Embed Size (px)
Citation preview
REGULAR ARTICLE
The right ventricular systolic to diastolic duration ratio: a simple prognosticmarker in congenital diaphragmatic hernia?Sanjeev Aggarwal ([email protected])1, Paul T Stockman2, Michael D Klein2, Girija Natarajan1
1.Department of Pediatrics, Children’s Hospital of Michigan, Detroit, MI, USA2.Department of Pediatric Surgery, Children’s Hospital of Michigan, Detroit, MI, USA
KeywordsDiaphragmatic hernia, Echocardiogram, Prognosis,Systolic to diastolic duration ratio
CorrespondenceSanjeev Aggarwal, M.D., Division of PediatricCardiology, Children’s Hospital of Michigan, 3901Beaubien Blvd, Detroit, MI 48201, USA.Tel: +313 745 6105 |Fax: +(313) 993 0894 |Email: [email protected]
Received17 February 2011; accepted 29 March 2011
DOI:10.1111/j.1651-2227.2011.02302.x
ABSTRACTAims: (i) To compare the ratio of right ventricular systolic to diastolic duration
(SD ⁄ DD) in infants with congenital diaphragmatic hernia (CDH) and normal controls and
(ii) to examine its association, if any, with outcomes in CDH.Methods: Retrospective chart and echocardiographic review of consecutive neo-
nates (<1 month old) with CDH and term controls without structural heart defects. Right
ventricular SD ⁄ DD was calculated by a single reader.Results: Infants with CDH (n = 29) were comparable to controls (n = 27) in their
mean (SD) age [2.2 (3.3) vs. 2 (4.0) days], birthweight [3 (0.67) vs. 3 (0.69) kg] and pro-
portion of males (48.2% vs. 72.4%). The DD and SD ⁄ DD were significantly abnormal in
the CDH group, compared to controls. Among infants with CDH, those who died (n = 15)
and those who died or required ECMO (n = 17) had significantly shorter DD and higher
SD ⁄ DD ratio. At a cut-off of 1.3, SD ⁄ DD ratio had a sensitivity of 92.8 (95% CI 64–99%)
and specificity of 61.5 (32–85%) for prediction of mortality. Significant independent asso-
ciations with mortality were observed with antenatal diagnosis (p = 0.003) and higher
SD ⁄ DD ratio (p = 0.04).Conclusion: The right ventricular SD ⁄ DD ratio is a sensitive objective prognostic mar-
ker in infants with CDH. Further studies incorporating SD ⁄ DD ratio as a guide to intervention
are warranted.
INTRODUCTIONCongenital diaphragmatic hernia (CDH) remains a condi-tion with high rates of mortality and morbidity, secondaryto lung hypoplasia and pulmonary hypertension (PHT) (1).PHT is an intrinsic part of the pathophysiology of CDH (2).Accurate detection of PHT, assessment of its severity and ofright ventricular function in young children is imprecise andfraught with difficulty (3,4).
The ratio of the durations of right ventricular systole todiastole (SD ⁄ DD) has emerged as an index of global ven-tricular function in paediatric cardiomyopathy and rightventricular function in hypoplastic left heart syndrome(5,6). Alkon et al. recently investigated this index in 47 chil-dren with pulmonary arterial hypertension and its associa-tion with right ventricle performance and clinical outcomes.SD ⁄ DD ratio was significantly higher in children with pul-monary artery hypertension, compared to controls. ASD ⁄ DD ratio of 1.0–1.4 was associated with a moderate riskand a ratio >1.4 was associated with a high risk of poor out-comes, including death or lung transplantation (7).
The SD ⁄ DD ratio, considered to be a ‘fundamental char-acteristic of cardiac action’, has not been previously evalu-ated in neonates with CDH (7). In this study, we sought tocompare right ventricular SD ⁄ DD ratio in infants with
CDH and normal controls. Our second objective was todetermine its association with clinical outcomes amonginfants with CDH. We hypothesized that infants with CDHwould have significantly abnormal right ventricular SD ⁄ DDratio compared to controls and further, that among infantswith CDH, a higher SD ⁄ DD ratio would be associated withadverse outcomes.
