Embed Size (px)
Citation preview

The Right Treatment for theRight Patient (at the Right Time):
Personalized Medicine and Statistics
Marie Davidian
Department of StatisticsNorth Carolina State University
http://www4.stat.ncsu.edu/~davidian
1/47 Personalized Medicine and Statistics

“Personalized Medicine ”
Source of graphic: http://www.personalizedmedicine.com/
2/47 Personalized Medicine and Statistics

“Personalized Medicine ”
Source of graphic: http://www.personalizedmedicine.com/
2/47 Personalized Medicine and Statistics

Why is a statistician talking to you about personalized medicine?
To convince you of the essential role of statistics in the developmentof optimal, evidence-based personalized treatment strategies
3/47 Personalized Medicine and Statistics

Why is a statistician talking to you about personalized medicine?
To convince you of the essential role of statistics in the developmentof optimal, evidence-based personalized treatment strategies
3/47 Personalized Medicine and Statistics

There should be a treatment for that
Modern expectation: A treatment for everything• Drugs• Biologics• Medical devices• Surgical procedures• Behavioral interventions• . . .
4/47 Personalized Medicine and Statistics

Does it work?
Fundamental – the randomized controlled clinical trial:• Evaluation of effectiveness• Comparison of a new treatment to standard of care• Comparison of existing treatments to establish new uses
5/47 Personalized Medicine and Statistics

The controlled clinical trial
Basics of a typical clinical trial:• A sample of subjects with the disease/disorder is recruited• Subjects are randomized to treatments under study⇒ eliminate bias, allow fair comparison
• A (primary) outcome is ascertained for each subject• E.g., overall survival time in cancer, viral load level after 1 year in
human immunodeficiency virus (HIV) infection, death,myocardial infarction, or urgent target vessel revascularizationwithin 30 days in cardiovascular disease
6/47 Personalized Medicine and Statistics

The controlled clinical trial
Assessment of effectiveness:• Comparison of some summary measure of outcome
between/among treatments• E.g., the average
• “Is the average outcome if all patients in the population were totake treatment A different from (better than) that if they allinstead were to take treatment B? ”
• Use statistical methods to evaluate the strength of the evidencein the data from the sample supporting a real difference in thepopulation (statistical hypothesis test )
7/47 Personalized Medicine and Statistics

The controlled clinical trial
Assessment of effectiveness:• Comparison of some summary measure of outcome
between/among treatments• E.g., the average• “Is the average outcome if all patients in the population were to
take treatment A different from (better than) that if they allinstead were to take treatment B? ”
• Use statistical methods to evaluate the strength of the evidencein the data from the sample supporting a real difference in thepopulation (statistical hypothesis test )
7/47 Personalized Medicine and Statistics

Results
Thus, usually:• Assessment of effectiveness (and regulatory approval ) are
based on a summary measure (e.g., an average) across theentire population
• Statistics is key
Success:• Countless treatments have been evaluated and approved on this
basis• And have benefited numerous patients
However:• All patients are not created equal
8/47 Personalized Medicine and Statistics

Results
Thus, usually:• Assessment of effectiveness (and regulatory approval ) are
based on a summary measure (e.g., an average) across theentire population
• Statistics is key
Success:• Countless treatments have been evaluated and approved on this
basis• And have benefited numerous patients
However:• All patients are not created equal
8/47 Personalized Medicine and Statistics

Results
Thus, usually:• Assessment of effectiveness (and regulatory approval ) are
based on a summary measure (e.g., an average) across theentire population
• Statistics is key
Success:• Countless treatments have been evaluated and approved on this
basis• And have benefited numerous patients
However:• All patients are not created equal
8/47 Personalized Medicine and Statistics

Patient heterogeneity
9/47 Personalized Medicine and Statistics

Patient heterogeneity
Sources of heterogeneity:• Demographic characteristics• Physiological characteristics• Medical history, concomitant conditions
• Genetic/genomic characteristics
Result: What is “best ” for a patient with one set of characteristicsmight not be “best ” for another• Well-recognized issue for decades• Subgroup analyses• Interest skyrocketed with the advent of the genomic era
10/47 Personalized Medicine and Statistics

Patient heterogeneity
Sources of heterogeneity:• Demographic characteristics• Physiological characteristics• Medical history, concomitant conditions• Genetic/genomic characteristics
Result: What is “best ” for a patient with one set of characteristicsmight not be “best ” for another• Well-recognized issue for decades• Subgroup analyses• Interest skyrocketed with the advent of the genomic era
10/47 Personalized Medicine and Statistics

