Embed Size (px)
Citation preview

Eur Respir J 1990, 3, 509--514
The relationship between neck circumference, radiographic pharyngeal anatomy, and the obstructive sleep apneoa
syndrome
R.J.O. Davies, J.R. Stradling
The relationship between neck circumference, radiographic pharyngeal anatomy, and the obstructive sleep apneoa syndrome. RJ.O. Davies, JR. Stradling.
The Sleep Clinic, Osier Chest Unit, Churchill Hospilal, Headington, Oxford OX3 7U, UK.
ABSTRACT: We have studied the predictive Importance of neck circumference, obesity, and several radiographic pharyngeal dimensions for obstructive sleep apnoea (OSA), In 66 patients. OSA was quantified as the mean hourly number of >4% dips in arterial oxygen saturation during sleep. Neck circumference (correlation coefficient (r)=0.63, 95% confidence Interval (C.I.) 0.4~.76), obesity Index (r=0.54, 95% C.I. 0.39~.69), hyoid position (r=0.40, 95% C.I. 0.17-0.59), soft palate length (r=0.31, 95% C.I. 0.08-0.51), and hard palate-to-spine angle (r=0.29, 95% C.I. 0.0~.49), correlated significantly with saturation dips in single regression analysis. In stepwlse multiple linear regression analysis (saturation dip rate as the dependant variable), only neck size and rctroglossai space were significant independent correlates (total r 2=0.42, 95% C.I. 0.22-0.61, p<O.OOOl). We conclude that the relationships between general obesity, hyoid position, soft palate length, and OSA are probably secondary to variation in neck circumference.
Correspondence: Dr R.J.O. Davies, The Sleep Clinic, Osier Chest Unit, Churchill Hospital, Headington, Oxford OX3 7U, UK.
Keywords: Neck; obesity; obstructive sleep apnoea syndrome; pharynx; radiology.
Received: September 30, 1989; accepted January 26, 1990.
Eur Respir ]., 1990, 3, 509-514.
In man, general obesity has been thought the single most important risk factor for obstructive sleep apnoea (OSA) [1). However, OSA patients also have anatomical cranial and pharyngeal abnormalities. Among these are bony features such as an elongated lower face [2], and an acute cranial base flexion [3]; as well as soft tissue changes which include a narrow retroglossal airway [4-7), a low set hyoid bone [3, 5-7], and a long sofl palate [2, 3, 5, 8]. Mass loading of the upper airway to simulate obesity reduces the calibre of the oropharynx, leading to airway obstruction in an animal model [9], and OSA patients have more fat deposited around the collapsing pharyngeal segment than do weight matched controls [10). In this study we have assessed the predictive value of neck obesity (assessed by measuring neck circumference), general obesity, and radiographic pharyngeal dimensions for OSA in a sleep clinic population. To test the hypothesis that small changes in head flexion during pharyngeal radiography can produce large variations in some of the pharyngeal dimensions mentioned above, we imaged a group of normals in varying head postures.
Methods
The study population consisted of 66 patients (52 male, 14 female) referred for the investigation of sleep
disorders (snoring, sleepiness, and possible OSA). Each underwent clinical examination, lateral pharyngeal radiography, and an eight hour overnight sleep study. The presence of OSA (quantified as the number of >4% arterial oxygen saturation dips per hour of sleep) was then correlated with radiographic pharyngeal measurements, obesity, and neck size.
Clinical examination
All subjects underwent full general medical examination including measurement of neck circumference at the level of the cricothyroid membrane, height, and weight. Obesity was expressed as the index weight·heighr2 [11]. To compensate for the increase in neck circumference with height in the normal population, patient measurements were corrected using a relationship established in 350 normals by this department (correlation coefficient (r)==0.18, 95 % confidence interval (C.I.) 0.08-0.28, p<0.02). The results were expressed as a percentage of the predicted normal neck circumference (PPNC) where;
IOO·neck circumference mm PPNC
(0.55·height cm)+ 310

510 R.J.O. DAVIES, J.R. STRADLING
Lateral pharyngeal radiograph
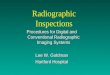
Each patient underwent lateral pharyngeal radiography using a variant of the technique described by BEAN et al. [12]. Subjects stood in a lateral position with the radiograph plate situated at the lateral tip of the acromion process. The X-ray source to radiograph plate distance was kept constant at six feet. Subjects were asked not to chew or swallow, and to occlude the teeth. The head was held in a comfortable position and a single radiograph taken. One investigator, (RJD), acting blind of the sleep study findings, measured the following dimensions directly from each radiograph (fig. 1).