Key notes• The echocardiographic ratio of right ventricular systolic
to diastolic duration (SD ⁄ DD) was significantly higher inneonates with congenital diaphragmatic hernia (CDH),compared to term controls.
• Among infants with CDH, those who died and thosewho died or required ECMO had significantly higherSD ⁄ DD ratios.
• At a cut-off of 1.3, SD ⁄ DD ratio had a sensitivity of 92.8(95% CI 64–99%) and specificity of 61.5 (32–85%) forprediction of mortality.
Acta Pædiatrica ISSN 0803–5253
ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 1315–1318 1315
PATIENTS AND METHODSThis was a retrospective analysis of medical records andechocardiograms performed for clinical indications. Ourstudy population included consecutive infants with a diag-nosis of (i) CDH admitted to Children’s Hospital of Michi-gan NICU within the first month of life between January 1,2002 and March 31, 2008 and (ii) an equal number of term(>37 weeks gestation) neonates (<1 month age) with nor-mal anatomy on an echocardiogram performed on the sameday as the index CDH infant for clinical evaluation of amurmur. The study cohort was identified using the elec-tronic NICU discharge database with the search words‘CDH’. Infants who did not have an echocardiogram orwho had a congenital structural heart lesion other than apatent ductus arteriosus (PDA) or a patent foramen ovale(PFO) were excluded from the study. The control group wasidentified using the electronic echocardiographic databaseof the Division of Cardiology. Infants who required oxygen,ventilation or hemodynamic support or were diagnosedwith a structural heart defect (except PDA or PFO) wereexcluded from the control group. Infants from both groupsin whom an inadequate tricuspid regurgitation jet precludedcalculation of SD ⁄ DD ratio were excluded. The study andwaiver of parental consent were approved by the HumanInvestigation Committee of Wayne State University.
Medical records were reviewed to obtain demographicdata for both groups of infants and details of the neonatalcourse and outcomes until discharge for infants with CDH.The initial echocardiogram performed on each infant wasreviewed by a single investigator, who was blinded to out-comes data. At our centre, all echocardiograms are per-formed by certified echocardiographic technicians orpaediatric cardiology fellows or attendings using a Phillips
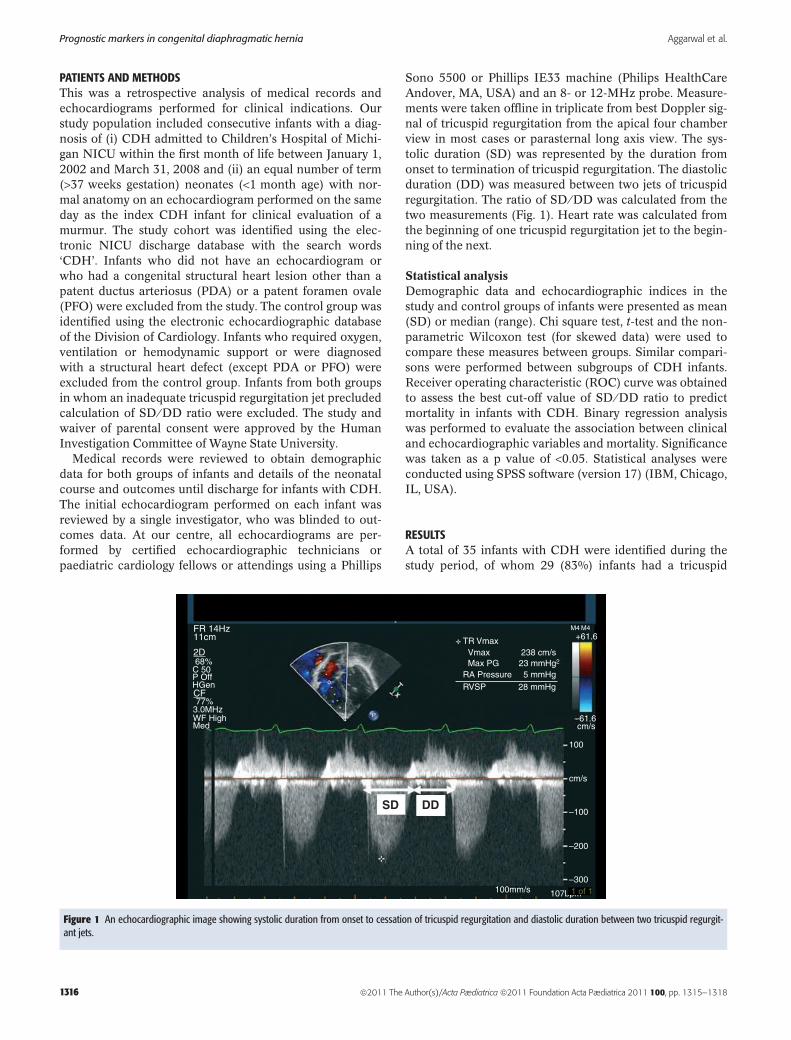
