Embed Size (px)
Citation preview

The recognition and assessmentof acute pain in children1
Implementation Guide
March 2001
ISBN 1873853 99 8Publication code: 001 309
RCN Members £6.50Non RCN Members £8.50
1 Article 1 of the UN convention states: For the purposes of thepresent convention a child means every human being below theage of 18 years unless under the law applicable to the childmajority is attained earlier

The recognition and assessment of acute pain in children Implementation guide
AuthorsLesley Duff, Senior Research and DevelopmentFellow, Royal College of Nursing Institute, RCNI(until 2000)
Gail Louw, Lecturer in Nursing Management,Brighton University
Alison Loftus-Hills, Research Associate, RCNI
Clare Morrell, Senior Research and DevelopmentFellow, RCNI
ContributorsDuncan Courtney, Lecturer, University of Hull
Sarah Cox, Research Nurse, King’s College Hospital,London
Pat Doorbar, Social Researchers, Pat Doorbar andAssociates
Susan Fisher, Pain Specialist Nurse, The RoyalHospital for Sick Children, Glasgow
Noelle Llewellyn, Pain Specialist Nurse,Birmingham Children’s Hospital and Chair of theRoyal College of Nursing Pain in Children Network
Rachel Lewington, Social Researcher, Pat Doorbarand Associates
Liz McArthur, Clinical Nurse Specialist, Children’sPain, Alder Hey Pain Service, Royal LiverpoolChildren’s NHS Trust
Claire Palmer, Project Manager, ClinicalGovernance Support Service, Royal College ofPsychiatrists’ Research Unit
Tessa Woodfield, Research and DevelopmentFellow, Quality Improvement Programme, RCNI
Members of the Steering Group for theImplementation of Clinical Guidelines Modules
PublicationsIt is recognised that paediatric pain services aredeveloping all the time and the RCN pain seriespublications are important and useful resources foranyone involved in the development of paediatricpain services or the education of staff. Other titles inthis series include:
Recognition and assessment of acute pain in children– technical report. Publication code: 000 989. Priced £18.50 for RCN members and £23.50 fornon-members (plus £1.50 p&p).
Recognition and assessment of acute pain inchildren. Clinical practice guidelines. Publication code: 001 114.
Priced £5.50 for RCN members and £7.50 for non-members (plus £1.50 p&p).
Ouch! Sort it out: children’s experience of pain.Publication code: 001 113. Priced £5.50 for RCN members and £7.50 for non-members (plus £1.50 p&p).
All about pain. Publication code: 001 310. Free in, packs of five to RCN members, £5.95 tonon-members (plus £1.50 p&p for members andnon-members)
All of the preceding publications are available fromRCN Publishing Ltd, Distribution Depot, PO Box 1,Portishead, Bristol BS20 9EG. Tel: 01275 847180,9am – 5pm, Monday to Friday.
2
Published byRoyal College of Nursing20 Cavendish SquareWIG 0RN
© 2001 Royal College of Nursing. All rights reserved. No part of this publication may bereproduced, stored in a retrieval system, or transmitted in anyform or by any means electronic, mechanical, photocopying,recording or otherwise, without prior permission of thePublishers or a licence permitting restricted copying issues bythe Copyright Licencing Agency, 90 Tottenham Court Road,London W1P 9HE. This publication may not be lent, resold,hired out or otherwise disposed of by ways of trade in any formof binding or cover other than that in which it is published,without the prior consent of the Publishers.

The recognition and assessment of acute pain in children Implementation guide 3
Introduction 4
Step 1: Decide who will lead and co-ordinate the work 5
Step 2: Determine where you are now 6
Step 3: Prepare the people and the environment for guideline 7implementation
Step 4: Decide which implementation techniques to use to promote 12use of the clinical guideline in practice
Step 5: Pulling it all together - devise an action plan for 15implementation
Step 6: Evaluate whether your recognition and assessment of acute 16pain in children improved
Summary 17
References 20
Appendix 1 – Further reading 21
Appendix 2 - Outline audit plan 22
Appendix 3 - Methods for reviewing the readiness of the environment 27
Appendix 4 - Checklist: disseminating the clinical guideline 29
Appendix 5 - Local initiatives for the assessment of acute pain 30in children
Appendix 6 - Patient information 51
Appendix 7 - Examples of pain assessment scales 52
Appendix 8 - Summary of methods of disseminating and 76implementing guidelines
Appendix 9 - Summary of the impact of disseminating and 78implementing strategies
Appendix 10 – Completed action plan for implementing a clinical 80practice guideline
Contents

The recognition and assessment of acute pain in children Implementation guide
Introduction
A recent strategy for nursing states ‘it is for everynurse, midwife and health visitor to strive for qualityimprovement in all aspects of practice’ (Department ofHealth, 1999). This implementation guide forms part ofa set of booklets that provide guidance about howto develop and improve care for children who arelikely to experience acute pain. The guide sets out inpractical ways how to strive for quality improvementusing the clinical practice guideline for the recognitionand assessment of acute pain in children (RoyalCollege of Nursing Institute [RCNI], 1999).† Theguideline was developed by a multi-professional groupfrom research findings and the views of children,collected by a qualitative study (RCNI, 2000).†† Parentswere also involved in developing the guideline.
Decisions about health care are complicated forprofessionals and for children and their carers. Thepotential benefits and hazards of differentinterventions have to be considered against abackground of limited resources and varying needs.Given this complexity, there is increasing interestin clinical guidelines as a way of assisting decisionmaking. Clinical guidelines are developed usingsystematic reviews of research findings. Systematicreviews classify research studies by design and givean indication of the reliability and validity of theirfindings. A clinical guideline takes those findingsand turns them into an active document by making
recommendations for practice. The RCN PaediatricNurse Managers Forum are currently producing adocument called Developing an effective clinicalgovernance framework for children’s acute healthcare services, which is designed as a checklist to beused when considering the implementation of aclinical governance framework within children’sacute health care settings. Increasingly, patients’views are included in guidelines, which ensure thatpatients’ preferences are highlighted and thusincluded in clinical decision making.
As well as having clinical information thatidentifies best practice, it is also important that theenvironment of care promotes improvements in theway children’s pain is recognised and assessed. Tohelp determine what such an environment shouldlook like, the RCN Institute guideline includes aphilosophy for care of children (RCNI, 1999).
The following are six key principles that influencethe quality of care provided.
� Children are listened to and believed.
� Children and families are viewed as partners in care.
� Care is individualised and holistic.
� Care is family centred.
� A collaborative, multi-professional approach isprovided by knowledgeable professionals.
� Attention is paid to the organisational issues andsystems that enable effective pain managementto take place.
4
Describe current practice
Critically review the available evidence
Develop a standard objectiveand criteria
Disseminate thestandard and develop a
monitoring tool
Implement the criteria
Identify sources of data andmethods for sampling
Collect valid and reliable dataCompare results to the objective
Feed back to participants
Generate a team actionplan and implement it
Re-audit andevaluate
Enlist the support of allstaff involved
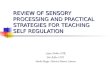
Figure 1 - The clinical audit cycle
† Royal College of Nursing Institute (1999) Clinicalpractice guidelines: the recognition andassessment of acute pain in children.Recommendations. London, RCN Publishing.
†† For a full description of the methods used to develop the guidelineplease see Royal College of Nursing Institute (2000) Clinical practiceguidelines: the recognition and assessment of acute pain in children.Technical Report. London, RCN Publishing.