V
D D \'--
Fig. 1. - Tracing of the lateral pharyngeal radiograph of a study patienL PNS: posterior nasal spine; P: tip of soft palate; HP: line subtended from hard palate; CS: line subtended from anterior border of spinal canal at the level of the 2nd and 3rd cervical vertebrae; RS: retroglossal space; MP: mandibular plane; H: anterior superior point of hyoid bone.
1) Soft palate length, PNS-P. Posterior tip of the hard palate to the end of the soft palate. 2) Mandibular plane to hyoid distance, MP-H. The distance from a line parallel to the inferior border of the mandibular ramus to the most anterior superior point of the hyoid bone. 3) Retroglossal space at its narrowest point, RS. Defined anteriorly by the root of the tongue, and posteriorly by the pharyngeal mucosa.
Head flexion at the time of film exposure was assessed by measurement of the internal angle between a line subtending from the hard palate and a line subtending from the anterior border of the spinal canal at the level of the second and third cervical vertebrae, HP-CS.
Where any radiographic landmark was insufficiently well defined to allow accurate measurement, that index was omitted, and the subject excluded from the multiple linear regression analysis (7 cases). All the data were used for the single regression analysis.
Sleep studies
To establish the presence or absence of OSA all 66 patients underwent either full polysomnography (61 cases), or overnight pulse oximetry (BIOX 3700) with sound and continuous video recording (5 cases). Of the five subjects studied by video and oximetry alone, none suffered more than one >4% arterial saturation dip per hour of sleep. Full polysomnography included recordings of electroencephalogram, electromyogram (EMG), electroocculogram, pulse oximetry, oro-nasal airflow, ribcage and abdominal movement.
For statistical analysis OSA was quantified as the number of >4% dips in arterial oxygen saturation per hour of sleep (>4% Sao2 dip rate). This is an established close correlate of the severity of OSA assessed in other ways [13-15]. Other causes of nocturnal arterial desaturation, such as hypoxic lung disease, were excluded by clinical examination and sleep study.
Variation of pharyngeal dimensions with head position in normal subjects
To establish the variation of pharyngeal dimensions with head posture, six normal volunteers underwent radiography in positions ranging from full head extension to full flexion, and from full head retraction to full protraction. In all subjects the range of angle HPCS was at least 85-120°. To minimise the X-ray dose required these radiographs were taken using fluoroscopic technique and 100 mm radiograph film (Phillips Electronics, Diagnost 64, and A.N.C. 6). The images produced were exactly half the size of the standard radiographs and a scaling factor of 2 was used to generate comparable data. PNS-P, MP-H, RS, and HP-CS, were measured from each image, and HP-CS was then correlated with the other variables.
80
• .. 70 :c • il • . e-60 , • • c • 0 • ~50 • ~
' :1 • • : 40 i • • • • i: • ~ 30 • • c • '/. 120 • • ••
10 0 • •
0 • 70 80 90 100 110 120 130 140
% Predicted normal neck clroomference
Fig. 2. - The relationship between OSA and neck circumference (n=66). r=0.63, 95% C.l. 0.46--0.76.

