Embed Size (px)
Citation preview

The relationship between changes in self-rated quality oflife after cochlear implantation and changes in individualcomplaints
Zhao, F.,* Bai, Z.†1 & Stephens, D.‡
*Centre for Hearing and Balance Studies, University of Bristol, Bristol, �Welsh Hearing Institute, University
Hospital of Wales, Cardiff, and �College of Medicine, Cardiff University, Cardiff, UK
Accepted for publication 5 June 2008
Clin. Otolaryngol. 2008, 33, 427–434
Objectives: To evaluate the changes in self-rated quality
of life (QoL) obtained following cochlear implantation in
relation to changes in the individual’s complaints.
Design: We have used repeated responses over a period
of at least 4 years following implantation so as to exam-
ine within-subject relationships.
Participants: Twenty-four consecutive post-lingually
deafened patients who had been fitted with
cochlear implants between 1991 and December
2000 at the University Hospital of Wales were
investigated.
Main outcome measures: The open-ended problems
questionnaire was used to assess what hearing impaired
people themselves considered to be the main problems
arising from their hearing loss. The participants were
asked to rate the severity of each one of these problems
as well as QoL on ‘0’ to ‘100’ visual analogue scales. Both
the individual problem ratings and the ratings of QoL
were re-administered to the subjects at each follow-up
session.
Results: Changes in the rated QoL of all patients were
significantly associated with changes in specific com-
plaints, for example, the ability to communicate, feeling
of isolation, telephone use, self-confidence, enjoyment of
music and watching the TV. Multiple stepwise regression
analysis showed that, after implantation, improvements in
communication abilities, reduced psychological problems
and improvements in abilities of daily life were the key
determinants of QoL improvement for individual
cochlear implant patients. These key predictors reached a -
plateau at about 1.5–3 years after cochlear implantation.
Conclusions: The relationships between changes in
specific complaints and the QoL in individual implantees
were highlighted. We suggest that cochlear implant
outcome measures should continue for at least 3 years after
implantation.
Since the development of cochlear implants (CI), there
has been considerable interest in their efficacy. Extensive
evaluations and assessments have been carried out on
profoundly deafened implanted patients to determine
how well they are able to perform using implants. Assess-
ments have included psychoacoustical tests, speech recog-
nition, speech production, music appreciation and
psychological changes.1–6 Most results show that CIs con-
stitute a successful and effective treatment for people with
severe and profound hearing impairment in terms of
providing improved audiological performance. However,
these results are often obtained in clinical or test situa-
tions and do not represent the ease or difficulty an indi-
vidual has in daily living. It is a well-known fact that
patients with identical audiometric characteristics may
have very different problems in daily life.7 Ultimately, the
aim of cochlear implantation is to minimise any disabili-
ties which an individual experiences as a result of pro-
found hearing loss, together with improving their quality
of life. Therefore, it is essential to evaluate the changes in
the specific activity limitations, participation restrictions
and quality of life (QoL) as perceived by CI patients so as
to define the effectiveness of the CI.
Following the current International Classification of
Functioning, Disability and Health (WHO ICF) formula-
tion,8 the concept of hearing impairment is defined as the
dysfunction measurable in the laboratory or in the clinic,
activity limitation being the auditory difficulties experi-
enced by the individuals (what they cannot do) and
Correspondence: Dr Fei Zhao, Centre for Hearing and Balance Studies,
University of Bristol, 5th Floor, 8 Woodland Road, Bristol BS8 1TN,
UK. Tel.: +44 117 928 7790; fax: +44 117 954 6809; e-mail:
[email protected] address: ENT ⁄ Head and Neck Surgery Department, Second
Affiliated Hospital of Kun Ming Medical College, Kun Ming, Yun Nan,
China
OR
IG
IN
AL
AR
TI
CL
E
� 2008 The Authors
Journal compilation � 2008 Blackwell Publishing Ltd • Clinical Otolaryngology 33, 427–434 427

participation restriction, the non-auditory effects of these
on their life (what they do not do). In addition, according
to WHO QoL working group, ‘Quality of Life (QoL) is
defined as an individual’s perception of their position in
life in the context of the culture and value systems in which
they live and in relation to their goals, expectations, stan-
dards, and concerns’9 It is frequently referred to and used
in relation to health in general and to the effects of disease
in particular. The QoL is a multi-dimensional construct,
with contributions from several different aspects, or
‘domains’ of life. It is more than just a reflection of health
status (i.e. physical, psychological and social well-being)
because it incorporates other life experiences such as eco-
nomic, occupational and domestic ⁄ family domains. There-
fore, evaluation of QoL should include different aspects of
the person’s physical health, psychological status, level of
independence and social relationships.
