Embed Size (px)
Citation preview

THE RELATIONSHIP BETWEEN TRANSFORMATIONAL LEADERSHIP AND
ORGANIZATIONAL COMMITMENT IN NONPROFIT LONG TERM CARE
ORGANIZATIONS: THE DIRECT CARE WORKER PERSPECTIVE
___________________________________
By
JEANETTE A. PORTER
___________________________________
A DISSERTATION
Submitted to the faculty of the Graduate School of Creighton University in Partial
Fulfillment of the Requirements for the degree of Doctor of Education in
Interdisciplinary Leadership
_________________________________
Omaha, NE
(October 7, 2014)

Copyright 2014, Jeanette A. Porter
This document is copyrighted material. Under copyright law, no part of this document may be reproduced without the expressed permission of the author.
iii
Abstract
The United States population is rapidly aging, impacting the demand and supply of direct
care workers who provide long term care services. Retaining direct care workers will be
a workforce concern for industry and policy leaders for decades to come. Issues such as
turnover, recognition, and supervisory practices have all been studied relative to direct
care worker retention, but leader behaviors are of special interest because of documented
influence on organizational commitment. Research on leader behaviors has been focused
on managerial and executive levels, with scant consideration in long term care at the
lower hierarchical levels. The quantitative correlational study explored the relationship
between transformational leadership and organizational commitment among 322 direct
care workers employed by nonprofit, multi-level long term care organizations located in
the Midwest. Results revealed a statistically significant relationship between
transformational leadership and affective and normative commitment dimensions, with
no significant relationship found between transformational leadership and continuance
commitment. In considering differences between long term settings, findings indicated
significance with organizational commitment, but not for transformational leadership,
suggesting that other factors, such as autonomy, may contribute more to organizational
commitment than does transformational leadership. The study results are beneficial to
industry leaders, researchers, and policymakers for addressing operational policies,
leadership training, human resource practices, and workforce policy development.
Keywords: transformational leadership, organizational commitment, affective
commitment, continuance commitment, normative commitment, Midwest, long term care
organizations, nonprofit
iv
Dedication
I first thank my parents, John and Patricia Gebhart, who instilled in me a love of lifelong
learning and who have always demonstrated God’s love to those around them. To my
husband, Chad, and our children, Jenae and Quinton, who demonstrated an incredible
level of patience for my limited availability in the evenings and on weekends; thank you
for your understanding and encouragement to meet my goals and for your love and
support during my moments of frustration. To the Creighton University faculty and staff
in the Ed.D. Leadership Program, thank you for helping me grow in my Catholic faith
and for living out the Jesuit values.
v
Acknowledgements
I wish to thank my committee members, Dr. Jenna Woster, Dr. Peggy Hawkins,
and Dr. Kathleen Zajic, who provided encouragement and direction throughout the
dissertation process. Thank you to Dr. Peggy Hawkins, who also served as my advisor
and provided me with support and encouragement along my journey. A special thank
you is extended to Dr. Isabelle Cherney for her words of wisdom, her personal interest in
every student, and her passion for leadership as the director of the Ed.D. Leadership
Program. A special thank you goes to Dr. Rob Koonz who inspired my dissertation topic
during the organizational behavior course. In addition to those already mentioned, I am
grateful to every faculty who taught me in the program and uniquely inspired me in my
learning. I sincerely appreciate Cohort 10 for all their encouragement and support
throughout my doctoral journey, especially Diana McGuire and Daniel Hoffman-Zinnel.
I would also like to acknowledge the University of South Dakota Beacom Opportunity
Fund for providing me a $2500 research stipend to complete the data collection phase of
my research.
vi
Table of Contents
Page
Abstract . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . iii
Dedication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iv
Acknowledgements. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . v
Table of Contents. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vi
List of Tables . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . ix
CHAPTER ONE: INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Background of the Problem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Statement of the Problem. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Purpose of the Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Research Questions and Hypotheses. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Method Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Definition of Terms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Assumptions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Delimitations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Limitations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Significance of the Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
CHAPTER TWO: LITERATURE REVIEW . . . . . . . . . . . . . . . . . . . . . . . 18
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Literature Search Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Transformational Leadership . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
vii
Historical Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Full Range Leadership Theory . . . . . . . . . . . . . . . . . . . . . . . . . . . .21
Transformational leadership constructs . . . . . . . . . . . . . . . . . . . . . 22
Idealized influence. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Inspirational motivation . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Intellectual stimulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Individualized consideration . . . . . . . . . . . . . . . . . . . . . . . . . 23
Transactional leadership constructs . . . . . . . . . . . . . . . . . . . . . . . 23
Contingent reward . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Management by exception . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Nontransactional laissez-faire construct. . . . . . . . . . . . . . . . . . . . . 24
Leadership Challenge Theory . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Leadership practice constructs . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Model the way . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Inspire a shared vision . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Challenge the process . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Enable others to act . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Encourage the heart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Other Theories . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Criticism of Transformational Leadership . . . . . . . . . . . . . . . . . . . . . . 27
Organizational Commitment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Affective Commitment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Continuance Commitment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
viii
Normative Commitment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Empirical Evidence. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
Transformational Leadership and Organizational Commitment . . . . . . . . . . . . . . 39
The Nonprofit Perspective . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
Leadership in Nonprofit Organizations . . . . . . . . . . . . . . . . . . . . . . . 46
Similarities to Transformational Leadership Theories. . . . . . . . . . . . . . . . 48
Summary. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
CHAPTER THREE: METHODOLOGY. . . . . . . . . . . . . . . . . . . . . . . . . . 52
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
Research Questions and Hypotheses . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
Description of Sample. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
Survey Instrumentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Leadership Practices Inventory . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Three-Component Model of Employee Commitment . . . . . . . . . . . . . . . 58
Demographics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
Pilot Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
Variables. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
Data Collection Procedures. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
Data Analysis Plan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
Assumptions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
Ethical Considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
ix
CHAPTER FOUR: FINDINGS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
Review of the Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .70
Data Analysis Procedures. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
Participant Characteristics. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
Survey Instrument Descriptive Statistics and Reliability Levels. . . . . . . . . . . 75
Research Question One and Related Hypotheses . . . . . . . . . . . . . . . . . . 77
Research Question Two and Related Hypothesis. . . . . . . . . . . . . . . . . . 80
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
CHAPTER FIVE: CONCLUSIONS AND RECOMMENDATIONS . . . . . . . . . . . 84
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84
Summary of the Study. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85
Summary of the Findings. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86
Implications for Action/Recommendations for Further Research . . . . . . . . . . . . . . 90
Scholarship . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91
Recommendation one: Further research is warranted. . . . . . . . . . . . . . . 91
Industry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
Recommendation two: Review operational policies. . . . . . . . . . . . . . . 93
Recommendation three: Incorporate leadership development training. . . . . . 94
Recommendation four: Revisit human resources practices. . . . . . . . . . . 94
Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96
Recommendation five: Evaluate the content of workforce resources . . . . . . 96
x
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100
Appendices. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 116
.

xi
List of Tables Page
Table 1. Parallels of Transformational Leadership Theories. . . . . . . . . . . . . . . 21
Table 2. Pilot Study Reliability Levels for LPI and TCM Survey Instruments, by
Subscales . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
Table 3. LPI and TCM Means and Standard Deviations . . . . . . . . . . . . . . . . 75
Table 4. Current Study Reliability Levels for LPI and TCM Survey Instruments, by
Subscales . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77 Table 5. Spearman’s rho Correlations between Transformational Leadership and
Organizational Commitment, Overall and by Subscales. . . . . . . . . . . . . 80
Running head: LEADERSHIP AND ORGANIZATIONAL COMMITMENT 1
CHAPTER ONE: INTRODUCTION
Background of the Problem
The failure to attract and retain direct care workers (DCWs) in long term care has
been described as the worst challenge facing the long term care industry (Stone, 2011).
For the last three decades, recruitment and retention of direct care workers has remained
a major issue for providers and policymakers at all government levels (Stone, 2004;
2011). At the same time, the Bureau of Labor Statistics (BLS) projects a large increase in
the demand for DCWs, spanning the long term care continuum (PHI, 2013a; 2013b;
Smith & Baughman, 2007). Salient factors affecting recruitment and retention include
challenging work environments, noncompetitive wages, and supervisor qualities (Culp,
Ramey, & Karlman, 2008; Decker, Harris-Kojetin, & Bercovitz, 2009; Lee, Coustasse, &
Sikula, Sr., 2011; Stearns & D’Arcy, 2008; Stone, 2004). Stone (2011) asserted that
interdependent factors such as regulations, wage levels, targeted government workforce
resources, organizational management, and society’s value of caregiving all influence
recruitment and retention. Of the organizational management elements, studies have
found that compensation, work environments and interpersonal relationships directly
affect DCWs (Culp, et al., 2008; Stearns & D’Arcy, 2008; Stone, 2004; 2011).
In 2012, the BLS reported a figure of 4 million DCWs, representing three
occupations: nursing assistants, home health aides, and personal care aides. This is an
under-reported statistic because there are an additional 800,000 DCWs working as
independent providers for consumers and state or county agencies (PHI, 2013b). The
nearly 5 million DCWs in the 2012 labor market represents an increase of over 30% from
2008 BLS numbers (PHI, 2011). BLS reports home health aides, nursing assistants, and
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 2
personal care aides within its top ten occupations projected to produce new jobs within
the U.S. economy (PHI, 2011; 2013b), primarily due to the growing aging population.
Projected demand indicates an additional 1.6 million DCW positions added to the labor
market by 2020 (PHI, 2013b). Despite the positive growth projections, median hourly
wages for DCWs ($10.63) are below the national median wage for all U.S. workers
($16.71), with inflation-adjusted hourly wages having declined over the last ten years
(PHI, 2013b). Many DCWs work part-time and lack health coverage; many also earn
below 200 percent of the federal poverty income level and rely on some level of public
assistance, such as food stamps (PHI, 2013b; Stone, 2004).
The Census Bureau projects the 65 and older age demographic to grow by 45
percent by 2025 (Census Bureau, n.d.) and the fastest growing segment of the population
are those 85 and older (Robnett & Chop, 2010). The growth and aging of the older adult
population will be accompanied by greater chronic disease burden (Dall et al., 2013;
Robnett & Chop, 2010; Stone, 2004). The growth in direct care employment will
depend on workforce supply and demand, particularly in rural areas. Workforce demand
outpaces supply (PHI, 2013a; Smith & Baughman, 2007), and health policy has a
substantial impact on leaders’ ability to determine wages, health insurance, and other
compensation (Smith & Baughman, 2007; Stone, 2004). As a result, other factors such as
leadership behaviors and practices become more prominent management considerations
in determining organizational commitment for DCWs.
The traditional hierarchy in long term care has assured that the locus of control
remains with those furthest from patient care (Caspar & O’Rourke, 2008). DCWs
provide over 80% of all patient care, have the least amount of education, receive the
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 3
lowest pay, and exercise the least amount of decision-making authority and autonomy
(Caspar & O’Rourke, 2008; Liu, Liu, & Wang, 2011; PHI, 2013a; 2013b; Stone, 2011).
DCWs have stated that what they desire most is respect, recognition and rewards, as well
as inclusion in decision-making and empowerment (Bowers, Esmond, & Jacobson, 2003;
Casper & O’Rourke, 2008; Leutz, Bishop & Dodson, 2009; Secrest, Iorio & Martz, 2005;
Stone, 2004; 2011). Such factors have influenced organizational commitment (Liou,
2008). As a result, it is important to consider the DCW perspective in understanding
commitment levels to long term care organizations.
Statement of the Problem
Similar to other industries and organizations, long term care leaders must consider
how leadership practices influence organizational commitment. To date, scant literature
exists that addresses the DCW perspective of leadership qualities and the effect on
organizational commitment. Furthermore, the existent literature primarily explores the
leadership qualities of higher hierarchical levels, despite evidence that transformational
leadership behaviors have been shown to cascade downward to other managerial, leader
positions, benefitting organizational performance as a whole (Bass, Waldman, & Avolio,
1987; Eaton, 2001; Godwin & Neck, 1998). The correlation between transformational
leadership and organizational commitment among DCWs in long term care organizations
has not been empirically tested. Job characteristics and work experiences have been
identified as influences, or antecedents, on organizational commitment; these
characteristics and experiences include job challenge, work relationships, feedback
quality, group attitudes, empowerment, role stress, job satisfaction and trust (Liou, 2008).
Transformational leadership has not been studied as an antecedent in the context of long
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 4
term care. To respond to this deficiency, additional research is warranted to study
leadership behaviors that are of immediate influence for DCWs, from the immediate
supervisor.
Furthermore, while leadership has been studied both empirically and conceptually
across many disciplines and industries, McMurray, Pirola-Merlo, Sarros, and Islam
(2010) argued that context is lacking in the literature relative to differences in for-profit
and nonprofit organizations. In their study of faith-based organizations specifically, they
contended unique challenges exist because organization and employee issues are
addressed with spirituality in mind (McMurray, et al., 2010). Thus, nonprofit-based
missions present complexity in understanding the relationship of leadership on
organizational and employee variables (McMurray et al., 2010). Contextually, the study
of nonprofit organizations reflects the importance of social missions in the provision of
welfare, health care, education and other services. The nonprofit long term care industry
has historically stressed a wide range of benefits of nonprofit management and
ownership, despite a lack of empirical evidence. This study intends to advance
knowledge in this area.
Purpose of the Study
The purpose of the quantitative correlational study was to explore the relationship
between transformational leadership and organizational commitment among DCWs in
nonprofit, long term care organizations. The predictor variable was defined as
transformational leadership, generally understood as a process whereby leaders have a
conscious goal to develop followers into leaders, exhibit behaviors that elicit trust, and
display self-sacrificial perspectives to build commitment and influence, and demonstrate
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 5
a moral compass towards mission and purpose (Avolio, 2011; Bass, 1985; Kouzes &
Posner,1988; 2012). The criterion, or outcome, variable was defined as organizational
commitment, generally described as a psychological state linking employees to their
organizations and considered along three dimensions: affective, continuance, and
normative (Meyer & Allen, 1997, p. 23).
Research Questions and Hypotheses
Two primary research questions were explored in the research study to better
understand the relationship between transformational leadership and organizational
commitment among direct care workers (DCW) in nonprofit long term care
organizations. The first question inquired about the relationship between
transformational leadership practices as measured by the subscales of the Leadership
Practices Inventory (LPI) (Kouzes & Posner, 2013) and organizational commitment as
measured by the Three-Component Model (TCM) of Employee Commitment Survey
(Meyer & Allen, 2004). The rationale for the question rested on the assumption that
DCWs perceive leadership practices to influence the work environment, thus affecting
DCW organizational commitment, or intent to stay. The second question inquired about
potential differences in the types of long term settings, such as nursing facilities, assisted
living, and senior housing. The question was important in understanding how differences
in long term settings might influence the variables of interest and where interventions
might be most valued by the industry (Kim, Wehbi, DelliFraine, & Brannon, 2013). The
research questions and specific hypotheses tested in this study included:
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 6
RQ1: What is the relationship between transformational leadership and organizational
commitment (affective, continuance, and normative) among direct care workers in
nonprofit long term care organizations?
H1: There is a significant positive relationship between transformational
leadership and DCW affective commitment.
H2: There is a significant inverse relationship between transformational
leadership and DCW continuance commitment.
H3: There is a significant positive relationship between transformational
leadership and DCW normative commitment.
RQ2: Is there a difference, if any, between types of long term care settings on
transformational leadership and organizational commitment?
H4: There is no difference between types of long term care settings for
transformational leadership and organizational commitment.
Method Overview
The theories of transformational leadership and organizational commitment
formed the theoretical framework of the study. For purposes of this theoretical
framework, the study addressed the transformational leadership theory of Kouzes and
Posner (1988; 2012), coined The Leadership Challenge. The theory reflects Burns
(1978) notion that the ultimate effects of leadership are only understood by way of
evaluating leader and follower interactions, or in research design, what is referred to as
causal mechanisms (Gerring, 2012). Kouzes and Posner (2012) have accumulated an
extensive database of survey responses spanning organizational sectors using the
Leadership Practices Inventory (LPI). The long term care industry, specifically nonprofit
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 7
organizations, prefers research applications that support its capacity to communicate in
terminology easily understood by all levels of an organization, suggesting the industry
will respond more favorably to a study utilizing the Kouzes and Posner (2012) theory.
Organizational commitment is considered one of many job attitudes studied
within the body of organizational behavior research (Robbins & Judge, 2012).
Substantial evidence exists to illustrate a predictive relationship of organizational
commitment (Meyer & Allen, 1997). The evolution of the concept of organizational
commitment has resulted in acknowledgment of and an empirical understanding of three
primary dimensions: affective, continuance, and normative (Liou, 2008; Meyer & Allen,
1997). Affective commitment represents the emotional component of organizational
commitment, or the degree to which employees are emotionally attached to the
organization and its beliefs and values (Liou, 2008; Meyer & Allen, 1997; Robbins &
Judge, 2012). Continuance commitment considers employees’ perceptions of value in
staying with the organization, including socioeconomic factors such as wages and
benefits (Liou, 2008; Meyer & Allen, 1997; Robbins & Judge, 2012). Normative
commitment occurs as a result of employees’ sense of obligation to remain with the
organization; a level of conformity exists between beliefs and values and organizational
norms (Liou, 2008; Meyer & Allen, 1997; Robbins & Judge, 2012). Because of the
depth and breadth of organizational commitment as a concept, it is important to
empirically study it along these commitment dimensions in order to further evaluate its
effect in the workplace. This study utilized the (TCM) of Employee Commitment Survey
developed by Meyer and Allen (2004), modified from their original Three-Component
Model of Commitment Survey (1997).
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 8
The study sample consisted of DCWs currently working at nonprofit long term
care organizations in the Midwest and utilized a quantitative correlational design.
Quantitative methods are more appropriate than qualitative methods to determine the
strength of relationships between the variables of interest (Gerring, 2012). Unlike a
qualitative study, use of a quantitative correlational design helps determine the strength
of the relationships existing between variables (Creswell, 2012). Because the purpose of
the study was to explore the relationship between transformational leadership and
organizational commitment among DCWs in nonprofit long term care organizations, a
quantitative approach was appropriate.
Participating organizations were required to provide permission for onsite surveys
with DCWs. Organization administrators completed a demographic information sheet in
order to obtain general information on the organization, such as types of long term care
services provided. All DCWs were invited to participate in the survey during designated
times throughout the day. Snacks were provided as an incentive to participate, as
approved by the IRB. As part of the survey completion, each participant was provided
with informed consent/assent documentation to further explain and solicit voluntary
participation in the study. Participants completed a demographic form and the LPI
survey (Kouzes & Posner, 2013) and the TCM Employee Commitment Survey (Meyer &
Allen, 2004), all of which were combined into one document for ease in instruction and
completion. Survey collection areas were chosen for accessibility to DCWs while also
providing for a private area to complete the surveys. Supervisors or other organization
agents were discouraged from access to the survey area during survey completion. To
ensure confidentiality and anonymity, no identifying information was collected from the
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 9
DCWs. Surveys were turned in directly to the study investigator and put in a confidential
box for transfer from the study site. No reports of DCW participation were provided to
the organization. Organizations were de-identified in the data software application. The
survey document was field tested in a pilot study with 13 DCWs prior to administering
the surveys for the study, to test for usefulness, ability to complete the surveys, and
reliability. The participants assisting in the field test were excluded from the study.
Internal reliability testing was conducted using Cronbach’s alpha to determine if
the survey scales were reliable (Creswell, 2012). Correlational, nonparametric statistical
analysis was used to evaluate the first research question, test the respective hypotheses,
and consider the strength of the variables based upon the specific survey subscales within
the transformational leadership and organizational commitment constructs. To evaluate
the data for the second research question regarding differences between types of long
term care settings, the independent t-test was used to compare groups (Creswell, 2012).
Definition of Terms
The following definitions of terms were used in this research study:
Activities of Daily Living (ADLs): Major everyday activities such as eating, bathing,
walking, and toileting.
Affective Commitment: “An employee’s emotional attachment to, identification with, and
involvement in the organization; employees remain with the organization because they
want to” (Meyer & Allen, 1997, p. 11).
Continuance Commitment: “An employee’s awareness of the costs associated with
leaving the organization; employees remain with the organization because they have to”
(Meyer & Allen, 1997, p. 11).
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 10
Direct Care Worker (DCW): A direct care worker is an individual who provides a high
level of direct care and service to others requiring long term care services in a broad set
of long term care settings. In addition to providing assistance with ADLs, a DCW also
provides assistance with instrumental activities of daily living (IADLs). A direct care
worker requires limited training beyond a high school education. For purposes of this
study, a DCW consisted of positions such as nursing assistants, medication assistants,
home health aides, personal care assistants, housekeeping/laundry assistants, universal
workers, cooks, dietary aides, and related positions.
Frontline Worker: A term used synonymously with direct care worker in this study.
Home Health Aides (HHAs): A direct care worker who provides the same care and
services as a nursing assistant but within the home or community setting (PHI, 2013b).
Instrumental Activities of Daily Living (IADLs): Normal everyday activities such as
housekeeping, food preparation, shopping, transportation, finances, and laundry.
Long Term Care Organization: Organizations that provide a broad set of medical,
nursing, rehabilitation, palliative care, and home assistance services to patients in assisted
living, home health, nursing facilities, hospice, and other community-based settings.
Long term care organizations may also be referred to as long term care providers. For the
purpose of this study, long term care organizations provide multiple levels of long term
care services.
Normative Commitment: “An employee’s feeling of obligation to continue employment;
employees remain with the organization because they feel they ought to” (Meyer &
Allen, 1997, p. 11).
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 11
Nursing Assistants (NAs): A direct care worker who assists residents with activities of
daily living (ADLs) and instrumental activities of daily living (IADLs). They may also
perform limited clinical tasks, such as blood pressure readings and range of motion
exercises. Nursing assistants work in nursing homes, assisted living facilities, hospitals,
and other community-based settings (PHI, 2013b).
Organizational Commitment: “A psychological state linking employees to their
organizations” (Meyer & Allen, 1997, p. 23). Organizational commitment is considered
along three dimensions: affective, continuance, and normative.
Personal Care Aides (PCAs): A direct care worker who provides assistance with ADLs
and IADLs. They work in many different long term care settings and may also be
employed and supervised directly by consumers, known as independent providers. They
may have many titles, including personal care attendant, home care worker, or personal
assistant (PHI, 2013b).
Transformational Leadership: A process whereby leaders have a conscious goal to
develop followers into leaders, exhibit behaviors that elicit trust, and display self-
sacrificial perspectives to build commitment and influence, and demonstrate a moral
compass towards mission and purpose (Avolio, 2011; Bass, 1985; Kouzes &
Posner,1988; 2012).
Assumptions
There were multiple assumptions for the study. First, it was assumed that
participants would answer the surveys honestly and completely and would complete the
surveys with their immediate supervisor in mind. It was also assumed that cultures
within the long term care organizational sites provide safe and confidential environments
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 12
for DCWs to participate in the study. Hence, local leadership was assumed to be
supportive of the study. Additionally, it was presumed that the sample size would be
high due to effective use of time and location for survey completion. The researcher also
presumed that participants would trust the researcher to maintain confidentiality and
anonymity, thus also affecting response rates. Finally, the researcher assumed that the
relationship between transformational leadership and organizational commitment can be
demonstrated using proper research rigor and methodology (Gerring, 2012).
Delimitations
The study was restricted to surveying DCWs in nonprofit long term care
organizations in the Midwest. Only those nonprofit long term care organizations with
multiple levels of long term care services were invited to participate in the study. The
study did not include supervisors or other employees not meeting the definition of a
DCW, thus limiting the perspective to the intent of the study. Survey instruments used
were limited to the demographic questions, the Kouzes and Posner LPI (Kouzes &
Posner, 2013), and the Meyer and Allen TCM of Employee Commitment Survey (Meyer
& Allen, 2004). The data collection and analysis occurred from May 2014 to July 2014.
The sample size included 322 DCWs from the participating organizations. A sample size
of 287 was targeted in order to achieve a 4-6% error rate with a 95% confidence interval
(Creswell, 2012). A target of 5-6 long term organizations was needed to achieve this
sample size, and nine organizations participated. Increasing the sample size would have
added time and costs.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 13
Limitations
The study was conducted on site at each participating location. Participants of the
study provided individual perspectives of leadership practices within their respective
location. Responses may contain bias or be affected by psychological and emotional
states at the time of the survey. Participants represented an unknown proportion of long
term care settings provided by their respective locations. Response rates varied
depending on the time and location of the surveys and the support of leadership.
Significance of the Study
The research study was stimulated by practical considerations. DCWs form the
core of the long term care industry, providing services essential to the quality of life and
quality of care for consumers. Demographic trends do not bode well for the future
availability of direct care workers because of the rapidly aging United States population.
The population of older adults is growing dramatically and will continue to do so over the
next 50 years; the baby boomer generation will reach 65 years of age between 2011 and
2029, those age 85 and older are the fastest growing group of older adults, and by 2050,
one in five Americans will be over the age of 65 (Center for Health Workforce Studies,
2006; Dall et al., 2013). Leaders must utilize practices that develop and sustain the
workforce at both policy and practice levels. Understanding the relationship of
leadership and organizational commitment may help provide a better understanding of
leadership factors affecting the commitment process and allow industry practitioners and
researchers to consider carefully the effect of leadership behavior and practices on
DCWs. Findings of the study can benefit scholarship, practice, and policy within the
long term care industry.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 14
Within scholarship, meta-analysis of transformational leadership has revealed an
influence on organizational commitment in industries other than long term care (Avolio,
2011). Researchers have supported additional study on transformational leadership
within hierarchical levels (Avolio, 2011; Heldenbrand & Simms, 2012). This study
responded to this deficiency, focusing research on leadership practices and behaviors that
have immediate influence for DCWs, their immediate supervisors. This study also
provided additional evidence-based insight into the relationship between transformational
leadership and organizational commitment among workers closest to patient care.
Furthermore, the study’s focus on nonprofit organizations will contribute to the
expanding literature in the nonprofit leadership arena. Such research will enhance the
literature as well as provide evidence-based support for leadership development in the
long term care industry.