Sono 5500 or Phillips IE33 machine (Philips HealthCareAndover, MA, USA) and an 8- or 12-MHz probe. Measure-ments were taken offline in triplicate from best Doppler sig-nal of tricuspid regurgitation from the apical four chamberview in most cases or parasternal long axis view. The sys-tolic duration (SD) was represented by the duration fromonset to termination of tricuspid regurgitation. The diastolicduration (DD) was measured between two jets of tricuspidregurgitation. The ratio of SD ⁄ DD was calculated from thetwo measurements (Fig. 1). Heart rate was calculated fromthe beginning of one tricuspid regurgitation jet to the begin-ning of the next.
Statistical analysisDemographic data and echocardiographic indices in thestudy and control groups of infants were presented as mean(SD) or median (range). Chi square test, t-test and the non-parametric Wilcoxon test (for skewed data) were used tocompare these measures between groups. Similar compari-sons were performed between subgroups of CDH infants.Receiver operating characteristic (ROC) curve was obtainedto assess the best cut-off value of SD ⁄ DD ratio to predictmortality in infants with CDH. Binary regression analysiswas performed to evaluate the association between clinicaland echocardiographic variables and mortality. Significancewas taken as a p value of <0.05. Statistical analyses wereconducted using SPSS software (version 17) (IBM, Chicago,IL, USA).
RESULTSA total of 35 infants with CDH were identified during thestudy period, of whom 29 (83%) infants had a tricuspid
FR 14Hz11cm
68%
TR VmaxVmax 238 cm/sMax PG
RA PressureRVSP
P
28 mmHg
M4 M4+61.6
–61.6cm/s
100
cm/s
–100
–200
–3001 of 1100mm/s
5 mmHg23 mmHg2
77%3.0MHzWF HighMed
C 50P OffHGen
2D
CF
107bpm
SD DD
Figure 1 An echocardiographic image showing systolic duration from onset to cessation of tricuspid regurgitation and diastolic duration between two tricuspid regurgit-ant jets.
Prognostic markers in congenital diaphragmatic hernia Aggarwal et al.
1316 ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 1315–1318
regurgitation jet enabling measurement of SD ⁄ DD ratio.Similarly, SD ⁄ DD ratio was measurable in only 27 of 60(45%) infants in the control group. Infants with CDH(n = 29) were comparable to controls (n = 27) in theirmean (SD) age [2.2 (3.3) vs. 2.0 (4.0) days], birthweight [3(0.67) vs. 3 (0.69) kg] and proportion of males [13 (48.2%)vs. 21 (72.4%)].Among infants with CDH, 16 (55%) werediagnosed antenatally. CDH was left sided in 21 (72%)infants and right sided in the remaining 8 (28%). Amongthose with CDH, 12 (41.4%) infants underwent extra cor-poreal membrane oxygenation (ECMO), 17 (58%) requiredinhaled nitric oxide, 25 (89%) underwent surgical repairand 14 (48%) survived to discharge.
Heart rate and SD were not significantly differentbetween the infants with CDH and infants in control group(Table 1). The DD was significantly shorter, and SD ⁄ DDratio was significantly increased in infants with CDH, com-pared to controls.