There have been many studies attempting to assess the
QoL changes in patients after cochlear implantation (e.g.
10–14) using questionnaires, which may comprise qualita-
tive and quantitative assessments. These studies have
shown that cochlear implantation leads to substantial
improvement in QoL. For example, the study by Mo
et al.,10 used the generic QoL measure SF36, the PQLF
(Patient Quality of Life Form) and the IRQF (Index Rela-
tive Questionnaire Form). Their results showed that CIs
were associated with significant improvement in QoL in
post-lingually deafened adults measured by the PQLF and
the IRQF. The improvement was mainly in the compo-
nents of communication, feelings of being a burden, iso-
lation and relationships with friends and family. There
was also a significant reduction in depression and anxiety.
Nevertheless, the SF-36 showed significant improvement
only in the scale of ‘general health’ but not in the other
seven scales, which indicated that the generic QoL mea-
sure SF-36 may not be suitable to detect change in QoL
in CI patients.
However, among the generic health-related QoL
(HRQol) measures, the HUI3 (Health Utilities Index
Mark 3) is recognised as one of the most effective tools
in measuring HRQoL improvements among CI recipients
because it contains a question related to hearing abil-
ity.11,12 This generic instrument is responsive not only to
diverse states of ill health and to intervention for them
but also to effects of profound deafness and of cochlear
implantation. It focuses on a person’s ability to undertake
certain tasks, such as hearing and speech production. In a
recent study by UK Cochlear Implant Study Group,13 it
was reported that adult implantees display significant
improvements on the hearing and speech attributes
measured by HUI3 9 months after the implantation. In
addition, long term benefits of CI were evaluated using
HUI3. The results were significantly better than those
obtained before CI in three domains (i.e. hearing, emo-
tions and the total utility score).
More recently, disease-specific HRQoL measures have
received increasing attention. For example, the Nijmegen
Cochlear Implant Questionnaire (NCIQ) was developed
by Hinderink et al.,14 and is a quantifiable, self-assess-
ment HRQoL instrument for use with CI users. Previous
studies have proved that NCIQ is reliable and valid and
sensitive to clinical changes. Moreover, the data obtained
from the NCIQ indicated that a CI had significant effects
on several aspects of HRQoL, including the social and
psychological domains.
In the present study, we have used patient-generated
methods to measure specific activity limitations, partici-
pation restrictions and the QoL in patients who had
received CIs in an attempt to define how changes in spe-
cific complaints influence the self-reported QoL in indi-
vidual implantees. In addition, we have used repeated
responses over a period of at least 4 years following
implantation so as to examine within-subject relation-
ships. The significant outcomes obtained from such an
analysis should provide further insight into the relation-
ship between QoL changes and improvements in specific
difficulties arising from the hearing impairment.
Materials and methods
Participants
Twenty-four consecutive postlingually deafened patients
who had been fitted with CIs between 1991 and Decem-
ber 2000 at the University Hospital of Wales comprised
the study population, and thus all patients had at least
4 years experience with their CIs by December 2004.
There were seven men and 17 women aged between 32
and 78 years (mean: 53.9 years, sd: 12.9 years). All partic-
ipants received information about the study and con-
sented to participate in the research.
The CIs fitted in this group of patients included: 16
Medel C40+, 3 Medel PRO+, 3 Nucleus 3G and 2
Nucleus Esprit22. Of those, six patients had received CIs
with the four-channel Ineraid initially, but four of these
had been upgraded to the Medel C40+, and two to Medel
PRO+ implants. Their median number of years of CI use
was 8.0 years. English was the first language of all the
patients. All were in good general health.