For industry practice application, long term care leaders must consider how
leadership practices and behaviors affect organizational commitment. Liou (2008)
argued that organizational commitment must be given more priority in health care
organizations. In prioritizing an emphasis on organizational commitment, long term care
leaders can focus their efforts on antecedents that foster increased organizational
commitment and, as a result, increase retention and performance. Organizational
commitment is an outcome of a complex set of factors. Simply providing more
education, higher pay, or better supervisors will not likely improve organizational
commitment to any appreciable degree. However, understanding how such factors
influence organizational commitment lends value to the interventions that should be
considered and reinforced to produce necessary improvement.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 15
Specifically, leadership styles have been shown to influence turnover (Donoghue
& Castle, 2009), and nursing home administrators specifically have been found to lack
leadership skills necessary to improve organizational performance (Scott, Vojir, Jones, &
Moore, 2005). Low organizational commitment contributes to turnover, which is costly
to long term care employers (Smith & Baughman, 2007), most recently estimated at over
$3300 for each turnover (Stone, 2004). High quality leadership and management,
including the offering of recognition, feedback, and a culture of value and respect for
DCWs has been associated with low turnover (Eaton, 2001). To develop and sustain a
quality workforce, leaders must have a broader understanding of what leadership factors
affect organizational commitment.
Furthermore, the evolution of person-centered care into the long term care
industry has demanded more of providers in the implementation of practices that
operationalize person-centered care concepts. Successfully implemented, person-
centered care models have been shown to positively influence the work environment by
inviting DCWs to actively participate in decision-making, encourage teamwork and
expand their job tasks beyond the traditional job role (Leutz, Bishop & Dodson, 2009;
Stone, 2011). As a result, transformational leadership is a consideration in the
supervisor-DCW relationship within the person-centered care approach. Understanding
the relationship between transformational leadership and organizational commitment will
lend value to the long term care industry in modifying operational practices, identifying
training and development needs, and revisiting human resource practices.
From a policy view, the healthcare environment is in the midst of drastic change
due to changes in existing regulations, broad health reform, and effects of the Patient
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 16
Protection and Affordable Care Act. Government reimbursements, regulations, and
workforce resources all influence recruitment and retention in the long term care
industry. Compensation in particular has been shown to directly affect DCWs (Stone,
2004; 2011) and is linked to continuance commitment, one of the three dimensions of
organizational commitment (Meyer & Allen, 2004). Such statistics reinforce the
challenges in retaining DCWs as a primary employee source in long term care.
Understanding the degree to which transformational leadership influences organizational
commitment, or the intent to stay on the job, is integral to the formation of long term care
policy that maintains the current DCW supply. As previously discussed, the aging
population is creating a demographic trend that will influence the demand for long term
care services. A quality long term care workforce is required to support the consumers of
long term care services and their informal caregiving networks. Recruiting and retaining
quality DCWs is a major issue for policymakers at state and federal levels. This study
can advance policymaker understanding of leadership factors affecting DCW
organizational commitment. Furthermore, it will assist in clarifying for policymakers the
degree to which the dimensions of organizational commitment are influencing DCWs
intent to stay. Knowledge of this relationship may assist policymakers in formulating
policies and targeting resources in ways that lead to successful development of the
frontline workforce.
Summary
A growing aging population and workforce shortage provide great challenges for
the long term care industry. Leaders within the industry must face these challenges not
only by addressing a wide range of external factors but also by looking inward to
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 17
leadership practices directly affecting the workforce they hope to retain. The purpose of
the study was to explore the relationship between transformational leadership and
organizational commitment among DCWs in nonprofit long term care organizations. A
quantitative correlational design study was used to assess the strength of the relationships
between the variables. The study included DCWs currently working in nonprofit long
term care organizations located in the Midwest. The research contributes to filling a gap
in the literature by identifying the relationship of leadership practices as a predictor of
organizational commitment for DCWs, an often ignored perspective in long term care.
As the health care landscape continues to change, long term care providers will need to
have the leadership skills necessary to overcome challenges, implement new operational
models, and address workforce retention. The research study provided an opportunity to
establish both external and internal validity based on the sampling quality and results of
the quantitative analysis (Gerring, 2012).
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 18
CHAPTER TWO: LITERATURE REVIEW
Introduction
Chapter one included an overview of the study and its purpose to explore the
relationship between transformational leadership and organizational commitment among
DCWs in nonprofit long term care organizations. Information was provided regarding
the problem statement and the significance of the study. The research questions
described the basis of the study. Chapter two presents a literature review of
transformational leadership, organizational commitment, and nonprofit considerations in
context to the intended study.
Chapter two contains five main sections: literature search process,
transformational leadership, organizational commitment, nonprofit considerations, and
conclusions. Each section contains discussion of the study variables addressing broadly
the perspectives of history, theory, and relationship to leadership and outcomes.
Literature Search Process
The review of the literature occurred manually and electronically via libraries,
library databases, and the Internet. The literature search primarily included the two
variables, transformational leadership and organizational commitment, in the initial broad
search and subsequently narrowed to the health care industry, the long term care industry,
and finally, the nonprofit sector. A search of the terms transformational leadership and
direct care workers, transformational leadership and long term care, transformational
leadership and nursing facilities, organizational commitment and direct care workers, in
addition to similar combinations attempting to isolate the variables to direct care workers
and long term care produced minimal results. Thus, more defined search terms were
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 19
required to isolate specific health care related studies on leadership and organizational
commitment. Specific search terms included nursing assistants, home health, personal
care assistants, employee commitment, worker commitment, nurses, nurse managers,
nurse supervisors, and frontline workers. Nonprofit search terms included nonprofit
sector, not-for-profit, nonprofit organizations and non-profit. Combining these search
terms with the study variables provided additional literature results. The databases used
to search for peer-reviewed research were EBSCOHost, ProQuest, ProQuest Digital
Dissertations, Thomson Gale, InfoTrac, ERIC, AgeLine, MEDLINE, EBSCO
MegaFILE, SocINDEX, PsychINFO, Business Source Premier, CINAHL, and Academic
Search Premier.
Transformational Leadership
Historical Overview
The term transformational leadership originated by Downton in his early writings
on charismatic leadership and leader follower relations in mass social movements
(Downton, 1973; Northouse, 2007). However, the term went unnoticed until it evolved
from Burns’ (1978) theoretical perspective of transforming leadership, whereby leaders
seek to identify the higher need motives of followers and convert followers into leaders
and ideally, moral agents, thus creating social change (emphasis added). Burns (1978)
discussed transforming and transactional leadership within a political context, evaluating
the behaviors and actions of leaders that led to political actions and social change. In his
seminal efforts in leadership research, Burns (1978) expressed a sincere curiosity about
leadership as a component of causation. He contended that leadership could be further
refined by definition and variety in order to deconstruct its multiple variables as causal
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 20
factors to a plethora of implications (Burns, 1978; Gerring, 2012). The application of
transforming leadership within the corporate context was suggested (Burns, 1978) and as
a result, transformational leadership was identified by Bass (1985) (emphasis added).
Bass (1985) distinguished leadership behavior via transformational (idealized
influence, inspirational motivation, intellectual stimulation, individualized consideration)
and transactional (contingent reward, management by exception) characteristics. Bass
incorporated concepts of Burns’ (1978) theory with elements of the path-goal theory
which House and colleagues expanded with regard to leadership and the pursuit of
employee performance and motivation (Northouse, 2007). Over time and in concerted
effort with colleagues Riggio and Avolio, the Full Range Leadership Theory (FRLT) was
developed, utilizing the aforementioned leadership behaviors to distinguish between
transformational, transactional, and laissez-faire leadership (Bass and Riggio, 2010).
During the same time Bass and colleagues were developing the FRLT, Kouzes
and Posner (1988; 2012) were exploring transformational leadership from a different
perspective. Kouzes and Posner (1988; 2012) suggested that leadership impact was best
understood by everyday leadership practices, or causal mechanisms (Gerring, 2012), that
occurred within a dynamic process. Through extensive qualitative research, five primary
leadership practices were identified as characteristic of effective leaders: model the way,
inspire a shared vision, challenge the process, enable others to act, and encourage the
heart, identified as the Leadership Challenge Theory (LCT) (Kouzes & Posner, 1988;
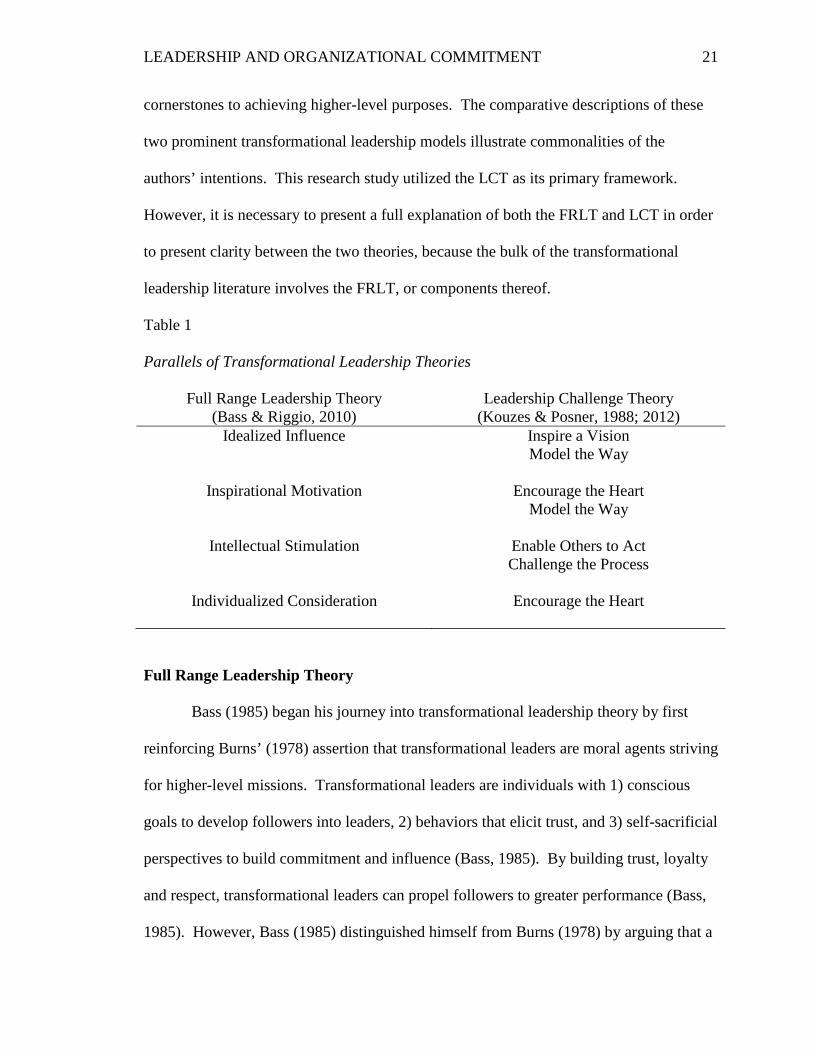
2012). As illustrated in Table 1, the Kouzes and Posner (1988; 2012) leadership practices
parallel the transformational leadership qualities identified in the FRLT such that
inspiration, vision, influence, motivation, development, and individual attention are
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 21
cornerstones to achieving higher-level purposes. The comparative descriptions of these
two prominent transformational leadership models illustrate commonalities of the
authors’ intentions. This research study utilized the LCT as its primary framework.
However, it is necessary to present a full explanation of both the FRLT and LCT in order
to present clarity between the two theories, because the bulk of the transformational
leadership literature involves the FRLT, or components thereof.
Table 1
Parallels of Transformational Leadership Theories
Full Range Leadership Theory (Bass & Riggio, 2010)
Leadership Challenge Theory (Kouzes & Posner, 1988; 2012)
Idealized Influence Inspire a Vision Model the Way
Inspirational Motivation Encourage the Heart
Model the Way
Intellectual Stimulation Enable Others to Act Challenge the Process
Individualized Consideration Encourage the Heart
Full Range Leadership Theory
Bass (1985) began his journey into transformational leadership theory by first
reinforcing Burns’ (1978) assertion that transformational leaders are moral agents striving
for higher-level missions. Transformational leaders are individuals with 1) conscious
goals to develop followers into leaders, 2) behaviors that elicit trust, and 3) self-sacrificial
perspectives to build commitment and influence (Bass, 1985). By building trust, loyalty
and respect, transformational leaders can propel followers to greater performance (Bass,
1985). However, Bass (1985) distinguished himself from Burns (1978) by arguing that a
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 22
progression existed in a leader’s evolution from a transactional to transformational leader.
As a result, the Full Range Leadership Theory (FRLT) was developed by Bass and
colleagues as a purported description of three typologies of leadership behavior:
transformational, transactional and nontransactional laissez-faire leadership, claiming a
need for balance between transformational and transactional leadership behaviors for
optimal effectiveness (Antonakis, Avolio, & Sivasubramaniam, 2003; Avolio, 2011). In
support of the FRLT, the Multi-factor Leadership Questionnaire (MLQ) was developed
for use in empirical research. Over time, the MLQ has been refined to its current nine
factor constructs representing distinction between transformational, transactional, and
laissez-faire characteristics.
Transformational leadership constructs. The transformational leadership
constructs were formulated by articulating the defining characteristics that motivate
followers to exceed their own expectations; they include idealized influence, inspirational
motivation, intellectual stimulation, and individualized consideration (Avolio, 2011;
Bass, 1985; Bass & Riggio, 2006).
Idealized influence. Followers seek to emulate leaders due to the leaders’ self-
sacrifice and higher-level mission and goals. Power is used to accomplish goals rather
than for personal gain. The idealized leader is seen as the central force for achieving the
vision. Followers rely on the leader to do the right thing despite how challenging it might
be to do so (Antonakis, Aviolio, & Sivasubramaniam, 2003; Avolio, 2011; Bass & Riggo,
2006; Bass & Riggio, 2010). In the nine factor MLQ, idealized influence is
differentiated by attribution (perception) and behavior (actions) (Antonakis, et al., 2003).
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 23
Inspirational motivation. Leaders are optimistic and enthusiastic and these
sentiments are positively perceived by followers. Such motivation is viewed as
meaningful to followers and inspires further spirit around the vision, mission, and goals
of the organization (Antonakis, et al., 2003; Avolio, 2011; Bass & Riggo, 2006; Bass &
Riggio, 2010).
Intellectual stimulation. Leaders challenge followers to improve, ask questions,
reframe problems, consider different perspectives, be innovative, and encourage new
approaches rather than the status quo (Antonakis, et al., 2003; Avolio, 2011; Bass &
Riggo, 2006; Bass & Riggio, 2010).
Individualized consideration. Leaders act as mentors and coaches to elicit
individual follower development. Differences are not only recognized in a supportive
manner, but also used to enhance creativity and innovation. Communication and
interaction is encouraged and personalized. Delegation is utilized as a development
mechanism rather than as an aspect of performance response (Antonakis, et al., 2003;
Avolio, 2011; Bass & Riggo, 2006; Bass & Riggio, 2010).
Transactional leadership constructs. Transactional leadership by itself mimics
the ideas of leader-member exchange and path-goal theories, whereby leaders reward or
discipline followers (members) based on the followers’ behaviors or performance
(Avolio, 2011; Northouse, 2007; Yukl, 2006). Leadership exchanges are driven by three
primary constructs, contingent reward, active management by exception, or passive
management by exception (Antonakis, et al., 2003; Avolio, 2011; Bass & Riggo, 2006;
Bass & Riggio, 2010).
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 24
Contingent reward. When followers satisfactorily meet expectations, leaders will
respond accordingly with rewards (Antonakis, et al., 2003; Avolio, 2011; Bass & Riggo,
2006; Bass & Riggio, 2010).
Management by exception. Management by exception involves the use of
corrective transactional behavior to monitor followers’ behaviors and performance.
Disincentives are utilized as warning for inadequate performance, and punitive action
may occur to correct unwanted behavior and performance. Whether management by
exception is defined as active or passive is distinguished by the level of ongoing
monitoring that occurs. Active management reflects an ongoing vigilance for mistakes,
whereas passive management waits for the mistakes to occur prior to taking action
(Antonakis, et al., 2003; Avolio, 2011; Bass & Riggo, 2006; Bass & Riggio, 2010).
Nontransactional laissez-faire construct. A nontransactional laissez-faire
leadership approach represents an absence of leadership. In essence, the leader avoids or
abdicates decision-making and does not use authority. When important situations arise,
actions are delayed and responsibility is ignored (Antonakis et al., 2003; Avolio, 2011;
Bass & Riggio, 2010).
Leadership Challenge Theory
Kouzes and Posner (2012) have studied leader behavior for over two decades and
identified transformational leadership as exemplified by five leadership practices that can
be learned: model the way, inspire a shared vision, challenge the process, enable others to
act, and encourage the heart. The Kouzes and Posner (2012) theory is coined The
Leadership Challenge and reflects Burns’ (1978) notion that the ultimate effects of
leadership are only understood by way of evaluating leader and follower interactions, or
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 25
in research design, what is referred to as causal mechanisms (Gerring, 2012). To support
research rigor, Kouzes and Posner (1988; 2012; 2013) developed a quantitative
measurement tool called the Leadership Practices Inventory (LPI). The LPI can be used
by leaders and followers to measure transformational leadership in a variety of
organizational settings (Kouzes & Posner, 2013). To date, over one million individuals
have completed the LPI to better understand the level of transformational leadership
within organizations, according to the researchers’ website.
Leadership practice constructs. The leadership practice constructs were
identified through early qualitative research with organizational executives striving to
understand and learn what key attributes existed when leaders were performing at their
personal best (Kouzes & Posner, 1988). Themes revealed qualities such as involvement,
persistence, vision, and encouragement (Kouzes & Posner, 1988). Using a qualitative
research approach, Kouzes and Posner (1988; 2012) established what they now call the
Five Practices of Exemplary Leadership: model the way, inspire a shared vision,
challenge the process, enable others to act, and encourage the heart.
Model the way. Modeling the way involves three distinct characteristics. First,
the leader must be self-aware of his or her personal beliefs and values. Once established,
the leader then needs to affirm the shared values of the group. Finally, the leader must
set the example, or model for others, what actions are aligned with the shared values
(Kouzes & Posner, 2012).
Inspire a shared vision. An exemplary leader has a dream, or vision, of what the
future can be. In inspiring the vision, the leader imagines and communicates the
possibilities and enlists others for the vision by appealing to common aspirations. The
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 26
leader frequently refers to the vision and creates a unity of purpose for followers (Kouzes
& Posner, 2012).
Challenge the process. In challenging the process, Kouzes and Posner (1988;
2012) believed that common experiences with change and the effects of change help both
leaders and followers in finding common ground. All individuals face change of one
sort or another, and exemplary leaders capitalize on this commonality of overcoming
uncertainty or fear. Leaders challenging the process seek opportunities for improvement,
seize initiatives, generate small wins to celebrate, and learn from experience (Kouzes &
Posner, 2012).
Enable others to act. Team effort is a consideration of leadership, and leaders
must foster collaboration among group members by building trust and facilitating
relationships (Kouzes & Posner, 2012). Enabling others also infers that development of
individuals is an important aspect to strengthening self-determination and competence.
Individuals that feel trusted and are empowered to make decisions will focus energies
toward the organization (Kouzes & Posner, 2012).
Encourage the heart. Encouraging the heart requires leaders to focus on
recognition, support, and appreciation for individuals (Kouzes & Posner, 2012).
Recognition is used to keep individuals motivated and to overcome the challenges of hard
work. Individuals that feel appreciated will direct additional energy to the organization.
Leaders must also create a sense of community by celebrating the values and successes of
the organization (Kouzes & Posner, 2012).
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 27
Other Theories
Bennis (1997) articulately described the differences between a manager and
leader, noting that managing is more about conducting and controlling whereas leading is
about influencing and guiding. Adaptations of transformational leadership theories have
occurred over time as transformational leadership studies have accumulated. For
instance, in the mid-80s, Bennis and Nanus (1985) identified four common strategies of
transformational leaders: presenting a clear vision, acting as social architects, creating
trust, and using creative deployment of leader strengths. Additionally, Podsakoff,
MacKenzie, Moorman, and Fetter (1990) conceptualized transformational leadership
based on six behavior-oriented dimensions: articulating a vision, providing an appropriate
model, fostering the acceptance of group goals, setting high performance expectations,
providing individualized support, and offering intellectual stimulation. Yukl (as cited in
Bass & Bass, 2008) also organized a taxonomy of leadership and management practices
based on extensive literature review, resulting in the origination of a managerial practices
survey instrument, which he later reported validation findings with colleagues. Despite
these adaptations, by far, the vast majority of empirical research exists with the FRLT
utilizing the MLQ (Avolio, 2011; Yukl, 2006). However Kouzes and Posner (2012) have
accumulated an extensive database of LPI survey responses spanning organizational
sectors.
Criticisms of Transformational Leadership
Primary criticisms of the FRLT revolve around clarity and overlap of constructs
(Northouse, 2007; Yukl, 2006), of which Bass and Avolio have considered and addressed
with further refinement of the MLQ (Antonakis et al., 2003; Avolio, Bass & Jung, 1999).
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 28
Bass and Riggio (2006) argued that both subjective and objective studies have
statistically supported the significance of transformational leadership on effects such as
job satisfaction, organizational commitment, and organizational performance. The
extensive collection of empirical research on the FRLT, using the MLQ (Avolio, 2011),
has supported the rigor needed to further investigate the ambiguities of leadership as a
concept (Gerring, 2012).
Kouzes and Posner (2012) posited that leader actions contribute to such factors as
commitment, engagement, loyalty, and productivity more than any other single variable.
Critics have claimed that the LPI has limited generalization to research due to its primary
use for educational purposes in leadership development (Tourangeau & McGilton, 2004).
Furthermore, Tourangeau and McGilton (2004) asserted the need for a shortened LPI to
relieve respondent burden and research costs, particularly for study in the health care
sector. They proposed a 21-item version of the LPI, which requires further testing for
validation (Tourangeau & McGilton, 2004). Additionally, there is limited research
illustrating a quantitative relationship between transformational leadership using the LPI
and organizational outcomes, such as organizational commitment. As previously noted,
Kouzes and Posner expressed support for additional research using the LPI.
Further criticism exists with respect to transformational leadership itself. Some
critics have asserted that the growth in transformational leadership studies and books
have advanced a blind view of the potential negative consequences of transformational
leadership (Tourish, 2013; Yukl, 1999). For instance, Tourish (2013) claimed that a
multitude of negative qualities exist with transformational leadership behaviors, including
but not limited to the creation of a monoculture, where organizational members conform
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 29
to similar norms, values, and beliefs to the detriment of dissenting feedback that may be
warranted to highlight problematic behaviors (Alatrista & Arrowsmith, 2004). Tourish
(2014) reinforced Yukl’s (1999) previous writings that transformational leadership
creates a false premise of heroic behavior by single leaders rather than advancing Burns’
(1978) initial perspective that transformational leadership should lead to shared
leadership. Such criticism should be carefully considered in order to continue to advance
research in the area of leadership theory. While transformational leadership theory has
dominated the literature in recent decades, it should not be viewed as diminishing the
opportunities that exist to further develop an understanding of leaders and organizational
behavior.
Organizational Commitment
Organizational commitment is a job attitude defined as the degree to which an
employee identifies with an organization and its goals and desires to remain with the
organization (Robbins & Judge, 2012). Liou (2008) argued that organizational
commitment must be given more priority in health care organizations, particularly as it
relates to addressing workforce shortages in the United States. In prioritizing an
emphasis on organizational commitment, health care leaders can focus their efforts on
antecedents that foster increased organizational commitment and, as a result, increase
retention and performance. As a construct, commitment addresses empowerment and its
effect on behavior; empowerment reflects the psychological and social attachments to
people, places or things, such as career professions or organizations (Liou, 2008; Meyer
& Allen, 1997), which in turn can be influenced by leadership behaviors (Avolio, 2011).
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 30
From an organizational perspective, having committed employees can be viewed
as a competitive advantage, particularly as it relates to outcomes such as productivity and
profitability. Committed employees may be described as those that work above and
beyond the call of duty, graciously accept overtime at the sacrifice of personal needs,
stick with the organization through the good and bad, look out for the interests of the
organization, publicly share the organization’s mission, and embrace changes to adapt to
the external environment. Employers may view a committed workforce as a measure of
leadership success in retaining employees, communicating vision and mission, and
implementing a successful strategic plan. However, there are potential repercussions for
committed employees, manifested by an imbalance of work and personal time or lack of
motivation or incentive to further develop professional skills that are marketable to other
organizations (Meyer & Allen, 1997).
In some organizations, turnover is used as a measurable outcome of
organizational commitment. While Meyer and Allen (1997) cautioned against this as a
sole focus, turnover is one of many key quality indicators within the long term care
industry, specifically within nursing facilities where regulators seek to understand the
influence of turnover on the quality of care for residents. Turnover is costly to long term
care employers (Smith & Baughman, 2007), most recently estimated at over $3300 in
direct cost for each turnover (Stone, 2004). In a study of Pennsylvania long term care
providers, the estimated cost of training due to turnover was over $35 million (Stone,
2004). In Iowa, direct cost of turnover in the direct care workforce was estimated at $189
million in 2011, an individual cost of $3839, representing the time and expenses in
addressing separation issues and replacing workers (Iowa Direct Care Worker Advisory
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 31
Council, 2012). A recent study by Mukamel and colleagues (2009) revealed a net
savings of $167,063 for every 10% increase in turnover for California nursing facilities,
as calculated using reported revenues and expenses on submitted cost reports; they
suggested this savings offered an explanation for persistent turnover in the industry.
However, not included in reported numbers for these studies are the indirect costs
associated with turnover, such as lost productivity, reduced service quality, lost patient
revenue, and declines in organizational reputation (Seavey, 2004), all of which contribute
to a complete understanding of turnover in long term care.
High quality leadership and management, including the offering of recognition,
feedback, and a culture of value and respect for DCWs has been associated with low
turnover (Eaton, 2001). However, simply focusing on turnover is short-sighted because
organizational commitment is a multidimensional construct with varied consequences
(Meyer & Allen, 1997). Low turnover is generally positively perceived, but if employees
have low levels of organizational commitment, then other factors such as quality,
customer satisfaction, and resident well-being can suffer (Bowers, Esmond, & Jacobson,
2003; Stone, 2004; Teal, 2002) . High turnover can have the same effects. To develop
and sustain a quality workforce, leaders must have a broader understanding of what other
factors affect organizational commitment. It behooves leaders to consider other factors,
not just retention and turnover rates (Meyer & Allen, 1997). A stable workforce is a
necessary condition for quality, but it should not be exercised as a strategy at the expense
of poor performers with low organizational commitment (Meyer & Allen, 1997).
