Embed Size (px)
DESCRIPTION
The Quality Colloquium at Harvard University August 27, 2003. Patient Safety Organizational Readiness Assessment Tool. Louis H. Diamond, MDBeverly A. Collins, MD Vice President & Medical DirectorMedical Director MedstatDelmarva Foundation for Medical Care. - PowerPoint PPT Presentation
Citation preview

The Quality Colloquium at Harvard UniversityAugust 27, 2003
Patient Safety Organizational Readiness Assessment Tool
Louis H. Diamond, MD Beverly A. Collins, MDVice President & Medical Director Medical DirectorMedstat Delmarva Foundation for Medical Care

2 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Employee survey
An Agenda to Improve Patient Safety
Leadership buy-in and commitment
Conduct OrganizationalReadiness Assessment*
Establish a non-blame culture
Train staff in thesafety sciences
Make errors visible**
Conduct root causeanalysis
Implement best practice
Disseminate and facilitate adoption
of best practice *Dimensions: Strategic, Cultural, etc. **Employee reporting, patient reporting, medical record review, data mining***Point of care and near term
Make tools available
to patientsand healthcareprofessionals***

3 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Crossing the Quality Chasm
Leadership
Statement of Purpose
Prioritize
OrganizationalChanges
New SetPrinciples
Create IT Infrastructure
EBMDecision Support
ToolPrepare
Workforce
Restructure PaymentReward Improvement
Ref: Adapted from IOM Report: March 01.

4 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Discussion Outline
• Overview of the Patient Safety Organizational
Assessment Tool (PSOAT)
• Conceptual Framework
• Project Steps
• Results of Delmarva Assessment

5 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Objectives of the Assessment
• Use an evidence-based process to:
– Provide gap analysis
– Highlight practices that contribute to errors
– Jump start safety programs
– Comply with regulatory requirements

6 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Patient Safety Organizational Assessment Tool Description
• Content
– 100+ focused practices from the literature organized by:
• Strategic
• Structural
• Cultural
• Technical
• Medication Administration
• Patient Involvement

7 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Literature Sources
• National Patient Safety Foundation, Institute of Medicine
• Agency for Healthcare Research and Quality
• Literature Citation Systems– PubMed, MEDLINE, MDConsult
• MEDSTAT internal resources– Clinical reference database (6000+ references)
• Medical and Patient Safety web sites and listservs
• Web engines

8 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Description of Shortell Framework
Category Description Examples
Strategic Organization articulates what is important; organization provides resources and focus
Mission statement Organizational safety plan Executive leadership Board involvement
Cultural Underlying beliefs, values, norms and behaviors
Open non-punitive milieu Teamwork Learning from mistakes
Technical Informational services and education
Safety training programs Information systems related
to safety Standards
Structural Operational structures for organizational learning
Best practices sharing Electronic communication
for shared learning Committee structures
Shortell S. Assessing the impact of Continuous Quality Improvement on Clinical Practice: What it will take to accelerate progress. The Milbank Quarterly, 76(4) 1998

9 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Impact on Quality Improvement
Strategic Cultural Technical Structural Results
X X X No significant results on anything really important
X X X Small, temporary effects; no lasting impact
X X X Frustration and false starts
X X X Inability to capture the learning and spread it throughout the organization
X X X X Lasting, organization-wide impact
Shortell S. Assessing the impact of Continuous Quality Improvement on Clinical Practice: What it will take to accelerate progress. The Milbank Quarterly, 76(4) 1998
X = fully present

10 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Impact on Safety Improvement
Cultural•no blame•process focused
Strategic•mission•executive leadership
Technical• training• information
systems
Patient Safety
Structural•committees• information sharing
Ref: Shortell: Milbank Quarterly, 76(4)1998

11 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Value to Participating
• Avoid costs
• Focus resources/attention
• Market to community
• Increase collaboration

12 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Project Steps
• Delmarva and MEDSTAT partner to customize and offer tool
to MD and DC health care organizations
• Invitation to participants
• 42 organizations assigned IDs; 24 completed
• Bedsize - 8 had <150 beds; 16 had >=150 beds
• Results aggregated and analyzed
• Obtain participant feedback

13 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Findings

14 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Overview of Results: Level of Action
Medication Administration
Structural
Strategic
Patient Involvement
Cultural
Technical
HighAction
LowAction

15 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
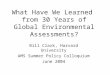
Percentage Response by Section
23.3
%65
.6%
23.5
%67
.2%
20.5
%69
.3%
30.4
%55
.4%
33.0
%49
.2%
20.3
%71
.0%
26.0
%61
.2%
0%10%20%30%40%50%60%70%80%
Ove
rall
Stra
tegi
c
Stru
ctur
al
Cul
tura
l
Tech
nica
l
Med
icat
ion
Patie
nt In
v
No Action*
High Action**
Response
*No Action – Answered 1 or 2 on assessment tool. 1 = Not considering the practice; 2 = Discussed the practice, but no action taken to put into place.
**High Action – Answered 4 or 5 on assessment tool. 4 = Considerable action taken to put practice into place; 5 = The practice is fully implemented in organization.
# of Questions
101 17 24 10 11 37 2

16 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
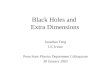
Difference by Bed Size: Patient Involvement
14.9
%
65.7
%
28.8
%
52.3
%
0%
10%
20%
30%
40%
50%
60%
70%
1-15
0B
eds
151+
Bed
s
No Action*
High Action**
Response
*No Action – Answered 1 or 2 on assessment tool. 1 = Not considering the practice; 2 = Discussed the practice, but no action taken to put practice into place.
**High Action – Answered 4 or 5 on assessment tool. 4 = Considerable action taken to put practice into place; 5 = The practice is fully implemented in organization.