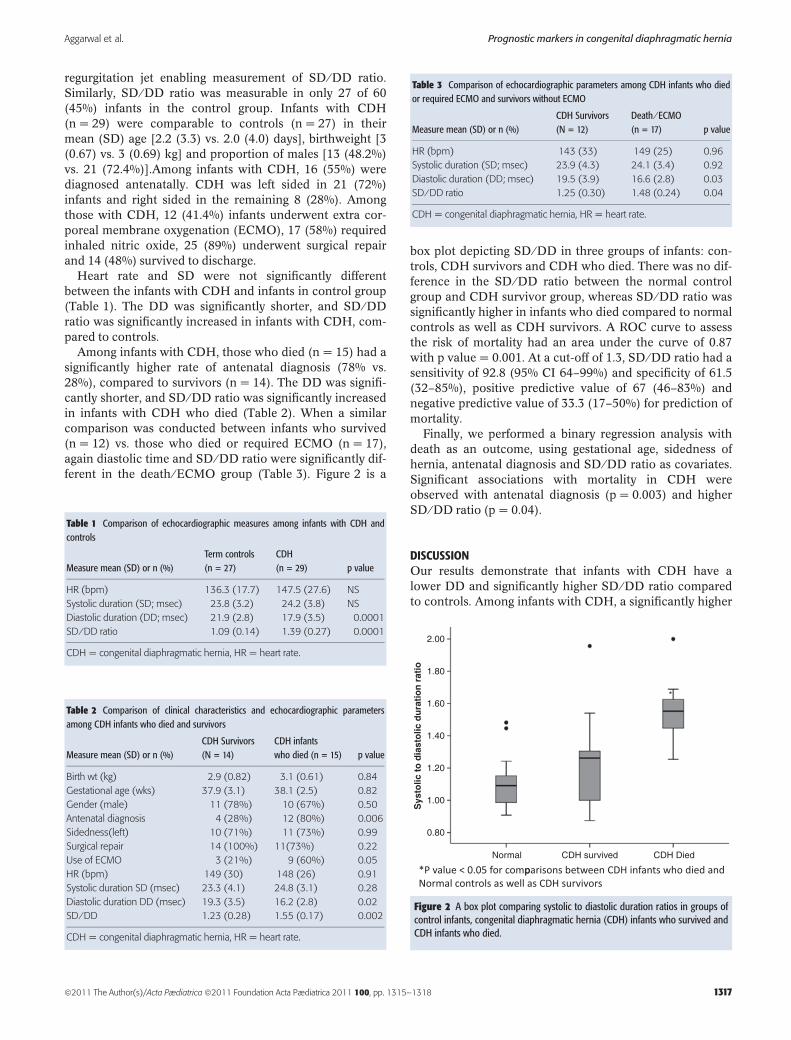
Among infants with CDH, those who died (n = 15) had asignificantly higher rate of antenatal diagnosis (78% vs.28%), compared to survivors (n = 14). The DD was signifi-cantly shorter, and SD ⁄ DD ratio was significantly increasedin infants with CDH who died (Table 2). When a similarcomparison was conducted between infants who survived(n = 12) vs. those who died or required ECMO (n = 17),again diastolic time and SD ⁄ DD ratio were significantly dif-ferent in the death ⁄ ECMO group (Table 3). Figure 2 is a
box plot depicting SD ⁄ DD in three groups of infants: con-trols, CDH survivors and CDH who died. There was no dif-ference in the SD ⁄ DD ratio between the normal controlgroup and CDH survivor group, whereas SD ⁄ DD ratio wassignificantly higher in infants who died compared to normalcontrols as well as CDH survivors. A ROC curve to assessthe risk of mortality had an area under the curve of 0.87with p value = 0.001. At a cut-off of 1.3, SD ⁄ DD ratio had asensitivity of 92.8 (95% CI 64–99%) and specificity of 61.5(32–85%), positive predictive value of 67 (46–83%) andnegative predictive value of 33.3 (17–50%) for prediction ofmortality.