Organizational goals should include a highly committed workforce and low levels of
turnover among its measures of organizational performance.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 32
As a job attitude, Liou (2008) discussed the variance in theoretical definitions of
organizational commitment. Despite its complexity, Morrow and McElroy (1993)
asserted that “organizational commitment is the most maturely developed of the work
commitment family of constructs” (p. 1). The evolution of the concept of organizational
commitment has resulted in commonalities among the many theoretical definitions:
psychological bond to the organization, a belief in the organization, an acceptance of the
organization’s goals and values, sacrifice for the good of the organization, and a
willingness to remain with the organization (Allen & Meyer, 2000; Liou, 2008; Meyer &
Allen, 1997). Early in its research history, organizational commitment was studied as
unidimensional relative to attitudinal commitment, calculative commitment, and
behavioral commitment, where distinctions were derived from observing the different
processes in which employees became attached to organizations and their ensuing
outcomes, such as absenteeism and turnover (Allen & Meyer, 2000; Becker, 1960;
Mowday, Porter, & Steers, 1982). These distinctions were important to the further
development of research about organizational commitment as a construct. Over time, an
empirical understanding of organizational commitment resulted in three broad themes
around commitment: 1) commitment toward an organization involves the affective
domain; 2) employees recognize that there are costs associated with leaving an
organization; and 3) commitment towards an organization reflects a level of obligation
from employees (Allen & Meyer, 2000; Meyer & Allen, 1997). Following their meta-
analysis of the literature, Meyer and Allen (1997) chose to address these three broad
themes within three primary dimensions: affective, continuance, and normative (Liou,
2008; Meyer & Allen, 1997). In clarifying the distinctions previously observed in the
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 33
literature, Meyer and Allen (1997) likened attitudinal commitment (Mowday, et al.,
1982) to affective commitment, compared calculative commitment (Becker, 1960) to
continuance commitment, and paralleled behavioral commitment (Mowday, et al., 1982)
with both continuance and normative commitment. Meyer and Allen’s (1991) work
resulted in the introduction of the multi-dimensional model of organizational
commitment called the Three-Component Model.
Affective commitment represents the emotional component of organizational
commitment, or the degree to which employees are emotionally attached to the
organization and its beliefs and values (Liou, 2008; Meyer & Allen, 1997; Robbins &
Judge, 2012). Continuance commitment considers the employees’ perceptions of value
in staying with the organization, including socioeconomic factors such as wages and
benefits (Liou, 2008; Meyer & Allen, 1997; Robbins & Judge, 2012). Normative
commitment occurs as a result of the employees’ sense of obligation to remain with the
organization; a level of conformity exists between the employees’ beliefs and values and
organizational norms (Liou, 2008; Meyer & Allen, 1997; Robbins & Judge, 2012).
Because of the depth and breadth of organizational commitment as a concept, it is
important to empirically study it along these commitment dimensions in order to further
evaluate its influence in the workplace. Accordingly, Meyer and Allen (1997) have
cautioned that organizational commitment should not be analyzed without considering
these dimensions independently because of the existential variation in employees’
relationships with their organizations. Employees will experience the affective,
continuance, and normative commitment dimensions in varying degrees, with each
contributing to overall organizational commitment; thus, each can be hypothesized
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 34
independently of each other when considered in relationship to antecedents and
intervening processes (Allen & Meyer, 2000; Meyer, Stanley, Herscovitch, &
Topolnytsky, 2002).
Affective Commitment
Affective commitment represents the emotional component of organizational
commitment, or the degree to which employees are emotionally attached to the
organization and its beliefs and values (Liou, 2008; Meyer & Allen, 1997; Robbins &
Judge, 2012). Affective commitment is analogous to the Mowday et al. (1982)
description of attitudinal commitment where the focus is on employee mindsets in which
values and beliefs are determined to be congruent with organizations. In this sense, the
commonality is found within the affective domain characteristic. Employees with strong
affective commitment stay with organizations because they “want” to (Meyer & Allen,
1991, p. 67). Of all of the dimensions, affective commitment has been studied the most,
primarily due to the benefits of building positive employee emotions toward
organizations (Allen & Meyer, 2000; Meyer & Allen, 1997). In meta-analyses research,
it has consistently shown to have positive correlations with desirable work behaviors,
such as attendance and organizational citizenship behavior (Allen & Meyer, 2000;
Mathieu & Zajac, 1990; Meyer et al., 2002).
Continuance Commitment
Continuance commitment considers employees’ perceptions of value in staying
with organizations, including socioeconomic factors such as wages and benefits (Liou,
2008; Meyer & Allen, 1997; Robbins & Judge, 2012). Early in the research, continuance
commitment was addressed along Becker’s (1960) side bets theory, which referred to the
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 35
idea that employees link extraneous interests, such as seniority, to calculative decisions
about staying or leaving organizations. But in its limited context, the application of the
side bets theory restricted the continuance commitment construct, and over time,
continuance commitment evolved analogous to the Mowday et al.’s (1982) description of
behavioral commitment, where focus is on the processes organizations use to retain
employees, such as competitive wages and benefits (Meyer & Allen, 1991). Employees
with strong continuance commitment stay with organizations because they “have” to
(Meyer & Allen, 1991, p. 67). Thus, continuance commitment can be thought of in an
economic sense. Continuance commitment for employees will vary depending on the
range of alternatives available (Meyer & Allen, 1997). Likewise, individual employee
situations will dictate whether continuance commitment is weak or strong. For example,
an employee may want to leave to find a position with better pay, but if a spouse has lost
a job, the employee is less likely to leave for a different position. In meta-analyses
research, continuance commitment has been shown to have primarily negative
correlations with desirable work behaviors, such as attendance and organizational
citizenship behavior (Allen & Meyer, 2000; Mathieu & Zajac, 1990; Meyer et al., 2002).
Normative Commitment
Normative commitment occurs as a result of employees’ sense of obligation to
remain with organizations; a level of conformity exists between an employees’ beliefs
and values and organizational norms (Liou, 2008; Meyer & Allen, 1997; Robbins &
Judge, 2012). Normative commitment is also analogous to the Mowday et al. (1982)
description of behavioral commitment where focus is on processes organizations use to
retain employees; however, organizational culture and practices that connect to employee
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 36
values and beliefs formulate a basis for normative commitment, rather than pay and
benefits. Employees with strong normative commitment stay with organizations because
they feel they “ought” to (Meyer & Allen, 1991, p. 67). Normative commitment is
believed to develop early in life based on parental role modeling and over time with
advancement of loyalty and social identity to organizations (Allen & Meyer, 2000; Meyer
& Allen, 1997), although Meyer and Allen’s survey instruments have been revised to
address the perceived decreased effect that early life plays in normative commitment
(Meyer et al., 2002). Loyalty and social identity, or internalization behaviors, have
become more prominent in focus (Meyer, et al., 2002). Loyalty involves a level of
faithfulness to organizations. Social identity suggests that employees seek to find their
sense of self through group membership and will pursue meaning within and among in-
groups and out-groups within organizations (Haslam, Reicher, & Platow, 2011). The
degree to which organizations can develop and implement practices that enhance loyalty
and social identity will inform the level of normative commitment. In meta-analyses
research, normative commitment has consistently shown to have positive correlations
with desirable work behaviors, such as organizational citizenship behavior and
performance (Allen & Meyer, 2000; Mathieu & Zajac, 1990; Meyer et al., 2002).
Empirical Evidence
Liou (2008) asserted that organizational commitment is directly related to
employee retention, based on broad business industry research on the subject. However,
there is little known about this relationship for DCWs. Turnover and retention are widely
studied for DCWs in nursing facilities. However, their study is largely targeted toward
understanding the relationship to quality of care and job satisfaction (Stone, 2011).
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 37
Specifically distinguishing between job satisfaction and organizational commitment is a
salient point because they do present differences. While both represent affective
responses, job satisfaction addresses responses to specific elements of the job itself, such
as level of responsibility, whereas organizational commitment addresses the affective
response to the whole organization (Williams & Hazer, 1986; Emery & Barker, 2007).
Furthermore, organizational commitment is not intended to be analogous to job or
occupational commitment, which refers to employees’ attachments to particular jobs or
occupations (Williams & Hazer, 1986; Meyer & Allen, 1997). For example, a DCW may
not be committed to an organization, but will remain committed to working in DCW
positions.
A multitude of variables have been studied relative to understanding the
antecedents, correlates, and consequences of affective, continuance, and normative
commitment. Three categories (organizational characteristics, personal characteristics,
and work experiences) encompass the variables considered in the broad range of research
on organizational commitment (Meyer & Allen, 1997). Organizational characteristics
consider such factors as structure (levels of hierarchy and decision-making), policies and
fairness (including pay), communication, and leadership behaviors. Personal
characteristics include factors such as gender, age, length of employment, and
personalities. And work experiences include factors such as job roles, job scope,
autonomy, empowerment, and supportive behaviors. Generally, researchers have
contended that affective commitment is mostly developed based on work experiences,
supportive leadership practices, and fairness; continuance commitment develops based on
economic conditions; and normative commitment develops based on early life role
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 38
modeling and over time through organizational work experiences (Allen & Meyer, 2000;
Meyer & Allen, 1997; Meyer et al., 2002). The variation in antecedent, correlate, and
consequential variables represent the complexity with which organizational commitment
can be studied.
Multiple variables have been studied as either antecedents or correlates of
organizational commitment relative to various outcomes, such as quality of care, job
satisfaction, and performance (Liou, 2008; Meyer et al., 2002). As affective and
normative commitments increase, turnover rates drop and organizational citizenship
behavior improves (Liou, 2008; Meyer et al., 2002). Furthermore, leader behaviors
exhibited in how DCWs were treated accounted for turnover more than low wages,
(Rosen, Stiehl, Mittal, & Leana, 2011; Secrest, Iorio & Martz, 2005) (emphasis added).
Leaders demonstrating behaviors that promote supportive work environments are more
effective in developing higher commitment levels, particularly with the affective and
normative dimensions, evidenced by positive correlations with transformational
leadership (Meyer et al., 2002).
Connections between demographic characteristics and organizational commitment
have been inconsistent (Emery & Barker, 2007; Meyer & Allen, 1997; Williams &
Hazer, 1996). Recent studies analyzing demographic characteristics and organizational
commitment have revealed significant correlations within a global context (Al-Hussami,
Darawad, Saleh, & Hayajneh, 2014; Qiao, Khilji, & Wang, 2009), supporting the small
scale evaluation of demographic variables done by Meyer et al. (2002) on studies
conducted outside of North America. These results suggest that cultural differences may
exist within this relationship. However, Mathieu and Zajac (1990) demonstrated that
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 39
demographic variables, such as age, should be viewed as inferior to other variables in
developing organizational commitment.
Work stressors such as role ambiguity and role conflict have consistently shown
to have negative correlations to normative commitment whereas autonomy,
empowerment, and fairness have revealed positive correlations with affective
commitment (Lambert, Kelley, & Hogan, 2013) and overall organizational commitment
(Al-Hussami, 2008; Meyer & Allen, 1997). While the aim of some of the research has
been to establish causal mechanisms, research methods around organizational
commitment have primarily involved cross-sectional and correlational designs, thus
limiting the ability to establish causality (Gerring, 2012; Meyer & Allen, 1997).
Summarily, according to Liou (2008), there are five stages of organizational
commitment (exploration, testing, passion, quiet boredom, and integration) that occur
within the workplace. These stages reflect the dynamic nature of organizational
commitment along temporal aspects, demonstrating a slow and consistent development
process (Liou, 2008), and represent the importance of leadership behaviors over time and
for all employees, regardless of length of employment or rank in the organization (Allen
& Meyer, 2000). This temporal aspect of organizational commitment illuminates the
need for its ongoing consideration within organizations, because levels of commitment
will vary within and among individual employees, units, and as a whole (Heldenbrand &
Simms, 2012).
Transformational Leadership and Organizational Commitment
Transformational leadership has been shown to influence individual, team, and
organizational performance due to the effect that transformational leadership has on
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 40
levels of commitment and trust of followers (Avolio, 2011; Avolio & Bass, 1995; Bycio,
Hackett, & Allen, 1995; DeChurch, Hiller, Murase, Doty, & Salas, 2010; Meyer et al.,
2002). The breadth and depth of empirical research has revealed that leaders cannot
directly control follower commitment; however, leaders can influence commitment
through effectively communicating the vision, sharing and modeling beliefs and values,
supporting followers, and managing leader self-awareness (Bass & Bass, 2008; Emery &
Barker, 2007; Goleman, 2013). These positive leadership practices increase the affective
connection between leaders and followers and result in an increased identification with
the vision, mission, and values of organizations, thus influencing commitment and
consequently, performance (Avolio, 2011). Furthermore, research has shown that
transformational leadership can be learned (Avolio, 2011; Duygulu & Kublay, 2011;
Kouzes & Posner, 2012). While the literature is minimal in addressing transformational
leadership in long term care, there are a variety of studies addressing transformational
leadership in a broader context.
In long term care, empowerment is a key determinant of workforce issues.
Empowerment prescribes the involvement of employees in organizational decision-
making processes and more specifically, in the patient dyadic relationship where patient-
centered customer orientation is of primary importance. Leaders that insist on
micromanaging DCWs risk decreased employee engagement and subpar continuous
improvement efforts, negatively affecting employee commitment over time, whereas
implementation of employee participation in decision-making has been shown to
positively influence employee behaviors at work (Heldenbrand & Simms, 2012). Among
nurses in Singapore, empowerment was found to be a mediating factor for
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 41
transformational leadership and organizational commitment (Avolio, Zhu, Koh, & Puja,
2004). Transformational leadership behaviors have been shown to cascade downward to
other managerial, leader positions, benefitting organizational performance as a whole
(Bass, Waldman, & Avolio, 1987; Eaton, 2001; Godwin & Neck, 1998). The leader
behaviors of immediate supervisors, as perceived by employees, have been shown to
influence employee attitudes (Culp, Ramey, & Karlman, 2008; Emery & Barker, 2007).
Thus, when residents report having negative views of care, they also report having
negative experiences with DCWs or report stories reminiscent of employees complaining
while providing care (Eaton, 2001).
Research outcomes emphasize the effects of transformational leadership in
motivating and influencing employees toward a collective goal (Bass & Riggio, 2010).
Substantial evidence exists to illustrate a predictive relationship of organizational
commitment (Bono & Judge, 2003; Meyer & Allen, 1997). Within the three dimensions
of organizational commitment, significant relationships have been shown to exist
between transformational leadership and affective and normative commitment, with
limited or no relationship with continuance commitment (Dunn, Dastoor, & Simms,
2012; Liou, 2008; Meyer & Allen, 1997; Meyer et al., 2002). McMurray et al. (2010)
found that transformational leadership is a limited predictor of overall commitment and
noted that articulating vision and fostering goal acceptance were observed to specifically
have a significant relationship. However, in a recent study of nonprofit employees,
transformational leadership was found to be positively correlated with normative
commitment and negatively correlated with both affective and continuance commitment,
contradicting earlier studies (Freeborough, 2013).
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 42
In long term care, high commitment levels have been demonstrated to enhance
dyadic patient-caregiver relationships and quality of life, as primarily influenced by
effective supervision and illustrated by supervisory support, autonomy, and respect
(Bishop et al., 2008; McGillis-Hall et al., 2005). Additional research has provided
support for decentralized structures combined with communication in reducing DCW
intent to leave (Kim, et al., 2013). Bureaucratic, or hierarchical cultures have been
shown to be negatively correlated to organizational commitment (Pennington, Townsend,
& Cummins, 2003). Furthermore, organizational structures that support openness for
suggestions, innovative mindsets, and a willingness to try new things may be more
conducive to transformational leadership styles (Emery & Barker, 2007). Podsakoff,
MacKenzie, and Bommer (1996) studied the effects of situational variables as potential
substitute behaviors for leaders; routine tasks, indifference to organizational rewards, and
rewards out of leaders’ control all resulted in decreased organizational commitment,
suggesting that participatory and inclusive cultures may advance a more committed
workforce.
Further study of nursing home administrators and directors of nursing found that
transformational leadership qualities have no statistically significant relationship on
quality of resident care (Marotta, 2010). This suggests that transactional leadership
qualities are necessary in highly regulated environments, such as nursing facilities.
Nursing facility providers have long touted the extreme level of regulations in the
industry, of which is supported by the literature (Forbes-Thompson & Gessert, 2006).
Because the long term care industry is highly regulated, transactional leadership
behaviors may be necessary to assure compliance. However, disputes exist about
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 43
whether regulations are adequate within such long term care settings as assisted living.
Crawford (2005) found that nursing home administrators rate high in both
transformational and transactional leadership behaviors, reinforcing the assertion by
Avolio, Bass and Jung (1999) that transformational leadership augments transactional
leadership. Administrators with consensus-based leadership styles, evidenced by
transformational leadership qualities (Bass, 1985), have been shown to influence turnover
at its lowest levels (Donoghue and Castle, 2009). Long term care leaders must balance
the need for transactional leadership qualities that benefit quality of care and regulatory
compliance and transformational leadership qualities that enhance innovation, change
orientation, and consumer/employee focus (Berndt, 2012; Dana & Olson, 2007).
Furthermore, the evolution of person-centered care into the long term care
industry has demanded more of providers in the implementation of practices that
operationalize person-centered care concepts. Successfully implemented, person-
centered care models have been shown to positively influence the work environment by
inviting DCWs to actively participate in decision-making, encourage teamwork and
expand their job tasks beyond the traditional job role (Leutz, Bishop & Dodson, 2009;
Stone, 2011). Implementation of person-centered care practices dictates the necessity for
transformational leadership practices because it directly affects job redesign and elements
of the job characteristics model, such as autonomy (Leutz, Bishop & Dodson, 2009;
Robbins & Judge, 2012). Transformational leaders can influence how employees
perceive their work, and when employees perceive it to be important and meaningful,
they are more committed (Bono & Judge, 2003). Person-centered care has also been
shown to influence low turnover (Stone, 2011). As a result, transformational leadership
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 44
is a consideration in the supervisor-DCW relationship within the person-centered care
approach. Understanding the relationship between transformational leadership and
organizational commitment will lend value to the long term care industry in formulating
public policy, modifying operational practices, identifying training and development
needs, and revisiting human resource practices.
The Nonprofit Perspective
Supportive nursing practice environments in nonprofit long term care settings
have been shown to positively influence nursing home patient outcomes, evidenced by
higher quality ratings (Lutfiyya, Gessert, & Lipsky, 2013). Since the 1970s, high
turnover has been associated with for-profit long term care organizations (Stone, 2004,
2011; Stryker-Gordon, 1979); however, no significant relationship was shown to exist in
the Donoghue & Castle (2009) study. Research is also mixed about whether nonprofits
are more efficient, have less code violations, experience higher customer satisfaction, or
offer lower wages than their counterparts (DiMaggio & Anheier, 2001). However, the
importance of the nonprofit sector cannot go unrecognized. Based on an analysis of data
from the Bureau of Labor Statistics (BLS), when compared with for-profit entities,
nonprofit organizations historically pay higher wages, are more resilient when faced with
change, employ more individuals (particularly in service sectors), are driven by moral
constructs and values, and are major job creators (Salamon, Sokolowski, & Geller, 2012).
Studying leadership in nonprofit long term care organizations will enhance the literature
focused on the nonprofit sector.
Many long term care organizations have their origins in voluntary associations or
religious or community-based affiliations (Pratt, 2010). Over time, they became
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 45
corporatized and adopted business principles to sustain operations; they can, and do,
make money. In many cases, nonprofit long term care organizations look nothing
different than their for-profit counterparts, other than their legal tax exempt status by the
Internal Revenue Service (Ott, 2001). Nonprofits do not have accountability to
shareholders; however, they do have accountability to their governing boards, and in
many cases, to the public because revenues most often come from taxpayers via
government programs. For instance, nonprofit long term care organizations have deep
roots in utilizing government programs like Medicaid and Medicare as revenue sources
and are subject to regulatory scrutiny in the use of such government funds (Pratt, 2010).
Beyond the tax legality that nonprofits observe, their missions are primarily
formed to encourage benevolence and minimize social injustices (Block, 2001; Felkins &
Croteau-Chonka, 2014; Ott, 2001). Nonprofit missions vary, but often similarities exist
in advancing quality of life and seeking the common good. Felkins and Croteau-Chonka
(2014) have characterized the commitment to the common good as the “Nonprofit Factor,
motivating people to donate time and resources to help others and to work together for
positive change at local and global levels” (p. 3). Nonprofit long term care organizations
pursue the common good by providing services to older adults and others with chronic
long term health care needs that otherwise have no other sufficient help to obtain
services. On this premise, they are able to appeal to the emotions of the public in their
cause. Nonprofit missions are also used to solicit the help of employees with similar
helping values. The idea of shared commitments for social good and the challenges that
encompass such goals are reasons that attract leaders to nonprofit organizations (Bear &
Fitzgibbon, 2005).
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 46
Leadership in Nonprofit Organizations
Nonprofit leadership has espoused the characteristics of transformational
leadership in order to effectively address the challenges of multiple stakeholders,
operational issues, and sufficient resources (Bear & Fitzgibbon, 2005). And yet, research
on transformational leadership in the nonprofit sector is lacking (Riggio & Orr, 2004).
Nonprofit leaders need to articulate a compelling vision and inspire followers
participation to move the vision forward (Bear & Fitzgibbon, 2005), focusing on shared
values and mutual benefits (Felkins & Croteau-Chonka, 2014). In nonprofit
organizations, the combination of these aspects has been described as a “social contract,”
or a commitment acknowledging that mutual obligations and responsibilities are
necessary to form and develop sustaining relationships among stakeholders and cooperate
accordingly to achieve the vision and mission (Felkins & Croteau-Chonka, 2014, p. 12;
Smith, 2001), representing a shared leadership model. While social contracts are not
necessarily formal in nature, they form the basis of a philosophy for cultural norms
within a nonprofit organization (Felkins & Croteau-Chonka, 2014). For instance, a
cultural norm within many nonprofit organizations is that profits are needed to survive
and expenses should be kept sufficiently low to meet objectives; a consequence often
involves low wages for employees (Pallotta, 2008). Palotta (2008) asserted the
elimination of this idea and reinforced that nonprofits should pay competitive wages
similar to their counterparts and rally around the benefits they provide to the public, thus
improving overall turnover among nonprofit leaders and their corresponding followers
who hold worthy values and beliefs but leave the sector due to the inability to balance the
stresses that come with nonprofit work and inadequate pay. Nonprofit leaders also often
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 47
lack leadership training. In a 2003 survey of nonprofit leaders, staff, and volunteers,
emotional leadership was isolated as a specific leadership training need, in addition to
fundraising and project management (Bear & Fitzgibbon, 2005). In addition to needing
business skills similar to those required in the private sector, Bear and Fitzgibbon (2005)
mimic Kouzes and Posner ‘s (2012) LCT by stating that nonprofit leaders also need
compassionate behaviors, those that guide the organization, empower others, and
encourage with the heart.
Andrew Carnegie and John D. Rockefeller were instrumental agents of change in
donating their large fortunes to a plethora of nonprofit organizations (Scott, 2001).
Carnegie was quoted as saying “no man will make a great leader who wants to do it all
himself, or to get all the credit for doing it” (Bear & Fitzgibbon, 2005, p. 101), and he
clearly understood the need for shared responsibility, as Burns (1978) encouraged in his
seminal writings on transforming leadership for social change. Among the many
challenges that exist in nonprofit organizations, leaders must be actively involved in
pursuing a healthy culture and workforce and can benefit from learning about best
practices from other sectors and applying them to nonprofit principles. Some interesting
studies exist that provide unique insight into the nonprofit sector. Galaskiewicz and
Bielefeld (2001) studied nonprofits from a variety of organizational theory perspectives
to better understand how organizational change has affected the nonprofit sector. Using
randomized sampling, data were collected from Midwest charitable organizations
between 1980 and 1992. Regarding the growth and/or decline of performance, data
revealed that niche, nonprofit organizations were more likely to increase income,
donations, employees and volunteers. Likewise, nonprofits that employed more
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 48
managerial and political tactics during change were more likely to increase income and
employees over time, whereas those that chose retrenchment strategies experienced the
opposite effects. Furthermore, nonprofit organizations that are more dependent on
commercial income with high resource dependence (employees) are more likely to
increase managerial and political tactics over time while also considering centralized
decision-making. This is important to the study of long term care organizations because
these types of organizations are highly resource dependent, both on staff and financial
reimbursements from government and other insurance programs. Long term care
organizations are also considered niche services because they isolate services to those
with chronic and long term care needs.
Similarities to Transformational Leadership Theories
Little empirical study has been conducted in the nonprofit sector relative to
transformational leadership and/or organizational commitment. However, nonprofit
leadership holds many similarities to transformational leadership theories and
organizational commitment frameworks. First, the vision and mission are front and
center for nonprofit organizations (Felkins & Croteau-Chonka, 2014). Nonprofit
founders are integral to the formulation and articulation of a vision and mission (Ott,
2001), but the commitment to the vision and mission must be sustained by others in the
organization (Felkins & Croteau-Chonka, 2014). Leaders must share the vision and
mission and inspire others to achieve it (Avolio, 2011; Bass, 1985; Kouzes & Posner,
2013). Furthermore, to the extent that these visions and missions seek to solve societal
injustices, they are analogous to the kinds of transforming social change Burns (1978)
stressed were the impetus for leader-follower exchange in developing a moral compass
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 49
and influencing change. Second, relationships are a key component to effective
leadership and built upon shared values (Felkins & Croteau-Chonka, 2014).
Transformational leadership theories promote shared values, transparency of information
for mutual goals, empowerment, and participatory decision-making. Transformational
leaders seek to understand what is meaningful to followers and then influence and guide
them to achieve the vision and mission (Avolio, 2011; Bass, 1985; Kouzes & Posner,
2013). Godwin and Neck (1998) found that those leaders within religious organizations
at closest proximity to followers ranked highest in importance for transformational
leadership, suggesting that followers are able to more visibly observe transformational
leader behaviors when they occur at lower levels in the organization. However, they also
found that vision and goal-setting are recognized by followers as more important at
higher leadership levels (Godwin & Neck, 1998). Successful application of positive
leadership practices are intended to positively influence organizations in such ways as
productivity, efficiency, profits, retention and turnover, and employee commitment.
Third, nonprofits use emotional elements to brand their missions (Felkins &
Croteau-Chonka, 2014). Transformational leadership behaviors utilize charismatic
qualities such as inspirational storytelling to share an organization’s purpose both
internally and externally. Such storytelling and other emotional methods are meant to
broaden a nonprofit’s reach within people’s affective domain, creating an emotional bond
with the organization. Emotional attachment garners additional support for the
organization from donors, volunteers, and the public (Felkins & Croteau-Chonka, 2014),
and has the potential to increase organizational commitment by employees (McMurray, et
al., 2010; Meyer & Allen, 1997). Finally, nonprofit leadership seeks to advance the
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 50
many advocacy efforts of nonprofits in addressing the social injustices and inequities that
exist in society (Felkins & Croteau-Chonka, 2014; Frumkin, 2002). Transformational
leadership theories promote behaviors that challenge the process (Kouzes & Posner,
2013) and encourage entrepreneurship and innovation (Avolio, 2011). There are
different perspectives regarding change management processes, but common to them all
is the importance of influence, power, and relationships (Burke, 2011), all of which are
addressed within the context of transformational leadership.