Procedures
For each patient with a CI, a clinical and audiometric
assessment was performed. The clinical history was
428 F. Zhao et al.
� 2008 The Authors
Journal compilation � 2008 Blackwell Publishing Ltd • Clinical Otolaryngology 33, 427–434

obtained at initial interview by an Audiological Physician
(one of the authors), including duration of hearing loss,
onset, history of tinnitus or vertigo and family history. The
aetiological investigation was based on medical history,
family history and clinical assessment, which included psy-
choacoustic tests and high resolution CT scans.
The external earhook and speech processor were fitted
6 weeks postoperatively. All received at least 3 months
intensive therapy carried out by the same Hearing Thera-
pist at the Welsh Hearing Institute, Cardiff. The patients
received approximately 50 hours of communication train-
ing in the first 9 months.
All CI patients had pre-CI assessment as well as a
number of follow-ups over a 9, 12, 18, 24, 36 and 48-
month periods of use of their CIs, followed by annual
intervals, extending up to 14 years. In the present study,
data obtained from the first six follow-ups were analysed.
The mean times post-implantation of the first six follow-
ups were 6.9, 12.7, 18.4, 24.9, 38.7 and 50.7 months.
Questionnaires
Each patient seen for consideration for a CI was sent
the open-ended problems questionnaire15 with their
appointment and asked to list any and all difficulties
they experienced as a result of their hearing loss. The
wording was as follows: ‘Please make a list of the diffi-
culties which you have as a result of your hearing loss.
List them in order of importance to you, starting with
the biggest difficulties. Write down as many as you can
think of’. In most cases the difficulties listed were expli-
cit [e.g. ‘hearing my wife when the television is on’, but
in some they were extremely general (e.g. ‘people speak-
ing’)]. In such cases, during the clinical interview, the
patient was asked to clarify the statement and ⁄ or be
more concise.
Next, the patients were asked to rate the severity of
each one of these problems on a ‘0’ to ‘100’ visual ana-
logue scales using the approach described by Habib and
Hinchcliffe.16 For example:
Hearing has no effect on confidence Complete loss of
Complaint: Loss of
0 100
Cochlear implant patients were reminded of their spe-
cific complaints when they attended follow-up sessions.
Their specific problems were repeated to patients on each
occasion so that the patients were able to rate the severity
of each initial individual complaint on the same scale.
Self-rated quality of life
The patients were asked to quantify their QoL on a simi-
lar scale. The following wording was used:
‘Please rate the effect of your hearing loss on the over-
all quality or enjoyment of life. If it has no effect the
score would be 0, if it completely ruined your life it
would be 100’.
Both the individual problem ratings and the ratings of
QoL were re-administered to the subjects at each follow-
up session, without the individual being informed of their
previous ratings.
Ethical considerations
All participants were provided written information before
joining in this study. They agreed to participate in the
study on a voluntary basis, and understood that they
could withdraw from this study at any time without
affecting their treatment. We obtained ethical approval
from the R&D Research Committee of the Cardiff and
Vale NHS trust.
Results
Specific problems reported by participants
All participants were asked to list the hearing difficulties
which they had as a result of their hearing loss. Table 1
shows all problems which were specified by this group of
the participants. It is noteworthy that ‘communication dif-
ficulties’ (18 ⁄ 24, 75.0%) and ‘feeling of isolation’ (17 ⁄ 24,
70.8%) were the most common complaints. Other com-
mon complaints were ‘difficulties in using telephone’, ‘loss
of confidence’, ‘difficulties in enjoying music’, ‘effect on
social life’ and ‘difficulties in watching TV’. Furthermore,
there were several other specific complaints which less
common, for example, ‘can’t hear alarms or voice’, ‘tinni-
tus’, ‘hearing speech in the presence of background noise’,
‘effect on career’, ‘worry about traffic’, ‘feeling of discrimi-
nation’, ‘tiredness’, ‘feeling of depression’, ‘feeling of bore-
dom’ and ‘need concentration’.
The magnitudes of QoL and the common complaints,
together with their changes post-implantation
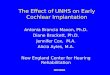
The magnitude of the mean changes over time for QoL
and the common problems are shown in Fig. 1. In gen-
eral, the changes over time for QoL were consistent with
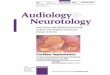
the changes across all complaints. Figure 2a shows such
an example of the subject’s responses in which there was
a consistent change across all complaints. However, the
Predictors of quality of life post-implantation 429
� 2008 The Authors
Journal compilation � 2008 Blackwell Publishing Ltd • Clinical Otolaryngology 33, 427–434

changes for various complaints in some other subjects
differed from each other, as shown in Fig. 2b. It is obvi-
ous that there will be stronger relationships between rated
QoL and the individual complaints in a subject whose
responses all show the same pattern than in cases in
which there are more disparate responses.
