialist qualification
• Will be submitted to SANC as a new qualification unrelated to legacy qualification. Thereafter it has to go through university structures
• After university approval the curriculum has to be submitted to SANC, CHE, SAQA, DHET and can then be presented. We might be able by 2019
• The neonatal clinical nurse specialist qualification (once approved) will be presented as a postgraduate diploma, which can be followed with a master's degree as advanced clinical nurse specialist.
• NNASA is pushing towards a national qualification.

Presently
• KZN (NELS Programme) Dr N. Mc Kerrow and Ruth Davidge
• And Limpopo, Lolly Mashao and Dr Anne Robertson are the ONLY Provinces acknowledging the expertise and necessity of a Neonatal Nursing Specialist......
• With results....
• Should the rest of the country wait any longer????.....
• Or FOLLOW
Thank You