This guide is designed to help you turn theguideline recommendations into reality. It aims toset out practical ways in which you can improvecare locally by implementing the clinical guidelinefor the recognition and assessment of acute pain inchildren. The clinical audit cycle provides a usefulframework for implementing guidelines andevaluating improvement. The audit cycle providesa systematic process for implementing guidelines,taking you through a range of activities to evaluatecare, plan and make changes and, finally, to re-evaluate care.
The guide follows this framework, describing theactivities involved as a series of six steps that leadto the implementation of a guideline. The clinicalaudit cycle is presented in Figure 1. Moving aroundthe audit cycle, and thus implementing clinicalguidelines, starts with involving the entire teamand finding the right leadership. The steps end witha re-evaluation of care and starting the cycle againto ensure that care is continually reviewed andimproved.
You may have been involved in clinical auditprojects before. Much time is spent in definingstandards or best practice. By using a clinicalguideline as a definition of best practice and anational audit tool to monitor, a great deal of timecan be saved. This enables the clinical team tofocus on the most important part of the audit cycle,taking action to implement the guidelinerecommendations to improve the service.
Preparing clinical guidelines for use in practice is acomplex undertaking. As well as taking youthrough the six steps to guideline implementation,the guide also describes a number of techniquesthat have been tried and tested to make the processeasier.
The guide takes you through the steps in turn,outlining things that you can do as you plan toimplement the guideline recommendations locally.The steps are illustrated with examples frompractice, which you will find in the appendices. Thesteps are intended to provide a flexible model,
recognising that organisations and teams will bestarting from different places. Wherever you arestarting from, we hope you find the guide useful asyou seek to improve the services your team is ableto offer locally.
Step 1: Decide who will leadand co-ordinate the work
The first step in implementing a clinical guidelineis to decide who will lead and co-ordinate thework. Successful behaviour change is usuallyachieved when people, who may not usually workin the same team, are brought together to achieve acommon goal. It is helpful, therefore, to set up amulti-professional group to lead and co-ordinatethe implementation of the guideline.
The group should include representatives ofeveryone who will be affected by the guideline.These people are often referred to as thestakeholders. Throughout this guide the groupleading on the implementation of the guideline willbe referred to as the implementation team.
Studies show that multi-professional work groupsachieve more when they have a facilitator (Harvey& Kitson, 1996). A facilitator is someone whoenables the group to work together to achieve itsgoals by attending to the group dynamics and theneeds of the participating individuals.
All members of the implementation team should beclear about their contribution to the group and tothe work involved in implementing the clinicalguideline. If roles and responsibilities are notagreed at the outset one or two people might takeon all the work thereby limiting the degree towhich others can feel involved and able toparticipate in the change.
Sharing the work will also make the tasks quickerand less onerous. The implementation team maythen carry out each step in the process ofimplementing the guideline themselves or mayenlist the support of others, for example, toconduct the clinical audit or to review theenvironment.
Identify a facilitator
Identify the stakeholders
Set up a group of stakeholder representatives tolead implementation of the guideline
Six steps to improve the recognition and assessment of pain in children
Step 1 Deciding who will lead the work
Step 2 Determining where you are now
Step 3 Preparing to implement the guideline
Step 4 Identifying techniques to assist you
Step 5 Devising an action plan
Step 6 Evaluating your progress
The recognition and assessment of acute pain in children Implementation guide 5

The recognition and assessment of acute pain in children Implementation guide
It is also important for the implementation team toagree what it wants the clinical guideline toaccomplish. Members may otherwise disagreeabout priorities and feel confused and disillusionedif their expectations are not met.
Step 2: Determine where youare now
To effectively prepare to implement a clinicalguideline you first have to know what changes areneeded, whether the organisation is ready to makethem and what resources you have to supportthem. That is, you need to evaluate current clinicalpractice to find out the degree to which careconforms with that recommended by the guideline.In addition, you need to review the environment tofind out how ready health professionals andpatients are to implement the guideline and whatsystems and structures are already in place, or areneeded, to support any changes required.
Evaluation of clinical careThe degree to which current care conforms to theguideline recommendations and what changes areneeded can be determined by measuring practice,sometimes referred to as a local audit.
Measurement is undertaken using a set of criteriaagainst which care is compared. A set of resourcesfor audit is currently being developed. Theseresources will form part of the set of documentsdesigned to help you implement and evaluate theimpact of the clinical guideline for the recognitionand assessment of acute pain in children. Asummary of the aspects of care that you mightusefully audit is provided in an outline audit planin Appendix 2. There are three stages in measuringthe quality of care:
� collecting audit data
� collating audit data
� summarising audit data.
During the audit you need to evaluate differentaspects of the care you provide including the
resources that are available (structure), the actionsand decisions you take in practice (process) and theoutcomes of care (outcomes). The audit planpresented in this guide focuses on the actions thattake place in clinical practice and some of theoutcomes that result from those actions. You mayalso want to ask questions to find out whether youhave all the resources, staffing and materials thatyou need to achieve the clinical guideline.
The audit should focus on evaluating whether andhow children’s acute pain is recognised andassessed. It is also important to find out whatchildren and parents think about the serviceoffered. Guidance notes on involving children,parents and other carers in the evaluation of theservice are being prepared as part of the series onimplementing the clinical guideline for therecognition and assessment of acute pain inchildren. These will be included within the set ofresources for audit.
Review the environmentReviewing the environment involves finding outmore about the people who will be affected by theproposed changes. For example, is everyonereceptive to the guideline and willing to use it inpractice? Does anyone need extra education ortraining to be able to provide care asrecommended? What kind of education or trainingwould be most useful to people from differingbackgrounds and where should it be provided?
Review of the environment also involves findingout what systems and structures there are in placewithin the organisation to support implementationof the guideline. There is a section within the auditplan to help you address these issues.
Example
At the Royal Hospital for Sick Children in Glasgow, theclinical nurse specialist audited the knowledge ofnursing staff on the analgesic techniques used in thewards and units. The audit pinpointed that there was alack of knowledge about the range of techniques thatcan be used. A teaching programme was then set upwhich concentrated on these areas. A variety ofmethods were used including: bedside teaching;formal and practical tutorials; lectures (within andoutside the hospital); and information handouts andleaflets. These methods were chosen to capitalise onopportunities for teaching as they presentedthemselves and to enable more detailed backgroundinformation to be given to nurses as well as morehands-on skills.
Play therapists and other staff also requested tutorialsfrom the pain relief service, particularly about the useof non-pharmacological analgesic techniques.
Measuring current clinical practice
Agree the purpose of the clinical guideline
Clarify and agree the roles andcontributions of all group members
6