Summary
Transformational leadership theories have advanced the notion that certain
behavioral characteristics (such as visioning, caring, and empowering) will transcend
organizational activities and employees toward higher goals, efficiencies, and
productivity. For decades, theorists have studied leadership in an attempt to identify,
understand, and develop optimal leader behavioral characteristics. Two transformational
leadership theories, the Full Range Leadership Theory (Avolio, 2011) and the Leadership
Challenge Theory (Kouzes & Posner, 2013) remain popular for researchers and
practitioners. Despite the positive advancement of these and other leadership theories,
criticism does remain, which stimulates further study. Additionally, organizational
commitment has been advanced over time as a multi-dimensional construct for
understanding the reasons employees stay or leave organizations. Three specific
dimensions, affective, continuance, and normative commitment, have become prominent
in the research literature. Transformational leadership has been studied in a limited
fashion as an antecedent to organizational commitment, and results have generally
provided consistent results, although recent studies in the nonprofit sector have been
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 51
contradictory (Freeborough, 2013). The need for additional research on transformational
leadership and organizational commitment within the nonprofit sector is warranted to
better understand the dynamics of nonprofit leadership as it pertains to organizational
practices and behavior. This study aims to address this gap within the context of the
nonprofit long term care industry, with a focus on DCWs and their perceptions of leader
behaviors of their immediate supervisors. The research methodology for this study will
be examined in Chapter three.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 52
CHAPTER THREE: METHODOLOGY
Introduction
Chapter three discusses the research design, research questions and hypotheses,
methodology rationale, the sample, survey instrumentation and its reliability and validity,
variables, data collection and analysis, and ethical considerations of this study. The
purpose of this quantitative study was to determine what relationship exists between
transformational leadership and organizational commitment for DCWs in nonprofit long
term care organizations. The research study was stimulated by practical considerations.
DCWs form the core of the long term care industry, providing services essential to the
quality of life and quality of care of consumers. Demographic trends do not bode well
for the future availability of direct care workers. The United States has a rapidly aging
society, with the population of older adults growing dramatically over the next 50 years;
the baby boom generation will reach 65 between 2011 and 2029, those 85 and older will
grow at the fastest rate, and by 2050, one in five Americans will be over the age of 65
(Center for Health Workforce Studies, 2006; Dall et al., 2013). These consumers will
demand choice and options for long term care services, which require a sufficient supply
of DCWs. Leaders must utilize practices that develop and sustain the workforce at both
policy and practice levels. Understanding the relationship of leadership and
organizational commitment will help provide a better understanding of factors affecting
the commitment process and allow industry practitioners and researchers to consider
carefully the effect of leadership behavior and practices on direct care workers. The
study sought to fill a gap in the literature representing the relationship of transformational
leadership and organizational commitment within the long term care industry, as well as
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 53
to add to the body of knowledge about leadership in nonprofit organizations. Findings of
the study may benefit scholarship, practice, and policy within the long term care industry.
Research Questions and Hypotheses
The correlation between transformational leadership and organizational
commitment among DCWs in nonprofit long term care organizations has not been
empirically tested. Demographics, job characteristics and work experiences have been
identified as influences, or antecedents, on organizational commitment, including but not
limited to job challenges, work relationships, feedback quality, group attitudes,
empowerment, role stress, job satisfaction and trust (Liou, 2008; Meyer et al., 2002). In
an extensive review of the literature, no study was found that evaluated transformational
leadership as an antecedent to organizational commitment in the context of long term
care and DCWs. The traditional hierarchy in long-term care has assured that the locus of
control remains with those furthest from patient care (Caspar & O’Rourke, 2008), such
that DCWs provide over 80% of all patient care, have the least amount of education,
receive the lowest pay and exercise the least amount of decision-making authority and
autonomy (Caspar & O’Rourke, 2008; Stone, 2011). DCWs have stated that what they
desire most is respect, recognition and rewards, as well as inclusion in decision-making
and empowerment (Casper & O’Rourke, 2008; Leutz, Bishop & Dodson, 2009; Secrest,
Iorio & Martz, 2005; Stone, 2011), all components of transformational leadership
behaviors.
A primary research question guided this quantitative study:
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 54
RQ1: What is the relationship between transformational leadership and organizational
commitment (affective, continuance, and normative) among direct care workers in
nonprofit long term care organizations?
Three specific hypotheses were investigated in this study:
H1: There is a significant positive relationship between transformational
leadership and DCW affective commitment.
H2: There is a significant inverse relationship between transformational
leadership and DCW continuance commitment.
H3: There is a significant positive relationship between transformational
leadership and DCW normative commitment.
A secondary research question inquired about potential differences in the types of long
term settings, such as nursing facilities, assisted living, and senior housing. This question
was important in understanding how differences in long term settings might influence the
variables of interest and where interventions might be most valued by the industry (Kim,
Wehbi, DelliFraine, & Brannon, 2013), particularly where DCWs are employed by
organizations providing multiple types of long term care settings on their campuses.
RQ2: Is there a difference, if any, between types of long term care settings for
transformational leadership and organizational commitment?
H4: There is no difference between types of long term care settings for
transformational leadership and organizational commitment.
Method
This study used a quantitative, correlational research design and nonprobability
sampling. For the study, transformational leadership was the predictor variable, and
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 55
organizational commitment was the criterion, or outcome, variable. The study design
utilized nonprobability sampling to obtain study participants, representing a purposeful
sampling approach (Creswell, 2012). This study was correlational in nature because the
research question was evaluating the relationship between two variables (Creswell,
2012), whereby manipulation of the predictor variable, transformational leadership was
not the purpose of the research. Specifically, the objective of the correlational study was
to examine the extent to which the variables co-vary (Creswell, 2012). Thus, a
correlational study design was appropriate for this study. However, the design was not
used to establish causality (Gerring, 2011), rather it assisted in predicting the relationship
of transformational leadership and organizational commitment.
Two instruments were used for this study: a) Leadership Practice Inventory (LPI)
Observer which measures transformational leadership (Kouzes & Posner, 2013), and b)
Three-Component Model Commitment Survey (TCM) which measures organizational
commitment (Meyer & Allen, 2004). Correlational, nonparametric statistical analysis
was used to test the hypotheses and consider the strength of the variables based upon the
specific survey subscales within the transformational leadership and organizational
commitment constructs.
Description of Sample
The population of the study consisted of DCWs employed by nonprofit
Midwestern long term care organizations. A purposeful sample approach was used for
the study, which is considered a nonprobability sampling method (Creswell, 2012).
Purposeful sampling was used to identify nonprofit long term care organizations that met
specific criteria. The criteria for selection included: a) long term care organizations that
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 56
were nonprofit; b) long term care organizations that provide multiple service lines, or
types of long term care settings on their campuses, including nursing facilities, assisted
living, and senior housing; and c) long term care organizations willing to participate in
the study. The rationale for selecting the first criterion was directly related to the need to
add to the body of knowledge about nonprofit organizations. The second criterion was
related to the secondary research question addressing differences between types of long
term care settings. The third criterion was related to the difficulty in obtaining
permission from long term care organizations to survey employees. Thus, executives of
nonprofit long term care organizations fitting the criteria were approached for their
willingness to participate. Based on the willingness of several nonprofit, long term care
organizations, approximately 1,100 DCWs were invited to participate in the study.
Survey Instrumentation
Two survey instruments, the LPI Observer (Kouzes & Posner, 2013) and the
TCM (Meyer & Allen, 2004), were utilized in this study. Permission to use each
instrument was obtained from the respective authors. Demographic information such as
gender, age, ethnicity, education, and length of employment was also obtained by
participants during survey completion in order to provide descriptive statistics of the
participants. Survey instrumentation is included in Appendix A.
Leadership Practices Inventory
Transformational leadership was measured using Kouzes’ and Posner’s (2013)
Leadership Practices Inventory (LPI) Observer. The long term care industry, specifically
those organizations of nonprofit status, prefers research applications that support its
capacity to communicate in terminology easily understood by all levels of the
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 57
organization, suggesting the industry will respond more favorably to a study utilizing the
LPI instrument (Kouzes & Posner, 2013). Such perception largely addresses the LPI
based on face validity and may be considered industry bias.
Participants responded to thirty items in the LPI using a 10-point scale with
responses ranging from 1 = almost never to 10 = almost always. A higher value
represents behaviors used more frequently (Kouzes & Posner, 2002).This scale was
treated as a continuous measure (Creswell, 2012). The LPI measured the five practices of
exemplary leaders as described in Kouzes’ and Posner’s (1988, 2012) theoretical
leadership challenge framework of core leadership competencies. The LPI utilizes thirty
descriptive, behavioral statements in which the respondent is asked to assess leader
behaviors. For this study, survey participants assessed leader behaviors based on the
supervisor to whom they directly report, as they perceive the supervisor’s leader
behaviors.
The thirty statements in the LPI are further broken down into five subscales (six
statements each): a) model the way, b) inspire a shared vision, c) challenge the process,
d) enable others to act, and e) encourage the heart (Kouzes & Posner, 2013). Permission
to use the LPI was conditioned upon results being shared with Kouzes and Posner as the
developers. This condition allows them to further advance their understanding of validity
and reliability of the instrument. To address construct validity, numerous researchers
have conducted factor analysis studies on the LPI and results have provided continued
empirical support for the categorization of leader behaviors within these five primary
leader practices across a variety of organizational settings (Kouzes & Posner, 2000;
Kouzes & Posner, 2002). Validity can be addressed at both internal (sample) and
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 58
external (population) levels (Creswell, 2012). For purposes of this study, internal validity
was of primary interest. The use of the LPI Observer instrument was particularly
important because it minimizes self-report bias that is often a concern with the use of the
LPI Self instrument. Participants in the current study were asked to assess their direct
supervisor, not themselves. Because the current study was based on a nonprobability
sampling approach, external validity was difficult to assert with regard to generalizations
of the broader population (Gerring, 2012).
Internal reliability refers to the level of precision and consistency of the survey
relative to measurement errors that can result in differing scores for reasons unrelated to
the participants (Gerring, 2012). For instruments with items scored as continuous
variables, the coefficient alpha is generally used to test for internal consistency (Creswell,
2012). For the LPI, internal reliability has been consistent in revealing reliability
coefficients above the .75 level as measured by Cronbach’s alpha (Kouzes & Posner,
2000). Reliability coefficients for the five subscales met acceptable levels: model the
way (.88), inspire a shared vision (.92), challenge the process (.89), enable others to act
(.88), and encourage the heart (.92) (Kouzes & Posner, 2002). Similarly, test-retest
reliability has been consistently strong (Kouzes & Posner, 2002). Test-retest reliability
procedures are used to examine the extent that the instrument is stable over time, with .6
as an acceptable level (Creswell, 2012).
Three-Component Model of Employee Commitment
Organizational commitment was measured using the academic version of the
Three-Component Model (TCM) of Employee Commitment Survey developed and
modified by Meyer and Allen (2004). The TCM consisted of eighteen statements among
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 59
three subscales (affective, continuance, normative) that represent employees’ mindsets
toward their organization. Study participants were asked to indicate the degree of
agreement with each statement based on their feelings about their respective
organizations. The statements required respondents to rate the degree of agreement on a
7-point Likert-type scale, ranging from 1 = strongly disagree to 7 = strongly agree. This
scale was treated as a continuous measure (Creswell, 2012; Meyer et al., 2002).
Numerous studies have assessed construct validity and have concluded consistency exists
for macro generalization of the model (Jaros, 2007; Meyer et al., 2002), although specific
wording among the normative and continuance commitment subscales still garners
interest by researchers in order to further address micro generalization considerations
such as employment status (Jaros, 2007; Meyer, Becker, & Van Dick, 2006).
Confirmatory factor analysis has provided empirical evidence that the subscales are
highly correlated (Hackett et al., 1994; Meyer et al., 2002) and internal reliability was
within acceptable rates (above .70) (Allen & Meyer, 2000; Meyer & Allen, 1997; Meyer
et al., 2002). The TCM dominates the research literature, and rather than creating new
survey instruments, researchers are adding to the TCM use for further refinement of the
model for micro generalization (Jaros, 2007) and cross-cultural application (Allen &
Meyer, 2000; Meyer et al., 2002).
Demographics
The demographic questions were developed to describe the characteristics of the
study participants as well as information about the organizations in general. Participants
were asked about gender, age, ethnicity, length of employment, service in the military,
wages, yearly income, benefits, relationship status, living arrangements, education,
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 60
government assistance, availability of transportation, type of long term care setting they
work in, and whether they are considering an employment change. These questions were
chosen based on the potential influence they have to the organizational commitment
subscales addressing affective, normative, and continuance commitment. Organizational
demographics were obtained by the administrators on site at the time of data collection.
Organization information included total employees, number of DCWs, year-to-date
turnover, wage ranges, availability of benefits, types of services provided, premium costs
of health insurance, and consideration of increasing wages. Similarly, these questions
were asked to address the potential implication of organization commitment as well as to
provide general descriptive information of the organizations for comparison purposes.
Pilot Study
The survey instruments were field tested with thirteen DCWs in a pilot study
conducted in a Midwestern long term care organization located in close proximity of the
researcher. The long term care organization was selected based on the willingness of the
administrator to participate in the pilot study. The pilot study utilized a focus group
method and was conducted mid-afternoon on a Monday. Data were analyzed using
SPSS® 22. Participants gathered as a group, grabbed snacks, and obtained instructions
for survey completion. After individually completing the survey, the researcher asked the
participants for feedback about the survey and process in general. The focus group lasted
one hour in duration. Of the pilot participants, 92.3% were female, the mean age was
49.58 years, and 84.6 percent classified themselves as white with regard to race. The
mean length of employment with the organization was coded as 2.75 and the mean length
of time working in long term care was coded as 4.53, indicating that many of the pilot
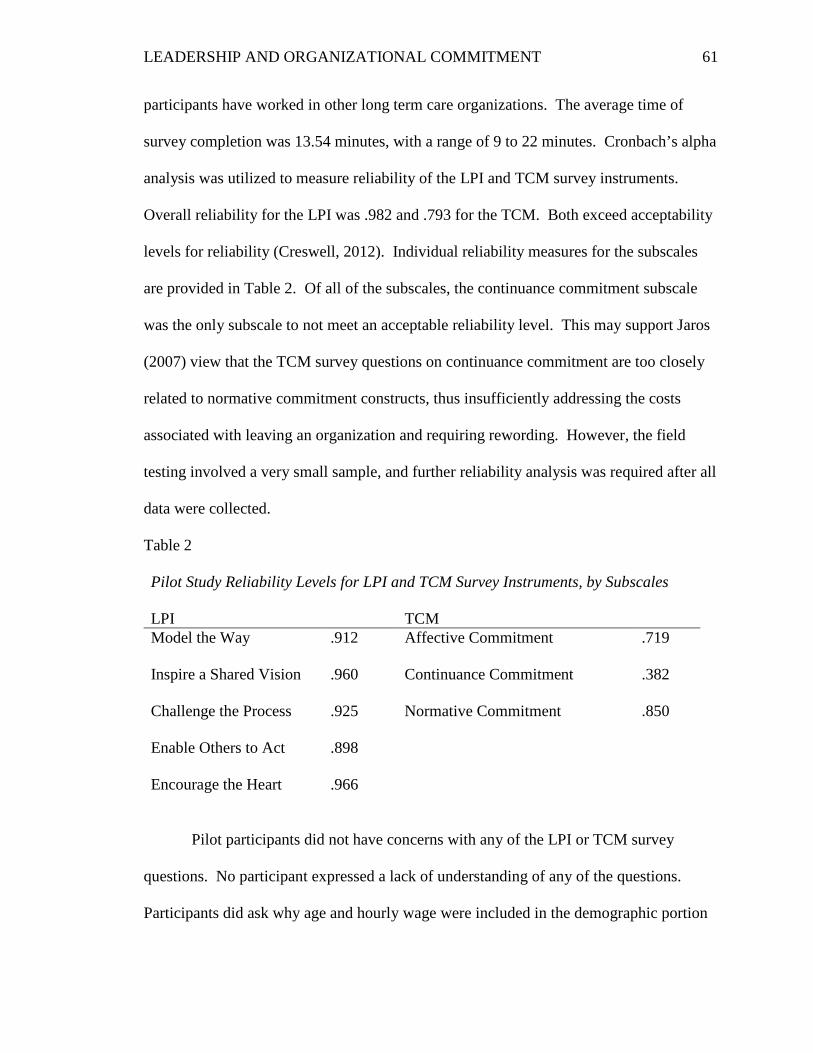
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 61
participants have worked in other long term care organizations. The average time of
survey completion was 13.54 minutes, with a range of 9 to 22 minutes. Cronbach’s alpha
analysis was utilized to measure reliability of the LPI and TCM survey instruments.
Overall reliability for the LPI was .982 and .793 for the TCM. Both exceed acceptability
levels for reliability (Creswell, 2012). Individual reliability measures for the subscales
are provided in Table 2. Of all of the subscales, the continuance commitment subscale
was the only subscale to not meet an acceptable reliability level. This may support Jaros
(2007) view that the TCM survey questions on continuance commitment are too closely
related to normative commitment constructs, thus insufficiently addressing the costs
associated with leaving an organization and requiring rewording. However, the field
testing involved a very small sample, and further reliability analysis was required after all
data were collected.
Table 2
Pilot Study Reliability Levels for LPI and TCM Survey Instruments, by Subscales LPI TCM Model the Way .912 Affective Commitment .719
Inspire a Shared Vision .960 Continuance Commitment .382
Challenge the Process .925 Normative Commitment .850
Enable Others to Act .898
Encourage the Heart .966
Pilot participants did not have concerns with any of the LPI or TCM survey
questions. No participant expressed a lack of understanding of any of the questions.
Participants did ask why age and hourly wage were included in the demographic portion
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 62
of the survey and stated they were uncomfortable in providing the information without
knowing how the information would be used. After an explanation, they expressed
agreement that the data should be gathered but suggested including a short note by the
specific questions to minimize skipped answers. In response to asking what methods
were best for reaching DCWs, flyers and change of shift reminders were agreed to be the
best methods. Invitation letters, whether mailed or distributed in advance onsite, were
not viewed as optimal because participants felt the invitation letters would be discarded
and forgotten. Participants suggested that flyers be posted around the organization and
particularly by the time clock. They added that a shift change reminder would enhance
participation. They suggested multiple opportunities (at least three) to participate. With
regard to snacks, they supported the use of snacks similar to what was provided to them
(pretzels, granola bars, and bottled water) and reinforced the need to tailor the snack to
the time of day, e.g. muffins for breakfast. Lunch was determined to be unnecessary due
to the perceived time and cost constraints and inequitable availability to all participants.
The pilot study concluded by informing the participants that their completed surveys
would be excluded from the overall study results and sharing appreciation for their
assistance. As a result of the pilot study, several changes were made to the survey
process. Flyers and shift change reminders were used to invite DCWs to participate in
the study. The survey document was revised to incorporate participant feedback. All
changes were submitted to and approved by the Creighton IRB for approval for use in the
primary study.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 63
Variables
Transformational leadership and organizational commitment were the variables of
interest for this study. The predicting variable was transformational leadership and was
defined as a process whereby leaders have a conscious goal to develop followers into
leaders, exhibit behaviors that elicit trust, and display self-sacrificial perspectives to build
commitment and influence, and demonstrate a moral compass towards mission and
purpose (Avolio, 2011; Bass, 1985; Kouzes & Posner,1988, 2012). The criterion, or
outcome, variable was organizational commitment. For purposes of this study,
organizational commitment was defined as a psychological state linking employees to
their organizations (Meyer & Allen, 1997, p.23). The study further considered
organizational commitment along three dimensions: affective, continuance, and
normative.
Data Collection Procedures
The target population for this study was DCWs employed by nonprofit long term
care organizations in the Midwest. Prior to data collection, approval for the research was
obtained by the Creighton University Institutional Review Board. Using a purposeful
sampling approach, nine nonprofit, long term care organizations in the Midwest agreed to
participate, contributing 1,127 DCWs for participation in the study. Utilizing both
conference calls and electronic mail communication, on site visits were scheduled and
data collection occurred between May and July 2014. In advance of onsite visits,
participants were provided with an invitation to participate in the study utilizing flyers
and change of shift reminders. Once onsite, DCWs were provided multiple opportunities
to participate in the study and complete a paper survey. Multiple opportunities were
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 64
intended to accommodate the varied work schedules of DCWs and provide ample
occasions to participate in the study. Survey completion time was estimated to be fifteen
minutes. Prior to completing the survey, participants were provided the informed
consent/assent information, followed by the two survey instruments and the demographic
information. Because no identifying information was collected by the participants,
informed consent/assent was implied through completion of the survey, as approved by
the IRB. Following survey completion, the surveys were transferred to a secure container
to ensure confidentiality. To thank participants, snacks were provided.
Data Analysis Plan
SPSS® 22 was used to calculate statistics and test the hypotheses. Following
onsite visits, survey data were coded and entered into the SPSS® 22 application. A code
key was utilized to ensure responses were coded correctly and consistently. Coding
involved assigning numerical values to all responses (Creswell, 2012). Data analysis
included the calculation of response rates, use of descriptive statistics (mean, standard
deviation, percentages) to identify general trends and results, and evaluation of
correlations using inferential statistical analysis. Data was checked to ensure the data met
the assumptions for the statistical tests used for the study. Nonparametric statistical tests
were used due to the nonprobability sampling approach for the study; however, normality
was tested using the Shapiro-Wilk test for confirmation (Creswell, 2012). The LPI and
TCM instruments used in the study utilized Likert-type measurement scales that were
treated as interval scales. Correlational analysis was used to measure the relationship
between the interval variables and to assist in making predictions about the variable
associations (Creswell, 2012). When investigating linear-related variables, the
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 65
Spearman’s rank order correlation (Spearman’s rho) can be used for nonparametric
testing and is recommended especially when normality is questioned (Kowalski, 1972;
Onwuegbuzie & Daniel, 2002). Internal reliability testing was conducted using
Cronbach’s alpha to determine if the survey scales were reliable (Creswell, 2012). To
evaluate the data for the research question regarding differences between types of long
term care settings, the independent t- test was used to allow a comparison of independent
groups (Creswell, 2012). The independent t-test has been found to be a valid statistical
test for both normally and non-normally distributed samples and in samples as small as
100 in size (Lumley, Diehr, Emerson, & Chen, 2002). A significant relationship was
defined using a 95% confidence interval for statistical testing of the hypotheses.
Assumptions
Numerous studies have assessed validity and reliability of the LPI and TCM
survey instruments and have concluded internal consistency and validity exist (Kouzes &
Posner, 2000, 2002; Jaros, 2007; Meyer et al., 2002). Demonstrated reliability indicated
that field testing was not necessary. However, given the lack of empirical research in the
long term care industry, the survey instruments were field tested to analyze reliability as
well as obtain feedback on the clarity of instructions and identification of best options for
survey invitation. Due to the nonprobability sampling approach for the study,
nonparametric statistical testing was utilized and normality tests were conducted.
Ethical Considerations
Ethical considerations were present for this study and addressed responsibility,
respect, and integrity for the participating organizations and their employees. This
research study was approved by the Creighton University Institutional Review Board
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 66
(IRB). Privacy, confidentiality, and anonymity were all applicable issues for this study.
Privacy was addressed with respect to providing DCWs a perceived safe location to
complete the onsite survey. Site administration and supervisors were discouraged access
to the room in which participants completed the surveys. Confidentiality was preserved
to the level that DCWs chose to avoid discussion with each other or other employees
about their participation in the study. Anonymity and confidentiality were preserved by
not obtaining identifying information from participants on the survey document or in any
other form. All completed surveys were put in a secure box for confidential transfer from
the study site. Additionally, all data were analyzed in the aggregate, thus strengthening
the commitment to anonymity for participants.
Each organization was required to formally address permissive rights for the
researcher to engage in research activities as a part of the study. Participation in the
study was voluntary, and there were no consequences for not participating. It was
possible that DCWs under the age of majority would participate in the study due to data
collection occurring in the summer. For this reason, the researcher reviewed the
inclusion of children as important to the study. This segment of the DCW population
completes the same DCW tasks as their colleagues, regardless of age. Likewise, those
under the age of majority have completed the same training to perform DCW tasks. No
more than minimal risk was expected for DCWs under the age of majority because they
were not being treated any differently than any of their corresponding colleagues. It
would have been difficult to obtain parental permission for these DCWs to participate in
the study because by doing so, identifying information would be collected, thus creating
an imbalance to the commitment of anonymity and confidentiality. As a result, a waiver
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 67
of assent was required and approved by the Creighton University IRB. Participants
received an informed consent/assent form prior to participation. To ensure anonymity
and confidentiality of participation, no signatures were obtained to indicate consent or
non-consent to participate. Completion of the survey constituted consent/assent to
participate.
There were no direct benefits to participating in the study. Participation in the
study provided insight into the relationship between transformational leadership and
organizational commitment. Participants had the option to not complete the survey. In
these instances, there were no other alternatives to participating in the study. Snacks
were provided to participants as an incentive to participate in the study. Not completing a
survey did not preclude DCWs from receiving the incentive, assisting the researcher in
alleviating any appearance of coercion.
The researcher intends to publish the results of the study, but no identifying
information will be disclosed. Participating organizations will receive a copy of the
research as a benefit to participating. However, to preserve anonymity and
confidentiality of participating DCWs, data were evaluated in the aggregate. Direct
benefits to the researcher involve completion of academic requirements of Creighton
University as well as future publication of research findings.
Summary
Chapter three discussed the research methodology employed to investigate the
research questions and corresponding hypotheses. The research methodology included a
review of methodology rationale, the sample, survey instrumentation and its reliability
and validity, variables, data collection and analysis, and ethical considerations of this
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 68
study. This quantitative correlational study described the relationship between
transformational leadership and organization commitment among direct care workers in
nonprofit, long term care organizations. A correlational design was the most appropriate
research design due to the need to understand how the variables co-vary (Creswell,
2012). The study also addressed any differences between long term care settings.
Nonparametric statistical testing methods were utilized given the nonprobability
sampling approach.
The survey document included the LPI (Kouzes & Posner, 2013) and TCM
(Meyer & Allen, 2004) survey instruments as well as demographic questions needed for
descriptive statistics. Both instruments have been established as valid and reliable
(Kouzes & Posner, 2000, 2002; Jaros, 2007; Meyer et al., 2002). The survey document
was field tested for additional internal consistency and to obtain feedback for potential
adjustments to the document and process in general. Ethical considerations were
addressed, reviewed, and approved by the Creighton University IRB.