Relationship between changes in self-rated QoL and
changes in their specific complaints across the different
follow-up sessions
The relationships between changes in rated QoL and in
their specific complaints across the different follow-up
Table 1. Summary of complaints specified by 24 individual cochlear implant patients and their significant correlations between
changes in self-rated quality of life and specific measures
Complaint list
Number reporting
as a problem
(out of 24 subjects)
Numbers of subjects
showing significant
correlations between
changes in QoL and
complaint
Numbers of subjects
showing complaint as
a determinant by multiple
stepwise regression
Effect on communication 18 15 9
Feeling of isolation 17 15 6
Difficulties using the telephone 13 10 4
Loss of confidence 13 10 3
Effect on enjoyment of music 12 11 3
Effect on social life 10 5 0
Effect on watching TV 9 7 4
Cannot hear alarms or voice 7 1 0
Tinnitus 6 3 1
Speech in noise 6 3 0
Effect on career 6 1 0
Worry about traffic 5 2 0
Feeling of discrimination 3 1 0
Tiredness 3 2 0
Need to concentrate 3 1 0
Feeling of depression 3 2 0
Feeling of boredom 3 1 0
Effect on relationship with son 1 1 0
No independence 1 0 0
QoL, quality of life.
60
70
80
90
100QoL
Communication
Feeling of isolation
Using phone
Loss of confidence
0
10
20
30
40
50
60
Pre-CI 6 months 12 months 18 months 24 months 36 months 48 months
Mea
n r
atin
g
Pre and post implantation
Enjoyment of music
Social life
Wathcing the TV
Fig. 1. The magnitude of the mean
changes over time for QoL and the com-
mon problems reported by cochlear
implant patients.
430 F. Zhao et al.
� 2008 The Authors
Journal compilation � 2008 Blackwell Publishing Ltd • Clinical Otolaryngology 33, 427–434

sessions for each participant were analysed with
Kendall’s tau correlation coefficients. The results for each
complaint are shown in Table 1. Post-implantation,
changes in QoL for all patients were significantly associ-
ated with changes in one or more specific complaints.
Of those, 15 out of 18 subjects’ improvements in QoL
was significantly correlated with improved communica-
tion. In 15 of 17 individuals improvements in QoL were
significantly associated with reduced feeling of isolation
and in 10 of 13 with improved using the telephone and
self-confidence, in 11 of 12 it was significantly related to
improved enjoyment of music. Furthermore, in five of
10 participants it was significantly associated with
improvements in social life and also in six of nine par-
ticipants with improved watching the TV; in three of six
participants QoL changes were significantly associated
with reductions in tinnitus.
Further multiple stepwise regression analysis showed
that, after implantation, different variables appeared to be
the key determinants for QoL improvement in different
patients with CIs. After implantation, improved commu-
nication in nine subjects (9 ⁄ 18, 50.0%) became the key
determinant of improvements in QoL. In addition,
reduced ‘feeling of isolation’ (6 ⁄ 17, 35.3%), improved use
of the telephone (4 ⁄ 13, 30.8%), enjoyment of music
(3 ⁄ 12, 25.0%), watching the TV (4 ⁄ 9, 44.4%), together
with increased self confidence (3 ⁄ 13, 23.1%) were also
key determinants of improvements in QoL.
The times, post-implantation, at which each complaint
reached a plateau for different individuals
The rating of each common complaint for each individ-
ual was analysed to determine when it reached a steady
60
70
80
90
100QoL
Communication
Feeling of isolation
Using phone
Enjoyment of music
0
10
20
30
40
50Loss of confidence
Social life
100QoL
80
90 Communication
Feeling of isolation
60
70 Worry about traffic
Enjoyment of music
Tinnitus
40
50Watching the TV
20
30
0
10
Ind
ivid
ual
rat
ing
Ind
ivid
ual
rat
ing
Pre-CI 6 months 12 months 18 months 24 months 36 months 48 months
Pre and post implantation
Pre-CI 6 months 12 months 18 months 24 months 36 months 48 months
Pre and post implantation
(a)
(b)
Fig. 2. (a, b) Examples of the relation-
ships between the changes of self-rated
quality of life and the changes of individ-
ual complaints in two individuals.