Patient heterogeneity
Sources of heterogeneity:• Demographic characteristics• Physiological characteristics• Medical history, concomitant conditions• Genetic/genomic characteristics
Result: What is “best ” for a patient with one set of characteristicsmight not be “best ” for another• Well-recognized issue for decades• Subgroup analyses• Interest skyrocketed with the advent of the genomic era
10/47 Personalized Medicine and Statistics

A contrived example
Average outcome in the patient population:• Larger outcomes are better (survival time)• If all patients took treatment A = 9 months• If all patients took treatment B =18 months• Treatment B is better on average
Genetic mutation:• 20% have it, 80% don’t• If all patients took treatment A = (0.2)(25) + (0.8)(5) = 9• If all patients took treatment B = (0.2)(10) + (0.8)(20) = 18• That is, patients with the mutation do much better on treatment A
(25 months vs. 10 months) on average
11/47 Personalized Medicine and Statistics

A contrived example
Average outcome in the patient population:• Larger outcomes are better (survival time)• If all patients took treatment A = 9 months• If all patients took treatment B =18 months• Treatment B is better on average
Genetic mutation:• 20% have it, 80% don’t
• If all patients took treatment A = (0.2)(25) + (0.8)(5) = 9• If all patients took treatment B = (0.2)(10) + (0.8)(20) = 18• That is, patients with the mutation do much better on treatment A
(25 months vs. 10 months) on average
11/47 Personalized Medicine and Statistics

A contrived example
Average outcome in the patient population:• Larger outcomes are better (survival time)• If all patients took treatment A = 9 months• If all patients took treatment B =18 months• Treatment B is better on average
Genetic mutation:• 20% have it, 80% don’t• If all patients took treatment A = (0.2)(25) + (0.8)(5) = 9
• If all patients took treatment B = (0.2)(10) + (0.8)(20) = 18• That is, patients with the mutation do much better on treatment A
(25 months vs. 10 months) on average
11/47 Personalized Medicine and Statistics

A contrived example
Average outcome in the patient population:• Larger outcomes are better (survival time)• If all patients took treatment A = 9 months• If all patients took treatment B =18 months• Treatment B is better on average
Genetic mutation:• 20% have it, 80% don’t• If all patients took treatment A = (0.2)(25) + (0.8)(5) = 9• If all patients took treatment B = (0.2)(10) + (0.8)(20) = 18
• That is, patients with the mutation do much better on treatment A(25 months vs. 10 months) on average
11/47 Personalized Medicine and Statistics

A contrived example
Average outcome in the patient population:• Larger outcomes are better (survival time)• If all patients took treatment A = 9 months• If all patients took treatment B =18 months• Treatment B is better on average
Genetic mutation:• 20% have it, 80% don’t• If all patients took treatment A = (0.2)(25) + (0.8)(5) = 9• If all patients took treatment B = (0.2)(10) + (0.8)(20) = 18• That is, patients with the mutation do much better on treatment A
(25 months vs. 10 months) on average
11/47 Personalized Medicine and Statistics

Personalized medicine
Moral:• While useful for evaluation and approval, summary measures are
not useful for determining how to treat individual patients• Ad hoc search for subgroups could be misleading
(e.g., false discovery )• May be much more complicated than finding a single “mutation ”
(no “magic bullet ”)
Needed: A formal, principled, evidence-based approach
12/47 Personalized Medicine and Statistics

Popular perspective on personalized medicine
Subgroup identification and targeted treatment:• Can we determine subgroups of patients who share certain
characteristics and who are likely to benefit from a particulartreatment?
• Can biomarkers be developed to identify such patients?• In fact, can a new treatment be developed to target a subgroup
that is likely to benefit?• Can clinical trials and approval be focused on particular
subgroups of patients?
Focus: “The right patient for the treatment ”
13/47 Personalized Medicine and Statistics

Popular perspective on personalized medicine
Subgroup identification and targeted treatment:• Can we determine subgroups of patients who share certain
characteristics and who are likely to benefit from a particulartreatment?
• Can biomarkers be developed to identify such patients?• In fact, can a new treatment be developed to target a subgroup
that is likely to benefit?• Can clinical trials and approval be focused on particular
subgroups of patients?
Focus: “The right patient for the treatment ”
13/47 Personalized Medicine and Statistics