Chapter four contains the results of the study. Data were interpreted through
statistical analysis and displayed in appropriate format.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 69
CHAPTER FOUR: FINDINGS
Introduction
The purpose of this quantitative study was to determine what relationship exists
between transformational leadership and organizational commitment for direct care
workers in nonprofit long term care organizations. Presented in Chapter four are the
results of the analyses addressing the research questions and hypotheses posed in the
study. The research questions and hypotheses tested were:
RQ1: What is the relationship between transformational leadership and
organizational commitment (affective, continuance, and normative) among direct care
workers in nonprofit long term care organizations?
Three specific hypotheses will be investigated in this study:
H1: There is a significant positive relationship between transformational
leadership and DCW affective commitment.
H2: There is a significant inverse relationship between transformational
leadership and DCW continuance commitment.
H3: There is a significant positive relationship between transformational
leadership and DCW normative commitment.
RQ2: Is there a difference, if any, between types of long term care settings for
transformational leadership and organizational commitment?
H4: There is no difference between types of long term care settings for
transformational leadership and organizational commitment.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 70
Review of the Methodology
This study used a quantitative, correlational research design and nonprobability
sampling. For the study, transformational leadership was the predictor variable, and
organizational commitment was the criterion, or outcome, variable. The study design
utilized nonprobability sampling to obtain study participants, representing a purposeful
sampling approach (Creswell, 2012). Two instruments were used for this study: a)
Leadership Practice Inventory (LPI) Observer which measured transformational
leadership (Kouzes & Posner, 2013), and b) Three-Component Model Commitment
Survey (TCM) which measured organizational commitment (Meyer & Allen, 2004).
Correlational, nonparametric statistical analysis was used to test the hypotheses. The
population of the study consisted of DCWs employed by Midwestern nonprofit long term
care organizations meeting specific criteria: a) nonprofit status, b) provision of multiple
lines of service, or types of long term care settings, and c) willingness to participate.
Following approval by the Creighton University IRB, the survey instruments were
field tested with thirteen DCWs in a pilot study conducted in a Midwestern long term
care organization located in close proximity of the researcher. Data were analyzed using
SPSS® 22. Cronbach’s alpha analysis was utilized to measure reliability of the LPI and
TCM survey instruments from the pilot study. Feedback from the pilot study also
informed the researcher of changes needed in the overall survey format as well as
provided input on perceived best methods for participant invitation in the study. Changes
to the survey document were submitted for review and approval by the Creighton
University IRB prior to data collection.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 71
Using a purposeful sampling approach, nonprofit, long term care organizations in
the Midwest were contacted to participate and conference calls, electronic mail, and
phone calls were utilized to schedule the dates and times for data collection. Based on
the number of DCWs employed at the organizations at the time of data collection, 1,127
DCWs were invited to participate through the use of flyer invitations posted at visibly
accessible locations on site, including the time clock areas. Data collection occurred
within an eight-week time frame during May, June, and July, 2014. Once onsite, DCWs
were provided multiple opportunities to participate in the study and complete a paper
survey in order to accommodate the varied work schedules of DCWs. Participants were
provided informed consent/assent information prior to completing the survey, and survey
completion time was approximately fifteen minutes. No identifying information was
collected by the participants, with informed consent/assent implied through completion of
the survey, as approved by the IRB. Following survey completion, the surveys were
transferred to a secured container to ensure confidentiality. To thank participants, snacks
were provided. The data collection process resulted in a sample of 322 surveys,
constituting a 28.6% response rate.
Data Analysis Procedures
SPSS® 22 was used to calculate statistics and test the hypotheses. Because the
data collection involved paper surveys and manual data entry, a ten percent random
sample of the data was used to identify any input errors in SPSS® 22. Participants were
allowed to skip survey questions, thus creating opportunity for missing data. Missing
data were coded uniquely and excluded as appropriate within the data analysis. The most
frequently excluded data were age, hourly wage, and income level. Nonparametric
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 72
statistical tests were used due to the nonprobability sampling approach for the study, and
normality was tested using the Shapiro-Wilk test, confirming the expected non-normal
distribution with significance levels ranging from .000 to .036 (Creswell, 2012). Q-Q
plots were also used to graphically review for normality and also confirmed non-normally
distributed data. The LPI and TCM instruments used in the study utilized Likert-type
measurement scales and were treated as interval scales. Correlational analysis was used
to measure the relationship between the interval variables and to assist in making
predictions about the variable associations (Creswell, 2012). When investigating linear-
related variables when normality is questioned, the Spearman’s rank order correlation
coefficient (Spearman’s rho) can be used and is recommended as more robust than the
Pearson correlation (Kowalski, 1972; Onwuegbuzie & Daniel, 2002).
Internal reliability testing was conducted using Cronbach’s alpha to determine if
the survey scales are reliable (Creswell, 2012). To evaluate the data for the research
question regarding differences between types of long term care settings, the independent
t-test was used to allow a comparison of two independent groups (Creswell, 2012), which
has been found to be a valid statistical test regardless of data distribution (Lumley, Diehr,
Emerson, & Chen, 2002). Normality testing was conducted using the Shapiro Wilk test
and homogeneity of variance was tested using Levene’s Test of Equality of Variances
(Creswell, 2012). A significant relationship was defined using a 95% confidence interval
for statistical testing of the hypotheses.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 73
Results
Participant Characteristics
Participants represented DCWs employed at nonprofit long term care
organizations offering multiple service settings (nursing facilities, assisted living, home
health, hospice, senior housing, and adult day services). Participant characteristics were
identified based on service setting and several demographic considerations, including
age, gender, ethnicity, hourly wage, annual income, education level, and years of
employment at the respective organization and in long term care in general. Of
participants responding (n=314), 79.3% work in nursing facilities, 15.2% in assisted
living facilities, 11.8% in independent living senior housing, 4.5% in home health, 2.9%
in hospice, 1.3% in affordable senior housing, and .6% in adult day services.
Female participants dominated the study sample at 82.7% (n=317). Participants
ranged in age from 17 to 77 years old, with a mean of 39.05 years (n=303). Regarding
ethnicity, white participants constituted a majority at 76.7%, with African/black
participants following at 11.8%. The remaining participants were Hispanic (5.6%), Asian
(2.2%), American Indian (1.2%), and other (.6%). Of the participants responding, 9.3%
indicated that English was their second language. The median hourly range of
participants was $12.00 (n=295, SD = 2.69), with a range of $7.35 to $30 per hour, with
88.5% of participants reporting an annual income less than $30,000 (n=304). Of those
responding (n=313), 20.4% stated they have more than one job, and 50.5% (n=317)
indicated a dissatisfaction with their pay. Of 314 responding participants, 11.5% reported
receiving government assistance, such as Medicaid, food assistance, and utilities
assistance. Participants reported a range of formal education (n=314); 52.5% reported
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 74
having a high school diploma or GED, while 38.2% have an undergraduate college
degree, 8% have a graduate college degree and 1.3% have less than a high school
education.
Length of employment was also evaluated, both from an organizational standpoint
as well as from an industry context. Organizationally, 21.2% of participants reported
being newly hired less than one year in their employment (n=316). Other tenure was
reported as follows: 1 to 3 years (32.3%), 4 to 6 years (15.8%), 7 to 9 years (10.4%), and
more than 10 years (20.3%). Based on survey coding, the average length of employment
was 2.76, representing employment between one and six years. Industry employment
tenure exceeds organizational tenure, with 32.3% of participants working in the industry
for over ten years (n=315). Just under ten percent (9.8%) of participants reported less
than one year of employment in the industry, with 40% indicating industry tenure
between one and five years and 17.8% indicating tenure between six and ten years.
Average employment tenure in the industry was 3.11, representing employment between
six and ten years. When asked whether participants were considering a job change,
26.3% indicated affirmatively and 25.7% stated “not sure, maybe” (n=315).
Site administrators at participating organizations reported employing 1,127
DCWs, accounting for 54.6% of total employees. A mean turnover rate of 33.4% was
reported, with turnover ranging between 16% and 51.5%. The wage range for DCWs
was $7.50 to $20.63 depending on position and experience. National median hourly
wage ranges between $9.57 and $11.74, depending on the type of DCW position (PHI,
2013b). All organizations reported providing health insurance benefits in addition to
benefits such as paid vacation, paid sick time, paid holiday time, and retirement plans.
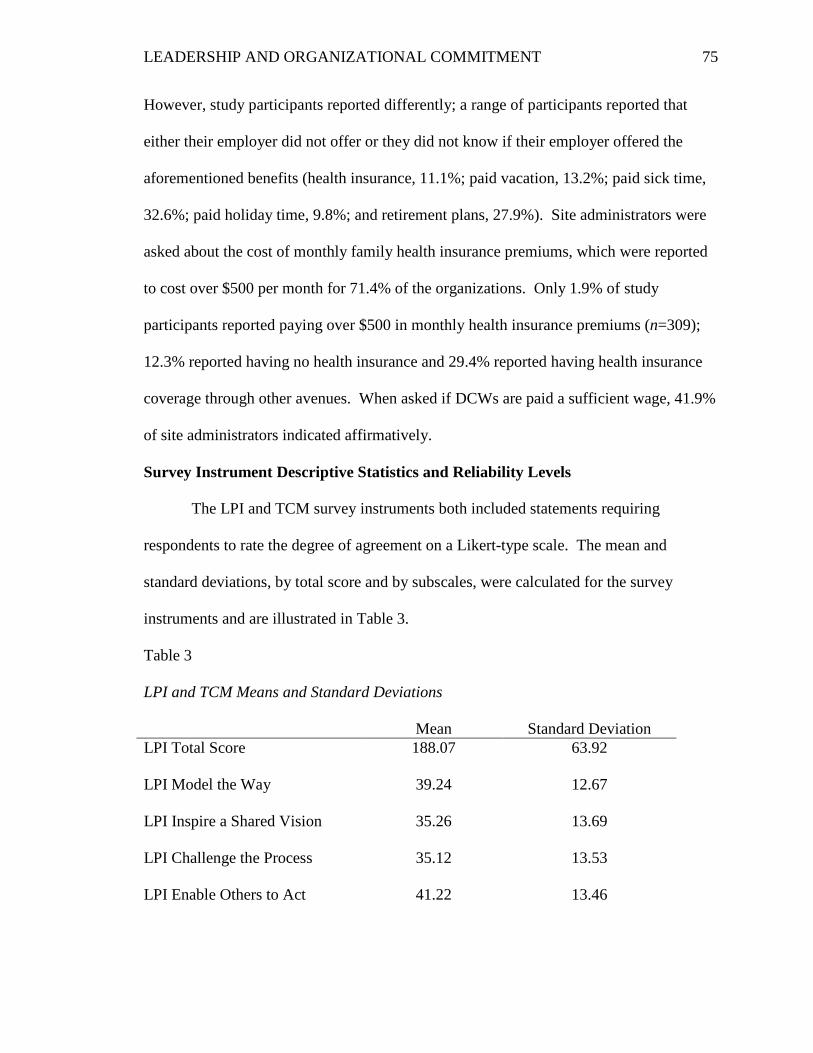
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 75
However, study participants reported differently; a range of participants reported that
either their employer did not offer or they did not know if their employer offered the
aforementioned benefits (health insurance, 11.1%; paid vacation, 13.2%; paid sick time,
32.6%; paid holiday time, 9.8%; and retirement plans, 27.9%). Site administrators were
asked about the cost of monthly family health insurance premiums, which were reported
to cost over $500 per month for 71.4% of the organizations. Only 1.9% of study
participants reported paying over $500 in monthly health insurance premiums (n=309);
12.3% reported having no health insurance and 29.4% reported having health insurance
coverage through other avenues. When asked if DCWs are paid a sufficient wage, 41.9%
of site administrators indicated affirmatively.
Survey Instrument Descriptive Statistics and Reliability Levels
The LPI and TCM survey instruments both included statements requiring
respondents to rate the degree of agreement on a Likert-type scale. The mean and
standard deviations, by total score and by subscales, were calculated for the survey
instruments and are illustrated in Table 3.
Table 3
LPI and TCM Means and Standard Deviations Mean Standard Deviation LPI Total Score 188.07 63.92
LPI Model the Way 39.24 12.67
LPI Inspire a Shared Vision 35.26 13.69
LPI Challenge the Process 35.12 13.53
LPI Enable Others to Act 41.22 13.46
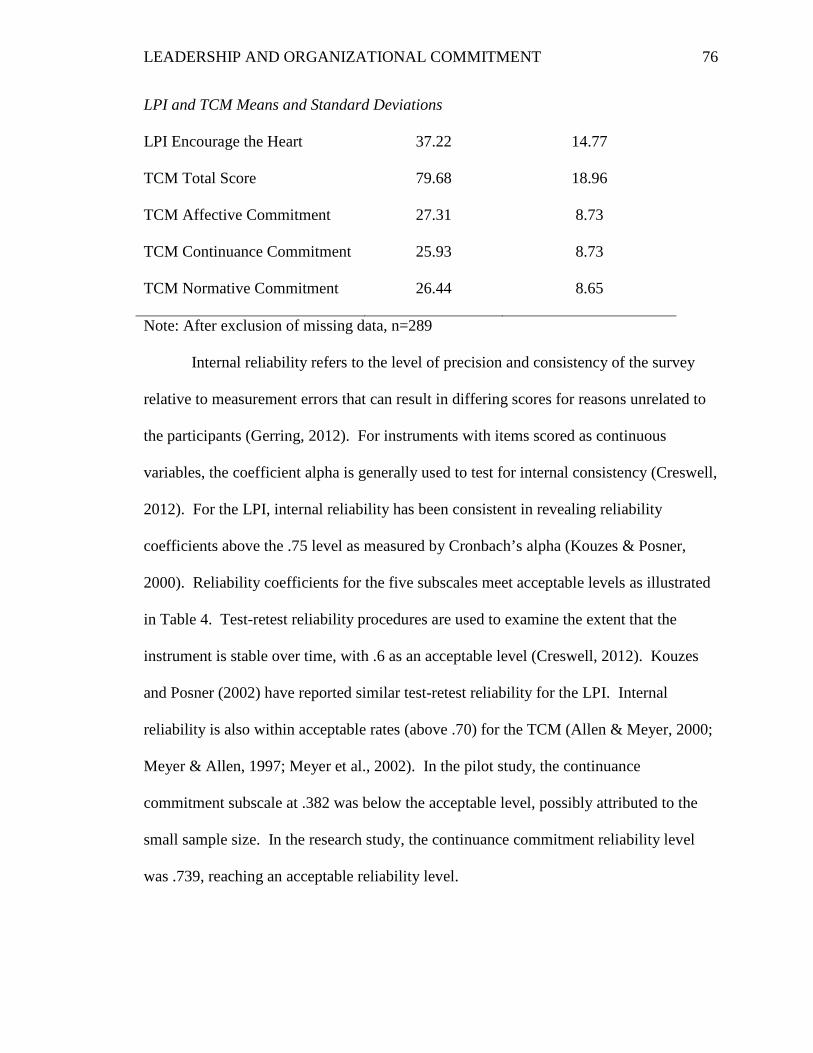
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 76
LPI and TCM Means and Standard Deviations LPI Encourage the Heart 37.22 14.77
TCM Total Score 79.68 18.96
TCM Affective Commitment 27.31 8.73
TCM Continuance Commitment 25.93 8.73
TCM Normative Commitment 26.44 8.65
Note: After exclusion of missing data, n=289
Internal reliability refers to the level of precision and consistency of the survey
relative to measurement errors that can result in differing scores for reasons unrelated to
the participants (Gerring, 2012). For instruments with items scored as continuous
variables, the coefficient alpha is generally used to test for internal consistency (Creswell,
2012). For the LPI, internal reliability has been consistent in revealing reliability
coefficients above the .75 level as measured by Cronbach’s alpha (Kouzes & Posner,
2000). Reliability coefficients for the five subscales meet acceptable levels as illustrated
in Table 4. Test-retest reliability procedures are used to examine the extent that the
instrument is stable over time, with .6 as an acceptable level (Creswell, 2012). Kouzes
and Posner (2002) have reported similar test-retest reliability for the LPI. Internal
reliability is also within acceptable rates (above .70) for the TCM (Allen & Meyer, 2000;
Meyer & Allen, 1997; Meyer et al., 2002). In the pilot study, the continuance
commitment subscale at .382 was below the acceptable level, possibly attributed to the
small sample size. In the research study, the continuance commitment reliability level
was .739, reaching an acceptable reliability level.
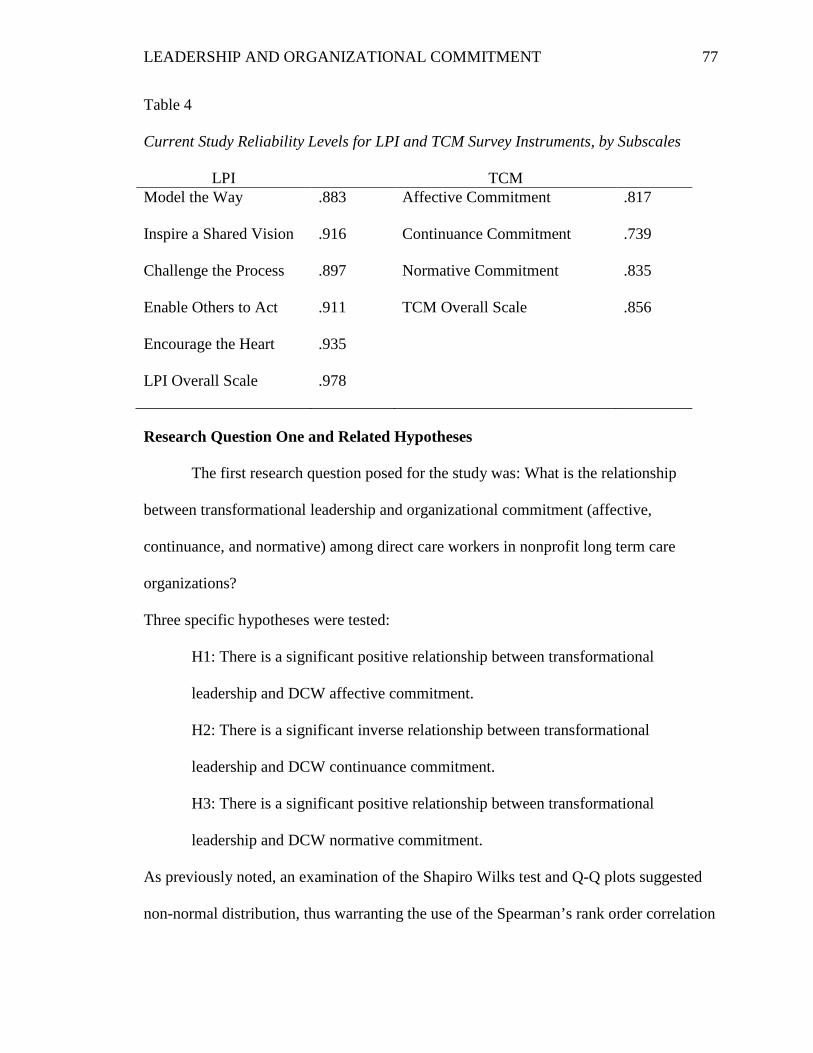
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 77
Table 4 Current Study Reliability Levels for LPI and TCM Survey Instruments, by Subscales
LPI TCM Model the Way .883 Affective Commitment .817
Inspire a Shared Vision .916 Continuance Commitment .739
Challenge the Process .897 Normative Commitment .835
Enable Others to Act .911 TCM Overall Scale .856
Encourage the Heart .935
LPI Overall Scale .978
Research Question One and Related Hypotheses
The first research question posed for the study was: What is the relationship
between transformational leadership and organizational commitment (affective,
continuance, and normative) among direct care workers in nonprofit long term care
organizations?
Three specific hypotheses were tested:
H1: There is a significant positive relationship between transformational
leadership and DCW affective commitment.
H2: There is a significant inverse relationship between transformational
leadership and DCW continuance commitment.
H3: There is a significant positive relationship between transformational
leadership and DCW normative commitment.
As previously noted, an examination of the Shapiro Wilks test and Q-Q plots suggested
non-normal distribution, thus warranting the use of the Spearman’s rank order correlation
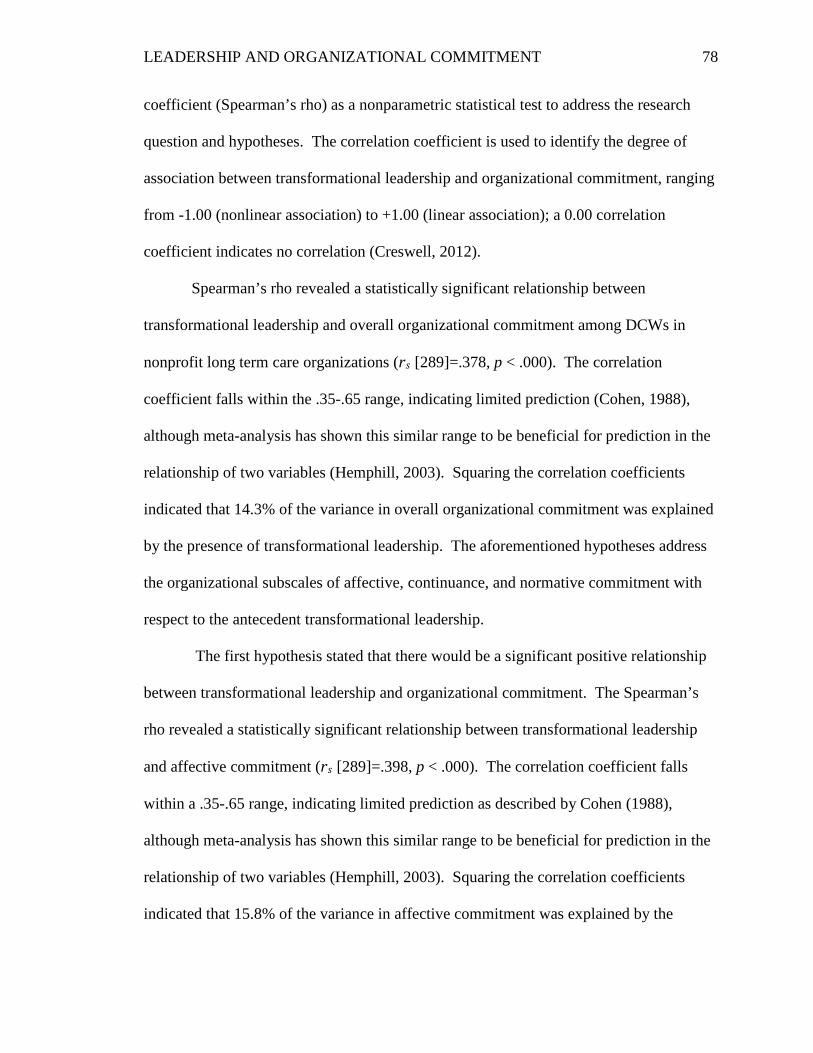
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 78
coefficient (Spearman’s rho) as a nonparametric statistical test to address the research
question and hypotheses. The correlation coefficient is used to identify the degree of
association between transformational leadership and organizational commitment, ranging
from -1.00 (nonlinear association) to +1.00 (linear association); a 0.00 correlation
coefficient indicates no correlation (Creswell, 2012).
Spearman’s rho revealed a statistically significant relationship between
transformational leadership and overall organizational commitment among DCWs in
nonprofit long term care organizations (rs [289]=.378, p < .000). The correlation
coefficient falls within the .35-.65 range, indicating limited prediction (Cohen, 1988),
although meta-analysis has shown this similar range to be beneficial for prediction in the
relationship of two variables (Hemphill, 2003). Squaring the correlation coefficients
indicated that 14.3% of the variance in overall organizational commitment was explained
by the presence of transformational leadership. The aforementioned hypotheses address
the organizational subscales of affective, continuance, and normative commitment with
respect to the antecedent transformational leadership.
The first hypothesis stated that there would be a significant positive relationship
between transformational leadership and organizational commitment. The Spearman’s
rho revealed a statistically significant relationship between transformational leadership
and affective commitment (rs [289]=.398, p < .000). The correlation coefficient falls
within a .35-.65 range, indicating limited prediction as described by Cohen (1988),
although meta-analysis has shown this similar range to be beneficial for prediction in the
relationship of two variables (Hemphill, 2003). Squaring the correlation coefficients
indicated that 15.8% of the variance in affective commitment was explained by the
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 79
presence of transformational leadership. Because the p value is less than the alpha level
(.05), the hypothesis is supported that there is a significant positive relationship between
transformational leadership and affective commitment.
The second hypothesis stated that there would be a significant inverse relationship
between transformational leadership and continuance commitment. This means that as
transformational leadership increases, continuance commitment decreases. The
Spearman’s rho revealed no significant relationship between transformational leadership
and continuance commitment (rs [289]=.021, p < .722). The correlation coefficient falls
below .20, indicating there is little usefulness or value in predicting the relationship
between transformational leadership and continuance commitment (Cohen, 1988;
Hemphill, 2003). Also, the p value (.722) is greater than the alpha level (.05). Thus, the
second hypothesis is rejected that there is a significant negative relationship between
transformational leadership and continuance commitment.