Predictors of quality of life post-implantation 431
� 2008 The Authors
Journal compilation � 2008 Blackwell Publishing Ltd • Clinical Otolaryngology 33, 427–434

state or plateau in terms of the different follow-ups after
implantation. These results are shown in Fig. 3. Most
individuals’ improvements in psychological problems (for
example, feeling of isolation and loss of confidence)
reached a plateau at the third to fourth follow-ups after
implantation (i.e. 1.5–2 years). The improvements in abil-
ities of daily life (such as using the telephone, enjoyment
of music, watching TV and social life) appeared to take
longer to reach a steady status. None or a few of these
problems reached a plateau within the first two follow-
ups after implantation. Most individuals’ improvements
in abilities of daily life reached a plateau at the third to
fifth follow-ups after implantation (i.e. 1.5–3 years). Over
80% of participants reported that improvements in their
tinnitus reached to a steady status within the first three
follow-ups after implantation. By contrast, the problem
with ‘effect on career’ took much longer than other prob-
lems to improve to a steady-state level.
Discussion
The effectiveness of cochlear implantation has been evalu-
ated in numerous studies.1–6 The studies have demon-
strated that CIs provide not only audiological benefits in
terms of sound awareness and improved speech percep-
tion, but also reduce the activity limitation and participa-
tion restriction, for example, improvement in general
communication and self-confidence, and consequently
improve the QoL. Mo et al.10 reported that duration of
deafness and audiological benefit did not show a signifi-
cant association with change in QoL, but found a signifi-
cant association between reduction in depression and
anxiety and improvement in QoL. Moreover, in the study
by Hallberg, the variance in psychological general well-
being can be partially explained by attitudes from others,
restricted social participation, perceived social support
and age.17
40
50
60
40
50
60
40
50
60 Communication Feeling of isolation Loss of confidence
0
10
20
30
0
10
20
30
10
20
30
40
50
60
40
50
60
40
50
60 Social life Using phone Enjoyment of music
10
20
30
10
20
30
10
20
30
40
0 0
50
60
50
60 Watching TV
0
50
60 Effect on careers Tinnitus
20
30
40
20
30
40
20
30
40
Th
e p
erce
nta
ge
of
coch
lear
imp
lan
t p
atie
nts
rea
chin
g a
ste
ady
stag
e le
vel
Different follow-ups stages after implantation
0
10
0
10
0
10
Months Months Months
Months Months Months
Months Months Months
Fig. 3. The percentage of cochlear implant patients reaching a steady state level for each complaint in terms of the different follow-
ups after implantation.
432 F. Zhao et al.
� 2008 The Authors
Journal compilation � 2008 Blackwell Publishing Ltd • Clinical Otolaryngology 33, 427–434

Although many structured questionnaires are available
to evaluate activity limitation and participation restriction
caused by hearing impairment, most of the scales are usu-
ally designed for the general hearing impaired population.
These often contain questions that are irrelevant to the
profoundly deafened. They may experience extremely var-
iable hearing difficulties and benefits from an implant.
An open-ended questionnaire approach used in this study
has been found to be a useful tool in highlighting specific
difficulties encountered by patients with hearing impair-
ment. It has also been used to assess the advantages and
disadvantages in patients after using CIs.18,19 Such a tech-
nique allows the patients to describe their important diffi-
culties in a more realistic and specific way than when
using structured questionnaires. There is evidence show-
ing that open-ended hearing problem questionnaires can
be worded to highlight the specific hearing activity limita-
tions and participation restrictions encountered by
patients with hearing difficulties.20,21 Moreover, the
impact of hearing impairment on QoL can also be exam-
ined by this technique.22 Compared with structured ques-
tionnaires, open-ended questionnaire tends to generate
large amounts of data that can take a long time to pro-
cess and analyse, using qualitative techniques.
