Embed Size (px)
Citation preview

Individual radiosensitivity
the quest to predict a complex trait
Andrzej WojcikCentre for Radiation Protection Research
Stockholm University

• Whole organism radiosensitivityrefers to radiation‐related mortality due to deterministic effects
• Normal tissue radiosensitivity or clinical radiosensitivityrefers to adverse reactions in non‐target tissues as consequence of radiotherapy (deterministic effects)
• Normal tissue radiosensitivity to non‐cancer, non deterministic effectsrefers to such effects as cataracts and cardio vascular disease
• Susceptibility to radiation carcinogenesisrefers to susceptibility amongst individuals to radiation‐induced cancer
• Tissue radiosensitivity for cancerrefers to in sensitivity of individual tissues to radiation‐induced cancer
• Cellular radiosensitivityrefers to endpoints measured at the cellular level such a DNA damage
Many definitions for the term „radiosensitivity“

Radiosensitivity decreases with age
Biological explanation• age effect: long life expectancy, many cell divisions• sex effect: mainly breast cancer
Children are radiosensitivewith respect to stochastic effects
Radiosensitivity increases with age
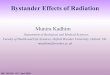
Median lethal dose as a function of age in mice
Biological explanation• Decreasing regenerative capacity of tissues with age
Children are radioresistantwith respect to deterministic effects
ERR for cancer as a function of age and sex in the LSS chort
D.L. Preston et al. Radiat. Res. 168: 1- 64, 2007 J. Spalding and T.T. Trujillo Radiat. Res. 16:125-129, 1962
The importance of defining the endpoint whentalking about individual radiosensitivity

Intrinsic Radiosensitivity in RT
The radiosensitivity of normal tissues and tumors varies considerably among individuals.
For any group of patients given the same treatment, some will experience more severe reactions than others, and a small proportion will experience unacceptable late sequelae.
The means of prospectively identifying in advance which individuals are particularly sensitive to radiation would be of tremendous benefit for clinical treatment.
Source: Eric J. Hall, James D. Cox, in Radiation Oncology (Ninth Edition), 2010

Early RT: 2D planning
Very low precision of dose delivery. Worked in manycases because cells of normal tissue, especially skin, tolerate higher doses of radiation then tumour cells, when applied in a fractionated manner.
Frequent severe side effects, especially to the skin.

Source: Bourland JD. Radiation oncology physics. In: Gunderson LL, Tepper JS, editors. Clinical radiation oncology. 3rd ed. Philadelphia: Saunders; 2012.
Modern intensity modulated external beam radiotherapy (IMRT)

Source: Thariat, J. et al. Nat. Rev. Clin. Oncol. 10, 52–60 (2013)
• The Gy is a unit of absorbed dose corresponding to 1 J per kg• In humans, the LD50 after whole body exposure is 3‐4 Gy
Development of external beam RT for prostate cancer

Despite the precision of dose delivery, some patients develop life‐threatening side effects
radiotherapy
Weeks months years
incide
nce
90 days
Early side effects – mechanism: inflammation
Late side effects – mechanisms: cell death
Idealised scheme of the development of early and late side effects
time
Usual grading of side effects: RTOG scale. Grade 0 (no effects) – 5 (death)

Despite the precision of dose delivery, a few patients develop life‐threatening side effects
early
late
Why do some patients overreact toradiotherapy?
They must be instrinsically radiosensitive!

A commonly made assumption: individual radiosensitivity is an „intrinsic“ trait and the radiosensitivity of cells isolated from an individual correlates with his/her normal tissue radiosensitivity (both for tissue reactions and
stochastic effects)
Functional assaysFibroblasts
Peripheral blood lymphocytes
Functional assays
Cellular radiosensitivity
Individual radiosensitivity
The ideal outcome...
SF2
Source: N. Foray et al. Individual response to ionizing radiation. Mutat Res. 770: 369‐386, 2016
Genomics

Why do we assume that the individual radiosensitivity is an „intrinsic“ (genetically determined) trait ?
There are rare genetic disorders like AT associated with impaired DNA repair capacity. The carriers of such mutations over‐react to radiation and their cells show a high in vitro radiosensitivity. See lecture of Penny Jeggo
Argument 2Argument 2
TCP(tumor control probability)
NTCP(normal tissue complication probability)
therapeuticindex
Individual radiosensitivity of
tumor tissue
Individual radiosensitivity of normal tissue
Herman Holthusen 1934The sigmoid dose‐response relationship is due to differences in individual radiosensitivity
Argument 1Argument 1