The recognition and assessment of acute pain in children Implementation guide
Who will be influenced by the clinicalguideline?
As well as the stakeholders involved in theimplementation team, there may be otherindividuals who need to be included and accountedfor in your strategy and plan. Many people withinor external to the organisation may influence theimplementation process including: fundingorganisations, health care professionals with theirown ideas, community health councils (in England)and other similar representative bodies andrepresentatives of children, their parents and othercarers. For example, you might like to includesomeone from the charity Action for Sick Children.
Receptivity to the guideline
Knowing who will be affected by the clinicalguideline and how they are likely to respond to itsintroduction should help you tailor the way inwhich the clinical guideline is implemented locally.Also, it may be helpful to think about how changesto clinical practice have been handled in the past.As well as helping you understand people’sexpectations, finding out about previous attemptsat managing change (successes and failures) willhelp you select the most suitable methods forimplementing the clinical guideline.
It may be helpful to talk to clinical audit staff,information specialists, medical records staff,contract managers, local healthcommission/authority/board, quality managementstaff and so on when you evaluate clinical practiceand review the environment. It could also behelpful to talk to people who have experience of
working in project groups, staff responsible for caretraining, development managers and children,parents and other carers.
Systems and structuresConducting a review of the structures and systems ofthe organisation into which the clinical guideline willbe introduced allows you to identify what aspects ofthat organisation will help you implement it andwhat aspects are likely to hamper you. Identifyingthese features means you can take action toovercome difficulties and to capitalise on thestrengths. You will then be able to plan how toprepare the organisation and the people who workwithin it to implement the clinical guideline. Forexample, does the organisation have an efficientmechanism for communication between itsemployees or will you need to set up something new?
Reviewing the environment is a complex goal.However, there are a number of tools that can beused including the SWOT analysis and the Fishbonediagram. Examples of these are included inAppendix 3.
Step 3: Prepare the peopleand the environment forguideline implementation
Preparing the peopleThere are two purposes in preparing people toimplement a guideline. Firstly, to ensure that theyare receptive to the clinical guideline and knowhow to use it and secondly, that they have theclinical skills and knowledge to carry out care asrecommended in the guideline - this is absolutelycrucial to your success in implementing theguideline.
Improving people’s receptivity to the clinicalguideline
Some of the people who will be affected by theclinical guideline will support its implementationand others may oppose it. Lots of people willprobably be indifferent. Health care professionals
Identify the systems and structures youneed to support implementation of theguideline
Find out what people think about theclinical guideline
What do health professionals know about theguideline recommendations?
Do children, their parents and carers have thesame views as professionals?
What are the implications of any differencesbetween professionals and children, their parentsand carers?
How do you think the introduction of thechange will be received?
Decide who should be involved in theimplementation of the clinical guidelines
When should they get involved?
To what extent should they become involved?
7

The recognition and assessment of acute pain in children Implementation guide
and children, their parents and carers, may reactdifferently to the proposed changes. Some peoplemay feel that the care provided is already the bestpossible, others may cling to outmoded practices,despite knowing that other practices are moreeffective. It is important to be aware of the views ofall the people who may influence theimplementation of the guideline and then to makeplans to either capitalise on their support or to limitthe amount to which they can sabotage progress.
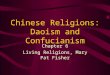
Block (1991) suggests that classifying people into oneof four groups can be a useful way of assessing whois likely to be enthusiastic about introducing aclinical guideline and those who will be morereluctant. Block classifies people as bedfellows, allies,adversaries and opponents. The willingness of eachgroup to change is summarised in Figure 2 below.
Allies are people who both support yourimplementation agenda, and in whom you havehigh trust. On the positive side, you can mobilisethem to support your aims, but on the negative sidethey will not necessarily challenge your view andhelp to create new perspectives. These people aresimilar to those described as ‘opinion leaders,’ or‘product champions’ and they can be found at anylevel within the organisation. A definingcharacteristic is their influence and credibilityrather than their status or rank.
Opponents are those people in whom you havegreat trust, but who do not necessarily share youraims. These individuals are useful because theyprovide a sounding board for your ideas and plans,and they can be counted on not to block your aimsunfairly or without notice. However, if you do notdeal with opponents openly, the trust you sharemay be eroded and they may become adversaries.
Bedfellows are those people whom you are not ableto trust fully. This is probably because you do notknow them very well, or because in the past yourdealings with them have been at arm’s length. Theydo, however, share some of your aims. Theseindividuals are useful because they can be includedin the implementation of the guideline by inviting
their involvement, seeking their opinions, and bydeveloping appropriate working relationships inwhich they feel able to trust your aims.
Adversaries are those people whom you feel unableto trust and who do not share your commitment toguidelines.
Fence-sitters are those people who neither agree nordisagree with your aims and in whom youconsequently have little trust. Block (1991)characterises these as the archetypal bureaucrat, theperson who always plays safe and takes refuge in therules. On the positive side, they generally encouragereview and debate but are reluctant to committhemselves. To counter this, Block suggests askingwhat they need for them to offer their support.
Here are some suggestions about how negativeattitudes to clinical guidelines can be tackled:
� explain what clinical guidelines are AND whatthey are not
� explain the implications of the guideline, howthe organisation is contributing to its successfulimplementation, and what is expected of staff
� demonstrate why a clinical guideline is needed,what its benefits are and how it can improve care
� be honest about the advantages anddisadvantages of the clinical guideline
� find out the myths and legends surroundingclinical guidelines and clarify the ways in whichthey threaten professionals and patients, thenoffset these with their advantages
� agree to review the use of the clinical guidelineand its impact on care and working practicesafter a set period.
A key factor in improving people’s receptivity to aclinical guideline is to make sure that everyone isaware of its existence, what it involves and itsbenefits. It is helpful for people to be given thechance to think about and comment on plans forimplementing the guideline before any changestake place in practice.
This two-way communication allows health careprofessionals to advise the implementation teamabout anything to do with the children they workwith, or their environment, skills and knowledgethat might influence the implementation of theguideline. It will also help share ideas about howdifficulties in implementation can be overcome andto encourage one another.
Plan activities to overcome negativeattitudes to clinical guidelines
Figure 2
High agreement Bedfellows Allieswith guidelines
Low agreement Adversaries Opponentswith guidelines
Low trust High trust
Identify your supporters and the possiblesaboteurs
8