Popular perspective on personalized medicine
How do we identify “the right patient ?”
Source of graphic: Christoph Meinel, Hasso-Plattner-Institut Potsdam
14/47 Personalized Medicine and Statistics

Another perspective on personalized medicine
Clinical practice: Clinicians make (a series of) treatment decision(s)over the course of a patient’s disease or disorder• Key decision points in the disease/disorder process• Multiple treatment options at each• Accrued information on the patient• Goal: Make the best decision(s) for this individual patient
Focus: “The right treatment for the patient ”
How do we identify “the right treatment ?”
15/47 Personalized Medicine and Statistics

Another perspective on personalized medicine
Clinical practice: Clinicians make (a series of) treatment decision(s)over the course of a patient’s disease or disorder• Key decision points in the disease/disorder process• Multiple treatment options at each• Accrued information on the patient• Goal: Make the best decision(s) for this individual patient
Focus: “The right treatment for the patient ”
How do we identify “the right treatment ?”
15/47 Personalized Medicine and Statistics

Cancer treatment
Two decision points:• Decision 1: Induction chemotherapy (C)• Decision 2: Maintenance treatment (M) for patients who
respond, Salvage chemotherapy (S) for those who don’t• Several options for each• Goal: Prolong survival (outcome)
16/47 Personalized Medicine and Statistics

Clinical decision-making
How are these decisions made?• Clinical judgment• Practice guidelines based on previous studies, expert opinion
• Synthesis of all information on/characteristics of the patient tomake a treatment decision from among the possible options
17/47 Personalized Medicine and Statistics

Clinical decision-making
How are these decisions made?• Clinical judgment• Practice guidelines based on previous studies, expert opinion• Synthesis of all information on/characteristics of the patient to
make a treatment decision from among the possible options
17/47 Personalized Medicine and Statistics

In either case
Needed: A formal , evidence-based approach to• Identifying patient characteristics like “mutation status” for which
the “best ” treatment changes with their value• “Tailoring variables ”• Determining how and in what combination tailoring variables
may be used to identify subgroups and select treatment optionsfor individual patients
• Evidence = data• Statistical design, modeling, and analysis
18/47 Personalized Medicine and Statistics

Cancer treatment
Two decision points• Decision 1: Two induction chemotherapy options C1, C2
• Decision 2: Two maintenance options M1, M2 for patients whorespond, two salvage options S1, S2 for those who don’t
• Goal: Prolong survival (outcome)
19/47 Personalized Medicine and Statistics

How “best” to make these decisions?
Conventional clinical trials:• Most primary analyses focus on a summary measure• Most trials focus on a single decision
How can we challenge this paradigm and move toward making the“best ” decisions for individual patients ?
20/47 Personalized Medicine and Statistics

Using statistics to formalize decision-making
Formalizing clinical decision-making: At any decision• Would like a formal rule that takes as input all available
information on the patient to that point and outputs a treatmentfrom among the possible options
• Decision 1: “If age < 50 years and progesterone receptor level< 10 fmol, give chemotherapy C2; otherwise, give C1”
Dynamic treatment regime: Aka adaptive treatment strategy• A set of such rules, each corresponding to a decision point• Ideally – find the regime that leads to the “best ” possible
outcome for each patient given the available information• Base this on data
21/47 Personalized Medicine and Statistics

Using statistics to formalize decision-making
Formalizing clinical decision-making: At any decision• Would like a formal rule that takes as input all available
information on the patient to that point and outputs a treatmentfrom among the possible options
• Decision 1: “If age < 50 years and progesterone receptor level< 10 fmol, give chemotherapy C2; otherwise, give C1”
Dynamic treatment regime: Aka adaptive treatment strategy• A set of such rules, each corresponding to a decision point• Ideally – find the regime that leads to the “best ” possible
outcome for each patient given the available information• Base this on data
21/47 Personalized Medicine and Statistics

Using statistics to formalize decision-making
Formalizing clinical decision-making: At any decision• Would like a formal rule that takes as input all available
information on the patient to that point and outputs a treatmentfrom among the possible options
• Decision 1: “If age < 50 years and progesterone receptor level< 10 fmol, give chemotherapy C2; otherwise, give C1”
Dynamic treatment regime: Aka adaptive treatment strategy• A set of such rules, each corresponding to a decision point• Ideally – find the regime that leads to the “best ” possible
outcome for each patient given the available information• Base this on data
21/47 Personalized Medicine and Statistics