Radiation kills cells by damaging the DNAThe fate of an irradiated cell/organism is determined by the level of DNA
damage and the capacity to repair it
Factors which influence cell’s sensitivity to radiation• Cell cycle phase• Oxygen content• Chromatin conformation• DNA repair capacity• Signalling Potential for individual variability
See lecture of Lovisa Lundholm

Homozygotic patients with a DNA repair disorders are very sensitive to radiation. So are their cells when irradiated under in vitro
conditions
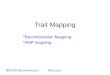
Source: J.M. Pollard and R.A. Gatti Clinical Radiation Sensitivity with DNA repair disordes: an overview. Int. J. Radiat. Oncol. Biol. Phys. 74: 1323‐1331, 2009.
Colony Survival Assay, following 1 Gy
AtaxiaTelangiectasiahomozygotes
AtaxiaTelangiectasiaheterozygotes
NijmegenBreakageSyndome
FanconiAnemia
Ligase 4DeficiencySyndome

Monogenic and multifactorial traits
A mutation involving a monogene may result in a so‐called monogenic disorder. It is a condition wherein a single pair of genes or a single allele is causing the disorder or the disease. There are several types of monogenic disorders. An autosomal monogenic disorder is a type of disorder involving a single gene dysfunction in the autosome. It may be dominant or recessive depending on the type of allele involved. Another type of monogenic disorder is sex‐linked, which involves either X or Y chromosome.
https://www.biologyonline.com/dictionary/monogenic‐trait
A monogenic trait is a trait produced by the effect of a gene or an allele. It is in contrast to a polygenic trait that is controlled by a polygene (multiple genes). Since the trait is produced by a single gene or allele it is less complicated compared with the trait produced by a polygene. It also follows Mendelian inheritance. Accordingly, the two alleles of a heterozygous pair, the allele that is expressed is the dominant allele whereas the allele that is not expressed is the recessive allele.
AT geneChrom 11band 11q22.3
AT is monogenic recessive diseasemeaning that both alleles must beinactivated for the phenotype to appear

Monogenic and multifactorial traits
Pisum sativum
YY gg
Yg Yg Yg Yg
YgYY Yg gg
Y = yellow dominant; g = green recessive
In a healthy person all traits are multifactorial(we only have ca 20 000 genes)
We all remember Mendel from school...Gregor Mendel discovered the inheritance of monogenic traits
Some disorders are monogenic, such as AT or achondroplasia
The inheritance pattern of yellow and green phenotype

Freq
uency
Normal Abnormal
Freq
uency
Severity of the trait
Freq
uency
Liability (predisposition)
NormalDiseased
Qualitative and quantitative traits
Trait Mode of inheritance
Environmental plus stochastic effects
Diseases
QualitativeExamples: DNA repairdefect diseases (such as AT)
SimpleMendelian (monogene)autosomal recessive
Little
Quantitative continuousExamples: height,side effects to radiotherapy in thenormal population
Complexpolygene
Moderate to great
Quantitative thresholdExamples: diabetes,cancer
Complexpolygene
Moderate to great
Mon
ogen
icPo
lygenic,
multifactoria
l, complex
Commonnames
DNA sequences involved are termed Quantitative Trait Loci (QTLs)
dichotomous
continuous
continuous threshold
Individual radiosensitivity among genetically normal people is certainly a polygenic (multifactorial, complex) trait.

René Descartesborn 31. March 1596 in La Haye en Tourainedied 11. February 1650 in Stockholm.
This knowledge leads you to regard an animal body as a machine. Having been made by the hands of God, it is incomparably better organised—and capable of movements that are much more wonderful—than any that can be devised by man, but still it is just a machine.
René Descartes and the mechanistic explanation of life
and its relation to individual radiosensitivity
Source: Discourse on the Method of Rightly Conducting one’s Reason and Seeking Truth in the Sciences, part 5.
In the field of radiation research:We intuitively assume that an organism is characterised by a genetically determined, permanent trait of “intrinsic radiosensitivity” which ‐ when properly assessed ‐ can serve as a predictor of individual response to radiation.

Multifactorial traits are influenced by the genotype, the environment and chance
The pattern of phenotypic expression of a single genotype across a range of environments is called the “norm of reaction”
Height of seven plant cuttings grown in different environments

Why the phenotype of an individual cannot always be predicted from their genome sequence and the
environment that they experienceBurga and Lehner. FEBS Journal 279: 3765–3775, 2012
Vt = Vg + Ve + chance
total variability
genotypic variability
environmental variability
Factors influencing the phenotype of an individual. In addition to the genome and environment experienced by individuals, there are non‐inherited parental genetic variants, parental environment and stochastic molecular variation (noise).