The third hypothesis stated that there would be a significant positive relationship
between transformational leadership and normative commitment. The Spearman’s rho
revealed a statistically significant relationship between transformational leadership and
normative commitment (rs [289]=.395, p < .000). The correlation coefficient falls within
the .35-.65 range, indicating limited prediction (Cohen, 1988), but meta-analysis has
described this level as beneficial for prediction in the relationship of two variables
(Hemphill, 2003). Squaring the correlation coefficients indicated that 15.6% of the
variance in normative commitment was explained by the presence of transformational
leadership. Because the p value is less than the alpha level (.05), the hypothesis is
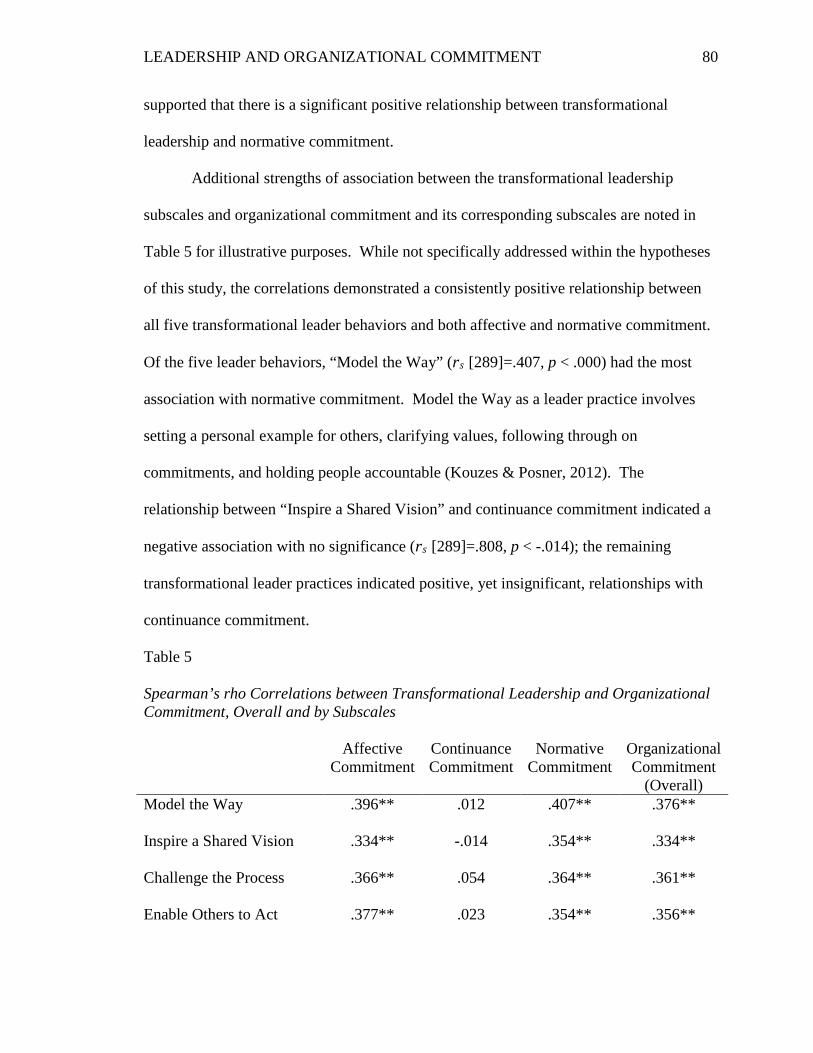
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 80
supported that there is a significant positive relationship between transformational
leadership and normative commitment.
Additional strengths of association between the transformational leadership
subscales and organizational commitment and its corresponding subscales are noted in
Table 5 for illustrative purposes. While not specifically addressed within the hypotheses
of this study, the correlations demonstrated a consistently positive relationship between
all five transformational leader behaviors and both affective and normative commitment.
Of the five leader behaviors, “Model the Way” (rs [289]=.407, p < .000) had the most
association with normative commitment. Model the Way as a leader practice involves
setting a personal example for others, clarifying values, following through on
commitments, and holding people accountable (Kouzes & Posner, 2012). The
relationship between “Inspire a Shared Vision” and continuance commitment indicated a
negative association with no significance (rs [289]=.808, p < -.014); the remaining
transformational leader practices indicated positive, yet insignificant, relationships with
continuance commitment.
Table 5 Spearman’s rho Correlations between Transformational Leadership and Organizational Commitment, Overall and by Subscales Affective
Commitment Continuance Commitment
Normative Commitment
Organizational Commitment
(Overall) Model the Way .396** .012 .407** .376**
Inspire a Shared Vision .334** -.014 .354** .334**
Challenge the Process .366** .054 .364** .361**
Enable Others to Act .377** .023 .354** .356**
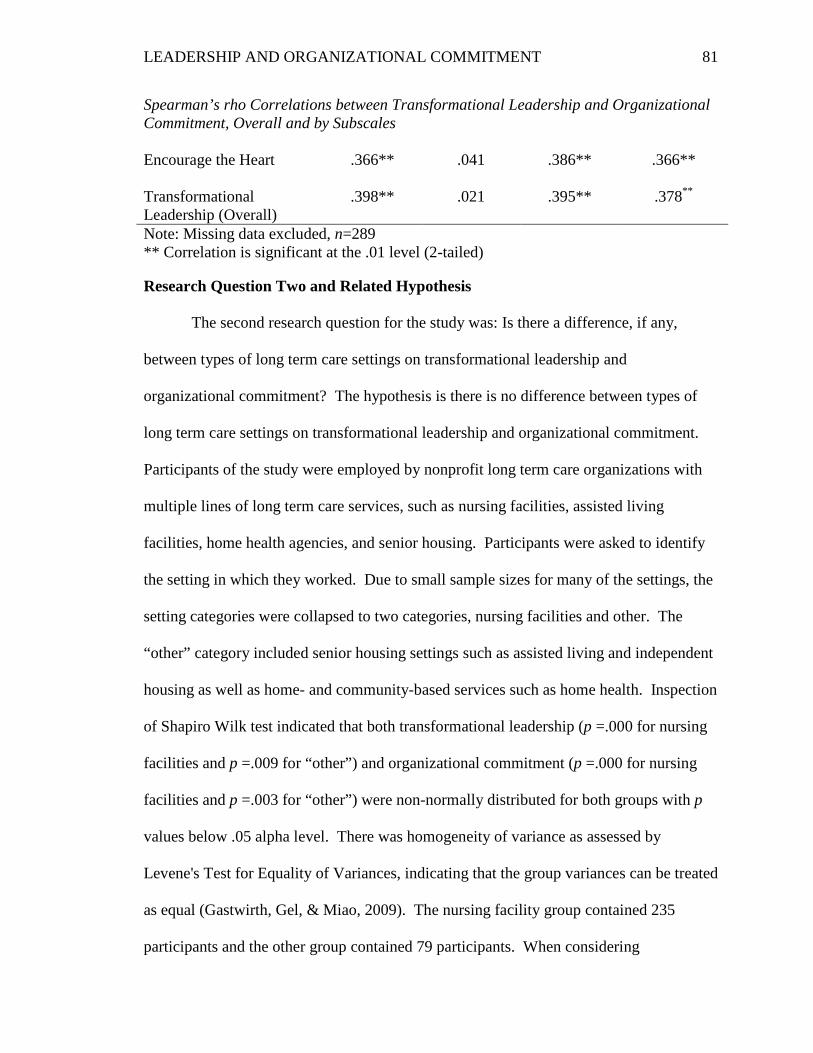
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 81
Spearman’s rho Correlations between Transformational Leadership and Organizational Commitment, Overall and by Subscales Encourage the Heart .366** .041 .386** .366**
Transformational Leadership (Overall)
.398** .021 .395** .378**
Note: Missing data excluded, n=289 ** Correlation is significant at the .01 level (2-tailed) Research Question Two and Related Hypothesis
The second research question for the study was: Is there a difference, if any,
between types of long term care settings on transformational leadership and
organizational commitment? The hypothesis is there is no difference between types of
long term care settings on transformational leadership and organizational commitment.
Participants of the study were employed by nonprofit long term care organizations with
multiple lines of long term care services, such as nursing facilities, assisted living
facilities, home health agencies, and senior housing. Participants were asked to identify
the setting in which they worked. Due to small sample sizes for many of the settings, the
setting categories were collapsed to two categories, nursing facilities and other. The
“other” category included senior housing settings such as assisted living and independent
housing as well as home- and community-based services such as home health. Inspection
of Shapiro Wilk test indicated that both transformational leadership (p =.000 for nursing
facilities and p =.009 for “other”) and organizational commitment (p =.000 for nursing
facilities and p =.003 for “other”) were non-normally distributed for both groups with p
values below .05 alpha level. There was homogeneity of variance as assessed by
Levene's Test for Equality of Variances, indicating that the group variances can be treated
as equal (Gastwirth, Gel, & Miao, 2009). The nursing facility group contained 235
participants and the other group contained 79 participants. When considering
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 82
transformational leadership in comparing the groups, the data showed the nursing facility
group reported lower transformational leader behaviors (M =184.37, SD = 64.83) than the
“other” group (M =196.72, SD = 57.43). For organizational commitment, the nursing
facility group (M =77.56, SD = 19.41) also reported lower organizational commitment
scores than the “other” group (M =85.85, SD = 18.72). Comparing the means for the
groups revealed the following results for each variable: a) transformational
leadership t(312) = -1.506, p = .133, and b) organizational commitment t(312) = -
3.311, p = .001. The conclusion is to fail to reject the hypothesis that there is no
difference between types of long term care settings (between nursing facilities and
“other”) with regard to transformational leadership. However, the data shows that the
hypothesis can be rejected that there is no difference between types of long term care
settings (between nursing facilities and “other”) with regard to organizational
commitment.
Summary
The first three hypotheses of the study were related to either significant positive
or inverse relationships between transformational leadership and organizational
commitment and the subscales of affective, continuance, and normative commitment
among DCWs in nonprofit long term care organizations. The Spearman’s rank order
correlation coefficient statistical test was used to analyze whether the variables co-vary.
The first hypothesis was supported, indicating there is a significant positive relationship
between transformational leadership and affective commitment. The second hypothesis
was rejected, indicating there is not a significant inverse relationship between
transformational leadership and continuance commitment. The third hypothesis was
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 83
supported, indicating there is a significant positive relationship between transformational
leadership and normative commitment. In evaluating the relationship of transformational
leadership with overall organizational commitment, a significant positive relationship
was revealed in the data analysis.
The fourth null hypothesis addressed no difference between types of long term
care settings for transformational leadership and organizational commitment. An
independent t-test was used to compare the means of two groups, those DCWs working
in nursing facilities and those DCWs working in other long term care settings. For
transformational leadership, the null hypothesis failed to be rejected, indicating there is
no difference between types of long term care settings. For organizational commitment,
the null hypothesis was rejected, indicating there is a significant difference between types
of long term care settings, specifically nursing facilities and “other” in this study.
Presented in Chapter five are the conclusions, implications, and recommendations of the
data analysis results.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 84
CHAPTER FIVE: CONCLUSIONS AND RECOMMENDATIONS
Introduction
The aim of this study was to gain further understanding about how leader
behaviors influence organizational commitment among DCWs in the nonprofit long term
care industry by providing DCWs an opportunity to voice their perspective and
advocating on their behalf. The purpose of the quantitative correlational study was to
explore the relationship between transformational leadership and organizational
commitment among DCWs in nonprofit, long term care organizations. Transformational
leadership, as the predictor variable is generally understood as a process whereby leaders
have a conscious goal to develop followers into leaders, exhibit behaviors that elicit trust,
and display self-sacrificial perspectives to build commitment and influence, and
demonstrate a moral compass towards mission and purpose (Avolio, 2011; Bass, 1985;
Kouzes & Posner,1988; 2012). Organizational commitment, as the outcome variable, is
generally described as a “psychological state linking employees to their organizations”
and considered along three dimensions: affective, continuance, and normative (Meyer &
Allen, 1997, p. 23).
Similar to other industries and organizations, long term care leaders must consider
how leadership practices influence organizational commitment and yet, little literature
exists that addresses the DCW perspective of leadership qualities and the importance to
organizational commitment. Because transformational leadership has not been studied as
an antecedent in the context of long term care, this study was intended to respond to this
deficiency as well as contribute to the nonprofit literature in reflecting the importance of
transformational leadership in this context. Findings of the study can benefit scholarship,
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 85
practice, and policy within the long term care industry. Within the scholarship arena, this
study responded to a research deficiency by focusing on DCWs and their immediate
supervisors; however, further research is warranted. For industry practitioners and policy
makers, the findings are useful in considering modifications of operational policies,
identifying training and development needs, revisiting human resources practices, and
evaluating workforce resources. Conclusions, implications, and recommendations are
addressed in Chapter five.
Summary of the Study
A growing aging population and workforce shortage provide great challenges for
the long term care industry. Leaders within the industry must tackle these challenges by
addressing a wide range of external factors and looking to leadership practices directly
affecting the workforce they hope to retain. The purpose of the study was to explore the
relationship between transformational leadership and organizational commitment among
DCWs in nonprofit long term care organizations. Two research questions were
addressed: a) What is the relationship between transformational leadership and
organizational commitment (affective, continuance, and normative) among direct care
workers in nonprofit long term care organizations? and b) Is there a difference, if any,
between types of long term care settings for transformational leadership and
organizational commitment? A quantitative correlational design study was used to assess
the strength of the relationships between the variables. The study included 322 DCWs
employed by nine nonprofit long term care organizations located in the Midwest. The
study participants completed a survey document including the LPI (Kouzes & Posner,
2013) and the TCM (Meyer & Allen, 2004) survey instruments and demographic
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 86
questions. For participants, the completion of the survey was confidential and
anonymous. SPSS® 22 was used to analyze the data, and statistical tests included
normality testing, Spearman’s rank order correlation coefficient, and independent t-tests.
Findings revealed a significant positive relationship between transformational leadership
and overall organizational commitment, a significant positive relationship between
transformational leadership and both affective and normative commitments and no
significant relationship between transformational leadership and continuance
commitment. Significant differences between types of settings (nursing facilities and
“other”) were only observed for organizational commitment and not transformational
leadership.
Summary of the Findings
Transformational leadership was found to significantly correlate with
organizational commitment among DCWs in nonprofit long term care organizations.
This finding supports the existing literature that organizational characteristics such as
leader practices contribute to organizational commitment (Kouzes & Posner, 2012;
Meyer & Allen, 1997). However, one critical aspect of the study hypotheses addressed
organizational commitment within its three dimensions of affective, continuance, and
normative commitment. This is an imperative component of the analysis because
organizational commitment as a job attitude is complex (Liou, 2008; Meyer & Allen,
1997; Morrow & McElroy, 1993). If organizational commitment is analyzed only in its
totality, it ignores the variation of employee relationships with their leaders and
organizations (Meyer & Allen, 1997). Thus, a dimensional view takes this complexity
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 87
into consideration when considering the impact of transformational leadership on
organizational commitment.
Affective commitment represents the emotional component of organizational
commitment (Liou, 2008; Meyer & Allen, 1997; Robbins & Judge, 2012) whereas
normative commitment represents an employee’s sense of obligation to remain with the
organization (Liou, 2008; Meyer & Allen, 1997; Robbins & Judge, 2012). In the study,
transformational leader behaviors were significantly positively related to both affective
commitment and normative commitment. In previous meta-analyses of correlations
between transformational leadership and affective and normative commitment, affective
commitment was shown to have a stronger relationship (Meyer et al., 2002). In this
study, affective and normative commitments were similar in their correlation strengths
(.398 and .395 respectively), although the variances attributable to transformational
leader behaviors was not high (15.8% and 15.6% respectively). This may be related to
the strength of DCW conformity between personal and organizational beliefs and the
emotional attachment this lends to nonprofit missions. It is possible that DCWs who
already have a desire to help others and work in a nonprofit setting feel compelled to
remain in nonprofit settings, and while transformational leader behaviors assist in
increasing affective and normative commitments, they may not be as compelling as the
nonprofit mission itself.
Supervisory support, autonomy, and respect were found to influence high
commitment levels in long term care (Bishop et al., 2008) and DCWs have expressed that
they most desire recognition, respect, rewards, empowerment, and inclusion in decision-
making (Bowers, Esmond, & Jacobson, 2003; Casper & O’Rourke, 2008; Leutz, Bishop
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 88
& Dodson, 2009; Secrest, Iorio & Martz, 2005; Stone, 2004; 2011). All such leader
behaviors are reflected in the five transformational leadership subscales in some fashion,
and the study results illustrated the statistically significant relationship between the
transformational leadership subscales and overall organizational commitment, affective
commitment, and normative commitment. For example, “model the way” exhibits
qualities that show respect for others, “inspire a shared vision” appeals to empowerment
by building goals to achieve a shared vision, “challenge the process” assures that support
exists for DCWs wanting to test new approaches to care, “enable others to act” ensures
that collaborative cultures are created for shared decision-making, and “encourage the
heart” recognizes and rewards DCWs for accomplishments and makes people feel valued.
In total, transformational leadership practices, described by Kouzes & Posner (2012) as
the five practices of exemplary leadership, are based on “mobilizing others to want to
struggle for shared aspirations” (p. 30). The leader/follower relationship is integral to
organizational commitment along the affective and normative commitment dimensions.
Continuance commitment considers the DCWs’ perceptions of costs in leaving
the organization (Liou, 2008; Meyer & Allen, 1997; Robbins & Judge, 2012). Contrary
to initial expectations for this study, there was no significant relationship between
transformational leader behaviors and organizational commitment. Results showed that
the relationship was in fact a slight positive relationship (.021) despite the hypothesized
inverse relationship. However, when looking at the transformational leadership
subscales, a negative relationship existed between “inspire a shared vision” and
continuance commitment. This is contrary to previous research (Dunn, Dastoor, & Sims,
2012). This reveals a potential linkage as to what hierarchy levels DCWs expect to
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 89
communicate the vision. Because immediate supervisors were the target for leader
behavior perception, DCWs may not hold them responsible for sharing the vision, thus
not providing them “credit” for doing so in the survey.
Continuance commitment also takes into account both the sacrifices involved in
leaving an organization as well as the awareness of available job alternatives (Hackett et
al., 1994; Meyer & Allen, 1997). Rather than leader behaviors affecting continuance
commitment, other personal (age, length of employment) or organizational factors
(autonomy, pay) may be more attributable to an understanding of continuance
commitment (Hackett et al., 1994; Meyer & Allen, 1997). While the study revealed that
the median hourly wage of DCWs ($12.00) was higher than the most recent national
report ($10.63), median hourly wage remains lower than the median wage for all U.S.
workers ($16.71) (PHI, 2013b). It is also worth considering that DCWs may feel their
skills in long term care are less transferrable to another organization or industry or they
perceive limited employment alternatives, thus increasing continuance commitment
levels (Meyer et al., 2002). Furthermore, the nonprofit mission may contribute to a
lessening of economic considerations with DCWs, thus reducing their desire to leave for
higher pay. For example, if a nonprofit organization provides desired support for work-
family balance, thus reducing stress for the DCW, higher pay may become less valuable
to the DCW. Each of these considerations are worthy of further exploration and research.
With regard to types of long term care settings, there was support for differences
between service settings for organizational commitment but not transformational
leadership. This may be explained by the reduced level of regulations in senior housing
and home- and community-based services (the “other” category) as compared to nursing
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 90
facilities. DCWs in these settings may have more autonomy and empowerment in their
roles, thus lending to an increase in organizational commitment levels. Furthermore,
because normative commitment includes social identity considerations, the smaller
employee numbers that senior housing and home- and community-based settings employ
may contribute to perceived ease of in-group membership, thus increasing commitment
levels. Because the study participants were employed at multi-level long term care
organizations, transformational leader behaviors may be consistent across types of
settings, thus limiting its influence, whereas employees consistently working in one type
of setting over another more closely identify with those issues and situations occurring in
their own work setting.
The study provided evidence for correlational understanding between leader
behaviors and organizational commitment but should not be construed as inferring
causality (Gerring, 2012; Onwuegbuzie & Daniel, 2002). Limitations of the study
included the purposeful sampling approach with data collection occurring at limited
points in time for each participating site. Furthermore, participants were limited to those
working at the time of data collection. Findings provide validity for the population
studied and may be valuable in understanding multi-level, nonprofit long term care
organizations in the Midwest; however, application to other geographic locations and
organizational capacities should be applied cautiously.
Implications for Action/Recommendations for Further Research
The aim of this study was to gain further understanding about how leader
behaviors influence organizational commitment among DCWs in the nonprofit long term
care industry by providing DCWs an opportunity to voice their perspective and
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 91
advocating on their behalf. The research study was inspired by practical considerations
because DCWs form the core of the long term care industry and the rapidly aging
demographic trends challenge the future availability of DCWs in the provision of long
term care services. Leaders are responsible for creating work environments that develop
and sustain the workforce. Findings of the study can benefit scholarship, practice, and
policy within the long term care industry.
Scholarship
Within scholarship, meta-analysis of transformational leadership has revealed an
influence on organizational commitment in industries other than long term care (Avolio,
2011), and researchers have advocated for further study on transformational leadership in
hierarchical levels other than middle to senior levels ((Avolio, 2011; Heldenbrand &
Simms, 2012). This study responded to this deficiency by focusing on DCWs and their
immediate supervisors. The study provided additional empirical evidence into the
relationship between transformational leadership and organizational commitment as well
as the nonprofit leadership arena.
Recommendation one: Further research is warranted. The current study was
conducted with the purpose of examining the relationship between transformational
leadership and organizational commitment among DCWs in nonprofit long term care
organizations. Study findings were valuable; however, further research is warranted to
evolve the long term care industry’s understanding of the relationship between
transformational leadership and organizational commitment. A larger sample of DCWs
would be helpful to increase the sample sizes of other types of long term care settings
besides nursing facilities. Furthermore, the lack of finding an inverse relationship
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 92
between leadership and continuance commitment does not lessen the need for further
research on the issue of pay in long term care.
Future researchers could take quantitative, qualitative, or mixed-method
approaches to collecting leadership and organizational commitment data. Examining
leader behaviors and organizational commitment through interviews, surveys, and
observation could provide additional insight into successful and exceptional leadership in
long term care. Additionally, following participants for an extended period of time rather
than collecting data at one point time could provide useful for data analysis.
Longitudinal studies may be useful in tracking data over time with long term care
organizations willing to commit to such an endeavor. For example, during the this study,
one organizational leader confidentially shared their organization’s story of initiating
leadership training utilizing the Kouzes & Posner’s (2012) Leadership Challenge Theory.
Conducting research that analyzes leadership training pre- and post- training would be
valuable for the industry.
With respect to the LPI survey instrument (Kouzes & Posner, 2013), Tourangeau
and McGilton (2004) encouraged revision of the LPI to shorten its length for use in
health care to relieve participant burden as well as decrease research costs. Subjectively,
participants in this study commented on the length of the survey, and some participants
did not complete the survey because they did not feel they had the time or could leave
their work, despite encouragement from others. Future researchers may wish to consider
tackling this issue. Other areas of further research on transformational leadership and
organizational commitment could include an analysis of other factors, such as
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 93
demographics, stress, health and well-being, and conflict as they relate to the variables
and a comparison of for-profit and nonprofit long term care organizations.
Industry Practice
Liou (2008) asserted that health care organizations must give more attention to
organizational commitment. Prioritizing an emphasis on commitment can assist leaders
in focusing on antecedents that foster increased organizational commitment, resulting in
increased retention and performance. This study aimed to understand how
transformational leadership may relate to organizational commitment in order to provide
value to leadership as a critical skill in long term care. Changes in long term care, partly
due to health care reform, are demanding more of long term care providers in the
implementation of effective care practices. Such demands can be taxing on both leaders
and DCWs who are instrumental to successful implementation. This study found that
leader behaviors are related to organizational commitment among DCWs. The findings
are useful in considering modifications of operational policies, identifying training and
development needs, and revisiting human resources practices.
Recommendation two: Review operational policies. Leaders would benefit
from collaborating with internal stakeholders to review operational policies. Policies
should reflect the values of the organization. The organization’s vision and mission
should be included in the policies and procedures and be visible to employees
implementing them on a daily basis. Policies can be used to establish standards of
excellence as goals for others to follow. However, operational policies follow a strategic
planning process that takes into consideration the organization’s vision and mission and a
complex set of stakeholders (Bryson, 2011). If a vision and/or mission statement is in
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 94
need of revision, leaders must first address the overall strategic direction. Creating,
communicating, and sharing a compelling (and collective) vision and mission is critical
to engaging employees in their work and appealing to shared aspirations.
Recommendation three: Incorporate leadership development training.
Leadership development training should be considered for continuing education
requirements for supervisors at all levels. Research has shown that leadership skills can
be developed (Avolio, 2011), and a recent qualitative study on coaching as a leader
practice in long term care revealed benefits in communication skills, staff empowerment,
and feedback processes (Cummings et al., 2014). Current education and training
requirements for administrators and managers are not sufficient in addressing leadership
skills development (Dana & Olson, 2007). Supplemental and focused leadership
education and training is needed. There are many external leadership programs, but
many are prohibitive due to financial constraints. Large nonprofit organizations may
benefit from corporate office support for internal leadership development training.
However, smaller independent nonprofit organizations may be more resource
constrained. Thus, leadership skills training must be accessible to supervisors in a
broader context. State and national long term care provider associations are one vehicle
for providing leadership training during highly attended association meetings where
continuing education is offered. For example, this study can be submitted as an
education session at state and national provider associations to advance the research
findings and further encourage leadership development.
Recommendation four: Revisit human resource practices. Oftentimes, human
resource practices are associated with operational policies and exhibit a transactional
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 95
approach to organizational issues. However, many human resource practices are also part
of the organization’s cultural norms. For example, many nonprofit long term care
organizations are faith-based and incorporate prayer into daily practice. Leaders in long
term care can revisit human resource practices to evaluate alignment with the
organization’s vision, mission, and values. Are the values and principles concerning the
way people should be treated consistent with and carried out through human resources
practices and leader behaviors? Leaders can collaborate with others to assess alignment
issues and modify expectations and practices accordingly. Research findings can assist
leaders in understanding which leader behaviors influence outcomes and concentrate
leadership training on a timelier basis. Other organizational tools, such as employee
satisfaction surveys, can be utilized to identify specific areas of concern and direct
training resources appropriately.
Additionally, human resource practitioners and administrators should consider the
communication methods used to share benefits information with employees. In this
study, up to 33% of DCWs indicated that their organization did not offer or they were
unsure if their organization offered benefits such as health insurance, paid vacation, paid
sick time, paid holiday time, and retirement plans. Because continuance commitment
involves benefits as an economic consideration to leaving an organization, it makes sense
that organizations should strive for a goal that 100% of their employees fully understand
the pay and benefit package offered. Furthermore, communication on benefit offerings
should be done on an ongoing basis, rather than just upon hire or at insurance enrollment
timeframes. Utilizing assessment through employee satisfaction surveys is one method
of obtaining employee input on this subject. Other methods might include organization
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 96
websites, paycheck reminders, informational postings in staff areas, reminders at staff
meetings, and direct mailings to employees. As society increasingly moves to electronic
communication methods, it is important to remember that not all DCWs have ready
access to computers and other electronic devices.
Policy
Government reimbursements, regulations, and workforce resources all influence
recruitment and retention in the long term care industry, and compensation in particular
has been shown to directly affect DCWs (Stone, 2004; 2011). Compensation is linked to
continuance commitment and is often the subject of long term care policy aimed at
maintaining current DCW supply. As previously discussed, the aging population is
introducing a demographic trend that will influence the demand for long term care
service, and a quality workforce is required to support the consumers of long term care
services and their informal caregiving networks. This study revealed that leader
behaviors are related to organizational commitment. The findings support the need to
evaluate the content of workforce resources incorporated into policy development.
Recommendation five: Evaluate the content of workforce resources. The
content of workforce resources incorporated into policy development should be
evaluated. Generally, compensation for DCWs is the focus of policy discussion;
however, pay as a component of continuance commitment is only one avenue for
influencing overall organizational commitment, as evidenced by the study findings.
Policymakers must consider other options for tackling the DCW supply challenge.