Single decision
Assume:• There is an outcome of interest, Y , e.g., survival time• Large outcomes are good• X = all available information on the patient• Set of treatment options, e.g., {C1,C2} = {0, 1}
Treatment regime: A rule of the form d(X ) such that
d(X ) = 0 or 1 depending on X
22/47 Personalized Medicine and Statistics

Single decision
Assume:• There is an outcome of interest, Y , e.g., survival time• Large outcomes are good• X = all available information on the patient• Set of treatment options, e.g., {C1,C2} = {0, 1}
Treatment regime: A rule of the form d(X ) such that
d(X ) = 0 or 1 depending on X
22/47 Personalized Medicine and Statistics

Dynamic treatment regime
d(X ) = 0 or 1 depending on X
Example regimes: X = {age,PR level}• Rule involving cut-offs
d(X ) = 1 (C2) if age < 50 and PR level < 10= 0 (C1) otherwise
written concisely as
d(X ) = I(age < 50 and PR < 10)
• Rule involving linear combinations
d(X ) = I{age + 8.7 log(PR)− 60 > 0}
23/47 Personalized Medicine and Statistics

Dynamic treatment regime
d(X ) = 0 or 1 depending on X
Example regimes: X = {age,PR level}• Rule involving cut-offs
d(X ) = 1 (C2) if age < 50 and PR level < 10= 0 (C1) otherwise
written concisely as
d(X ) = I(age < 50 and PR < 10)
• Rule involving linear combinations
d(X ) = I{age + 8.7 log(PR)− 60 > 0}
23/47 Personalized Medicine and Statistics

Defining the optimal regime
Clearly: An infinite number of rules/regimes d(X ) are possible• Can we find the “best ?”• That is, “best ” or optimal, regime dopt(X ) among all possible
d(X )?
• What do we mean by “best ?”
24/47 Personalized Medicine and Statistics

Defining the optimal regime
Clearly: An infinite number of rules/regimes d(X ) are possible• Can we find the “best ?”• That is, “best ” or optimal, regime dopt(X ) among all possible
d(X )?• What do we mean by “best ?”
24/47 Personalized Medicine and Statistics

Defining the optimal regime
Make the “best” decision at the time a patient presents:• Everything we know about a patient is contained in X• For a patient with a particular set of information X , the “best ”
decision is to give the treatment that leads to the largestexpected outcome for such a patient
Thus: Optimal regime dopt should satisfy• If a patient with information X were to receive treatment
according to dopt , his/her expected outcome is as large aspossible
• And if all patients in the population were to follow dopt , theexpected (average) outcome across the entire population shouldbe as large as possible
25/47 Personalized Medicine and Statistics

Defining the optimal regime
Make the “best” decision at the time a patient presents:• Everything we know about a patient is contained in X• For a patient with a particular set of information X , the “best ”
decision is to give the treatment that leads to the largestexpected outcome for such a patient
Thus: Optimal regime dopt should satisfy• If a patient with information X were to receive treatment
according to dopt , his/her expected outcome is as large aspossible
• And if all patients in the population were to follow dopt , theexpected (average) outcome across the entire population shouldbe as large as possible
25/47 Personalized Medicine and Statistics

Defining the optimal regime
Make the “best” decision at the time a patient presents:• Everything we know about a patient is contained in X• For a patient with a particular set of information X , the “best ”
decision is to give the treatment that leads to the largestexpected outcome for such a patient
Thus: Optimal regime dopt should satisfy• If a patient with information X were to receive treatment
according to dopt , his/her expected outcome is as large aspossible
• And if all patients in the population were to follow dopt , theexpected (average) outcome across the entire population shouldbe as large as possible
25/47 Personalized Medicine and Statistics

Defining the optimal regime
Expected outcome: A = treatment received
E(Y |X ,A)
is the expected outcome for patients with characteristics X were theyto receive treatment A• With two options {0, 1}:
dopt(X ) = 0 if E(Y |X ,A = 1) < E(Y |X ,A = 0)= 1 if E(Y |X ,A = 1) > E(Y |X ,A = 0)
• E(Y |X ,A) is the regression of outcome on characteristics andtreatment received (expected outcome given X and A)
26/47 Personalized Medicine and Statistics