The recognition and assessment of acute pain in children Implementation guide
To make sure that everyone is aware of the clinicalguideline and what its recommendations mean forpractice it is important that it is widely disseminated.A common reason why clinical guidelines are notused is that the intended audience has never heard ofthem (Gupta et al, 1997; Tunis et al, 1994).Dissemination and consultation will be promoted byan effective communication strategy. Appendix 4provides you with an example of a checklist that youcan use to identify everyone who should receive acopy of the clinical guideline. In addition, there maybe other people who should know that the guideline isbeing implemented. It is useful to list the members ofthis second group to ensure that no one is forgotten.
A communication strategy needs to take account ofthe following:
People
� all those who are influenced by the clinicalguideline
� all those who will use it in practice
� the ‘gatekeepers’ through which information ischannelled. For example, to get information tostaff nurses do you need to go through wardmanagers?
What makes information about theguideline more accessible for differentindividuals or groups?
� vary the media of presentation rather than onlyusing paper formats. For example, use visualrepresentation of the guideline or audit results
� use different settings, for example, presentations,meetings, educational, administrative, hand-overmeetings, ward rounds, social
� use information technology
� use incentives that highlight and ‘sell’ theguideline
� use different methods for different individualsand groups
� promote the credibility and rigour of the clinicalguideline.
Evaluation
� how will you know that everyone who needs tohear about the clinical guideline has done so?
� how can you collate and feedback ideas aboutimplementing the guideline?
A wide range of methods have been used todisseminate information within health servicesettings. It may be helpful to think of thestakeholders you previously identified as different‘audiences’ for information. Each audience mayrespond differently to the dissemination methodsused. Therefore, your dissemination strategy mayneed to vary for each one. For example, making apresentation to one group and sending a newsletterto another. Strategies may also vary by whether thetarget audience is a group of allies, adversaries,bedfellows or opponents.
Example
Local guidelines were developed for analgesia inchildren by a team in Oxford. Following completion ofthe guideline, it was decided to present them at alaunch evening using a group educational approach.The evening was advertised in all departments involvedin the care of children.
About 25 people attended the evening event, mostlystaff from the Children’s Unit. The organisers reportthat they were disappointed that few colleagues fromother departments participated, particularly medicalstaff. However, with some members of otherdepartments present, the organisers felt that the eventprovided a good chance for multi-professionaldiscussions. The format of the evening was designed toencourage such discussion. The evening began with abuffet dinner to ensure the event was perceived as asocial occasion. The guidelines were then presentedand the participants were split into small groups whoworked together to solve problems presented inscenarios by using the clinical guidelines. This methodencouraged staff to become familiar with actuallyapplying the guidelines. Feedback from the eveningshowed that the problem-solving scenarios were asuccessful way of helping them to become familiar withthe guidelines and how to use them.
The low turn out of medical staff at the evening meetingmeant that alternative methods had to be found toensure they knew about and received the guidelines.Heads of departments were asked to circulate theguidelines. Some carried out further presentations forparticular groups of staff considered to be crucial to thesuccess of the guidelines – for example, anaesthetists.The presentations were well received and feedbacksuggests that the guidelines have been warmly welcomedas an aid to the management of paediatric pain. A formalaudit will provide information about the impact of theguidelines on practice.
Devise a communication strategy to supportimplementation of the clinical guideline
Change or add to systems and structures toenable effective organisation-widecommunication
Communicate plans to implement theclinical guideline to everyone affected
9

The recognition and assessment of acute pain in children Implementation guide
Ensure professionals have the skillsand knowledge to make changes toclinical care
The clinical management of children’s pain isusually provided by paediatric nurses, painspecialist nurses, community children’s nurses,doctors and parents. However, other health careprofessionals may also be involved in assessingand managing children’s pain, for example, staff inA&E, play therapists, physiotherapists, generalpractitioners.
The recognition and assessment of acute pain inchildren is specialised work, requiring in-depthknowledge about causes of pain, how children ofdifferent age groups and levels of developmentexpress pain and the use of pain assessment tools.For the guideline to be successfully implementedeveryone in the team and, importantly, parentsneed to have the knowledge and skills toimplement the guideline recommendations.
You may wish to liaise with a local educationprovider to obtain clinical training on therecognition and assessment of children’s pain forthe health care professionals in your team.However, you should bear in mind that differentprofessional groups may be more responsive totraining if it is offered outside their usual place ofwork and if it carries some reward in the form of,for example, continuing education points.
A number of areas have educational initiatives toimprove the clinical care of children likely toexperience pain. Examples of local initiatives can
be accessed through the contact names provided inAppendix 5. Such examples can give you goodideas about educating and supporting professionalsto recognise and assess acute pain in children inline with the guideline recommendations.
Further help and advice on managing pain inchildren is available from the RCN Pain in Childrennational forum (enrolment code 1227). The forumaims to enable nurses to provide effective, efficientand holistic care to children (from birth throughchildhood and adolescence) who are likely toexperience pain, whatever the duration, origin or setting.
If you are an RCN member and would like to jointhe forum, a form is available on the RCN web site:www.rcn.org.uk or alternatively contact RCN Directon 0845 772 6100. Additionally, forms are sent outto members with membership renewal packs.
Preparing children and parents (orother carers)Children, their parents and other carers must beinvolved in planning how the clinical guidelinewill be used to make sure that their preferences and views are to be included in the decision-making process. Involving children and parentscan also ensure that they understand the reasonsfor the care they receive and their contribution toits success. For example, children may be more willing to complete a pain scale if they understandthe reasons why and if they believe that it is a wayof ensuring that they receive pain relief.
How can children and parents be preparedto complete pain scales?
Do nurses have the skills and knowledge toexplain pain scales and the assessment ofpain to children, their parents and carers –how can they be developed?
Prepare nurses to educate children andtheir parents and carers about theimportance of expressing pain
Prepare information leaflets about theclinical guideline for children, theirparents and carers
Do the nurses need to know more abouthow to recognise and assess acute pain inchildren?
How can you ensure they have the clinicalskills and knowledge that they need toimplement the guideline?
Provide an agreed education programmeto ensure professionals have the skills andknowledge they need to implement theguideline
Set up a system for clinical supervision toensure clinical practice is in accordancewith guideline recommendations
10