Factors responsible for variance of multifactorial traits
stochastic m
olecular variatio
n (noise)
Modified after: M. Civelek and A. Lusis. Systems genetics approaches to understand complex traits. Nature Genetics Reviews 2014.
Phenotype = genotype + environment + chance

Stochastic nature of cancercell inactivation
Based on: TR Munro and CW Gilbert, Br J Radiol: 34:246‐251, 1961.
Stochastic nature of normal cell inactivation
The sigmoid dose‐response relationship is due to the stochastic nature of radiation induced cell death
In the field of radiation effects there is another “layer of randomness”: the stochastic distribution of lethal events in cells
Poisson (random) distribution of dicentric chromosomes in human lymphocytes exposed to 2 Gy of X‐rays
Cell death due to radiation exposure is a random process

Source: Repair capacity of mouse lung after total body irradiation alone or combined with cyclophosphamide. A. Safwat et al. Radiother Oncol. 40:249‐57, 1996
The ventilation rate (a late lung effect after RT) dose‐response curves after single fraction TBI given at high dose rate (HDR) and low dose rate (LDR) alone or following cyclophosphamide (CTX).
Sigmoidal dose response curves are also observed in genetically identical inbred mice

Relationship between normal distribution of quantitative traits and monogene diseases explained for the trait “height”
Achondroplasia(mutation in FGFR3)
Marfan syndrome(mutation in FBN1)
Monogenic diseases
Data source: NCD Risk Factor Collaboration 2016
Average height as a function of birth year
Normal

Individual radiosensitivity is a multifactorial traitThe distribution of patients according to a “Standardized Total Average Toxicity”
Source: G. C. Barnett et al. Standardized TotalAverage Toxicity score: a scale‐ and grade‐independent measure of late radiotherapy toxicityto facilitate pooling of data from different studies.Int.J.Radiat.Oncol.Biol.Phys. 82 :1065‐1074, 2012.
radiosensitive
radioresistant

RADIATION-INDUCED DAMAGE TO NORMAL TISSUES AFTER RADIOTHERAPY IN PATIENTS TREATED FOR GYNECOLOGIC TUMORS: ASSOCIATION WITH SINGLE
NUCLEOTIDE POLYMORPHISMS IN XRCC1, XRCC3, AND OGG1 GENES AND IN VITRO CHROMOSOMAL RADIOSENSITIVITY IN LYMPHOCYTES
Kim de Ruyck et al. Gent, Belgium
Patients with a low G2-sensitivity appear to have a survival advantage

Int J Radiation Oncol Biol Phys, Vol. 94, No. 3, pp. 450e460, 2016
Low level of ATM nucleoshuttling = high toxicity

High apoptosis = low toxicity
RILA: radiation‐induced lymphocyte apoptosis

O Nuta et al. Correlation between the radiation responses of fibroblasts cultured from individual patients and the risk of late reaction after breast radiotherapy. Cancer Lett. 374:324‐330, 2016.
Residual 53BP1 foci counts 24 h after in vitro irradiation were significantly higher in fibroblasts from RT‐sensitive versus RT‐resistant patients
No association was observed between apoptosis and residual focus levels in breast cancer patient groups with various late toxicities
M. Chua et al. DNA double‐strand break repair and induction of apoptosis in ex vivo irradiated blood lymphocytes in relation to latenormal tissue reactions following breast radiotherapy. Radiat EnvironBiophys. 53:355‐364, 2014.
P. Lobachevsky et al. Compromized DNA repair as a basis for identification of cancer radiotherapy patients with extreme radiosensitivity. Cancer Lett. 383:212‐219, 2016.
The most powerful predictor of extreme toxicity was a combination of the fraction of the unrepairable component of γ‐H2AX foci and repair rate in PBL
K. Brzozowska et al. In vivo versus in vitro individual radiosensitivity analysed in healthy donors and in prostate cancer patients with and without severe side effects after radiotherapy. Int J Radiat Biol. 88: 405–413, 2012.
There is no obvious correlation between clinical and cellular radiosensitivity in lymphocytes (foci and apoptosis) of prostate cancer patients
Selected other studies focusing on residual DNA damage (repair foci), apoptosis and clinical radiosensitivity

