Embed Size (px)
Citation preview

IN the 1960s, wellbe-ing was a rebel child, adopted by tie dye and ripped jeans-wearing devotees of the alternative health and lifestyle move-ment.
Fast forward to today, wellbeing has gone mainstream. Its supporters are just as likely to be wearing a suit and tie. Some even walk the cor-
ridors of power, such as Professor Richard Layard from the London School of Economics, who sits in the ermine-clad confines of the UK’s House of Lords.
It was in his landmark 2006 book, Happiness — Lessons from a
New Science, that Professor Layard wrote pennies are not necessarily from heaven: “There is a paradox at the heart of our lives. All the evidence shows that, on average, people have grown no happier in the last 50 years, even as average incomes have more than doubled.”
This statement struck a chord in the material world, eventually becoming a crescendo following the disastrous singular pursuit of Mammon exposed by the global financial crisis of 2008.
In its aftermath the UK Prime Minister, David Cameron, announced that there’s more to life than money. “It’s time we focused not just on GDP but on GWB — general wellbeing,” he declared.
In the context of health and dis-ease, the wellbeing movement has
become important. Population studies have found a reduction in all-cause mortality associated with high wellbeing levels that is of the same magnitude as not smoking.1,2 The US Centers for Disease Con-trol and Prevention (CDC), for instance, now states that “wellbe-ing is a valid population outcome measure, beyond morbidity, mor-tality, and economic status”.
What is wellbeing?So then, life is more than just about money, it’s about wellbeing. But what is well-being?
When the average person talks about wellbeing, they often sim-ply mean feeling happy, says Dr Melissa Weinberg, honorary fellow at Deakin University’s Australian Centre for Quality of Life.
“However, the wealth of research conducted on wellbeing has found
it’s more nuanced and complex.”Wellbeing may be defined as a
holistic understanding of life — be it for an individual or a population group — that is made up of multi-ple factors or domains.
Three years ago, the OECD set out to measure something more than the cash of economic growth and came up with its Better Life Index, which it said could be used to rate countries on their wellbeing performance.
The index set out a series of differ-ent categories — the ‘material living conditions’ category (which includes income, housing and jobs) and a ‘quality of life’ category (which includes objective factors like health status and social connections, as well as subjective wellbeing).
Importantly, all these factors interconnect with each other in a two-way flow, says Dr Weinberg.
“One of the key tasks of wellbe-ing researchers is to identify and translate the complexity that is a
www.australiandoctor.com.au 3 July 2015 | Australian Doctor | 31
The pursuit of happIness
populaTIon sTudIes have found a reducTIon In all-cause morTalITy assocIaTed wITh hIgh
wellbeIng levels ThaT Is of The same magnITude as noT smokIng.
News Review
cont’d next page
JOHN KRON charts the rise of the wellbeing movement and what it means for doctors.

result of the interconnections,” she says.
“Money may improve health status and overall wellbeing for a person on a low income, but a rich person can be unhappy due to poor relationships.”
In another example, parents can experience increased anxi-ety, reduced sleep and less time to do activities they enjoy. How-ever, their overall wellbeing may be counterbalanced by feeling a greater sense of meaning and pur-pose in life because of the role of their children in their lives.
Of all these interconnecting fac-tors, it’s subjective wellbeing that’s a particular focus of attention for many in the wellbeing movement. Subjective wellbeing is the factor that most closely relates to happi-ness, says Dr Weinberg.
However “the research shows that subjective wellbeing is a partic-ular type of happiness. As opposed to short-term happiness, such as when you eat an ice-cream on a hot day, subjective wellbeing is a deeper, underlying long-term mood of happiness and contentment”, she says.
“This mood can be measured by asking: ‘How satisfied are you with your life?’ or more specific ques-tions such as ‘How satisfied are you with your relationships?’ or ‘your community connections?’”
Not fluffyThe medical profession hasn’t traditionally taken a great inter-est in wellbeing, perhaps because many doctors regard it as ‘nice, but fluffy’.
“However, just because some-thing is difficult and complex, doesn’t make it fluffy,” says Profes-sor Jill Gordon, a Sydney GP and chair of the RACGP’s psychologi-cal medicine special interest group.
“The connection between well-being and health isn’t always obvi-ous. A patient may experience low wellbeing, which makes them do less physical activity, contributing to the development of a condition such as osteoporosis years later,” says Professor Gordon.
“Population studies are good at identifying such associations between mental wellbeing and physical flourishing, and the body of evidence they’ve produced is impressive.”
“Enjoyment of life”, another example of subjective wellbeing, was the key measure question in a longitudinal study of 50-plus-year-olds in England.3
The study found that “enjoyment of life” was associated with a 28% reduction in mortality risk, even after taking into account depres-sion, as well as health behaviours and socioeconomic factors.
The finding suggests that it offered a protective benefit for both unhealthy and healthy people.