Furthermore, Self-rating measures have become increas-
ingly popular and are expanding in audiological and
related research and practice in the assessment of hearing
aids benefits, communication strategy, and the effectiveness
of CIs.23 In the present study, the new technique modified
by combination of self-rating measure and the open-ended
questionnaire offers a useful and relevant tool in not only
highlighting the specific complaints of CI patients, but also
reflecting the quantitative changes in them.
Thus in the 24 profoundly deafened adults, whose CI
experiences were more than 4 years and who were asked
to report their difficulties using the open-ended hearing
problem questionnaire, the most commonly reported
hearing difficulties problems were with communication,
feeling of isolation, using the telephone, enjoyment of
music, watching TV, loss of confidence and loss of social
life. These common complaints come in both the ‘live
speech’ and ‘psychosocial’ domains. This clearly provides
the valuable insights for understanding activity limitation
and participation restriction in CI patients.
Furthermore, the improvement in the QoL in pro-
foundly deafened adults after they had received CI and its
relationships toward changes in individual complaints
were also investigated in this study. Overall, the changes
over time for QoL were consistent with the changes
across all complaints. However, the changes in some
complaints did not follow the same patterns of the
changes for QoL. This result may imply the variety of the
effectiveness of CI in meeting the patients’ specific needs.
In addition, it also indicates that some less important
complaints are not significantly associated with improved
QoL.
Further correlational analyses showed that changes in
QoL for all patients were significantly associated with
changes in specific complaints. Moreover, multiple step-
wise regression analysis indicated that improvements in
communication abilities, psychological problems (for
example, feeling of isolation and loss of confidence) and
abilities of daily life (such as using the telephone, enjoy-
ment of music, watching the TV) are the key determi-
nants of QoL improvement for individual CI patients.
Improvement in some CI recipients was often a gradual
process. Previous studies have shown that improvements
in psychological state after cochlear implantation have
occurred from 12 to 36 months after surgery.24 Tyler
et al.25 found that most gains in performance occur in
the first 9–12 months of use of the CIs, but many
patients continue to improve over the first one-and-a-half
to two-and-a-half years, and even longer. In our study,
we found that improvements in specific complaints for
most individuals had reached a steady state at third to
fifth follow-ups after implantation (i.e. 1.5–3 years). For
example, most individuals’ improvements in psychologi-
cal problems reached a plateau at third to fourth follow-
ups (i.e. 1.5–2 years), and improvements in abilities of
daily life reached a plateau at third to fifth follow-ups
after implantation (i.e. 1.5–3 years). However, our results
showed that the problem with ‘effect on career’
needs much longer than other problems to improve to a
steady-state level. We therefore suggest that CI
outcome measures should continue at least 3 years after
surgery.
Acknowledgements
The work was performed when Zhong Bai was a visiting
scholar researching in Welsh Hearing Institute. Dr Bai
was supported by China Scholarship Council (CSC). We
would like to thank the Cardiff Cochlear Implant Team
for their help throughout the study.
Conflict of interest
None to declare.
References
1 Tye-Murray N., Tyler R.S., Woodworth G.G. et al. (1992) Per-
formance over time with a nucleus or ineraid cochlear implant.
Ear Hear. 13, 200–209
Predictors of quality of life post-implantation 433
� 2008 The Authors
Journal compilation � 2008 Blackwell Publishing Ltd • Clinical Otolaryngology 33, 427–434

2 Hinderink J., Mens L.H.M., Bronx J.P.L. et al. (1995) Perfor-
mance of prelingually and postlingually deaf patients using sin-
gle-channel or multi-channel cochlear implants. Laryngoscope
105, 619–622
3 Parkinson A.J., Parkinson W.S., Tyler R.S. et al. (1998)
Speech perception performance in experienced cochlear-
implant patients receiving the SPEAK processing strategy in
the Nucleus Spectra-22 cochlear implant. J. Speech Lang. Hear
Res. 41, 1073–1087
4 Labadie R.F., Carrasco V.N., Gilmer C.H. et al. (2000) Cochlear
implant performance in senior citizens. Otolaryngol. Head Neck
Surg. 123, 419–423
5 Djalilian H.R., King T.A., Smith S.L. et al. (2002) Cochlear
implantation in the elderly: results and quality-of-life assess-
ment. Ann. Otol. Rhinol. Laryngol. 111, 890–895
6 Dorman M.F., Basham K., McCandless G. et al. (1991) Speech
understanding and music appreciation with the Ineriad cochlear
implant. Hearing J. 44, 34–35
7 Bai Z. & Stephens S.D.G. (2005) Subjective outcome measures
after cochlear implantation: overall measures. Audiological Med.