Finally, we performed a binary regression analysis withdeath as an outcome, using gestational age, sidedness ofhernia, antenatal diagnosis and SD ⁄ DD ratio as covariates.Significant associations with mortality in CDH wereobserved with antenatal diagnosis (p = 0.003) and higherSD ⁄ DD ratio (p = 0.04).
DISCUSSIONOur results demonstrate that infants with CDH have alower DD and significantly higher SD ⁄ DD ratio comparedto controls. Among infants with CDH, a significantly higher
Table 1 Comparison of echocardiographic measures among infants with CDH andcontrols
Measure mean (SD) or n (%)Term controls(n = 27)
CDH(n = 29) p value
HR (bpm) 136.3 (17.7) 147.5 (27.6) NS
Systolic duration (SD; msec) 23.8 (3.2) 24.2 (3.8) NS
Diastolic duration (DD; msec) 21.9 (2.8) 17.9 (3.5) 0.0001
SD ⁄ DD ratio 1.09 (0.14) 1.39 (0.27) 0.0001
CDH = congenital diaphragmatic hernia, HR = heart rate.
Table 2 Comparison of clinical characteristics and echocardiographic parametersamong CDH infants who died and survivors
Measure mean (SD) or n (%)CDH Survivors(N = 14)
CDH infantswho died (n = 15) p value
Birth wt (kg) 2.9 (0.82) 3.1 (0.61) 0.84
Gestational age (wks) 37.9 (3.1) 38.1 (2.5) 0.82
Gender (male) 11 (78%) 10 (67%) 0.50
Antenatal diagnosis 4 (28%) 12 (80%) 0.006
Sidedness(left) 10 (71%) 11 (73%) 0.99
Surgical repair 14 (100%) 11(73%) 0.22
Use of ECMO 3 (21%) 9 (60%) 0.05
HR (bpm) 149 (30) 148 (26) 0.91
Systolic duration SD (msec) 23.3 (4.1) 24.8 (3.1) 0.28
Diastolic duration DD (msec) 19.3 (3.5) 16.2 (2.8) 0.02
SD ⁄ DD 1.23 (0.28) 1.55 (0.17) 0.002
CDH = congenital diaphragmatic hernia, HR = heart rate.
Table 3 Comparison of echocardiographic parameters among CDH infants who diedor required ECMO and survivors without ECMO
Measure mean (SD) or n (%)CDH Survivors(N = 12)
Death ⁄ ECMO(n = 17) p value
HR (bpm) 143 (33) 149 (25) 0.96
Systolic duration (SD; msec) 23.9 (4.3) 24.1 (3.4) 0.92
Diastolic duration (DD; msec) 19.5 (3.9) 16.6 (2.8) 0.03
SD ⁄ DD ratio 1.25 (0.30) 1.48 (0.24) 0.04
CDH = congenital diaphragmatic hernia, HR = heart rate.
2.00
1.80
1.60*
1.40
1.20
1.00
0.80
Normal
Sys
tolic
to
dia
sto
lic d
ura
tio
n r
atio
CDH survived CDH Died
Figure 2 A box plot comparing systolic to diastolic duration ratios in groups ofcontrol infants, congenital diaphragmatic hernia (CDH) infants who survived andCDH infants who died.
Aggarwal et al. Prognostic markers in congenital diaphragmatic hernia
ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 1315–1318 1317

SD ⁄ DD ratio was observed in those who died as well asthose who died or required ECMO, compared to survivors.SD ⁄ DD was found to have an independent association withdeath and to have very good sensitivity at a cut-off value of1.3 in its prediction.
Cui et al. (8) established paediatric norms for SD and DDand reported their correlation with heart rates. While SDand DD decrease as heart rate increases, SD ⁄ DD ratioincreased linearly with heart rate. The advantage of theSD ⁄ DD ratio over previous indices such as pre-ejectiontime to ejection time is that it uses the entire duration of sys-tole and diastole, rather than smaller time interval segments(9). The index is thought to reflect right ventricle (RV)response to afterload, not merely the afterload (7). Otheradvantages are the simplicity of measurement of tricuspidregurgitation using standard widely available Doppler tech-niques. Moreover, this measurement is performed on thesame heart cycle.