Defining the optimal regime
Expected outcome: A = treatment received
E(Y |X ,A)
is the expected outcome for patients with characteristics X were theyto receive treatment A• With two options {0, 1}:
dopt(X ) = 0 if E(Y |X ,A = 1) < E(Y |X ,A = 0)= 1 if E(Y |X ,A = 1) > E(Y |X ,A = 0)
• E(Y |X ,A) is the regression of outcome on characteristics andtreatment received (expected outcome given X and A)
26/47 Personalized Medicine and Statistics

Estimating the optimal regime
dopt(X ) = 0 if E(Y |X ,A = 1) < E(Y |X ,A = 0)= 1 if E(Y |X ,A = 1) > E(Y |X ,A = 0)
Data: Recorded (X ,A,Y ) from n patients• From a conventional clinical trial comparing treatments 0 and 1,
baseline information X• Develop a regression model and fit to the data
• E.g., if X = (X (1),X (2)), a linear model (need not be linear)
E(Y |X ,A) = α0 + α1X (1) + A(β0 + β1X (2))
• Or a logistic regression model
logit{E(Y |X ,A) } = α0 + α1X (1) + A(β0 + β1X (2))
27/47 Personalized Medicine and Statistics

Estimating the optimal regime
dopt(X ) = 0 if E(Y |X ,A = 1) < E(Y |X ,A = 0)= 1 if E(Y |X ,A = 1) > E(Y |X ,A = 0)
Data: Recorded (X ,A,Y ) from n patients• From a conventional clinical trial comparing treatments 0 and 1,
baseline information X• Develop a regression model and fit to the data• E.g., if X = (X (1),X (2)), a linear model (need not be linear)
E(Y |X ,A) = α0 + α1X (1) + A(β0 + β1X (2))
• Or a logistic regression model
logit{E(Y |X ,A) } = α0 + α1X (1) + A(β0 + β1X (2))
27/47 Personalized Medicine and Statistics

Estimating the optimal regime
dopt(X ) = 0 if E(Y |X ,A = 1) < E(Y |X ,A = 0)= 1 if E(Y |X ,A = 1) > E(Y |X ,A = 0)
Data: Recorded (X ,A,Y ) from n patients• From a conventional clinical trial comparing treatments 0 and 1,
baseline information X• Develop a regression model and fit to the data• E.g., if X = (X (1),X (2)), a linear model (need not be linear)
E(Y |X ,A) = α0 + α1X (1) + A(β0 + β1X (2))
• Or a logistic regression model
logit{E(Y |X ,A) } = α0 + α1X (1) + A(β0 + β1X (2))
27/47 Personalized Medicine and Statistics

Estimating the optimal regime
dopt(X ) = 0 if E(Y |X ,A = 1) < E(Y |X ,A = 0)= 1 if E(Y |X ,A = 1) > E(Y |X ,A = 0)
Data: Recorded (X ,A,Y ) from n patients• From a conventional clinical trial comparing treatments 0 and 1,
baseline information X• Develop a regression model and fit to the data• E.g., if X = (X (1),X (2)), a linear model (need not be linear)
E(Y |X ,A) = α0 + α1X (1) + A(β0 + β1X (2))
• Or a logistic regression model
logit{E(Y |X ,A) } = α0 + α1X (1) + A(β0 + β1X (2))
27/47 Personalized Medicine and Statistics

Estimating the optimal regime
dopt(X ) = 0 if E(Y |X ,A = 1) < E(Y |X ,A = 0)= 1 if E(Y |X ,A = 1) > E(Y |X ,A = 0)
Data: Recorded (X ,A,Y ) from n patients• These models imply
dopt(X ) = 0 if β0 + β1X (2) < 0= 1 if β0 + β1X (2) > 0
• Estimated optimal regime: Substitute estimates for β0, β1
dopt(X ) = I( β0 + β1X (2) > 0 )
• The same idea applies to fancier models
28/47 Personalized Medicine and Statistics

Multiple decisions
Two decisions (cancer example):• Decision 1: X1 = information available, set of treatment options,
e.g., {C1,C2}• Decision 2: X2 = additional information collected, set of
treatment options, e.g., {M1, M2, S1, S2}• X2 includes responder status
Regime: A set of rules d = {d1(X1),d2(X1,A1,X2)}• d1(X1) dictates treatment at decision 1 given information
available at that point• A1 is treatment received at decision 1 (determined by X1)• d2(X1,A1,X2) dictates treatment at decision 2 given all accrued
information at that point
29/47 Personalized Medicine and Statistics