17 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Strategic - Low vs. High Action: 17 Questions
Not considering or no action taken (>60% of Responses)
Practice fully implemented or considerable action taken (>90% of Responses)
Mission statement includes patient
safety Written patient safety plan-board
reviewed
Employee patient safety handbook Section on safety improvement in annual review
Established safety program; focus on culture

18 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Structural - Low vs. High Action: 24 Questions
Not considering or no action taken (>60% of Responses)
Practice fully implemented or considerable action taken (>90% of Responses)
Patient safety discussed at staff
meetings Safety reports reviewed by
multidisciplinary teams
HR policy for avoiding potential safety errors due to fatigue, stress
CMS compliant restraint policy
Fall protocol in place
Infection control program in place with monitors/trends
Risk management and patient safety program integrated
Life safety integrated in patient safety

19 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Cultural - Low vs. High Action: 10 Questions
Not considering or no action taken (>60% of Responses)
Practice fully implemented or considerable action taken (>90% of Responses)
Financial reward for suggested improvement
Encourage near miss reporting for improvement
Annual survey of perceptions on culture
Simple, confidential, standardized reporting forms
No ‘incident reports’ – rename No incident reports in personnel files
Use root cause analysis for improvement

20 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Technical - Low vs. High Action: 11 Questions
Not considering or no action taken (>60% of Responses)
Practice fully implemented or considerable action taken (>90% of Responses)
Videotape procedures (e.g. surgery) for improvement
Voluntary, open, confidential, non-punitive, objective error reporting system in place
Bar code blood transfusions
IT for order entry

21 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Medication Safety - Low vs. High Action: 37 Questions
Not considering or no action taken (>60% of Responses)
Practice fully implemented or considerable action taken (>90% of Responses)
Electronic xmit of orders;
Information system available to all clinical staff
Ongoing education of drug administration
Bar coding at point of administration
Allergy info visible on patient orders
Lab/vital sign monitoring in place for hazardous drugs
All drug orders reviewed by pharmacist before dispensing
Lab and medical records at bedside
No rarely used narcotics in patient care areas
Morphine – limited doses, well marked

22 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Medication Safety - Low vs. High Action: 37 Questions
Not considering or no action taken (>60% of Responses)
Practice fully implemented or considerable action taken (>90% of Responses)
No stocking or unique storage of
look-alike drugs
Pharmacy or manufacturer responsible for admixing or preparing unit doses
Antidotes for high risk drugs widely available
Standardized stocking of drugs on unit
Standardized drug admin times

23 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Medication Safety - Low vs. High Action: 37 Questions
Not considering or no action taken (>60% of Responses)
Practice fully implemented or considerable action taken (>90% of Responses)
Drug information widely available
for new or unusual drugs
IV compatibility charts on care unit
Alphabetic list of drugs by brand name/generic on care unit
24/7 Pharmacist staffing

24 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Recommendations Based Upon Survey Results

25 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Strategic/Structural
• Incorporate patient safety into mission statement
• Improve policy and departmental standards to incorporate safety discussion into operational meetings

26 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Cultural
• Raise awareness at all levels of organization
• Reward staff for improvements; consider
alternative reward systems
• Celebrate achievements
• Gather baseline staff perceptions for both
information and awareness

27 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03

28 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Technical
• Bar coding for patient identification, patient tracking, CPOE
• Explore other techniques for potential error review e.g. user centered design
• Electronic decision support for clinicians

29 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Medication Safety
• Standard policies in place to monitor patients on hazardous drugs
• Availability of medication information system to all clinical staff dealing with a patient
• Bar-coding to detect adverse drug reaction and other administration errors at point of care

30 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Patient Involvement
• Educate patients and families on key safety issues regarding their care while hospitalized
• Educate patients and families about medication safety after discharge
• Develop safety educational programs geared towards patients
• Be mindful of following hand washing procedures

31 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03

32 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03

33 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Questions
Discussion
&

34 Copyright 2003 Thomson MedstatHarvard Quality Colloquium 8-27-03
Contacts
Louis H. DiamondMedstat4301 Connecticut Avenue, NW, Suite 330Washington, DC 20008202-719-7833 Fax: 202-719-7866Email: [email protected]
Beverly A. CollinsDelmarva Foundation for Medical Care7240 Parkway Drive, Suite 400Hanover, MD 21076410-712-7404 Fax: 410-712-4357Email: [email protected]