Studies have also found evidence to suggest that wellbeing is related to positive health behaviours, which may help to explain observed reductions in mortality due to car-diovascular disease and renal dis-ease.4,5,6,7 It is also associated with reduced infection risk such as the common cold, improved wound healing and speedier recovery from illness, says Professor Gordon.7,8,9
It’s been the accumulation of such research that led to the US CDC now regarding wellbeing as effective and beneficial for public health.
Its key reasons are that wellbeing “integrates mental health and phys-ical health resulting in more holistic approaches to disease prevention and health promotion ... advances in psychology, neuroscience and measurement theory suggest that wellbeing can be measured with some degree of accuracy” and it is “an outcome that is meaningful to the public”.
Patchy actionOnce wellbeing is identified as important, the next step should be to do something about it. But while programs to measure wellbe-ing have been established, such as the Australian Unity Well-being Index, conducted by the Austral-ian Centre on Quality of Life, much less is being done to actually improve wellbeing.
For instance, the Victorian Gov-ernment has a Community Indica-tors program that collects wellbeing data to “improve citizen engage-ment, community planning and policymaking”. However, there’s no compulsion for local councils or state departments to act on the program’s findings.
“Australia is slower than nations such as the UK,” says Dr Nicholas Gruen, author of the Fairfax-Lat-eral Economics Wellbeing Index, published by the Age and Sydney Morning Herald.
“Sadly we’re behind on this stuff,
and countries that have had better leadership on both sides of the political aisle, like the UK, are set-ting the pace,” he says.
A stand-out example from the UK is the Community Wellbeing Practice, where GPs in 17 practices in Halton, north-east England, are able to refer patients for a ‘well-being review’.
As a result, they can be recomm-ended free services and support networks, which can give these patients access to hobby and inter-est groups, life skills courses, and social connections such as comm-unity gardens.
The program delivers 4000 inter-ventions per year, with an assess-ment finding that 67% of patients improve their subjective wellbe-ing and 55% have a reduction in depression symptoms.
There are some positive exam-ples of wellbeing interventions in Australia. The Family by Family service — which runs in Marion, Adelaide, and Mount Druitt, Syd-ney — coaches and links up fami-lies to develop each other’s goals and connections, which helps connect family members to new opportunities, and offers positive feedback and mutual support.
Going too far?The flipside of needing to do more with wellbeing, has in some cases gone too far. First there is com-mercial exploitation. Soft-drink giant Coca-Cola, unsurprisingly, has a happiness website that credi-bly discusses the “modern science,” but then concludes with the advice:
“Open an ice-cold Coca-Cola and choose happiness!”
More disturbing are cases of wellbeing used as justifications for getting rid of people you don’t like.
There have been examples of psy-chologists demanding that employ-ees unenthusiastic about wellbeing interventions in the workplace be sacked because their lack of “engagement” is considered conta-gious, according to a recent book, The Happiness Industry: How the Government and Big Business Sold Us Well-Being.
Perhaps the greatest concern is the push for everybody to be hap-pier.
“Wellbeing is thrown around in the same way as fad cures for all sorts of diseases ... [however] there’s no evidence a person who’s already experiencing normal sub-jective wellbeing levels can be made chronically happier,” says Dr Weinberg.
In fact, the research shows that subjective wellbeing is governed by homeostasis, in the same way as core body temperature.
“Subjective wellbeing can vary as a person deals with life events such as a new medical diagnosis. But over time there’s adaptation and subjective wellbeing usually goes back to a set point after we utilise our resources such as social supp-ort,” says Dr Weinberg. “But at the same time, subjective wellbeing homeostasis can break down when a person is unable to adapt to nega-tive life events.
“That’s when the risk of medical conditions, such as depression and
anxiety, are increased.”Twin studies have suggested that
up to 40% of subjective wellbeing is genetic, determining features such as whether a person tends to be pessimistic.10
“A naturally pessimistic ... per-son should not be made to feel that they’re failing for not being hap-pier more often,” says Professor Gordon.
“Wellbeing and happiness also shouldn’t be conflated. It‘s not realistic to expect to feel happy all the time ... we can, however, exper-ience a sense of wellbeing if we pay attention to the things that are important to us as individuals.”
The message is that while the ‘Times are a-Changin’ with well-being, it’s important to ensure it doesn’t become an evangelistic movement. l
References1. Applied Psychology: Health and
Wellbeing 2011; 3:1-43.2. Behavior Genetics 2015; 45:137-56.3. Archives of Internal Medicine 2012;
172:273-75.4. Lancet 2015; 385:640-48.5. European Heart Journal 2010;
31:1065-70.6. Psychosomatic Medicine 2008;
70:741-56.7. Journal of Behavorial Medicine
2012; 35:538-47.8. Psychosomatic Medicine 2003;
65:652-57.9. UK Department of Health.
Wellbeing; Why it matters for health policy. London, 2014.