Policymakers may want to consider including leadership skills as a continuing education
requirement for administrators and other licensed professionals working in long term care
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 97
in positions of supervisory authority. Leadership skills training may also be a
consideration within reimbursement incentives, such as inclusion as a pay for
performance criterion on workforce practices. Even non-monetary incentives, such as
state-level government awards, can be designed to recognize long term care organizations
that include leadership skills development for improving workforce practices and
engaging DCWs as much as possible in planning and executing activities to improve
performance. Study findings can be shared with policymakers, state agencies, and
provider association policy advocates as vehicles for communicating the benefits of
transformational leader behaviors on organizational commitment of DCWs in long term
care organizations.
Summary
The aim of this study was to gain further understanding about how leader
behaviors influence organizational commitment among DCWs in the nonprofit long term
care industry by providing DCWs an opportunity to voice their perspective and
advocating on their behalf. Two research questions were addressed: a) What is the
relationship between transformational leadership and organizational commitment
(affective, continuance, and normative) among direct care workers in nonprofit long term
care organizations? and b) Is there a difference, if any, between types of long term care
settings for transformational leadership and organizational commitment? A quantitative
correlational design study was used to assess the strength of the relationships between the
variables. The study included 322 DCWs employed by nine nonprofit, multi-level long
term care organizations located in the Midwest. The study participants completed a
survey document including the LPI (Kouzes & Posner, 2013) and the TCM (Meyer &
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 98
Allen, 2004) survey instruments and demographic questions. For participants, the
completion of the survey was confidential and anonymous. Findings revealed a
significant positive relationship between transformational leadership and overall
organizational commitment, a significant positive relationship between transformational
leadership and both affective and normative commitment and no significant relationship
between transformational leadership and continuance commitment. Significant
differences between types of settings (nursing facilities and “other”) were only observed
for organizational commitment and not transformational leadership.
The study provided evidence for correlational understanding between leader
behaviors and organizational commitment but should not be construed as inferring
causality (Gerring, 2012; Onwuegbuzie & Daniel, 2002). Limitations of the study
included the purposeful sampling approach with data collection occurring at limited
points in time for each participating site. Furthermore, participants were limited to those
working at the time of data collection conducted onsite at the participating organizations.
Findings provided validity for the population studied and may be valuable in
understanding multi-level, nonprofit long term care organizations in the Midwest;
however, application to other geographic locations and organizational capacities should
be applied cautiously.
The research study was inspired by practical considerations because DCWs form
the core of the long term care industry and demographic trends will challenge the future
availability of DCWs in providing long term care services to aging consumers. Leaders
are responsible for creating work environments that develop and sustain the workforce.
Findings of the study can benefit scholarship, practice, and policy within the long term
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 99
care industry. Within the scholarship arena, this study responded to a research deficiency
by focusing on DCWs and their immediate supervisors. The study provided additional
empirical evidence into the relationship between transformational leadership and
organizational commitment as well as for the nonprofit leadership arena. For the long
term care industry, this study found that leader behaviors are related to organizational
commitment among DCWs. The findings are useful in considering modifications of
operational policies, identifying training and development needs, and revisiting human
resources practices. For policymakers, the findings support the need to evaluate the
content of workforce resources incorporated into policy development. The aging
population is introducing a demographic trend that will influence the demand for long
term care services, and a quality workforce is required to support the consumers of long
term care services and their informal caregiving networks.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 100
References
Alatrista, J., & Arrowsmith, J. (2004). Managing employee commitment in the not-for-
profit sector. Personnel Review, 33(5), 536-
548. http://dx.doi.org/10.1108/00483480410550143
Al-Hussami, M. (2008). A study of nurses’ job satisfaction: The relationship to
organizational commitment, perceived organizational support, transactional
leadership, transformational leadership, and level of education. European Journal
of Scientific Research, 22(2), 286-295.
Al-Hussami, M., Darawad, M., Saleh, A., & Hayajneh, F. A. (2014). Predicting nurses’
turnover intentions by demographic characteristics, perception of health, quality
of work attitudes. International Journal of Nursing Practice, 20(1), 79-88. Doi:
101111/ijn.12124
Allen, N. J., & Meyer, J. P. (2000). Construct validation in organizational behavior
research: The case of organizational commitment. In R. D. Goffin & E. Helmes
(Eds.). Problems and solutions in human assessment: Honoring Douglas N.
Jackson at seventy (pp. 285-314). Norwell, MA: Kluwer Academic Publishers.
Antonakis, J., Avolio, B. J., & Sivasubramaniam, N. (2003). Context and leadership:
An examination of the nine-factor full-range leadership theory using the
multifactor leadership questionnaire. The Leadership Quarterly, 14, 261-
295. http://dx.doi.org/10.1016/S1048-9843(03)00030-4
Avolio, B. J. (2011). Full range leadership development (2nd ed.). Thousand Oaks,
CA: Sage Publications.
Avolio, B. J. & Bass, B. M. (1995). Individual consideration viewed at multiple levels
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 101
of analysis: A multi-level framework for examining the diffusion of
transformational leadership. Leadership Quarterly, 6(2), 199-
218. http://dx.doi.org/10.1016/1048-9843(95)90035-7
Avolio, B. J., Bass, B. M., & Jung, D. I. (1999). Re-examining the components of
transformational and transactional leadership using the multi-factor leadership
questionnaire. Journal of Occupational and Organizational Psychology, 72, 441-
462. http://dx.doi.org/10.1348/096317999166789
Avolio, B. J., Zhu, W., Koh, W., & Puja, B. (2004). Transformational leadership and
organizational commitment: Mediating role of psychological empowerment and
moderating role of structural distance. Journal of Organizational Behavior, 25,
951-968. http://dx.doi.org/10.1002/job.283
Bass, B. M. (1985). Leadership and performance beyond expectations. New York,
NY: Free Press.
Bass, B. M., & Bass, R. (2008). The Bass handbook of leadership: Theory, research &
managerial applications (4th ed.). New York, NY: Free Press.
Bass, B. M., & Riggio, R. E. (2006). Transformational leadership (2nd ed.). Mahweh,
NJ: Lawrence Erlbaum Associates.
Bass, B. M., & Riggio, R. E. (2010). The transformational model of leadership. In G.
R. Hickman (Ed.), Leading organizations: Perspectives for a new era (2nd ed.)
(pp. 76-86). Thousand Oaks, CA: Sage.
Bass, B. M., Waldman, D. A., & Avolio, B. J. (1987). Transformational leadership
and the falling dominoes effect. Group & Organization Studies, 12(1), 73-
87. http://dx.doi.org/10.1177/105960118701200106
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 102
Bear, A. B., & Fitzgibbon, M. A. (2005). Leadership in a not-for-profit world: A mixed
Toolbox. In R. R. Sims & S. A. Quatro (Eds.). Leadership: Succeeding in the
private, public, and not-for-profit sectors (pp. 87-104). Armonk, NY: M.E.
Sharpe.
Becker, H. S. (1960). Notes on the concept of commitment. American Journal of
Sociology, 66, 32-42. http://dx.doi.org/10.1086/222820
Bennis, W. G. (1997). Learning to lead: A workbook on becoming a leader. New York,
NY: Perseus.
Bennis, W. G., & Nanus, B. (1985). Leaders: Strategies for taking charge. New York,
NY: Harper & Row.
Berndt, J. (2012). Ever forward: Identifying effective change leadership in social ministry
organizations. (Doctoral thesis). Bethel University.
Bishop, C. E., Weinberg, D. B., Leutz, W., Dossa, A., Pfefferle, S. G., & Zincavage, R.
M. (2008). Nursing assistants’ job commitment: Effect of nursing home
organizational factors and impact on resident well-being. Gerontologist, 48(1),
36-45. PMID:18694985
Block, S. R. (2001). The history of the discipline. In J. S. Ott (Ed.), The nature
of the nonprofit sector (pp.97-111). Boulder, CO: Westview Press.
Bono, J. E., & Judge, T. A. (2003). Self-concordance at work: Toward understanding the
motivational effects of transformational leaders. Academy of Management
Journal, 46(5), 554-571. http://dx.doi.org/10.2307/30040649
Bowers, B. J., Esmond, S., & Jacobson, N. (2003). Turnover reinterpreted: Cnas talk
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 103
about why they leave. Journal of Gerontological Nursing, 29(3), 36-
43. http://dx.doi.org/10.3928/0098-9134-20030301-09
Bryson, J. M. (2011). Strategic planning for public and nonprofit organizations: A guide
to strengthening and sustaining organizational achievement (4th ed.). San
Francisco, CA: John Wiley & Sons.
Burke, W. W. (2011). Organization change: Theory and practice (3rd ed.). Thousand
Oaks, CA: Sage Publications.
Burns, J. M. (1978). Leadership. New York, NY: Harper & Row.
Bycio, P., Hackett, R. D., & Allen, J. S. (1995). Further assessments of Bass’s (1985)
conceptualization of transactional and transformational leadership. Journal of
Applied Psychology, 80, 468-478. http://dx.doi.org/10.1037/0021-9010.80.4.468
Caspar, S., & O’Rourke, N. (2008). The influence of care provider access to structural
empowerment on individualized care in long-term care facilities. Journal of
Gerontology: Social Sciences, 63B(4), S255-
S265. http://dx.doi.org/10.1093/geronb/63.4.S255
Census Bureau. (n.d.). 2012 national population projections. Retrieved from
http://www.census.gov/population/projections/data/national/2012.html
Center for Health Workforce Studies. (2006). The impact of the aging population on the
health workforce in the United States: Summary of key findings. Washington, DC:
Health Resources and Services Administration. Retrieved from
http://www.albany.edu/news/pdf_files/impact_of_aging_excerpt.pdf
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.).
Hillsdale, NJ: Erlbaum.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 104
Crawford, D. B. (2005). The bases for executive action: A multiple case study of
leadership in the highly regulated long-term health care industry. (Doctoral
dissertation). Regent University School of Business and Leadership.
Creswell, J. W. (2012). Educational research: Planning, conducting, and evaluating
quantitative and qualitative research (4th ed.). Boston, MA: Pearson Education.
Culp, K., Ramey, S., & Karlman, S. (2008). Iowa certified nursing assistants study: Self-
reported ratings of the nursing home work environment. Research in
Gerontological Nursing, 1(2), 87-96. http://dx.doi.org/10.3928/19404921-
20080401-01
Cummings, G., Mallidou, A. A., Masaoud, E., Kumbamu, A., Schalm, C., Laschinger,
H., & Estabrooks, C. A. (2014). On becoming a coach: A pilot intervention study
with managers in long-term care. Health Care Management Review, 39(3), 198-
209. doi:10.1097/HMR.obo13e318294e586
Dall, T. M., Gallo, P. D., Chakrabarti, R., West, T., Semilla, A. P., & Storm, M. V.
(2013). An aging population and growing disease burden will require a large and
specialized health care workforce by 2025. Health Affairs, 32(11), 2013-
2020. http://dx.doi.org/10.1377/hlthaff.2013.0714
Dana, B., & Olson, D. (2007). Effective leadership in long term care: The need and the
opportunity. (American College of Health Care Administrators Position Paper).
Retrieved from
http://www.achca.org/content/pdf/ACHCA_Leadership_Need_and_Opportunity_
Paper_Dana-Olson.pdf
DeChurch, L. A., Hiller, N. J., Murase, T., Doty, D., & Salas, E. (2010). Leadership
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 105
across levels: Levels of leaders and their levels of impact. The Leadership
Quarterly, 21, 1069-1085. http://dx.doi.org/10.1016/j.leaqua.2010.10.009
Decker, F. H., Harris-Kojetin, L. D., & Bercovitz, A. (2009). Intrinsic job satisfaction,
overall satisfaction, and intention to leave the job among nursing assistants in
nursing homes. The Gerontologist, 49(5), 596-610, doi: 10.1093/geront/gnp051
DiMaggio, P. J. & Anheier, H. K. (2001). The sociology of nonprofit organizations and
sectors. In J. S. Ott (Ed.), The nature of the nonprofit sector (pp.274-287).
Boulder, CO: Westview Press.
Donoghue, C., & Castle, N. G. (2009). Leadership styles of nursing home administrators
and their association with staff turnover. The Gerontologist, 49(2), 166-174.
doi:10.1093/geront/gnp021
Downton, J. V. (1973). Rebel leadership: Commitment and charisma in revolutionary
process. New York, NY: Free Press.
Dunn, M. W., Dastoor, B., & Sims, R. L. (2012). Transformational leadership and
organizational commitment: A cross-cultural perspective. Journal of
Multidisciplinary Research, 4(1), 45-59.
Duygulu, S., & Kublay, G. (2011). Transformational leadership training programme for
charge nurses. Journal of Advanced Nursing, 67(3), 633-
642. http://dx.doi.org/10.1111/j.1365-2648.2010.05507.x
Eaton, S. C. (2001). What a difference management makes: Nursing staff turnover
variation within a single labor market. In Abt Associates (Eds.). Appropriateness
of minimum nurse staffing ratios in nursing homes (pp. 5-1 – 5-64). Phase II Final
Report to Congress. Washington, DC: Department of Health and Human Services.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 106
Emery, C. R., & Barker, K. J. (2007). The effect of transactional and transformational
leadership styles on the organizational commitment and job satisfaction of
customer contact personnel. Journal of Organizational Culture, Communication
and Conflict, 11(1), 77-90.
Felkins, P. K., & Croteau-Chonka, C. C. (2014). The nonprofit factor: Gathering at the
table for the common good. New York, NY: Hampton Press.
Forbes-Thompson, S., & Gessert, C. E. (2006). Nursing homes and suffering: Part of the
problem or part of the solution? The Journal of Applied Gerontology, 25(3), 234-
251. doi:10.1177/0733464806288561
Freeborough, R. E. (2013). Exploring the affect of transformational leadership on
nonprofit leader engagement and commitment. (Doctoral dissertation). Capella
University.
Frumkin, P. (2002). On being nonprofit: A conceptual and policy primer. Cambridge,
MA: Harvard University Press.
Galaskiewicz, J., & Bielefeld, W. (2001). Nonprofit organizations in an age of
uncertainty. In J. S. Ott (Ed.), The nature of the nonprofit sector (pp.297-310).
Boulder, CO: Westview Press.
Gastwirth, J. L., Gel, Y. R., & Miao, W. (2009). The impact of Levene’s test of equality
of variances in statistical theory and practice. Statistical Science, 24(3), 343-360,
doi:10.1214/09-STS301
Gerring, J. (2012). Social science methodology: A unified framework (2nd ed.). New
York, NY: Cambridge University Press.
Godwin, J. L., & Neck, C. P. (1998). Desired transformational leadership behaviors in a
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 107
religious organization: Analysis by hierarchical organizational level. International
Journal of Organization Theory & Behavior, 1(2), 163-179.
Goleman, D. (2013). The focused leader: How effective executives direct their own – and
their organizations’ – attention. Harvard Business Review, 91(12), 50-60.
Hackett, R. D., Bycio, P., & Hausdorf, P. A. (1994). Further assessments of Meyer and
Allen’s (1991) three-component model of organizational commitment. Journal of
Applied Psychology, 79(1), 15-23. http://dx.doi.org/10.1037/0021-9010.79.1.15
Haslam, S. A., Reicher, S. D., & Platow, M. J. (2011). The new psychology of leadership:
Identity, influence and power. New York, NY: Psychology Press.
Heldenbrand, L., & Simms, M. S. (2012). Missing link: integrated individual leadership
development, employee engagement, and customer value-added improvement.
Performance Improvement, 51(2), 28-35. http://dx.doi.org/10.1002/pfi.21247
Hemphill, J. F. (2003). Interpreting the magnitudes of correlation coefficients. American
Psychologist, 58(1), 78-80, doi:10.1037/0003-066X.58.1.78
Iowa Direct Care Worker Advisory Council. (2012). Costs of turnover in the direct care
workforce. Des Moines, IA: Iowa Department of Public Health. Retrieved from
http://www.idph.state.ia.us/directcare/Council.aspx
Jaros, S. (2007). Meyer and Allen model of organizational commitment: Measurement
issues. Icfai Journal of Organizational Behavior, 4(4), 7-25.
Kim, J., Wehbi, N., DelliFraine, J. L., & Brannon, D. (2013). The joint relationship
between organizational design factors and HR practice factors on direct care
workers’ job satisfaction and turnover intent. Health Care Management Review,
1-11, doi: 10.1097/HMR.0b013e31828c8b8f
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 108
Kouzes, J. M., & Posner, B. Z. (1988). The leadership challenge: How to get
extraordinary things done in organizations. San Francisco, CA: Jossey-Bass
Publishers.
Kouzes, J. M., & Posner, B. Z. (2000). Leadership practices inventory: Psychometric
properties. Retrieved from
http://www.leadershipchallenge.com/UserFiles/lc_jb_psychometric_properti.pdf
Kouzes, J. M., & Posner, B. Z. (2002). The leadership practices inventory: Theory and
evidence behind the five practices of exemplary leaders. Retrieved from
http://www.leadershipchallenge.com/UserFiles/lc_jb_appendix.pdf
Kouzes, J. M., & Posner, B. Z. (2012). The leadership challenge: How to make
extraordinary things happen in organization (5th ed.). San Francisco, CA: Jossey-
Bass Publishers.
Kouzes, J. M., & Posner, B. Z. (2013). Leadership practices inventory: Observer (4th
ed.). San Francisco, CA: Wiley.
Kowalski, C. J. (1972). On the effects of non-normality on the distribution of the sample
product-moment correlation coefficient. Journal of the Royal Statistical Society:
Series C (Applied Statistics), 21(1), 1-12.
Lambert, E., Kelley, T., & Hogan, N. (2013). The association of occupational stressors
with different forms of organizational commitment among correctional staff.
American Journal of Criminal Justice. 38(3), 480-501. doi:10.1007/s12103-012-
9183-1
Lee, D., Coustasse, A., & Sikula Sr., A. (2011). Transformational leadership and
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 109
workplace injury and absenteeism: Analysis of a national nursing assistant survey.
Health Care Management Review, 36(4), 380-387.
doi:10.1097/HMR.0b013e3182100bf7
Leutz, W., Bishop, C. E., & Dodson, L. (2009). Role for a labor-management partnership
in nursing home person-centered care. The Gerontologist, 50(3), 340-351. doi:
10.1093/geront/gnp123
Liou, S. (2008). An analysis of the concept of organizational commitment. Nursing
Forum, 43(3), 116-125. http://dx.doi.org/10.1111/j.1744-6198.2008.00103.x
Liu, L., Liu, W., & Wang, J. (2011). Work autonomy of certified nursing assistants in
long-term care facilities: Discrepant perceptions between nursing supervisors and
certified nursing assistants. Journal of the American Medical Directors
Association, 12(7), 524-534. http://dx.doi.org/10.1016/j.jamda.2010.05.006
Lumley, T., Diehr, P., Emerson, S., & Chen, L. (2002). The importance of the normality
assumption in large public health data sets. Annual Review Public Health, 23,
151-169. doi:10.1146/annurev.publheath.23.100901.140546
Lutfiyya, M. N., Gessert, C. E ., & Lipsky, M. S. (2013). Nursing home quality: A
comparative analysis using CMS nursing home compare data to examine
differences between rural and nonrural facilities. Journal of the American Medical
Directors Association, 14(8), 593-
8. http://dx.doi.org/10.1016/j.jamda.2013.02.017
Marotta, J. (2010). Leadership, emotional intelligence, and quality care in long-term care
facilities. Doctoral dissertation). Retrieved from ProQuest Dissertation Database.
(UMI Number: 3441253).
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 110
Mathieu, J. E., & Zajac, D. (1990). A review and meta-analyses of the antecedents,
correlates, and consequences of organizational commitment. Psychological
Bulletin, 108, 171-194. http://dx.doi.org/10.1037/0033-2909.108.2.171
McGillis-Hall, L., McGilton, K. S., Krejci, J., Pringle, D., Johnston, E., Fairley, L., &
Brown, M. (2005). Enhancing the quality of supportive supervisory behavior in
long-term care facilities. Journal of Nursing Administration, 35(4), 181-187.
McMurray, A. J., Pirola-Merlo, A., Sarros, J. C., & Islam, M. M. (2010). Leadership,
climate, psychological capital, commitment, and wellbeing in a non-profit
organization. Leadership and Organization Development Journal, 31(5), 436-
457. http://dx.doi.org/10.1108/01437731011056452
Meyer, J. P., & Allen, N. J. (1991). A three-component conceptualization of
organizational commitment. Human Resource Management Review, 1, 61-
89. http://dx.doi.org/10.1016/1053-4822(91)90011-Z
Meyer, J. P., & Allen, N. J. (1997). Commitment in the workplace: Theory, research and
application. Thousand Oaks, CA: Sage Publications.
Meyer, J. P., & Allen, N. J. (2004). TCM employee commitment survey academic users
guide 2004. Ontario: University of Western Ontario.
Meyer, J., Becker, T., & Van Dick, R. (2006). Social identities and commitments at
work: Toward an integrative model. Journal of Organizational Behavior, 27, 665-
683. http://dx.doi.org/10.1002/job.383
Meyer, J. P., Stanley, D. J., Herscovitch, L., & Topolnytsky, L. (2002). Affective,
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 111
continuance, and normative commitment to the organization: A meta-analysis of
antecedents, correlates, and consequences. Journal of Vocational Behavior, 61,
20-52. http://dx.doi.org/10.1006/jvbe.2001.1842
Morrow, P. C., & McElroy, J. C. (1993). Introduction: Understanding and managing
loyalty in a multi-commitment world. Journal of Business Research, 26(1), 1-
3. http://dx.doi.org/10.1016/0148-2963(93)90038-Q
Mowday, R. T., Porter, L. W., & Steers, R. (1982). Organizational linkages: The
psychology of commitment, absenteeism, and turnover. San Diego, CA:
Academic Press.
Mukamel, D. B., Spector, W. D., Limcangco, R., Wang, Y., Feng, Z, & Mor, V. (2009).
The costs of turnover in nursing facilities. Medical Care, 47(10), 1039-1045.
doi:10.1097/MLR.0b013e3181a3cc62
Northouse, P. G. (2007). Leadership theory and practice (4th ed.). Thousand Oaks, CA:
Sage Publications.
Onwuegbuzie, A. J., & Daniel, L. G. (2002). Uses and misuses of the correlation
coefficient. Research in the Schools, 9(1), 73-90.
Ott, J. S. (Ed.). (2001). The nature of the nonprofit sector. Boulder, CO: Westview Press.
Palotta, D. (2008). Uncharitable: How restraints on nonprofits undermine their potential.
Medford, MA: Tufts University Press.
Paraprofessional Health Institute (PHI). (2011, February). Who are direct-care workers?
(Facts Brief 3). New York, NY: PHI. Retrieved from PHI website:
http://www.phinational.org/sites/phinational.org/files/clearinghouse/PHI%20Facts
%203.pdf
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 112
Paraprofessional Health Institute (PHI). (2013a, February). Occupational projections for
direct-care workers 2010-2020. (Facts Brief 1). New York, NY: PHI. Retrieved
from PHI website:
http://phinational.org/sites/phinational.org/files/phi_factsheet1update_singles_2.p
df
Paraprofessional Health Institute (PHI). (2013b, November). America’s direct-care
workforce. (Facts Brief 3). New York, NY: PHI. Retrieved from PHI website:
http://phinational.org/sites/phinational.org/files/phi-facts-3.pdf
Pennington, P., Townsend, C., & Cummins, R. (2003). The relationship of leadership
practices to culture. Journal of Leadership Education, 2(1), 27-
44. http://dx.doi.org/10.12806/V2/I1/RF2
Podsakoff, P. M., MacKenzie, S. B., & Bommer, W. H. (1996). Transformational leader
behaviors and substitutes for leadership as determinants of employee satisfaction,
commitment, trust, and organizational citizenship behaviors. Journal of
Management, 22(2), 259-298. http://dx.doi.org/10.1016/S0149-2063(96)90049-5
Podsakoff, P. M., MacKenzie, S. B., Moorman, R. H., & Fetter, R. (1990).
Transformational leader behaviors and their effects on followers’ trust in leader,
satisfaction, and organizational citizenship behaviors. Leadership Quarterly, 1,
107–142. http://dx.doi.org/10.1016/1048-9843(90)90009-7
Pratt, J. R. (2010). Long-term care: Managing across the continuum, (3rd ed.). Sudbury,
MA: Jones and Bartlett.
Qiao, K., Khilji, S., & Wang, X. (2009). High-performance work systems, organizational
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 113
commitment, and the role of demographic features in the People's Republic of
China. International Journal of Human Resource Management, 20(11), 2311-
2330. doi:10.1080/09585190903239682
Riggio, R. E., & Orr, S. S. (Eds.). (2004). Improving leadership in nonprofit
organizations. San Francisco, CA: Jossey-Bass.
Robbins, S. P., & Judge, T. A. (2012). Essentials of organizational behavior (11th ed.).
Upper Saddle River, NJ: Prentice Hall.
Robnett, R. H., & Chop, W. C. (2010). Gerontology for the health care professional (2nd
ed.). Sudbury, MA: Jones and Bartlett.
Rosen, J., Stiehl, E. M., Mittal, V., & Leana, C. R. (2011). Stayers, leavers, and switchers
among CNAs in nursing homes: A longitudinal investigation of turnover intent,
staff retention, and turnover. The Gerontologist, 51(5), 597-
609. http://dx.doi.org/10.1093/geront/gnr025
Salamon, L. M., Sokolowski, S. W., & Geller, S. L. (2012). Holding the fort: Nonprofit
employment during a decade of turmoil. (Nonprofit Employment Bulletin No.
39). Johns Hopkins University Center for Civil Society Studies. Retrieved
from http://ccss.jhu.edu/wp-
content/uploads/downloads/2012/01/NED_National_2012.pdf
Scott, J. T. (2001). Voluntary sector. In J. S. Ott (Ed.), The nature of the nonprofit sector
(pp. 40-45). Boulder, CO: Westview Press.
Scott, J., Vojir, C., Jones, K., & Moore, L. (2005). Assessing nursing homes’ capacity to
create and sustain improvement. Journal of Nursing Care Quality, 20(1), 36-
42. http://dx.doi.org/10.1097/00001786-200501000-00007
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 114
Seavey, D. (2004). The cost of turnover in long-term care. Washington, DC: Better Jobs
Better Care. Retrieved from
http://www.leadingage.org/uploadedFiles/Content/About/Center_for_Applied_Re
search/Center_for_Applied_Research_Initiatives/Cost_Frontline_Turnover.pdf
Secrest, J., Iorio, D. H., & Martz, W. (2005). The meaning of work for nursing assistants
who stay in long-term care. Journal of Clinical Nursing, 14, 90-
97, doi:10.1111/j.1365-2702.2005.01282.x
Smith, D. H. (2001). The impact of the voluntary sector on society. In J. S. Ott (Ed.), The
nature of the nonprofit sector (pp.79-87). Boulder, CO: Westview Press.