The recognition and assessment of acute pain in children Implementation guide
A children’s version (All About Pain RCN, 2000) ofthe clinical practice guideline The Recognition andAssessment of Acute Pain in Children (RCNI, 2000)is available. You may choose to adopt thispublication or adapt it to suit the needs of thechildren that you care for.
The preparation of written materials for use bypatients, especially children, is a skilled task. It canbe helpful to look at information leaflets that othergroups have prepared. In Appendix 6 you will findcontact details and sources of guidance aboutdeveloping patient information and informationfor children.
You might want to consider setting up some studydays on how to communicate effectively withchildren, their parents and carers. Details aboutwhere to find communication workshops can befound in Appendix 6.
Prepare the environmentTo implement many clinical guidelines, structuresand systems have to be changed. For example,pathology test order forms, outpatient clinicappointment letters or computer systems mayhave to be altered. Systems may have to becreated, such as the inclusion of reminders inchildren’s notes or teaching sessions for clinicalstaff. The structures and systems you alreadyreviewed and set up to support theimplementation of the clinical guideline will helpidentify what else is needed.
In addition, a number of resources may be requiredto enable the clinical guideline to be implemented.Such resources include:
� pain assessment tools (see Appendix 7)
� documentation for recording assessments andnoting observations (see Appendix 5)
� pain history documentation (see Appendix 5).
The main resource that you will need is a pain tool,or a set of pain tools, to assess children’s pain. Youwill probably need a set of scales because it is likelythat you will care for children of different ages, atdifferent levels of development and possibly fromdifferent cultural backgrounds who may evenspeak different languages.
Choosing the right pain assessment tool for yourarea is important. Key characteristics to look forare:
� the reliability and validity of the tool are knownto be acceptable for the group of children withwhom you plan to use it. These characteristicsare really important so you can be confident thatthe tool does the job you need
� the tool is applicable to your clinical area
� the tool is simple to use. Again, this is importantif you are to encourage staff to use a painassessment tool on a regular basis
� the tool is appealing to children. If children arenot attracted to the tool it will be more difficultto persuade them to use it.
To help you review the available tools, the keycharacteristics of a number of pain assessment toolsare summarised in Appendix 7. Many areas adapttools to fit their own circumstances. Whilst this canbe a helpful way of encouraging professionals tofeel that they own a tool and that it fits with theirclinical area, care must be taken not to alter theproperties of a tool. Where possible it is advisable touse tools in the format in which they are published.To help you do that, a number of commonly usedscales are also reproduced in Appendix 7. Thereliability and validity of tools are influenced by theway they are used. It is important, therefore, thatthe pain assessment scales are used in the way
Do you need to create new systems andstructures to implement the guideline?
Who do you need to involve in creating them?
Do you have the resources you need, inparticular a pain assessment tool?
Examples
Research demonstrates the importance of parentsfeeling they receive adequate information about theirchildren’s pain management (Finley et al, 1996; Sikichet al, 1997; Watt-Watson, et al, 1990). The RoyalHospital for Sick Children in Glasgow addressed thisissue by producing a series of leaflets about thedifferent types of analgesia which children mightreceive. In addition, when members of the pain reliefservice visit the children they include parents in theirdiscussions with the children. As a result of this activityan audit found that all 29 parents who were asked saidthe visits were helpful.
As shown by the following quotes, children also are keento receive information and to be included inassessments of their pain (Doorbar & McClarey, 1999).
“I have a bad pain in my back. I should be able to saywhen I need something not the doctor!”
“He said it would hurt and it did, I trust him”
“The anaesthetist explained it good so it was all right!”
11

The recognition and assessment of acute pain in children Implementation guide
recommended by their authors. Where possible,instructions for the use of scales are included withthe tools reproduced. The list of references on pages66-71 also includes examples of the use of thescales described in Appendix 7.
Step 4: Decide whichimplementation techniquesto use to promote use ofclinical guidelines in practice
This section outlines a range of techniques, whichhave been used to implement changes in practice inhealth care settings. Research findings show that itis important to use a variety of implementationmethods and to integrate them with a strategy forchange (NHS Centre for Reviews and Dissemination[CRD], 1999; Dunning et al, 1997; Grimshaw andRussell, 1993; Thomas et al, 1998).
Traditionally, education and training have beenused to change the behaviour and practices ofhealth care professionals, to inform and convincepeople about the need to change and to ensure thatthere is consistency in care provided. However,knowledge and information by themselves are notenough to persuade people to change theirbehaviour (Freemantle et al, 1997). Instead othermethods and techniques also need to be usedincluding education, social influence, facilitation,audit, sanctions, marketing and reminders.
Appendix 8 provides a brief overview of studiesthat examine the effectiveness of methods todisseminate and implement guidelines. You mayfind this information helpful in selecting themethods you will use in your implementationstrategy. Various factors such as the targetaudience, the educational influence and practicalconsiderations for each implementation techniqueare outlined in Appendix 9.
Education and trainingTo implement the clinical guideline it is importantto provide education and training to everyonewithin an organisation so that they understand:
� the benefits of clinical guidelines
� how and why they are developed
� what is needed to implement guidelines, in thiscase the recognition and assessment of acutepain in children guideline
� the content of the guideline and how it applies
� what they are being asked to do with theguideline
� how they can use the guideline
� how they can monitor its use and ensure that thecare of children improves.
Education may also be required by those staffneeding to develop clinical skills relevant to theguidelines. It is more likely to be effective when itis tailored to the needs of the individuals concernedand opportunities for small group discussion areprovided. Education is also more likely to beeffective if it is combined with another activity, forexample, audit and feedback.
Education alone may be sufficient to achieveguideline implementation with those you haveidentified as being your keen supporters, but isunlikely to achieve guideline implementation withother groups. As we all know, people reactdifferently to change.
An alternative strategy is to use techniques thatwork by using social influence (Mittman et al,1992). Social influence techniques include clinicalleadership, opinion leaders, product champions,peer support, clinical audit and feedback andrewards.
Clinical leadershipMuch of the literature on guidelineimplementation, as well as that on qualityimprovement, stresses the need for gaining thesupport of influential and/or senior colleagues forany changes proposed. It is important to getsupport from senior colleagues even where thedevelopment and implementation activity ismanaged as a ‘bottom-up’ process. To enlist the
Devise and agree an education programmefor the health professionals you work with
What would the aims of an educationalinitiative be?
What type of education is likely to be mosteffective?
How would the education be delivered? Bywhom? When?
What other techniques can be usedalongside the education you provide?
12