10. Behavior Genetics 2009; 39:605-15.
happIness
Top 211. Switzerland
2. Iceland3. Denmark4. Norway5. Canada6. Finland
7. Netherlands8. Sweden
9. New Zealand10. AuStrAlIA
11. Israel12. Costa rica
13. Austria14. Mexico
15. uS16. Brazil
17. luxembourg18. Ireland
19. Belgium20. uAE21. uK
Source: UN Sustainable Development Solutions Network
32 | Australian Doctor | 3 July 2015 www.australiandoctor.com.au
from previous page
‘a naTurally pessImIsTIc ... person should noT be made To feel ThaT They’re faIlIng for noT beIng happIer more ofTen.’ — Professor Gordon
chair of the RACGP’s psychological medicine special interest group
News Review
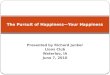
AustrAliA rAnks wellAustralia ranks highly on wellbeing compared with the rest of the world. We come in at 10th, according to the latest World
Happiness Report of 158 countries, produced this year by the UN Sustainable Development Solutions Network. The lowest-
ranked countries were sub-Saharan African nations Togo, Benin and Central African Republic. In the first World Happiness
Report (2010), Australia was ranked ninth.
Source: UN Sustainable Development Solutions Network.
1
21
9
10
15
16
12
14
13
20
11
1873
1917
24
86
5
Dr Melissa weinberg, of the Australian Centre for Quality of life, says subjective wellbeing is the factor that most closely relates to happiness.

34 | Australian Doctor | 3 July 2015 www.australiandoctor.com.au
2 DAY SEMINAR
14-15 NOVEMBERMANLY BEACH | SYDNEY
For full agenda and registration detailswww.ruraldoctorseminar.com.au
News Review
happiness and care on the cancer ward
I HAD been mulling over the meaning of happi-ness a whole month as I cared for a patient near-
ing the end of her life. She had young children, a supportive husband and, most of all, an abiding faith that allowed her to imagine heaven as a better place now that treatment was no longer possible for her advanced cancer.
It struck me as extraor-dinary that she could mus-ter such unflappable peace in the face of something as momentous as death. But I also thought that if everyone shared a drop of her equa-nimity, the inevitability of dying would be so much eas-ier on all of us, the deceased and the ones left behind.
Some days on the ward, happiness is avoiding the fate of many of my patients. Eve-ryone who works in oncol-ogy is only too aware of the flick of the wheel of fortune
that transforms happiness into its opposite.
But if being an oncologist is sobering stuff, it’s also a job where happiness steals into your life in unexpected ways. My working week is filled with diverse roles ... but my favourite moments in medicine are those spent in direct patient care.
Lately, I have been hearing a lot about disillusionment in medicine. How doctors would not recommend the profession to their children. How doctors are burning out amid skyrocketing rates of drug and alcohol abuse, and mental illness.
Medicine is just another form of consumerism. Bureaucrats breathe down our necks, tired of our inabil-ity to distinguish cost-effec-tive measures from plainly wasteful ones. Patients no longer regard us with the level of respect, or even affec-
tion, that they once did.Here is what I have real-
ised. More beds, shiny wards and more scanners don’t make anyone happy. More beds without more staff means more patients per overworked doctor and nurse. More scanners mean more scans but not necessar-ily better care.
I have rarely met a patient who felt better for being on a new ward that was staffed by jaded doctors and nurses. So while pouring money into medicine is usually well-intentioned, it’s a stretch to
say it makes doctors happy.What does make doctors
happy is happy patients. In a profession where established beliefs are routinely turned on their heads, this seems to be a fairly irrefutable one. In fact, the capacity to make a palpable difference to the human condition is what sets medicine apart from other prestigious jobs. But how can the modern doctor make the modern patient happy?
In this age of unrelenting dissatisfaction with every aspect of our life, is it even possible to aim for a happy
patient, or should doctors just accept that customer ser-vice delivered with civility, efficiency and accuracy ought to be enough?
This would be a shame because the wonder of medi-cine lies in its human touch. The rest Google keeps getting better at. Take the example of a skin rash that a patient took to Google for a diagno-sis. Google reassured her that the rash should get better by itself. It took the triage nurse’s radar to sense that although Google was right about the rash, it couldn’t possibly
diagnose the patient’s distress at remembering that a similar rash had heralded the death of her mother from leukae-mia when the patient was merely seven years old.
I have met some wonderful doctors in my career, loved by patients and their colleagues. They all have something in common — they have honed the art of communication.
These doctors look at their computer screen less and their patients more. They smile, wince, celebrate and commis-erate with their patients and they look them in the eye.
I asked a very busy GP once how he managed to keep so many patients happy. “I behave as if for those 10 minutes the patient before me is my only concern in the world,” he said. l
Dr Srivastava is an oncologist and author based in Melbourne at Monash Health. this is an edited extract of an article published by the Conversation for their collection ‘On Happiness: New Ideas for the twenty-First Century’. See: bit.ly/1SIMD1t
Oncologist Dr Ranjana Srivastava says happiness can be the heart of medicine.
Dr srivastava says happy
patients make doctors happy.