Halina Lisowska et al.
Material:38 patients with head-and-neck cancer treated with radiotherapy40 healthy donors
Methods:Analysis of chromosomal aberrations in peripheralblood lymphocytes irradiated in G2 with 2 Gy (G2 assay)
Aims:To find a correlation between the in vitro radiosensitivity and side effects

aber
ratio
ns p
er 1
00 c
ells Figure 5. Relationships between radiation-induced aberration
frequencies and early (left panels) as well as late (right panels) reactions to therapy. Horizontal lines mark the mean values.
Figure 6. Radiation-induced aberrations in lymphocytes ofpatients who survived or not the period of follow up.Horizontal lines mark the mean values.
Is there a correlation between the G2 aberration level and side effects in HN patients?
Enhanced chromosomal radiosensitivity in peripheral blood lymphocytes of
larynx cancer patientsH. Lisowska et al., Int. J. Radiat. Oncol.
Biol. Phys. 66: 1245-1252, 2006
Level of side effects (EORTC/RTOG scale)

Is the comet assay a good endpoint to assess theindividual risk of developing late effects?
Wolfgang Mueller et al. Radiat. Environ. Biophys., 2001
healthy donors
cancer patients
residual damage per group
A retrospective studyVarious cancer entities

Comparative analysis of three functional predictive assays in lymphocytes of patients with breast and gynaecological cancer treated by radiotherapy
Material:35 patients with breast cancer34 patients wit gynecological cancer (endometrium, cervix)
Methods:Analysis of DNA repair kinetics (alkaline comet assay) and chromosomal aberrations (G0 and G2) in peripheralblood lymphocytes irradiated with 2 Gy
Aims:to find a correlation between the in vitro radiosensitivity and side effects
Anna Padjas, Piotr Kedzierawski, Agnieszka Florek, Pawel Kukolowicz, Tomasz Kuszewski, Stanislaw Gózdz, Anna Lankoff, Andrzej Wojcik, Halina Lisowska
J. Contemp Brachyther. 4: 219–226, 2012

Kinetics of DNA repair in lymphocytes of breast cancer (BC) and gynecological cancer (GC) patients
Inserts: distribution of AUC values (area under curve)

Patients and healthy donors: Scatter of G0 and G2 radiation-induced aberration frequencies

Relationships between radiation-induced aberration frequencies plus AUC values and early (black symbols) and late (open symbols) reactions to
radiotherapy, expressed as cumulative grades. earlylateTop panels: breast cancer patients, bottom panels: gynaecological cancer patients.
Panels A: G0 aberrations, panels B: G2 aberrations, panels C: AUC.

Patients with side effectsCo: 0.52 ± 0.2
Patients withoutside effectsCo: 0.35 ± 0.3
Patients with side effectsCo: 0.49 ± 0.5
Patients withoutside effectsCo: 0.64 ± 0.5
Breast cancer patients – skin reactionsS. Skiöld et al. Mutat Res 756: 152– 157, 2013
H&N cancer patients – osteonecrosisD. Danielsson et al. Head Neck 38: 387‐93, 2016
8‐Oxo‐2'‐deoxyguanosine (8‐oxo‐dG ‐major product of DNA oxidation) in blood serum as a predictive marker reflecting coping with oxidative stress

Impact of dose rate and temperature at exposure on the level of radiation‐induced MN in human peripheral blood lymphocytes
Calibration curves for MN among RENEB labs scoring manually(based on table 2 in J Depuydt et al. RENEB intercomparison exercises analyzing micronuclei
(Cytokinesis‐block Micronucleus Assay). Int J Radiat Biol. 2017 Jan;93(1):36‐47.
RT: room temperature at exposure, 37 oC: 37 oC at exposure


Distribution of D0 values of lymphocytes and skin fibroblasts from 22 individuals.
Source: Kushiro et al. Radiat Res 122, 1990
Area of 95% CL
Intra‐ and interindividual variability in MN frequencies in peripheral blood lymphocytes of 10 normal donors exposed to 3.5 Gy at 4 mGy/min.
Source: Vral et al. Tox Let 149, 2004
Normal individuals: lack of correlation between radiosensitivity of lymphocytes and fibroblasts
Normal individuals: high intraindividual variability in radiation‐induced MN frequency
Correlations between cells from the same personand intraindividual variability of response

Findings of the 2017 C1 ICRP WG on individual radiosensitivity arein line with the AGIR 2013 report
Conclusions
Although theoretical and empirical considerations suggest that individuals differ in their response to radiation exposure, no strong and consistently validated biomarkers of tissue effects have been identified to date. There may be several reasons for this:
• Functional assays are not standardised and there has been little attempt to ensure transferability across laboratories. The studies involve different radiation doses, dose rates, parameters, and assay conditions;
• Replication and validation studies are rarely carried out;
• Patient cohorts are heterogeneous, and different scales are often used to quantify adverse tissue effects
• Study designs vary considerably, and few involve power calculation and multivariate analysis.
Do sensitive and specific biomarkers of individual radiosensitivity exist?
Annals of the ICRP 2017
Studies published during 2013‐2017
• 11 studies using the gamma‐H2AX/53BP1/ATM focus assay (functional assays)
• 7 studies investigating chromosomal aberrations, micronuclei, apoptosis, and oxidative stress markers (functional assays)
• 12 studies investigating SNPs in selected genes
• 4 studies using the GWAS approach