The recognition and assessment of acute pain in children Implementation guide
support of key people you need to identify theobvious leaders within your organisation, forexample, locality managers, clinical directors,clinical leaders, nursing leaders, generalpractitioners, practice managers, chief executives.These people can then be targeted withinformation.
Opinion leadersOpinion leaders are influential, respectedindividuals who are experts in their chosen field(Lomas et al, 1988; Rogers, 1995). When comparedto their peers, opinion leaders tend to have a highersocial status, are more innovative and tend to bethe centre of an interpersonal network. Opinionleaders encourage others to use new informationby using it themselves, thus setting an example andcreating new implicit or explicit social norms.Opinion leaders are highly visible and areaccessible to others because of their extensiveinterpersonal networks. This enables their influenceto travel beyond their immediate clinical team.
Product championsSome individuals literally ‘champion’ a productand ‘sell’ it to their colleagues (Stocking, 1985). Theamount of time that the product champions putinto supporting an innovation is directly related tohow well it is implemented.
Once you have identified who the opinion leadersand product champions are in your team andorganisation, think about how to enlist their help in
implementing the clinical guideline. What is itabout the clinical guideline that will appeal tothem?
� Might it save money?
� Might it reduce the chances of litigation?
� Does it relate to targets set by commissioners orthe health authority?
� Does it address a personal interest?
� Is it a guideline recommended by a royal collegeor other professional organisation?
� Do children like the guideline? Is itrecommended by parents?
Peer supportPeople commonly learn and formulate newopinions through discussion with their peers andare influenced by opinion leaders within theorganisation (Mittman et al, 1992). For example,nurses may want to talk to others in their groupabout the implications of the guideline to helpthem decide whether to use it. They will ask eachother questions such as:
� is the guideline valid?
� does it apply to the work we do and the patientswe see?
� will it improve practice or may it have a harmfuleffect?
These conversations often happen in socialsituations, for example, whilst taking the lift or inthe staff canteen, and often have a great influenceon people’s decision-making. It has been arguedthat this social influence may be the biggest factorin whether a new initiative is implemented.Providing opportunities for discussion is, therefore,likely to have a beneficial effect on the adoption ofthe guideline. Discussion can be incorporated intoeducation sessions, team meetings andpresentations.
How can support for the clinical guidelinebe obtained from opinion leaders andproduct champions?
What activities can they undertake for/withyou to promote acceptance and use of theguideline?
Identify the ‘opinion leaders’ and ‘productchampions’ in your clinical team and/ororganisation
Who else has influence over the opinions ofthe health professionals and children, theirparents and carers, whom you work with?
Which senior or managerial people shouldagree the implementation of the guideline?
How can you enlist their support?
How can you demonstrate to others in theorganisation that you have the support ofthe senior and managerial people for theproposed changes?
13

The recognition and assessment of acute pain in children Implementation guide
Feedback and rewardManagement theorists and psychologists describehow important it is for us to achieve and for othersto recognise our achievements. Achievement andrecognition motivate us and give us the confidenceto continue to perform well and to develop further,to try new things and to perform even better. A keypart of an implementation strategy is reward andcelebration.
How can your achievements be recognisedand rewarded?
Positive results from clinical audit demonstrateachievements. There may be opportunities tocelebrate these at routine team meetings, to tellothers about the achievements through theorganisation’s internal communications systems, orat one-off events. Internal or external rewards oraccreditation schemes can also be used.Recognising and rewarding success not onlymotivates those already involved in implementinga guideline, but it also acts as a marketing devicefor those who remain sceptical. Benchmarking mayprovide a useful structure for this process (Ellis &Morris, 1997). This is described in Step 6.
As well as social influence techniques there are alsoa number of other practical steps that you can taketo improve implementation of the clinicalguideline. These include the use of recordingsystems and care pathways.
Recording systemsIncorporating the recommendations of a clinicalguideline into the systems you use to recordclinical information can be a powerful way ofreminding yourselves to adhere to the guideline.Recording systems can also be helpful inpromoting a systematic approach to clinical careand the recording of information. Examples of theuse of patient records as a memory prompt areprovided in Appendix 5.
Integrated care pathwayIntegrated care pathways (ICPs) present a plan forthe clinical management of patients with aparticular condition that specifies the optimumcourse of events to happen within a set time-scale.They are developed by local multi-professionalteams and may be based on, or include,recommendations from clinical guidelines.Variations from the pathway are documented and the reasons for the variations analysed.Avoidable variations from the pathway can beaddressed and changes made to the pathway ifnecessary.
Having reviewed the range of techniques that youcan use to encourage people to use the clinicalguideline in practice, now you need to decidewhich ones will be most useful in your locality.
Decide which combination of techniques is mostsuitable for implementing the clinical guidelinewhere you work.
To help you decide which techniques to use, reviewthe issues raised above. This information gives youinsight into the people who will be implementingthe guideline and the environment in which theyare working. As well as helping you plan how bestto prepare professionals, children and parents, andthe environment for guideline implementation, theinformation also helps you identify whichtechniques will be most effective. Using theinformation that you have about your localitythink about:
� which implementation techniques are mostattractive?
� which are most feasible?
� what are the resource implications of each idea?
� are some ideas more suitable for some of thegroups of people you work with than others?
� are some ideas more suitable for different stagesof the work?
� how effective (based on the knowledge you havegained whilst working through this guide) doyou think the different techniques will be?
You will probably want to use different techniquesat different stages in the process of implementingthe guideline. For example, in the early stages,
Can any of your patient record forms beused or re-designed for use as reminders toprofessionals about implementing theguideline recommendations?
Identify activities and events that you canuse to promote the guideline
How can you capitalise on social situationsto get your messages to professionals andchildren, their parents and carers?
How can you make formal situations moreenjoyable and memorable?
14