NECK SIZE, RADIOLOGY, AND SLEEP APNOEA 511
Table 1. -The characteristics of the sleep clinic patients studied
n=66 Median 95% Range
Age yrs 47 24-64 Weight kg 90 63-156 Obesity index kg·m-2 30 22-50 Neck circumference cm 42 35-50 % Predicted neck circumference 102 87-123 >4% Sao2 dip rate·hr1 6 0.2-59 Hard palate to spine angle 105° 83-123 Mandibular plane to hyoid mm 25 15-40 Soft palate length mm 45 29-60 Retroglossal airway mm 10 4.4-20
Statistical analysis of patient data
Pearson's correlation coefficient, Speannan's rank correlation, and stepwise multiple linear regression analysis (using the stepwise option) were performed using the SAS statistical analysis software package (SAS Institute Inc., Cary, North Carolina, USA). A single regression significance level of p<0.5 was fixed for entry into the multiple regression analysis, with a significance level of p<0.15 to remain in the analysis. As the relationship between PPNC and >4% Sao2 dip rate is non-linear (fig. 2), Spearman's rank correlation analysis was used to confirm the correlation between these variables.
Table 2. - Pearson correlation coefficient matrix for the 66 study patients
>4% Sao2 obesity dip rate PPNC index MP-H PNS-P RS HP-CS
>4% Sao2 0.629. 0.536 0.404 0.307 -0.024 0.285 dip rate <0.0001 .. <0.0001 <0.002 <0.02 NS <0.03
0.46, 0.76 ... 0.34, 0.69 0.17, 0.59 0.08, 0.51 -0.2, 0.2 0.04, 0.49
PPNC 0.629 0.728 0.305 0.572 0.259 0.405 <0.0001 <0.0001 <0.02 <0.0001 <0.04 <0.001 0.46, 0.76
obesity 0.536 0.728 0.177 0.222 0.296 0.224 index <0.0001 <0.0001 NS NS <0.02 NS
0.34, 0.69
MP-H 0.404 0.305 0.177 0.220 -0.144 0.476 <0.002 <0.02 NS NS NS <0.0001 0.17, 0.59
PNS-P 0.307 0.572 0.222 0.220 0.141 0.194 <0.02 <0.0001 NS NS NS NS 0.08, 0.51
RS -0.024 0.259 0.296 -0.144 0.141 0.055 NS <0.04 <0.02 NS NS NS -0.2, 0.2
HP-CS 0.285 0.405 0.224 0.476 0.194 0.055 <0.03 <0.001 NS <0.0001 NS NS 0.04, 0.49
": correlation coefficient, r; ••: p value; •••: 95% C.I. for r if applicable; PPNC: % predicted normal neck circumference; MP-H: mandibular plane to hyoid distance; PNS-P soft palate length; RS: retroglossal space at its narrowest point; HP-CS: head flexion angle; NS: not significant.
Table 3. -Multiple linear regression analysis of the sleep clinic patient data (n=59)
r 95% %variance p C.l. explained (r) (r2)
% predicted neck size 0.65 0.47-0.78 42 <0.0001 Obesity index 0.02 -0.24-0.27 <1 NS Hyoid distance 0.16 -0.10-0.40 3 NS Soft palate length 0.06 -0.20-0.31 <1 NS Hard palate to spine angle 0.02 -0.24-0.27 <1 NS Retroglossal airway 0.26 0.00-0.48 7 <0.01
Total model r2 = 0.42, 95% C.l. 0.22-0.61 (see text)
r: correlation coefficient; 95% C.l.: 95% confidence interval; NS: not significant. Dependent variable= >4% Sao2 dip rate.

512 R.J.O. DAVIES, J.R. STRADLING
Results
The study population characteristics are shown in table 1, and the results of the regression analysis in tables 2 and 3, and figure 2. In Pearson's correlation coefficient analysis neck size, obesity index, PPNC, PNS-P, l\1P-H, and HP-CS, were all significantly correlated with >4% Sao2 dip rate. No other variable demonstrated a significant correlation. Spearman's rank correlation analysis confirmed the relationship between PPNC and saturation dip rate, (r=0.69, 95% C.I. 0.53-0.80, p<O.OOOI).