The striking association between the SD ⁄ DD ratio andclinical outcomes is concordant with a previous study inchildren with pulmonary arterial hypertension (7). In thatstudy, a higher SD ⁄ DD ratio was associated with worsecatheterization hemodynamics, worse echocardiographicright ventricular fractional area of change, shorter 6 minwalk distance and worse clinical outcomes including deathand lung transplantation. As coronary artery perfusionoccurs mainly during diastole, a significant decrease in theDD may worsen right ventricular function. Therefore, theassociation of a higher SD ⁄ DD ratio with adverse outcomesis certainly biologically plausible.
To our knowledge, ours is the first study to evaluate thissimple, easily obtainable objective echocardiographic indexin infants with CDH. Our data confirm the existence of RVdysfunction in infants with CDH and suggest that as mea-sured by the SD ⁄ DD ratio, it has pathogenic implications.The SD ⁄ DD ratio appears to be a robust measure of RV dys-function and prognosis in this population. It may have someutility in directing timely targeted interventions. Furtherstudies incorporating echocardiographic indices as prog-nostic markers of CDH are warranted to optimize outcomesin this population.
Our study has a number of limitations. This is a retrospec-tive study with its inherent biases. The effect of high
ventilatory support, high frequency oscillation, pressors,nitric oxide and indeed, any therapy on the SD ⁄ DD ratioare unclear and have not been accounted for. Our samplesize was small, although in line with other similar studies.The SD ⁄ DD ratio may be affected by loading conditionsand may not be possible to obtain in infants without tricus-pid regurgitation. Nonetheless, the exploration of theSD ⁄ DD ratio, a measure of global right ventricular functionin CDH is novel and potentially important for further inves-tigation.
References
1. Keijzer R, Puri P. Congenital diaphragmatic hernia. Semin Pedi-atr Surg 2010; 19: 180–5.
2. Dillon PW, Cilley RE, Mauger D, Zachary C, Meier A. The rela-tionship of pulmonary artery pressure and survival in congenitaldiaphragmatic hernia. J Pediatr Surg 2004; 39: 307–12. discus-sion 307–12.
3. Boucek RJ Jr, Martinez R. Echocardiographic determination ofright ventricular function. Cardiol Young 2005; 15(Suppl 1): 48–50.
4. Skinner JR, Hunter S, Hey EN. Haemodynamic features at pre-sentation in persistent pulmonary hypertension of the newbornand outcome. Arch Dis Child Fetal Neonatal Ed 1996; 74: F26–32.
5. Friedberg MK, Silverman NH. Cardiac ventricular diastolic andsystolic duration in children with heart failure secondary to idio-pathic dilated cardiomyopathy. Am J Cardiol 2006; 97: 101–5.
6. Friedberg MK, Silverman NH. The systolic to diastolic durationratio in children with hypoplastic left heart syndrome: a novelDoppler index of right ventricular function. J Am Soc Echocardi-ogr 2007; 20: 749–55.
7. Alkon J, Humpl T, Manlhiot C, McCrindle BW, Reyes JT, Fried-berg MK. Usefulness of the right ventricular systolic to diastolicduration ratio to predict functional capacity and survival in chil-dren with pulmonary arterial hypertension. Am J Cardiol 2010;106: 430–6.
8. Cui W, Roberson DA, Chen Z, Madronero LF, Cuneo BF. Sys-tolic and diastolic time intervals measured from Doppler tissueimaging: normal values and Z-score tables, and effects of age,heart rate, and body surface area. J Am Soc Echocardiogr 2008;21: 361–70.
9. Friedberg MK, Silverman NH. The systolic to diastolic durationratio in children with heart failure secondary to restrictive car-diomyopathy. J Am Soc Echocardiogr 2006; 19: 1326–31.
Prognostic markers in congenital diaphragmatic hernia Aggarwal et al.
1318 ª2011 The Author(s)/Acta Pædiatrica ª2011 Foundation Acta Pædiatrica 2011 100, pp. 1315–1318