Multiple decisions
Two decisions (cancer example):• Decision 1: X1 = information available, set of treatment options,
e.g., {C1,C2}• Decision 2: X2 = additional information collected, set of
treatment options, e.g., {M1, M2, S1, S2}• X2 includes responder status
Regime: A set of rules d = {d1(X1),d2(X1,A1,X2)}• d1(X1) dictates treatment at decision 1 given information
available at that point• A1 is treatment received at decision 1 (determined by X1)• d2(X1,A1,X2) dictates treatment at decision 2 given all accrued
information at that point
29/47 Personalized Medicine and Statistics

Optimal multi-decision regime
Optimal regime: dopt is such that the expected outcome for a patientwith initial characteristics X1, if s/he were to receive all subsequenttreatments according to dopt , is as large as possible
dopt = {dopt1 (X1),d
opt2 (X1,A1,X2) }
• Can we use data and regression modeling as before?• I.e., consider each decision separately and use data from
separate clinical trials comparing the options at each?• Unfortunately not. . .
30/47 Personalized Medicine and Statistics

Optimal multi-decision regime
Optimal regime: dopt is such that the expected outcome for a patientwith initial characteristics X1, if s/he were to receive all subsequenttreatments according to dopt , is as large as possible
dopt = {dopt1 (X1),d
opt2 (X1,A1,X2) }
• Can we use data and regression modeling as before?• I.e., consider each decision separately and use data from
separate clinical trials comparing the options at each?• Unfortunately not. . .
30/47 Personalized Medicine and Statistics

Complications for multiple decisions
Delayed effects: For example• C1 may yield higher proportion of responders than C2 but may
also have other effects that render subsequent maintenancetreatments (M) less effective in regard to survival
• C1 may not appear best initially but may have enhancedeffectiveness over the long term when followed by M1
• Result – Must use data from a single study (same patients)reflecting the entire sequence of decisions
Data: (X1,A1,X2,A2,Y ) recorded from n patients• A1 = treatment received at decision 1,
A2 = treatment received at decision 2
31/47 Personalized Medicine and Statistics

Complications for multiple decisions
Delayed effects: For example• C1 may yield higher proportion of responders than C2 but may
also have other effects that render subsequent maintenancetreatments (M) less effective in regard to survival
• C1 may not appear best initially but may have enhancedeffectiveness over the long term when followed by M1
• Result – Must use data from a single study (same patients)reflecting the entire sequence of decisions
Data: (X1,A1,X2,A2,Y ) recorded from n patients• A1 = treatment received at decision 1,
A2 = treatment received at decision 2
31/47 Personalized Medicine and Statistics

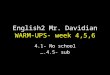
SMART
SMART: Sequential, Multiple Assignment, Randomized Trial• Randomize subjects at each decision point• Collect not only baseline information X1 but intervening
information X2
• Goal: Provide rich data for estimation of optimal treatmentregimes
Pioneered by Susan Murphy, Phil Lavori, and others
32/47 Personalized Medicine and Statistics

SMART
Schematic of a SMART: Cancer example (randomization at •s)
Cancer
Response
NoResponse
Response
NoResponse
C
C
1
2
M1
M2
M1
M2
S1
S2
S1
S2
33/47 Personalized Medicine and Statistics

Sequential regression (Q-learning)
Estimating dopt : dopt = {dopt1 (X1),d
opt2 (X1,A1,X2) }
• Start at the final decision and work backwards• Backward induction, dynamic programming
34/47 Personalized Medicine and Statistics

Sequential regression (Q-learning)
Decision 2: Given the patient’s accrued history to this point,determine the optimal rule to be used now• Decision 2 options coded {0, 1}
dopt2 (X1,A1,X2)
= 0 if E(Y |X1,A1,X2,A2 = 1) < E(Y |X1,A1,X2,A2 = 0)= 1 if E(Y |X1,A1,X2,A2 = 1) > E(Y |X1,A1,X2,A2 = 0)
• E(Y |X1,A1,X2,A2) is the regression of outcome on bothtreatments received and accrued characteristics
• Can develop and fit a regression model
35/47 Personalized Medicine and Statistics