30 • • • • 25 r:0.83, 95% C.l. 0.74-UO,
pc0.0001
E 20 •
E "' 15 • a: • •
10 • 5
0
so r:0.44, 95% C.l. 0.21-U2, pc0.001 • • 40 • • • • • E
~ 30 ci. :1
20 • • • • • • •• •
10 •
70 80 90 100 110 120 130
Hard paiBtt·to-cervlcal spine angle •
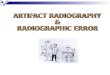
Fig. 3. - The variation of lateral pharyngeal radiographic dimensions with head flexion/cxtension in normals (n=6). RS: retroglossal space: MP-H: mandibular plane to hyoid distance.
Using stepwise multiple linear regression with >4% Sao2 dip rate as the dependent variable, the model best describing the variance was:
>4% Sao2 dip rate = 1.46PPNC - 1.17RS - 121.4 The r2 for this model was 0.42, (95% C.l. 0.22--0.61,
p<O.OOOl), thus explaining 42% of the total variance in >4% Sao2 dip rate. Obesity index, soft palate length , mandibular plane to hyoid distance, and hard palate-to-spine angle, did not contribute significantly to the model. If a >4% Sao
2 dip rate of 10 or more is taken
as evidence of significant OSA, then a PPNC of 105% (a 42.5 cm (16.75 inch) neck circumference for a 1.78 m (5 feet lO inch) man) is 77% sensitive and 82% specific for significant OSA. This is a positive predictive value of 75%.
Pearson's correlation coefficient analysis (figure 3) of the normal subject data demonstrated that the retroglossal space, and mandibular plane to hyoid distance, correlated significantly with hard palate-to-spine angle
(fig. 3); soft palate length did not. A previous study in six normals (unpublished) has shown neck circumference does not systematically vary with head posture.
Djscussioo
For most adult patients with obstructive sleep apnoea, obesity has been regarded as the most important element provoking their rusease (1]. This study has shown that variation in neck size fully explains this relationship. We have also shown that two radiographic pharyngeal dimensions which correlate with the presence of sleep apnoea (l\1P-H, and PNS-P) [2, 3, 5-8), appear to be secondary effects of neck obesity rather than independently important aetiological influences.
In this study, we have used a radiological technique which differs from those used elsewhere. All previous studies have attempted to generate a reproducible image by ensuring the head lies with the pituitary sella to nasion line within seven degrees of the horizontal [3, 7, 8, 16]. To achieve this, subjects have either been fixed in a cephalostat, or asked to maintain a horizontal gaze by fixing vision on their reflection in a mirror. In our technique we have removed these constraints, and allowed the subject to adopt a comfortable unrestrained posture. Our nonnal subject analysis has shown that small changes in angle HP-CS produce large variations in pharyngeal dimensions. Therefore, in order to establish whether conclusions drawn from our technique are comparable with those of others, we have measured angle HP-CS in 16 randomly selected adult orthodontic cephalostats drawn from a large library. The range of HP-CS was substantial, (median 91°,95% range 80-107), presumably due to movement of the body under the fixed head. Varying HP-CS across this 95% range generates at least a three fold variation in retroglossal space, and significant variation in hyoid position (fig. 3) [17). Cephalometry demands that the head be fixed in a selected posture. However, we have preferred to image the pharynx in a physiological position chosen by the patient. This avoids unnatural changes in pharyngeal dimensions induced by forcing an arbitrary head position. Although an unrestrained head position varies between subjects, it has been shown to be reproducible in an individual [18], and allows any compensatory responses for airway abnormalities to occur and be recorded in the final image.
We have found obesity index, l\1P-H, PNS-P, and HP-CS, to be correlated with >4% Sao
2 dip rate in single
regression analysis. Other groups have reported similar findings [3-8], and the increase in neck size among patients with OSA has been reported by this unit and others [19, 20]. However, this is the first work to relate neck size to radiographic pharyngeal dimensions in the sleep apnoea syndrome. In our multiple linear regression analysis obesity index, MP-H, PNS-P, and HPCS, do not explain significantly more variation in >4% Sao2 dip rate than does neck size alone. Thus the single regression correlations of these indices with OSA are

NECK SIZE, RADIOLOGY, AND SI..EEP APNOEA 513
secondary phenomena consequent on variation in neck size. We consider there may be several explanations for each of these secondary relationships. Soft palate size may simply be an indirect marker of neck obesity, since sleep apnoea patients have fat deposits in the uvula which are absent from weight matched controls [10]. Furthermore, since neck size is a powerful predictor of complete pharyngeal obstruction (OSA), it is likely to be a powerful predictor of partial obstruction: partial pharyngeal obstruction leads to snoring which is, itself, suggested to provoke oedema and elongation of the uvula [21].