3, 212–219
8 Stephens S.D.G. & Hetu R. (1992) Impairment, disability and
handicap in audiology: toward a consensus. Audiology 30, 185–
200
9 WHO QOL Group. (1993) Measuring Quality of Life: The Devel-
opment of the World Health Organization Quality of Life Instru-
ment (WHO QOL). WHO, Geneva
10 Mo B., Lindbaek M. & Harris S. (2005) Cochlear implants and
quality of life: a prospective study. Ear Hear. 26, 186–194
11 Abrams H.B., Chisolm T.H. & McArdle R. (2005) Health-related
quality of life and hearing aids: a tutorial. Trends Amplif. 9, 99–
109
12 Damen G.W., Beynon A.J., Krabbe P.F. et al. (2007) Cochlear
implantation and quality of life in postlingually deaf adults:
long-term follow-up. Otolaryngol. Head Neck Surg. 136, 597–604
13 UK Cochlear Implant Study Group. (2004) Criteria of candidacy
for unilateral cochlear implantation in postlingually deafened
adults I: theory and measures of effectiveness. Ear Hear. 25,
310–335
14 Hinderink J.B., Krabbe P.F. & Van Den Broek P. (2000) Develop-
ment and application of a health-related quality-of-life instrument
for adults with cochlear implants: the Nijmegen cochlear implant
questionnaire. Otolaryngol. Head Neck Surg. 123, 756–765
15 Barcham L.J. & Stephens S.D.G. (1980) The use of an open-
ended problems questionnaire in auditory rehabilitation. Br. J.
Audiol. 14, 49–54
16 Habib R.G. & Hinchcliffe R. (1978) Subjective magnitude of
auditory impairment. Audiology 17, 68–76
17 Hallberg L.R.M.A., Ringdahl A. & Holmes C.C. (2005) Psycho-
logical general well-being (quality of life) in patients with cochl-
ear implants: importance of social environment and age. Int. J.
Audiol. 44, 706–711
18 Zhao F., Stephens S.D.G., Sim S.W. et al. (1997) The use of
qualitative questionnaires in cochlear implant candidates. Clin.
Otolaryngol. 22, 254–259
19 Tyler R.S. (1994) Advantages and disadvantages expected and
reported by cochlear implant patients. Am. J. Otol. 15, 523–531
20 Zhao F. & Stephens S.D.G. (1996) Hearing complaints of patients
with King-Kopetzky Syndrome. Br. J. Audiol. 30, 397–402
21 Lormore K.A. & Stephens S.D.G. (1994) Use of the open-ended
questionnaire with patients and their significant others. Br. J.
Audiol. 28, 81–89
22 Maillet C.J., Tyler R.S. & Jordan H.N. (1995) Change in the
quality of life of adult cochlear implant patients. Ann. Otol. Rhi-
nol. Laryngol. Suppl. 165, 31–48
23 Cox R., ed. (2000) Proceedings of the workshop ‘Self-reported
outcome measures in audiological rehabilitation including hear-
ing aids’. Ear Hear. 21, S1–S115
24 Knutson J.F., Murray K.T., Husarek S. et al. (1998) Psychologi-
cal change over 54 months of cochlear implant use. Ear Hear.
19, 191–201
25 Tyler R.S., Parkinson A.J., Woodworth G.G. et al. (2007) Perfor-
mance over time of adult patients using Ineraid or Nucleus
cochlear implant. J. Acoust. Soc. Am. 102, 508–522
434 F. Zhao et al.
� 2008 The Authors
Journal compilation � 2008 Blackwell Publishing Ltd • Clinical Otolaryngology 33, 427–434

























![Introduction to hearing implairment & cochlear implantation]](https://img.pdfslide.us/doc/110x75/58707d261a28ab57368b58b9/introduction-to-hearing-implairment-cochlear-implantation.jpg)