The recognition and assessment of acute pain in children Implementation guide
techniques that promote people’s awareness of theguideline will be most useful. Later, you will needto use techniques that encourage and maintainguideline use. Whatever techniques you decide touse, success is more likely if you ‘mix and match’them according to the group, or groups, into whichyou are introducing the guidelines.
Jot down your ideas about implementation. Have you:
� identified everyone who will be affected by theguideline?
� used a range of different techniques for eachgroup?
� chosen techniques according to how ready thegroup members are to implement the guideline?
� chosen techniques that suit the differentbackgrounds and preferred learning styles of allyour target groups, for example, children,parents, nurses?
� included a technique which addresses educationand information provision?
� included a technique which makes use of socialinfluences?
� considered the different techniques you will useover time?
� considered and addressed the practicalimplications of the techniques you haveidentified?
� considered the cost implications of eachtechnique?
� Identified which techniques are realistic andachievable?
Step 5: Pulling it all together– devise an action plan forimplementation
The answers to the questions posed during thisguide provide you with the information that youneed to devise a strategy for improving care locally.The final parts of developing the strategy areorganising the information into a set of sequentialactions, allocating each action to a namedindividual (or individuals) and setting targets anddeadlines for each activity – this will turn yourstrategy into manageable activities in the form ofan action plan.
An action plan needs careful consideration. Foreach issue identified you will need to consider:
� the appropriate course of action - havingidentified the priorities for action these need tobe clearly documented and broken down intosteps if necessary
� a named person responsible for the action - it isimportant that the group identifies a namedindividual/s to be responsible for leading or co-ordinating each of the actions specified. Most ofthe clinical audit group will have responsibilityfor some aspect of the plan depending on theirparticular skills and the group that theyrepresent. Agree how that named person will besupported and by whom
� the time-scale for action - the group need todetermine how long they need to implementeach of the actions identified. This depends onthe nature of the problem and the type of actionrequired. Short-term actions are those which canbe remedied almost immediately, in less than sixweeks. Medium-term actions require a longerperiod of up to six months to implement, whilelong-term actions are those which will take morethan six months to achieve
� contingency plans - what problems might youencounter? How will you deal with problemsshould they arise? For example, are you preparedfor annual leave by staff, maternity and sick leave?
A worked example of a comprehensive action planis shown in Appendix 10. You may of course haveyour own approach to project planning which youwould rather use.
To ensure that your action plan will be effectivecheck it against the following criteria:
Is the timetable realistic?
Have you communicated your plans toeveryone involved in implementing theguideline?
Have you found someone to co-ordinatethe work?
Who will ensure the work has been done?
How will all those affected by the work bekept informed?
Who will monitor variance from the actionplan?
Have you made contingency plans?
15

The recognition and assessment of acute pain in children Implementation guide
Once the strategy is agreed and you have an actionplan you are ready to implement the guideline.
Step 6: Evaluate whetheryour recognition andassessment of acute pain inchildren improved
The ongoing task is to re-audit and to see whethercare has improved in comparison with yourprevious results. Clinical audit is a continuousprocess and you will need to continue to measurepractice against the audit criteria at regularintervals. You may choose to monitor care morefrequently to track your progress as care isimproved.
As a part of your clinical audit programme youmay wish to consider internal benchmarking (Ellis& Morris, 1997). Quality improvement occurs bycomparison between teams, and sharing howresults were achieved. Internal benchmarking mayprovide a useful first step to benchmarkingbetween trusts. In this way, once health care teamshave collected their data, results are sharedinternally, across the trust.
Trust comparisons can be particularly helpful forareas in which there is only a single ward or unitspecialising in the care of children. A particularward or unit may score highly on one criterion, forexample, use of a pain assessment tool. The staffmight then take on a role of sharing their practiceand supporting others within the trust. Those withhigh scores could then share their practice withother groups across the region. A network of thosewithin similar settings, such as clinics andcommunity, could be formed to share best practiceand support development.
It is vital that you establish a programme of regularclinical audit in order to maintain the highstandards you achieve. As staff change and otherissues compete for people’s attention, it is easy tolose the momentum necessary to sustain clinicalexcellence.
Re-audit
Feedback the results to healthprofessionals, children and parents
Celebrate
Consider internal benchmarking
Identify further improvements to care
Devise a new action plan
Plan a programme of regular clinical audit
16

Summary
Step 1: Decide who will lead and co-ordinate the work
The recognition and assessment of acute pain in children Implementation guide 17
Step 3: Prepare the people and theenvironment for guidelineimplementation
Step 2: Determine where you are now
What knowledge do healthprofessionals have about theguideline recommendations?
Find out what people think about theclinical guideline
How much should they get involved?
When should they get involved?
What are the implications of anydifferences between professionalsand children and their parents?
Identify the systems and structuresyou need to support implementation
of the guideline
Do children and their parents andcarers have the same views as
professionals?
Identify the stakeholders
Set up a group of stakeholderrepresentatives to lead
implementation of the guideline
Identify a facilitator
Clarify and agree the roles andcontributions of all group members
Agree the purpose of the clinicalguideline
Measure current clinical practiceusing the audit protocol
Decide who should be involved in theimplementation of the clinical
guidelines
Identify your supporters and possiblesaboteurs
Plan activities to overcome negativeattitudes to clinical guidelines
Devise a communication strategy tosupport implementation of the
clinical guideline
Change or add to systems andstructures to enable effective
organisation-wide communication
Communicate plans to implementthe clinical guideline to everyone
affected
Do the nurses and other healthprofessionals need to know more about
how to carry out the clinical caredescribed in the guideline, for example,
using a pain assessment tool?
How can you ensure they have theclinical skills and knowledge that
they need to implement theguideline?
How do you think the introduction ofthe change will be received?
Agree standards of education