The increase in MP-H may also be explained in several ways. T AILGREN and Soww have shown that MP-H varies with head flexion [17], as is seen in both our normal and patient data (fig. 3, table 2). We have shown variation in head flexion can occur even during cephalostatic radiography. Since angle HP-CS is positively correlated with >4% Sao2 dip rate (table 2), some of the increase in MP-H in OSA patients compared to controls may be explained by systematic head extension during imaging, even in the cephalostatic series. Since our normal subject data shows that head extension markedly widens the retroglossal airway (fig. 3), we hypothesise that the increase in angle HP-CS is a response learned by OSA patients to reduce the increased upper airway resistance caused by a small pharynx [4, 22, 23].
After surgical mandibular shortening (when the airway is narrowed by repositioning of the tongue), WICKWIRE et al. have shown that the hyoid descends, drawing the root of the tongue down and out of the overcrowded pharynx [24]. We suggest a similar response may occur when it is neck obesity which results in narrowing of the pharyngeal airway. If this is so, some of the increase in MP-H seen in OSA patients would represent a compensatory response to airway narrowing. In OSA patients with an increased mandibular plane to hyoid distance, the hyoid bone has been surgically elevated as part of treatment [25, 26]. If a low set hyoid is a secondary phenomena consequent on neck obesity, such an approach may be inappropriate if weight loss and thus reduction in neck size can be achieved.
Other groups have reported observations which support a significant role for neck fat deposition in OSA. In a rabbit model, simulating obesity by mass loading the pharynx leads to concentric airway narrowing and pharyngeal obstruction [9]. in man, sleep apnoea has been provoked by a superficial neck lipoma loading the airway, and cured by its resection [27]. There is also supportive evidence for compensatory pharyngeal responses protecting the airway from collapse. SURATT et al. [28] have shown that the genioglossus musculature exhibits more phasic EMG activity in OSA patients than controls during both wakefulness and sleep, and that this correlates with the resistance of the nasopharyngeal airway. Similar increases in genioglossus activity have been reported in children with OSA due to structural upper airway abnormalities [29]. If pharyngeal patency has to be maintained by extra muscular activity, collapse of the airway with sleep onset might be anticipated since there are other examples of respiratory compensations which fail on falling asleep. For example,
subjects breathing against added positive end-expiratory pressure accommodate to maintain a constant functional residual capacity (FRC) when awake. However, with the onset of sleep this adjustment fails and FRC rises [30].
The retroglossal space is not significantly correlated with >4% Sao2 dip rate in our single regression analysis, but is significant in the multiple linear regression, and thus is acting as a suppressor variable [31]. Therefore, its contribution to the multiple linear regression analysis cannot be interpreted reliably and it is not discussed further.
In conclusion, we have shown variation in neck circumference to be a close correlate of sleep apnoea, and thus a powerful physical sign when considering OSA in the sleepy patient who snores. We have also demonstrated that the widely recognised relationship between general obesity and sleep apnoea is fully explained by variation in neck size, implying that obesity mediates its effect through fat deposition in the neck. Finally, the relationships of soft palate length and mandibular plane to hyoid distance with the severity of OSA, both appear to be secondary to variation in neck circumference. In 1988, LuoAREsi et al. suggested that the anatomical upper airway changes seen in OSA patients may be secondary effects of the disease process [32]. We now present some evidence suggesting that for mandibular plane to hyoid distance and soft palate length this is likely to be true.