Biomarkers of individual sensitivity to radiation‐induced cancer
• A factor which contributes to intrinsic cancer susceptibilityis the genetic background which is associated with genomic instability leading to an increased level of mutations and to sensitivity to environmental factors.
• Genomic instability can be identified as increased spontaneous or radiation‐induced frequency of chromosomal aberrations. The latter is called the Mutagen Sensitivity Assay. Radiation can be substituted by bleomycin (BLM).

Normaldonors
Donorswith geneticdisorders
„cancer‐prone“
Cancerpatients
Tumourcells
A high chromosomal radiosensitivity of skin fibroblasts is a hallmark of cancer susceptibility

The idea of the study
Find a database withspontaneous aberration scoresin lymphocytes of a cohort
Follow up the cohort for cancer incidence/mortality
Correlate the aberration score with RR (calculated as SIR, SMR or HR)
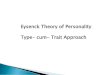
High spontaneous aberration frequency in lymphocytes is a hallmark of cancer susceptibility
Low aberration score
High aberration score
Median aberration score
Kaplan–Meier curves for total cancer incidence tertile of CA frequency based on pooled data from 11 European cohorts. Cancer‐free probability refers to time from CA test to the first cancer diagnosis.
Source: S. Bonassi et al. Chromosomal aberration frequency in lymphocytes predicts the risk of cancer: results from a pooled cohort study of 22 358 subjects in 11 countries. Carcinogenesis 29: 1178–1183, 2008.
High CA frequency was associated with the risk of stomach cancer.
The presence of chromosome instability stomach cancers may be linked to the metabolisms of agents involved in stomach carcinogenesis, such as folic acid and vitamin B12.
However, Helicobacterpylori infection is also known to increase the level of chromosomal damage in lymphocytes.

10%
40%
Cytogenet Genome Res 104:365–370 (2004)
Lymphocytes of breast cancer patients show an enhanced radiation‐induced aberration frequency (G2 test)
G2 chromosomal radiosensitivity of normal donors and breast cancer patients. The dashed vertical lines indicate the cut‐off point between a normal and a sensitive response.
G2 chromosomal radiosensitivity of patients with breast cancer selected as being sensitive in the assay and first degree relatives. The dashed vertical lines indicate the cut‐off point between a normal and asensitive response, from historic control data (see Fig. to the left).
A heritable trait?
63%

Source: Lisowska et al. Int. J. Radiation Oncology Biol. Phys., 66: 1245–1252, 2006
H&N cancer
Source: Brzozowska et al. Int. J. Radiat. Biol. 88: 405–413, 2012
Prostate cancer
Source: Padjas, PhD thesis, Kielce, unpublished
Gynecological cancers
Lymphocytes of patients with some other cancers may also show enhanced radiation‐inducedaberration frequencies

Is a high mutagen sensitivity really a marker of genetically‐determined cancer susceptibility?
*
M. Khosravifarsani et al. The study of radiosensitivity in left handed compared to right handed healthy women.
BMC Medical Physics 12:3, 2012

No evidence of genomic instability in survivors of childhood cancers

Can you reduce your individual radiosusceptibility?Remember: all risks are conditional
• Cancer risk models recommended for use by the ICRP depend to a large extent on excess relative as opposed to excess absolute risk.
• This suggests that the risk of radiation‐induced cancer is to a great extent determined by the same factors that determine cancer risk in the general population.
• Therefore, measures that reduce population cancer risk incidence and mortality should help reduce the incidence of radiation‐associated cancer in populations.
• Can the risk of radiation‐induced cancer be reduced after a radiation exposure has taken place? • If this is the case then people who have been exposed to radiation (e.g. due to Chernobyl or
Fukushima Daiichi accidents) can ‐ to some extent ‐ control their risk. • This can have an enormous implication for their well being and, eventually, for their health.

Cancer risk is conditional
Yoshida et al. PNAS 94:265‐2619, 1997
Survival of mice kept on different caloric restrictions and exposedto a single dose of ionising radiation
No restriction, 0 Gy
No restriction, 3 Gy
Restriction, 0 Gy
Restriction, 3 Gy

THE END