The recognition and assessment of acute pain in children Implementation guide18
Agree methods for supervision ofpractice
How can children and parents beprepared and encouraged to express
their pain and to use painassessment tools?
Do nurses have the skills andknowledge to explain the use of paintools to children and parents - how
can they be developed?
Prepare nurses to educate childrenand their parents and carers about
how to use pain assessment tools andthe importance of expressing pain
Prepare information leaflets aboutthe clinical guideline for use bychildren and parents and carers
Do you need to create new systemsand structures to implement the
guideline?
Who do you need to involve increating them?
Step 4: Decide which implementationtechniques to use to promote use of theclinical guideline in practice
Agree standards of education for allprofessionals involved
What would the aims of aneducational initiative be?
What type of education is likely to bemost effective?
How would the education bedelivered? By whom? When?
What other techniques can be usedalongside the education you provide?
Which senior or managerial peopleshould agree the implementation of
the guideline?
How can you enlist their support?
How can you demonstrate to othersin the organisation that you have thesupport of the senior and managerial
people for the proposed changes?
Who else has influence over theopinions of the health professionalsand children and parents and carers
you work with?
Identify the ‘opinion leaders’ and‘product champions’ in your clinical
team and/or organisation
How can support for the clinicalguideline be obtained from opinion
leaders and product champions?
What activities can they undertakefor/with you to promote acceptance
and use of the guideline?
Provide education to ensureprofessionals have the skills and
knowledge they need to implementthe guideline
Do you have the resources you need, forexample, documentation for recording
pain histories, prompts for painassessment scores on temperature,
pulse, respiration charts?
Identify activities and events thatyou can use to promote the guideline
What type of education about theguideline and the clinical care it
represents do the people you workwith require?

The recognition and assessment of acute pain in children Implementation guide 19
How can you capitalise on socialsituations to get your messages toprofessionals, children and their
parents and carers ?
How can you make formal situationsmore enjoyable and memorable?
Review the results of your audit ofthe recognition and assessment of
acute pain in children
Feedback and discuss the resultswith everyone involved in the audit
Identify opportunities forimprovement
Prioritise the improvements
Devise an action plan - guidelinesare easier to implement when people
can clearly see that care does notcompare well with that
recommended
Take action
Re-evaluate to find out whether carehas improved
How can your achievements berecognised and rewarded?
Try to devise a patient record formthat can be used to remind
professionals to implement theguideline recommendations
Step 5: Pulling it all together - devise anaction plan for improvement
Is the timetable realistic?
Have you communicated your plansto everyone involved in
implementing the guideline?
Have you found someone to co-ordinate the work?
Who will ensure that the work hasbeen done?
How will all those affected by thework be kept informed?
Who will monitor variance from theaction plan?
Have you included contingencyplans?
Step 6: Evaluating your progress
Re-audit
Feedback results to healthprofessionals, children and their
parents and carers
Celebrate
Identify next improvements
Devise new action plan
Consider internal benchmarkingDecide which combination of
implementation techniques is mostsuitable for implementing the
clinical guideline where you workEstablish a programme of regular
clinical audit

The recognition and assessment of acute pain in children Implementation guide20
References
Block, P. (1991) The empowered manager: positivepolitical skills at work. San Francisco, Jossey Bass.
Clinical Guidelines Resource Pack Steering Group(in press) Implementing national clinical guidelines- a resource pack. London, Baillière Tindall.
Dopson, S., Gabbay, J., Locock, L., Chambers, D.(1999) Evaluation of the PACE Programme: FinalReport. Oxford Healthcare Management Institute,Templeton College, University of Oxford andWessex Institute for Health Research andDevelopment, University of Southampton.
Doorbar, P., McCarey, M. (1999) Ouch! sort it out:children’s experiences of pain. Report of aqualitative study of children’s experience of pain.London, RCN. Publication code: 001 113.†
Dunning, M., Abi-Aad, G., Gilbert, D., Gillam, S.,Livett, H. (1998) Turning evidence into everydaypractice. London, King’s Fund.
Ellis, J., Morris, A. (1997) Paediatric benchmarking:a review of its development, Nursing Standard, 12(2), pp.43-46.
Fenner, J., Palmer C (1997) FOCUS ondissemination: draft report. London: Royal Collegeof Psychiatrists’ Research Unit.
Freemantle, N., Harvey, F., Wolf. (1997) Printededucational materials: effects on professionalpractice and health care outcomes. UpdateSoftware. The Cochrane Library, Oxford.
Gupta, L., Ward, J., Hayward, R. (1997) Clinicalpractice guidelines in general practice: a nationalsurvey of recall, attitudes and impact. MedicalJournal of Australia, 166, pp69-72.
Grimshaw, J.M., Russell, I.T. (1993) Effect of clinicalguidelines on medical practice: a systematic reviewof rigorous evaluations. Lancet, 342, pp1317-1320.
Harvey, G., Kitson, A. (1996) Achievingimprovement through quality: an evaluation of thekey factors in the implementation process. Journalof Advanced Nursing, 24, pp185-195.
Lomas, J., Haynes, R.B. (1988) A taxonomy andcritical review of tested strategies for theapplication of clinical practice recommendations:from ‘official’ to ‘individual’ clinical policy.American Journal of Preventative Medicine, 4(Suppl.), pp77-94.
Mittman, B.S., Tonesk, X., Jacobson, P.D. (1992)Implementing clinical practice guidelines: socialinfluence strategies and practitioner behaviourchange. Quality Review Bulletin, 18 (12), pp413-422.
National Health Service Centre for Reviews andDissemination (1999) Getting evidence into practice.Effective Health Care Bulletin, 5 (1), pp1-16.
RCN (2001) Developing an effective clinical governanceframework for children’s acute health care services.London: RCN. Publication code: 001 390.
RCNI (2000) The recognition and assessment ofacute pain in children. London, RCN Publicationcode: 001 114.†
Rogers, E.M. (1995) Diffusion or innovation (4thedition). New York, Free Press.
Scrivener, R., Doorbar, P., Llewellyn, N., Duff.(2000) All about pain. London, RCN. Publicationcode: 001 310.†
Stocking, B. (1985) Initiative and inertia: casestudies in the NHS. London, Nuffield ProvincialHospitals Trust.
Thomas, L., McColl, E., Cullum, N., Rousseau, N.,Soutter, J., Steen, N. (1998) Effect of clinicalguidelines in nursing, midwifery, and the therapies:a systematic review of evaluations. Quality inHealth Care, 7, pp183-91.
Tunis, S.R. et al (1994) Internists’ attitudes aboutclinical practice guidelines. Annals of InternalMedicine, 120, pp956-63.
Zaltman, G., Duncan, R. (1977) Strategies forplanned change. New York, Wiley.
† These publications can be ordered from RCN Publishing Company Ltd, Distribution Department, PO Box 1, Portishead,Bristol BS20 9EG. Priced £5.50 RCN members; £7.50 non-members (£1.50 p&p). All about pain (packs of five) areavailable to members at £1.50 only; non-members £5.95, plus £1.50 p&p.