References
1. Guilleminault C, Tilkian A, Dement W. - The sleep apnea syndromes. Ann Rev Med, 1976, 27, 465-484. 2. Deber:ry-Borowiecki B, Kukwa A, Blanks RHI, Irvine CA. - Cephalometric analysis for diagnosis and treatment of obstructive sleep apnoea. Laryngoscope, 1988, 98, 226-234. 3. Jamicson A, Guilleminault C, Partinen M, Quera-Salva MA. - Obstructive sleep apnea patients have craniofacial abnormalities. Sleep, 1986, 9, 4, 469-477. 4. Crumley RL, Stein M, Gamsu G, Golden J, Dermon S. -Determination of obstructive site in obstructive sleep apnoea. Laryngoscope, 1987, 97, 301-308. 5. Gislason T, Lindholm CE, Almqvist M, Birring E, Boman G, Eriksson G, Larsson S, Lidell C, Svanholm H. -Uvulopalatopharyngoplasty in the sleep apnoea syndrome. Arch Otolaryngol Head Neck Surg, 1988, 114, 45-51. 6. Guillem.inault C, Riley R, Powell N.- Obstructive sleep apnoea and abnormal cephalometric measurements. Chest, 1984, 86, 5, 793-794. 7. Partinen M, Guilleminault C, Quera-Salva MA, Jamieson A. - Obstructive sleep apnoea and cephalometric roentgenograms. Chest, 1989, 93, 6, 1199-1205. 8. Riley R, Guilleminault C, HerT8n J, Powell N. -Cephalometric analysis and flow volume loops in obstructive sleep apnoea patients. Sleep, 1983, 64, 4, 303-311. 9. Koenig JE, Thach BT. -Effects of mass loading on the upper airway. J Appl Physiol, 1988, 64, 6, 2294-2299. 10. Homer RL, Mohiaddin RH, Lowell DG, Shea SA, Burman ED, Longmore DB, Guz A. - Sites and sizes of fat deposits around the pharynx in obese patients with obstructive sleep apnoea and weight matched controls. Eur Respir J, 1989, 2, 613-622. 11. Revicki DA, Israel RG. - Relationship between body

514 R.J.O. DA VIES, J.R. STRADLING
mass indices and measures of body adiposity. Am J Public Health, 1986, 76, 8, 992- 994. 12. Bean LR, Kramer JR. Khoow FE. - A simplified method of taking radiographs for cephalometric analysis. J Oral Surg, 1970, 28, 675--678. 13. Famey RI, Walker LE, Jensen RL, Walker JM. - Ear oximetry to detect apnea and differentiate rapid-eye-movement (REM) and nonREM sleep. Chest, 1988, 89, 533-539. 14. George CF. Millar TW, Kryger MH. - Identification and quantification of apneas by computer-based analysis of oxygen saturation. Am Rev Respir Dis, 1988, 137, 1238-1240. 15. Gould GA, Whyte KF, Airlie MAA, Rhind GB, Catterall JR. Shapiro CM, Douglas NI. - Criteria for diagnosing abnormal breathing during sleep. Thorax, 1987, 42, 722. 16. Riley R, Guilleminault C, Powell N, Simmons FB. -Palatopharyngoplasty failure, cephalomelric roentgenograms, and obstructive sleep apnea. Otolaryngol Hemi Neck Surg, 1985, 93, 2. 240-243. 17. Tallgren A, Solow B. - Hyoid bone position, facial morphology, and head posture in adults. Eur J Orthod, 1987, 9, 1-8. 18. Solow B, Tallgren A. - Natural head position in standing subjects. Acta Odont Scand, 1971, 29. 591-607. 19. Katz I, Sttadling J, Slutsky AS, Zamel N. Hoffstein V. Do patients with obstructive sleep apnoea have a short and fat neck? Am Rev Respir Dis, 1989, 139, 4, A622. 20. Crosby J, Warley A, S!radling J. - Sleep hypoxaemia and its correlates in 480 men aged 35 to 65 years. Thorax, 1989, 44, 353P. 21. Fairbanks DNF. - Snoring: an overview with historical perspectives. Fujita S. - Pharyngeal surgery for obstructive sleep apnea and snoring. In: Snoring and obstructive sleep apnoea. D.N.F. Fairbanks, S. Fujita, T . Ikematsu, F.B. Simmons eds, Raven Press, New York, 1987. 