Sequential regression (Q-learning)
Decision 1: Trickier• Must take into account that the optimal rule at decision 2 will be
followed in the future• I.e., dopt
1 (X1) must make the expected outcome as large aspossible when also dopt
2 (X1,A1,X2) will be used to determinetreatment at decision 2
• Mathematically messy; best explained by illustration
36/47 Personalized Medicine and Statistics

Sequential regression (Q-learning)
Decision 1: Trickier• Must take into account that the optimal rule at decision 2 will be
followed in the future• I.e., dopt
1 (X1) must make the expected outcome as large aspossible when also dopt
2 (X1,A1,X2) will be used to determinetreatment at decision 2
• Mathematically messy; best explained by illustration
36/47 Personalized Medicine and Statistics

Sequential regression (Q-learning)
Implementation:• Develop a regression model for decision 2, e.g.,
E(Y |X1,A1,X2,A2) = α20 + α21X1 + α22X2 + α23A1X1
+ A2(β20 + β21X2 + β22A1),
fit to the data, and estimate dopt2 (X1,A1,X2)
d2(X1,A1,X2) = I( β20 + β21X2 + β22A1 > 0 )
37/47 Personalized Medicine and Statistics

Sequential regression (Q-learning)
Implementation:• Develop a regression model for decision 2, e.g.,
E(Y |X1,A1,X2,A2) = α20 + α21X1 + α22X2 + α23A1X1
+ A2(β20 + β21X2 + β22A1),
fit to the data, and estimate dopt2 (X1,A1,X2)
d2(X1,A1,X2) = I( β20 + β21X2 + β22A1 > 0 )
37/47 Personalized Medicine and Statistics

Sequential regression (Q-learning)
Implementation:• For each subject, form Y , the predicted value with the decision 2
optimal treatment determined by the estimated dopt2 (X1,A1,X2)
substituted for A2 actually received, i.e.,
Y = α20 + α21X1 + α22X2 + α23A1X1
+ dopt2 (X1,A1,X2)(β20 + β21X2 + β22A1)
• Develop a regression model for decision 1 with Y as theoutcome, e.g.,
E(Y |X1,A1) = α10 + α11X1 + A1(β10 + β11X1),
fit to the data, and estimate dopt1 (X1)
d1(X1) = I( β10 + β11X1 > 0 )
38/47 Personalized Medicine and Statistics

Sequential regression (Q-learning)
Implementation:• For each subject, form Y , the predicted value with the decision 2
optimal treatment determined by the estimated dopt2 (X1,A1,X2)
substituted for A2 actually received, i.e.,
Y = α20 + α21X1 + α22X2 + α23A1X1
+ dopt2 (X1,A1,X2)(β20 + β21X2 + β22A1)
• Develop a regression model for decision 1 with Y as theoutcome, e.g.,
E(Y |X1,A1) = α10 + α11X1 + A1(β10 + β11X1),
fit to the data, and estimate dopt1 (X1)
d1(X1) = I( β10 + β11X1 > 0 )
38/47 Personalized Medicine and Statistics

Result
• An approach exists for estimating optimal treatment regimesfrom appropriate data
• So why isn’t everyone doing this ?
39/47 Personalized Medicine and Statistics

Issues
• This all depends on the chosen regression models• If the regression model(s) are not correct, an estimated optimal
regime could be very different from the true optimal regime• Are there other ways to estimate an optimal regime that are less
sensitive to chosen models?
• If X1, X2 are high-dimensional, rules could be very complicated(and how to select the likely tailoring variables?)
• Distrust of “black boxes” – can we restrict attention only toregimes that are feasible and interpretable in practice?
• Linear models produce rules involving linear combinations ofcharacteristics – what if we want to restrict to rules involvingcut-offs/thresholds ?
40/47 Personalized Medicine and Statistics

Issues
• This all depends on the chosen regression models• If the regression model(s) are not correct, an estimated optimal
regime could be very different from the true optimal regime• Are there other ways to estimate an optimal regime that are less
sensitive to chosen models?• If X1, X2 are high-dimensional, rules could be very complicated
(and how to select the likely tailoring variables?)• Distrust of “black boxes” – can we restrict attention only to
regimes that are feasible and interpretable in practice?
• Linear models produce rules involving linear combinations ofcharacteristics – what if we want to restrict to rules involvingcut-offs/thresholds ?
40/47 Personalized Medicine and Statistics