Smith, K., & Baughman, R. (2007, September). Caring for America’s aging population:
A profile of the direct-care workforce. Monthly Labor Review, 20-26.
Stearns, S. C., & D’Arcy, L. P. (2008). Staying the course: Facility and profession
retention among nursing assistants in nursing homes. Journal of Gerontology:
SOCIAL SCIENCES, 63B(3), S113-
S121. http://dx.doi.org/10.1093/geronb/63.3.S113
Stone, R. (2004). The direct care worker: The third rail of home care policy. Annual
Review of Public Health, 25, 521-
537. http://dx.doi.org/10.1146/annurev.publhealth.25.102802.124343
Stone, R. (2011). Long-term care for the elderly. Washington, DC: The Urban Institute.
Stryker-Gordon, R. (1979). Minnesota study suggests means of reducing turnover rates in
nursing homes. Journal of Nursing Administration, 9(4), 17-
20. http://dx.doi.org/10.1097/00005110-197904010-00003
Teal, C. (2002). Direct care workers – number one quality indicator in long-term care: A
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 115
consumer’s perspective [Commentary]. North Carolina Medical Journal, 63(2),
102-105.
Tourangeau, A. E., & McGilton, K. (2004). Measuring leadership practices of nurses
using the leadership practices inventory. Nursing Research, 53(3), 182-
189. http://dx.doi.org/10.1097/00006199-200405000-00005
Tourish, D. (2013). The dark side of transformational leadership: A critical perspective.
New York, NY: Routledge.
Williams, L. J., & Hazer, J. T. (1986). Antecedents and consequences of satisfaction and
commitment in turnover models: A reanalysis using latent variable structural
equation methods. Journal of Applied Psychology, 71(2), 219-231.
http://dx.doi.org/10.1037/0021-9010.71.2.219
Yukl, G. (1999). An evaluation of conceptual weaknesses in transformational and
charismatic leadership theories. Leadership Quarterly, 10(2), 285-
305. http://dx.doi.org/10.1016/S1048-9843(99)00013-2
Yukl, G. (2006). Leadership in organizations (6th ed.). Upper Saddle River, NJ: Prentice
Hall.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 116
Appendix A
IRB#: 14-17015 Questionnaire Number: _________ Study Site Number: ____________
Leadership and Organizational Commitment: The Direct Care Worker Perspective
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 117
NOTE: Do NOT write your name or any identifying information on this form. This is to maintain anonymity and confidentiality to the survey process. Thank you!
Leadership Instructions: You are being asked to assess leadership behaviors for your direct/immediate supervisor. When selecting your response to each statement:
• Be realistic about the extent to which this person actually engages in the behavior.
• Be as honest and accurate as you can be.
• DO NOT answer in terms of how you would like to see this person behave or in terms of how you think he or she should behave.
• DO answer in terms of how this person typically behaves on most days, on most projects, and with most people.
• Be thoughtful about your responses. For example, giving this person 10s on all
items is most likely not an accurate description of his or her behavior. Similarly, giving someone all 1s or 5s is most likely not an accurate description either. Most people will do some things more or less often than they do other things.
• If you feel that a statement does not apply, it’s probably because you don’t see or
experience the behavior. That means this person does not frequently engage in the behavior, at least around you. In that case, assign a rating of 3 or lower.
For each statement, decide on a response and then record the corresponding number in the box to the right of the statement. After you have responded to all thirty statements, go back through one more time to make sure you have responded to each statement. Every statement must have a rating. The Rating Scale runs from 1 to 10. Choose the number that best applies to each statement. Rating Scale 1- Almost Never 3-Seldom 5-Occasionally 7-Fairly Often 9-Very Frequently 2-Rarely 4-Once in a While 6-Sometimes 8-Usually 10-Almost Always
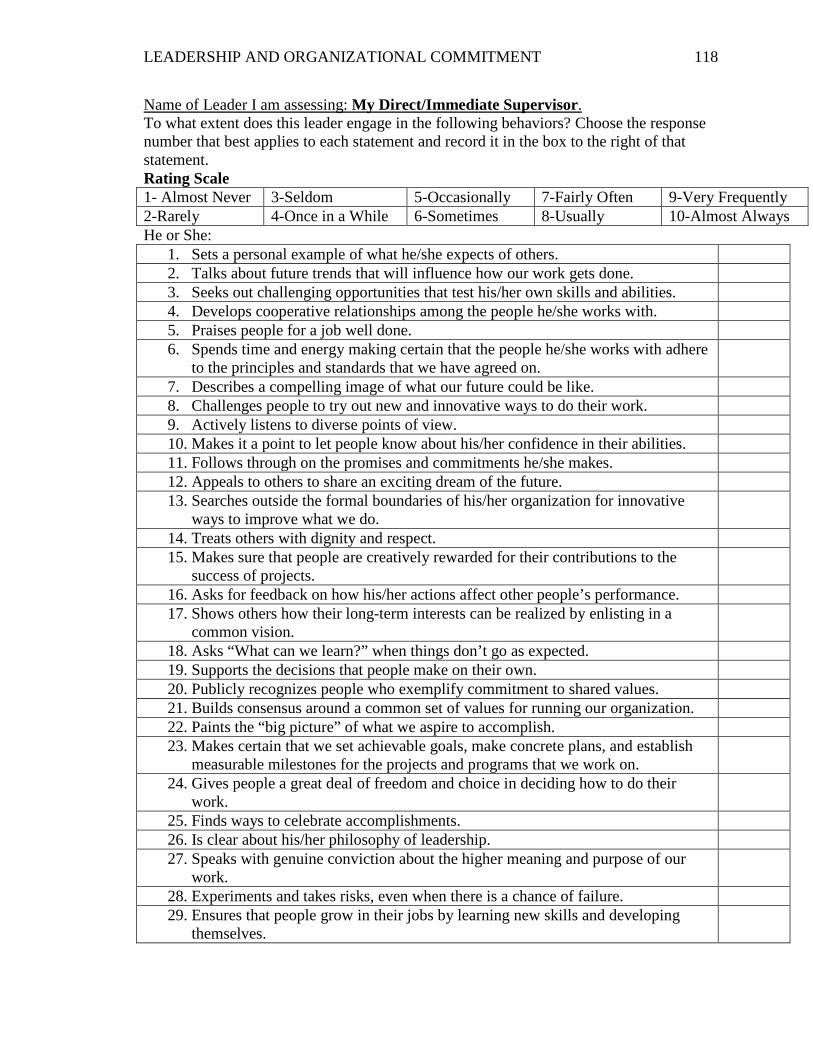
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 118
Name of Leader I am assessing: My Direct/Immediate Supervisor. To what extent does this leader engage in the following behaviors? Choose the response number that best applies to each statement and record it in the box to the right of that statement. Rating Scale 1- Almost Never 3-Seldom 5-Occasionally 7-Fairly Often 9-Very Frequently 2-Rarely 4-Once in a While 6-Sometimes 8-Usually 10-Almost Always He or She:
1. Sets a personal example of what he/she expects of others. 2. Talks about future trends that will influence how our work gets done. 3. Seeks out challenging opportunities that test his/her own skills and abilities. 4. Develops cooperative relationships among the people he/she works with. 5. Praises people for a job well done. 6. Spends time and energy making certain that the people he/she works with adhere
to the principles and standards that we have agreed on.
7. Describes a compelling image of what our future could be like. 8. Challenges people to try out new and innovative ways to do their work. 9. Actively listens to diverse points of view. 10. Makes it a point to let people know about his/her confidence in their abilities. 11. Follows through on the promises and commitments he/she makes. 12. Appeals to others to share an exciting dream of the future. 13. Searches outside the formal boundaries of his/her organization for innovative
ways to improve what we do.
14. Treats others with dignity and respect. 15. Makes sure that people are creatively rewarded for their contributions to the
success of projects.
16. Asks for feedback on how his/her actions affect other people’s performance. 17. Shows others how their long-term interests can be realized by enlisting in a
common vision.
18. Asks “What can we learn?” when things don’t go as expected. 19. Supports the decisions that people make on their own. 20. Publicly recognizes people who exemplify commitment to shared values. 21. Builds consensus around a common set of values for running our organization. 22. Paints the “big picture” of what we aspire to accomplish. 23. Makes certain that we set achievable goals, make concrete plans, and establish
measurable milestones for the projects and programs that we work on.
24. Gives people a great deal of freedom and choice in deciding how to do their work.
25. Finds ways to celebrate accomplishments. 26. Is clear about his/her philosophy of leadership. 27. Speaks with genuine conviction about the higher meaning and purpose of our
work.
28. Experiments and takes risks, even when there is a chance of failure. 29. Ensures that people grow in their jobs by learning new skills and developing
themselves.
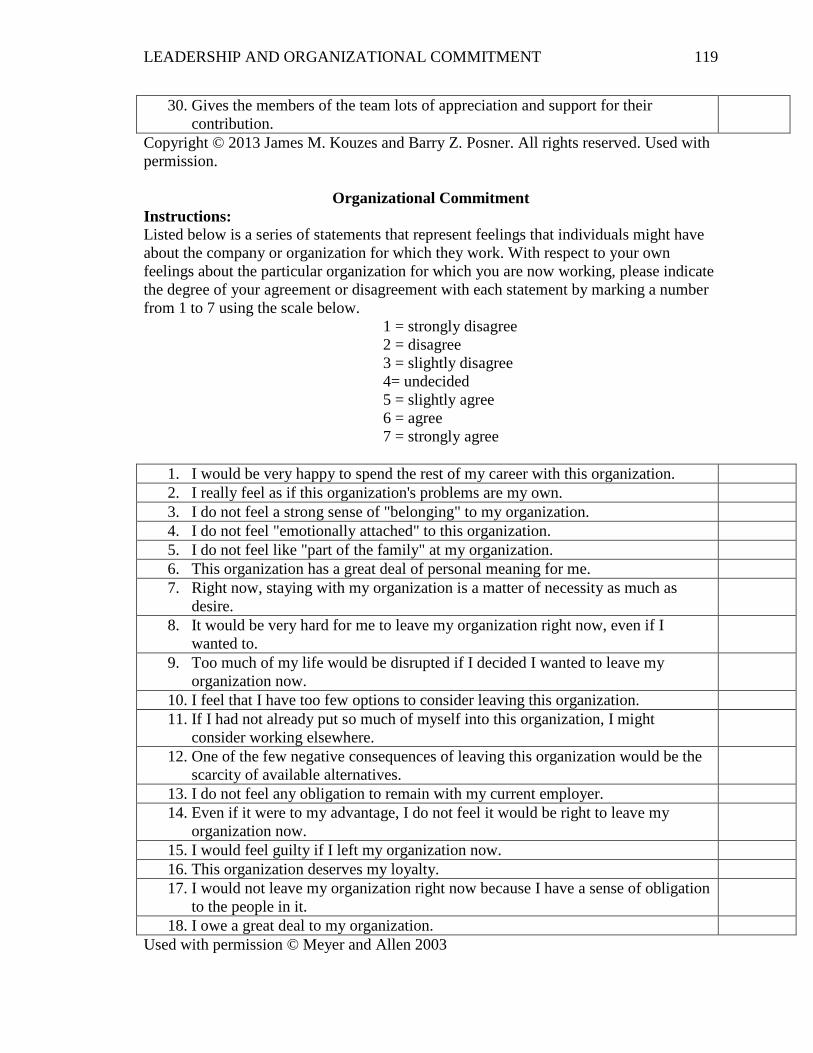
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 119
30. Gives the members of the team lots of appreciation and support for their contribution.
Copyright © 2013 James M. Kouzes and Barry Z. Posner. All rights reserved. Used with permission.
Organizational Commitment Instructions: Listed below is a series of statements that represent feelings that individuals might have about the company or organization for which they work. With respect to your own feelings about the particular organization for which you are now working, please indicate the degree of your agreement or disagreement with each statement by marking a number from 1 to 7 using the scale below.
1 = strongly disagree 2 = disagree 3 = slightly disagree 4= undecided 5 = slightly agree 6 = agree 7 = strongly agree
1. I would be very happy to spend the rest of my career with this organization. 2. I really feel as if this organization's problems are my own. 3. I do not feel a strong sense of "belonging" to my organization. 4. I do not feel "emotionally attached" to this organization. 5. I do not feel like "part of the family" at my organization. 6. This organization has a great deal of personal meaning for me. 7. Right now, staying with my organization is a matter of necessity as much as
desire.
8. It would be very hard for me to leave my organization right now, even if I wanted to.
9. Too much of my life would be disrupted if I decided I wanted to leave my organization now.
10. I feel that I have too few options to consider leaving this organization. 11. If I had not already put so much of myself into this organization, I might
consider working elsewhere.
12. One of the few negative consequences of leaving this organization would be the scarcity of available alternatives.
13. I do not feel any obligation to remain with my current employer. 14. Even if it were to my advantage, I do not feel it would be right to leave my
organization now.
15. I would feel guilty if I left my organization now. 16. This organization deserves my loyalty. 17. I would not leave my organization right now because I have a sense of obligation
to the people in it.
18. I owe a great deal to my organization. Used with permission © Meyer and Allen 2003
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 120
Demographic Information
Instructions: Please answer the following questions based on the options provided by placing a checkmark or X for your answer. All answers will remain confidential and will not be used to identify you, thus providing you anonymity in your responses. If you have any questions about any of the items, please ask the researcher.
What is your gender? ☐Female ☐Male What is your age? ____________ (This information will be used to understand the average age of direct care workers in the study. It will NOT be used to identify you or others in the study.) What is your ethnicity? ☐White ☐African/Black ☐Hispanic ☐American Indian ☐Asian ☐Other (specify) ____________________________ Have you ever served in the U.S. military? ☐Yes ☐No What is your highest level of formal education (if you have education in another country, please rate according to the option that best represents education levels in your country)? ☐Elementary School ☐Middle School ☐High School/GED ☐College/University with undergraduate degree ☐College/University with a graduate degree
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 121
What of the following best describes your relationship status? ☐Married ☐Single, never married ☐Single, but living with a significant other ☐Separated ☐Divorced ☐Widowed ☐In a domestic partnership or civil union Is English your first language? ☐Yes ☐No What is your length of employment at this organization? ☐Less than one year ☐1 to 3 years ☐4 to 6 years ☐7 to 9 years ☐More than 10 years What is your total time of experience working in long term care, with ANY employer? ☐Less than one year ☐1 to 5 years ☐6 to 10 years ☐11 to 15 years ☐16 to 20 years ☐21 to 25 years ☐More than 25 years What is your hourly wage? ___________________ (This information will be used to understand the average wage of direct care workers in the study. It will NOT be used to identify you or others in the study.) Are you satisfied with your pay at its current level? ☐Extremely satisfied ☐Somewhat satisfied ☐Somewhat dissatisfied ☐Extremely dissatisfied Do you belong to a union at your workplace? ☐Yes ☐No
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 122
How would you describe your yearly income? ☐Under $5000 ☐$5001-$10,000 ☐$10,001-$15,000 ☐$15,001-$20,000 ☐$20,001-25,000 ☐$25,001-30,000 ☐Over $30,000 Do you receive any income from Social Security? ☐Yes ☐No Do you receive any government assistance, such as Medicaid, food assistance, or utility (gas/fuel) assistance? ☐Yes ☐No Do you rent or own the place where you live? ☐Rent ☐Own ☐Neither, I am living with someone but do not pay rent Do you have more than one job? ☐Yes ☐No Does your employer provide health insurance benefits? ☐Yes ☐No ☐ I do not know How much do you pay in health insurance premiums? ☐Less than $100 per month ☐$101-$200 per month ☐$201-$300 per month ☐$301-$400 per month ☐$401-$500 per month ☐Over $500 per month ☐ I do not have health insurance ☐ I have health insurance, but not through this organization
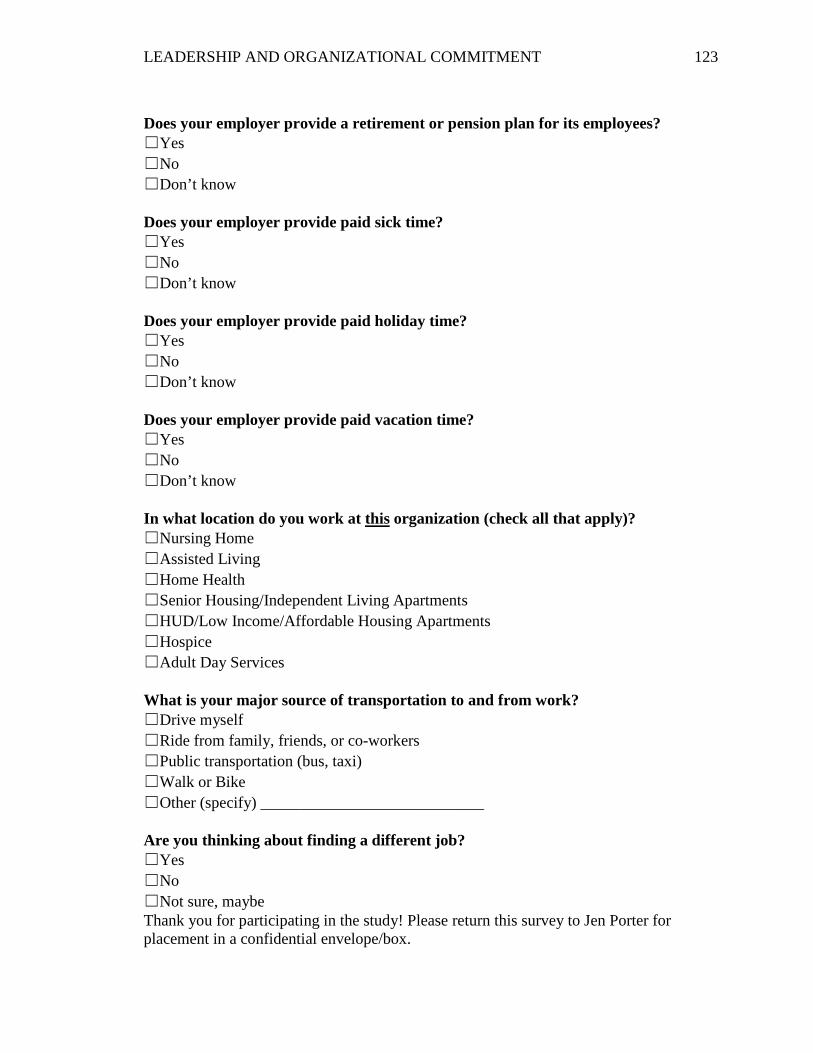
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 123
Does your employer provide a retirement or pension plan for its employees? ☐Yes ☐No ☐Don’t know Does your employer provide paid sick time? ☐Yes ☐No ☐Don’t know Does your employer provide paid holiday time? ☐Yes ☐No ☐Don’t know Does your employer provide paid vacation time? ☐Yes ☐No ☐Don’t know In what location do you work at this organization (check all that apply)? ☐Nursing Home ☐Assisted Living ☐Home Health ☐Senior Housing/Independent Living Apartments ☐HUD/Low Income/Affordable Housing Apartments ☐Hospice ☐Adult Day Services What is your major source of transportation to and from work? ☐Drive myself ☐Ride from family, friends, or co-workers ☐Public transportation (bus, taxi) ☐Walk or Bike ☐Other (specify) ____________________________ Are you thinking about finding a different job? ☐Yes ☐No ☐Not sure, maybe Thank you for participating in the study! Please return this survey to Jen Porter for placement in a confidential envelope/box.
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 124
IRB#: 14-17015 Study Site Number: ____________
Study Site Administrator Site Information
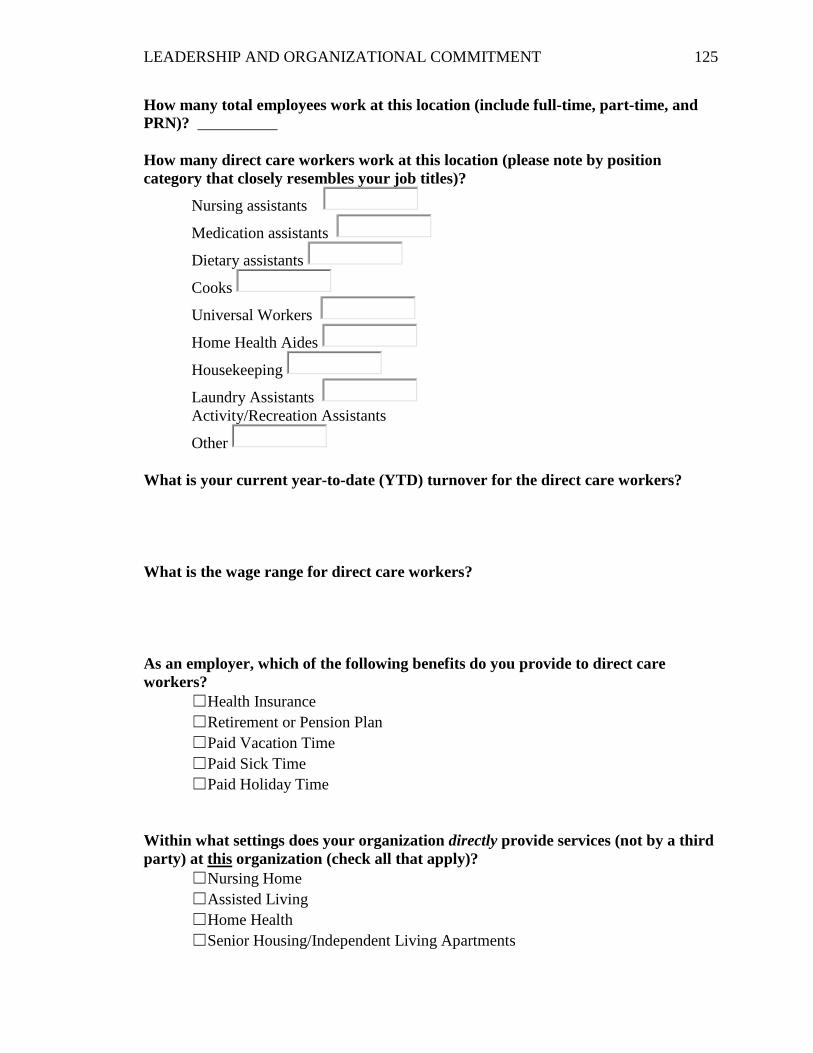
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 125
How many total employees work at this location (include full-time, part-time, and PRN)? __________
How many direct care workers work at this location (please note by position category that closely resembles your job titles)?
Nursing assistants
Medication assistants
Dietary assistants
Cooks
Universal Workers
Home Health Aides
Housekeeping
Laundry Assistants Activity/Recreation Assistants
Other What is your current year-to-date (YTD) turnover for the direct care workers? What is the wage range for direct care workers? As an employer, which of the following benefits do you provide to direct care workers?
☐Health Insurance ☐Retirement or Pension Plan ☐Paid Vacation Time ☐Paid Sick Time ☐Paid Holiday Time
Within what settings does your organization directly provide services (not by a third party) at this organization (check all that apply)?
☐Nursing Home ☐Assisted Living ☐Home Health ☐Senior Housing/Independent Living Apartments
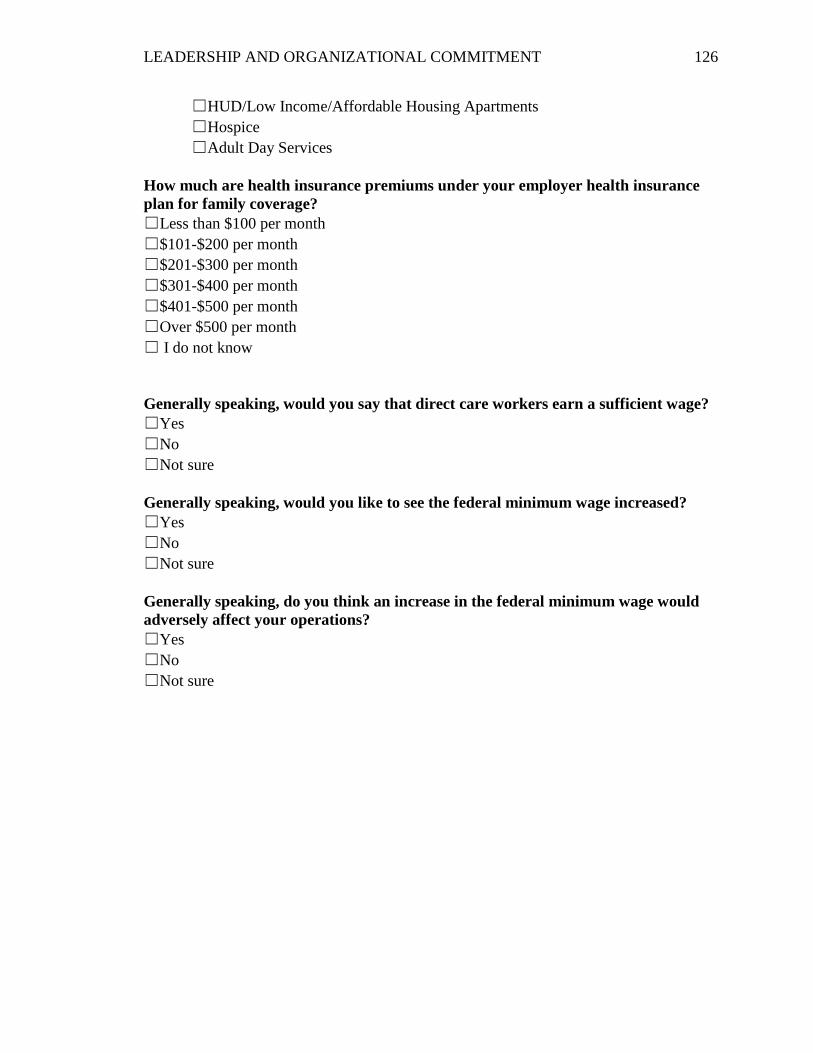
LEADERSHIP AND ORGANIZATIONAL COMMITMENT 126
☐HUD/Low Income/Affordable Housing Apartments ☐Hospice ☐Adult Day Services
How much are health insurance premiums under your employer health insurance plan for family coverage? ☐Less than $100 per month ☐$101-$200 per month ☐$201-$300 per month ☐$301-$400 per month ☐$401-$500 per month ☐Over $500 per month ☐ I do not know
Generally speaking, would you say that direct care workers earn a sufficient wage? ☐Yes ☐No ☐Not sure Generally speaking, would you like to see the federal minimum wage increased? ☐Yes ☐No ☐Not sure Generally speaking, do you think an increase in the federal minimum wage would adversely affect your operations? ☐Yes ☐No ☐Not sure





