22. Rivlin J, Hoffstein V, Kalbfeisch J, McNicholas W, Zamel N, Bryan C. - Upper airway morphology in patients with idiopathic obstructive sleep apnoea. Am Rev Respir Dis, 1984, 129, 355-360. 23. Stein MG, Gamsu G, de Greer G, Golden JA, Crumley RL. Webb RW. - Cine CT in obstructive sleep apnoea. AJR, 1987, 148, 1069- 1074. 24. Wickwire NA. White RP, Proffit WR. - The effect of mandibular osteotomy on tongue position. J Oral Surg, 1972, 30. 184-190. 25. Riley R, Guilleminault C, Powell N, Derman S. -Mandibular osteotomy and hyoid bone advancement for obstructive sleep apnea: a case report. Sleep, 1984, 7, 1, 79-82. 26. Guilleminault C, Riley RW, Powell NB. - Surgical treatment of obsttuctive sleep apnoea. In: Principles and
practice of sleep medicine. M.H. Kryger, T. Roth, W.C. Dement, Saunders, Philadelphia Pennsylvania, 1989, 571-583. 27. Koopman CF, Feld RA, Coulthard SW. - Sleep apnea syndrome associated with a neck mass. Otolaryngol Head Neck Surg, 1981, 89, 949-952. 28. Suratt PM, MeTier RP, Wilhoit SC. - Upper airway muscle activation is augmented in patients with obstructive sleep apnoea compared with that in normal subjects. Am Rev Respir Dis, 1988, 137, 889-894. 29. Jefferies B, Brouillette RT. Hunt CE. - Eleclromyographic study of some accessory muscles of respiration in children with obstructive sleep apnea. Am Rev Respir Dis, 1984, 129, 696-702. 30. Bogie RL, Skatrud JB. - Effect of lung volume on expiratory muscle recruitment during wakefulness and NREM sleep. Am Rev Respir Dis, 1989, 139, A82. 31. Pedhazur EJ. - Multiple regression in behavioural research. Holt, Rinehart, and Winston, Fort Worth, Texas. 1982. 32. Lugaresi E, Cirignotta F. Montagna P. - Pathogenic aspects of snoring and obstructive apnea syndrome. Schweiz Med Wschr, 1988, 118, 1333-1337.
Relation entre la circonference du cou, /'anatomie pharyngee radiologique, et le syndrome d'apnie obstructive du sommeil. R. Davies, J. Stradling. RESUME: Nous avons etudie, chez 66 patients, la valeur predictive de la circonference du cou, de l'obesite, et de ccrtaines dimensions du pharynx obtenues par etude radiologique, en ce qui conceme le syndrome d'apnee obstructive du sommeil (OSA). OSA a ete quantifie comme le nombre moyen horaire de chutes de la saturation oxygenee du sang arteriel > 4% pendent le sommeil. La circonference du cou (r=0.63, 95% C.I. 0.46-0.76), l'index d'obesite (r=0.54, 95% C.I. 0.39-0.69), la position de l'hyoi'de (r=0.40, 95% C.I. 0.19-0.59), la longueur du voile du palais (r=Q.31, 95% C.l. 0.08-0.51), et I' angulation de palais osseux a la colonne (r=0.29, 95% C.J. 0.04-0.49). sont en correlation significative avec Ies creux de saturation dans une analyse de regression simple. Dans une analyse de regression lineaire multiple par echelons (ou le taux de creux de saturation est la variable dependante), seuls la dimension du cou e t l'espace retro-lingual sont en correlation independante significative (total rl=0.42, 95% C.I. 0.22 a 0.61, p<0.0001). Nous concluons que les relations enlre l'obesite generale, la position de l'os hyoide, la longueur du voile du palais, et le syndrome d'apnee du sommeil, sont probablement secondaires aux modifications de la circonference du cou. Eur Respir J., 1990, 3, 509- 514.