Issues
• This all depends on the chosen regression models• If the regression model(s) are not correct, an estimated optimal
regime could be very different from the true optimal regime• Are there other ways to estimate an optimal regime that are less
sensitive to chosen models?• If X1, X2 are high-dimensional, rules could be very complicated
(and how to select the likely tailoring variables?)• Distrust of “black boxes” – can we restrict attention only to
regimes that are feasible and interpretable in practice?• Linear models produce rules involving linear combinations of
characteristics – what if we want to restrict to rules involvingcut-offs/thresholds ?
40/47 Personalized Medicine and Statistics

Issues
• What if more than one outcome is of interest? E.g., balancingefficacy and toxicity in cancer treatment?
• Assessment of uncertainty (e.g., standard errors, confidenceintervals)?
• Design principles (e.g., sample size) for SMARTs?• Once an optimal regime is estimated, should it be compared to
standard of care in a conventional clinical trial?• Can real-time regimes be developed?
41/47 Personalized Medicine and Statistics

Issues
• What if more than one outcome is of interest? E.g., balancingefficacy and toxicity in cancer treatment?
• Assessment of uncertainty (e.g., standard errors, confidenceintervals)?
• Design principles (e.g., sample size) for SMARTs?• Once an optimal regime is estimated, should it be compared to
standard of care in a conventional clinical trial?• Can real-time regimes be developed?
41/47 Personalized Medicine and Statistics

Next steps
• Statistical research is ongoing to address all of these issues (andis way ahead of what is actually being done in practice)
• SMARTs and estimation of optimal regimes have beenembraced in behavioral and mental health research
• But much less so in chronic diseases like cancer, CVD, HIVinfection
(with notable exceptions. . . )• Must challenge the conventional clinical trial paradigm and
myopic view of treatment
42/47 Personalized Medicine and Statistics

Next steps
• Statistical research is ongoing to address all of these issues (andis way ahead of what is actually being done in practice)
• SMARTs and estimation of optimal regimes have beenembraced in behavioral and mental health research
• But much less so in chronic diseases like cancer, CVD, HIVinfection (with notable exceptions. . . )
• Must challenge the conventional clinical trial paradigm andmyopic view of treatment
42/47 Personalized Medicine and Statistics

Next steps
• Statistical research is ongoing to address all of these issues (andis way ahead of what is actually being done in practice)
• SMARTs and estimation of optimal regimes have beenembraced in behavioral and mental health research
• But much less so in chronic diseases like cancer, CVD, HIVinfection (with notable exceptions. . . )
• Must challenge the conventional clinical trial paradigm andmyopic view of treatment
42/47 Personalized Medicine and Statistics

Next steps
• Statistical research is ongoing to address all of these issues (andis way ahead of what is actually being done in practice)
• SMARTs and estimation of optimal regimes have beenembraced in behavioral and mental health research
• But much less so in chronic diseases like cancer, CVD, HIVinfection (with notable exceptions. . . )
• Must challenge the conventional clinical trial paradigm andmyopic view of treatment
42/47 Personalized Medicine and Statistics

Thought Leaders
2013 MacArthur Fellow Susan Murphy and Jamie Robins
43/47 Personalized Medicine and Statistics

Thought Leaders
Peter Thall
44/47 Personalized Medicine and Statistics

Summary
The goal of truly personalized medicine is still elusive
I hope I have convinced you that statistical science is essential toreaching this goal
45/47 Personalized Medicine and Statistics

Summary
The goal of truly personalized medicine is still elusive
I hope I have convinced you that statistical science is essential toreaching this goal
45/47 Personalized Medicine and Statistics

All things statistics
http://www.worldofstatistics.org/
http://thisisstatistics.org/
46/47 Personalized Medicine and Statistics

References
Schulte, P. J., Tsiatis, A. A., Laber, E. B., and Davidian, M. (2014). Q-and A-learning methods for estimating optimal dynamic treatmentregimes. Statistical Science, in press.
Zhang, B., Tsiatis, A. A., Laber, E. B., and Davidian, M. (2012). Arobust method for estimating optimal treatment regimes. Biometrics68, 1010–1018.
Zhang, B., Tsiatis, A.A., Davidian, M., Zhang, M., and Laber, E.B.,(2012). Estimating optimal treatment regimes from a classificationperspective. Stat 1, 103–114.
Zhang, B., Tsiatis, A. A., Laber, E. B., and Davidian, M. (2013).Robust estimation of optimal dynamic treatment regimes forsequential treatment decisions. Biometrika 100, 681–694.
47/47 Personalized Medicine and Statistics